Back to Journals » Journal of Pain Research » Volume 18
Minimal Clinically Important Difference in Patients with Acute Neck Pain Undergoing Conservative Treatment with Korean Medicine
Authors Kim JS, Kim E, Shin S, Ha IH ![]() , Lee YJ
, Lee YJ ![]()
Received 19 March 2025
Accepted for publication 17 July 2025
Published 23 July 2025 Volume 2025:18 Pages 3709—3716
DOI https://doi.org/10.2147/JPR.S525359
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Ji Sun Kim,1 Eunsan Kim,2 Seungwon Shin,3 In-Hyuk Ha,2 Yoon Jae Lee2
1Jaseng Hospital of Korean Medicine, Seoul, Republic of Korea; 2Jaseng Spine and Joint Research Institute, Jaseng Medical Foundation, Seoul, Republic of Korea; 3College of Korean Medicine, Sangji University, Wonju, Republic of Korea
Correspondence: Yoon Jae Lee, Jaseng Spine and Joint Research Institute, Jaseng Medical Foundation, 2F Vision Tower, 540 Gangnam-Daero, Gangnam-Gu, Seoul, Republic of Korea, Tel +82-2-2222-2740, Email [email protected]
Purpose: To determine the minimal clinically important difference (MCID) and substantial clinical benefit (SCB) for patients with acute neck pain undergoing conservative treatment.
Patients and Methods: This secondary data analysis of a randomized controlled trial investigated 128 individuals with acute neck pain receiving conservative treatment. The MCID and SCB of pain, functional disability, and quality of life were assessed using anchor-based methods. Patients’ global impression of changes at week 9 was used as the anchor. A receiver operating characteristic curve was constructed, and the Youden index was employed to determine the optimal cut-off point. Area under the curve (AUC) values were calculated to assess accuracy. Minimal detectable changes (MDCs) were estimated using a distribution-based approach.
Results: The study cohort comprised 60.2% female patients with an average age of 40.7 ± 12.7 years. The visual analog scale (VAS) score for pain during movement at baseline was 64.5 ± 10.6. The outcome measures’ estimated MCID values (AUC) were as follows: VAS for pain during movement, − 19.9 (0.89) and at rest, − 17.5 (0.83); Northwick Park Neck Pain Questionnaire score, − 14.7 (0.78); neck disability index, − 10.6 (0.77); and physical component summary (PCS), 2.0 (0.83). The SCB estimates indicated thresholds of outcome improvement to be 1.5– 3-fold higher. The MDC for PCS (9.49) exceeded its MCID and SCB.
Conclusion: This study provides estimates for multidimensional MCID and SCB in acute neck pain treated conservatively. These values may assist clinicians in interpreting outcomes and setting meaningful treatment goals in clinical practice.
Keywords: acute neck pain, minimal clinically important difference, conservative treatment, disability, quality of life
Introduction
Neck pain is a common condition and one of the leading contributors to disability worldwide.1,2 The point prevalence of neck pain per 100,000 population is estimated to be 3551.1. In terms of age and sex patterns, the point prevalence of neck pain is higher in females and increases with age.2 The highest prevalence is observed in individuals aged 45–54 years.3 Risk factors for neck pain include psychopathology, lifestyle, and medical history.4,5 Neck pain can be categorized as acute, sub-acute, or chronic based on the duration of pain. Nearly half of affected individuals develop persistent pain.4,6 Approaches for treating and managing neck pain include conservative treatment, injections, and surgery.7 Conservative treatments for neck pain include therapeutic exercise, electrotherapy, medications such as non-steroidal anti-inflammatory drugs (NSAIDs), and acupuncture.8 In East Asia, particularly in Korea, traditional Korean medicine—including acupuncture, Chuna manual therapy, and pharmacopuncture—is widely used as a conservative treatment for neck pain.9–11
Minimal clinically important difference (MCID) and substantial clinical benefit (SCB) have been developed and utilized for evaluating meaningful changes for patients, and there has been growing interest in patient-reported outcome measures in recent years. MCID is defined as the minimal improvement perceived as beneficial by patients, with no side effects and within a cost-effective range,12 while SCB is defined as a substantial improvement experienced and reported by patients.13 Anchor-based methods, which use an external reference as an independent measure, are commonly used for calculating MCID and SCB.14 Estimating thresholds of improvement perceived and reported by patients based on these approaches can be useful in designing clinical trials, determining sample sizes, interpreting clinical outcomes, and making clinical decisions.
