Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
MHR and CRP/Albumin Ratio Correlate with Wagner Grade in Diabetic Foot Ulcers: A Chinese Retrospective Study with Pathogen Analysis
Authors Song J, Liu T, Yu Y, Sun K, Zheng L
Received 17 March 2026
Accepted for publication 19 May 2026
Published 4 June 2026 Volume 2026:19 605013
DOI https://doi.org/10.2147/DMSO.S605013
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Juan Song,* Ting Liu,* Ying Yu, Ke Sun, Liu Zheng
Department of Clinical Laboratory, The 82nd Group Army Hospital of The Chinese People’s Liberation Army, Baoding, Hebei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Juan Song, Department of Clinical Laboratory, The 82nd Group Army Hospital of The Chinese People’s Liberation Army, Baoding, Hebei, People’s Republic of China, Email [email protected]
Background: Assessing the severity of diabetic foot ulcers (DFU) is critical for prognosis and treatment. While the Wagner classification is widely used, it lacks systemic inflammatory and nutritional assessment. Composite markers like the monocyte-to-high-density lipoprotein cholesterol ratio (MHR) and C-reactive protein-to-albumin ratio (CAR) may fill this gap. Furthermore, regional data on pathogen distribution in China are essential for guiding antibiotic therapy.
Aim: To investigate the correlation of MHR and CAR with Wagner grades in Chinese DFU patients, identify independent predictors for severity, and analyze pathogen distribution and drug resistance patterns across different grades.
Patients and Methods: A retrospective analysis was conducted on 136 DFU patients hospitalized from January 2022 to May 2024. Patients were categorized into three groups based on Wagner grades: Grade 1– 2 (n=17), Grade 3 (n=42), and Grade 4– 5 (n=77). Clinical data, MHR, and CAR were analyzed. Spearman correlation and ordinal logistic regression determined associations with severity. Receiver operating characteristic (ROC) curves evaluated the predictive value of MHR and CAR for severe infection (Wagner 4– 5). Pathogen profiles were analyzed per group.
Results: MHR (r=0.451, P< 0.001) and CAR (r=0.521, P< 0.001) were significantly and positively correlated with Wagner grades. Logistic regression identified serum albumin (OR=0.88, 95% CI: 0.82– 0.95, P=0.002) and HDL-C (OR=0.11, 95% CI: 0.02– 0.68, P=0.017) as independent protective factors against higher Wagner grades. For predicting severe infection, the optimal cut-off values were 0.775 for MHR (AUC=0.760) and 2.04 for CAR (AUC=0.777). Among 183 isolated strains, Staphylococcus aureus (24.59%) was predominant. Notably, as Wagner grades increased, the prevalence of Gram-negative bacteria (e.g. Escherichia coli, Pseudomonas aeruginosa) and mixed infections rose significantly (P< 0.01).
Conclusion: MHR and CAR are valuable biological markers for assessing DFU severity in the Chinese population. Albumin and HDL-C serve as independent protective factors. The study reveals a grade-dependent shift in pathogen spectra toward Gram-negative bacteria and mixed infections, providing region-specific evidence for optimizing empirical antibiotic strategies.
Keywords: diabetic foot ulcer, Wagner classification, monocyte to high-density lipoprotein cholesterol ratio, C-reactive protein to albumin ratio, pathogenic bacteria
Introduction
The rising prevalence of diabetes mellitus has made diabetic foot ulcer (DFU) a challenging complication worldwide.1 Characterized by prolonged healing, high recurrence, and significant disability and mortality rates, DFU imposes a heavy economic burden on healthcare systems and patients.2–4 Accurate severity assessment is paramount for formulating individualized treatment plans.
Currently, the Wagner classification system is the clinical standard for staging DFU based on ulcer depth and extent. A recent systematic review has confirmed that the Wagner scale demonstrates appropriate reliability for evaluating diabetic foot wounds, with weighted kappa values ranging from 0.41 to 0.55 for inter-observer agreement.5 However, this anatomical-based system has limitations: it fails to adequately reflect the patient’s systemic inflammatory status, metabolic derangements, and nutritional reserves, which are critical determinants of healing potential and amputation risk.
Recent research suggests that composite inflammatory markers may offer superior prognostic value. The monocyte‑to‑high‑density lipoprotein cholesterol ratio (MHR) reflects the balance between pro‑inflammatory monocytes and anti‑inflammatory HDL‑C, which exerts protective effects through anti‑inflammatory, antioxidant, and immunomodulatory functions6. Elevated MHR has been independently associated with type 2 diabetes and cardiovascular disease.7–9 Similarly, the C‑reactive protein‑to‑albumin ratio (CAR) integrates acute‑phase inflammation with nutritional status10 and has been validated as a strong predictor of early mortality.11 Although these markers are cost‑effective and accessible, their correlation with DFU severity-specifically within the Chinese population-remains understudied.
Furthermore, the complexity of wound infection directly impacts prognosis. Pathogen distribution and antibiotic resistance patterns in DFU vary significantly by geography.12 However, data describing how pathogenic flora evolve across different Wagner grades in Chinese patients are scarce. Understanding these regional characteristics is crucial for guiding empirical anti‑infective therapy.
Therefore, this study aims to: (1) analyze the correlation between MHR/CAR levels and Wagner grades in Chinese DFU patients; (2) evaluate their predictive value for severe infection; and (3) explore the distinct distribution and resistance profiles of pathogens across different grades. This study seeks to provide region-specific clinical evidence to optimize DFU assessment and treatment.
