Back to Journals » Journal of Pain Research » Volume 19
Liposomal Bupivacaine for Serratus Anterior Plane Block in Modified Radical Mastectomy: Protocol for a Randomized, Double-Blind Trial Evaluating Pain-Related and Early Recovery Outcomes
Authors Wei M, Tong J, Pang Y, Zhou X, Qiu Y, Wang Z ![]()
Received 27 April 2026
Accepted for publication 27 June 2026
Published 8 July 2026 Volume 2026:19 617864
DOI https://doi.org/10.2147/JPR.S617864
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Karina Gritsenko
Mengping Wei1,*, Jie Tong1,*, Yanrong Pang2,*, Xiushi Zhou3, Yue Qiu4, Zhiyao Wang2
1Department of Anesthesiology, Zhongshan Hospital (Xiamen), Fudan University, Xiamen, Fujian, People’s Republic of China; 2Department of Anesthesiology, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China; 3Department of Population Health Sciences, Duke University School of Medicine, Durham, NC, USA; 4Department of Anesthesiology and Perioperative Medicine, University of Pittsburgh, School of Medicine, Pittsburgh, PA, USA
*These authors contributed equally to this work
Correspondence: Zhiyao Wang, Department of Anesthesiology, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China, Email [email protected]
Purpose: Modified radical mastectomy is commonly associated with substantial postoperative pain, opioid use and impaired early recovery. Serratus anterior plane block (SAPB) is increasingly used as part of multimodal analgesia for breast surgery. Although SAPB and quality of recovery outcomes have both been studied in breast surgery, published evidence regarding the use of liposomal bupivacaine in SAPB for modified radical mastectomy remains limited. This trial was designed to address whether adding liposomal bupivacaine to bupivacaine hydrochloride (bupivacaine HCl) for SAPB improves pain-related and early recovery outcomes after surgery.
Patients and Methods: This is a prospective, randomized, double-blind, controlled trial. Seventy-six patients undergoing elective modified radical mastectomy for breast cancer are being randomly assigned in a 1:1 ratio to receive unilateral ultrasound-guided SAPB after induction of general anesthesia and before skin incision with either liposomal bupivacaine plus bupivacaine HCl (Group L) or bupivacaine HCl alone (Group B). The primary endpoint is the Quality of Recovery-15 (QoR-15) score at 24 h postoperatively. Secondary outcomes include postoperative pain intensity up to 72 h, opioid-related outcomes expressed as morphine milligram equivalents (MME), QoR-15 scores at 48 and 72 h, time to first demand of patient-controlled analgesia (PCA), Overall Benefit of Analgesia Score (OBAS), postoperative nausea and vomiting, sleep quality, perioperative complications and patient-reported neuropathic pain symptoms at 3 months assessed using the Douleur Neuropathique 4 interview (DN4i). The primary analysis will follow the intention-to-treat (ITT) principle. Prespecified sensitivity analyses will include a modified ITT (mITT) set excluding participants who did not receive the allocated SAPB injection and an exploratory per-protocol (PP) set excluding major protocol deviations.
Conclusion: This trial will evaluate whether adding liposomal bupivacaine to bupivacaine HCl for SAPB provides additional benefit for pain-related and early recovery outcomes after modified radical mastectomy compared with SAPB using bupivacaine HCl alone.
Trial Registration: Chinese Clinical Trial Registry, Registration No. ChiCTR2500111732. Registered on 5 November 2025.
Keywords: bupivacaine, liposomes, nerve block, ultrasonography, mastectomy, patient-reported outcome measures
Introduction
Breast surgery is frequently associated with moderate-to-severe postoperative pain, which may impair early mobilization, delay functional recovery, and increase the risk of postoperative nausea and vomiting and chronic pain development.1–4 Optimal perioperative analgesia therefore remains a key component of postoperative recovery.3,5,6
The serratus anterior plane block (SAPB) has emerged as an effective regional anesthesia technique for breast surgery by providing analgesia to the lateral thoracic wall through blockade of the thoracic intercostal nerves. When combined with general anesthesia and multimodal analgesia, SAPB has been shown to reduce postoperative pain intensity and opioid consumption, and opioid-related adverse events.7–11 However, the duration of analgesia provided by conventional local anesthetics is often limited, which may not be sufficient for sustained pain control during the early postoperative recovery.12,13
The Quality of Recovery-15 (QoR-15) questionnaire is a validated patient-reported measure of early postoperative recovery. It has been widely used in perioperative research and captures multidimensional postoperative recovery including physical comfort, emotional state, physical independence, psychological support, and pain.3,8 Several breast studies of regional anesthesia have included the QoR-15 as an outcome, but evidence that SAPB with conventional local anesthetic improves QoR-15 is sparse and inconsistent.13,14 A sham-controlled trial by Abdallah et al found that single-injection deep SAPB did not significantly improve QoR-15 or secondary analgesic outcomes in ambulatory breast cancer surgery.13 This null result indicates that recovery benefit cannot be assumed with conventional SAPB alone and supports the need to evaluate whether alternative SAPB strategies may provide measurable recovery benefit in more invasive breast surgery settings such as modified radical mastectomy. One prior study suggested that deep SAPB with dexmedetomidine as an adjuvant to ropivacaine may improve QoR-15 after modified radical mastectomy.15 Together with the inconsistent QoR-15 findings for conventional SAPB, these findings support further evaluation of optimized SAPB strategies in this surgical setting.
Liposomal bupivacaine is a long-acting formulation that provides prolonged local anesthetic exposure. Although it has been used in various surgical settings, existing findings regarding its clinical benefit in fascial plane blocks remain limited.16–18 In particular, the impact of SAPB using liposomal bupivacaine on QoR-15 following modified radical mastectomy has not been adequately evaluated. Compared with adjunct-based approaches, a liposomal bupivacaine-based strategy represents a clinically relevant add-on approach that warrants evaluation against SAPB with bupivacaine hydrochloride (bupivacaine HCl) alone.
In this context, the key clinical question is not whether SAPB provides analgesia, but whether adding liposomal bupivacaine to bupivacaine HCl for SAPB provides additional clinical benefit compared with SAPB using bupivacaine HCl alone after a modified radical mastectomy. Therefore, we designed this randomized, double-blind, controlled trial to evaluate this add-on liposomal bupivacaine SAPB strategy in patients undergoing modified radical mastectomy. We hypothesize that this strategy will improve early postoperative recovery as measured by the QoR-15, while also influencing pain burden, opioid exposure, and related recovery outcomes.