MCID values for conservative treatment for neck pain have mainly been determined based on the numeric rating scale (NRS) for pain and the Neck Disability Index (NDI). MCID estimates were represented in terms of changes in NRS scores (range: 0–10) by 1.5–2.5 points,15,16 and changes in NDI scores (range: 0–50) by 3.5–7.5 points.16,17 However, these estimates were obtained from patient populations with chronic neck pain or mixed durations of pain and are not applicable to patients with acute neck pain. There have been only a limited number of studies on the calculation of MCID for patients with acute neck pain.18 One study conducted in Spain (2008) reported an MCID estimate in terms of changes in NRS score by 0.5 points using an anchor-based method,15 while another study in the Netherlands (2006) reported an MCID estimate in terms of changes in NDI score by 1.66 points.19 In the present study, we aim to update findings from previous studies by estimating the MCID and SCB for patients with acute neck pain using an anchor-based method. In addition to outcome measures for pain and functional disability, EuroQol 5-Dimension 5-Level (EQ-5D-5L) and the 12-Item Short-Form Health Survey (SF-12), which are instruments for quality-of-life (QoL) assessment, were used to provide a comprehensive and multidimensional perspective on acute neck pain. We also investigated the responsiveness of measures by assessing the standard error of measurement (SEM) and minimal detectable change (MDC) using a distribution-based approach.
Methods
Patient Sample
This study employed secondary analysis of data from a multicenter randomized controlled trial (RCT)20 to explore the effectiveness of motion-style acupuncture (MSAT) for non-specific acute neck pain. MSAT is an acupuncture method involving active or passive movement stimulation after needle insertion, and its effectiveness has been evaluated in a published RCT for acute low back pain.21,22
In the original RCT,20 A total of 128 patients with acute neck pain were recruited from four hospitals in Korea. The inclusion criteria were individuals experiencing neck pain onset or worsening within the past month, with a Visual Analog Scale (VAS) rating of 5 or higher for neck pain at rest or during movement (flexion, extension, rotation, left and right lateral flexion). Exclusion criteria included neck pain due to specific causes such as trauma, tumors, infections, or inflammatory diseases, as detailed in the original study protocol. Patients were randomized to either MSAT, which involves neck rotations performed with acupuncture needles in place, or standard acupuncture. In both groups, needles were inserted at common points (TE15, SI15, LI16) with manual stimulation to elicit the deqi sensation. The standard acupuncture group additionally received needling at points such as GB20, BL10, and SI14 based on clinical judgement. Each 15 min session was conducted two to three times per week over a two-week period (total of 4–6 sessions), with the frequency adjusted based on pain severity and clinical judgement by the treating physician. All patients signed an informed consent form, and detailed information about the clinical study can be found in the published study protocol.20 Both intervention arms from the original RCT were included in this secondary analysis. The primary results of the study will be published in a separate paper. The study protocol was approved by the Institutional Review Board of Jaseng Hospital of Korean Medicine (JASENG 2020–07-014, JASENG 2020–07-015, JASENG 2020–07-016, JASENG 2020–07-017). As this analysis used only de-identified data and aligned with the original objectives of the clinical trials, additional institutional review board approval was not required. All investigators were trained to follow the Declaration of Helsinki, the Korean Good Clinical Practice Guidelines, study protocol, and standard operating procedure.
Measurement
In this study, MCID estimates for outcomes of pain, functional disability, and QoL were measured for patients with acute neck pain. All outcomes were measured as per patient-reported outcomes. These were measured by trained and blinded investigators through interviews with patients. Pain was measured using the VAS.23 During the pain assessment with VAS, patients were instructed to indicate the level of neck pain on movement and at rest along a continuous line of 100 mm in length, with one end indicating no pain and the other indicating the worst pain imaginable; larger scores on the scale represent greater pain intensity.
Functional disability caused by neck pain was assessed using the Northwick Park Neck Pain Questionnaire (NPQ)24 and NDI.25 NPQ is a self-reported questionnaire on the subjective feeling of pain intensity experienced by a patient for neck pain during activities of daily living and the consequent disability. It consists of nine questions in total. Each question is rated on a 5-point scale from 0 to 4, where 4 points indicate the worst pain and disability. The NDI is the most commonly used instrument for assessing disability due to neck pain, and it measures the extent of disability affecting a patient’s daily life. It consists of 10 questions in total, and each item of the question is rated on a 6-point scale from 0 to 5, where 5 points indicate the most severe level of disability. NDI and NPQ scores were converted into percentage values with 100 points as the full score. Both instruments have demonstrated adequate reliability and validity in Korean populations.26,27
Patient QoL was assessed using the EQ-5D-5L28 and SF-12 version 2.29 EQ-5D-5L is used for the assessment of five dimensions—mobility, self-care, usual activities, pain, and anxiety/depression—into five levels. In the present study, the estimates of Korean preference weights for EQ-5D-5L reported in a previous study were applied.30 SF-12 is a self-reported measure consisting of 12 questions on physical and mental health. In SF-12, weights are applied for conversion into physical component summary (PCS) and mental component summary (MCS) scores. PCS and MCS scores range from 0 to 100, with higher scores indicating higher QoL. The PCS and MCS scores were calculated using PROCoRE version 2.1 (©QualityMetric, Inc.) with reference to the US population norms (2009). The Korean validated version of the SF-12 was used in this study.31
The Patient Global Impression of Change (PGIC) was used as an anchor for the calculation of MCID and SCB estimates.32 This instrument measures changes in the overall clinical status perceived by patients as they undergo treatment, and the patients rate their change based on a 7-point single-item scale ranging from “very much worse” to “very much improved”. The response scale used is as follows: 1, very much improved; 2, much improved; 3, minimally improved; 4, no change; 5, minimally worse; 6, much worse; or 7, very much worse. MCID was defined as a threshold value that differentiates between PGIC scores 1–3 (responders) and PGIC scores 4–7 (non-responders). SCB was defined as a threshold value that differentiates PGIC scores 1–2 (responders) from PGIC scores 3–7 (non-responders).
