")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Metformin Reduces the Risk of Total Hip Arthroplasty in Elderly Patients with Hip Osteoarthritis and Type 2 Diabetes Mellitus
Authors Li F
Received 16 June 2023
Accepted for publication 7 September 2023
Published 2 November 2023 Volume 2023:16 Pages 3481—3487
DOI https://doi.org/10.2147/DMSO.S419830
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Fuchun Li
Fourth Department of Orthopedics, The First Affiliated Hospital of Harbin Medical University, Harbin, 150001, People’s Republic of China
Correspondence: Fuchun Li, Fourth Department of Orthopedics, The First Affiliated Hospital of Harbin Medical University, 23 Youzheng Str, Nangang District, Harbin, 150001, People’s Republic of China, Email [email protected]
Purpose: To assess if metformin could reduce the risk of total hip arthroplasty (THA) in elderly patients with hip osteoarthritis and type 2 diabetes (T2DM).
Patients and Methods: It is a retrospective study among elderly patients (≥ 65 years) with hip osteoarthritis and T2DM. All included patients were divided into metformin group and non-metformin group, then propensity-score match (PSM) was performed to control potential confounding factors. The primary endpoint was the incidence of the first THA during the study period. Multivariate Cox regression analysis was employed to evaluate the association of metformin with the risk of THA.
Results: A matched cohort of 716 patients were finally included, with 308 metformin users and 308 metformin non-users. During a maximum follow-up of 10 years, the incidence of THA in metformin users was significantly lower than that in non-users (4.9% vs 25.0%, P< 0.01). Multivariate Cox regression analysis indicated that metformin users were significantly associated with a lower risk of THA compared with non-users (HR = 0.17, 95% CI: 0.10– 0.30; P< 0.01). In addition, further analyses indicated that participants with long-term metformin use (HR = 0.10, 95% CI: 0.02– 0.46; P< 0.01) or high metformin dosage (HR = 0.15, 95% CI: 0.04– 0.57; P< 0.01) had a lower risk of THA.
Conclusion: Metformin use could reduce the risk of THA in patients with hip osteoarthritis and T2DM, and the effect is accumulative and dose dependent.
Keywords: hip osteoarthritis, total hip arthroplasty, type 2 diabetes, metformin
Introduction
Hip osteoarthritis is one of the most common joint diseases in elderly people.1,2 Its incidence experienced a significant increase from 0.74 million in 2009 to 1.58 million in 2019, bringing about a substantial health and economic burden.3 It is a leading cause of pain and disability that may progress to the point where total hip arthroplasty (THA) is unavoidable.4
Diabetes mellitus has been reported to be independently associated with an increased risk of osteoarthritis.5 A US study in adults ranging from 18 to 64 years indicated that the incidence of arthritis in patients with diabetes was higher than those without diabetes (52% vs 27%).6 Metformin is the first-line therapy for the management of blood glucose in patients with type 2 diabetes mellitus (T2DM). As metformin also causes weight loss and has anti-inflammatory and chondroprotective effects, it has the potential to slow the progression of osteoarthritis. The potential shielding effect of metformin on the worsening of knee osteoarthritis has been reported in several studies, which revealed that regular metformin users had 19–74% lower hazards of total knee arthroplasty (TKA).7,8 However, the effect of metformin on hip osteoarthritis is rarely reported. Currently, only a subgroup analysis from a recent study reported by Zhu et al9 was found, reporting an association between regular use of metformin and about a 29% reduced likelihood of needing total hip arthroplasty (THA), but the association was not statistically significant.
The present study aims to determine if metformin could reduce the risk of THA in elderly patients with hip osteoarthritis and T2DM.
