Back to Journals » Psychology Research and Behavior Management » Volume 18
Metacognitions in Young and Middle-Aged Patients with Acute Myocardial Infarction: A Psychometric Study of the Metacognitions Questionnaire-30
Authors Liu Z, Wang P ![]() , Wang Y, He W, Qin Y, Wang L, Zhang Q
, Wang Y, He W, Qin Y, Wang L, Zhang Q ![]() , Yang R, Sun C
, Yang R, Sun C
Received 13 July 2025
Accepted for publication 22 September 2025
Published 2 October 2025 Volume 2025:18 Pages 2107—2120
DOI https://doi.org/10.2147/PRBM.S553537
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Bao-Liang Zhong
Zizheng Liu,1,* Panpan Wang,1,2,* Yiwen Wang,3 Wenqian He,4 Ying Qin,1 Lianke Wang,1 Qiang Zhang,1 Ruiyi Yang,1 Changqing Sun1,2
1School of Nursing and Health, Zhengzhou University, Zhengzhou, Henan, 450001, People’s Republic of China; 2College of Public Health, Zhengzhou University, Zhengzhou, Henan, 450001, People’s Republic of China; 3The Affiliated Cancer Hospital of Zhengzhou University & Henan Cancer Hospital, Zhengzhou, Henan, 450008, People’s Republic of China; 4School of Public Health, Department of Environmental Health Sciences, University of Alabama at Birmingham, Birmingham, AL, 35487, USA
*These authors contributed equally to this work
Correspondence: Changqing Sun, Email [email protected]
Objective: The study aimed to conduct a psychometric validation of the Chinese version of the Metacognitions Questionnaire-30 (MCQ-30) and to explore the association between metacognitive factors and post-traumatic growth (PTG).
Methods: 313 young and middle-aged patients with acute myocardial infarction (AMI) were recruited between October 2023 and June 2024 from a tertiary hospital in Zhengzhou, China. Confirmatory factor analysis (CFA) was used to test established factor structures of the MCQ-30. The reliability tests, criterion-related validity analyses, and regression models were conducted.
Results: CFA results supported the five-factor structure of the MCQ-30, with satisfactory model fit and good reliability. Criterion-related validity was also supported by significant positive correlations between the five factors and depression/anxiety symptoms. All five metacognition factors were also significantly correlated with PTG.
Conclusion: The findings support the use of the Chinese version of the MCQ-30 as a potentially reliable and valid instrument for assessing metacognitive beliefs in young and middle-aged AMI patients. Given the sampling method and cross-sectional design, results should be interpreted cautiously. Further research with larger sample sizes, and longitudinal design is needed to validate the above results.
Keywords: myocardial infarction, metacognition, post-traumatic growth, anxiety, depression, psychometrics
Introduction
Acute myocardial infarction (AMI), characterized by rapid progression and a high pre-hospital mortality rate, is the leading cause of premature deaths globally.1,2 Many studies have reported a high incidence of psychological disorders such as anxiety and depression among the patients with AMI.3,4 In recent years, the morbidity of AMI has risen in the young and middle-aged population,5–7 who are more likely to experience anxiety and depression owing to special social roles. Anxiety and depression are linked to a higher risk of future cardiac events, lower quality of life, and increased healthcare costs.8 Therefore, it is important to develop effective intervention methods to reduce anxiety and depression in young and middle-aged patients with AMI.
Metacognition refers to an individual’s conscious effort to appraise and regulate their own cognitive processes,9,10 and is characterized by the close relationship between experiences, thoughts, beliefs, and emotions.11 Based on the Self-Regulatory Executive Function (S-REF) model, dysfunctional metacognition contributes to the development of various psychological disorders such as anxiety disorders, depressive disorders, paranoia, and obsessive-compulsive disorder,12 through the mechanism of the cognitive attentional syndrome (CAS).13 The CAS refers to a cognitive state in which negative self-relevant information is prioritized, leading to its persistent and repetitive processing, such as rumination and worry.14 However, the development of positive psychology has led to a progressive extension of the concept of metacognition. The post-traumatic growth (PTG) model developed by Tedeschi and Calhoun15 highlights the crucial role of cognitive processing in fostering an individual’s growth following trauma, especially rumination. This perspective closely aligns with the views of the S-REF model, suggesting that functional metacognition may facilitate PTG by regulating patients’ cognitive processing, guiding them toward positive cognitive appraisal of traumatic events.16 Such patterns can help patients perceive their illness as an opportunity for growth and prevent them from falling into vicious cycles of worry and ineffective coping strategies.17,18 Therefore, metacognition can effectively reflect an individual’s psychological attributes and may serve as a potential target for psychological intervention.
There are already established tools to measure an individual’s salient types of metacognition.19 The 65-item Metacognition Questionnaire (MCQ) based on the S-REF model was first developed by Cartwright-Hatton and Wells in 1997.20 It measures five dimensions, including: positive beliefs about worry (POS), negative beliefs about uncontrollability and danger (NEG), cognitive confidence (CC), beliefs about the need to control thoughts (NC), and cognitive self-consciousness (CSC). Although the reliability and validity of the questionnaire have already been proved, Wells and Cartwright-Hatton21 shortened the questionnaire to a 30-item version for the promotion and clinical application. Up to now, this version has shown stable factor structure and good reliability and validity across multiple samples, such as cancer patients, Parkinson’s patients, cardiac patients, and university student population.22–26 It has also been translated into various languages, including Spanish, French, Korean, Turkish, and Chinese.27–31 At present, the original five-factor model has been shown to be acceptable according to findings of the confirmatory factor analysis (CFA) for MCQ-30 in most adults.25,31,32 However, the reliability and validity of the Chinese version have not been tested in chronic disease populations, including patients with AMI. In addition, many studies, considering the potential cultural difference, researchers conduct cross-loadings or add item error covariances to achieve a better fit.31
To reduce the CAS and modify metacognition, Wells first developed the metacognitive therapy (MCT) based on the S-REF model.33 Systematic reviews and meta-analyses provided robust evidence for the efficacy of the MCT in the cardiovascular disease patients.4,34 But fewer studies have examined the feasibility and efficacy of MCT in the Chinese AMI patients, which could be attributed to the lack of suitable and valid measures of metacognitions in this context. Therefore, to facilitate the development of future MCT, we aim to explore the structure, validity, and reliability of the five-factor model of the MCQ-30 and expect it to be replicated and utilized in the Chinese cardiac rehabilitation population, especially among young and middle-aged patients with AMI.
Given previous studies, metacognition assessed by the MCQ-30 is positively correlated with depressive and anxiety symptoms.35,36 This study hypothesizes a positive association between metacognitions and anxiety as well as depression, and a negative correlation between dimensions of the MCQ-30 and PTG among Chinese AMI patients.
Methods
Participants and Procedure
We consecutively recruited 320 patients with AMI from the cardiovascular medicine departments of a tertiary hospital in China, between October 2023 and June 2024. Convenience sampling was used to include eligible participants who met the following criteria in this study. Inclusion criteria: (1) diagnosed with AMI; (2) aged between 18 and 60 years old. Exclusion criteria: (1) accompanied by severe complications such as acute pulmonary edema, severe arrhythmias, and cardiogenic shock; (2) diagnosed with dementia or other psychiatric diseases; (3) having hearing or communication impairment; (4) currently participating in other psychological therapies or interventions.
All participants carefully signed the informed consent forms and then filled out the questionnaires. Subsequently, the questionnaires were reviewed with any missing responses promptly corrected. Participants with more than half of the answers the same on the questionnaire (n = 7) were excluded. Ultimately, 313 patients were included in the study, with a valid response rate of 97.81%. The study was conducted according to the Declaration of Helsinki and was also approved by the Ethics Committee of Zhengzhou University (Approval No. ZZUIRB2023-284).
