")
Back to Journals » Advances in Medical Education and Practice » Volume 8
Medicons: toward clinical examination diagrams standardization in medical documentation
Authors Pafitanis G , Hadjiandreou M, Withers L, Dent H
Received 2 February 2017
Accepted for publication 21 March 2017
Published 19 May 2017 Volume 2017:8 Pages 347—351
DOI https://doi.org/10.2147/AMEP.S133681
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Georgios Pafitanis,1 Michalis Hadjiandreou,2 Leo Withers,1 Helen Dent3
1The Royal London Hospital, Barts Health NHS Trust, London, UK; 2Barts and the London School of Medicine and Dentistry, London, UK; 3St Richard’s Hospital, Chichester, UK
Background: Electronic patient records (EPRs) allow efficient and accurate medical documentation. Diagrams have traditionally been used to document clinical signs in patient notes. The interpretation of these diagrams may vary among doctors across a range of specialties, but this has never been tested previously. This study investigated how common diagrams were interpreted and explored the use of digitalized diagrams – Medicons in creating a common language to be used in digital clinical examination proformas.
Materials and methods: A cross-sectional survey utilizing a multiple-choice questionnaire was carried out across London hospitals. Seventeen digitalized examination diagrams were included in a multiple-choice questionnaire to test doctors’ perception and explore their opinions of diagram usage. The questionnaire was sent to junior doctors in training.
Results: A total of 206 responses were received from 31 foundation year 1 trainees, 45 foundation year 2 trainees, 94 core surgical trainees and 36 core medical trainees. Diagrams were interpreted correctly, on average, 75% of the time. The majority of doctors (94%) felt that diagrams facilitated the understanding of clinical examination, documentation of pathologic site (98%) and improved the efficiency of documentation (89.8%). All doctors felt that diagrams may benefit overall medical care provision.
Conclusion: Digitalizing signs and symptoms in EPR will enhance clinical documentation and may contribute to better patient care. New initiatives need to be employed to increase the use of diagrams – Medicons, as young doctors perceived these to improve clinical documentation. Standardized electronic proformas should be included into EPR to improve the efficiency and accuracy of clinical examination documentation.
Keywords: electronic patient record, medical documentation, clinical diagrams
Introduction
Hand-drawn diagrams have traditionally been used in medical documentation to visually portray a patient’s clinical picture by the use of shading and symbols on a stylized representation of a body part. Electronic patient records (EPRs) allow patients’ full medical records to be updated and be readily available to doctors at the click of a button.1,2 This technology is in stark contrast to traditional, existing administrative methods, whereby patients’ records are kept on paper and entries are made and updated by hand.3 Electronic records have helped revolutionize the way patient information is recorded, leading to improved patient care, staff satisfaction and financial efficiency; however, there is limited evidence of incorporation of diagrams in EPRs.4–9 The introduction of EPRs provides an exciting opportunity to standardize the commonly used method of using diagrams to visually represent a patient’s signs and examination findings.
Diagrams are often used to literally portray “the clinical picture”; however, there is no accepted standard of diagrams used and interpretation of them is thought to differ across specialties and vary among individuals. To our knowledge, no research has ever been performed to investigate this issue. This study examines how doctors perceive commonly used clinical examination diagrams (CEDs) with the aim of providing the basis for the development of a common language (Medicons) to be used in medical curricula and in electronic digital records.
Materials and methods
A qualitative study was performed using a cross-sectional survey of doctors across different hospitals. The study was divided into two parts: first, 40 doctors, blind to the study rationale, were initially approached to document diagrams of various clinical examination findings. These individual responses were collated from a cohort of doctors regularly performing documentation in consultant-based National Health Service provision, generating 17 digitalized “CEDs – Medicons” (Figure 1). Seventeen diagrams were copied from previous documentations from the included doctors. No specific theoretical design or method was utilized. The Medicons were purely generated directly from the clinical environment to represent real-life professional medical documentation. We included diagrams that represent key clinical diagnosis, management, outcome and examination signs. These diagrams were then included in a questionnaire, which was sent out to doctors in the second part of the study. The Medicons were presented within a multiple-choice questionnaire aimed to test the doctors’ clinical interpretation of each diagram. Each diagram was given alongside five possible answers, and the respondents had to match each Medicon with the best corresponding statement. The questionnaire also incorporated further questions to seek the opinion of the respondents regarding whether they felt that diagram usage improved the efficiency of documentation, whether they assisted documentation of the site of the pathology and whether they led to a better understanding of the clinical examination findings. Questionnaires were circulated electronically among junior doctors in training across different specialties.
