Back to Journals » Risk Management and Healthcare Policy » Volume 14
Medication Error Concept and Reporting Practices in Saudi Arabia: A Multiregional Study Among Healthcare Professionals
Authors Alshammari FM ![]() , Alanazi EJ
, Alanazi EJ ![]() , Alanazi AM
, Alanazi AM ![]() , Alturifi AK
, Alturifi AK ![]() , Alshammari TM
, Alshammari TM ![]()
Received 11 September 2020
Accepted for publication 29 April 2021
Published 4 June 2021 Volume 2021:14 Pages 2395—2406
DOI https://doi.org/10.2147/RMHP.S281154
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Kent Rondeau
Faizah M Alshammari,1 Entisar J Alanazi,1 Afnan M Alanazi,1 Abdulrahman K Alturifi,2 Thamir M Alshammari3,4
1Department of Clinical Pharmacy, College of Pharmacy, University of Hail, Hail, Saudi Arabia; 2Department of Infection Prevention and Control, Hail Health Affairs, Ministry of Health, Hail, Saudi Arabia; 3Department of Pharmacy Practice, College of Pharmacy, Riyadh Elm University, Riyadh, Saudi Arabia; 4Medication Safety Research Chair, King Saud University, Riyadh, Saudi Arabia
Correspondence: Thamir M Alshammari
Department of Pharmacy Practice, College of Pharmacy, Riyadh Elm University, P.O. Box 2457, Riyadh, 11451, Saudi Arabia
Tel +966 505192886
Email [email protected]
Background: Medication errors pose a risk for individual patients and for public health, with the misuse and overuse of medications being linked to severe patient safety problems. Therefore, the objective of this study was to investigate healthcare professionals’ (HCPs’) knowledge about medication errors, their knowledge about medication error reporting systems, and predictors for HCPs to report medication errors in Saudi Arabia.
Methods: An observational cross-sectional study was conducted among HCPs (physicians, pharmacists, and nurses) between January and March 2020. The study included 6 distinct locations in the Saudi Arabian regions of Hail, Al-Qassim, Al-Jouf, Al-Madinah, the eastern region, and the western region. Descriptive statistical and inferential analyses were computed using Statistical Package for the Social Sciences (SPSS) v.22.
Results: In total, 980 questionnaires for 348 (35.5%) physicians, 144 (14.7%) pharmacists, and 488 (49.8%) nurses were distributed with a response rate of 100%. Interestingly, only 277 (28.3%) of the HCPs had a good understanding of the stages of medication errors. With regard to reporting practices, a high number of the HCPs, 576 (58.8%), had not reported medication errors in their workplaces, and nearly 369 (37.7%) of respondents said they believe that legal implications are a major barrier to the reporting of medication errors. More than half, 524 (53.5%), of HCPs revealed that no clear electronic system is available for the reporting of medication errors in most hospitals. In addition, 537 (54.8%), of the HCPs had not attended any training programs regarding medication error reporting systems within the past year, which is alarming.
Conclusion: Our study identified a huge lack of the reporting of medication errors, knowledge about medication error stages, and training on medication errors. Therefore, an urgent need to address these weaknesses exists.
Keywords: medication errors, knowledge and attitude, healthcare professionals, patient safety, Saudi Arabia
Introduction
Medication errors are considered to be a global concern, as they are the most underreported types of medical errors.1–3 Medication errors can be defined as “any preventable event that may account to an inappropriate medication use which has the ability to cause harm to patient.”1,4 Although medications offer many benefits, they can harm patients if used incorrectly.5 Various factors of the medication use process might be the reason for such harm, such as a lack of performance, a shortage of knowledge, slips, and lapses.6 Medication errors are costly for patients and their families, hospitals and their medical staff, and insurance companies, and they lead to serious complications, such as prolonged hospitalization, poor outcomes, and a lack of quality of life.7–9 Therefore, the need exists to raise awareness of the occurrence and consequences of medication errors in an effort to reduce them.7 In hospitals, medication errors can happen at any stage, such as prescribing, transcribing, dispensing, administration, or monitoring.1,3,6,10 Prescribing errors represent approximately one-fifth of all medication errors encountered in primary care settings in the Kingdom of Saudi Arabia (KSA).11 However, the percentages of the errors that occur in the various stages are different.1,4,12 Healthcare professionals (HCPs) should be focused on their knowledge, attitudes, and practices toward medication errors and reporting them.13,14 Having a medication error reporting system is necessary for assessing and minimizing medication errors, which, in turn, protects patients from harm.15 In addition, using computerized physician order entry (CPOE) contributed to reducing the incidence of these errors.16–18 Most reported medication errors are unintentional; however, they might still increase morbidity and mortality rates.8 Thus, having a safe health care environment will help to reduce the occurrence of medication errors.10,19 In countries that have advanced health care systems and HCPs with various educational and practice backgrounds (eg, the KSA), dealing with the medication use process might be different based on nations’ backgrounds.4 Our study hypothesis for this research was that a lack of both knowledge about medication errors and medication error reporting practices exists among HCPs. Therefore, HCPs working in Saudi Arabia need to understand that reporting medication errors is everyone’s responsibility, as our main aim is to improve quality health care and safety for patients.1,3 To our knowledge, no data were available on medication errors and their reporting practices among HCPs from various health care facilities in the regions of Hail, Al-Qassim, Al-Jouf, Al-Madinah, the eastern region, and the western region. In addition, a need exists to understand the current knowledge and practice in an effort to build specific plans and programs to enhance these concepts and practices as needed. Therefore, our study covered 6 distinct locations out of 13 regions in the KSA and featured a decent sample size. On the other hand, this study shed light on the importance of applying Saudi Central Board for Accreditation of Healthcare Institutions (CBAHI) standards for reducing medication errors at health care facilities in Saudi Arabia. The CBAHI is the official agency authorized to grant accreditation certificates to all governmental and private health care facilities operating today in Saudi Arabia. The CBAHI emerged from the Saudi Health Council as a nonprofit organization. The principal function of the CBAHI is to establish the health care quality and patient safety standards against which all health care facilities are evaluated for evidence of compliance. In this study, our main objective was to evaluate healthcare professionals’ knowledge about medication errors, medication error reporting systems, and predictors for HCPs to report medication errors in several hospitals from various regions in the KSA.
