")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 9
Medical student perspective: reducing patient waiting times in the UK National Health Service
Authors Vink J, Oyewole F, Jamshaid S, Patel R, Froogh Z, Bhambra M
Received 23 February 2016
Accepted for publication 24 February 2016
Published 2 May 2016 Volume 2016:9 Pages 207—209
DOI https://doi.org/10.2147/JMDH.S106958
Checked for plagiarism Yes
Editor who approved publication: Dr Scott Fraser
Jasper Vink, Folashade Oyewole, Shiraz Jamshaid, Rohin Patel, Zubair Froogh, Maninder Bhambra
Faculty of Medicine, Imperial College London, London, UK
We read with great interest the article by Zaghloul and El Enein and agree with the conclusions made in particular regarding overbooking of outpatient services due to a mismatching of resources and the need for efficient outpatient scheduling. We believe these points to be relevant to the current status of the National Health Service (NHS), which is facing an ever growing demand for its services, leading to increasing waiting times as a result. Across NHS England, 838,600 patients were waiting for a key diagnostic test at the end of November 2015, a 5.6% increase from November 2014. Waiting times have been associated with lower patient satisfaction and reduced clinical outcomes. It is therefore crucial that management teams take an active approach to reducing waiting times.
View the original paper by Zaghloul and El Enein
Dear editor
We read with great interest the article by Zaghloul and El Enein and agree with the conclusions made in particular regarding overbooking of outpatient services due to a mismatching of resources and the need for efficient outpatient scheduling.1 We believe these points to be relevant to the current status of the National Health Service (NHS), which is facing an ever growing demand for its services, leading to increasing waiting times as a result.2 Across NHS England, 838,600 patients were waiting for a key diagnostic test at the end of November 2015, a 5.6% increase from November 2014.3 Waiting times have been associated with lower patient satisfaction and reduced clinical outcomes.4,5 It is therefore crucial that management teams take an active approach to reducing waiting times. Figure 1 illustrates a process map through which we have developed strategies for minimization of waiting times by facilitating patient flow.
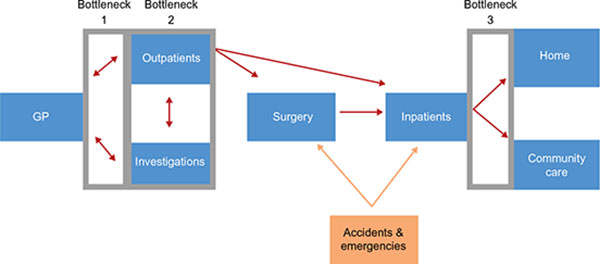 | Figure 1 Process map of patient pathway through NHS trust. |
Strategy
Minimizing unnecessary appointments
The current referral process involves too many steps causing delays in access to consultations with hospital specialists. As highlighted by Zaghloul and El Enein, follow-up appointments contribute significantly to overall outpatient appointments.1 There are 37 million yearly follow-up appointments in the NHS, many of which are deemed clinically unnecessary. Furthermore, there are currently 6 million missed appointments each year where patients have failed to notify the hospital in advance. Ultimately, this wastes valuable resources such as time, labor, and money, which would be better suited to treating others in true need of medical attention.6
These issues can be improved by eliminating steps, which do not create patient value within the referral process, in accordance with lean transformation model.7 Referrals should be direct between hospital departments rather than the traditional path of returning referrals to general practitioners. Furthermore, NHS England found that only 50% of general practitioners use e-referral effectively, despite the system’s ability to reduce the number of DNA appointments by up to 60% when its use is optimized throughout a trust.8 A qualitative analysis should be performed to understand the current barriers to the use of e-referrals among practitioners.9
Optimizing appointment scheduling
Currently, the scheduling of outpatient and investigation appointments is not aligned to the predictable, fluctuating demands of patient care. The national audit office identified that between Friday and Saturday demand for elective and emergency services falls dramatically, with the former dropping more significantly.8 Multiple carve-out queues add inefficiency throughout this process, especially at times of high demand, increasing waiting times for patients.6
Hence, when forecasted emergency admissions are low, strain on the system is relieved; thus, we propose shifting the demand for elective services to these periods.8 Alternatively, transferring capacity within the system may allow meeting overflow demand. This will include adding appointment slots as needed or making infrastructural changes such as outsourcing demand to other departments.10
Reducing delays in transfer of care
Delays in transfer of care create a bottleneck at the end of the patient process pathway, resulting in backlog throughout the entire trust. Data from NHS England have shown that these delays have been increasing consistently, despite one-third of delays having been shown to be avoidable.11 Two clear problems facilitate these delays; absence of a clear protocol in the discharge process and a lack of available, trained staff competent in discharging patients.