Measures
Metacognition
MCQ-30 was developed by Wells et al21, in 2004. Fan et al37 translated the MCQ-30 into Chinese using standard translation and back-translation. The Chinese version has demonstrated good reliability and validity in Chinese college students’ sample, with Cronbach’s α for the five factors ranging from 0.735 to 0.897.37 The MCQ-30 is a self-report tool consisting of 30 items divided into five metacognitive belief dimensions, each with six items: 1) CC (eg, “I do not trust my memory”), 2) POS (eg, “Worrying helps me solve problems”), 3) NEG (eg, “My worrying thoughts persist no matter how I try to stop them”; “My worrying could make me go mad”), 4) CSC (eg, “I am constantly aware of my thinking”), and 5) NC (eg, “I should be in control of my thoughts all of the time”). This questionnaire employs a 4-point Likert scoring system, with a total score ranging from 30 to 120. A higher score indicates that respondents are more likely to engage in a particular type of metacognition.
Depression
Depressive symptoms were assessed using the Patient Health Questionnaire-9 (PHQ-9), which is a reliable and validated screening tool for depression.38 This self-report screening scale has been validated in Chinese people.39 It includes nine items based on DSM-IV depressive symptoms, evaluated on a four-point Likert-type scale (0 = not at all, 3 = almost every day) with higher total scores indicating a higher degree of depressive symptoms (α = 0.85).38
Anxiety
Anxiety symptoms were assessed using the Generalized Anxiety Disorder-7 (GAD-7), which consists of seven aspects based on the DSM-IV and is a helpful and accurate way to gauge the severity of anxiety symptoms within two weeks.40 The GAD-7 is a self-rating scale that has been validated in China to detect anxiety and assess the severity of anxiety symptoms.41 The score of each item ranges from 0 to 3 and, The overall score of the GAD-7 ranges from 0 to 21. When a GAD-7 score was >5, anxiety symptoms were identified.42
Post-Traumatic Growth
PTG was measured by the 20-item Chinese Version of Post-traumatic Growth Inventory (C-PTGI),43 which was adapted from the Post-traumatic Growth Inventory.44 C-PTGI is comprised of the following five subscales: relating to others, new possibilities, personal strength, spiritual change, and appreciation for life. Each item was answered on a 6-point Likert scale from 0 (strongly disagree) to 5 (strongly agree), with total scores ranging from 0 to 100. High scores indicated high PTG. Previous studies have demonstrated the reliability and validity of this instrument in Chinese youth populations with myocardial infarction.45
Statistical Analyses
Preliminary analyses were conducted, including descriptive statistics and a normality test. We used confirmatory factor analysis (CFA) with maximum likelihood (ML) estimation to evaluate the structure and dimensionality of the MCQ-30. The ML method was selected due to its superiority in overall fitting and parameter estimation, especially with ordinal data. The sample size of the study was 313, which exceeded the recommended minimum of 200 for CFA.46 First, a unidimensional model was fitted to serve as a baseline for comparison. Then, the two pre-specified models (five-factor model and bi-factor model) for the MCQ-30’s factor structure were tested.
The model with lower Akaike information criterion (AIC) and Bayesian information criterion (BIC) values was chosen in the CFA.47 A cutoff of 0.30 for factor loadings was established for larger sample sizes. The selected model was adjusted to improve model fit as needed, using the statistical significance of path coefficients, modification indices (MIs), expected parameter change (EPC > 0.10), and standardized expected parameter change (SEPC > 0.20).48 Good model fit was evaluated using the chi-square (χ²) value, comparative fit index (CFI > 0.09), incremental fit index (IFI > 0.09), Tucker-Lewis index (TLI > 0.09), root mean square error of approximation (RMSEA < 0.08), and standardized root mean square residual (SRMR<0.08).46,49 Internal consistency of subscales was tested using Cronbach’s alpha (α > 0.70 for acceptable, α > 0.80 for good), and criterion validity was tested through correlations of the MCQ-30 with depression and anxiety measures.
Hierarchical multiple regression was used to determine the most significant metacognitive factor predicting depression, anxiety, and PTG. Based on previous research,50,51 age and gender are important variables that influence psychological factors in patients with AMI. Therefore, to control for potential confounding bias, we set age and gender as covariates. Assumptions of linearity, homoscedasticity, independence of residuals, and normality of error distribution were tested to ensure the appropriateness of the regression analysis.
All analyses were performed using SPSS 26.0 and MPLUS 8.3, and a two-sided p-value < 0.05 was considered statistically significant.
Results
Sociodemographic and Clinical Characteristics of the Participants
The sample in this study comprised 313 young and middle-aged patients with AMI. Male patients accounted for 85.3%, with an average age of 50.87 years. The detailed sociodemographic and clinical characteristics of the participants are presented in Table 1.
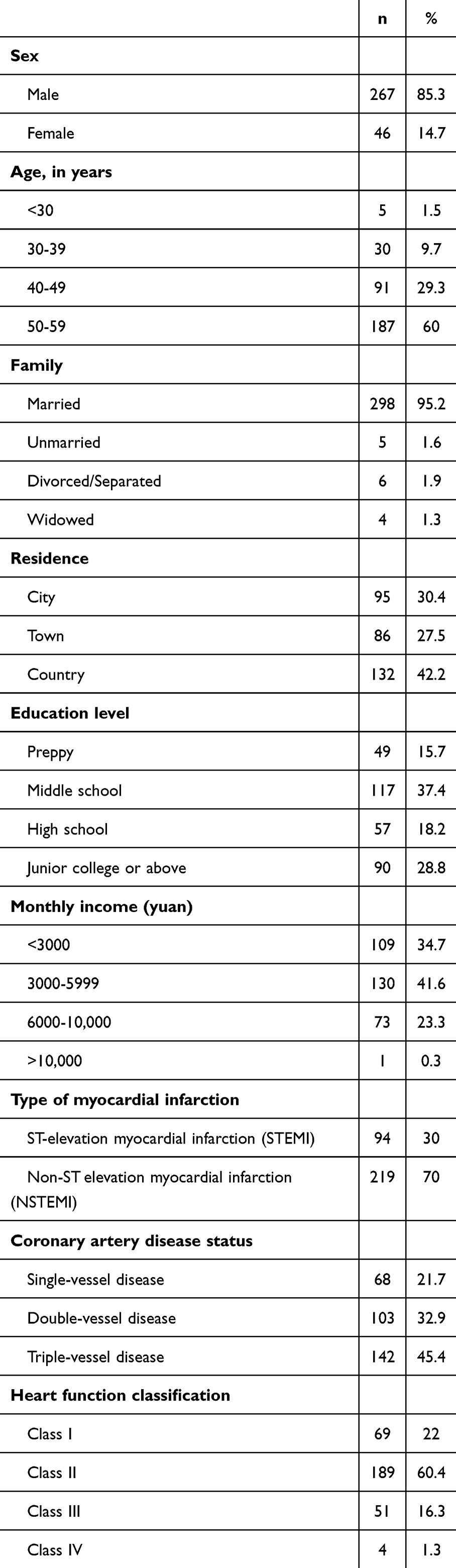 |
Table 1 Sociodemographic Characteristics of the Sample |
Reliability and Inter-Factor Correlation
Table 2 shows high reliability of the Chinese version of the MCQ-30 sub-scales (α = 0.81 to 0.89), and Cronbach’s α value for the Chinese version of the MCQ-30 was 0.93. The correlation analysis revealed significant positive relationships among the five factors in the MCQ-30 scale (r = 0.23 to 0.61, p < 0.001).
