Back to Journals » Advances in Medical Education and Practice » Volume 10
Maximizing the acquisition of core communication skills at the start of medical training
Authors Mohiaddin H ![]() , Malik A, Murtagh GM
, Malik A, Murtagh GM ![]()
Received 18 April 2019
Accepted for publication 29 July 2019
Published 27 August 2019 Volume 2019:10 Pages 727—735
DOI https://doi.org/10.2147/AMEP.S212727
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Hasan Mohiaddin,1 Anam Malik,1 Ged M Murtagh2
1Faculty of Medicine, Sir Alexander Fleming Building, South Kensington Campus, Imperial College London, London SW7 2AZ, UK; 2Division of Surgery, Department of Surgery and Cancer, St Mary’s Campus, Imperial College London, London W2 1BL, UK
Correspondence: Hasan Mohiaddin
Faculty of Medicine, Sir Alexander Fleming Building, South Kensington Campus, Imperial College London, London SW7 2AZ, UK
Tel +44 207 589 5111
Email [email protected]
Background: Clinical communication teaching for medical undergraduates may involve real patient contact alongside simulated patient (SP) contact. However, there is still comparatively little known about the experience of learning with real patients and how that may impact on the SP encounter.
Aim: To explore the impact of real patient contact on the experience of communication skills training and SP contact for first-year medical undergraduate students.
Methods: As part of the 6-year MBBS undergraduate medical degree at Imperial College London, students are obliged to undertake communication skills training, which involves teaching with simulated and real patients. In 2017 (toward the end of formal teaching), a small sample of Year 1 medical students, who had taken part in extra-curricular teaching with real patients were recruited for the study to compare their performance with a control group in a SP encounter. The performance of both groups was analyzed alongside follow-up focus group data from a sample of the study group.
Results: Quantitative analysis revealed there was no significant difference in communication skills during a scored SP interview between students with real patient contact and those without. Focus group data, however, revealed valuable insights into the experience of learning with real patients. Students reported a marked increase in their confidence and ability to naturalize their communication skills as a result of real patient contact. Students also reported that skills gained through real patient contact may not always transfer easily to the SP setting.
Conclusion: Real patient contact is an invaluable component of communication training for undergraduate medical students. For successful implementation, there needs to be a clear curricular purpose at pedagogical, practical and organizational levels. Students’ experience of real patient contact can provide an informed foundation upon which to implement other modes of teaching.
Keywords: real patient contact, communication skills training, early years curriculum
Introduction
The General Medical Council describes effective clinical communication as a defining feature of professionalism in clinical practice.1,2 The teaching and examination of clinical communication forms a core part of the curriculum in most UK medical schools.3 Curricular activities involving interaction with patients are critical to ensuring application and integration of professionalism with medical knowledge.
Communication training in medical schools typically involves real patient interaction as well as simulated patient (SP) interaction. Both types of contact are designed to integrate knowledge and skills with professionalism, but they do so in different ways. Interviewing SPs enables students to explore specific issues they may have little or no direct experience of, and to do so within a safe environment.4 The “patient’s experience”, albeit by proxy can provide an invaluable platform for learning, particularly if SPs are trained to give feedback.5–7 Moreover, the SP encounter can encourage creative thinking and reasoning, a vital component of the naturalization of communication skills.8
In contrast, real patient encounters engender direct involvement with patient experience in the exchange between patient and student. Littlewood et al (2005) have shown that early (pre-clinical) exposure to real patients can be a catalyst for students’ clinical skills development and can also improve students’ ability to relate to patients and communicate empathy.9 Nestel and Bentley (2011) suggest that contact with real patients provides students with a deeper appreciation of the psychosocial aspects of illness.7
Both forms of patient contact have their advantages and disadvantages. Whilst interaction with real patients provides a direct line of sight into patient experience, students may lack confidence and therefore be less inclined to approach real patients whilst on their clinical attachments. Real patients themselves may feel compromised and therefore less willing to talk about personal illness issues purely for the purposes of improving a student’s communication skills.7 These issues would seem to strengthen the case for the use of SPs only in communication skill training. However, as a singular mode of training, SP encounters, if used in isolation from the realities of real patient contact, may in fact negatively impact on the effective transfer of communication skills to improved practice.10
On its own, the SP encounter limits exploration of the multifaceted aspects of clinical practice, which demand more in terms of professionalism and communication skills.11 Early exposure to real patient contact, however, has been shown to improve empathic attitudes toward others, self-awareness and even performance in assessments, providing an alternative method to develop clinical communication skills.12 The evidence would seem to suggest that optimum training should consist of an integrated model of SP training alongside real patient contact; however, it is still unclear exactly how this may work to ensure optimal learning particularly in the early years of medical training. This paper reports findings relating to students’ experiences of real patient contact and SP contact, when it comes to the acquisition of communication skills.