Statistical Analysis
We used measures at the baseline and 9th week in the analysis. The pain, functional, and QoL outcomes were translated into changes from baseline to the 9th week. The change from baseline in terms of PGIC was also presented.
Missing data at the end of treatment were handled using the method of multiple imputation. Woaye-Hune33 underlined the necessity for appropriate management of missing data in studies on the estimation of MCID, and the multiple imputation method was used for this purpose. Multiple imputation is a representative method of handling missing data in clinical trials.34 Procedures of multiple imputation under the missing at random (MAR) assumption enable unbiased imputation for missing values. The procedures of multiple imputation introduced by Van Buuren et al35 were used to build an imputation model considering missing data patterns, their values, and distribution, and the Markov chain Monte Carlo algorithm was applied to perform multiple imputation. Twenty imputation sets were generated, and estimates were pooled based on Rubin’s rule.
The estimates of MCID and SCB were calculated using anchor-based methods. The receiver operating characteristic (ROC) curve was used to estimate the optimal cut-off point to differentiate responses. The ROC curve was constructed based on sensitivity and specificity. The Youden index was used to determine the optimal cut-off point on the ROC curve. The Youden index identifies the threshold that maximizes the sum of sensitivity and specificity, which is the farthest from the diagonal line of the ROC curve. The estimated cut-off point was validated based on the area under the ROC curve (AUC).36 The confidence interval (CI) of the AUC was estimated with 2000 bootstraps. We determined the estimated threshold to be reliable when the AUC was ≥ 0.7 and the lower interval of the CI was ≥ 0.5. MCID and SCB were also estimated according to sex.
A distribution-based approach was applied to estimate the SEM and MDC. SEM was calculated using the formula, SD × √(1-r), where SD denotes the standard deviation of the baseline outcome, and r indicates the test-retest reliability. For the value of r, the intraclass correlation coefficient reported in a previous study was used: VAS: 0.97;37 NPQ: 0.83;26 NDI: 0.93;27 EQ-5D-5L: 0.75;38 PCS: 0.73; MCS: 0.64.39 MDC values were calculated as 1.96 × √2 × SEM.40 R version 4.1.1 (©The R Foundation for Statistical Computing) was used for our analysis.
Results
In the present study, data from all 128 enrolled participants were analyzed. Table 1 presents the baseline characteristics of the participants. Seventy-seven of the participants (60.2%) were female. The mean age of the study population was 40.7 ± 12.7 years, and the BMI was 23.9 ± 4.2. Radiographic findings showed forward head posture in 105 patients (82.0%), narrowing in 27 patients (21.1%), and degeneration in 8 patients (6.2%). Both groups received nearly the same number of treatments (MSAT group: 5.5 ± 0.8; Control group: 5.5 ± 1.0). The values of outcome measures at week 9 and representation in terms of change from baseline are presented in Supplementary Table 1.