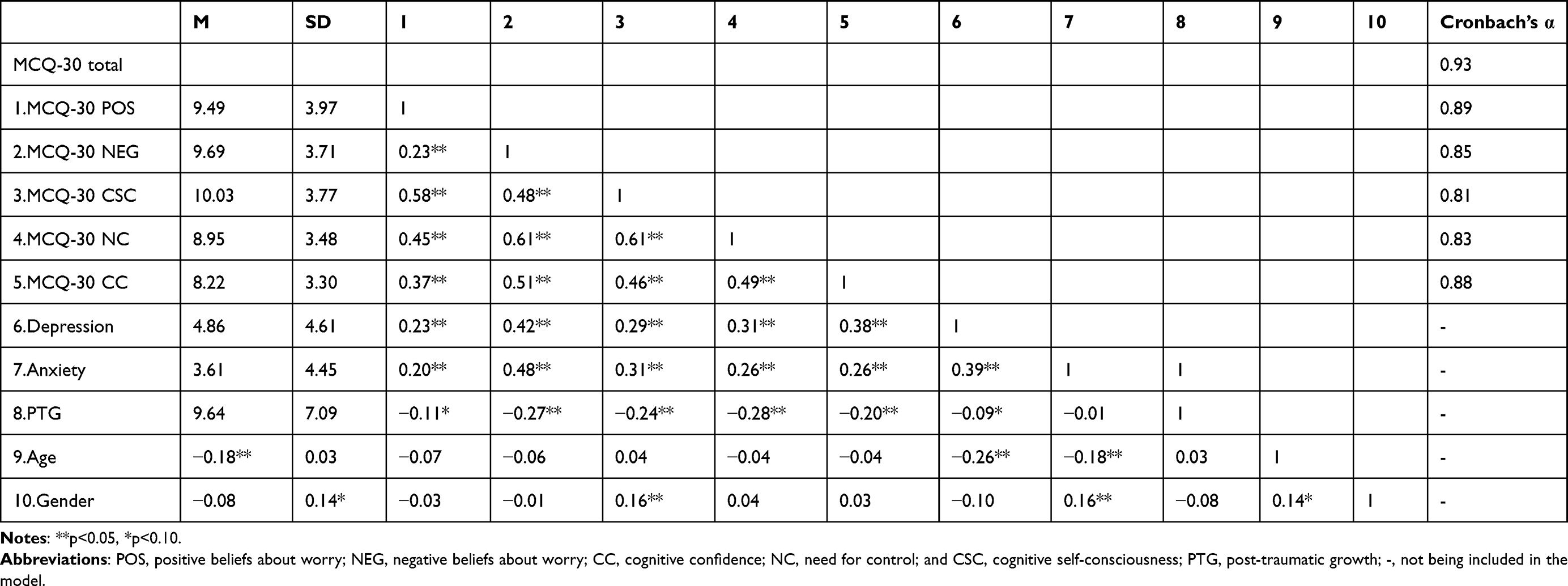 |
Table 2 Descriptive Statistics, Internal Consistency and Inter-Correlations of Constructs of the MCQ-30, Depression, Anxiety, PTG, and Demographics. (N = 313) |
Confirmatory Factor Analysis
The path diagram of the normalized parameter estimation for the model is shown in Figure 1. As we can see, its respective factors influenced each of the 30 items, all residual errors were irrelevant, and all factor loadings were greater than 0.30. Table 3 shows the Goodness-of-fit statistics for each model. As expected, the standard five-factor model demonstrated acceptable fit in step 1, χ2(395) = 1290.31, p<0.001, CFI = 0.826, IFI = 0.828, TLI = 0.809, RMSEA = 0.080, SRMR = 0.073. Although the CFI of the five-factor model was slightly lower than the recommended value, its overall goodness-of-fit was adequate, with satisfactorily high factor loadings for all items. We also examined the Bi-factor model, in which the five factors of the MCQ-30 loaded on one higher-level construct, and found that its model fit, χ2(399) = 1368.43, p<0.001, CFI = 0.812, IFI = 0.815, TLI = 0.795, RMSEA = 0.088, SRMR = 0.085, was close to that of the five-factor model. We also tested the One-factor model. However, its fit indices were significantly unacceptable, CFI = 0.562, IFI = 0.563, TLI = 0.530, RMSEA =0.133, SRMR = 0.113.
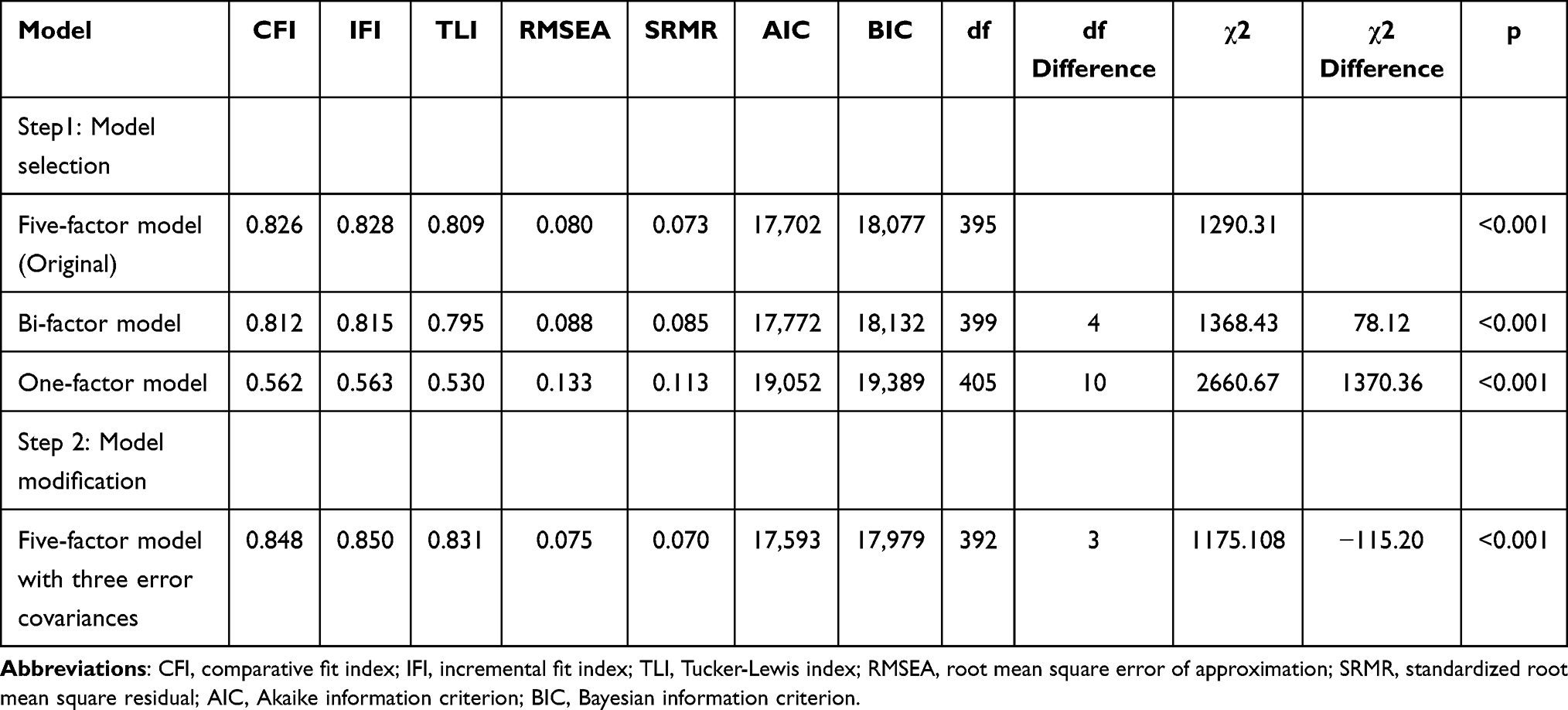 |
Table 3 Results of χ2 Test for Model Selection and Modification |
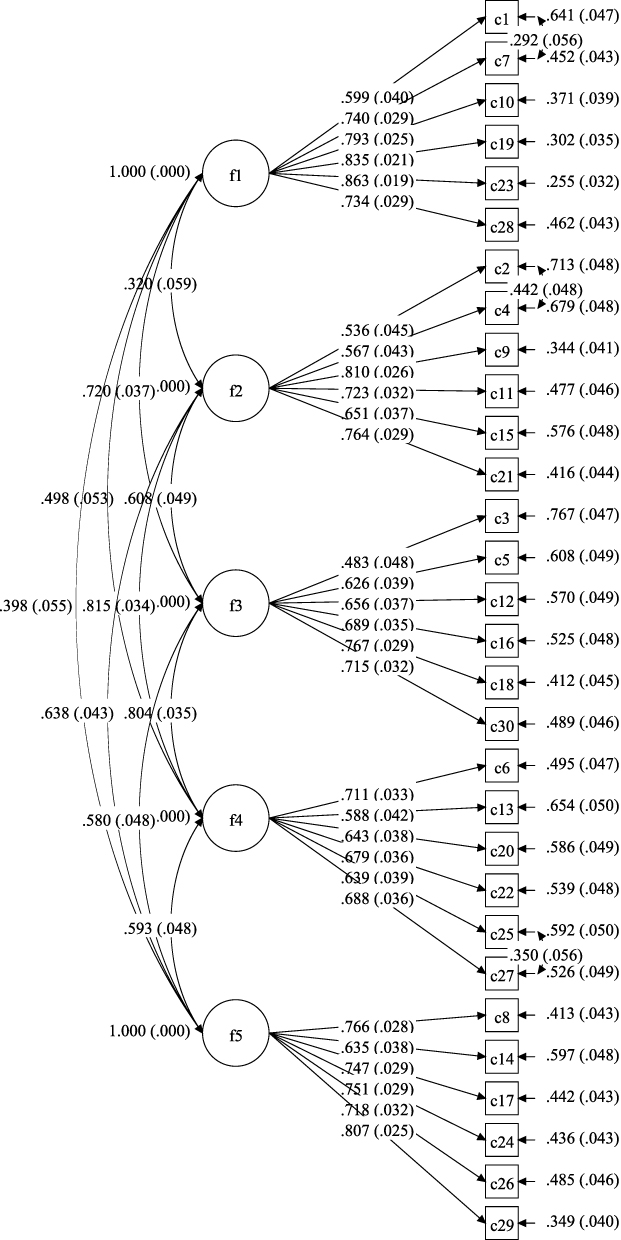 |
Figure 1 Five-factor model of the MCQ-30. |
In step 2, we considered modifying the five-factor model because of its only fair model fit. All path coefficients in the five-factor model were statistically significant, and no paths were removed. Then, based on MIs, EPC, and SEPC, three error covariances were added to the model to improve the model fit, χ2(392) = 1175.11, p < 0.001, CFI = 0.848, IFI = 0.850, TLI = 0.831, RMSEA = 0.075, SRMR = 0.070. Although the CFI value was slightly lower than the recommended value, the overall goodness-of-fit of the revised five-factor model was adequate. Additionally, its AIC, BIC, and χ² values were the smallest among all models, and the factor loadings were satisfactory.