Materials and Methods
Study Design
This study is a prospective, randomized, double-blind, controlled clinical trial conducted at a single tertiary medical center. The study was approved by the Ethics Committee of Zhongshan Hospital (Xiamen Branch), Fudan University (Approval No. B2025-071R) on 8 October 2025 and was registered with the Chinese Clinical Trial Registry (Registration No. ChiCTR2500111732) on 5 November 2025. Written informed consent will be obtained from all participants. The trial will be conducted in accordance with the Declaration of Helsinki and reported following the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) statement.19 The completed SPIRIT checklist is provided as Supplementary File 1. A total of 76 eligible patients (n = 38 per group) will be enrolled from November 2025, and the recruitment phase will continue until the predetermined sample size is achieved. The study flow diagram is shown in Figure 1. Prior meta-analyses and randomized trials suggested that SAPB can reduce postoperative pain and opioid consumption in breast surgery.7–10 Accordingly, both groups will receive SAPB as part of multimodal analgesia.
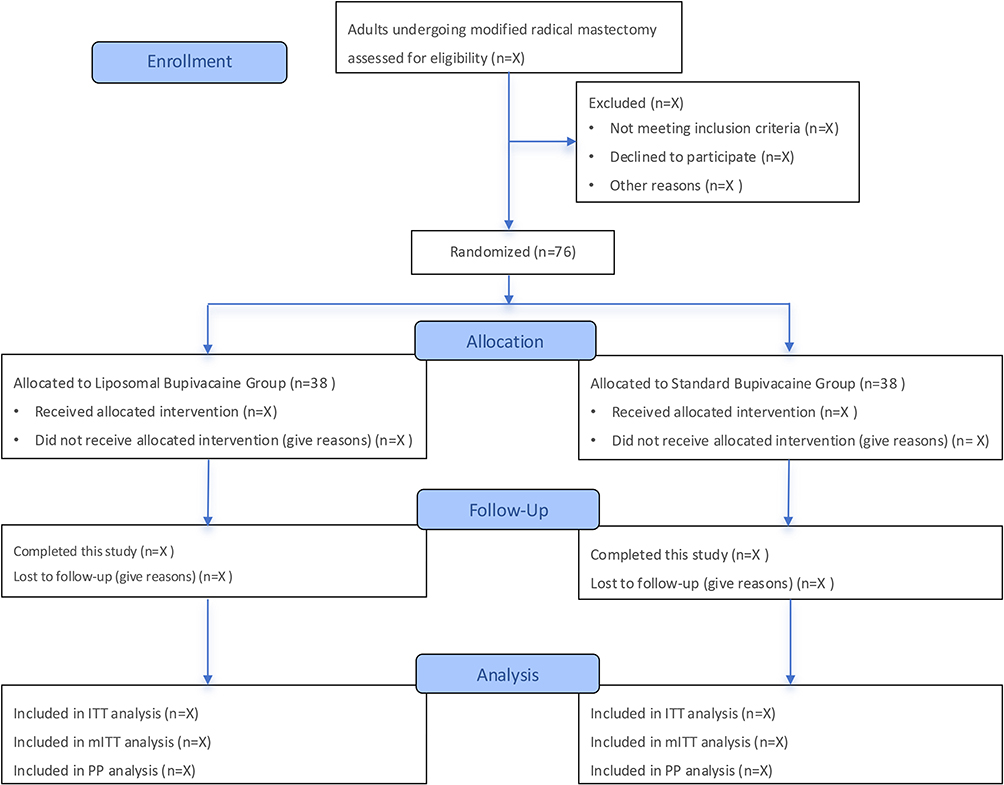 |
Figure 1 Study flow diagram of this trial. |
Study Participants
Inclusion Criteria
- Age 18 to 85 years.
- Female patients scheduled for elective modified radical mastectomy for breast cancer.
- Body Mass Index (BMI) ranging from 18 to 32 kg/m2.
- Voluntary participation with signed informed consent.
Exclusion Criteria
- Hepatic insufficiency, including significantly elevated transaminases, bilirubin, ALP/GGT, decreased albumin or prolonged PT/INR.
- Renal insufficiency, including persistently elevated serum creatinine, eGFR <60 mL/min/1.73 m2 or significant proteinuria/hematuria.
- Severe central nervous system diseases, cognitive impairment, severe psychiatric disorders, communication difficulty or other condition that precludes informed consent, reliable completion of patient-reported questionnaires, or adherence to study procedures. A history of stable anxiety or depression alone will not constitute an exclusion criterion.
- Infection at the planned block puncture site.
- Coagulopathy.
- History of chronic pain, long-term alcohol abuse, or substance abuse.
- Pregnancy.
- Refusal to use patient-controlled analgesia (PCA) pump.
- Known allergy to the investigational drugs.
Withdrawal, Loss to Follow-Up and Discontinuation Criteria
The following events may lead to withdrawal, loss to follow-up or discontinuation of study procedures.
- Participant requests to withdraw or revokes consent.
- Scheduled surgical procedure is changed to an alternative technique.
- Secondary surgical intervention required during follow-up.
- Participant loss to follow-up despite predefined contact attempts.
- Death, severe malignant arrhythmia or other major cardiovascular events precluding safe completion of follow-up assessments.
Protocol Deviations (PD) Criteria
The following events constitute PD. Participants affected by these events will remain in the study, and their outcome data will continue to be collected. Protocol deviations will not lead to exclusion from the primary intention-to-treat (ITT) analysis, whenever outcome data are available. Prespecified sensitivity analyses will include a received-intervention (modified ITT) set and an exploratory per-protocol (PP) set, as defined below.
- PD-1. Technical failure of the SAPB procedure, such that the allocated intervention was not successfully administered.
- PD-2. Failure of intravenous patient-controlled analgesia (PCA) device. This deviation will be accounted for in sensitivity analyses.
All protocol deviations will be prospectively recorded in the case report form (CRF), reviewed by the principal investigator, and reported in the final publication regardless of their impact on the primary analysis.