Materials and Methods
Study Setting
The study was conducted in 6 distinct locations—in the regions of Hail, Al-Qassim, Al-Jouf, Al-Madinah, the eastern region, and the western region—between January and March of 2020. The study included 16 tertiary care governmental hospitals. Moreover, teaching and specialist hospitals, which provide highly specialized medical services, were included in this study. Different regions and types of hospitals in the KSA were used to generate more precise results reflecting the various standards of health care services among regions and hospitals. This study received approval from the Institutional Review Board (IRB; project log number: IRB 2020-2) at the General Directorate of Hail Health Affairs, Hail Region, KSA.
Study Design and Population
This study featured an observational cross-sectional study design involving physicians, pharmacists, and nurses, and it was conducted in hospital settings. The questionnaire was adapted from a published study assessing the knowledge, attitudes, and practices of HCPs regarding medication error reporting in Riyadh, KSA.1 The questionnaire was designed in English because the study participants is HCPs. For research validation purposes, a research team with extensive experience with such studies assessed the questionnaire. In addition, 5 healthcare practitioners and clinicians who also have research experience, to assess content validity. Based on results, the questionnaire was slightly modified, and these modifications were in the English language. Afterward, a pilot testing technique was conducted among 13 experienced HCPs with both clinical and research backgrounds to assess the face validity. In addition, the Cronbach-alpha reliability test (0.82) was performed based on the results obtained, which indicated good internal consistency. The data collected in a pilot study was excluded from the final results. The questionnaire comprised of 37 close-ended questions, and the participants’ responses were recorded on a five-point Likert scale ranging from “strongly disagree” to “strongly agree.” Furthermore, four sections were used in the validated questionnaire. The first section contained questions related to the demographic characteristics of the HCPs, including hospital setting, health profession, age, gender, nationality, education level, and years of work experience. In the second section were questions about their knowledge about medication errors and medication error reporting systems. Their attitudes regarding medication errors and reporting systems were assessed in the third section through several questions. In the final section, questions about practices related to medication error reporting systems were discussed (see Additional File 1).
Data Collections
Self-administered questionnaires were used to assess the knowledge, attitude, and practice of HCPs regarding medication errors and medication errors reporting system. The questionnaire was hand distributed to HCPs at each hospital in the Hail region within 10 days. Completing the questionnaire and participation in the study were voluntary. However, the HCPs consented to participate after they were given full details about the study and its intended purpose. In addition, for the purpose of ensuring complete questionnaires for HCPs who consented to participate and received the questionnaires, the data collection process included conducting face-to-face interviews. In regions such as Al-Qassim, Al-Jouf, Al-Madinah, the eastern region, and the western region, 5 trained research team members who were full-time employees at their hospitals completed the data collection process. The data collectors explained the study and its aims to each HCP, then informed the HCPs that participation was voluntary. Afterward, we received the questionnaires from our trained research team members through the Saudi Post within a time period of 5 to 10 days. The completion and returning of questionnaires were viewed as providing consent to participate.
Power Calculation
The sample size for our study was calculated using an alpha of 5%, an estimation of absolute error of 5%, and a 95% confidence level. Furthermore, data from a previous study that was conducted under similar settings found that 44.8% had not reported medication errors during their work experiences.1 The aforementioned information was used to calculate our study sample size, which yielded a minimum recommended sample size of 380 participants. We considered a risk of attrition (ie, to consider non-respondents); therefore, the attrition rate was 20%. The total required number of participants considered in our sample size was 456. This was the minimum number of participants needed to have enough power to investigate our research question, and we had more than this number. We tried to make it representative by conducting the study in different geographical areas.
Statistical Analyses
The data were entered and coded, descriptive statistics analyses (frequencies and percentages) were conducted using Statistical Package for the Social Sciences (SPSS v. 22) for all survey items. Furthermore, inferential analyses were also conducted to assess the relationships among various independent variables in the study outcome. The dependent variable was the status of reporting medication errors, and it was dichotomous (ie, reporting or not reporting). The relationship between the dependent variable and the independent variables was determined through bivariate analysis, such as the chi-square test. The independent variables that were statistically significant and that were associated with the dependent variable were entered into the logistic regression to determine the predictors for HCPs to report medication errors. Phi and Cramer’s test was used to determine the relationship between training programs and the number of medication errors that HCPs reported. A p-value less than 0.05 was considered to be statistically significant different in all analyses.
Results
Demographic Data
Various HCPs participated in this study, including 348 (35.5%) physicians, 144 (14.7%) pharmacists, and 488 (49.8%) nurses. These HCPs were from 16 government Saudi hospitals from various regions from all over the country. These regions include Hail, Al-Qassim, Al-Jouf, Al-Madinah, and the eastern and western regions. A large proportion 593 (60.5%) of the participants were female, with half of the HCPs being younger than 35 years of age, and with 350 (35.7%) being 35 to 45 years old. Furthermore, more than half 526 (53.7%) of the participants had been in practice for 5–15 years, and 522 (53.3%) of the HCPs have bachelor’s degrees. Table 1 describes the demographic characteristics of the HCPs, including health profession, nationality, gender, age group, work experience in specialty, and education level.