Criterion-Related Validity
In terms of criterion-related validity, we evaluated the correlations between the five factors of the MCQ-30 and symptoms of depression and anxiety in Table 2. Each factor showed a significant positive correlation with depression and anxiety symptoms (r =0.20 to 0.48, p <0.001). We used the hierarchical multiple regression to identify salient and unique metacognitive correlates of depression and anxiety. Assumptions of linearity, homoscedasticity, independence of residuals, and normally distributed errors were met for the regression analyses. As shown in Table 4, the five factors of the MCQ-30 when entered together explained significant additional variance in anxiety symptoms (F change = 6.25, p < 0.001) after controlling for the impact of gender, age, and depression. Even after we controlled the effects of gender, age, and anxiety, the five factors of the MCQ-30 also explained significant additional variance in depression symptoms (F change = 9.15, p < 0.001). When we tested predictors of depression, the CC emerged as an independent and significant metacognitive factor (β = 0.21, 95% CI [0.15, 0.42], p < 0.001). However, in the predictors of anxiety, the NEG emerged as the most significant metacognitive factor (β = 0.31, 95% CI [0.25, 0.50], p < 0.001), the POS emerged as the only non-significantly and independent metacognitive factor (β = 0.03, 95% CI [−0.08, 0.14], p > 0.05).
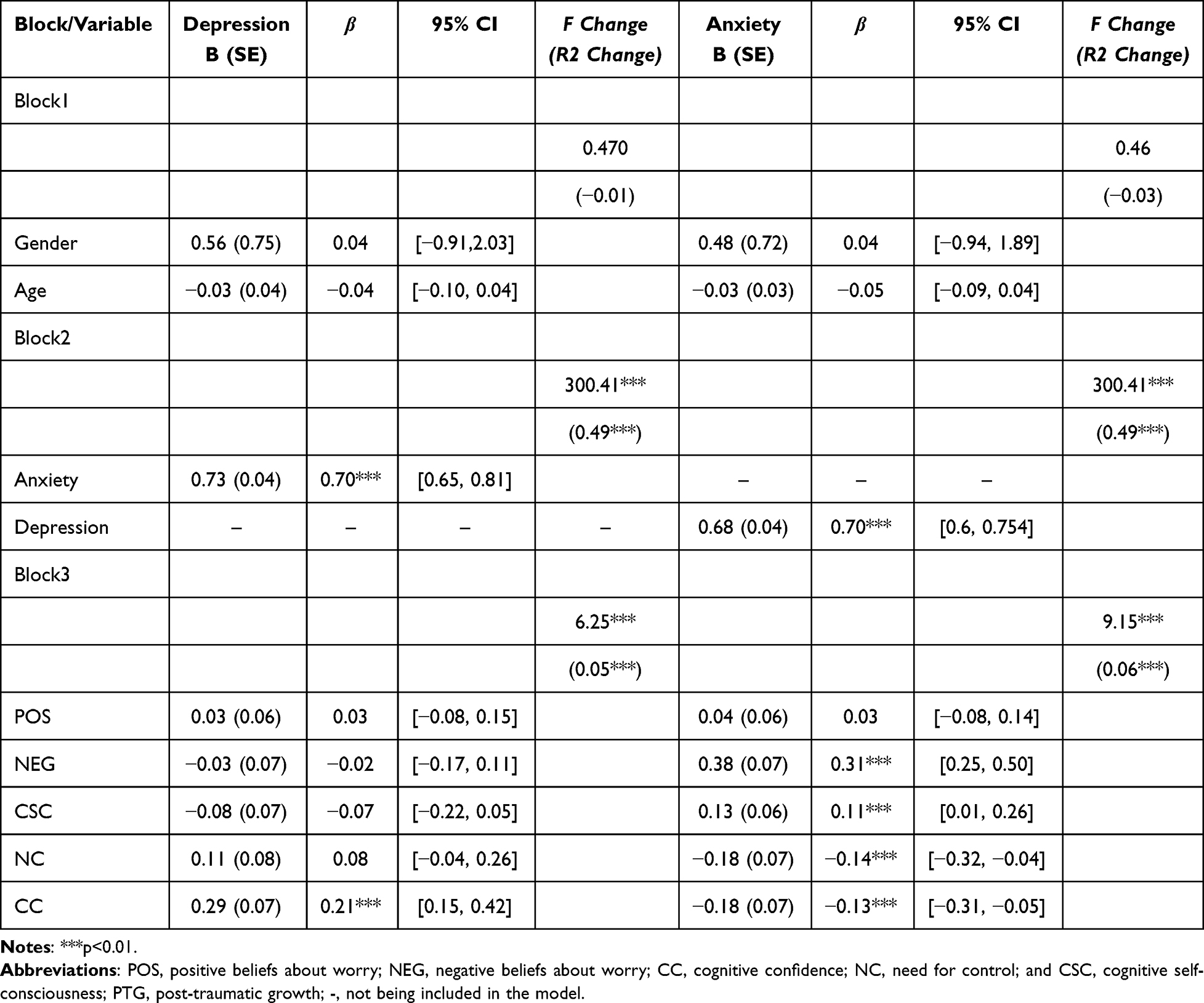 |
Table 4 The Results of the Model of Hierarchical Multiple Regression of MCQ-30 Factors on Depression and Anxiety Symptoms |
The Relationship Between Metacognition and PTG
As shown in Table 2, all five factors of the MCQ-30 exhibited significant negative correlations with PTG (r = 0.201 to 0.28, p < 0.001). What is worth noting is that the correlation between NC and PTG is the strongest. Then we used hierarchical multiple regression to examine the relationship between PTG and metacognition. In Table 5, the model was adjusted for gender and age in block 2, and the results showed that all the factors of metacognition significantly accounted for the additional variance in PTG (F change = 7.5, p < 0.05). Further analysis revealed that NC was an independent predictor of changes in PTG (β = −0.17, 95% CI [−2.18, −0.14], p < 0.05). To control for the potential confounding effects of anxiety and depression on PTG, we further examined the association between metacognitive factors and PTG (Table 6). The results of Block 3 showed that, after controlling for demographic variables, anxiety, and depression, metacognition significantly contributed to the additional variance in PTG (F change = 7.93, p<0.05). Furthermore, NEG independently explained changes in PTG (β = −0.16, 95% CI [−2.00, −0.08], p<0.05).