Patients and Methods
Study Design and Population
This retrospective study enrolled 136 patients with DFU hospitalized in the Department of Diabetic Foot at a tertiary care hospital from January 2022 to May 2024.
Inclusion Criteria
- Diagnosis of DFU according to the 2024 Chinese consensus on the diagnosis and treatment of diabetic foot ulcer complicated with lower extremity vasculopathy;13
- Positive wound bacterial cultures;
- Complete clinical and laboratory data.
Exclusion Criteria
- Ulcers of non-diabetic etiology;
- Concurrent infections at other sites (eg., pneumonia, urinary tract infection);
- Co-existing inflammatory conditions such as malignancies or autoimmune diseases.
Grouping
Patients were categorized into three groups based on the Wagner classification system:14
Wagner Grade 1–2 Group (n=17): Superficial or deep ulcers without abscess or osteomyelitis.
Wagner Grade 3 Group (n=42): Deep ulcers with abscess or osteomyelitis.
Wagner Grade 4–5 Group (n=77): Localized or whole-foot gangrene.
Data Collection
Clinical data (gender, age, diabetes duration) were retrieved from electronic medical records. Peripheral blood samples collected upon admission were analyzed for: white blood cell (WBC) count, monocytes, hemoglobin (Hb), albumin (ALB), C-reactive protein (CRP), and HDL-C.
Composite indicators were calculated as follows:


Microbiological Analysis
Deep wound secretions or tissue specimens were collected aseptically using sterile swabs after debridement. Specimens were immediately cultured on Columbia blood agar and China Blue plates (Autobio, Zhengzhou, China) at 35°C for 24–72 h. Identification and antimicrobial susceptibility testing (AST) were performed using the BD Phoenix™ M50 system. Results were interpreted according to CLSI 2025 standards.15 Anaerobic cultures were not performed due to the lack of anaerobic culture facilities in our laboratory.
Statistical Analysis
Data were analyzed using SPSS 22.0 (IBM Corp, Armonk, NY) and WHONET 5.6. Normal distribution was tested using the Shapiro–Wilk method. Continuous variables were presented as mean ± standard deviation ( ) or median (interquartile range, IQR). Group comparisons used one-way ANOVA or Kruskal–Wallis tests. Categorical data were compared using the χ2-test. Spearman rank correlation assessed relationships between serum markers and Wagner grades. Ordinal logistic regression identified independent factors associated with higher grades. ROC curves evaluated the predictive value of MHR and CAR for severe infection (Wagner 4–5); the reported cut-off values were derived from the original data without cross-validation, and external validation is warranted in future studies. A P-value < 0.05 was considered statistically significant. The small sample size in the Wagner grade 1–2 group (n=17) is acknowledged as a limitation, which may affect the statistical power of subgroup comparisons.
) or median (interquartile range, IQR). Group comparisons used one-way ANOVA or Kruskal–Wallis tests. Categorical data were compared using the χ2-test. Spearman rank correlation assessed relationships between serum markers and Wagner grades. Ordinal logistic regression identified independent factors associated with higher grades. ROC curves evaluated the predictive value of MHR and CAR for severe infection (Wagner 4–5); the reported cut-off values were derived from the original data without cross-validation, and external validation is warranted in future studies. A P-value < 0.05 was considered statistically significant. The small sample size in the Wagner grade 1–2 group (n=17) is acknowledged as a limitation, which may affect the statistical power of subgroup comparisons.
For the analysis of pathogen distribution, each isolate was counted individually to reflect the complete microbiological profile, which is standard practice in diabetic foot ulcer microbiology studies. We acknowledge that this approach may violate the assumption of statistical independence for some comparisons. Therefore, the results are presented primarily as descriptive data to guide clinical expectations, without formal statistical inference within patients.
Results
Clinical Characteristics and Serum Markers Demographic baselines (gender, age, diabetes duration) were comparable across groups (P > 0.05). However, disease severity markers differed significantly. The Wagner 4–5 group exhibited significantly higher WBC, monocytes, CRP, MHR, and CAR levels, and lower Hb, ALB, and HDL-C levels compared to Grade 1–2 and Grade 3 groups (P < 0.05) (Table 1).