Study context
A study was conducted comparing two groups of first-year medical students. In addition to their first-year communication training, the study group experienced repeated real patient contact as part of a volunteer organization at Imperial College called Connect (aiming to reduce isolation of elderly in-patients through interaction with students). The control group received only the formal curriculum teaching on clinical communication which included lectures on clinical communication and a single SP experience. Both groups were compared in their performance during a SP interview at the end of their first year of clinical communication training. The study aimed to assess if real patient contact alongside curriculum teaching advances communication skill development.
Materials and methods
As part of the 6-year MBBS undergraduate medical degree, students are obliged to undertake communication skills training in their first year. Three hundred and sixty students take part and in their first year attend clinical communications lectures, small group teaching and a mix of SP and real patient encounters toward the end of the course. In 2017, 20 first-year medical students, who had self-registered interest in the Connect volunteer organization (a medical society run by Year 5 students to provide access to patients on the wards for early years students) were recruited for the study. Following a safety induction, students visited geriatric wards fortnightly to talk to patients to find out about the patient’s wider context and establish the patient’s perspective on their condition, care and treatment. Each encounter lasted between 10 and 15 minutes for 2 hours each session. These first-year students were supervised by students in years 2, 3 and 5, who guided them through the session and provided informal feedback at the end. The first-year students were exposed to a wide variety of patients, including those with dementia and cognitive impairment. Of these students, all those who attended at least 6 of the 8 volunteering sessions available (the study selection criterion) were included in the study group (n=14). A control group (n=14) was randomly selected from the remainder of the entire first-year cohort who did not register any interest in the volunteer organization (with an inclusion criterion of no previous experience of health care volunteering to isolate the impact of real patient contact vs formal skills training). Both study group and control group were then (quantitively) assessed using a SP interview at the end of their first year of clinical communication training. Those in the volunteer group were also later invited to partake in a focus group, forming the qualitative component of the study data. Ethical approval was gained from Imperial College Medical Education Ethics Committee (Process Number: MEEC1617-20). Students provided written informed consent to participate in the study after reading an information sheet and signing a consent form (Appendices 1 and 2).
Quantitative assessment
As part of their first year of formal communication training, all medical students undertake a 5-minute SP interview toward the end of the first year of training after all other teaching has been completed. This was used as a tool to measure and compare the communication skills of both the study and control group students. The interview required students to gather basic information from an SP, including the patient’s wider context as well as their perspective. Students were assessed on their ability to introduce themselves to the SP, gather basic information (using open questions, actively listening and showing awareness of non-verbal communication), find out about the patient’s ideas, concerns and expectations and close the interview. Whilst the interview took place, a clinical communication tutor and two peer students observed the interview from a teaching room through a video screen. When the interview ended, the student and SP then returned to the teaching room where the student received feedback from their peers, the tutor and the SP.
Video recordings of the SP interviews from both groups were obtained with written informed consent after providing the information sheet (Appendices 1 and 2). Recordings were sent to four clinical communications tutors. Each tutor received seven recorded interviews consisting of a random mix of both study and control group students and were asked to assess the performance of the students to evaluate the effectiveness of the clinical communication program. The tutors were not informed that some of the students had experience of real patient contact. Tutors were only allocated to students whom they had not taught during the year. Each interview was assessed according to a mark scheme devised by GM based on skills that a Year 1 medical student is expected to acquire by the end of their first year (Appendix 3). This mark scheme was validated by senior faculty staff and an external examiner. Scores were compiled on Microsoft Excel and averages between the study group and control were compared statistically using an unpaired two-sided Student’s t-test.
Qualitative assessment
Following the SP interview, the study groups were invited to a 1-hour focus group (with a semi-structured interview schedule – Appendix 4) to discuss their volunteering experience, its potential impact on clinical communication skills and their thoughts on the curriculum teaching they received. This aimed to gather contextual data which may elaborate on the performance data collected. The focus group included eight students only from the original study group (n=14). The focus group took place in March around the same time Year 1 students were involved in formative exams which possibly explains why six of the original study group did not respond to the invite for the focus group. Data from the focus group were transcribed and thematically analyzed (to develop codes and themes) with any discrepancies resolved through discussion by all three authors.