Materials and Methods
Patients
It is a retrospective study. Medical records from elderly patients (≥65 years) who hospitalized at the Department of Orthopedics, First Affiliated Hospital of Harbin Medical University, China, from January 2012 to December 2021 were reviewed. Inclusion criteria include 1) discharge diagnosis of hip osteoarthritis, hip osteoarthropathy or degenerative joint disease of the hip, and 2) T2DM. Hip osteoarthritis was defined as a symptomatic hip joint that had patients’ complaints of hip pain and had radiological evidence of osteoarthritis (ie, joint space narrowing, sclerotic changes of the subchondral bone, osteophyte formation, or a bone cyst). Exclusion criteria include 1) inflammatory arthritis such as rheumatoid arthritis, psoriatic arthritis, and gout, 2) systemic lupus erythematosus (SLE), and 3) history of injury or surgery around the hip joint.
Study Design
All patients who met inclusion and exclusion criteria were divided into metformin group and non-metformin group. Participants were classified into metformin group if they had medical history of metformin use for more than 6 months. Patients who never took metformin were classified into non-metformin group. Additionally, the durations of metformin use were classified as short-term or long-term metformin use according to the median duration (1650 days). To examine the potential dose–response relationship between metformin use and risk of THA, we categorized participants into two groups based on daily dosage of metformin (low dose with <1.0 g and high dose with ≥1.0 g).
Data Collection
Patients’ first visit during the study period was regarded as the index date, and they were followed up until admission for THA surgeries by medical records review or by telephone interview.
The primary outcome was the incidence of THA. Covariates included demographics, comorbidities, hip pain, medications for pain management, and other antihyperglycemic therapies. Hip pain was assessed using the numeric rating scale (NRS) ranging from 0 to 10. The degree of hip pain was collected from the medical records, which was only evaluated in the resting state, with 0 representing no pain and 10 representing the most intensive pain.
Statistical Analysis
Propensity-score matching (PSM) was employed to reduce confounding biases. We calculated the propensity score (probability) of metformin use by logistic regression with age, gender, BMI, comorbidities, pain medications, other antihyperglycemic agents at baseline as predictors. Then, we matched each metformin nonuser 1:1 to a participant who did use metformin with a similar propensity score using the nearest neighbor greedy algorithm with the caliper of 0.01.
The Kaplan–Meier survival analyses were used to estimate the time from the index date to the first THA, and the Log rank test was used to compare the differences in survival free of THA between two groups. The Cox proportional-hazards model was used for multivariate analysis. Potential factors associated with THA in previous publications or in our clinical experience were included in the initial model. Variables were removed from the model by a backward selection procedure if alpha >0.05. We also used a time-dependent Cox model to explore the effects of time-varying exposure of metformin after adjustment for the time-dependent covariates.
Results
Patients’ Characteristics
The flowchart of study population selection is shown in Figure 1. From 2012 to 2021, a total of 1057 patients hospitalized with hip osteoarthritis and diabetes were recorded. After excluding 159 patients, the remaining 898 patients included 491 metformin users and 407 non-users. Finally, a matched cohort of 764 patients was included, with 308 metformin users and 308 metformin non-users.
 |
Figure 1 The flowchart of study population selection. |
Table 1 shows the descriptive statistics of patients in both groups before and after PSM. Before PSM, differences in age, BMI, obesity, opioids, and insulin were statistically significant between two groups (all P<0.05). After PSM, there was no significant difference in all baseline characteristics between the two groups (all P>0.05).
 |
Table 1 Patients’ Baseline Characteristics Between Metformin Users and Non-Metformin Users |
During a maximum follow-up period of 120 months (median 52 months), the hip pain was significantly improved in the metformin group compared with non-metformin group (1.6 ± 0.5 vs 2.2 ± 0.8; P<0.01), and the cumulative incidence of THA in metformin users was significantly lower than that in the metformin non-users (4.9% vs 25.0%, P<0.01). As shown in Figure 2, the Kaplan–Meier survival curve indicated a lower risk of THA in the metformin group (HR = 0.23, 95% CI: 0.15–0.34; P<0.01).