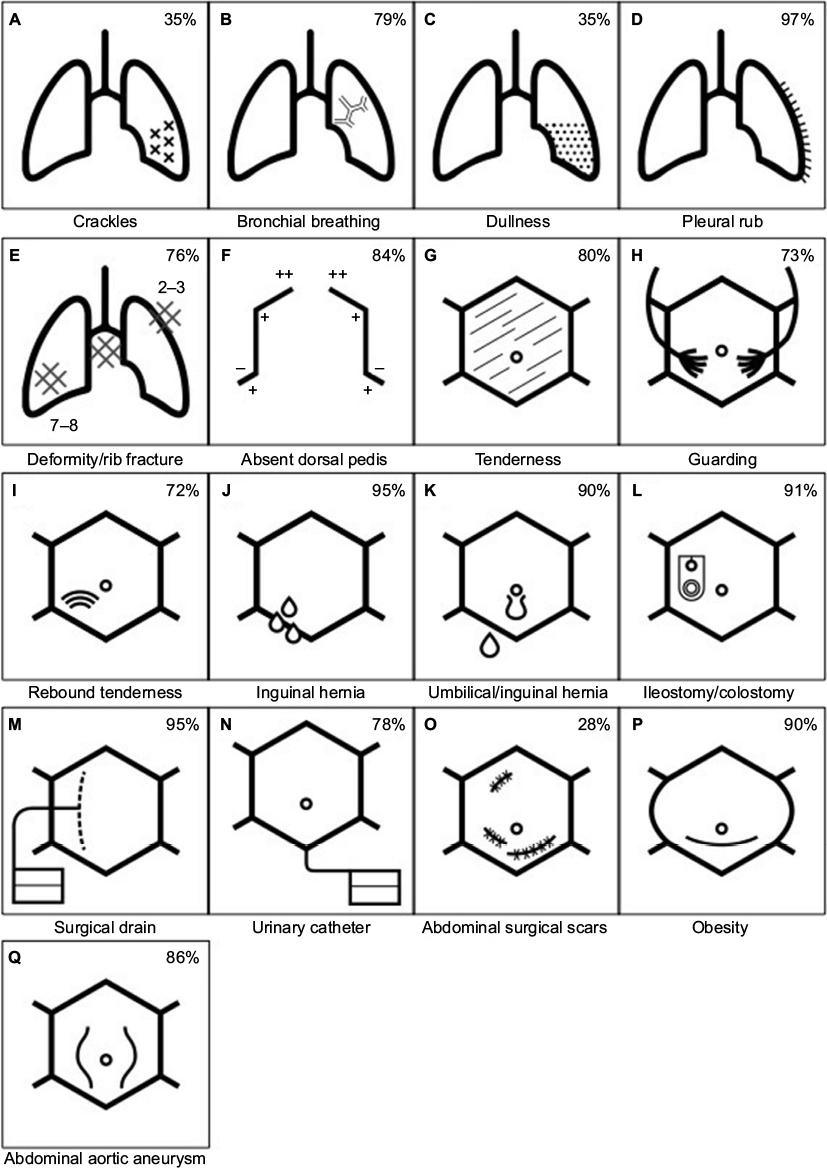 | Figure 1 All 17 CEDs – Medicons used to test doctor’s perception across different specialities (A–Q), with their specific conditions written below. Notes: Percentage of correct answer shown in top right (A–J). Abbreviation: CEDs, clinical examination diagrams. |
This survey-based study was conducted without involving any risk for the participating doctors or medical students; hence, the authors’ institutions (Queen Mary University of London, The Royal London Hospital, Barts Health NHS Trust) did not require any further ethical approval. All doctors or participants provided informed consent to participate in this study.
Results
A total of 206 (male:female=98:108) junior doctors responded. Thirty-one foundation year 1 trainees, 45 foundation year 2 trainees, 94 core surgical trainees and 36 core medical trainees responded.