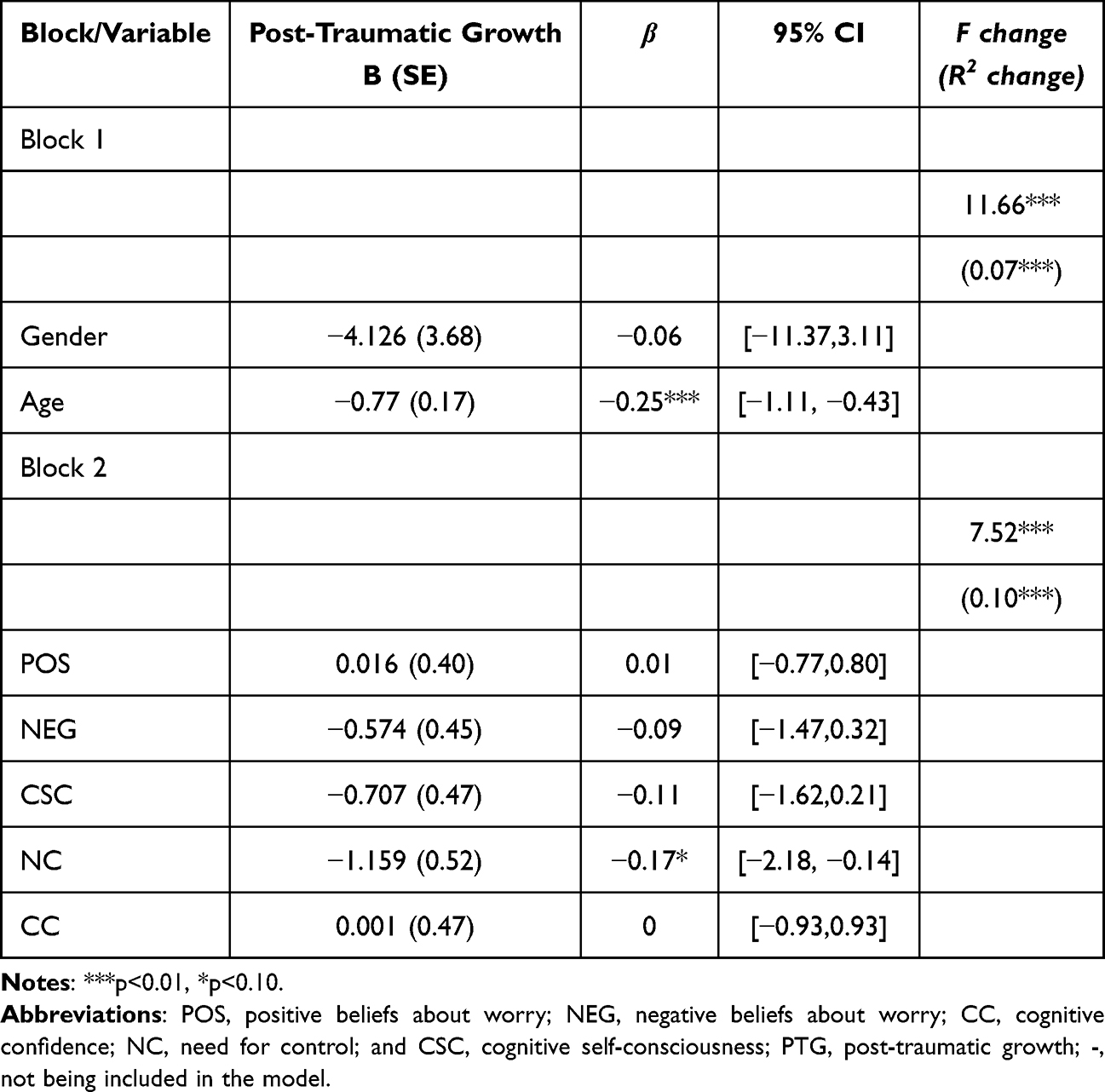 |
Table 5 The Results of Model of Hierarchical Multiple Regression of MCQ-30 Factors on Post-Traumatic Growth |
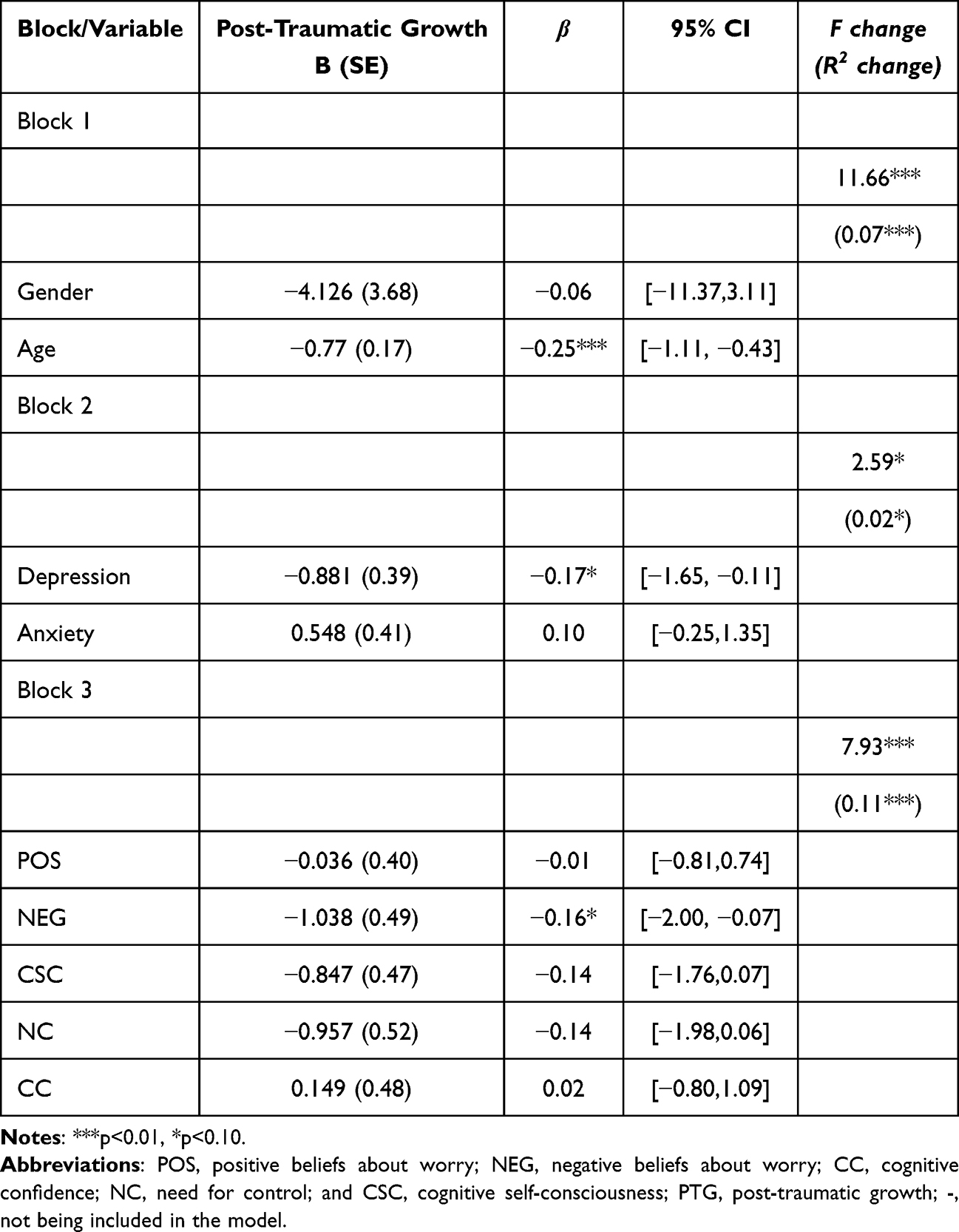 |
Table 6 The Results of the Model of Hierarchical Multiple Regression of MCQ-30 Factors on Post-Traumatic Growth (After Adjusting for Anxiety and Depression) |
Discussion
Currently, research has explored the effectiveness of the MCQ-30 in cardiovascular patients.25 However, few studies have been reported on cardiovascular disease in young and middle-aged patients in China, especially those with acute myocardial infarction. The internal consistency of the MCQ-30 questionnaire in young and middle-aged patients with AMI was assessed using Cronbach’s α coefficient. The results of a high Cronbach’s α coefficient indicate that the questionnaire demonstrates reliable measurement consistency in this population. Additionally, the correlation analysis reveals significant correlations among the five factors of the metacognition questionnaire. This suggests the presence of a common psychological mechanism underlying these metacognitive factors.21 According to previous research, individuals utilize the Metacognitive Control System (MCS) to orchestrate the interaction of various metacognitive elements within the self-regulation process, thereby fostering a coordinated influence on self-awareness and psychological health.52 The CFA results showed that in the original five-factor model, except for the CFI value, which was slightly below the recommended level, other indices were within the acceptable range, similar to previous findings reported in the Chinese population.31 We also examined the two-factor and one-factor models, but the fit results were not promising. The original five-factor model distinguishes multiple dimensions of metacognition, such as cognitive monitoring, emotional responses, and control strategies, providing a more accurate reflection of an individual’s metacognitive processes.21 The validation of its fit in this study further supports this view. As previous studies have shown, to improve the model fit, we further made minor modifications to the model by adding three error covariances. Despite the overall improvement in fit indices, the CFI value remained just below the threshold considered satisfactory, which certain studies indicate that values > 0.8 are acceptable.53 This is a preliminary study validating metacognition in young and middle-aged patients with AMI. It suggests that inherent cultural differences between the East and West may influence the representativeness in these two domains.27,29 To validate these findings, further studies involving a larger population of Chinese myocardial infarction patients are needed.