Randomization, Allocation and Blinding
A computer-generated randomization sequence using randomly varied block sizes of 4 and 6 will be created by an independent statistician not involved in recruitment, anesthesia management or outcome assessment. Allocations will be concealed using sequentially numbered, opaque, sealed envelopes, which will be opened by a study nurse immediately before block preparation. The study solutions will be prepared according to the randomization code by a designated anesthesia nurse. The prepared solutions will be placed in identical opaque syringes with the same total volume and labeled only with the participant study number. The syringes will be connected to opaque extension tubing and syringe-tubing connections will be covered to prevent visualization of the injectate. All SAPB procedures will be performed by a senior anesthesiologist experienced in ultrasound-guided regional anesthesia, who will perform ultrasound-guided needle placement while the same designated anesthesia nurse injects the study solution through the extension tubing according to verbal instruction. Therefore, the block performer will not directly inspect the injectate or manipulate the syringe plunger. The senior anesthesiologist and the designated anesthesia nurse involved in block administration will not participate in subsequent intraoperative anesthesia management, postoperative follow-up, outcome assessment, data collection or data analysis. Patients, anesthesiologists responsible for intraoperative anesthesia management, surgeons, postoperative care providers, outcome assessors, and statisticians will remain blinded until completion of data analysis. Blinding integrity will be assessed using the Bang Blinding Index. Emergency unblinding will be permitted only when required for clinical management of a serious adverse event. The principal investigator will authorize unblinding. The reason, timing and personnel involved will be documented.
Perioperative Management
All patients will follow standard fasting guidelines. After the patient enters the operating room, multi-parameter monitoring including ECG, non-invasive blood pressure (NIBP), peripheral oxygen saturation (SpO2) and end-tidal carbon dioxide (ETCO2) will be established. Anesthesia depth will be monitored using the bispectral index (BIS, Medtronic, Minneapolis, MN, USA). General anesthesia will be induced intravenously with propofol (2–2.5 mg/kg), rocuronium (0.6 mg/kg), and remifentanil (1 µg/kg) to facilitate tracheal intubation. A single-lumen endotracheal tube will be inserted. Patients will be ventilated with a tidal volume of 6–8 mL/kg and a respiratory rate of 10–12 breaths/min, maintaining EtCO2 between 35 and 40 mmHg. Positive end-expiratory pressure (PEEP) will be set at 5–10 cmH2O.
Anesthesia will be maintained using target-controlled infusion (TCI) of propofol (target plasma concentration 2.5–3.5 µg/mL), with additional rocuronium as required. Sufentanil may be titrated in 5 µg boluses based on hemodynamic parameters and BIS monitoring, which will be maintained between 40 and 60. Intravenous rehydration will be provided mainly with Ringer’s lactate solution. A low-dose norepinephrine infusion may be administered as needed to maintain hemodynamic stability. The propofol infusion will be discontinued at skin closure, with antiemetic prophylaxis administered according to institutional protocol based on individual postoperative nausea and vomiting (PONV) risk. The agents and doses used will be recorded. Intravenous paracetamol 1000 mg will be administered before the end of surgery, unless contraindicated. For participants weighing <50 kg or with risk factors for hepatotoxicity, dosing will be adjusted according to institutional safety policy. Sufentanil will be titrated based on respiratory rate, or nalmefene may be administered, to maintain a spontaneous respiratory rate of approximately 15 breaths per minute. After the return of spontaneous respiration and consciousness assessment, extubation will be performed. Time to extubation will be recorded. All patients will be observed in the post-anesthesia care unit (PACU) for 1 h with supplemental oxygen delivered at 3 L/min via face mask after extubation. A modified Aldrete score of ≥9 will indicate readiness for discharge from the PACU to the surgical ward.
For postoperative analgesia, all participants will receive standardized multimodal analgesia. Intravenous paracetamol 1000 mg will be administered every 6 h for the first 24 h with the first postoperative dose administered no earlier than 6 h after the intraoperative dose and without exceeding 4000 mg/day from all paracetamol-containing products. For participants weighing <50 kg or with risk factors for hepatotoxicity, dosing will be adjusted according to institutional safety policy. The same paracetamol regimen will be applied in both groups. Both groups will receive intravenous PCA with sufentanil 150 µg + granisetron 6 mg diluted to 150 mL with normal saline. The background infusion will be 0 mL/h, with a PCA bolus dose of 4 mL and a lockout interval of 10 min. All participants will receive standardized PCA instructions before surgery and again after recovery of consciousness in the PACU. PCA function and patient understanding of bolus use will be checked before transfer to the surgical ward and during scheduled ward pain assessments. Rescue analgesia will be standardized across groups. It will be administered by blinded clinical staff according to the prespecified criteria. For each rescue event, the contemporaneous pain score, time, medication dose, and administrator will be recorded. In the PACU, pain will be assessed using the Numeric Rating Scale (NRS, 0–10). If NRS > 3, intravenous fentanyl will be administered in 25 µg boluses with reassessment every 5–10 min until NRS ≤ 3 or predefined safety limits are reached including respiratory rate <10/min, SpO2 <92% despite oxygen, or excessive sedation. On the surgical ward, rescue analgesia will be considered when pain remains inadequately controlled (NRS > 3) despite PCA being active and functioning as prescribed. Prior to initiating additional rescue analgesia, PCA function including pump status, line patency, and patient understanding of bolus use will be checked. Rescue analgesia will prioritize non-opioid agents to minimize additional opioid exposure. Intravenous ketorolac will be administered unless contraindicated. If pain remains uncontrolled despite PCA and ketorolac, additional short-acting opioid rescue may be administered at the discretion of the treating team in accordance with institutional policy and will be recorded and included in total opioid exposure calculations. All rescue medications, including agent, dose and timing will be recorded.
