Back to Journals » Infection and Drug Resistance » Volume 17
Microbiological Profile of Patients with Aspiration Pneumonia Identified by Combined Detection Methods
Authors Xu H, Zhang R, Zhang X, Cheng Y, Lv L ![]() , Lin L
, Lin L
Received 30 January 2024
Accepted for publication 12 May 2024
Published 25 May 2024 Volume 2024:17 Pages 2077—2088
DOI https://doi.org/10.2147/IDR.S461935
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sandip Patil
Hui Xu,1 Ruixue Zhang,1 Xiaoxue Zhang,1 Yueguang Cheng,2 Liping Lv,3 Lianjun Lin1
1Department of Geriatrics, Peking University First Hospital, Beijing, People’s Republic of China; 2Department of Emergency, Beijing Jingmei Group General Hospital, Beijing, People’s Republic of China; 3Department of Interventional Pulmonology, Anhui Chest Hospital, Hefei, People’s Republic of China
Correspondence: Lianjun Lin, Department of Geriatrics, Peking University First Hospital, Xishiku Avenue 8, Xicheng District, Beijing, 100034, People’s Republic of China, Tel +8613671246076, Fax +86-10-83572981, Email [email protected]
Purpose: Aspiration pneumonia (AP) challenges public health globally. The primary aim of this study was to ascertain the microbiological profile characteristics of patients with AP evaluated by combined detection methods, including conventional microbiological tests (CMTs), chips for complicated infection detection (CCID), and metagenomic next-generation sequencing (mNGS).
Patients and Methods: From June 2021 to March 2022, a total of thirty-nine patients with AP or community-acquired pneumonia with aspiration risk factors (AspRF-CAP) from 3 hospitals were included. Respiratory specimens, including bronchoalveolar lavage fluid (BALF), sputum, and tracheal aspirate, were collected for microorganism detection.
Results: Patients with AP were more inclined to be older, to have a shorter duration from illness onset to admission, to have a higher prevalence of different underlying diseases, particularly diabetes mellitus, chronic heart disease, and cerebrovascular disease, and to have a higher CURB-65 score (all P < 0.05). A total of 213 and 31 strains of microorganisms were detected in patients with AP and AspRF-CAP, respectively. The most common pathogens in AP were Corynebacterium striatum (17/213, 7.98%), Pseudomonas aeruginosa (15/213, 7.04%), Klebsiella pneumoniae (15/213, 7.04%), and Candida albicans (14/213, 6.57%). Besides, the most common pathogens in AspRF-CAP were Candida albicans (5/31, 16.13%), Pseudomonas aeruginosa (3/31, 9.68%) and Klebsiella pneumoniae (3/31, 9.68%). Moreover, Klebsiella pneumoniae (7/67, 10.45%) and Candida glabrata (5/67, 7.46%) were the most common pathogens among the 9 non-survived patients with AP.
Conclusion: The prevalent pathogens detected in cases of AP were Corynebacterium striatum, Pseudomonas aeruginosa, Klebsiella pneumoniae, and Candida albicans. Early combined detection methods for patients with AP enhance the positive detection rate of pathogens and potentially expedites the initiation of appropriate antibiotic therapeutic strategies.
Keywords: aspiration, pneumonia, microbiology, metagenomic next-generation sequencing, chips, combined detection
Introduction
Aspiration is defined as the inhalation of oropharyngeal or gastric contents into the larynx and lower respiratory tract.1 Aspiration pneumonia (AP) refers to the process of alveolar and systemic inflammation caused by the inhalation of oropharyngeal or gastrointestinal secretions colonized by pathogenic bacteria into the lower respiratory tract.2 Multiple risk factors, such as impaired swallowing, impaired cough reflex, impaired consciousness, degenerative neurologic diseases, dementia, stroke, and enteral tube feeding, are associated with AP.1,3 Our previous study has reported that the incidence rates of hospitalized AP and pneumonia patients with aspiration risk factors (AspRF) were 9.4 and 102.9 per 100,000 person-years, respectively.4 The incidences of AP increased rapidly with age.4 It has been reported that patients with AP have higher morbidity and mortality than those with non-aspiration community-acquired pneumonia (CAP).5 Significant healthcare and economic burdens are foreseeable as the population ages and the prevalence of AP increases.
However, prophylactic use of antibiotics in AP does not provide clinical benefit and may drive resistance, resulting in the need for escalation of antibiotic therapy for patients with AP.6 Additionally, inadequate empirical antimicrobial therapy may contribute to significant increase of mortality.7 Therefore, early identification and characterization of AP pathogens is critical for administering appropriate antimicrobial treatment and improving clinical outcomes. Accumulating evidence revealed a fading importance of anaerobic bacteria in AP, with Escherichia coli, Staphylococcus aureus, Klebsiella pneumoniae, and Pseudomonas aeruginosa, becoming common causative organisms.5,8 Besides, another study reported that Streptococcus pneumoniae was the leading pathogen in CAP patients with AspRF (AspRF-CAP).9 There are many difficulties in the detection of AP and AspRF-CAP pathogens. Firstly, the isolation and identification rates of the causative pathogens of AP and AspRF-CAP are usually tend to be low, with poor sensitivity and time-consuming due to the application of empirical therapy and antimicrobial agents.10 Secondly, polymicrobial infections are common in severe pneumonia, while conventional microbial culture is not easy to detect simultaneously. Moreover, conventional microbiological tests (CMTs) utilized in clinical microbiology laboratories have certain limitations.11 The technique is time-consuming and limited in their scope for pathogen detection, making it unsuitable for identifying unknown or difficult-to-culture pathogens. Advances in molecular diagnostic techniques have improved the potential of the identification and characterization of the role of existing and previously unrecognized AP and AspRF-CAP pathogens. Chips for complicated infection detection (CCID) is a novel technique for rapid detection of pathogenic microorganisms.12 Our previous multicenter prospective observational study has shown that CCID was promising in elderly patients with pneumonia due to its potential to rapidly and accurately detect multiple pathogenic microorganisms and was less affected by prior antimicrobial therapy.12 In addition, metagenomic next-generation sequencing (mNGS), as a hypothesis-free, unbiased, and culture-independent modality, has been progressively applied in the etiological diagnosis of respiratory tract infection.13,14 In view of the complexity of the etiology of AP and AspRF-CAP and the unsatisfactory detection techniques of pathogens, multiplexed detection techniques with high sensitivity and accuracy are required.