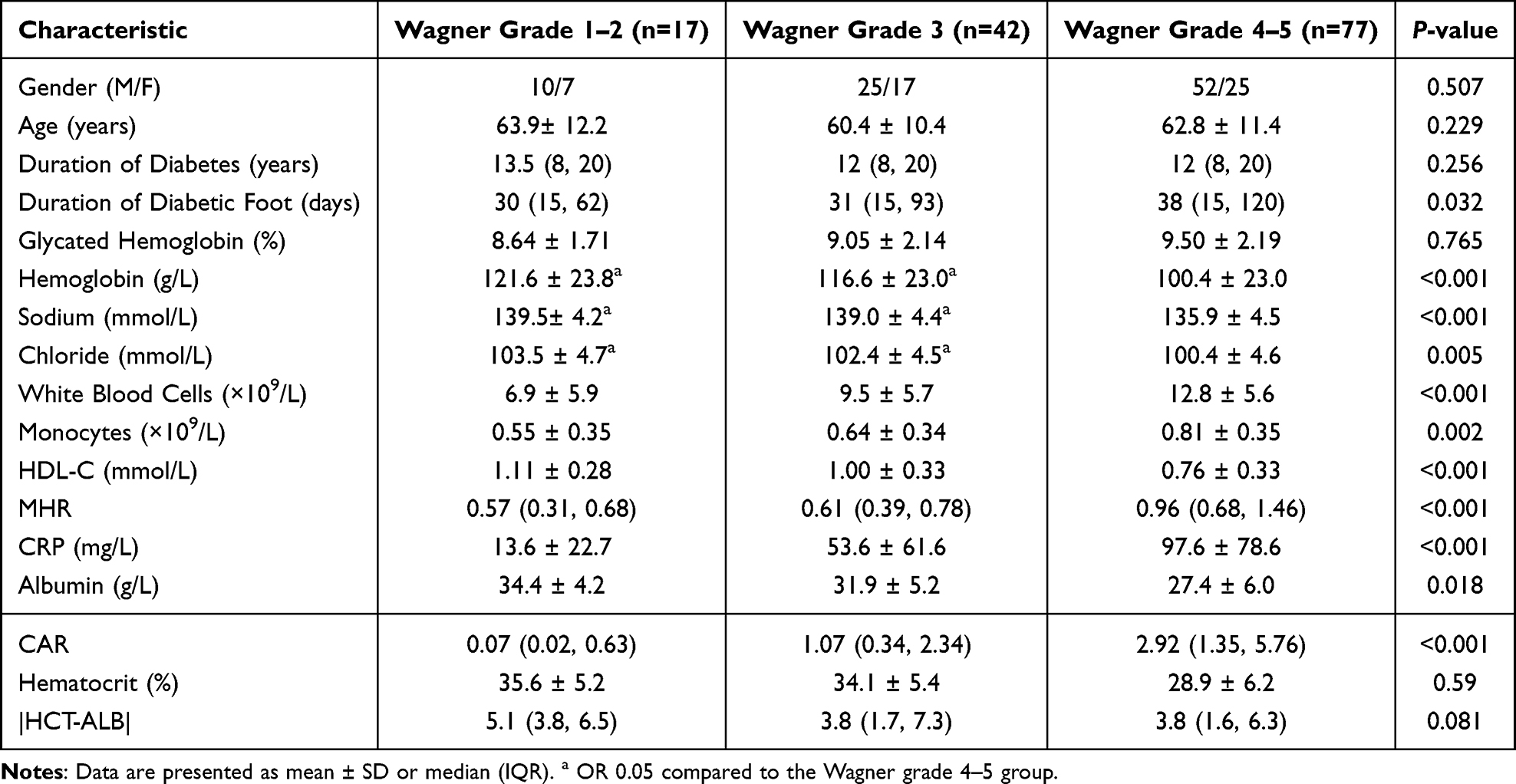 |
Table 1 Clinical Characteristics of DFU Patients by Wagner Grade |
Correlation Analysis
Spearman analysis revealed strong positive correlations between Wagner grade and inflammatory markers: CAR (r=0.521), CRP (r=0.491), MHR (r=0.451), and WBC (r=0.450) (all P < 0.001). Conversely, negative correlations were observed with ALB (r=−0.455) and HDL-C (r=−0.451) (Table 2).
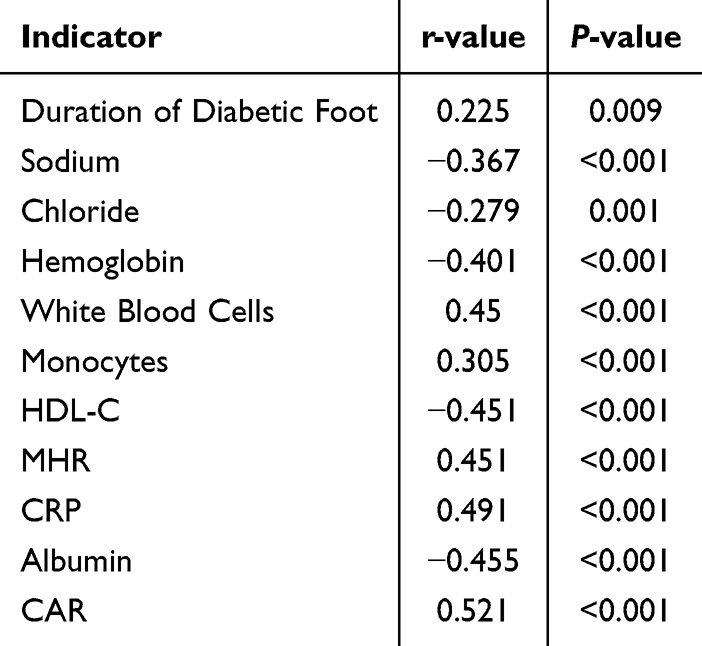 |
Table 2 Correlation Between Clinical Indicators and Wagner Grade (Spearman’s Rho) |
Independent Predictors of Severity
Ordinal logistic regression indicated that traditional inflammatory markers (WBC, CRP) and the composite ratios (MHR, CAR) were not independent predictors when adjusted for other variables. However, serum albumin (OR=0.88, 95% CI: 0.82–0.95, P=0.002) and HDL-C (OR=0.11, 95% CI: 0.02–0.68, P=0.017) emerged as independent protective factors. Specifically, a 1 mmol/L increase in HDL-C reduced the risk of a higher Wagner grade by approximately 89%.
Predictive Value for Severe Infection
For predicting severe infection (Wagner Grade 4–5), ROC analysis showed:
MHR: AUC = 0.760 (95% CI: 0.662–0.830), cut-off 0.775.
CAR: AUC = 0.777 (95% CI: 0.699–0.855), cut-off 2.04.
Both markers demonstrated moderate predictive accuracy (Figure 1).