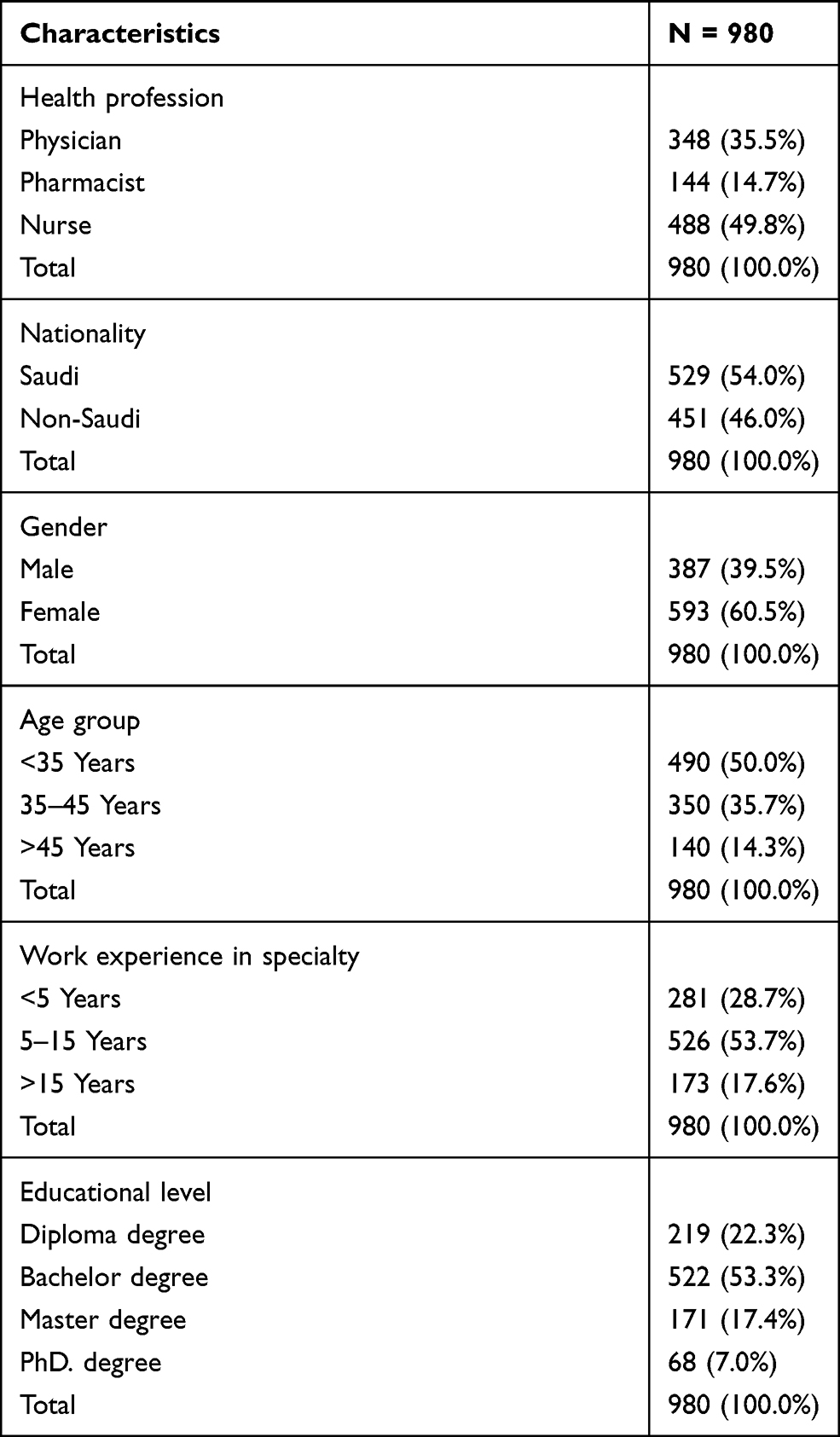 |
Table 1 Demographic Characteristics of Participating Health Care Professionals |
Knowledge and Attitude of Medication Error Reporting
The majority 860 (87.8%) of the HCPs reported having an adequate knowledge of medication errors and reporting forms. Of these HCPs, pharmacists made up the highest percentage with a count of 139 (96.5%), followed by 438 (89.8%) nurses and 283 (81.3%) physicians. The differences between the HCPs and knowledge about medication error reporting forms were statistically significant (p = 0.003). The graphical representation of the various HCPs’ knowledge about medication error reporting in hospitals is shown in Figure 1.
 |
Figure 1 Knowledge of medication errors reporting system among HCPs. |
Regarding HCPs’ knowledge about the main objective of a medication error reporting system, 37 (3.8%) said it is used to calculate the incidence of medication errors in hospitals. Approximately 753 (76.8%) of the HCPs were aware of medication error reporting as a requirement for their institutions’ reliability. Only 277 (28.3%) of the HCPs had favorable amounts of knowledge of the stages of medication errors.
HCPs’ attitudes regarding medication error reporting are shown in Table 2. A good number of the HCPs 719 (73.4%) agreed that their information would be confidential if they reported medication errors. More than half of the participants 627 (63.9%) acknowledged that it is their responsibility to report medication errors, even if someone else causes them. As for education, 434 (44.3%) of the HCPs would have preferred to educate those who made medication errors, rather than reporting them. Only 511 (52.1%) of the HCPs reported that they would not hesitate to reporting medication errors, and a considerably high number of HCPs 284 (29%) feared being blamed if they reported the medication errors they had made.
 |
Table 2 Attitudes of Healthcare Professionals Toward Medication Errors Reporting |
Interestingly, approximately 102 (10.4%) of the HCPs said they believe that the pharmacist is solely responsible for the reporting of medication errors as shown in Figure 2. In addition, to foster an understanding of HCPs’ behavior toward medication error reporting, the participants were asked what kinds of medication errors should be reported. Only 103 (10.5%) of the HCPs mentioned that they would report medication errors that led to patient deaths (Table 3). Ninety percent of the HCPs would report the wrong dose of a drug as a medication error, but 178 (18.2%) would not report the wrong duration of a drug as a medication error. The participants were asked whether they would consider reporting near-misses as medication errors. The results showed that 786 (80.2%) said yes. However, only 616 (62.9%) would report near-misses. As for the remaining HCPs, 364 (37.1%) said they would not consider near-misses to be medication errors and thus would not report them.