Study Intervention
Following anesthesia induction and after confirming the operative side, the SAPB will be performed within 10 minutes of intubation under ultrasound guidance using a two-point technique at the level of the 2nd and 4th ribs. This modified two-point SAPB approach was selected to promote cephalocaudal spread and facilitate coverage of the broad anterolateral chest wall and axillary surgical field involved in modified radical mastectomy. This approach is supported by cadaveric evidence suggesting that double-injection SAPB may achieve more extensive and consistent spread and by a clinical study comparing double-point versus single-point SAPB in patients undergoing modified radical mastectomy.20,21 Representative ultrasound images of the two-point deep SAPB at the 2nd and 4th rib levels are shown in Figure 2. A horizontal, in-plane approach will be used. Technical success is defined as the clear visualization of the needle tip and the subsequent spread of the local anesthetic solution within the deep serratus plane between the serratus anterior muscle and the intercostal musculature. Because the block is performed after the induction of general anesthesia, sensory testing to confirm the block plane is not feasible. Therefore, the adequacy of the block will be defined technically by ultrasound visualization and hydrodissection of the target plane. Intraoperative hemodynamic responses and postoperative pain scores will be recorded as clinical observations but will not be used as definitive confirmation of block success. A technical failure is defined as the inability to correctly identify the anatomical plane under ultrasound, the failure to observe clear hydrodissection of the target plane or accidental vascular puncture during the procedure. Each failed case will be recorded, and the patient will be managed according to the prespecified protocol deviation procedures with continued follow-up and outcome collection whenever feasible. After aspiration confirms absence of blood, 20 mL of the local anesthetic solution will be injected at each of the two points. The study solutions are as follows:
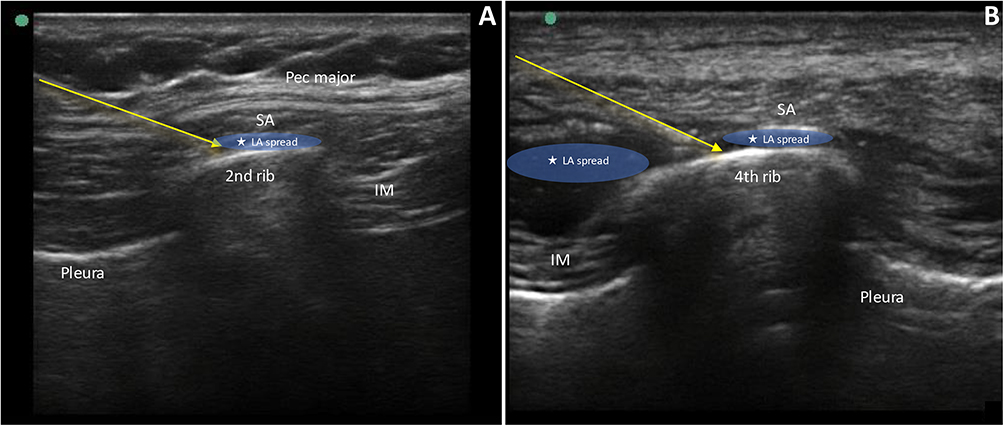 |
Figure 2 Representative ultrasound images of the two-point deep SAPB performed at the (A) 2nd rib level and (B) 4th rib level using an in-plane approach. Local anesthetic spread is shown in the deep serratus plane between the serratus anterior muscle and the intercostal musculature. Arrows indicate the needle trajectory, and asterisks indicate local anesthetic spread. Abbreviations: Pec major, pectoralis major; SA, serratus anterior; IM, intercostal musculature; LA, local anesthetic. |
- Group L (Liposomal Bupivacaine Group): bupivacaine HCl 112.5 mg + liposomal bupivacaine 266 mg, diluted to a total volume of 40 mL with normal saline.
- Group B (Bupivacaine HCl Group): bupivacaine HCl 112.5 mg, diluted to a total volume of 40 mL with normal saline.
The total dose of bupivacaine HCl is 112.5 mg in both groups. This dose will be checked against body weight before block administration. If the planned bupivacaine HCl dose would exceed institutional weight-based safety limits, dosing will follow institutional safety policy at the discretion of the attending anesthesiologist. Liposomal bupivacaine 266 mg was selected based on the maximum adult dose described in the EXPAREL prescribing information for local infiltration.22 According to the prescribing information, bupivacaine HCl may be admixed with liposomal bupivacaine provided that the milligram ratio of bupivacaine HCl to liposomal bupivacaine does not exceed 1:2. In this study, the ratio is 112.5:266, approximately 0.42:1, which is below this limit.22 Different formulations of bupivacaine are not bioequivalent or directly dose-convertible on a milligram-for-milligram basis.22 However, the toxic effects of bupivacaine HCl and liposomal bupivacaine are additive, and participants will be monitored for neurologic and cardiovascular signs of local anesthetic systemic toxicity. The study solution will be prepared in the operating room immediately before block administration according to the EXPAREL prescribing information and institutional drug-preparation procedures. Bupivacaine HCl will be diluted with normal saline before admixture. Liposomal bupivacaine will be gently inverted multiple times immediately before withdrawal to re-suspend the particles. To standardize preparation, liposomal bupivacaine will be drawn into the syringe first, followed by the prepared bupivacaine HCl solution. The admixture will be gently inverted to ensure uniform suspension and will not be vigorously shaken. The study solution will be administered within 4 h after preparation. The preparation time, administration time, and preparer will be documented in the CRF. In both groups, the total injection volume is standardized to 40 mL with each group receiving the same dose of bupivacaine HCl (112.5 mg; final concentration approximately 0.28%). Thus, the bupivacaine HCl component is matched between groups. Because Group L also receives liposomal bupivacaine, this trial should be interpreted as a pragmatic add-on strategy comparison rather than a dose-equivalent pharmacokinetic comparison.
Safety Monitoring and Adverse Event Reporting
A pharmacokinetic substudy of pecto-serratus and serratus anterior plane blocks using a similar combination found that plasma bupivacaine concentrations exceeded a predefined toxic threshold of 2000 ng/mL in 31% of patients, although without clinical evidence of toxicity.23 In light of this, all participants will be monitored for signs of local anesthetic systemic toxicity (LAST) intraoperatively, in the PACU and on the surgical ward.
Intraoperative monitoring will include continuous ECG and pulse oximetry, regular blood pressure measurement, and observation for cardiovascular manifestations suggestive of LAST, including unexplained hypotension, bradycardia, arrhythmia, or cardiac arrest. In the PACU and after transfer to the surgical ward, blinded clinical staff will assess participants during routine postoperative observations and scheduled study follow-up visits for neurologic symptoms, including perioral numbness, metallic taste, tinnitus, dizziness, visual disturbance, agitation, confusion, muscle twitching, or seizure, and for cardiovascular manifestations suggestive of LAST. Assessments will be emphasized during the first 6 h after block administration and continued during the 72-h postoperative observation period. Any suspected LAST event will trigger immediate notification of the attending anesthesiologist and activation of the institutional emergency response pathway. Standard resuscitation equipment and 20% lipid emulsion will be immediately available in the operating room and PACU and accessible on the surgical ward through the institutional emergency response system.
All adverse events (AEs) and serious adverse events (SAEs), including suspected LAST, will be recorded, graded, and reported according to institutional safety reporting procedures. Perioperative AEs and SAEs will be collected from enrollment through 72 h postoperatively. The principal investigator will assess severity and relatedness. Any SAE and any confirmed or strongly suspected LAST event will be reported to the ethics committee within 24 h of awareness in accordance with institutional requirements. Enrollment will be paused and safety data reviewed if any confirmed or strongly suspected LAST occurs, or if two or more suspected LAST events occur pending adjudication.
Outcome Measurement
Primary Outcome
The primary outcome of this study is the quality of recovery at 24 hours postoperatively, assessed using the QoR-15 scale (scores 0–150, higher scores indicating better recovery). In addition to the total QoR-15 score, exploratory item-level and recovery component analyses will be performed to describe which components contribute to any between-group difference, with particular attention to pain-related and physical comfort items. These exploratory analyses will not replace the prespecified total QoR-15 primary endpoint.