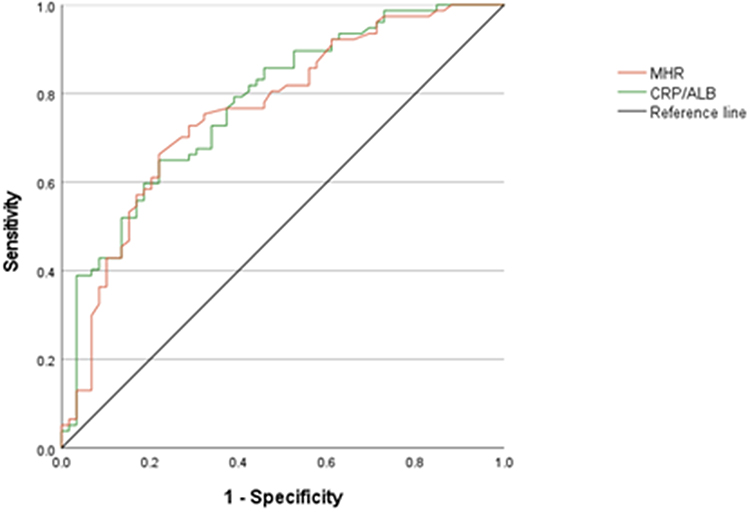 |
Figure 1 Receiver operating characteristic (ROC) curves of MHR and CAR for predicting severe diabetic foot infection (Wagner grade 4–5). The diagonal reference line (y = x) represents the performance of a random classifier (area under the curve [AUC] = 0.5); curves that lie above this line indicate better‑than‑random discriminative ability. The calculated AUC values were 0.760 for MHR and 0.777 for CAR, suggesting moderate predictive accuracy. |
Pathogen Distribution and Shift
There were no patients with grade 0 diabetic foot infection. The distribution of pathogens varied significantly across Wagner grades. The total number of isolates exceeded the number of patients, as multiple isolates were obtained from some individuals (Table 3). We isolated a total of 183 strains, with the predominant pathogens being Staphylococcus aureus (24.59%). As Wagner grades increased, the prevalence of Gram-negative bacteria (eg., Escherichia coli, Pseudomonas aeruginosa) and mixed infections rose significantly (P<0.01). No statistically significant differences were found among groups for other pathogens (P > 0.05) (Figure 2).
 |
Table 3 Distribution of Pathogen Types by Wagner Grade [n (%)] |
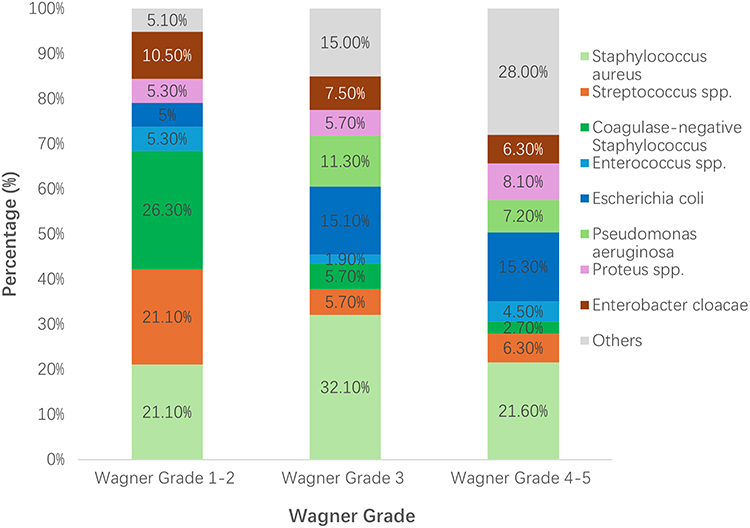 |
Figure 2 Composition of major bacterial species isolated from diabetic foot ulcers, stratified by Wagner grade (1–2, 3, and 4–5). The stacked bar chart shows the proportional distribution of each pathogen within each grade group. Pathogens that accounted for less than 5% of isolates in all groups are combined into the category “Others”. A clear shift from Gram‑positive bacteria (e.g., Staphylococcus aureus) toward Gram‑negative organisms (e.g., Escherichia coli, Pseudomonas aeruginosa) is observed as Wagner grade increases, together with a rise in mixed infections. |
Antibiotic Resistance Profiles
G+ Bacteria: S. aureus and coagulase-negative staphylococci showed 100% susceptibility to vancomycin, teicoplanin, and linezolid, but high resistance to penicillin and clindamycin. The MRSA detection rate was 24.44%, with no significant difference across Wagner grades (Supplementary Table S1).
G− Bacteria: E. coli and P. aeruginosa demonstrated high resistance to third-generation cephalosporins but remained highly sensitive to carbapenems (imipenem/meropenem) and amikacin (Supplementary Table S2).
Subgroup Analysis by Wagner Grade: When resistance profiles were analyzed according to DFU severity, no significant differences were observed in the resistance rates of S. aureus (Table 4) or E. coli (Table 5) across Wagner grade groups (P > 0.05 for all antibiotics tested). This suggests that while the distribution of pathogens shifts with increasing Wagner grade (as shown in Tables 3 and 6), the antibiotic resistance patterns of these key pathogens remain relatively stable across different stages of infection.