Establishing the etiological diagnosis of AP and AspRF-CAP enables individualized treatment, such as appropriate selection of antibiotics, mitigating broad-spectrum antibiotic abuse, promoting effective antimicrobial stewardship, and ultimately improving patient recovery.15 Increased sensitivity, affordability, and availability of molecular pathogen detection techniques have significantly improved the understanding of AP and AspRF-CAP etiology.16 However, there is a lack of research on the etiology of Chinese AP and AspRF-CAP. Therefore, the primary objective of this prospective study was to describe the microbiological profile and clinical features of adult patients with AP and AspRF-CAP and to evaluate the benefit of combined testing for the etiological diagnosis of AP and AspRF-CAP in China.
Materials and Methods
Study Design and Participants
From June 2021 to March 2022, we consecutively recruited patients from 3 hospitals, including Anhui Chest Hospital, Beijing Jingmei Group General Hospital, and Aerospace Center Hospital in China. Only inpatients aged ≥18 years with a definite diagnosis of CAP were included in the study.17 Patients with hospital-acquired or ventilator-associated pneumonia, active tuberculosis or bronchiectasis, immunosuppressed, with missing data, and not sent for mNGS, CCID, and CMTs simultaneously were excluded. The subjects were stratified in AP and AspRF-CAP groups. The diagnosis of AP primarily rests on the principles of a characteristic clinical history (witnessed macro-aspiration), risk factors, and chest radiographic findings.2,3 AspRF includes advanced age, male, dysphagia, head and neck cancer, upper gastrointestinal disease, reduced conscious level, degenerative neurologic diseases (parkinsonism, dementia, and multiple sclerosis), chronic obstructive pulmonary disease, alcohol dependence, and sedative drug abuse.2,3,18 AspRF-CAP was defined as CAP patients with AspRF.3,9
A total of 94 patients with CAP from three hospitals were eligible for screening (Figure 1). After exclusion of 12 (12.8%) patients with active tuberculosis or bronchiectasis, 9 (9.6%) patients in immunosuppressive condition, 8 (8.5%) cases with missing data, and 26 (27.6%) patients not sent for mNGS, CCID, and CMTs simultaneously, 39 (41.5%) patients were finally included for the following analysis.
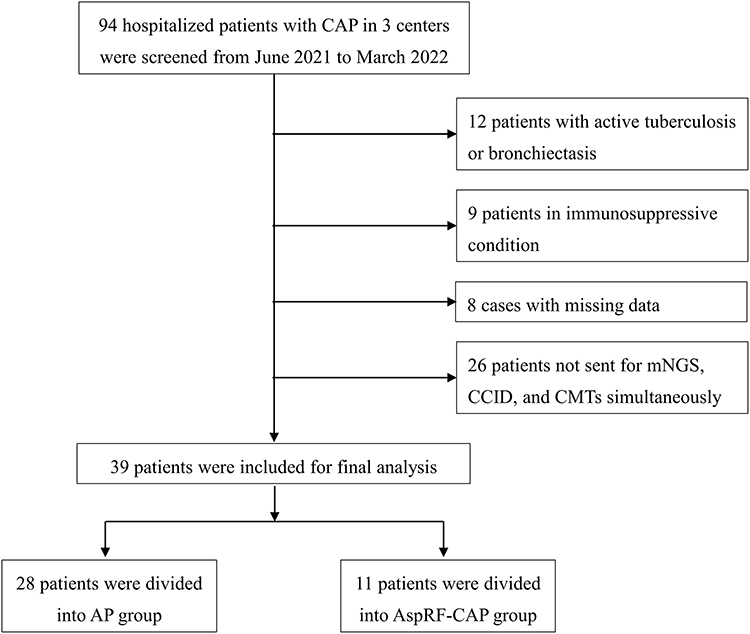 |
Figure 1 Flowchart of the participants included in the present study. |
Study protocols were reviewed and approved by the Ethics Committee of Peking University First Hospital (approval number 2021–132). All procedures followed were in accordance with the ethical standards of the responsible committees and with Declaration of Helsinki. Informed consents were obtained from each participant or legal guardians.
Data Collection and Definition
Data on demographic and clinical characteristics, including age, sex, smoking status, medical history (including chronic obstructive pulmonary disease, diabetes mellitus, hypertension, chronic renal disease, chronic heart disease, cerebrovascular disease, malignant), and duration from illness onset to admission were collected. Respiratory rate and blood pressure were measured by professional nurses. Biochemical parameters, including blood routine, liver function, kidney function, serum electrolytes, and coagulation function were extracted during hospitalization. In-hospital mortality was taken from medical records. BALF amylase levels were measured using an enzyme-linked immunosorbent assay kit (ab137969, Abcam, Cambridge, UK). The CURB-65 score was determined in patients with pneumonia for the assessment of severity in CAP, consisting of 5 variables, one point for each item: new onset confusion, Urea > 7 mmol/L, respiratory rate ≥ 30 times/minute, systolic blood pressure < 90 mmHg and/or diastolic blood pressure ≤ 60 mmHg, and age ≥ 65 years.19 CURB-65 ≥ 3 was defined as severe pneumonia.20
Sample Collection and Pathogen Detection
Blood samples and qualified respiratory specimens, including sputum, tracheal aspirates, and BALF were collected for pathogen detection. CMTs included smear, culture, antigen detection, and serological tests. Culture and smear microscopy (except for special staining) were performed on each included specimen. Other CMT tests were performed according to the type of specimen and clinically suspected pathogens, and it is not required that every patient receives all types of CMTs testing.
For CCID, the volume of sputum and BALF should be at least 2 mL and 3 mL, respectively. Pathogens were detected by the Pathogenic Bacteria Nucleic Acid Detection Kit (CapitalBio Technology, Beijing, China) and RTisochip-A nucleic acid analyzer (CapitalBio Technology, Beijing, China). Data were analyzed by nucleic acid detection software. The chip was able to identify 47 bacterial species, 22 fungal species and 21 viruses.12
The workflow of mNGS includes sample pretreatment and nucleic acid extraction, library preparation, high-throughput sequencing, and bioinformatics analysis. Nucleic acid extraction and library preparation were performed. Sequenced on the BioelectronSeq 4000 sequencer (CapitalBio Corporation, Beijing, China). High-quality sequencing data was generated by removing low-quality and short (<50 bp in length) reads. The human host sequence mapping to the human reference genome (hg19) was then computationally subtracted using the Burrows-Wheeler alignment. The remaining data after the removal of low-complexity reads were classified by simultaneous comparison of four microbial genome databases, including bacteria, fungi, viruses, and parasites.21
Statistical Analysis
Continuous variables were presented as median and interquartile range (IQR) and compared by Mann–Whitney U-test. Categorical variables were reported as frequency and percentages (%) and analyzed by Fisher’s exact test. The concordance between the different detection methods was examined using kappa statistics. Statistical analysis and figures were performed using GraphPad Prism 9.0 software (GraphPad Prism Inc., San Diego, CA, USA), R software (version 4.3.1, R Development Core Team), and SPSS 26.0 software (SPSS, Chicago, IL, USA), and data were transferred to Excel spreadsheets. P values <0.05 signified statistical significance.