Secondary Outcomes
The secondary outcomes include the following:
- Cumulative opioid consumption within 72 hours postoperatively. Postoperative opioid requirement will be quantified as morphine milligram equivalents (MME). This will include opioids delivered via PCA, extracted from PCA device logs (total delivered dose and number of successful demands), and any additional non-PCA opioids administered in the PACU or on the surgical ward obtained from the electronic medication administration record. All opioid doses will be converted to MME using a prespecified conversion table (Supplementary Table S1). PCA log-derived opioid consumption will be reported as a prespecified component measure and will also be analyzed as a sensitivity outcome.
- Intraoperative supplemental opioid consumption, including sufentanil administered after SAPB, will be recorded separately and converted to MME.
- Total perioperative opioid consumption, calculated as the sum of intraoperative supplemental opioid consumption after SAPB and postoperative opioid consumption within 72 h after surgery.
- Postoperative NRS scores at rest and during coughing will be assessed at 2, 6, 12, 24, 48, and 72 h postoperatively.
- Quality of recovery (QoR-15) at 48 and 72 hours postoperatively.
- Incidence of postoperative nausea and vomiting (PONV).
- Time to first demand of PCA, defined as the interval from PCA pump activation to the first successful PCA bolus recorded by the device.
- Overall Benefit of Analgesia Score (OBAS), assessed orally by trained blinded assessors using a study-specific Chinese version prepared through forward translation, back-translation, and expert review. OBAS will be interpreted as an exploratory secondary outcome.
- Sleep quality on the night of surgery, assessed using the Chinese version of the Richards-Campbell Sleep Questionnaire (RCSQ), a brief 5-item patient-reported visual analogue scale evaluating perceived sleep depth, sleep latency, awakenings, return to sleep, and overall sleep quality during the preceding night.24,25 RCSQ findings will be interpreted as exploratory secondary sleep-quality outcomes.
- Incidence of anesthesia-related complications within 3 postoperative days, including hypotension, hypertension, bradycardia, tachycardia, dizziness, pruritus, respiratory depression, cognitive dysfunction, delirium.
- Time to first ambulation.
- Total hospital length of stay.
- Surgical complications.
- Patient-reported neuropathic pain symptoms at 3 months postoperatively, assessed by telephone using the DN4-interview (DN4i), which includes the first seven symptom-based patient-reported items of the DN4 questionnaire and excludes the three physician-performed sensory examination items. The DN4i score ranges from 0 to 7, with higher scores indicating more neuropathic pain characteristics. A DN4i score ≥3 will be used as an exploratory screening threshold.
Data Collection and Follow-Up
Table 1 outlines the timeline for participant enrollment, interventions and data collection, structured in accordance with SPIRIT guidelines.
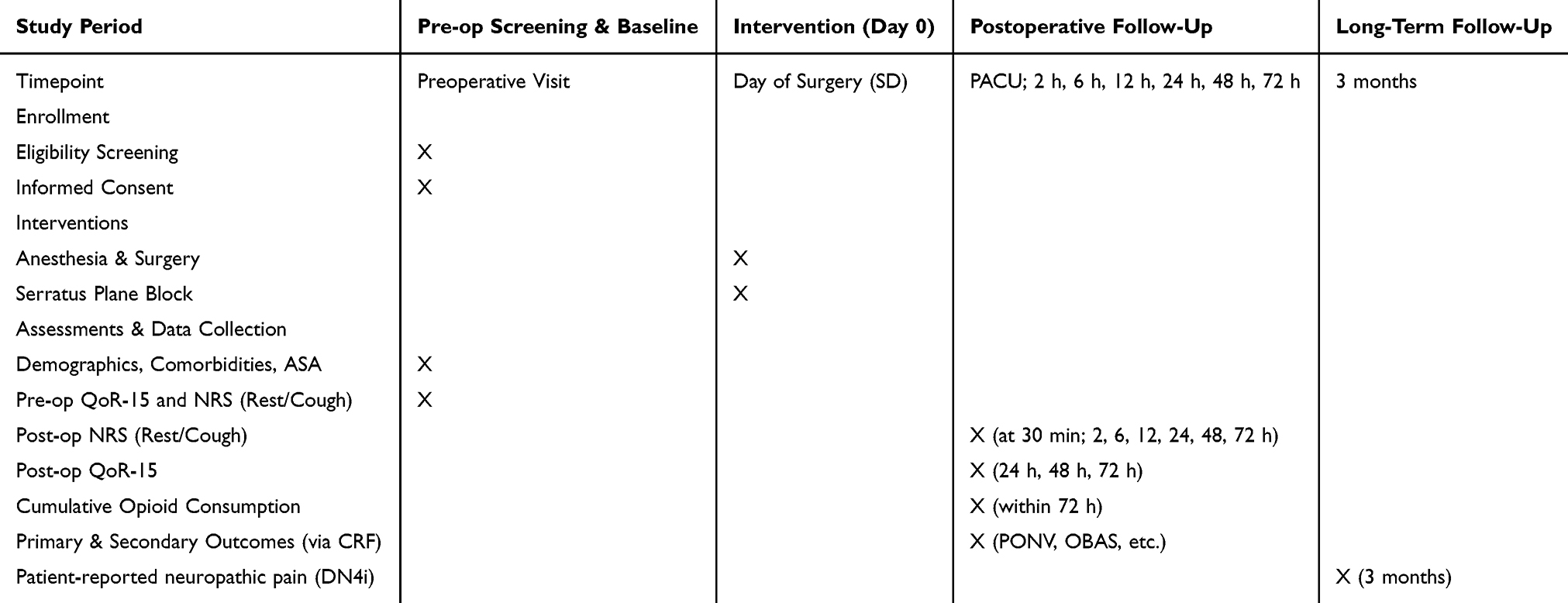 |
Table 1 The Schedule Below Outlines the Timeline for Participant Enrollment, Interventions, and Data Collection, Structured in Accordance with SPIRIT Guidelines |
Preoperative Visit, Screening, and Baseline Assessment: An anesthesiologist will conduct a preoperative visit at least 24 hours before surgery, explain the study, and obtain informed consent, ensuring participants have sufficient time to consider their decision. Baseline data including demographics, comorbidities, American Society of Anesthesiologists (ASA) physical status, preoperative QoR-15 score recorded within 24 hours before surgery, and NRS scores at rest and during coughing will be recorded by a blinded assessor.
Intraoperative and Immediate Postoperative Assessment: NRS pain scores will be recorded upon recovery from anesthesia. In the PACU, NRS scores will be reassessed at 30 min.