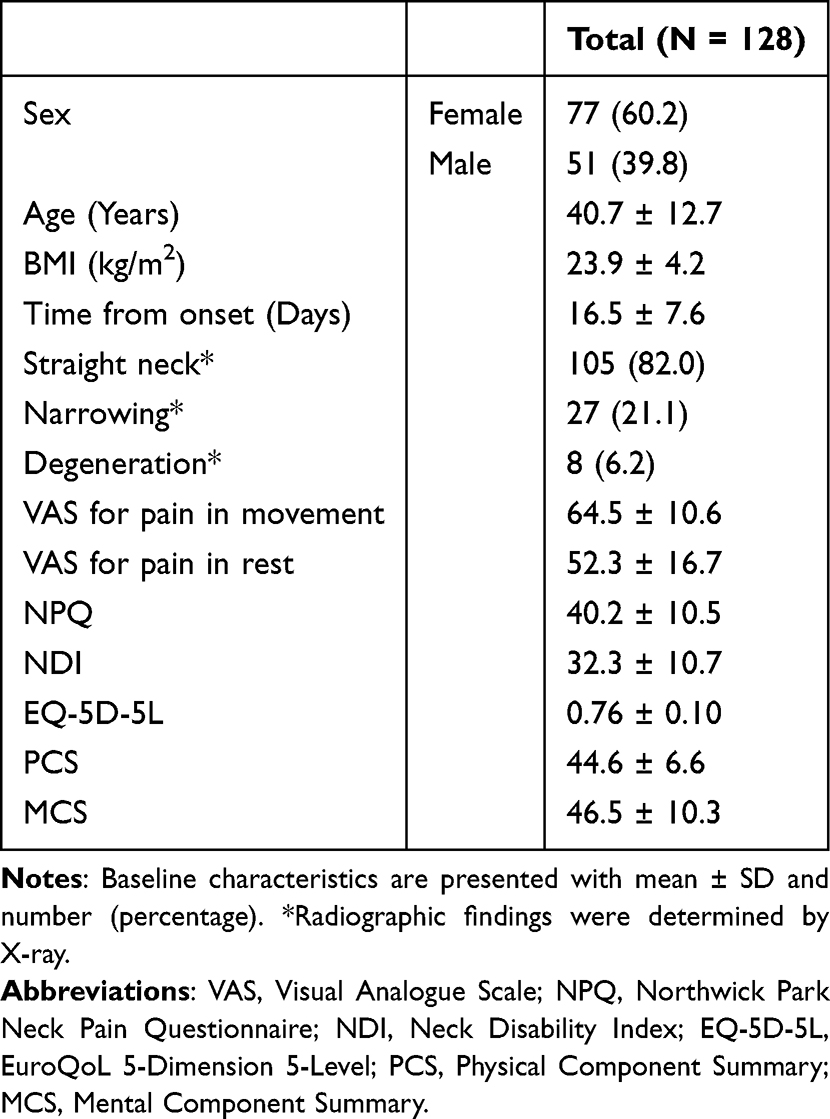 |
Table 1 Baseline Characteristics of Participants |
Table 2 presents the 9-week changes in outcomes for categories of PGIC. The VAS score for pain during movement decreased by 30.9 ± 17.9 in the minimally improved group of PGIC (48 patients, 37.5%) and by 12.2 ± 14.6 in the no-change group of PGIC (16 patients, 12.5%). The NPQ score decreased by 12.7 ± 10.8 and 8.3 ± 9.5 in each of these groups, respectively, and the NDI score decreased by 10.1 ± 9.5 and 6.4 ± 8.4, respectively. The EQ-5D value increased by 0.05 ± 0.10 and 0.03 ± 0.08 in each group, respectively; the PCS score increased by 3.1 ± 5.1 and decreased by 2.1 ± 5.2, respectively. Outcome improvement was consistently greater for patients who reported being “much improved” (37 patients, 28.9%) or “very much improved” (27 patients, 21.1%) compared with those who reported being “minimally improved”.
 |
Table 2 Mean Changes in Outcomes by Response to PGIC |
Table 3 presents the estimation results of MCID and SCB for each outcome measure: The MCID values of the outcome measures were as follows: the VAS score for pain during movement, −19.9 (AUC: 0.89 [95% CI: 0.81–0.96]); the VAS score of pain at rest, −17.5 (AUC: 0.83 [95% CI: 0.72–0.93]); the NPQ score, −14.7 (AUC: 0.78 [95% CI: 0.66–0.88]); the NDI score, −10.6 (AUC: 0.77 [95% CI: 0.65–0.87]); and the PCS score, 2.0 (AUC: 0.83 [95% CI: 0.71–0.92]). The instruments for these outcome measurements showed 1.5- to 3-fold higher thresholds in the estimation of SCB. The reliability in the estimation of SCB for each outcome was similar to that of MCID. Additionally, the reliability in the estimation of SCB increased for EQ-5D-5L (threshold: 0.02; AUC: 0.71 [95% CI: 0.61–0.79]).
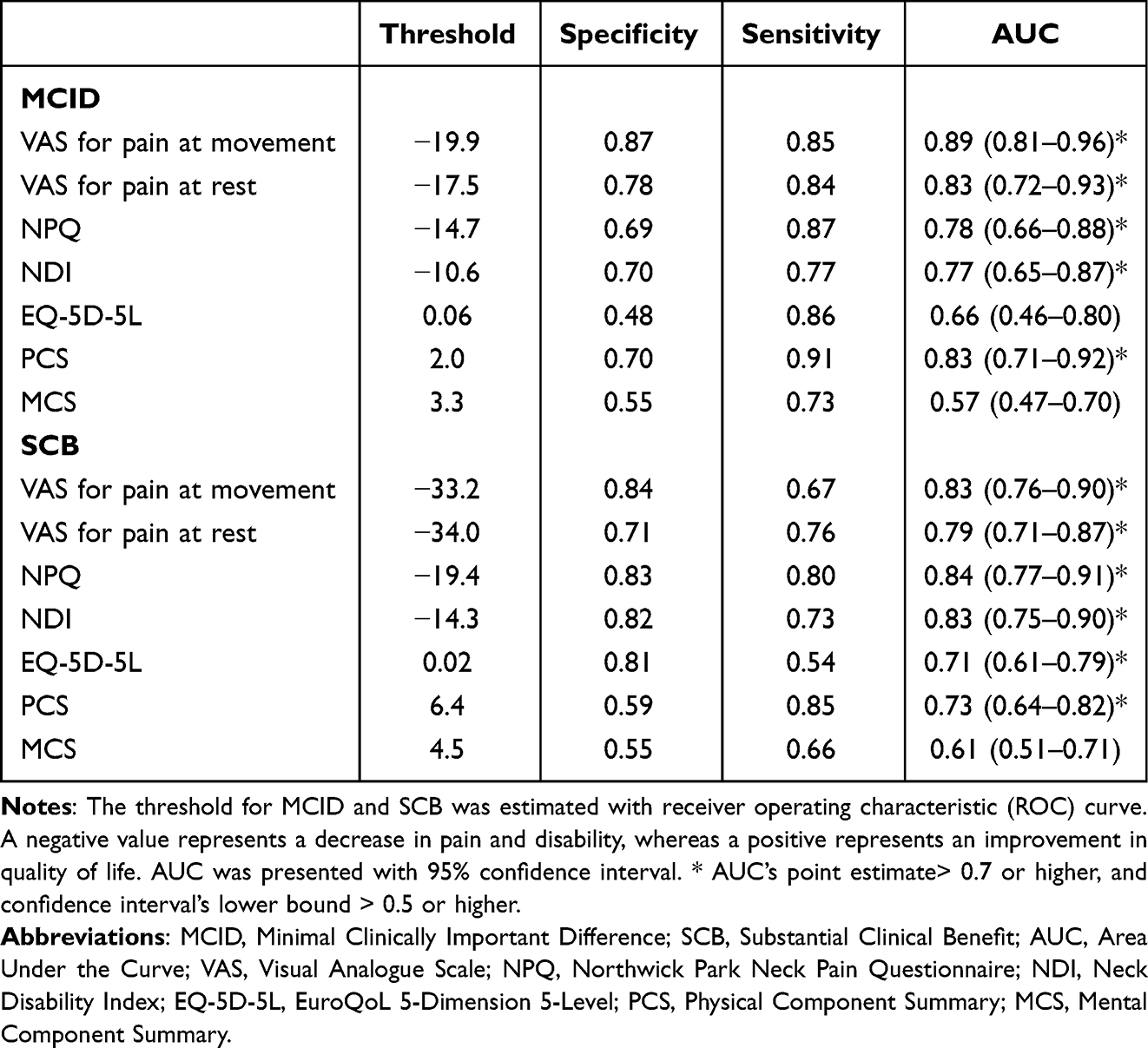 |
Table 3 Estimated MCID and SCB |
In addition to the above analyses, we performed subgroup analyses according to sex (female and male) and age group (≥40 and <40 years). For the VAS score, thresholds with high reliability were obtained for all subgroups. Apart from the PCS, the estimated thresholds were generally higher in female patients than in male patients (female threshold: 0.9, male threshold: 2.1) and in the ≥40 years age group than in the <40 years age group (age ≥ 40 years threshold: 1.1, age < 40 years threshold: 2.5) (Supplementary Tables 2–1 and Supplementary Table 2–2). The calculated SEM and MDC values are presented in Supplementary Table 3. The absolute value of MDC was smaller than MCID and SCB of VAS, NPQ, and NDI, except for EQ-5D-5L, PCS, and MCS.