Doctors’ opinions of Medicons were similar across all specialties: 94% of trainee doctors stated they felt diagrams helped improve the efficiency of documentation and all responders agreed that diagrams would overall benefit the provision of medical care. Ninety-eight percent thought that they aided documentation of the site of pathology. Also, 89.8% felt that they usually understood the clinical examination findings from Medicons seen in patient notes, and all responders agreed that diagrams would overall benefit the provision of medical care.
Figure 1 gives a pictorial representation of the 17 Medicons used in the questionnaire. The specific condition represented is indicated below each diagram and the percentage of correct answers given by the respondents is shown in each top right hand corner.
Overall, the correct answers were given 75% of the time. Figure 1D, E, G and H was all easily recognized and answered correctly over 90% of the time. In contrast, only 35% of respondents answered Figure 1A and C accurately and only 28% understood Figure 1O. There was no statistically significant difference between males and females. However, subgroup analysis of the 94 core surgical trainees versus the rest medical trainee doctors revealed higher response rate for Figure 1O (47% versus 11%, respectively). All other common diagrams were correctly identified between 70% and 90% of the time by trainees across all specialties.
Top right corner of images represents the percentage of trainees that correctly identified the clinical sign demonstrated by the CED – Medicon.
Discussion
In our study, an overwhelming majority of trainee doctors felt Medicons improved identification of the site of and the efficiency of examination findings documentation. This indicates doctors would like iconic language to continue to be used in medical practice, and thus suggests further use of digitalized icons in EPRs. The concept of iconic representation in medicine is currently reported by several software tools; nevertheless, the intended use of these systems differs from our intended use of iconic clinical findings documentation. Hsu and Taira reported a mapping software tool that, indeed, utilizes iconic representation with the aim of generating a timeline interface visualizing the changes in neuro-oncology patients.10 Karahoca et al reported a Medical Emergency Department Software Iconic that presents nurses’ tasks in the Emergency Department in iconic language.11 Both software tools have the potential to incorporate Medicons as a useful part of their general software system. We believe that surveys with similar structure and perception studies of similar protocol are required to achieve quality outcomes in communication between health care providers while using iconic systems.
Systems of similar concepts currently exist, with Chae et al reporting an advanced digitalized EPR system in a South Korean tertiary hospital, which allows easier and more efficient documentation.8 In addition, the Visualization of Medical Knowledge graphical language developed by Lamy et al uses iconic language such as Visualization of Medical Knowledge pathology or medical sign icons to represent pathology or clinical findings.9 Despite the higher degree of similarity of these two systems, our study design adds in representing the perception of doctors toward these novel systems and demonstrates potential drawbacks of misinterpretation of iconic representations with the potential safety risks. Undoubtedly, further studies need to be performed to investigate whether this perceived efficiency is reflected in practice, with a true impact on patient care. Nevertheless, should such technologies be introduced alongside EPRs in the UK, trainee doctors felt this would benefit their everyday practice. Specifically, in surgery, the development of a multimedia EPR for image-assisted minimally invasive spine surgery demonstrates the potential of digitalized tools to allow the operating surgeon to document informatics data in the form of real-time multimodality imaging and iconography.12
Understanding and interpretation of digitalized CEDs – Medicons was shown to have a consensus of 75% across all clinical specialties. This figure is good, considering there is no common practice available, and therefore no expectation that diagrams created by individuals would be widely recognized. This also suggests that CEDs do enhance current documentation methods. On the other hand, not all images were perceived accurately; Figure 1O, for example, was only answered correctly by 30% of participants. Surgical trainees responded to Figure 1O more accurately than medical trainees due to their surgical exposure. Nevertheless, results on general doctors’ perception in the early years of training should be consistent to allow iconic representation of clinical findings to be perceived correctly for safe and accurate digital documentation. In any case, this low accuracy raises clinical concerns, as a failure to correctly interpret a patient’s records could potentially lead to clinical error and patient harm. This highlights the need to create standard CEDs, while also suggesting some images should be refined, to ensure that interpretation is 100% accurate. Despite this, there was no great variation in CEDs interpretation between different specialties, which supports the potential for a common “Medicons” language.