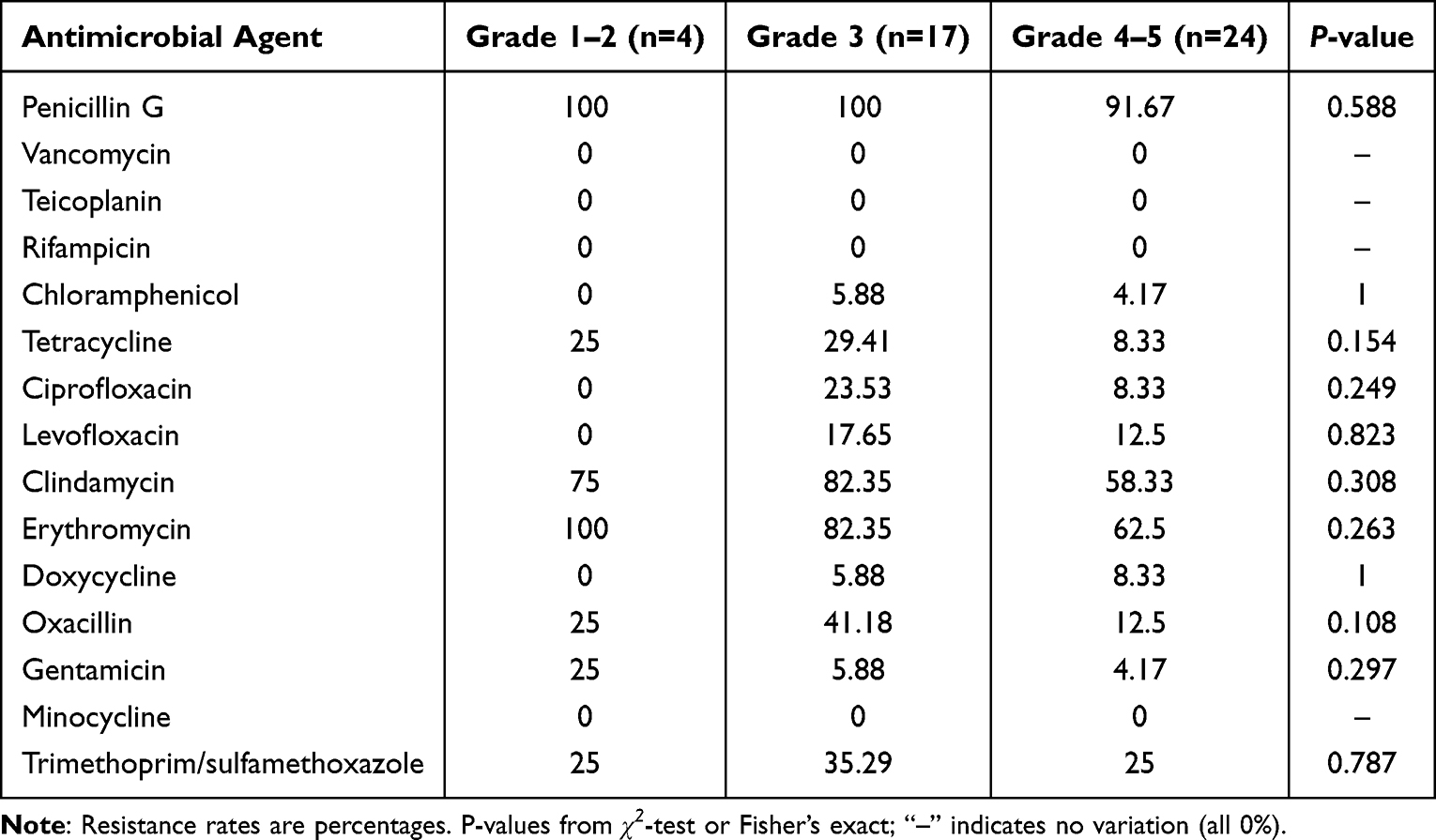 |
Table 4 Resistance Rates of S. aureus to Antimicrobial Agents by Wagner Grade (%) |
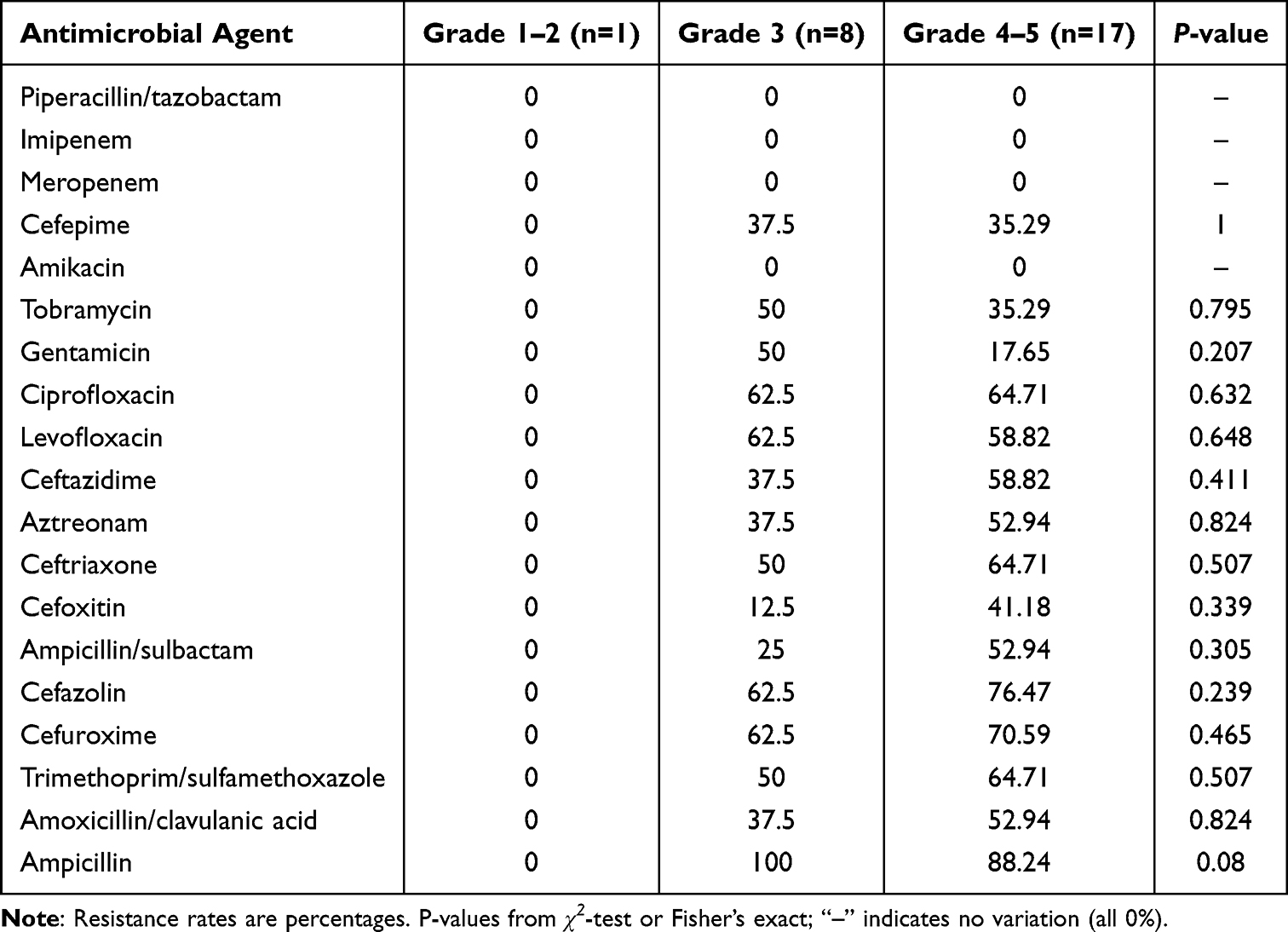 |
Table 5 Resistance Rates of E. coli to Antimicrobial Agents by Wagner Grade (%) |
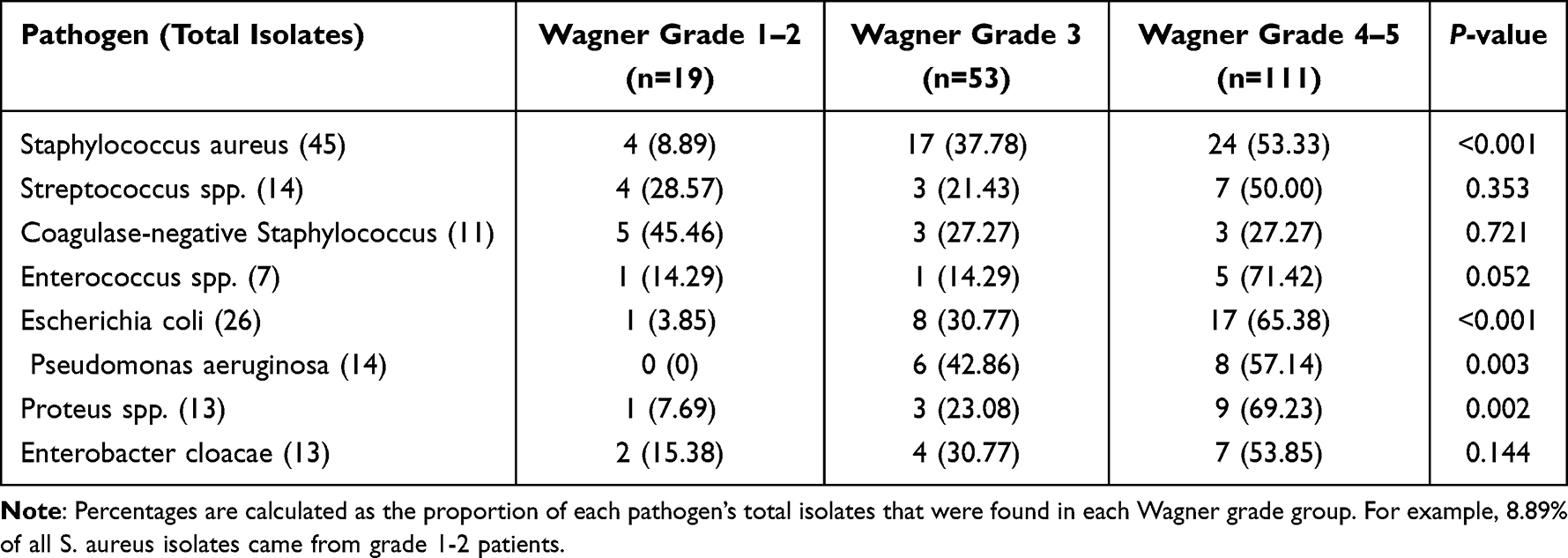 |
Table 6 Distribution of Major Pathogens by Wagner Grade [n (%)] |
Discussion
This study investigated the role of MHR and CAR in Chinese patients with diabetic foot ulcers (DFU) and found a significant positive correlation between these biomarkers and Wagner grades. However, in multivariate analysis, neither MHR nor CAR emerged as independent predictors. This finding reveals the complex relationship between inflammatory markers and the pathological process of DFU, suggesting that when assessing DFU severity, we should not rely on a single indicator but rather combine multiple clinical parameters for comprehensive evaluation.