A diagrammatic summary of the study methods is shown in Figure 1.
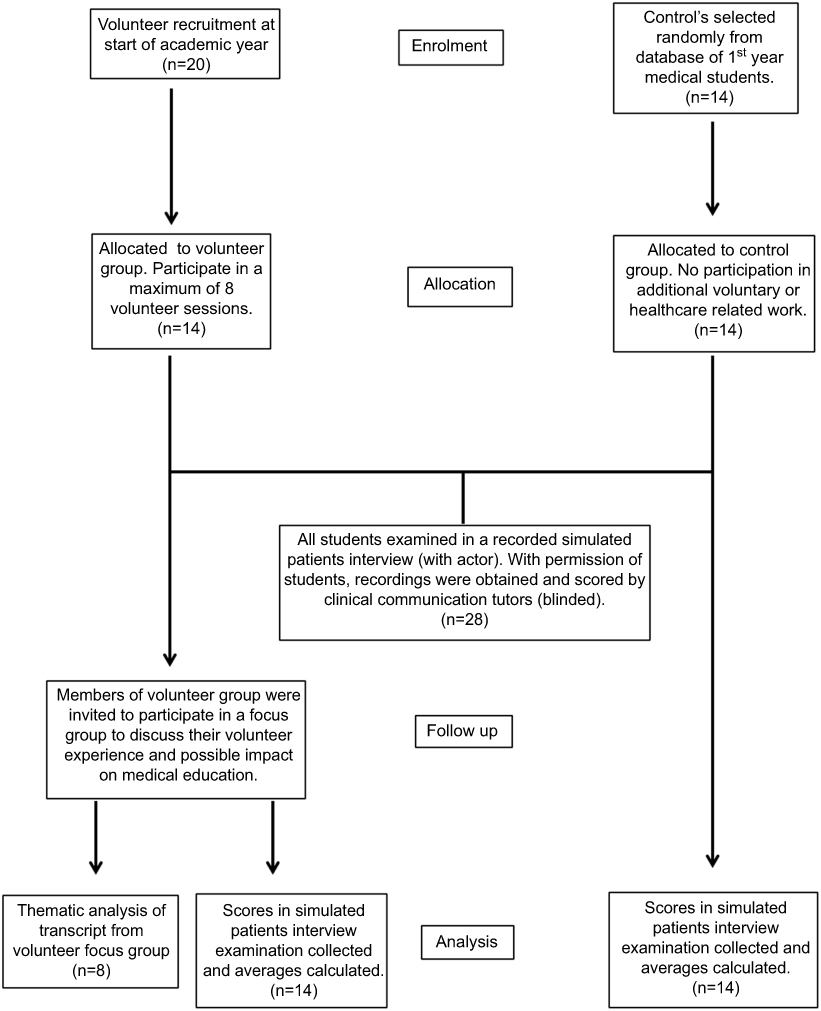 |
Figure 1 Diagrammatic summary of study methods. |
Results
SP interview
Comparing the assessment results of both study group and control group, we aimed to ascertain whether the intervention had reached the highest level of measurable effectiveness (level 4) in the Kirkpatrick model of evaluation.13 Results indicate this did not occur, since there was no significant difference in average scores between the study and control groups. In the study group, students scored an average of 15.1 of 20 compared with an average of 13.9 of 20 in the control group, which was not a statistically significant increase (Student’s t-test p=0.29, Bonferroni corrected p=2.037). A further breakdown of the average scores per mark-scheme subsection between the study and control groups is shown in Table 1. The second part of the study involved a focus group with the study group students to explore in more depth the experiences of the students’ contact with both real and SPs during their first year.