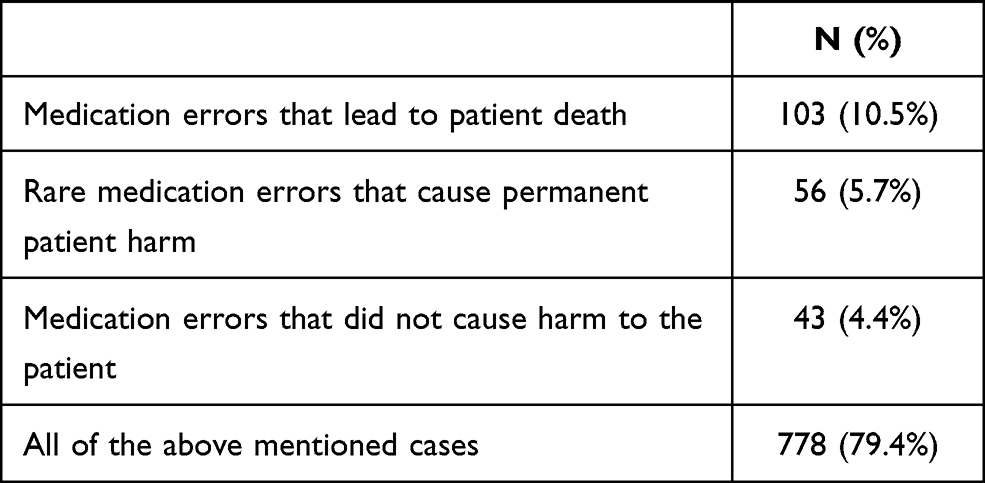 |
Table 3 Kinds of Medication Errors Should Be Reported by Participating HCPs |
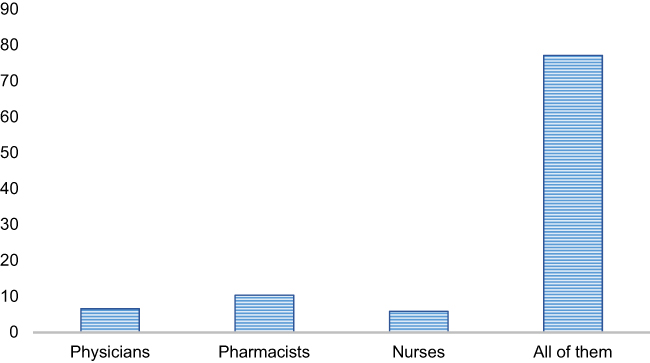 |
Figure 2 Responsibility for filling out of medication errors reporting among HCPs. |
The Difference Between HCPs’ Characteristics and Knowledge About the Stages of Medication Errors
Some of the participants’ characteristics were statistically tested against knowledge about the stages of medication errors. Pearson chi-square testing indicated that statistically significant differences exist among health profession (p = 0.004), age group (p = 0.001) educational level (p = 0.008), and a clear knowledge about the stages of medication errors. However, the differences among gender (p = 0.467), work experience in a specialty (p = 0.322), and knowledge about the stages of medication errors were not statistically significant.
Regarding the best category among the demographic characteristics of HCPs for knowledge about the stages of medication errors, pharmacists made up the best category among the health professions with a count of 58 (40.3%), followed by 150 (30.7%) nurses and 69 (19.8%) physicians. Among the age groups, the HCPs who were less than 35 years old made up the best category with a count of 169 (34.5%), followed by 79 (22.6%) in the age range of 35–45 years and 29 (20.7%) older than 45 years. Of these participants, HCPs who hold diplomas were in the best category with a count of 75 (34.2%), followed by 153 (29.3%) with bachelor’s degrees, 18 (26.5%) with PhD degrees, and 31 (18.1%) with master’s degrees.
Practice of Medication Error Reporting
Around 136 (13.9%) of the HCPs mentioned that they encounter medication errors daily (Figure 3). Approximately 404 (41.2%) of the HCPs reported medication errors at their institutions. Of these HCPs, 140 (34.7%) claimed that the procedure of medication error reporting is somewhat complicated, 127 (31.4%) said it is easy and fast, 77 (19.1%) said it is complicated and lengthy, and 60 (14.8%) said it is somewhat easy.
 |
Figure 3 Incidence of medication errors at hospitals. |
However, a high proportion of the HCPs 576 (58.8%) do not report any medication errors at their workplaces. The participating HCPs mentioned several factors and barriers, including legal implications, which made up the highest percentage. A total of 369 (37.7%) mentioned legal implications, 273 (27.9%) expressed being worried about conflict with others, 231 (23.6%) expressed having no time because they are busy, and 107 (10.8%) mentioned being worried about having impaired reputations. Nevertheless, 442 (45.1%) of the HCPs perceive that the levels of their efforts to prevent medication errors are somewhat effective. Around 366 (37.3%) of the HCPs believe that look-alike and sound-alike (LASA) medication problems are the main reasons for/contributing factors to medication errors in their hospitals, and almost half 459 (46.8%) of the HCPs agree that high-alert medication errors have been reduced due to applying CBAHI standards in their hospitals (Table 4).
 |
Table 4 Practices of Healthcare Professionals Toward Medication Errors Reporting System |
Unfortunately, more than half 524 (53.5%) of the HCPs do not use or have electronic systems for reporting medication errors at their institutions. An alarming number 537 (54.8%) of the HCPs had not attended any training programs regarding medication error reporting systems within the past 24 months. Furthermore, only 293 (30%) of the HCPs believe that training programs regarding medication error reporting should be held annually.
Table 5 shows the results of the multivariable logistic regression analyses. HCPs’ belief that medication error reports are an important patient safety topic (odds ratio (OR) = 2.260, 95% confidence interval (CI) = 1.254–4.075) was a predictor for the HCPs to report medication errors at their institutions. However, their awareness of their institutions’ reliability in filling out medication error report forms (OR = 0.494, 95% CI = 0.356–0.686) was a negative predictor for reporting medication errors. In addition, the presence of CBAHI standards and recommendations regarding a medication error reporting system (OR = 0.772, 95% CI = 0.559–1.067) was also a negative predictor for the HCPs to report medication errors at their institutions, but it was not statistically significant.