Results
Clinical Characteristics
A total of 39 patients were included for the following analysis, including 28 (71.8%) AP patients and 11 (28.2%) AspRF-CAP subjects. The median age was 77 years old (IQR: 69–84 years), 25 (64.1%) patients were male, the median duration from illness onset to admission was 2 days (IQR: 1–15 days). Besides, 33 (84.6%) cases suffered from different underlying diseases, cerebrovascular disease (28/39, 71.8%) and hypertension (21/39, 53.8%) were the most common underlying conditions. Compared with AspRF-CAP, patients with AP were more inclined to be older, to have a shorter duration from illness onset to admission, to have a higher prevalence of different underlying diseases, especially diabetes mellitus, chronic heart disease, and cerebrovascular disease, to have a lower proportion of cough, and to have a higher CURB-65 score (all P < 0.05, Table 1). Besides, 11 patients (28.2%) died in hospital, 9 of whom were diagnosed with AP. Moreover, the levels of BALF amylase and blood glucose in AP group were significantly higher than those with AspRF-CAP, as presented in Table S1. No significant differences were observed in other investigated biochemical parameters.
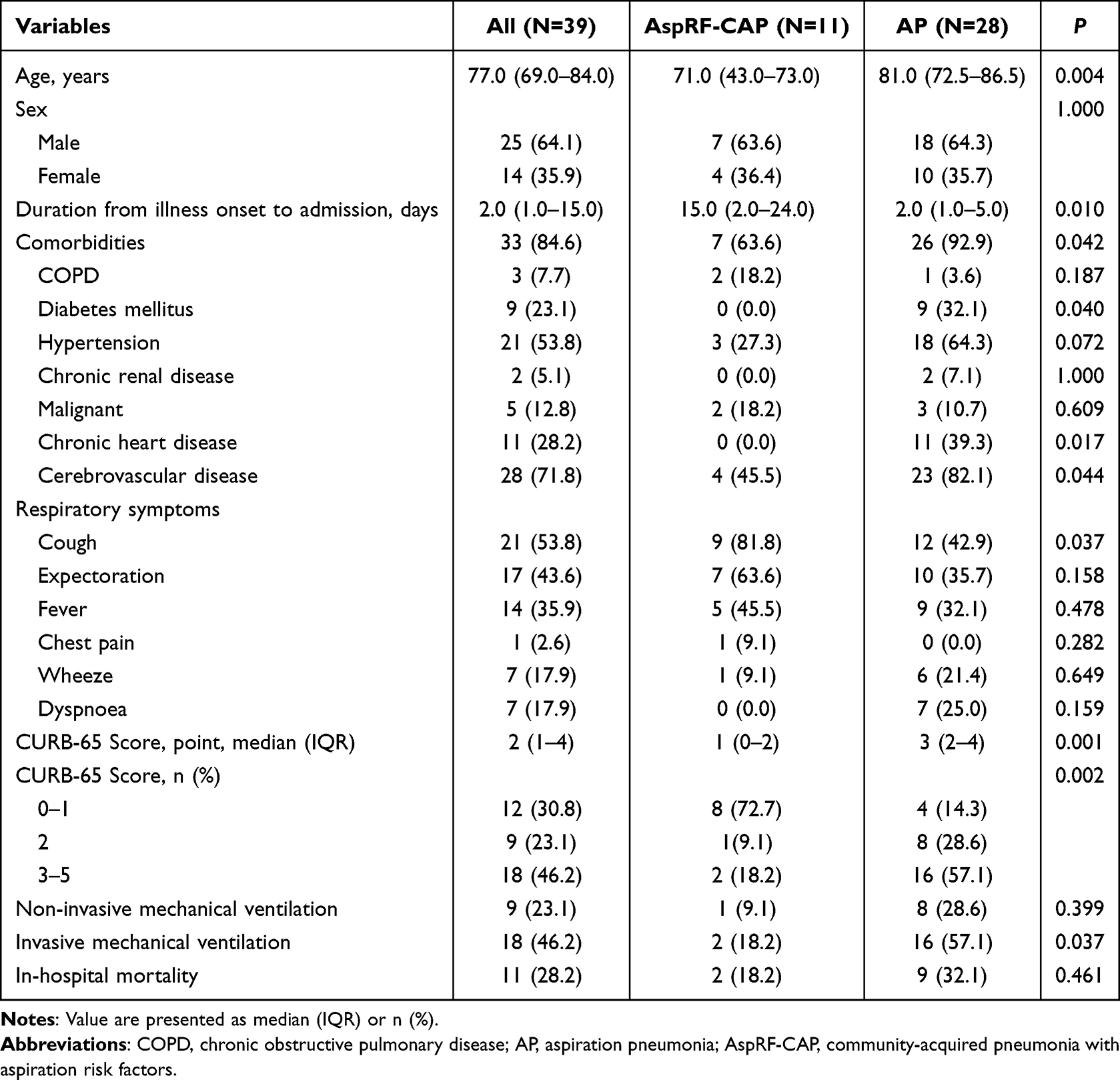 |
Table 1 Clinical Characteristics of the Study Participants |
Microorganisms in AP and AspRF-CAP
Of the 28 patients with AP, 1 (3.57%) case was bacterial pathogen only, 27 (96.43%) cases were co-detection, of which 13 (48.15%) were bacterial and fungal co-detection, 1 (3.70%) was bacterial and viral co-detection, 13 (48.15%) were bacterial, fungal and viral co-detection (Figure 2). Among the 213 strains of isolated pathogens, the predominant detected microorganisms were Corynebacterium striatum (17/213, 7.98%), Pseudomonas aeruginosa (15/213, 7.04%) and Klebsiella pneumoniae (15/213, 7.04%). In addition, the most common fungal pathogen was Candida albicans (14/213, 6.57%) and the most common viral pathogen was herpes simplex virus type 1 (7/213, 3.29%). Moreover, a total of 31 strains of pathogens were determined in the 11 patients with AspRF-CAP. The most common pathogens were Candida albicans (5/31, 16.13%), Pseudomonas aeruginosa (3/31, 9.68%) and Klebsiella pneumoniae (3/31, 9.68%).