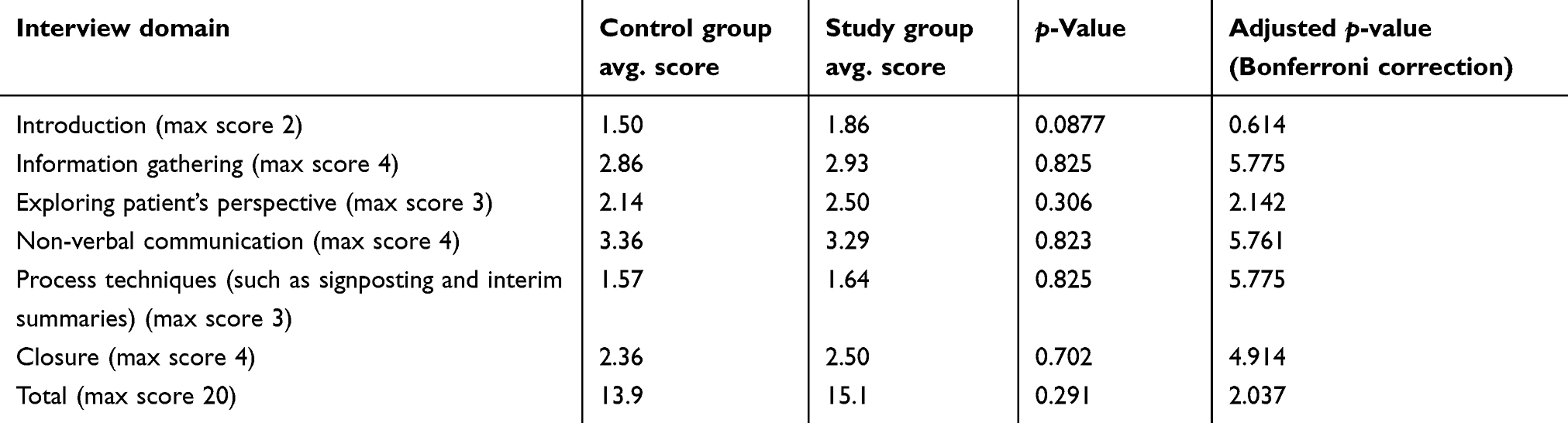 |
Table 1 Simulated patient interview scores: average scores shown for both the study group and control group across all assessed domains |
Focus group data
Themes derived from the focus group transcript are summarized in Table 2.
 |
Table 2 Themes arising from thematic analysis of focus group transcript |
Benefits of real patient contact vs SP contact
Building confidence skills
Half of the students (n=4) reported that real patient contact accelerated their skill development and improved their confidence in approaching and communicating with real patients.
I guess the more people you speak to, the more people with like illnesses that you speak to, like you gain more experience in how to speak to them, what type of questions to ask, that sort of side of it. Student E
Yeah I definitely agree that it’s helped me gain confidence in just approaching patients. And that was one of my main fears and one of the things I wanted to get over when I first joined Connect, so I would definitely say it’s helped a lot.
Student D
It’s one of those things - the more you do it, the more confident you are. So um … I guess by introducing yourself to patients rather than having a doctor or a nurse do it for you, Connect was more useful in that sense. Student C
I would agree that it has made me feel much more confident. Student A
Naturalizing communication
Five students (62.5% of the focus group sample) commented on how conversing with real patients on the wards enabled more naturalised interactions with patients. They contrasted this with formal communication teaching in the simulated patient encounter where they felt they had to adapt to a set structure which could be restrictive reinforcing the perception to “perform skills” in the SP encounter.
And I think that if you’re just so used to talking to patients it becomes more normal, and I think it’s just the extra patient contact just makes it all less textbooky and more natural. Student F
I wouldn’t know how to keep conversation going … this has kind of let me practise that. Student C
But yeah just the whole thing [SP encounter] felt … like you know it’s fake and it just felt kind of forced, my reactions felt forced. Student D
But I think it’s one thing doing it in an acted sort of simulated environment, but I think going into the hospital I always found it easier … it was actually easier than being in that sort of forced simulated environment. So I think that was a relief almost that it was actually not … it was actually easier than what we do in the practice sessions. Student A
I’m not nervous at all, and I can ask the right questions, but you seem to be under a lot of pressure in these simulated patient interviews, and it sort of gets to you. So like … it’s like I see how they’re trying to get you to practise certain skills, certain really specific skills that you might not be able to practise with normal patients, because they just might not be able to say what needs to be said. But I just remember being under so much pressure I don’t think it’s a true representation of what you can do. Student E
Talking to difficult patients
Another benefit reported was the opportunity to interact with patients who were more difficult to communicate with such as those with dementia. Learning how to engage with such patients has been historically left for later clinical years. However, first-year volunteers reported that exposure to “difficult patients” with support from the Connect team, was a very useful experience, enabling them to be more confident and comfortable when confronted with the situation in the future.