Discharging a patient must become a core goal in treatment, and hence the discharge process must be planned as soon as a patient is admitted. Implementing a guideline-based discharge system, specific to various patient pathways, would significantly decrease length of stay.12,13 Diversifying the workforce by multiskilling nurses can speed up the discharge process when doctors are scarce, allowing discharges to proceed more efficiently.14,15 An educational program must be established, with focus on protocol-driven discharge, ensuring a regulated diffusion of responsibility from doctors to nurses.16
Conclusion
There are many factors contributing to the growing waiting times within the NHS. We have identified three key areas that contribute to waiting and have outlined general strategies for their improvement. We agree with Zaghloul and El Enein that each health care system must focus on scheduling of patients as a key method of optimizing resources,1 although we have highlighted further areas to supplement reduction of waiting times. Ultimately, we believe that it is important to focus on all areas simultaneously in order to improve patient flow, as focusing on just one would shift strain on the system to a different area.
Disclosure
The authors report no conflicts of interest in this communication.
References
Zaghloul AAZ, El Enein NYA. Hourly-block and standard patient scheduling systems at two private hospitals in Alexandria. J Multidiscip Healthc. 2010;3:225—232. | ||
Smith P, McKeon A, Blunt I, Edwards N. NHS hospitals under pressure: trends in acute activity up to 2022. London, UK: Nuffield Trust, 2014. Report. | ||
England NHS. NHS diagnostic waiting times and activity data. Leeds, UK: 2015. Report. | ||
Spahos T, Hindmarsh A, Cameron E, et al. Endoscopy waiting times and impact of the two week wait scheme on diagnosis and outcome of upper gastrointestinal cancer. Postgrad Med J. 2005;81(961):728—730. | ||
Bar-dayan Y, Leiba A, Weiss Y, Carroll JS, Benedek P. Waiting time is a major predictor of patient satisfaction in a primary military clinic. Mil Med. 2002;167(10):842—845. | ||
Agency NHSM. 10 high impact changes for service improvement and delivery. London, UK: 2004. Report. | ||
Chadha R, Singh A, Kalra J. Lean and queuing integration for the transformation of health care processes: a lean health care model. Clin Governance. 2012;17(3):191—199. | ||
Comptroller, Auditor G. NHS waiting times for elective care in England. London, UK: National Audit Office, 2014. Report. | ||
Straus SG, Chen AH, Yee H Jr, Kushel MB, Bell DS. Implementation of an electronic referral system for outpatient specialty care. AMIA Annu Symp Proc. 2011;2011:1337—1346. | ||
Cymru A. NHS waiting times for elective care in Wales technical report. Wales Audit Office; 2015 Contract No: Report. | ||
England NHS. Delayed Transfer of Care Time Series. NHS England. Delayed Transfer of Care Time Series. Leeds, UK: 2015. Report. | ||
Nottingham University H. Discharge case study – Nottingham University Hospital NHS Trust. Nottingham, UK: 2014. Report. | ||
Maloney CG, Wolfe D, Gesteland PH, Hales JW, Nkoy FL. A tool for improving patient discharge process and hospital communication practices: the “patient tracker”. AMIA Annu Symp Proc. 2007;2007: | ||
Improvement IfH. Try Scheduling Hospital Discharges. Cambridge, MA: Improvement IfH; 2015. | ||
Crocker C, Keller R. Nurse-led discharge to the ward from high dependency: a service improvement project. Intensive Crit Care Nurs. 2005;21(6):363—366. | ||
Lees L. Making nurse-led discharge work to improve patient care. Nurs Times. 2004;100(37):30—32. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.