 |
Figure 2 Microorganisms detected in patients with AP and AspRF-CAP. The column chart showed the numbers of microorganisms detected. A total of 213 and 31 strains of microorganisms were detected in patients with AP and AspRF-CAP, respectively. The left pie chart showed the detailed proportions of microorganism distribution in AP patients, including bacterial pathogen only (1/28, 3.57%), bacteria-fungi co-detection (13/28, 46.43%), bacteria-virus co-detection (1/28, 3.57%), and bacteria-fungi-virus co-detection (13/28, 46.43%). The right pie chart showed the detailed proportions of microorganism distribution in AspRF-CAP patients, including not detected (1/11, 9.09%), fungal pathogen only (1/11, 9.09%), bacteria-bacteria co-detection (1/11, 9.09%), fungi-fungi co-detection (1/11, 9.09%), bacteria-fungi co-detection (3/11, 27.28%), and bacteria-virus co-detection (4/11, 36.36%). |
Microorganisms in Severe and Non-Severe AP
Of the 16 patients with severe AP, a total of 123 pathogens have been identified, the most common pathogens were Corynebacterium striatum (10/123, 8.13%), Klebsiella pneumoniae (10/123, 8.13%), Candida albicans (9/123, 7.32%), and Pseudomonas aeruginosa (9/123, 7.32%). All of them were co-detected, of which bacterial and fungal co-detection (9/16, 56.25%) were the most common types. In addition, in 12 patients with non-severe AP, 90 pathogens were determined, and Candida glabrata (8/90, 8.89%) and Corynebacterium striatum (7/90, 7.78%) were the most common detected pathogens (Figure 3).
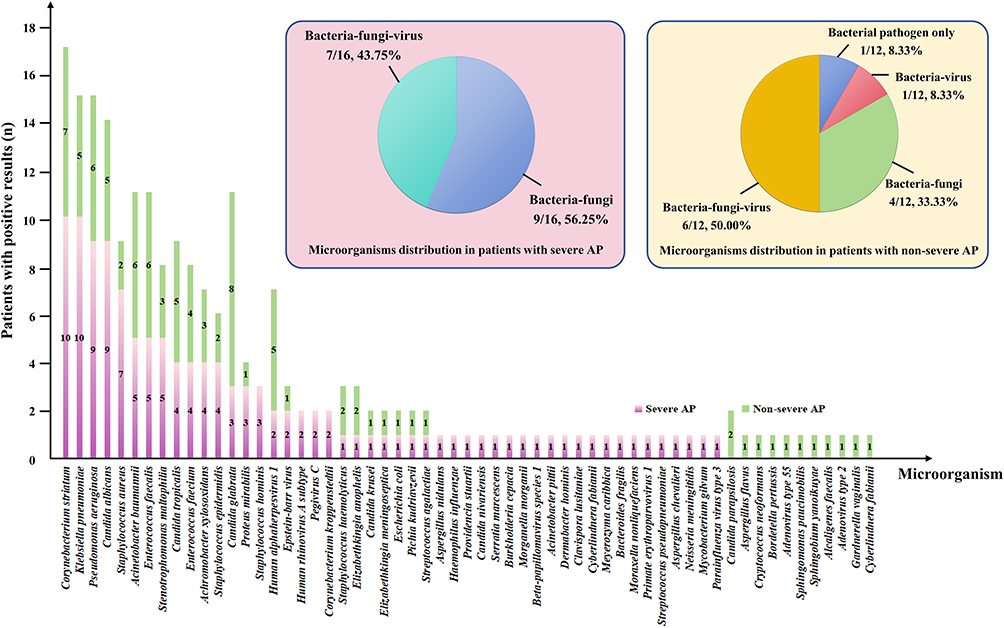 |
Figure 3 Comparison and overlap of isolated microorganisms between severe AP and non-severe AP. The column chart showed the numbers of microorganisms detected. A total of 123 and 90 strains of microorganisms were detected in 16 severe AP cases and 12 non-severe AP cases, respectively. The left pie chart showed the detailed proportions of microorganism distribution in severe AP patients, including bacteria-fungi co-detection (9/16, 56.25%) and bacteria-fungi-virus co-detection (7/16, 43.75%). The right pie chart showed the detailed proportions of microorganism distribution in non-severe AP patients, including bacterial pathogen only (1/12, 8.33%), bacteria-virus co-detection (1/12, 8.33%), bacteria-fungi co-detection (4/12, 33.33%), and bacteria-fungi-virus co-detection (6/12, 50.00%). |
Microorganisms in Non-Survived Patients
A total of 67 and 12 strains of pathogens were detected in non-survived patients with AP and AspRF-CAP, respectively. Klebsiella pneumoniae (7/67, 10.45%) and Candida glabrata (5/67, 7.46%) were the most common pathogens among the 9 non-survived patients with AP, whereas Corynebacterium striatum (2/12, 16.67%) and Candida glabrata (2/12, 16.67%) were the most common pathogens in the 2 non-survived AspRF-CAP patients (Figure 4).