Postoperative Follow-up: During the 72-h postoperative period, postoperative outcomes will be recorded by blinded assessors using a CRF. Data on hemodynamic events, hospital stay, and complications will be collected from medical records.
Long-term Follow-up (3 months): A blinded assessor will conduct telephone follow-up to assess patient-reported neuropathic pain symptoms using the DN4i. Because the DN4i excludes the physician-performed sensory examination items of the full DN4, this outcome will be interpreted as exploratory screening for patient-reported neuropathic pain symptoms rather than as a definitive diagnosis of chronic neuropathic pain. To minimize loss to follow-up, participants’ contact information, including an alternative contact, will be recorded at enrollment, and a reminder will be sent via telephone or messaging platform one week before the scheduled assessment. Adjuvant therapy exposure during the postoperative period will also be recorded from medical records and participant interview, including chemotherapy regimen, exposure to chemotherapy drugs such as taxanes or platinum compounds, number of completed cycles, radiotherapy status and field, and clinician-documented chemotherapy-induced peripheral neuropathy, radiation-related neuropathy, or post-mastectomy pain syndrome.
This trial will be monitored by the principal investigator, and all data will be stored in electronic files. Entered data will be verified by another research team member to ensure accuracy. Access to the database will be granted only to personnel authorized by the principal investigator. To protect participant anonymity, each participant will be assigned a study identification number in the electronic files. Files containing study identification numbers and corresponding electronic health record identification numbers will be stored in a locked cabinet in a secure area. Because this is a small, single-center trial, no formal independent data monitoring committee will be established.
Sample Size Calculation
The sample size was planned for the prespecified primary endpoint, the QoR-15 score at 24 h postoperatively. The target between-group difference was selected based on clinical relevance, published QoR-15 data, and preliminary pilot observations. An updated minimal clinically important difference (MCID) of 6.0 points has been reported for the QoR-15 scale.26 In a recent two-center randomized trial in breast cancer surgery, the between-group difference in QoR-15 at 24 h was 6.6 points (95% CI, 4.87–8.40), and the investigators used the updated QoR-15 MCID of 6.0 points for sample-size planning.27 This was consistent with our pilot observations (Group L: 129.14 ± 8.63, n = 7; Group B: 122.14 ± 8.34, n = 7). Therefore, a between-group difference of 7 points was selected as the target effect for sample-size estimation. Using the pooled SD from the pilot data, a two-sided two-sample t-test with α = 0.05 and 90% power yielded 64 patients, with 32 patients per group. Accounting for potential dropouts, 76 patients, with 38 patients per group, will be enrolled. The primary analysis will use ANCOVA adjusting for baseline QoR-15, which may improve precision compared with the t-test-based planning approach. The small pilot sample limits the precision of the SD estimate. If the observed variability is larger than anticipated, the study may be underpowered to detect effects smaller than the prespecified target difference. Sample size calculation was performed using PASS 15.0 software. No interim analysis for efficacy is planned.
Statistical Analysis
All analyses will be conducted using SPSS (version 26.0) and R (version 4.3.2). All tests will be two-sided and a p value <0.05 will be considered statistically significant. The primary analysis will follow the ITT principle, including all randomized participants analyzed according to assigned group, regardless of intervention receipt or protocol deviations, whenever outcome data are available. Prespecified sensitivity analyses will include a mITT set including participants who received the allocated SAPB injection, excluding prespecified technical failures where the block could not be administered, and an exploratory PP set excluding participants with major protocol deviations. Primary conclusions will be based on ITT, with sensitivity analyses used to assess robustness.
All primary, secondary, and other exploratory outcomes will also be reported descriptively. Categorical data will be presented as frequency and percentage and compared using the chi-squared test or Fisher’s exact test as appropriate. Continuous variables will be assessed for normality using the Shapiro–Wilk test. Normally distributed variables will be presented as mean ± standard deviation and compared using the independent two-sample t-test. Non-normally distributed variables will be presented as median and interquartile range and compared using the Mann–Whitney U-test. For the primary outcome, the QoR-15 score at 24 h postoperatively will be compared between groups using an analysis of covariance (ANCOVA) model, adjusting for the baseline QoR-15 score recorded during the preoperative visit. The adjusted mean difference with 95% confidence interval will be reported. Exploratory QoR-15 item-level and recovery-component results will be summarized descriptively and interpreted as hypothesis-generating, without formal adjustment for multiplicity. For repeated-measures outcomes, such as NRS pain scores and QoR-15 at multiple time points, linear mixed-effects models will be used to account for the correlation between measurements within the same individual. Given the large number of secondary outcomes, no formal correction for multiple comparisons will be applied. These outcomes will be interpreted as exploratory and hypothesis-generating, with unadjusted p-values and 95% confidence intervals reported. For missing outcome data, if the primary outcome is missing, multiple imputation by chained equations will be performed under the missing at random (MAR) assumption. Imputation models will include treatment group, baseline QoR-15, age, BMI, ASA physical status, and duration of surgery. Sensitivity analyses under alternative missing data assumptions will be conducted to assess the robustness of the primary result. For the 3-month DN4i assessment, DN4i scores and the proportion of participants with DN4i ≥3 will be summarized descriptively as exploratory outcomes, and the rate and pattern of missing data will also be reported.
Discussion
This trial was designed to evaluate whether adding liposomal bupivacaine to bupivacaine HCl for SAPB provides additional benefit in postoperative recovery after modified radical mastectomy. The analgesic efficacy of SAPB has been supported by previous studies,28,29 but improvement in global recovery cannot be assumed from analgesic efficacy alone. In particular, Abdallah et al reported that single-injection deep SAPB did not significantly improve QoR-15 or secondary analgesic outcomes compared with sham block in ambulatory breast cancer surgery. Therefore, the present trial should not be interpreted as assuming that conventional SAPB already provides a consistent QoR-15 benefit. Instead, it evaluates whether an add-on SAPB strategy using liposomal bupivacaine can provide measurable recovery benefit in the specific setting of modified radical mastectomy. This distinction is important because the present protocol differs from the previous trial in surgical setting, block technique and comparator structure. Although postoperative pain intensity and opioid consumption remain important outcomes in breast surgery, they may not fully reflect the overall recovery experience after modified radical mastectomy.30,31 By selecting QoR-15 at 24 h as the primary endpoint and prespecifying complementary pain, opioid, and recovery-related secondary outcomes, this trial aims to assess whether the add-on liposomal bupivacaine strategy improves early postoperative recovery status under the assigned analgesic regimen.