 |
Figure 2 Kaplan–Meier curve illustrating the pattern of survival free of total Hip arthroplasty (THA) by metformin using status. |
Multivariate Cox regression analysis (Table 2) showed that after adjusting for potential confounding factors, metformin users were significantly associated with a lower risk of THA compared non-users (HR = 0.17, 95% CI: 0.10–0.30; P<0.01). The time-dependent Cox model generated a similar result (HR = 0.12, 95% CI: 0.06–0.22; P<0.01). In addition, subgroup analyses indicated that long-term metformin use (HR = 0.10, 95% CI: 0.02–0.46; P<0.01) and high metformin dosage (HR = 0.15, 95% CI: 0.04–0.57; P<0.01) were significantly associated with lower risks of THA (Table 3).
 |
Table 2 Association of Metformin Use with the Risk of Total Hip Arthroplasty |
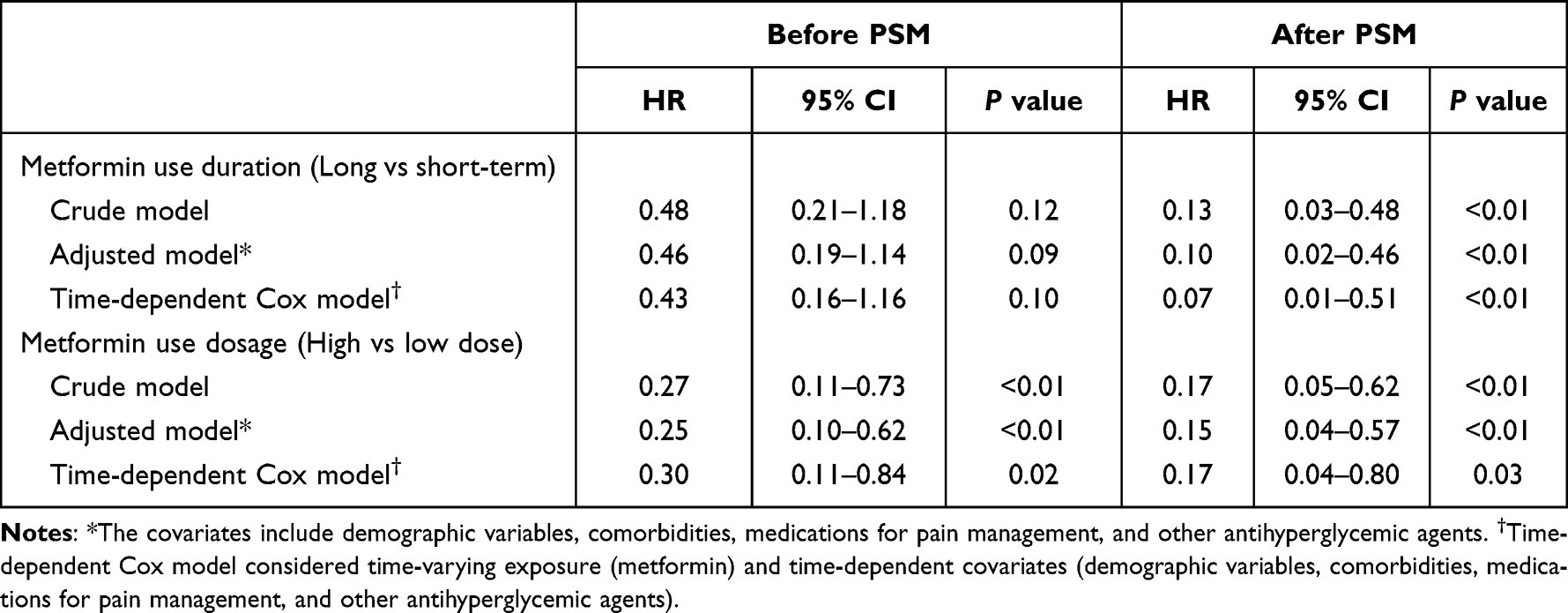 |
Table 3 Association of Metformin Use Duration and Dosage with the Risk of Total hip Arthroplasty |
Discussion
This retrospective study investigated the association of metformin use with the risk of THA in elderly patients with hip osteoarthritis and T2DM. Metformin users were found to have a significantly lower incidence of THA. Moreover, multivariate Cox regression indicated that metformin use was substantially associated with a lower risk of THA after controlling for potential confounders. Subgroup analyses showed that increased duration and dosage of metformin use were significantly associated with reduced risks of THA, suggesting a potential accumulative and dose-dependent effect.