On the ward that we go to … there’s a couple with dementia, and you kind of went round and round … I think Connect [volunteering] definitely made me feel more comfortable with that. Student F
And like actually having someone difficult like I felt benefitted me more than someone who was easy to talk to. So, having a difficult patient to try and actually bring out a conversation was more beneficial than sitting with someone who’s like … you could chat to for hours on end. Student C
Low pressure during skill acquisition
The SP interview typically takes place in the context of formal teaching. Interviews are recorded and students often feel increased pressure to perform well and to approach patients in the way they have been taught.
I think like doing Connect you sort of listen more to like the patient story rather than sort of like (inaudible) of like a disease or condition. So when it came to actually doing the simulated like patient interview you didn’t sort of like … one of the mistakes is sort of “Oh what am I going to ask next, what am I going to ask next?” but actually Connect sort of helped you sort of just listen what they’re saying and then sort of develop like a question from there. Student C
I didn’t think it was that useful for the simulated patient interview stuff, because that was such a set process. When we did Connect [volunteering] we found that we were just talking to the patient, chatting about anything. Student D
I’m fine speaking with people [volunteering], I’m not nervous at all … but you seem to be under a lot of pressure in these simulated recorded interviews, and it sort of gets to you. Student E
in the simulated patient one … I knew that people would [be] reviewing my footage, and I felt that that there was that pressure on me. Student G
Simulated vs real
Biopsychosocial disadvantages of real patient contact vs SP contact
Students reported that contact with real patients on the ward enabled exposure to a variety of different patients and to develop a fuller appreciation of the biopsychosocial impact of disease. This enabled an improved student–patient relationship by providing a more informative opportunity to listen to the view of the patient.
Speaking to all the patients who’ve come from all sorts, you hear so many different stories … it sort of widens your horizons. Student E
doing Connect [real patient contact] you listen more to the patient story … not just the disease. Student C
Lack of feedback
Although students recognized the benefits of real patient contact, they also reported on what they felt are its shortcomings. A concern expressed by some of the students was that with real patient encounters, there were fewer feedback opportunities and feedback was less specific. This contrasted with the SP encounter in teaching sessions, which typically involves much more focussed feedback on specific skills and interaction styles. This difference in feedback presents one of the limiting factors connected with real patient contact.
the simulated patient interviews were really good because of the feedback … it was a professional actor who you were talking to, they actually knew what they were talking about when they were giving you feedback, so I found that really useful compared to the real patients. Student H
And about the simulated patient interviews, it went by really really quickly … but I feel like I got so much more out of the video one with the trained actor. And I think that’s just because I took it … like I took both [real patient contact and simulated contact] seriously obviously, but there was much more valuable feedback in the simulated one. Student B
having the actors giving … having them give their own feedback I thought that was a really good part of it. Like it really did help my communication … they clarified some key points which I know now that I can improve on. Student D
the simulated interview helped with the amount of feedback that you get given. Student A
Organizational barriers to learning
Other than comparing simulated and real patient contact, the issue of access to real patients was the most discussed topic with all focus group participants commenting on it. Specific examples from four students and their difficulty in being able to access the wards are given below.
Staff
I think it wasn’t what I expected it to be because I found that the nurses in particular had been quite unwelcoming, so we kind of had to push to go and see the patients every time. And the patients definitely really enjoy us being there, and you know some of them even like profusely thank you. But I found kind of interacting with the hospital staff very difficult because they’ve kind of been very strict with how much time we can spend with the patients, or sometimes we’ve even been sent away. Student A
Most of time we’re like “We’re here from Connect” and they say “Oh why are you here?” “Oh but they’ve just had dinner” “Oh but they’re sleeping” … and we’ve like switched wards, which one we go to first, and which one to go to next … the nurses complain and the other people complain … and then sometimes they’re like “Oh no the Sister on duty doesn’t like Connect, you can’t come today”. Student F
I think yeah what she [fellow student] said is how I feel as well. I wouldn’t recommend the Connect programme unless they made changes with just making … I don’t know, making the nurses more aware … just that. Like everything else it was fine, it was just like going into the wards and trying not to be too intimidated by the nurses. It kind of felt like we were getting in their way, which is understandable cos like they’re busy and they’ve got all their things to do, which is understandable but like … yeah if somehow … if it didn’t feel like we were getting in the way of nurses too much and them doing their jobs then I would happily come back and do it again. Student D
I remember a similar thing. The first couple of times we went they told us it’s too late or something, that a lot of them were tired, but eventually they still let us talk to them. Student B
Timing
Another barrier to learning identified by two students was the issue of timing. Given the agreed time for students visiting was after 6:00 PM, some of the patients would be asleep toward the end of the 2-hour sessions and not wanting to be disturbed.