The results of the subscales’ criterion-related validity showed that metacognition is significantly correlated with depression and anxiety symptoms in Chinese young and middle-aged patients with AMI. These findings are consistent with previous studies funded by the National Institute for Health Research (NIHR),25 providing evidence for the criterion-related validity of these subscale.54,55 Among the five factors of metacognition in regression analysis, cognitive confidence was the most significant factor correlated with depression symptoms. Patients with lower cognitive confidence tend to be more prone to ruminative thinking, which is characterized by repeatedly questioning their decisions or memories of past events, and feeling uncertain and pessimistic about the future. These manifestations are positively correlated with depressive symptoms.56,57 At the same time, negative beliefs about worry were the most significant factor correlated with anxiety symptoms, similar to findings from previous studies.9,56 When patients hold the belief that “worry is harmful”, they are likely to focus more on their anxiety symptoms, which can lead to an amplification of those symptoms. Such increased attention shows a close correlation with the occurrence of anxiety symptoms.36 Young and middle-aged patients are at a crucial stage of life, often burdened with increasing social responsibilities and multiple roles, which render them more susceptible to psychological disorders after AMI.58–60 Therefore, these findings highlight the importance of addressing cognitive confidence and negative beliefs about worry to effectively manage anxiety and depression symptoms in young and middle-aged patients within future MCT in China.
In the present study, we explored the correlation between metacognition and PTG, aiming to expand the position of metacognition within positive psychology. Significant negative correlations were found between the subscales of the Chinese version of the MCQ-30 and PTG, and the results remained unchanged after controlling for age and gender. Considering the potential mediating effects of anxiety and depression, we also adjusted them in a new model and subsequently found similar results to previous models. Notably, before controlling for anxiety and depression, need for control was identified as the most prominent metacognitive factor. In contrast, after making these adjustments, negative beliefs about worry emerged as the most significant. Our findings add to the growing evidence that metacognition may have a negative impact on the mental health of CVD patients.54,61 Previous studies have revealed that the sudden onset of AMI and the prolonged course of treatment result in significant physical and emotional distress, accompanied by a pervasive sense of helplessness, which is difficult to resolve in the short term.60 A plausible interpretation, in conjunction with the S-REF model, is that the negative aspects of metacognition contribute to the persistence and exacerbation of psychological disorders, while also negatively correlating with an individual’s growth from traumatic experiences.62
Surprisingly, after adjusting for anxiety and depression, the significant metacognitive factors in the regression model changed from need for control to negative beliefs about worry. Previous studies suggest that depression symptoms can intensify negative metacognitive beliefs and drive a heightened need for control.36,63 This process may initiate a vicious cycle, ultimately undermining an individual’s capacity for recovery. For example, individual growth involves self-regulation and cognitive control, both of which are grounded in the need for control. The activation of these control beliefs, however, is contingent upon the presence of negative beliefs about worry. These findings offer key references for MCT in Chinese. When delivering psychological rehabilitation within the framework of positive psychology, the programs need to guide clinical healthcare providers to attach importance to the mediating role of anxiety and depression symptoms, and to accurately identify patients’ negative metacognitive beliefs—an essential direction for enhancing the relevance and effectiveness of interventions.
This study also had some limitations. Firstly, this is a cross-sectional study that lacks longitudinal data, which not only makes it difficult to establish a causal relationship between metacognition and psychological disorders but also prevents exploration of the cross-time stability of the factor structure. Secondly, although we explored the criterion-related associations between the five factors of metacognition and anxiety, depression, and PTG, we did not include more emotional and psychiatric disturbances. Thirdly, due to the specificity of the study population, this study only recruited participants from one hospital in China, which may lead to potential sampling bias and limit the generalizability of the findings.
Conclusion
This preliminary validation study supports the five-factor model of the original MCQ-30 in a specific clinical population through CFA and confirms good reliability and validity. However, some psychometric indices, such as the CFI, are below the ideal threshold. All five factors of metacognition are associated with PTG, demonstrating the first application of the S-REF model to PTG. This study provides empirical evidence for the potential efficacy of assessing metacognition and metacognitive therapy in young and middle-aged patients with AMI. However, a larger sample size and a longitudinal design are still required to verify its generalizability before it can be promoted and applied.
Ethics
This study was approved by the Research Ethics Review Committee of Zhengzhou University, China (Approval No. ZZUIRB2023-284).
Acknowledgments
We express our sincere gratitude to all the participants of this study. The abstract of this paper was presented at the NWC Conference name 8th Edition of Nursing World Conference as a conference talk with interim findings.