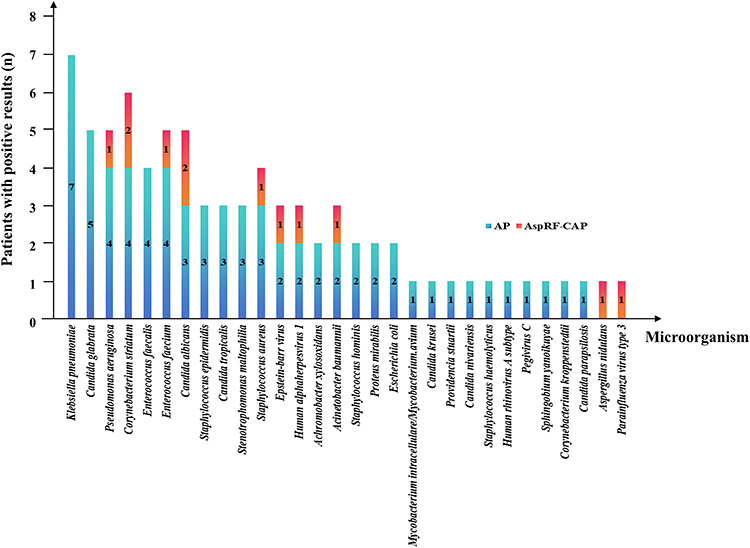 |
Figure 4 Microorganisms detected in non-survived patients. Klebsiella pneumoniae and Candida glabrata were the most common pathogens among the 9 non-survived AP patients, whereas Corynebacterium striatum and Candida glabrata were the most common pathogens in 2 non-survived AspRF-CAP patients. |
Comparison of Diagnostic Performance
Thirty-eight BALF samples, 30 sputum samples, and 1 tracheal aspirate sample were collected. The positive rate of pathogen in BALF was significantly higher than that of sputum samples (97.4% vs 70.0%, P = 0.002, Figure 5A). Among the 25 cases with consistent BALF samples, the positive rate of mNGS was significantly higher than that of CMTs (88.0% vs 80.0%, P = 0.004, Figure 5B). Figure 5C showed the specific pathogens detected by different detection methods. Additionally, the concordance between mNGS and CMTs was moderate (Kappa value = 0.435, Figure S1). Moreover, 27 (69.23%) cases had used antibiotics prior to specimen collection. No significant difference was observed between patients treated with antibiotics for ≤3 days and those >3 days (Figure S2).
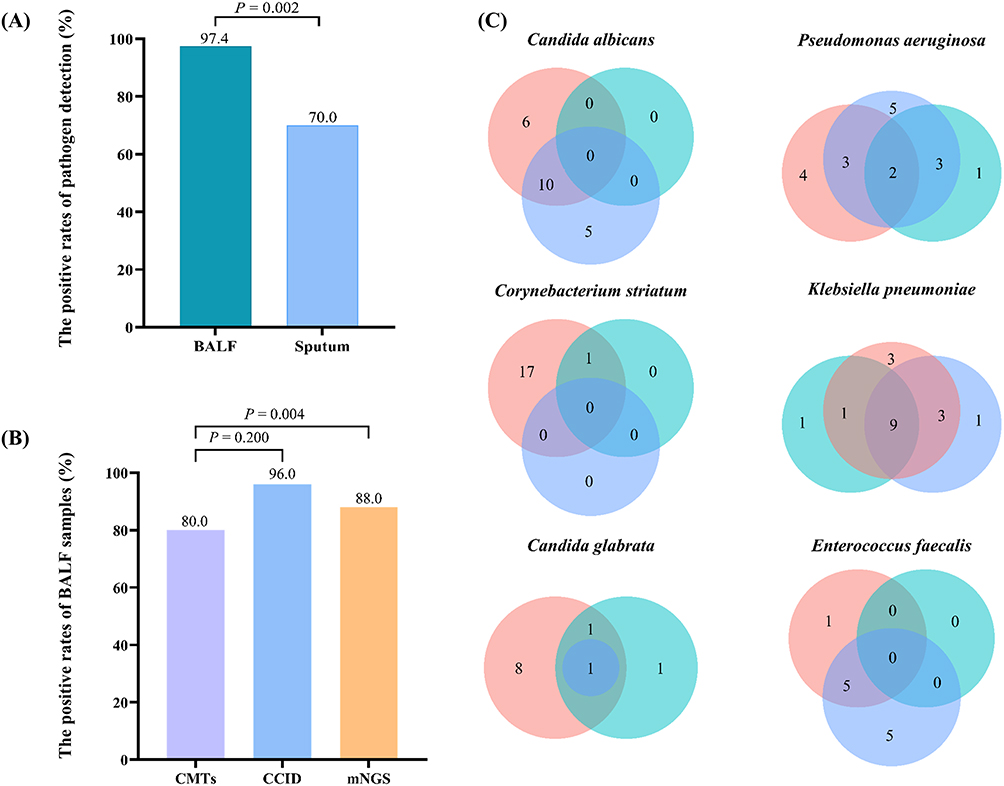 |
Figure 5 Comparison of diagnostic performance. (A) The positive rate of pathogen in BALF was significantly higher than that of sputum samples (97.4% vs 70.0%, P = 0.002). (B) The positive rate of pathogen with consistent BALF samples. The positive rate of mNGS was significantly higher than that of CMTs (88.0% vs 80.0%, P = 0.004). (C) Venn diagrams for specific pathogens detected according to different detected methods. Pink for mNGS. Blue for CCID. Cyan for CMTs. The numbers in the circles stand for cases. |
Discussion
In this prospective study, we evaluated the microbiological profile of AP and AspRF-CAP by combined detection techniques, including CMTs, CCID, and mNGS. The most commonly detected pathogens in AP were Corynebacterium striatum, Pseudomonas aeruginosa and Klebsiella pneumoniae, whereas the most common pathogens in AspRF-CAP were Candida albicans, Pseudomonas aeruginosa and Klebsiella pneumoniae. These findings update our understanding of the etiology of AP and may substantially improve the positive rate of clinical pathogen detection.
AP accounts for approximately 10–20% of CAP. Our data showed that patients with AP were more inclined to be older and to have a higher prevalence of different underlying conditions, particularly diabetes mellitus, chronic heart disease, and cerebrovascular disease, which was generally consistent with previous reports.18,22 The integrity of the oropharyngeal sensory system is essential for maintaining swallowing function. With the increase of age and underlying diseases, pharyngeal sensitivity and swallowing reactivity impaired, the protective reflex of epiglottis and glottis reduced, especially in the setting of cerebrovascular diseases, the swallowing function and cough reflex impaired, leading to an increased risk of AP.23–25 Clinically, AP is principally diagnosed relying on clinical history (witnessed macro-aspiration), risk factors, and chest radiography findings. It has been reported that bronchoalveolar lavage amylase serve as potential diagnostic biomarkers for distinguishing AP.26 In the present study, we observed that the levels of BALF amylase in AP group were significantly higher than those with AspRF-CAP (P = 0.004). Amylase was rarely generated in tracheal or bronchoalveolar cells. Thus, detection of BALF amylase indicated dysfunction of the swallowing reflex, which may hint aspiration of oral secretions. Unexpectedly, no significant difference was observed among the positive rate of CMTs, CCID, and mNGS between antibiotic treatment >3 days and ≤3 days. This may be partly attributable to the small sample size. Moreover, AP is a pulmonary infectious disease with a high mortality rate. The mortality of AP in our study was 32.1%, which was generally consistent with previous findings.4,27 The higher mortality rate in patients with AP may be explained by older age and a higher prevalence of comorbidities. Advanced age was at higher risk of mortality in AP, possibly due to reductions in immune responses and alternations in lung function, including age-related decline in functional residual capacity, pulmonary elasticity, and mucociliary transport.28,29 In view of the increase of the old population and physical degradation and compromised immunity in the elderly, it is necessary to strengthen the nursing of AP-related comorbidities.