Discussion
In this study, MCID and SCB estimates for pain, functional disability, and QoL were calculated and analyzed for 128 patients with acute neck pain. The estimated MCID for the VAS score for neck pain was −19.9 during movement and −17.5 at rest. For functional outcomes, the MCID was −14.7 for the NPQ score and −10.6 for NDI. Regarding QoL, the estimated MCID for the PCS of SF-12 was 2.0. SCB estimates for the respective outcome measures were also obtained, with a high reliability.
Most existing research on MCID values of conservative treatment in patients with neck pain has been conducted on patient populations with chronic pain or mixed populations regarding pain duration. Only two studies have been conducted on patients with acute or subacute pain. Vos et al19 obtained a threshold estimate for the NDI score (range: 0–50) to be 1.66 for 79 Dutch patients with acute neck pain. However, the estimated threshold in their study is a minimal detectable change calculated using a distribution-based method. Clinically important differences should primarily be based on thresholds estimated by anchor-based methods, with distribution-based methods used as secondary means to support anchor-based methods.41 In this study, MCID estimates were calculated using anchor-based methods for a larger number of samples compared to those in the previous study, making the results more relevant for clinical decision-making.
The estimated MCID for the NRS score for pain (scale: 0–10) for 290 Spanish patients reported by Kovacs et al15 was 0.5. When the estimates were compared on the same scale, their result was approximately four times smaller than the estimate in this study. It is challenging to pinpoint the exact cause of this difference. The patient population in their study included a higher percentage of women (Kovacs et al:15 77.5%; our study: 60.2%) and older patients (Kovacs et al:15 54.1%; our study: 40.7%) and reported more severe pain intensity (NRS [0 to 10] in Kovacs et al:15 7.2; VAS for pain during movement [0 to 100] in our study: 64.5). However, there is no evidence that this level of difference in age and pain intensity could have led to such a remarkable difference in MCID estimation. Alternatively, the difference may be attributable to ethnicity. Pain sensitivity varies depending on the ethnicity of the patient population,42–44 and several previous studies have reported high pain sensitivity and low pain threshold among Asians.43,45,46 In such cases, more substantial clinical improvement may be needed to reduce the pain perceived by the patient below the threshold level. However, there has been a paucity of studies on pain sensitivity conducted for the Asian population,43 making it difficult to come to a definitive conclusion on this issue.