Funding
This study was supported by the funding from National Natural Science Foundation of China (72274180), Science and Technology Department of Henan Province in China (232102311023) and the Training Program for Young Backbone Teachers of Zhengzhou University (2024ZDGGJS041).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ahn S, Ko E, Ro YS. Acute myocardial infarction diagnosed in emergency departments: a report from the national emergency department information system (NEDIS) of Korea, 2018–2022. Clin Exp Emerg Med. 2023;10(S):S42–S47. doi:10.15441/ceem.23.140
2. Panduranga P, Al-Rashidi M, Al-Hajri F. In-hospital and one-year clinical outcome of percutaneous coronary intervention in a tertiary hospital in Oman: Oman PCI registry. Oman Med J. 2017;32(1):54. doi:10.5001/omj.2017.10
3. Rao A, Zecchin R, Newton P, et al. The prevalence and impact of depression and anxiety in cardiac rehabilitation: a longitudinal cohort study. Euro J Prev Cardiol. 2019;27(5):478–489. doi:10.1177/2047487319871716
4. Wells A, Reeves D, Capobianco L, et al. Improving the effectiveness of psychological interventions for depression and anxiety in cardiac rehabilitation: pathway—a single-blind, parallel, randomized, controlled trial of group metacognitive therapy. Circulation. 2021;144(1):23–33. doi:10.1161/circulationaha.120.052428
5. Arora S, Stouffer GA, Kucharska-Newton AM, et al. Twenty year trends and sex differences in young adults hospitalized with acute myocardial infarction. Circulation. 2019;139(8):1047–1056. doi:10.1161/circulationaha.118.037137
6. Yang J, Biery DW, Singh A, et al. Risk factors and outcomes of very young adults who experience myocardial infarction: the partners young-mi registry. Am J Med. 2020;133(5):605–612.e1. doi:10.1016/j.amjmed.2019.10.020
7. Chang J, Deng Q, Guo M, et al. Trends and inequalities in the incidence of acute myocardial infarction among Beijing townships, 2007–2018. Int J Environ Res Public Health. 2021;18(23):12276. doi:10.3390/ijerph182312276
8. Palacios J, Khondoker M, Mann A, Tylee A, Hotopf M. Depression and anxiety symptom trajectories in coronary heart disease: associations with measures of disability and impact on 3-year health care costs. J Psych Res. 2018;104:1–8. doi:10.1016/j.jpsychores.2017.10.015
9. Sheppard LC. Emotional disorders and metacognition: innovative cognitive therapy. Psychol Med. 2002;32(4):750–752. doi:10.1017/S0033291702225702
10. Shea N, Boldt A, Bang D, Yeung N, Heyes C, Frith CD. Supra-personal cognitive control and metacognition. Trends Cog Sci. 2014;18(4):186–193. doi:10.1016/j.tics.2014.01.006
11. Lysaker PH, Cheli S, Dimaggio G, et al. Metacognition, social cognition, and mentalizing in psychosis: are these distinct constructs when it comes to subjective experience or are we just splitting hairs? BMC Psychiatry. 2021;21(1):329. doi:10.1186/s12888-021-03338-4
12. Sun X, Zhu C, So SHW. Dysfunctional metacognition across psychopathologies: a meta-analytic review. Eur Psychiatry. 2017;45:139–153. doi:10.1016/j.eurpsy.2017.05.029
13. Lawrie SM. Attention and emotion: a clinical perspective: a. wells and g. matthews; lawrence erlbaum associates, Hove, UK, 1994, ISBN 0-86377-339-7. J Psych Res. 2000;48(2):203. doi:10.1016/S0022-3999(99)00082-3
14. Capobianco L, Morris JA, Wells A. Worry and rumination: do they prolong physiological and affective recovery from stress? Anx Stress Coping. 2018;31(3):291–303. doi:10.1080/10615806.2018.1438723
15. Butow P, Kelly S, Thewes B, Hruby G, Sharpe L, Beith J. Attentional bias and metacognitions in cancer survivors with high fear of cancer recurrence. Psycho Oncol. 2014;24(4):416–423. doi:10.1002/pon.3659
16. Feng WY, qi KQ, yi ZX, Xiong J-M, Li Y-M, Yang Q-H. Latent profile analysis and related factors of post-traumatic growth in young and middle-aged patients with acute myocardial infarction. Heart Lung. 2023;62:145–151. doi:10.1016/j.hrtlng.2023.07.003
17. MaJ NN, Mordeno IG. Positive metacognitions and meta-emotions as predictors of posttraumatic stress disorder and posttraumatic growth in survivors of a natural disaster. J Loss Trauma. 2018;23(5):381–394. doi:10.1080/15325024.2017.1415734
18. Tedeschi RG, Blevins CL. From mindfulness to meaning: implications for the theory of posttraumatic growth. Psychol Inq. 2015;26(4):373–376. doi:10.1080/1047840x.2015.1075354
19. Martiadis V, Pessina E, Raffone F, Iniziato V, Martini A, Scognamiglio P. Metacognition in schizophrenia: a practical overview of psychometric metacognition assessment tools for researchers and clinicians. Front Psychiatry. 2023;14:1155321. doi:10.3389/fpsyt.2023.1155321
20. Cartwright-Hatton S, Wells A. Beliefs about worry and intrusions: the meta-cognitions questionnaire and its correlates. J Anx Disord. 1997;11(3):279–296. doi:10.1016/s0887-6185(97)00011-x
21. Wells A, Cartwright-Hatton S. A short form of the metacognitions questionnaire: properties of the MCQ-30. Behav Res Therapy. 2004;42(4):385–396. doi:10.1016/S0005-7967(03)00147-5
22. Cook SA, Salmon P, Dunn G, Fisher P. Measuring metacognition in cancer: validation of the metacognitions questionnaire 30 (MCQ-30). Macleod U, ed. PLoS One. 2014;9(9):e107302. doi:10.1371/journal.pone.0107302
23. Allott R, Wells A, Morrison AP, Walker R. Distress in Parkinson’s disease: contributions of disease factors and metacognitive style. Br J Psychiatry. 2005;187(2):182–183. doi:10.1192/bjp.187.2.182
24. Brown RG, Fernie BA. Metacognitions, anxiety, and distress related to motor fluctuations in Parkinson’s disease. J Psych Res. 2015;78(2):143–148. doi:10.1016/j.jpsychores.2014.09.021
25. Faija CL, Reeves D, Heal C, Wells A. Metacognition in cardiac patients with anxiety and depression: psychometric performance of the metacognitions questionnaire 30 (MCQ-30). Front Psychol. 2020;11:1064. doi:10.3389/fpsyg.2020.01064
26. Li F, Yuan D, Gao C, Xiong K, Geng F, Zhang L. Validity and reliability of the metacognitions questionnaire-30 (MCQ-30) among Chinese adolescents. Child Psychiatry Hum Dev. 2025;56(4):1031–1040. doi:10.1007/s10578-023-01625-7
27. Martín J, Padierna A, Unzurrunzaga A, González N, Berjano B, Quintana JM. Adaptation and validation of the metacognition questionnaire (MCQ-30) in Spanish clinical and nonclinical samples. J Affective Disorders. 2014;167:228–234. doi:10.1016/j.jad.2014.06.009
28. Baptista A, Soumet-Leman C, Visinet A, Jouvent R. Metacognitive beliefs in depressed in-patients: adaptation and validation of the short version of the metacognitions questionnaire (MCQ-30) for French clinical and non-clinical samples. Behav Cog Psychotherap. 2020;48(4):498–502. doi:10.1017/s1352465820000065
29. Cho Y, Jahng S, Chai S. The factor structure and concurrent validity of the Korean version of the metacognitions questionnaire 30 (K‐MCQ‐30). J Clin Psych. 2012;68(3):349–391. doi:10.1002/jclp.20867
30. Gündüz A, Gündoğmuş İ, Sertçelik S, et al. Validity and reliability of the turkish version of generalized anxiety disorder scale-revised. Psychiatry Invest. 2021;18(10):949–957. doi:10.30773/pi.2021.0174
31. Zhang MX, Lei LSM, Wells A, Dang L, Wu AMS. Validation of a Chinese version of the short form of metacognitions questionnaire (MCQ-30). J Affective Disorders. 2020;277:417–424. doi:10.1016/j.jad.2020.08.028
32. Dammen T, Papageorgiou C, Lindstrøm JC, Einvik G. Metacognitions in patients with chronic obstructive pulmonary disease: a psychometric study of the metacognitions questionnaire-30. Front Psychol. 2023;14:1265102. doi:10.3389/fpsyg.2023.1265102
33. Wells A. Meta-cognition and worry: a cognitive model of generalized anxiety disorder. Behav Cog Psychotherap. 1995;23(3):301–320. doi:10.1017/S1352465800015897
34. Wells A, Reeves D, Heal C, et al. Metacognitive therapy home-based self-help for anxiety and depression in cardiovascular disease patients in the UK: a single-blind randomised controlled trial. Tomlinson M, ed. PLoS Med. 2023;20(1):e1004161. doi:10.1371/journal.pmed.1004161
35. Normann N, van Emmerik AAP, Morina N. The efficacy of metacognitive therapy for anxiety and depression: a meta-analytic review. Depression Anxiety. 2014;31(5):402–411. doi:10.1002/da.22273
36. Anderson R, Capobianco L, Fisher P, et al. Testing relationships between metacognitive beliefs, anxiety and depression in cardiac and cancer patients: are they transdiagnostic? J Psychosom Res. 2019;124:109738. doi:10.1016/j.jpsychores.2019.109738
37. Fan W, Fu Z, Xu W, Zhu Y, Yu M, Wang J. Revision of the meta-cognitions questionnaire in chinese college students. Chin J Clin Psychol. 2017;25(2):448–452.