A few metabolic processes that regulate cartilage growth and nutrition were reported to influence cartilage health, and if altered, it can lead to cartilage degradation.10 Some studies have focused on scavenging excessive reactive oxygen species (ROS) to alleviate oxidative stress in OA pathogenesis, such as using nanozymes as natural antioxidant enzyme equivalents.11–14 An increasing number of investigators have postulated that diabetes induces the progression of osteoarthritis by chronic hyperglycemia, insulin resistance and excess reactive oxygen species.15,16 Metformin has been reported to reduce the risk of total joint replacement through reducing inflammation, improving insulin sensitivity, and inhibiting ROS production.9,17,18
The association of metformin use and the risk of TKA has been widely explored. In a recently published cohort study, metformin use was reported to be significantly associated with a reduced risk of TKA over 14-year follow-up (prevalence ratio: 0.26, 95% CI: 0.15 to 0.45, P< 0.001).9 In addition, a large retrospective cohort with 93,330 patients and a 4-year follow-up indicated that regular metformin users had a 19% lower risk of TKA than non-users.19 However, studies reporting the association of metformin use with the risk of THA were limited. In a recently published study,9 metformin use in patients with type 2 diabetes mellitus was associated with a significantly reduced risk of total joint replacement including THA and TKA (HR = 0.75, 95% CI: 0.62–0.89), but in the subgroup analysis, the association of metformin use and the incidence of THA was not significant (HR = 0.71, 95% CI: 0.44–1.13). In contrast, our study found a significantly negative association between metformin use and THA incidence, and the effect of metformin on the lower risk of THA is accumulative and dose dependent.
The current study has several limitations. First, lifestyle and sociodemographic variables, which might be potential confounding factors, were not available in the dataset and may lead to bias. In addition, as included patients were diagnosis with both hip osteoarthritis and T2DM, further studies are needed to generalize our findings to all hip osteoarthritis patients.
Conclusions
In conclusion, metformin use was significantly associated with a reduced risk of THA in participants with hip osteoarthritis and T2DM. Moreover, there are accumulative and dose-dependent effects of metformin use with the reduced risk of THA.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of The First Affiliated Hospital of Harbin Medical University (approval no. 2020054). All procedures were conducted according to the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Informed consent was waived by the Ethic Committee of The First Affiliated Hospital of Harbin Medical University because of the retrospective nature of the study. Patient participation was anonymous, whose names or identifying information were not collected.
Funding
There is no funding to report.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Zhu Z, Li J, Ruan G, Wang G, Huang C, Ding C. Investigational drugs for the treatment of osteoarthritis, an update on recent developments. Expert Opin Investig Drugs. 2018;27(11):881–900. doi:10.1080/13543784.2018.1539075
2. Dell’Isola A, Allan R, Smith SL, Marreiros SS, Steultjens M. Identification of clinical phenotypes in knee osteoarthritis: a systematic review of the literature. BMC Musculoskelet Disord. 2016;17(1):425. doi:10.1186/s12891-016-1286-2
3. Fu M, Zhou H, Li Y, Jin H, Liu X. Global, regional, and national burdens of Hip osteoarthritis from 1990 to 2019: estimates from the 2019 Global Burden of Disease Study. Arthritis Res Ther. 2022;24(1):8. doi:10.1186/s13075-021-02705-6
4. Evans JT, Walker RW, Evans JP, Blom AW, Sayers A, Whitehouse MR. How long does a knee replacement last? A systematic review and meta-analysis of case series and national registry reports with more than 15 years of follow-up. Lancet. 2019;393(10172):655–663. doi:10.1016/S0140-6736(18)32531-5
5. Louati K, Vidal C, Berenbaum F, Sellam J. Association between diabetes mellitus and osteoarthritis: systematic literature review and meta-analysis. RMD Open. 2015;1(1):e000077. doi:10.1136/rmdopen-2015-000077
6. Centers for Disease C, Prevention. Arthritis as a potential barrier to physical activity among adults with diabetes--United States, 2005 and 2007. MMWR Morb Mortal Wkly Rep. 2008;57(18):486–489.