Interpretation of MHR and CAR as Non‑independent Predictors
Although MHR and CAR were significantly correlated with Wagner grade in univariate analysis, they lost significance after adjustment for albumin and HDL‑C. This is likely due to the fact that both composite ratios are mathematically derived from their components (monocytes, HDL‑C, CRP, albumin). The strong protective effects of HDL‑C and albumin may overshadow the combined signal of the ratios. Additionally, the relatively small sample size, particularly in the lower Wagner grades, may have limited our power to detect an independent effect.5,14 Future studies with larger cohorts are needed to clarify whether MHR and CAR provide incremental value beyond their individual components.
Comparison of ROC Thresholds with Literature
The optimal cut‑off values for predicting severe infection (Wagner 4‑5) were 0.775 for MHR and 2.04 for CAR. To our knowledge, no prior study has reported MHR or CAR cut‑offs specifically for DFU severity in a Chinese population. Our MHR cut‑off is slightly higher than the threshold of 0.51 reported for identifying type 2 diabetes risk in a general population,9 which may reflect the greater inflammatory burden in DFU patients. The CAR cut‑off is comparable to the value of 2.29 reported by Keskinkılıç Yağız et al for predicting major amputation in DFU patients,16 supporting its clinical relevance. External validation of these thresholds is warranted.
Protective Roles of HDL‑C and Albumin
Furthermore, our study confirmed the independent protective roles of HDL‑C and albumin in DFU patients. HDL‑C not only has anti‑inflammatory and antioxidant effects but also modulates immune cell function, mitigating excessive inflammation caused by both Gram‑negative and Gram‑positive bacteria.6,17,18 Albumin reflects the patient’s nutritional status; hypoalbuminemia is associated with poor healing and worse prognosis in DFU.19 Therefore, clinical management should focus not only on local wound care but also on systemic nutritional support and lipid regulation to improve healing rates.
Pathogen Distribution and Clinical Implications
In terms of pathogen distribution, we found that the detection rate of Gram‑negative bacteria (eg., Escherichia coli, Pseudomonas aeruginosa) significantly increased with higher Wagner grades. This finding is consistent with previous studies20–22 and suggests regional differences in DFU pathogen profiles, highlighting the importance of tailoring antibiotic strategies according to disease severity. Moreover, mixed infections were common in severe DFU cases, indicating that empirical antibiotics targeting only Gram‑positive bacteria may be insufficient for high‑risk patients.12
Limitations
Several limitations should be acknowledged. This was a single‑center retrospective study with a relatively small sample size, especially in the Wagner grade 1‑2 group (n=17), which may introduce selection bias and limit statistical power.5,14 Causality cannot be inferred due to the cross‑sectional design. The Wagner classification, while widely used, does not fully capture vascular status or systemic health.5,14 Additionally, potential confounders such as glycemic control, ulcer duration, osteomyelitis, and renal function were not included in the regression model. Our ROC cut‑offs were derived without cross‑validation and require external validation in independent cohorts.
Conclusion and Future Directions
In summary, this study provides new insights into the clinical utility of MHR and CAR as adjunctive tools for DFU severity assessment, while highlighting the important protective roles of HDL‑C and albumin. Large‑scale, multicenter prospective studies are needed to externally validate our findings and to determine optimal antibiotic strategies targeting region‑specific pathogen spectra, thereby offering more precise guidance for the management of DFU patients.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethical Approval And Institutional Review Board Approval
The study was approved by the Medical Ethics Committee of the 82nd Group Army Hospital (Approval No. 2022064). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent To Participate
Informed consent was waived by the ethics committee due to the retrospective nature of the study.
Acknowledgments
This study was supported by the Baoding City Science and Technology Bureau (Grant No. 2241ZF386). The authors thank the staff of the Department of Clinical Laboratory and Department of Diabetic Foot at The 82nd Group Army Hospital of the Chinese People’s Liberation Army for their assistance in sample collection and clinical data management.
Author Contributions
Juan Song and Ting Liu contributed equally to this work and share first authorship.
Juan Song: Conceptualization, Methodology, Formal analysis, Writing-original draft, Writing -review & editing, Supervision, Project administration.
Ting Liu: Methodology, Investigation, Data curation, Formal analysis, Writing-review & editing.
Ying Yu: Investigation, Resources, Validation, Writing-review & editing.
Ke Sun: Investigation, Resources, Validation, Writing-review & editing.
Liu Zheng: Investigation, Data curation, Writing-review & editing.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by the Baoding City Science and Technology Bureau (Grant No. 2241ZF386).
Disclosure
The authors declare no conflict of interest.