38. Kroenke K, Spitzer RL, Williams JBW. The PHQ-9. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
39. Wang W, Bian Q, Zhao Y, et al. Reliability and validity of the Chinese version of the patient health questionnaire (PHQ-9) in the general population. General Hospital Psychiatry. 2014;36(5):539–544. doi:10.1016/j.genhosppsych.2014.05.021
40. Yang Y, Song Y, Lu Y, Xu Y, Liu L, Liu X. Associations between erectile dysfunction and psychological disorders (depression and anxiety): a cross‐sectional study in a Chinese population. Andrologia. 2019;51(10). doi:10.1111/and.13395
41. Tong X, An D, McGonigal A, Park SP, Zhou D. Validation of the generalized anxiety disorder-7 (GAD-7) among Chinese people with epilepsy. Epilepsy Res. 2016;120:31–36. doi:10.1016/j.eplepsyres.2015.11.019
42. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092. doi:10.1001/archinte.166.10.1092
43. Lilien TA, Groeneveld NS, Van etten-jamaludin F, et al. Association of arterial hyperoxia with outcomes in critically Ill children: a systematic review and meta-analysis. JAMA Network Open. 2022;5(1):e2142105. doi:10.1001/jamanetworkopen.2021.42105
44. Tedeschi RG, Calhoun LG. The posttraumatic growth inventory: measuring the positive legacy of trauma. J Trauma Stress. 1996;9(3):455–471. doi:10.1007/bf02103658
45. Cheng CH, Ho SM, Rochelle TL. Examining the psychometric properties of the Chinese post-traumatic growth inventory for patients suffering from chronic diseases. J Health Psychol. 2015;22(7):874–885. doi:10.1177/1359105315617330
46. Kline RB. Principles and Practice of Structural Equation Modeling. Guilford Publications; 2023.
47. Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Modeling. 1999;6(1):1–55. doi:10.1080/10705519909540118
48. Whittaker TA. Using the modification index and standardized expected parameter change for model modification. J Exp Educ. 2012;80(1):26–44. doi:10.1080/00220973.2010.531299
49. Garver MS, Mentzer JT. Logistics research methods: employing structural equation modeling to test for construct validity. J Bus Logist. 1999;20(1):33.
50. Tao XU, Wei L, Xing-yu W, et al. Association of psychological risk factors and acute myocardial infarction in China: the INTER-HEART China study. Chinese Med J. 2011;124(14):2083–2088. doi:10.3760/cma.j.issn.0366-6999.2011.14.001
51. Faresjö Å, Karlsson JE, Segerberg H, Lebena A, Faresjö T. Cardiovascular and psychosocial risks among patients below age 50 with acute myocardial infarction. BMC Cardiovasc Disord. 2023;23(1):121. doi:10.1186/s12872-023-03134-w
52. Wells A. Breaking the cybernetic code: understanding and treating the human metacognitive control system to enhance mental health. Front Psychol. 2019;10:2621. doi:10.3389/fpsyg.2019.02621
53. Salum GA, Patrick DL, Isolan LR, et al. Youth quality of life instrument-research version (YQOL-R): psychometric proprieties in a community sample. Jornal de Pediatria. 2012. doi:10.2223/jped.2193
54. Mansueto G, Jarach A, Caselli G, et al. A systematic review of the relationship between generic and specific metacognitive beliefs and emotion dysregulation: a metacognitive model of emotion dysregulation. Clin Psychol Psychother. 2024;31(1):e2961. doi:10.1002/cpp.2961
55. Capobianco L, Faija C, Husain Z, Wells A. Metacognitive beliefs and their relationship with anxiety and depression in physical illnesses: a systematic review. PLoS One. 2020;15(9):e0238457. doi:10.1371/journal.pone.0238457
56. Mansueto G, Marino C, Palmieri S, et al. Difficulties in emotion regulation: the role of repetitive negative thinking and metacognitive beliefs. J Affect Disord. 2022;308:473–483. doi:10.1016/j.jad.2022.04.086
57. Baumgartner H, De Backer J, Babu-Narayan SV, et al. ESC guidelines for the management of adult congenital heart disease. Eur Heart J. 2020;42(6):563–645. doi:10.1093/eurheartj/ehaa554
58. Barresi F, Foster-Witassek F, Rickli H, et al. Predictors of work inability after acute myocardial infarction in Switzerland. Sci Rep. 2024;14(1):13429. doi:10.1038/s41598-024-63988-8
59. Wasfy JH, Hidrue MK, Ngo J, et al. Association of an acute myocardial infarction readmission-reduction program with mortality and readmission. Circ Cardiovasc Qual Outcomes. 2020;13(5):e006043. doi:10.1161/CIRCOUTCOMES.119.006043
60. Lin Z, Han H, Qin Y, et al. Outcomes after readmission at the index or nonindex hospital following acute myocardial infarction complicated by cardiogenic shock. Clin Cardiol. 2021;44(2):200–209. doi:10.1002/clc.23526
61. Mansell W, McEvoy PM. A test of the core process account of psychopathology in a heterogenous clinical sample of anxiety and depression: a case of the blind men and the elephant? J Anxiety Disord. 2017;46:4–10. doi:10.1016/j.janxdis.2016.06.008
62. Clauss K, Benfer N, Thomas KN, Bardeen JR. The interactive effect of event centrality and maladaptive metacognitive beliefs on posttraumatic stress symptoms and posttraumatic growth. Psychol Trauma. 2021;13(5):596–602. doi:10.1037/tra0001010
63. Zhou H, Dang L, Lam LW, Zhang MX, Wu AMS. A cross-lagged panel model for testing the bidirectional relationship between depression and smartphone addiction and the influences of maladaptive metacognition on them in Chinese adolescents. Addict Behav. 2021;120:106978. doi:10.1016/j.addbeh.2021.106978
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Subjective Sleep Disruption and Mood Disorders are Associated with the Risk of Chronic Pain in Patients with Obstructive Sleep Apnea
Liu L, Li X, Xue P, Wu M, Zeng S, Dai Y, Zhou J
Nature and Science of Sleep 2022, 14:2023-2032
Published Date: 7 November 2022
Vitamin B12, Folate, Homocysteine, Inflammatory Mediators (Interleukin-6, Tumor Necrosis Factor-α and C-Reactive Protein) Levels in Adolescents with Anxiety or Depressive Symptoms
Tan Y, Zhou L, Huang J, Chen X, Wu Y, Song X, Wang J, Hu H, Yang Q
Neuropsychiatric Disease and Treatment 2023, 19:785-800
Published Date: 7 April 2023
AI Technology panic—is AI Dependence Bad for Mental Health? A Cross-Lagged Panel Model and the Mediating Roles of Motivations for AI Use Among Adolescents
Huang S, Lai X, Ke L, Li Y, Wang H, Zhao X, Dai X, Wang Y
Psychology Research and Behavior Management 2024, 17:1087-1102
Published Date: 12 March 2024
Longitudinal Problematic Social Media Use in Students and Its Association with Negative Mental Health Outcomes
Shannon H, Bush K, Shvetz C, Paquin V, Morency J, Hellemans KGC, Guimond S
Psychology Research and Behavior Management 2024, 17:1551-1560
Published Date: 8 April 2024
Mushrooms, Microdosing, and Mental Illness: The Effect of Psilocybin on Neurotransmitters, Neuroinflammation, and Neuroplasticity
Kinderlehrer DA
Neuropsychiatric Disease and Treatment 2025, 21:141-155
Published Date: 29 January 2025