Furthermore, in the present study, we investigated MCID for QoL using PCS scores. To the best of our knowledge, this is the first MCID research on the QoL of patients with acute neck pain who received conservative treatment. Neck pain is one of the leading causes of disability and compromised QoL.47–49 The perceived improvement in neck pain by the patients signifies not only an improvement in terms of pain but also in biomechanical performance, activities of daily living, and self-efficacy.50 In other words, clinical improvement perceived by patients signifies an improvement in QoL, including physical capacity and role participation.51 Therefore, the findings of this study provide a multidimensional approach to clinical decisions regarding the treatment of neck pain.
This study has some limitations. First, although we validated MCID and SCB based on AUC, MCID and SCB of EQ-5D, MCS and PCS were smaller than MDC. In this case, although patients achieved MCID in QoL, we could not ignore that those achievements were within the measurement errors or chance. Clinicians should fully consider the pain and disability of patients. Second, the sample size in some PGIC categories might be insufficient. In particular, the number of patients reporting no change in the PGIC score outcome was small (12.5%). Previous studies also observed this trend; for example, in the study by Kovacs et al,15 only 8% of the patients reported no change. Third, patients in the present study were followed up for only 9 weeks. To establish a long-term management plan for neck pain, further studies with long-term follow-up are required. Fourth, in this study, acupuncture and motion-style acupuncture were both administered as conservative treatments. If types of treatment interact with the relationship between clinical outcomes and patient satisfaction, this may influence the generalized interpretation of findings in this study. Finally, pain was considered the primary outcome of the RCT study; therefore, the question in the PGIC specified pain as an example. Thus, patients might respond to the PGIC only based on their pain, not on their overall symptoms.
In conclusion, through measurements and analyses in this study, estimates for multidimensional MCID for conservative treatment in patients with acute neck pain were derived. These findings are expected to serve as useful information in the design of clinical trials and clinical decision-making for pain, disability, and QoL in patients with acute neck pain. To enhance the applicability of these thresholds in clinical settings, future studies should explore their integration with other treatment modalities and consider factors such as patient satisfaction, pain sensitivity, and ethnicity. Furthermore, identifying potential barriers to implementation in real-world practice may enhance their clinical utility. Studies with larger and more diverse populations and longer follow-up periods are warranted to assess long-term effects and generalizability.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to the potential identification of individuals, but they can be obtained from the corresponding author upon reasonable request.
Ethical Considerations
The study protocol was approved by the Institutional Review Board of Jaseng Hospital of Korean Medicine (JASENG 2020-07-014, JASENG 2020-07-015, JASENG 2020-07-016, JASENG 2020-07-017). All investigators were trained to follow the Declaration of Helsinki, the Korean Good Clinical Practice Guidelines, study protocol, and standard operating procedure.
Funding
This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: RS-2021-KH111842).
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Hoy D, March L, Woolf A, et al. The global burden of neck pain: estimates from the global burden of disease 2010 study. Ann Rheumatic Dis. 2014;73(7):1309–1315. doi:10.1136/annrheumdis-2013-204431
2. Safiri S, Kolahi -A-A, Hoy D, et al. Global, regional, and national burden of neck pain in the general population, 1990-2017: systematic analysis of the global burden of disease study 2017. BMJ. 2020;368. doi:10.1136/bmj.m791
3. Kazeminasab S, Nejadghaderi SA, Amiri P, et al. Neck pain: global epidemiology, trends and risk factors. BMC Musculoskeletal Disorders. 2022;23(1):26. doi:10.1186/s12891-021-04957-4
4. Cohen SP, Hooten WM. Advances in the diagnosis and management of neck pain. BMJ. 2017;2017:358.
5. Kazeminasab S, Nejadghaderi SA, Amiri P, et al. Neck pain: global epidemiology, trends and risk factors. BMC Musculoskeletal Disorders. 2022;23(1):1–13. doi:10.1186/s12891-021-04957-4