A standardized two-point deep SAPB technique was selected to promote consistency of dermatomal coverage while reducing operator-related variability and improving reproducibility. Because the protocol uses liposomal bupivacaine in combination with bupivacaine HCl, drug preparation, LAST monitoring, postoperative analgesia, and adverse-event reporting have been standardized to support consistent implementation and safety surveillance across both groups.
Several limitations of this study should be acknowledged. First, this is a single-center study with a modest sample size, so the generalizability may be influenced by institution-specific perioperative practices, and uncommon adverse events may not be fully captured. The findings will require confirmation in larger multicenter studies. Second, the two treatment arms are not dose-equivalent because the liposomal bupivacaine group receives additional local anesthetic exposure. Therefore, this trial cannot isolate the sustained-release pharmacokinetic effect of liposomal bupivacaine from the overall clinical effect of the add-on strategy. Any observed benefit should be interpreted as the effect of a liposomal bupivacaine-based SAPB strategy rather than as evidence of a formulation-specific effect. In addition, plasma bupivacaine concentrations will not be routinely measured, so subclinical systemic exposure cannot be excluded. Third, the study population is limited to patients undergoing elective modified radical mastectomy for breast cancer within the prespecified BMI range, which may limit applicability to broader real-world surgical populations. Fourth, several patient-reported outcomes require cautious interpretation. QoR-15 is a multidimensional outcome and should be interpreted together with the secondary outcomes. Moreover, because the primary endpoint is assessed at 24 h postoperatively, QoR-15 may partly reflect concurrent analgesic activity and should not be interpreted as evidence of recovery benefit persisting after resolution of regional analgesia. The OBAS will be administered using a study-specific Chinese translation rather than a formally validated Chinese version and will therefore be interpreted as exploratory. Fifth, although the trial was powered for the prespecified 24-h QoR-15 endpoint, the sample-size assumptions were partly informed by a small pilot sample. Therefore, the results should be interpreted with attention to the estimated effect size and its 95% confidence interval. Finally, the 3-month DN4i-based assessment of patient-reported neuropathic pain symptoms is exploratory and may be confounded by adjuvant chemotherapy, radiotherapy, chemotherapy-induced peripheral neuropathy, and post-mastectomy pain syndrome. This outcome will be interpreted descriptively rather than as a definitive long-term efficacy endpoint.
In conclusion, this protocol describes a randomized, double-blind trial designed to evaluate whether adding liposomal bupivacaine to bupivacaine HCl for ultrasound-guided SAPB improves early postoperative recovery and pain-related outcomes after modified radical mastectomy compared with SAPB using bupivacaine HCl alone. The findings may help inform the clinical interpretation of an add-on liposomal bupivacaine SAPB strategy within multimodal analgesia for breast cancer surgery.
Data Sharing Statement
The data in this trial will be publicly available from the corresponding author upon reasonable request. All data will be available after publication in peer-reviewed journals.
Ethics Approval and Informed Consent
This study protocol was approved by the Ethics Committee of Zhongshan Hospital (Xiamen Branch), Fudan University (Approval No. B2025-071R) on 8 October 2025 and was registered with the Chinese Clinical Trial Registry (Registration No. ChiCTR2500111732) on 5 November 2025, prior to enrollment of the first participant. This trial will adhere to the principles outlined in the Declaration of Helsinki. Written informed consent will be obtained from all patients.
Acknowledgments
The authors would like to express their sincere gratitude to the patients who participated in this trial, and also thank the medical, nursing and research teams for their valuable assistance in carrying out this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This research received no external funding and has no external sponsor.
Disclosure
Dr Yue Qiu reports meeting/travel support from BD, outside the submitted work. The authors declare no other competing interests in this work.
References
1. Broyles JM, Tuffaha SH, Williams EH, Glickman L, George TA, Lee Dellon A. Pain after breast surgery: etiology, diagnosis, and definitive management. Microsurgery. 2016;36(7):535–13. doi:10.1002/micr.30055
2. FitzGerald S, Odor PM, Barron A, Pawa A. Breast surgery and regional anaesthesia. Best Pract Res Clin Anaesthesiol. 2019;33(1):95–110. doi:10.1016/j.bpa.2019.03.003
3. McCartney CJL, Abdallah F. Pain relief and recovery after breast cancer surgery: translating best evidence into practice. Anaesthesia. 2020;75(9):1136–1138. doi:10.1111/anae.15033
4. Cheung CK, Adeola JO, Beutler SS, Urman RD. Postoperative pain management in enhanced recovery pathways. J Pain Res. 2022;15:123–135. doi:10.2147/JPR.S231774
5. Abola RE, Bennett-Guerrero E, Kent ML, et al. American society for enhanced recovery and perioperative quality initiative joint consensus statement on patient-reported outcomes in an enhanced recovery pathway. Anesth Analg. 2018;126(6):1874–1882. doi:10.1213/ANE.0000000000002758
6. Jacobs A, Lemoine A, Joshi GP, Van de Velde M, Bonnet F, Collaborators PWG. PROSPECT guideline for oncological breast surgery: a systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2020;75(5):664–673. doi:10.1111/anae.14964
7. Makkar JK, Singh NP, Khurana BJK, Singh PM. Relative perioperative analgesic efficacy of single-shot serratus anterior plane block versus thoracic paravertebral block in breast and thoracic surgeries - A systematic review and meta-analysis of randomised controlled trials. Indian J Anaesth. 2025;69(1):54–64. doi:10.4103/ija.ija_1027_24
8. Yu J, Qi Y, Shen Y, et al. Effects of rhomboid intercostal nerve, serratus anterior plane, and paravertebral block on the quality of recovery after breast cancer surgery: a randomized controlled clinical trial. BMC Anesthesiol. 2025;25(1):184. doi:10.1186/s12871-025-03049-3