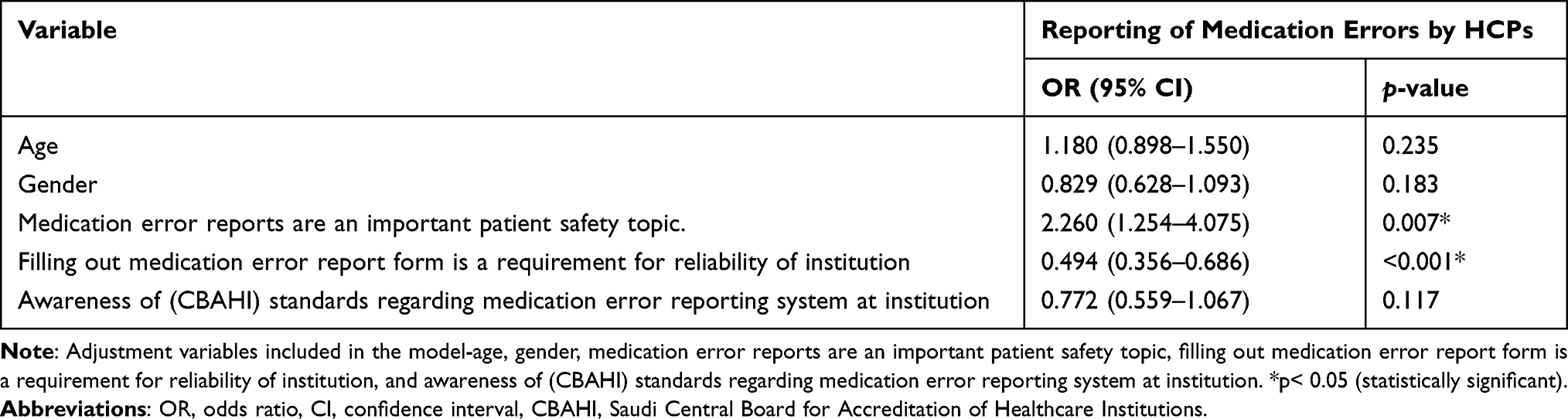 |
Table 5 Multivariable Logistic Regression Analysis Identifying Predictors for Medication Errors Reporting Among the Participating HCPs |
The Relationship Between Training Programs and Number of Medication Error Reports by HCPs
A direct and proportional relationship appears to exist between training programs and the number of medication error reports. The Pearson correlation analyses showed a statistically significant relationship (r = 0.23), (p < 0.001), which was further confirmed through the Phi and Cramer’s test.
Discussion
Medication errors pose a real threat to patient safety. Nearly 6–15% of hospital admissions are due to medication-related problems.20 The reason for this is that we still face some challenges in Saudi Arabia regarding these errors, including the use of handwritten prescriptions and a lack of awareness about medication error reporting systems.4,10 Reducing these errors is one of the main roles of HCPs that will have a positive impact on patient safety.21,22 Therefore, the study was aimed at evaluating the knowledge, attitudes, and practices of healthcare professionals toward medication errors, medication error reporting systems, and predictors for HCPs to report medication errors. In this study, the response rate (100%) was higher compared with previous studies by Salma et al (73%) and Abdel-Latif et al (64.6%). We believe that we achieved this high response rate due to the methods we used for collecting the data. The study also reflected an issue of concern to the HCPs, which may have encouraged them to participate.
Half of the study participants were younger than 35 years old, which is similar to studies conducted in other countries.19,23 We are witnessing the presence of an enthusiastic young generation in the Saudi work environment in large numbers, especially in the health field, within only 4 years since the launch of Saudi Vision 2030.24 In addition, women made up the largest number of participants in this study, which might be due to the type of population found in Saudi Arabia. Most members of the Saudi population are female, and this is common with other studies as well.1,4,19 Furthermore, this study demonstrated the adequate knowledge possessed by HCPs who have between 5 and 15 years of experience with reporting medication errors. This is in contrast to a study conducted by Salma et al, who found that those with less than 5 years of experience also possess this knowledge. This may be attributed to the courses they take related to patient safety or drug safety. This has a positive effect in raising the level of knowledge and the rate of reporting medication errors regardless of years of experience.1
Achieving the safe use of medicine, calculating the incidence of medication errors, and identifying factors that cause medication errors were the main driving factors for HCPs to report medication errors. More than half of the HCPs said they believe that the pharmacists have an important role in reducing medication errors, and this is consistent with a study conducted in the Netherlands.25 In fact, this finding is not surprising, as pharmacists have a unique role in providing health care. They possess more expert knowledge about medications compared with other HCPs, and they use their clinical experience along with their practical knowledge to provide the best advice on the medication use process.
The occurrence of medication errors was related to many causes. About 69.4% of the HCPs said they believe that LASA is a contributing factor to medication errors at their institutions, and this is consistent with a study conducted in Malaysia.26 In July 2015, the United States Food and Drug Administration issued a notification alert regarding LASA errors in two drugs. The medicines of concern were the antidepressant Brintellix® (vortioxetine) and the antiplatelet Brilinta® (ticagrelor). This error was due to brand name confusion resulting in both prescribing and dispensing errors.27 Given that tens of thousands of medications are on the market today, the likelihood of making these errors is really high. However, some strategies contribute to reducing these errors, such as having a list of LASA medications in all storage areas and ensuring that LASA medications are stored separately. Also, tall man lettering practices help with distinguishing LASA drugs from one another to prevent medication errors. Nonetheless, in a study conducted in the United Arab Emirates, researchers found that environmental factors, such as other noises in the hospital ward, are considered to be causes of medication errors.28
Medication errors have a major impact on patient safety. These errors occur at any stages of medication use.29 The errors that occur in the prescribing and administration stages represent the largest percentage among the stages.4 Therefore, we assessed HCPs’ knowledge about the medication error stages of prescribing, transcription, dispensing, administration, monitoring, patient education, independent double-checking, and clinical verification. Only 28.3% of the HCPs had a good understanding of the stages of medication errors, such as prescribing, transcription, dispensing, administration, and monitoring. In fact, this might be due to the fact that medical colleges do not provide enough detailed information on medication safety and medication errors. In addition, HCPs do not continue their education following graduation or working.