6. Woodhouse A, Pape K, Romundstad PR, Vasseljen O. Health care contact following a new incident neck or low back pain episode in the general population; the HUNT study. BMC Health Serv Res. 2016;16(1):1–10. doi:10.1186/s12913-016-1326-5
7. Cohen SP. Epidemiology, diagnosis, and treatment of neck pain. Mayo Clin Proc. 2015;90(2):284–299. doi:10.1016/j.mayocp.2014.09.008
8. Castellini G, Pillastrini P, Vanti C, et al. Some conservative interventions are more effective than others for people with chronic non-specific neck pain: a systematic review and network meta-analysis. J Physiother. 2022;68(4):244–254. doi:10.1016/j.jphys.2022.09.007
9. Lee YJ, M-r K, Lee E-J, et al. An evidence-based approach for the development of a clinical practice guideline for the treatment of neck pain using traditional Korean medicine. Eur J Int Med. 2021;44:101337. doi:10.1016/j.eujim.2021.101337
10. Lee J, Cho J-H, Kim K-W, et al. Chuna manual therapy vs usual care for patients with nonspecific chronic neck pain: a randomized clinical trial. JAMA Network Open. 2021;4(7):e2113757–e2113757. doi:10.1001/jamanetworkopen.2021.13757
11. Park K-S, Kim S, Kim C, et al. A comparative study of the effectiveness of pharmacopuncture therapy for chronic neck pain: a pragmatic, randomized, controlled trial. J Clin Med. 2021;11(1):12. doi:10.3390/jcm11010012
12. Jaeschke R, Singer J, Guyatt GH. Measurement of health status: ascertaining the minimal clinically important difference. Controlled Clin Trials. 1989;10(4):407–415. doi:10.1016/0197-2456(89)90005-6
13. Glassman SD, Copay AG, Berven SH, Polly DW, Subach BR, Carreon LY. Defining substantial clinical benefit following lumbar spine arthrodesis. JBJS. 2008;90(9):1839–1847. doi:10.2106/JBJS.G.01095
14. McGlothlin AE, Lewis RJ. Minimal clinically important difference: defining what really matters to patients. JAMA. 2014;312(13):1342–1343. doi:10.1001/jama.2014.13128
15. Kovacs FM, Abraira V, Royuela A, et al. Minimum detectable and minimal clinically important changes for pain in patients with nonspecific neck pain. BMC Musculoskeletal Disorders. 2008;9(1):1–9. doi:10.1186/1471-2474-9-43
16. Pool JJ, Ostelo RW, Hoving JL, Bouter LM, De Vet HC. Minimal clinically important change of the Neck Disability Index and the Numerical Rating Scale for patients with neck pain. Spine. 2007;32(26):3047–3051. doi:10.1097/BRS.0b013e31815cf75b
17. Young BA, Walker MJ, Strunce JB, Boyles RE, Whitman JM, Childs JD. Responsiveness of the Neck Disability Index in patients with mechanical neck disorders. Spine J. 2009;9(10):802–808. doi:10.1016/j.spinee.2009.06.002
18. Lee Y-S, Lee S, Lee YJ, Ha I-H. Minimum clinically important difference for nonsurgical interventions for spinal diseases: choosing the appropriate values for an integrative medical approach. Perspect Integr Med. 2023;2(2):86–99. doi:10.56986/pim.2023.06.003
19. Vos CJ, Verhagen AP, Koes BW. Reliability and responsiveness of the Dutch version of the Neck Disability Index in patients with acute neck pain in general practice. Eur Spine J. 2006;15(11):1729–1736. doi:10.1007/s00586-006-0119-7
20. Kim D, Lee YJ, Park KS, et al. The effectiveness and cost-effectiveness of motion style acupuncture treatment (MSAT) for acute neck pain: a multi-center randomized controlled trial. Medicine. 2020;99(44):e22871.
21. Shin J-S, Ha I-H, Lee J, et al. Effects of motion style acupuncture treatment in acute low back pain patients with severe disability: a multicenter, randomized, controlled, comparative effectiveness trial. Pain®. 2013;154(7):1030–1037. doi:10.1016/j.pain.2013.03.013
22. Kim D, Lee YJ, Ha I-H. A scoping review of clinical research on motion style acupuncture treatment. Perspect Integr Med. 2023;2(2):65–76. doi:10.56986/pim.2023.06.001
23. Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: visual analog scale for pain (vas pain), numeric rating scale for pain (nrs pain), mcgill pain questionnaire (mpq), short‐form mcgill pain questionnaire (sf‐mpq), chronic pain grade scale (cpgs), short form‐36 bodily pain scale (sf‐36 bps), and measure of intermittent and constant osteoarthritis pain (icoap). Arthritis Care Res. 2011;63(S11):S240–S252.
24. Leak A, Cooper J, Dyer S, Williams K, Turner-Stokes L, Frank A. The Northwick Park Neck Pain Questionnaire, devised to measure neck pain and disability. Rheumatology. 1994;33(5):469–474. doi:10.1093/rheumatology/33.5.469
25. Vernon H, Mior S. The Neck Disability Index: a study of reliability and validity. J Manipulative Physiol Therapeut. 1991;14:409–15.
26. Lee K-W, Seo H-D, Jung K-S, Kim S-H, Chung Y-J. Reliability and validity of Korean version Northwick Park Neck Pain Questionnaire in neck pain patients. Phys Ther Korea. 2010;17(3):68–76.