A complex taxonomic landscape of lung bacteria has been described. However, the role of the microbiome in health and disease, especially in the pathogenesis of pneumonia, remains unclarified. Among the eligible patients, co-detection was identified in 96.43% and 81.82% of the patients with AP and AspRF-CAP, respectively, in which bacterial, fungal and viral co-detection was the most frequent types. A prospective study of 62 older adult hospitalized patients with AP revealed that anaerobic bacteria and aerobic bacteria co-existed in 66.7% of the dead patients.30 Moreover, it has been reported that polymicrobial infections are common in patients with AP.31
Over the past few decades, there has been a notable shift in the pathogens implicated in AP. In our study, Corynebacterium striatum, Pseudomonas aeruginosa, and Klebsiella pneumoniae were the most common pathogens in patients with AP. Corynebacterium striatum is part of the human skin and nasal mucosa microbiota that has been increasingly reported as an etiologic cause of pulmonary infection.32 A systematic review identified that Escherichia coli, along with Klebsiella pneumoniae and Pseudomonas aeruginosa, were pathogenic microorganisms in the oral microbiome of elderly patients with AP, especially for those in residential care.33 Klebsiella pneumoniae and Pseudomonas aeruginosa regularly inhabit the gut and respiratory tract of healthy individuals and are common causative pathogens of pneumonia. Poor oral hygiene was considered to be the primary source of pathogens for AP.34 In addition, the presence of gut microbiota in respiratory specimens may connected with the gastro-esophageal reflux experienced by many patients with AP, particularly those with dysphagia. A study of patients with AP in respiratory intensive care unit revealed that the predominant isolated microorganisms were Candida spp, Pseudomonas aeruginosa, Staphylococcus aureus, Acinetobacter baumannii, and Klebsiella pneumoniae in community-acquired cases, whereas Acinetobacter baumannii, Pseudomonas aeruginosa, Candida spp, and Klebsiella pneumonia were the main isolates in hospital-acquired AP.35
Viruses play an increasingly important role in the pathogenesis of AP. In the present study, herpes simplex virus type 1 was the top virus in AP. It has been reported that herpes simplex virus type 1 was in connection with lung disease and usually identified in respiratory secretions of critically ill patients.36 A multicenter retrospective study exploited mNGS testing of BALF revealed that herpes simplex virus type 1 was one of the most common reactivated viruses in the lower respiratory tract of patients with severe pneumonia and was associated with an increased risk of mortality.37 Therefore, large-scale prospective studies are required to determine the causative role of herpes simplex virus type 1 and other viruses in AP. The management strategies of AP should include rapid detection of viruses and to assess whether individual patients need antiviral therapy.
Among patients with AspRF-CAP, Candida albicans, Pseudomonas aeruginosa and Klebsiella pneumoniae were the main microorganisms. In contrast to our findings, an analysis of a hospitalized UK cohort reported that the predominant microorganisms isolated in patients at risk of aspiration were Streptococcus pneumoniae, Haemophilus influenzae, Gram-negative Enterobacteriaceae, and Staphylococcus aureus.38 Patients with AP had a higher rate of Pseudomonas aeruginosa (11.3% vs 3.8%, P = 0.015) and a lower rate of Streptococcus pneumoniae (1.4% vs 5.9%, P = 0.032) compared to patients with AspRF-CAP.9
Additionally, in our study, Candida spp were a significant emerging microorganism isolated from patients with AP and AspRF-CAP, contributing to 18.3% and 19.4% of the AP and AspRF-CAP cases, respectively. Infectious disease specialists suggest that pneumonia caused by Candida spp is a “very rare event”.39 These microorganisms normally colonize the mouth. Depending on respiratory sample cultures for etiological diagnosis of pneumonia does not always distinguish between colonization and infection.40 Recent studies have revealed the potential causative role of the combination of Candida spp and bacterial pathogens in pneumonia. Patients with CAP who had large amounts of Candida spp in their respiratory samples all had a history consistent with aspiration and in each case was polymicrobial infection, suggesting a contributing role of Candida spp in the etiology of AspRF-CAP.41
Moreover, of patients with severe AP, the most common isolated microorganisms were Corynebacterium striatum, Klebsiella pneumoniae, Candida albicans, and Pseudomonas aeruginosa. A study included hospitalized elderly patients with severe AP, Gram-negative bacteria (Escherichia coli, Klebsiella pneumoniae, Serratia spp and Proteus mirabilis) were the most pathogens, followed by anaerobic bacteria (Prevotella and Fusobacterium) and Staphylococcus aureus.42 Another study showed that among the bacterial pathogens of AP pleural infection identified by mNGS, the most common was Fusobacterium nucleatum, followed by Parvimonas micra and Filifactor alocis.43 The microbial etiology of AP and AspRF-CAP may hinge on multiple aspects. Demographics (such as age, sex, smoking habits), comorbidities (such as neurological disorders), laboratory techniques (sample collection and culture techniques, etc.), patient-related factors (such as host factors and past antibiotic use), and clinical definitions and diagnostic criteria for AP may contribute to differences in pathogen detection results.44,45 Notably, advances in molecular diagnostic techniques have improved the potential of the identification and characterization of the role of existing and previously unrecognized AP and AspRF-CAP pathogens.
Some limitations are noted. Firstly, while we characterized the microbiological profile of AP using combined detection methods, we did not differentiate between colonizing and responsible microorganisms. Future research should aim to address this gap by employing additional diagnostic tools and clinical correlations to better understand the role of microorganisms in the pathogenesis of AP. Secondly, our CCID and mNGS assays were sent to the central laboratory rather than an in-house microbiological laboratory, which may have sacrificed sensitivity rate due to increased turnaround times from bedside to bench. Thirdly, the sample size of the present study was small, and there was a potential selection bias. Large multicenter studies are needed to strengthen and improve the findings.