7. Chen S, Ruan G, Zeng M, et al. Association between metformin use and risk of total knee arthroplasty and degree of knee pain in knee osteoarthritis patients with diabetes and/or obesity: a retrospective study. J Clin Med. 2022;11(16):4796.
8. Lai FTT, Yip BHK, Hunter DJ, et al. Metformin use and the risk of total knee replacement among diabetic patients: a propensity-score-matched retrospective cohort study. Sci Rep. 2022;12(1):11571. doi:10.1038/s41598-022-15871-7
9. Zhu Z, Huang JY, Ruan G, et al. Metformin use and associated risk of total joint replacement in patients with type 2 diabetes: a population-based matched cohort study. CMAJ. 2022;194(49):E1672–E1684. doi:10.1503/cmaj.220952
10. Piva SR, Susko AM, Khoja SS, Josbeno DA, Fitzgerald GK, Toledo FG. Links between osteoarthritis and diabetes: implications for management from a physical activity perspective. Clin Geriatr Med. 2015;31(1):67–87, viii. doi:10.1016/j.cger.2014.08.019
11. Zhang C, Chen S, Li Q, et al. Ultrasound-Targeted Microbubble Destruction Mediates Gene Transfection for Beta-Cell Regeneration and Glucose Regulation. Small. 2021;17(31):e2008177. doi:10.1002/smll.202008177
12. Xie F, Li R, Shu W, Zhao L, Wan J. Self-assembly of Peptide dendrimers and their bio-applications in theranostics. Mater Today Bio. 2022;14:100239. doi:10.1016/j.mtbio.2022.100239
13. Liu S, Xu J, Xing Y, et al. Nanozymes as efficient tools for catalytic therapeutics. View. 2021;3(2):20200147. doi:10.1002/VIW.20200147
14. Zhong D, Du Z, Zhou M. Algae: a natural active material for biomedical applications. VIEW. 2021;2(4):20200189. doi:10.1002/VIW.20200189
15. Courties A, Sellam J. Osteoarthritis and type 2 diabetes mellitus: what are the links? Diabetes Res Clin Pract. 2016;122:198–206. doi:10.1016/j.diabres.2016.10.021
16. Veronese N, Cooper C, Reginster JY, et al. Type 2 diabetes mellitus and osteoarthritis. Semin Arthritis Rheum. 2019;49(1):9–19. doi:10.1016/j.semarthrit.2019.01.005
17. Park MJ, Moon SJ, Baek JA, et al. Metformin augments anti-inflammatory and chondroprotective properties of mesenchymal stem cells in experimental osteoarthritis. J Immunol. 2019;203(1):127–136. doi:10.4049/jimmunol.1800006
18. Bandow K, Kusuyama J, Kakimoto K, Ohnishi T, Matsuguchi T. AMP-activated protein kinase (AMPK) activity negatively regulates chondrogenic differentiation. Bone. 2015;74:125–133. doi:10.1016/j.bone.2014.12.001
19. Kuusalo L, Felson DT, Wang N, et al. Metabolic osteoarthritis - relation of diabetes and cardiovascular disease with knee osteoarthritis. Osteoarthritis Cartilage. 2021;29(2):230–234. doi:10.1016/j.joca.2020.09.010
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.