27. Song K-J, Choi B-W, Choi B-R, Seo G-B. Cross-cultural adaptation and validation of the Korean version of the neck disability index. Spine. 2010;35(20):E1045–E1049. doi:10.1097/BRS.0b013e3181df78e9
28. Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20:1727–1736. doi:10.1007/s11136-011-9903-x
29. Ware JE Jr, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–233. doi:10.1097/00005650-199603000-00003
30. Kim S-H, Ahn J, Ock M, et al. The EQ-5D-5L valuation study in Korea. Qual Life Res. 2016;25:1845–1852. doi:10.1007/s11136-015-1205-2
31. Kim S-H, Jo M-W, Ahn J, Ock M, Shin S, Park J. Assessment of psychometric properties of the Korean SF-12 v2 in the general population. BMC Public Health. 2014;14:1–7. doi:10.1186/1471-2458-14-1086
32. Dworkin RH, Turk DC, Farrar JT, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005;113(1–2):9–19. doi:10.1016/j.pain.2004.09.012
33. Woaye-Hune P, Hardouin J-B, Lehur P-A, Meurette G, Vanier A. Practical issues encountered while determining minimal clinically important difference in patient-reported outcomes. Health Qual Life Outcomes. 2020;18(1):1–13. doi:10.1186/s12955-020-01398-w
34. Jakobsen JC, Gluud C, Wetterslev J, Winkel P. When and how should multiple imputation be used for handling missing data in randomised clinical trials–a practical guide with flowcharts. BMC Med Res Method. 2017;17(1):1–10. doi:10.1186/s12874-017-0442-1
35. Van Buuren S, Boshuizen HC, Knook DL. Multiple imputation of missing blood pressure covariates in survival analysis. Stat Med. 1999;18(6):681–694. doi:10.1002/(SICI)1097-0258(19990330)18:6<681::AID-SIM71>3.0.CO;2-R
36. Angst F, Aeschlimann A, Angst J. The minimal clinically important difference raised the significance of outcome effects above the statistical level, with methodological implications for future studies. J Clin Epidemiol. 2017;82:128–136. doi:10.1016/j.jclinepi.2016.11.016
37. Bijur PE, Silver W, Gallagher EJ. Reliability of the visual analog scale for measurement of acute pain. Acad Emergency Med. 2001;8(12):1153–1157. doi:10.1111/j.1553-2712.2001.tb01132.x
38. Kim TH, Jo M-W, S-i L, Kim SH, Chung SM. Psychometric properties of the EQ-5D-5L in the general population of South Korea. Qual Life Res. 2013;22:2245–2253. doi:10.1007/s11136-012-0331-3
39. Hayes CJ, Bhandari NR, Kathe N, Payakachat N. Reliability and validity of the medical outcomes study short form-12 version 2 (SF-12v2) in adults with non-cancer pain. MDPI. 2017;2017:1.
40. Portney LG, Watkins MP. Foundations of Clinical Research: Applications to Practice. Vol. 892. Pearson/Prentice Hall Upper Saddle River, NJ;2009.
41. Revicki D, Hays RD, Cella D, Sloan J. Recommended methods for determining responsiveness and minimally important differences for patient-reported outcomes. J Clin Epidemiol. 2008;61(2):102–109. doi:10.1016/j.jclinepi.2007.03.012
42. Rahim-Williams B, Riley JL III, Williams AK, Fillingim RB. A quantitative review of ethnic group differences in experimental pain response: do biology, psychology, and culture matter? Pain Med. 2012;13(4):522–540. doi:10.1111/j.1526-4637.2012.01336.x
43. Kim HJ, Yang GS, Greenspan JD, et al. Racial and ethnic differences in experimental pain sensitivity: systematic review and meta-analysis. pain. 2017;158(2):194–211. doi:10.1097/j.pain.0000000000000731
44. Campbell CM, Edwards RR. Ethnic differences in pain and pain management. Pain Manag. 2012;2(3):219–230. doi:10.2217/pmt.12.7
45. Ostrom C, Bair E, Maixner W, et al. Demographic predictors of pain sensitivity: results from the OPPERA study. J Pain. 2017;18(3):295–307. doi:10.1016/j.jpain.2016.10.018
46. Ahn H, Weaver M, Lyon D, et al. Differences in clinical pain and experimental pain sensitivity between Asian Americans and whites with knee osteoarthritis. Clin J Pain. 2017;33(2):174. doi:10.1097/AJP.0000000000000378
47. Rezai M, Côté P, Cassidy JD, Carroll L. The association between prevalent neck pain and health-related quality of life: a cross-sectional analysis. Eur Spine J. 2009;18:371–381. doi:10.1007/s00586-008-0823-6
48. Nolet PS, Côté P, Kristman VL, Rezai M, Carroll LJ, Cassidy JD. Is neck pain associated with worse health-related quality of life 6 months later? A population-based cohort study. Spine J. 2015;15(4):675–684. doi:10.1016/j.spinee.2014.12.009
49. Hey HWD, Lim JXY, Ong JZ, Luo N. Epidemiology of neck pain and its impact on quality-of-life—A population-based, cross sectional study in Singapore. Spine. 2021;46(22):1572–1580. doi:10.1097/BRS.0000000000004071
50. Evans R, Bronfort G, Maiers M, Schulz C, Hartvigsen J. “I know it’s changed”: a mixed-methods study of the meaning of global perceived effect in chronic neck pain patients. Eur Spine J. 2014;23:888–897. doi:10.1007/s00586-013-3149-y
51. Walton DM, MacDermid JC, Taylor T. What does ‘recovery’mean to people with neck pain? Results of a descriptive thematic analysis. Open Orthopaedics J. 2013;7(1):420–427. doi:10.2174/1874325001307010420
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Hemophilic Arthropathy: Barriers to Early Diagnosis and Management
Cuesta-Barriuso R, Donoso-Úbeda E, Meroño-Gallut J, Ucero-Lozano R, Pérez-Llanes R
Journal of Blood Medicine 2022, 13:589-601
Published Date: 17 October 2022