Medical education curricula should consider including the topic of CEDs during the early years of training. With the launch of EPRs, CEDs – Medicons should be merged with new advancements in technology to enhance image-based medical records. New technological advancements, such as the digital pens, could make CEDs easier to reproduce and efficient to utilize.13 A nationally approved digital documentation standard could be introduced into medical education and help reduce interindividual variability in the visual documentation of clinical signs and symptoms. As a result, patient care may improve due to better doctor communication and shared decision making, as our respondents agreed.14 Potentially, Medicons can be used in EPRs in a similar manner to texting and chatting in electronic social media, which is currently a well-perceived practice.
Conclusion
Diagrammatic representation of clinical signs and examination findings should be accurately documented. Our study shows that a large majority of trainee doctors agree that CEDs – Medicons help improve documentation efficiency, identification of the site of pathology and the understanding of clinical findings. Furthermore, perception of these diagrams was considered to be very similar across different specialties, although still with a significant level of interpretation error using the diagrams we created. Together, these findings suggest that digitalizing CEDs – Medicons and creating a standard visual document can potentially enhance EPR accuracy and efficiency, therefore potentially improving patient care. The images created for this study could be used as a potential standard platform, but further research should be done to establish current common usage. Medical education curricula should consider formally including Medicons during medical training. With the launch of EPRs, Medicon language should be merged with new advancements in technology to allow drawings and standard diagrams to be incorporated in medical records.
Acknowledgment
The authors owe many thanks to Mr Robert Hume (Graphic Designer) for digitalizing hand-drawn diagrams for display in Figure 1.
Disclosure
The authors report no conflicts of interest in this work.
References
Future of patient records. Care for records for care: an appraisal of the practicalities of electronic patient record. Proceedings of the 8th European Health Records Conference. Maastricht, the Netherlands, May 21–24, 1996. | ||
Peckham D, Whitaker P, White H. Research in progress-electronic patient records: a new era. Thorax. 2015;70(5):473–475. | ||
Benjamin R. Finding my way to electronic health records. N Engl J Med. 2010;363(6):505–506. | ||
Peckham D, Etherington C, White H, et al. The development and deployment of integrated electronic care records in a regional adult and paediatric cystic fibrosis unit. J Cyst Fibros. 2014;13(6):681–686. | ||
Schaeffer AJ. Electronic medical records and data warehouses improve patient care and reduce costs. J Urol. 2011;186(1):7–8. | ||
Shephard EA, Neal RD, Rose PW, Walter FM, Hamilton WT. Quantifying the risk of non-Hodgkin lymphoma in symptomatic primary care patients aged ≥40 years: a large case-control study using electronic records. Br J Gen Pract. 2015;65(634):e281–e288. | ||
Tasa UB, Ozcan O, Yantac AE, Unluer A. A case study on better iconographic design in electronic medical records’ user interface. Inform Health Soc Care. 2008;33(2):125–138. | ||
Chae YM, Yoo KB, Kim ES, Chae H. The adoption of electronic medical records and decision support systems in Korea. Healthc Inform Res. 2011;17(3):172–177. | ||
Lamy J-B, Duclos C, Bar-Hen A, Ouvrard P, Venot A. An iconic language for the graphical representation of medical concepts. BMC Med Inform Decis Mak. 2008;8(1):16. | ||
Hsu W, Taira RK. Tools for improving the characterization and visualization of changes in neuro-oncology patients. AMIA Ann Symp Proc. 2010;2010:316–320. | ||
Karahoca A, Bayraktar E, Tatoglu E, Karahoca D. Information system design for a hospital emergency department: a usability analysis of software prototypes. J Biomed Inform. 2010;43(2):224–232. | ||
Documet J, Le A, Liu B, Chiu J, Huang HK. A multimedia electronic patient record (ePR) system for image-assisted minimally invasive spinal surgery. Int J Comput Assist Radiol Surg. 2010;5(3):195–209. | ||
Yen PY, Gorman PN. Usability Testing of a Digital Pen and Paper System in Nursing Documentation. AMIA Annu Symp Proc. 2005;2005:844–848. | ||
Samoutis G, Soteriades ES, Kounalakis DK, Zachariadou T, Philalithis A, Lionis C. Implementation of an electronic medical record system in previously computer-naive primary care centres: a pilot study from Cyprus. Inform Prim Care. 2007;15(4):207–216. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.