Our finding showed that 79% of the HCPs believe that all medication errors should be reported whether this leads to death or permanent harm, and even if an error did not cause harm to the patient. This finding illustrates that HCPs have very positive attitudes toward medication error reporting, regardless of the error state. However, in this study, 10.5% of the HCPs mentioned that they would report only those medication errors that led to patient deaths, which is likely due to the perception that common errors are inevitable, are acceptable, and do not cause much harm. Hence, they do not need to be reported. Only serious and unusual errors that potentially jeopardize lives must be reported.
Furthermore, 80.2% of the HCPs said they consider near-misses to be medication errors, and 37.1% of them would not report about them. This finding is in agreement with a study by Alsulami et al.1 This might be due to HCPs’ lack of knowledge about what needs to be reported. On the contrary, in studies conducted in Malaysia and Australia, it was shown that the severity of the error is the main factor in reporting medication errors.30,31
Lesar et al32 mentioned that errors can result from wrong medication, wrong dose, wrong strength, wrong frequency, incorrect route of administration, and inadequate instruction regarding the use of medications. However, in this study, the wrong dose was one of the most common types of errors that HCPs preferred to report, rather than the wrong duration of a medication. This is due to the fact that a wrong dose is a common occurrence compared with other medication error categories. Previous studies confirmed this.33,34
In our study, among the 980 HCPs, only 41.2% of the HCPs report medication errors, which is consistent with a study conducted in Al-Madinah Al-Munwwarah. This low number of medication errors being reported might be due to a lack of knowledge about medication errors, a lack of familiarity with reporting systems, or a fear of reporting errors.4 Pharmacists displayed more knowledge about the reporting of medication errors in our study, and this is consistent with a study conducted in the Philippines.19 Conversely, nurses showed better medication error reporting practices compared with other healthcare professionals in a study by Salma et al Knowledge, attitudes, and practices are interrelated but may not always be mutual.
In the analysis of the factors discouraging HCPs from reporting medication errors, it was shown that HCPs are concerned about the legal implications (37.7%), that they are worried about conflict with colleagues (27.9%), that they do not have time because they are busy (23.6%), and that they are afraid of having impaired reputations (10.8%). Losing credibility as a professional was a factor that prevented HCPs from reporting medication errors in a Philippines study,19 whereas in a study conducted in Iran, researchers found that inadequate managerial feedback is a main reason for not reporting.35 A lack of medical staff and a high workload were among the reasons contributing to the underreporting of these errors in a study conducted in Riyadh and Pakistan.36,37 In addition, 20% of the HCPs feared being blamed if they reported the medication errors they had made. This is consistent with a study by Teoh et al, who found that the participants did not believe that a high workload was a barrier to reporting; rather, a fear of blaming was the reason for the underreporting of medication errors.23 On the other hand, 44.3% of the HCPs prefer to educate those who have made medication errors, instead of reporting them, and this consistent with a study by Salma et al Based on this finding, it is necessary to raise awareness among HCPs through courses that provide education on medication errors. However, 45.1% of the HCPs consider themselves to be somewhat effective in reporting medication errors.
The reasons contributing to the low level of reporting in our study are that 53.5% of the HCPs do not use or have electronic systems for reporting medication errors at their institutions, and they said they perceive the reporting form to be complex (53.8%). The lack of an electronic reporting system at the HCP’s institution contributed to the issue of underreporting, along with the complexity of reporting procedures. Therefore, the presence of such systems may help to facilitate and speed up the reporting process, thus decreasing the amount of time that HCPs spend on reporting, in addition to increasing health care accuracy. However, barriers to implementing these systems may include the high initial cost and the time required for HCPs to train on and adapt to these systems. The unsuccessful implementation of these systems may lead to the reluctance of HCPs to report medication errors.
In addition, more than half of the HCPs had not received any training on reporting medication errors during the past 24 months. This might be due to a lack of educational programs related to medication safety, as well as a lack of support for education and training from their institutions. In addition, HCPs may not have enough time to be involved in training programs due to the workloads at their institutions. Educational and training programs on reporting medication errors should be established to encourage HCPs to report; this is in agreement with another study as well.30 The training presents a prime opportunity to expand the knowledge base of all HCPs and to give them a greater understanding of their responsibilities with regard to medication error reporting. An increased awareness of medication error reporting will help to ensure the safety of the hospital environment, which, in turn, will improve patients’ quality of life.
As patient safety is one of the most important priorities of the health system, the principal function of the CBAHI is to establish the health care quality and patient safety standards against which all health care facilities will be evaluated for evidence of compliance. In addition, the Saudi Patient Safety Center was recently established. It is one of the initiatives of the National Health Transformation Program to improve health care safety and reduce medication errors. Accordingly, we found that the HCPs agree on the importance of reporting medication errors as a requirement for their institutions to be reliable, and they believe that errors related to high alert medications were reduced according to CBAHI standards. Therefore, most of the HCPs believe that they have a professional obligation and a moral responsibility to report medication errors, but they prefer for the information they disclose to be confidential.
A strength of our study is that the study participants were from 6 distinct regions and from a quite high number of hospitals (16 hospitals) in the KSA, and we had a decent sample size. Our study findings shed light on HCPs’ knowledge, attitudes, and practices regarding medication errors and reporting practices. However, a limitation of the study is that the number of participants is relatively uneven among the participating HCPs, as pharmacists represent a small number of the HCPs participating in this study. Also, the study may be prone to recall bias issues due to its nature as a cross-sectional study. In addition, the fact the study covered 6 distinct regions may not be enough to generalize the results to all Saudi Arabian regions.
Recommendations
Our study revealed the need for several interventions to improve the culture of addressing medication errors in Saudi Arabia. The practice of medication error underreporting remains a challenging issue. Therefore, promoting the regular education and training of HCPs is a very important step toward improving the safety and quality of patients’ lives. This could be done by continuously offering seminars and workshops that provide education on medication errors in medical and residency programs. In addition, mandatory training for new HCP employees in hospitals could be implemented.