References
1. International Diabetes Federation. IDF Diabetes Atlas.
2. Armstrong DG, Boulton AJM, Bus SA. Diabetic foot ulcers and their recurrence. N Engl J Med. 2017;376(24):2367–10. doi:10.1056/NEJMra1615439
3. Jiang Y, Wang X, Xia L, et al. A cohort study of diabetic patients and diabetic foot ulceration patients in China. Wound Repair Regen. 2015;23(2):222–230. doi:10.1111/wrr.12263
4. Zhang P, Lu J, Jing Y, Tang S, Zhu D, Bi Y. Global epidemiology of diabetic foot ulceration: a systematic review and meta-analysis. Ann Med. 2017;49(2):106–116. doi:10.1080/07853890.2016.1231932
5. Jalilian M, Shiri S. The reliability of the Wagner scale for evaluation the diabetic wounds: a literature review. Diabetes Metab Syndr Clin Res Rev. 2022;16(1):102369. doi:10.1016/j.dsx.2021.102369
6. Bonacina F, Pirillo A, Catapano AL, Norata GD. HDL in immune-inflammatory responses: implications beyond cardiovascular diseases. Cells. 2021;10(5):1061. doi:10.3390/cells10051061
7. Zhang H, Lu J, Gao J, et al. Association of monocyte‐to‐hdl cholesterol ratio with endothelial dysfunction in patients with type 2 diabetes. J Diabetes Res. 2024;2024(1):5287580. doi:10.1155/2024/5287580
8. Arabi A, Abdelhamid A, Nasrallah D, et al. Monocyte-to-HDL ratio (MHR) as a novel biomarker: reference ranges and associations with inflammatory diseases and disease-specific mortality. Lipids Health Dis. 2025;24(1):343. doi:10.1186/s12944-025-02755-8
9. Yu H, Yang C, Lv J, Zhao Y, Wang G, Wang X. The association between monocyte-to-high-density lipoprotein cholesterol ratio and type 2 diabetes mellitus: a cross-sectional study. Front Med. 2025;12:1521342. doi:10.3389/fmed.2025.1521342
10. Eckart A, Struja T, Kutz A, et al. Relationship of nutritional status, inflammation, and serum albumin levels during acute illness: a prospective study. Am J Med. 2020;133(6):713–722.e7. doi:10.1016/j.amjmed.2019.10.031
11. Capurso C, Lo Buglio A, Bellanti F, Serviddio G. C-reactive protein/albumin ratio vs. prognostic nutritional index as the best predictor of early mortality in hospitalized older patients, regardless of admitting diagnosis. Nutrients. 2025;17(17):2907. doi:10.3390/nu17172907
12. Lee J, Mashayamombe M, Walsh TP, et al. The bacteriology of diabetic foot ulcers and infections and incidence of Staphylococcus aureus small colony variants. J Med Microbiol. 2023;72(6). doi:10.1099/jmm.0.001716
13. Wang K, Wang Y, Shi W, et al. Diagnosis and treatment of diabetic foot ulcer complicated with lower extremity vasculopathy: consensus recommendation from the Chinese Medical Association (CMA), Chinese Medical Doctor Association (CMDA). Diabetes Metab Res Rev. 2024;40(3):e3776. doi:10.1002/dmrr.3776
14. Wagner FW. The dysvascular foot: a system for diagnosis and treatment. Foot Ankle. 1981;2(2):64–122. doi:10.1177/107110078100200202
15. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing.
16. Yağız B K, Keskin Y, Demirkan NA, Öa Ç. Prognostic role of HALP score, CRP/albumin ratio and CALLY index in diabetic foot ulcer-related major amputations. Langenbecks Arch Surg. 2025;410(1):314. doi:10.1007/s00423-025-03884-5
17. De Tymowski C, Stern J, Zappella N, et al. Impact of the type of bacteria on high-density lipoprotein cholesterol level during sepsis. Sci Rep. 2025;15(1):33556. doi:10.1038/s41598-025-18473-1
18. Brunham LR. The role of high-density lipoproteins in sepsis. J Lipid Res. 2025;66(1):100728. doi:10.1016/j.jlr.2024.100728
19. Xu S, Wang Y, Hu Z, Ma L, Zhang F, Liu P. Effects of neutrophil‐to‐lymphocyte ratio, serum calcium, and serum albumin on prognosis in patients with diabetic foot. Int Wound J. 2023;20(5):1638–1646. doi:10.1111/iwj.14019
20. Sultana R, Ahmed I, Saima S, Salam MT, Sultana S. Diabetic foot ulcer-a systematic review on relevant microbial etiology and antibiotic resistance in Asian countries. Diabetes Metab Syndr Clin Res Rev. 2023;17(6):102783. doi:10.1016/j.dsx.2023.102783
21. Du F, Ma J, Gong H, et al. Microbial infection and antibiotic susceptibility of diabetic foot ulcer in china: literature review. Front Endocrinol. 2022;13:881659. doi:10.3389/fendo.2022.881659
22. Liu Q, Lu W, Zhou S, Chen X, Sun P. A U shaped association between the HCT-ALB and hospital mortality in patients with sepsis. Sci Rep. 2025;15(1):14785. doi:10.1038/s41598-025-99459-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Distribution and Drug Resistance of Pathogenic Bacteria and Prognosis in Patients with Septicemia Bloodstream Infection with Renal Insufficiency
Pan D, Peng P, Fang Y, Lu J, Fang M
Infection and Drug Resistance 2022, 15:4109-4116
Published Date: 28 July 2022
Diabetic Foot Ulcers: Surgical Characteristics, Treatment Modalities and Short-Term Treatment Outcomes at a Tertiary Hospital in South-Western Uganda
Sikhondze MM, Twesigye D, Odongo CN, Mutiibwa D, Tayebwa E, Tibaijuka L, Ayana SD, Cabrera Dreque C
Open Access Surgery 2022, 15:75-87
Published Date: 3 November 2022
Distribution of Pathogenic Bacteria in Health Care Associated Sepsis in Preterm Infants and Ten Years Variation in Their Drug Resistance
Ni SW, Wang L, Wang Y, Shen JL
Infection and Drug Resistance 2025, 18:5067-5077
Published Date: 23 September 2025