9. Tang W, Luo G, Lu Y, Chen C, Liu H, Li Y. Application of a new serratus anterior plane block in modified radical mastectomy under ultrasound guidance: a prospective, randomized controlled trial. J Clin Anesth. 2021;74:110377. doi:10.1016/j.jclinane.2021.110377
10. Perez-Herrero MA, Fajardo Perez M, Yamak Altinpulluk E, Ergonenc T. Usefulness of ultrasound-guided serratus-anterior block in prevention of postoperative pain after breast surgery. A cohort study. J Clin Anesth. 2024;93:111360. doi:10.1016/j.jclinane.2023.111360
11. Liang W, Zhang W, Wu Y, et al. Efficacy and safety of ultrasound-guided serratus anterior plane block for postoperative analgesia in thoracic surgery and breast surgery: a systematic review and meta-analysis of randomized controlled studies. Front Anesthesiol. 2022;1. doi:10.3389/fanes.2022.980483
12. Sulak M, Ahiskalioglu A, Yayik A, et al. The effect of ultrasound-guided serratus plane block on the quality of life in patients undergoing modified radical mastectomy and axillary lymph node dissection: a randomized controlled study. Anaesthesiol Intensive Ther. 2022;54(1):48–55. doi:10.5114/ait.2022.114203
13. Abdallah FW, Patel V, Madjdpour C, Cil T, Brull R. Quality of recovery scores in deep serratus anterior plane block vs. sham block in ambulatory breast cancer surgery: a randomised controlled trial. Anaesthesia. 2021;76(9):1190–1197. doi:10.1111/anae.15373
14. Wang S, Shi J, Dai Y, et al. The effect of different nerve block strategies on the quality of post-operative recovery in breast cancer patients: a randomized controlled study. Eur J Pain. 2024;28(1):166–173. doi:10.1002/ejp.2178
15. Xu X, Chen X, Zhu W, et al. Efficacy and safety of ultrasound guided-deep serratus anterior plane blockade with different doses of dexmedetomidine for women undergoing modified radical mastectomy: a randomized controlled trial. Front Med Lausanne. 2022;9:819239. doi:10.3389/fmed.2022.819239
16. Nguyen TH, Iturriaga C, Verma R. Efficacy of liposomal bupivacaine in spine surgery: a systematic review. Spine J. 2021;21(9):1450–1459. doi:10.1016/j.spinee.2021.02.014
17. Zhang Y, Li W, Wei A, Chen S, Wang X. Comparing liposomal bupivacaine and ropivacaine in serratus anterior plane block for thoracoscopic lobectomy: a randomized controlled trial. Drug Des Devel Ther. 2025;19:4717–4726. doi:10.2147/DDDT.S513287
18. Zhang M, Zheng Z, Xie X, et al. Comparison of continuous Serratus Anterior Plane Block (cSAPB) with bupivacaine versus single liposomal bupivacaine block in postoperative analgesia after Video-Assisted Thoracoscopic Surgery (VATS): a randomized controlled trial. BMC Anesthesiol. 2025;25(1):399. doi:10.1186/s12871-025-03249-x
19. Chan AW, Tetzlaff JM, Gotzsche PC, et al. SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ. 2013:346e7586. doi:10.1136/bmj.e7586
20. Biswas A, Castanov V, Li Z, et al. Serratus plane block: a cadaveric study to evaluate optimal injectate spread. Reg Anesth Pain Med. 2018;43(8):854–858. doi:10.1097/AAP.0000000000000848
21. Xu J, Ling D, Xu Q, et al. Ultrasound-guided double-point versus single-point serratus anterior plane block for modified radical mastectomy: a randomized controlled trial. Clin J Pain. 2025;41(1). doi:10.1097/AJP.0000000000001256
22. Pacira Pharmaceuticals I. EXPAREL (bupivacaine liposome injectable suspension). Available from: https://dailymed.nlm.nih.gov/dailymed/getFile.cfm?name=bb5a9e59-0f51-11df-8a39-0800200c9a66&setid=bb5a9e59-0f51-11df-8a39-0800200c9a66&type=pdf.
23. Alfirevic A, Almonacid-Cardenas F, Yalcin EK, et al. Blood bupivacaine concentrations after pecto-serratus and serratus anterior plane injections of plain and liposomal bupivacaine in robotically-assisted mitral valve surgery: sub-study of a randomized trial. J Clin Anesth. 2024;95:111470. doi:10.1016/j.jclinane.2024.111470
24. Chen LX, Ji DH, Zhang F, et al. Richards-Campbell sleep questionnaire: psychometric properties of Chinese critically ill patients. Nurs Crit Care. 2019;24(6):362–368. doi:10.1111/nicc.12357
25. Nurhayati N, Waluyo A, Kariasa IM, Asih SR, Pujasari H, Hayat B. Sleep quality assessment in hospitalized postoperative surgical patients: a COSMIN-based systematic review. Front Sleep. 2025;4:1714777. doi:10.3389/frsle.2025.1714777
26. Myles PS, Myles DB. An updated minimal clinically important difference for the QoR-15 scale. Anesthesiology. 2021;135(5):934–935. doi:10.1097/ALN.0000000000003977
27. Tong P, Guo Y, Wang Y, et al. Opioid-free anaesthesia protocol based on thoracic paravertebral block enhances postoperative recovery after breast cancer surgery: a two-center, prospective, randomized, controlled trial. J Clin Anesth. 2025;105:111904. doi:10.1016/j.jclinane.2025.111904
28. Singh NP, Makkar JK, Kuberan A, Guffey R, Uppal V. Efficacite des techniques d’anesthesie regionale pour l’analgesie postoperatoire chez les patientes subissant des chirurgies mammaires oncologiques majeures: une revue systematique et une meta-analyse en reseau d’etudes randomisees controlees [Efficacy of regional anesthesia techniques for postoperative analgesia in patients undergoing major oncologic breast surgeries: a systematic review and network meta-analysis of randomized controlled trials]. Can J Anaesth. 2022;69(4):527–549. doi:10.1007/s12630-021-02183-z
29. Sansone P, Giaccari LG, Faenza M, et al. What is the role of locoregional anesthesia in breast surgery? A systematic literature review focused on pain intensity, opioid consumption, adverse events, and patient satisfaction. BMC Anesthesiol. 2020;20(1):290. doi:10.1186/s12871-020-01206-4
30. Jaensson M, Nilsson U, Dahlberg K. Methods and timing in the assessment of postoperative recovery: a scoping review. Br J Anaesth. 2022;129(1):92–103. doi:10.1016/j.bja.2022.04.015
31. Bowyer A, Jakobsson J, Ljungqvist O, Royse C. A review of the scope and measurement of postoperative quality of recovery. Anaesthesia. 2014;69(11):1266–1278. doi:10.1111/anae.12730
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Minimum Effective Volume of Liposomal Bupivacaine for Interscalene Block in Arthroscopic Rotator Cuff Repair: A Prospective, Biased-Coin Up-and-Down Dose-Finding Study
Wang HT, Xue Q, Li HJ, Zhao YY, Tian K, Yang JJ
Drug Design, Development and Therapy 2025, 19:11789-11797
Published Date: 26 December 2025
The Efficacy and Safety of Ultrasound-Guided Nerve Block in the Treatment of Cervical Spondylotic Radiculopathy: A Systematic Review and Meta-Analysis
Deng M, Wu D, Tang N, Kuang J
Journal of Pain Research 2026, 19:573563
Published Date: 4 March 2026