A higher authority at each institution should also encourage participation in symposiums on patient safety and drug safety. In addition, and based on the study results, the need exists to launch “No Blame, No Punishment” campaigns in hospitals and other health institutions to enhance medication error reporting. Adopting the concept of a medication safety officer whose duties involve medication safety only is necessary as well. The inclusion of pharmacovigilance in the curricula of health colleges at universities is also critical.
Conclusion
Our findings demonstrate a lack of the reporting of medication errors in Saudi Arabia, as well as a lack of education and training on medication errors. These are major issues that should have been addressed up to now to avoid endangering patients. A lack of knowledge about medication error stages among the study participants is a concern that the higher authorities at health institutions in Saudi Arabia need to aggressively address moving forward.
Abbreviations
HCPs, healthcare professionals; LASA, look-alike and sound-alike; CBAHI, Saudi Central Board for Accreditation of Healthcare Institutions; CPOE, computerized physician order entry; IRB, Institutional Review Board; SPSS v.22, Statistical Package for the Social Sciences version 22.
Data Sharing Statement
Data collected were kept in a secure setting, available only to the corresponding author. Moreover, all data and materials are available upon reasonable request.
Ethics Approval and Participants Informed Consent
The study received an ethical approval from the Institutional Review Board (project log number: IRB 2020-2) at the General Directorate of Hail Health Affairs, Hail Region, KSA. The ethics committee at the General Directorate of Hail Health review all protocols to meet all internationals and nationals standards including the Declaration of Helsinki; therefore, the study was conducted in accordance with Declaration of Helsinki. Verbal informed consent was approved by the IRB (project log number: IRB 2020-2) at the General Directorate of Hail Health Affairs, Hail Region, KSA. All the study participants were informed about the study and the purpose of the study at the time of questionnaires’ distribution and the filling of the questionnaire was a voluntary process.
Acknowledgments
The authors would like to thank the General Directorate of Hail Health Affairs for supporting this research, and all healthcare professionals who participated in the study. The authors are grateful to all colleagues from different regions working at Ministry of Health (Sanaa Alshammari, Samirah Aljuhani, Moudi Alazami, Roqiah Aljulasi and Abdullah Alhadayan) for their efforts and time during the data collection process.
Author Contributions
TMA started the conception of the study. TMA and AKA played a role in designing the study and methods. FMA, EJA, AMA and AKA participated in the manuscript content. FMA and TMA have analyzed and interpreted the data. TMA worked on supervising manuscript writing. FMA critically reviewed the manuscript. All authors read and approved the final manuscript. All authors made a substantial contribution to the conception, study design, acquisition of data or analysis and interpretation of data; took part in drafting the article or revising it for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for- profit sectors.
Disclosure
The authors declare that they have no competing interests.
References
1. Alsulami SL, Sardidi HO, Almuzaini RS, et al. Knowledge, attitude and practice on medication error reporting among health practitioners in a tertiary care setting in Saudi Arabia. Saudi Med J. 2019;40(3):246. doi:10.15537/smj.2019.3.23960
2. Aljadhey H, Alhusan A, Alburikan K, Adam M, Murray MD, Bates DW. Medication safety practices in hospitals: a national survey in Saudi Arabia. Saudi Pharm J. 2013;21(2):159–164. doi:10.1016/j.jsps.2012.07.005
3. Donaldson LJ, Kelley ET, Dhingra-Kumar N, Kieny M-P, Sheikh A. Medication without harm: WHO’s third global patient safety challenge. Lancet. 2017;389(10080):1680–1681. doi:10.1016/S0140-6736(17)31047-4
4. Abdel-Latif MM. Knowledge of healthcare professionals about medication errors in hospitals. JBCP. 2016;7(3):87. doi:10.4103/0976-0105.183264
5. Abdel-Latif MM, Abdel-Wahab BA. Knowledge and awareness of adverse drug reactions and pharmacovigilance practices among healthcare professionals in Al-Madinah Al-Munawwarah, Kingdom of Saudi Arabia. Saudi Pharm J. 2015;23(2):154–161. doi:10.1016/j.jsps.2014.07.005
6. Sheikh D, Mateti UV, Kabekkodu S, Sanal T. Assessment of medication errors and adherence to WHO prescription writing guidelines in a tertiary care hospital. Fut J Pharm Pharm Sci. 2017;3(1):60–64. doi:10.1016/j.fjps.2017.03.001
7. Ranchon F, Salles G, Späth H-M, et al. Chemotherapeutic errors in hospitalised cancer patients: attributable damage and extra costs. BMC Cancer. 2011;11(1):478. doi:10.1186/1471-2407-11-478
8. Al-Zaagi IA, Al-Dossari DS, Salem SO, Qureshi NA. Medication safety unit programs in King Saud Medical City, 2012–2013: safe medication management and use with a focus on patient safety. J Adv Med Med Res. 2015;8(5):384–407. doi:10.9734/BJMMR/2015/17221
9. Shimada Y, Fujimoto M, Nogami T, et al. Patient safety incident reports related to traditional Japanese Kampo medicines: medication errors and adverse drug events in a university hospital for a ten-year period. BMC Complement Altern Med. 2017;17(1):547. doi:10.1186/s12906-017-2051-2
10. Altebainawi A, Aljofan M, Alrashidi MN, Alshammari TM. Completeness of medication prescriptions: prescription errors study in Hail region, Saudi Arabia (PeSHR). Pharmacoepidemiol Drug Saf. 2019.
11. Khoja T, Neyaz Y, Quresh N, Mogzoub M, Haycox A, Walley T. Medication errors in primary care in Riyadh city, Saudi Arabia. East Mediterr Health J.2011;17(2):156–159.