Conclusion
Through the combination of CMTs, CCID and mNGS techniques, the multicenter prospective study clarified the microbiological profile of patients with AP and AspRF-CAP. Corynebacterium striatum, Pseudomonas aeruginosa, Klebsiella pneumoniae, and Candida albicans were the most common pathogens detected of AP in China, whereas Candida albicans, Pseudomonas aeruginosa and Klebsiella pneumoniae were the most common isolated microorganisms of AspRF-CAP. In the new era of emerging molecular techniques, early combined detection improves the identification rate of pathogens and may facilitate early antibiotic de-escalation, thereby avoiding unnecessary broad-spectrum antibiotics and pernicious consequences. Moreover, application of mNGS may facilitate early identification of uncommon pathogens.
Abbreviations
AP, aspiration pneumonia; CMTs, conventional microbiological tests; CCID, chips for complicated infection detection; mNGS, metagenomic next-generation sequencing; BALF, bronchoalveolar lavage fluid; AspRF-CAP, community-acquired pneumonia with aspiration risk factors.
Data Sharing Statement
Due to the personal privacy of the patients included in this study, the data sets used and analyzed in this study are not publicly available but are available from the corresponding authors upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by The Ethics Committee of Peking University First Hospital (approval number 2021-132) and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from each participant or legal guardians.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This work was supported by National Key Research and Development Program of China (Grant number: 2020YFC2005401).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ogura K, Endo M, Hase T, et al. Potential biomarker proteins for aspiration pneumonia detected by shotgun proteomics using buccal mucosa samples: a cross-sectional case–control study. Clin Proteomics. 2023;20(1):9. doi:10.1186/s12014-023-09398-w
2. Simpson AJ, Allen JL, Chatwin M, et al. BTS clinical statement on aspiration pneumonia. Thorax. 2023;78(Suppl 1):s3–s21. doi:10.1136/thorax-2022-219699
3. Mandell LA, Niederman MS. Aspiration Pneumonia. New England Journal of Medicine. 2019;380(7):651–663. doi:10.1056/NEJMra1714562
4. Zhang Y, Wang K, Yu H, et al. Incidence and characteristics of aspiration pneumonia in adults in Beijing, China, 2011–2017. Public Health. 2023;220:65–71. doi:10.1016/j.puhe.2023.04.021
5. Neill S, Dean N. Aspiration pneumonia and pneumonitis: a spectrum of infectious/noninfectious diseases affecting the lung. Curr Opin Infect Dis. 2019;32(2):152–157. doi:10.1097/QCO.0000000000000524
6. Dragan V, Wei Y, Elligsen M, Kiss A, Walker SAN, Leis JA. Prophylactic antimicrobial therapy for acute aspiration pneumonitis. Clin Infect Dis. 2018;67(4):513–518. doi:10.1093/cid/ciy120
7. Maskell NA, Batt S, Hedley EL, Davies CWH, Gillespie SH, Davies RJO. The bacteriology of pleural infection by genetic and standard methods and its mortality significance. Am J Respir Crit Care Med. 2006;174(7):817–823. doi:10.1164/rccm.200601-074OC
8. DiBardino DM, Wunderink RG. Aspiration pneumonia: a review of modern trends. J Crit Care. 2015;30(1):40–48. doi:10.1016/j.jcrc.2014.07.011
9. Marin-Corral J, Pascual-Guardia S, Amati F, et al. Aspiration risk factors, microbiology, and empiric antibiotics for patients hospitalized with community-acquired pneumonia. Chest. 2021;159(1):58–72. doi:10.1016/j.chest.2020.06.079
10. Li N, Ma X, Zhou J, et al. Clinical application of metagenomic next-generation sequencing technology in the diagnosis and treatment of pulmonary infection pathogens: a prospective single-center study of 138 patients. J Clin Lab Anal. 2022;36(7):e24498. doi:10.1002/jcla.24498
11. Deng W, Xu H, Wu Y, Li J. Diagnostic value of bronchoalveolar lavage fluid metagenomic next-generation sequencing in pediatric pneumonia. Front Cell Infect Microbiol. 2022;12:950531. doi:10.3389/fcimb.2022.950531
12. Wei S, Wang L, Shi M, et al. Rapid, accurate, and novel diagnostic technique for respiratory pathogens: clinical application of loop-mediated isothermal amplification assay in older patients with pneumonia, a multicenter prospective observational study. Frontiers in Microbiology. 2022;13:1048997. doi:10.3389/fmicb.2022.1048997
13. Chen S, Kang Y, Li D, Li Z. Diagnostic performance of metagenomic next-generation sequencing for the detection of pathogens in bronchoalveolar lavage fluid in patients with pulmonary infections: systematic review and meta-analysis. Int J Infect Dis. 2022;122:867–873. doi:10.1016/j.ijid.2022.07.054
14. Li J, Zhou C, Wei S, et al. Diagnostic value of metagenomic next-generation sequencing for pneumonia in immunocompromised patients. Can J Infect Dis Med Microbiol. 2022;2022:5884568. doi:10.1155/2022/5884568
15. Papadopoulos D, Bader I, Gkioxari E, et al. Microbiology and prognosis assessment of hospitalized patients with aspiration pneumonia: a single-center prospective cohort study. Infez Med. 2018;26(2):103–114.