12. Morrison M, Cope V, Murray M. The underreporting of medication errors: a retrospective and comparative root cause analysis in an acute mental health unit over a 3‐year period. Int J Ment Health Nurs. 2018;27(6):1719–1728. doi:10.1111/inm.12475
13. Yung HP, Yu S, Chu C, Hou IC, Tang FI. Nurses’ attitudes and perceived barriers to the reporting of medication administration errors. J Nurs Manag. 2016;24(5):580–588. doi:10.1111/jonm.12360
14. Vincent C Incident reporting and patient safety. British Medical Journal Publishing Group; 2007.
15. Alsafi E, Baharoon S, Ahmed A, Al Jahdali H, Al Zahrani S, Al Sayyari A. Physicians’ knowledge and practice towards medical error reporting: a cross-sectional hospital-based study in Saudi Arabia. East Mediterr Health J. 2015;21(9):655–664. doi:10.26719/2015.21.9.655
16. Shulman R, Singer M, Goldstone J, Bellingan G. Medication errors: a prospective cohort study of hand-written and computerised physician order entry in the intensive care unit. Crit Care. 2005;9(5):R516. doi:10.1186/cc3793
17. Rishoej RM, Almarsdóttir AB, Thybo Christesen H, Hallas J, Juel Kjeldsen L. Identifying and assessing potential harm of medication errors and potentially unsafe medication practices in paediatric hospital settings: a field study. Ther Adv Drug Saf. 2018;9(9):509–522. doi:10.1177/2042098618781521
18. Bates DW, Leape LL, Cullen DJ, et al. Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. JAMA. 1998;280(15):1311–1316. doi:10.1001/jama.280.15.1311
19. Carandang R, Resuello D, Hocson G, Respicio K, Reynoso C. Knowledge, attitude and practices on medication error reporting among health practitioners from Hospitals in Manila. Sch Acad J Pharm. 2015;4:293–300.
20. Jose J, Rao PG. Pattern of adverse drug reactions notified by spontaneous reporting in an Indian tertiary care teaching hospital. Pharmacol Res. 2006;54(3):226–233. doi:10.1016/j.phrs.2006.05.003
21. Mrayyan MT, Shishani K, Al‐faouri I. Rate, causes and reporting of medication errors in Jordan: nurses’ perspectives. J Nurs Manag. 2007;15(6):659–670. doi:10.1111/j.1365-2834.2007.00724.x
22. Vazin A, Delfani S. Medication errors in an internal intensive care unit of a large teaching hospital: a direct observation study. Acta Med Iran. 2012;50(6):425–432.
23. Teoh B, Alrasheedy A, Hassali M, Tew M, Samsudin M. Perceptions of doctors and pharmacists towards medication error reporting and prevention in Kedah, Malaysia: a Rasch model analysis. Adv Pharmacoepidemiol Drug Saf. 2015;4(192):1052–2167.
24. Vision 2030 Overview - Vision 2030 [internet]. Available from: https://www.vision2030.gov.sa/v2030/overview/. Accessed May 17, 2021.
25. Buurma H, De Smet PA, Leufkens HG, Egberts AC. Evaluation of the clinical value of pharmacists’ modifications of prescription errors. Br J Clin Pharmacol. 2004;58(5):503–511. doi:10.1111/j.1365-2125.2004.02181.x
26. Ludin SM, Ariffin SM, Ilias NA. Nurse perception on medication error in intensive care unit. J Med Biomed App Sci. 2019;7(7):267–271.
27. Lizano-Díez I, Figueiredo-Escribá C, Piñero-López MÁ, Lastra CF, Mariño EL, Modamio P. Prevention strategies to identify LASA errors: building and sustaining a culture of patient safety. BMC Health Serv Res. 2020;20(1):1–5. doi:10.1186/s12913-020-4922-3
28. Johnson J, Thomas M. Medication errors: knowledge and attitude of nurses in Ajman. UAE Gulf Med J. 2012;1(S1):143–147.
29. Elden NMK, Ismail A. The importance of medication errors reporting in improving the quality of clinical care services. Glob J Health Sci. 2016;8(8):243. doi:10.5539/gjhs.v8n8p243
30. Samsiah A, Othman N, Jamshed S, Hassali MA. Perceptions and attitudes towards medication error reporting in primary care clinics: a qualitative study in Malaysia. PLoS One. 2016;11(12):e0166114. doi:10.1371/journal.pone.0166114
31. Evans SM, Berry JG, Smith BJ, et al. Attitudes and barriers to incident reporting: a collaborative hospital study. BMJ Qual Saf. 2006;15(1):39–43. doi:10.1136/qshc.2004.012559
32. Lesar TS, Briceland L, Stein DS. Factors related to errors in medication prescribing. JAMA. 1997;277(4):312–317. doi:10.1001/jama.1997.03540280050033
33. Björkstén KS, Bergqvist M, Andersén-Karlsson E, Benson L, Ulfvarson J. Medication errors as malpractice-a qualitative content analysis of 585 medication errors by nurses in Sweden. BMC Health Serv Res. 2016;16(1):431. doi:10.1186/s12913-016-1695-9
34. Pham JC, Story JL, Hicks RW, et al. National study on the frequency, types, causes, and consequences of voluntarily reported emergency department medication errors. J Emerg Med. 2011;40(5):485–492. doi:10.1016/j.jemermed.2008.02.059
35. Amrollahi M, Khanjani N, Raadabadi M, Hosseinabadi M, Mostafaee M, Samaei S. Nurses’ perspectives on the reasons behind medication errors and the barriers to error reporting. Nurs Midwifery J. 2017;6(3):132–136. doi:10.4103/nms.nms_31_17
36. Alshaikh M, Mayet A, Aljadhey H. Medication error reporting in a university teaching hospital in Saudi Arabia. J Patient Saf. 2013;9(3):145–149. doi:10.1097/PTS.0b013e3182845044
37. Shahzadi S, Afzal MM, Kousar R, Waqas MA. Barriers to Reporting Medication Administration Errors among Nurses in Services Hospital Lahore. Saudi J Med Pharm Sci. Published online 2017. doi:10.21276/sjmps.2017.3.9.2.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.