16. Cilloniz C, Liapikou A, Torres A. Advances in molecular diagnostic tests for pneumonia. Curr Opin Pulm Med. 2020;26(3):241–248. doi:10.1097/MCP.0000000000000668
17. Cao B, Huang Y, She D, et al. Diagnosis and treatment of community‐acquired pneumonia in adults: 2016 clinical practice guidelines by the Chinese Thoracic Society, Chinese Medical Association. Clin Respir J. 2018;12(4):1320–1360. doi:10.1111/crj.12674
18. Zhao T, Zhang Y, Wang K, et al. Identifying risk factors for aspiration in patients hospitalized with community-acquired pneumonia. Int J Clin Pract. 2023;2023:2198259. doi:10.1155/2023/2198259
19. Nguyen Y, Corre F, Honsel V, et al. Applicability of the CURB-65 pneumonia severity score for outpatient treatment of COVID-19. J Infect. 2020;81(3):e96–e98. doi:10.1016/j.jinf.2020.05.049
20. Hamaguchi S, Suzuki M, Sasaki K, et al. Six underlying health conditions strongly influence mortality based on pneumonia severity in an ageing population of Japan: a prospective cohort study. BMC Pulm Med. 2018;18:88. doi:10.1186/s12890-018-0648-y
21. Miao Q, Ma Y, Wang Q, et al. Microbiological diagnostic performance of metagenomic next-generation sequencing when applied to clinical practice. Clin Infect Dis. 2018;67(suppl_2):S231–S240. doi:10.1093/cid/ciy693
22. Wakabayashi T, Hamaguchi S, Morimoto K; Adult Pneumonia Study Group – Japan. Clinically defined aspiration pneumonia is an independent risk factor associated with long-term hospital stay: a prospective cohort study. BMC Pulm Med. 2023;23(1):351. doi:10.1186/s12890-023-02641-y
23. Rofes L, Ortega O, Vilardell N, Mundet L, Clavé P. Spatiotemporal characteristics of the pharyngeal event-related potential in healthy subjects and older patients with oropharyngeal dysfunction. Neurogastroenterol Motil. 2017;29(2). doi:10.1111/nmo.12916
24. Costa A, Carrión S, Puig-Pey M, Juárez F, Clavé P. Triple adaptation of the Mediterranean diet: design of a meal plan for older people with oropharyngeal dysphagia based on home cooking. Nutrients. 2019;11(2):425. doi:10.3390/nu11020425
25. Banda KJ, Chu H, Kang XL, et al. Prevalence of dysphagia and risk of pneumonia and mortality in acute stroke patients: a meta-analysis. BMC Geriatr. 2022;22(1):420. doi:10.1186/s12877-022-02960-5
26. Suzuki T, Saitou M, Utano Y, Utano K, Niitsuma K. Bronchoalveolar lavage (BAL) amylase and pepsin levels as potential biomarkers of aspiration pneumonia. Pulmonology. 2023;29(5):392–398. doi:10.1016/j.pulmoe.2022.04.003
27. Gupte T, Knack A, Cramer JD. Mortality from aspiration pneumonia: incidence, trends, and risk factors. Dysphagia. 2022;37(6):1493–1500. doi:10.1007/s00455-022-10412-w
28. Palacios-Ceña D, Hernández-Barrera V, López-de-Andrés A, et al. Time trends in incidence and outcomes of hospitalizations for aspiration pneumonia among elderly people in Spain (2003–2013). Eur J Intern Med. 2017;38:61–67. doi:10.1016/j.ejim.2016.12.022
29. Shin D, Lebovic G, Lin RJ. In-hospital mortality for aspiration pneumonia in a tertiary teaching hospital: a retrospective cohort review from 2008 to 2018. J Otolaryngol Head Neck Surg. 2023;52(1):23. doi:10.1186/s40463-022-00617-2
30. Tokuyasu H, Harada T, Watanabe E, et al. Effectiveness of meropenem for the treatment of aspiration pneumonia in elderly patients. Intern Med. 2009;48(3):129–135. doi:10.2169/internalmedicine.48.1308
31. Wang H, Wu X, Wang Q, Liu G, Li C. Clinical features and prognosis of aspiration pneumonia compared with non-aspiration pneumonia in the elderly patients. Journal of the American Geriatrics Society. 2016; 64:S344–S345.
32. Yang K, Kruse RL, Lin WV, Musher DM. Corynebacteria as a cause of pulmonary infection: a case series and literature review. Pneumonia. 2018;10:10. doi:10.1186/s41479-018-0054-5
33. Khadka S, Khan S, King A, Goldberg LR, Crocombe L, Bettiol S. Poor oral hygiene, oral microorganisms and aspiration pneumonia risk in older people in residential aged care: a systematic review. Age and Ageing. 2021;50(1):81–87. doi:10.1093/ageing/afaa102
34. Nomura Y, Takei N, Ishii T, et al. Factors That Affect Oral Care Outcomes for Institutionalized Elderly. Int J Dent. 2018;2018:2478408. doi:10.1155/2018/2478408
35. Wei C, Cheng Z, Zhang L, Yang J. Microbiology and prognostic factors of hospital- and community-acquired aspiration pneumonia in respiratory intensive care unit. Am J Infect Control. 2013;41(10):880–884. doi:10.1016/j.ajic.2013.01.007
36. Meyer A, Buetti N, Houhou-Fidouh N, et al. HSV-1 reactivation is associated with an increased risk of mortality and pneumonia in critically ill COVID-19 patients. Crit Care. 2021;25(1):417. doi:10.1186/s13054-021-03843-8
37. Huang L, Zhang X, Pang L, et al. Viral reactivation in the lungs of patients with severe pneumonia is associated with increased mortality, a multicenter, retrospective study. J Med Virol. 2023;95(1):e28337. doi:10.1002/jmv.28337
38. Taylor JK, Fleming GB, Singanayagam A, Hill AT, Chalmers JD. Risk factors for aspiration in community-acquired pneumonia: analysis of a hospitalized UK cohort. Am J Med. 2013;126(11):995–1001. doi:10.1016/j.amjmed.2013.07.012
39. Meersseman W, Lagrou K, Spriet I, et al. Significance of the isolation of Candida species from airway samples in critically ill patients: a prospective, autopsy study. Intensive Care Med. 2009;35(9):1526–1531. doi:10.1007/s00134-009-1482-8
40. Bennett J, Doli In R, Blaser M. Candida species. In: Mandell D, editor. Principles and Practice of Infectious Diseases. Elsevier; 2020:3087–3102.
41. Moss BJ, Musher DM. Candida species in community-acquired pneumonia in patients with chronic aspiration. Pneumonia. 2021;13(1):12. doi:10.1186/s41479-021-00090-x
42. El-Solh AA, Pietrantoni C, Bhat A, et al. Microbiology of severe aspiration pneumonia in institutionalized elderly. Am J Respir Crit Care Med. 2003;167(12):1650–1654. doi:10.1164/rccm.200212-1543OC
43. Zhu L, Hao Y, Li W, Shi B, Dong H, Gao P. Significance of pleural effusion detected by metagenomic next-generation sequencing in the diagnosis of aspiration pneumonia. Front Cell Infect Microbiol. 2022;12:992352. doi:10.3389/fcimb.2022.992352
44. Almirall J, Boixeda R, de la Torre MC, Torres A. Aspiration pneumonia: a renewed perspective and practical approach. Respiratory Medicine. 2021;185:106485. doi:10.1016/j.rmed.2021.106485
45. Bowerman TJ, Zhang J, Waite LM. Antibacterial treatment of aspiration pneumonia in older people: a systematic review. Clin Interv Aging. 2018;13:2201–2213. doi:10.2147/CIA.S183344
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.