I felt sometimes the timing wasn’t great. Like I know it’s difficult you know trying to organise the time, but usually you know half the ward are sleeping by the time you sort of get there in the evening after lectures, so it’s quite … you know you’ve only got a few patients you can really talk to. Student C
so we go at 6.30[pm] and we might finish in the women’s ward at 7.30[pm], move on to the male ward … and usually that was too late, so a lot of them would be sleeping, the nurses were more reluctant. They still said oh which patients were awake and which we could talk to, but I think it was a bit harder, so maybe if we started a bit earlier perhaps in the afternoon - that might be something to think about. Student E
Discussion
Our findings indicate that under the conditions of this study increased real patient exposure, in the first year of the medical degree does not correlate with an improvement in performance in a SP encounter. We recognize that this may partly have to do with clear differences in context between real patient contact on the hospital ward and SP contact in the formal teaching setting which merit further consideration some of which we discuss below in the limitations section. Our findings also indicate that overall students favored real patient contact more highly than SP encounters. However, when it came to receiving feedback, the SP encounter was preferred, a finding supported by previous research on this topic.6,12,14 Therefore, if educators consider the use of real patient contact as an integrated learning tool, it is suggested that specific opportunities for formal feedback are designed into the teaching model. In this study, volunteering with senior students allowed opportunities for informal peer-to-peer feedback, providing a possible solution. However, students found formal feedback from experienced SPs of a higher quality than senior student feedback. One solution may be to provide training to senior students, in order to improve the quality of peer feedback when teaching on the wards.
Fifty-seven percent of the study group students reported increased confidence and ability from regular exposure to real patients as benefits of real patient contact. Confidence, from a psychological point of view, can be a major influencing factor in the ability of health care professions to communicate effectively and has even been shown to positively influence competence.15
There are also correlations with experience; early exposure to real clinical scenarios has been shown to increase confidence in clinical communication skills and the ease with which students interview real patients.16,17 Furthermore, real patient contact provides the opportunity to naturalize many vital communication skills such as relating to patients and communicating empathy effectively.18
Again, studies which report students’ experiences of both SP and real patient encounters shed important light on these issues.12,14,19 For example, SP encounters provide more scope for experimentation with communication skills and students view feedback from SPs as better than that from real patients.14,19 However, students find interactions with real patients more instructive than with SPs and the authenticity of real patient encounters is a key advantage over SP encounters.6,12,14,20 This is important, since we know that a close relation between the scenario and real life is a catalyst for more effective skill acquisition.4 More recent research also finds that students self-report better experiences with real patients (when unblinded – in terms of factors such as comfort, friendliness and overall meeting of communication skill training needs); however, this still did not translate to more objective methods of assessment (much like our own findings).21
Exposure to “difficult patients” is a key advantage of real patient contact since the degree to which heterogeneous disease states such as dementia can be replicated in a SP encounter is limited.12,14,20 Studies looking at community-based exposure of medical students to dementia patients have not only reported improved communication skills but also self-efficacy and attitudes, further building a case for the addition of real patient contact early into communication teaching.18,22 Again, if delivered in the early years of medical training, this would have to be carefully planned to align closely with the curriculum and specific learning objectives.
Our findings are congruent with previous studies which also identify factors such as understanding patient perspectives of disease, improving attitudes toward those with sickness and awareness of the professional duties of doctors as benefits of real patient contact.23,24 The findings from these studies indicate the importance of this mode of learning in changing student attitudes and developing communication skills, particularly in the early years.25,26
Another theme brought to light by the focus group was that of barriers to learning in the real hospital setting. Early patient contact is not without its challenges and our findings suggest that effective organization of this mode of teaching is critical. If, for example, as some of our focus group students reported, students are made feel unwelcome on the wards this can be detrimental to their experience of learning. Although these barriers can be regarded as more of a logistical issue with regards to the delivery of real patient contact to students, they are nonetheless important to consider moving forward to improve the student experience of our intervention. This can be done through ensuring all ward personnel are aware of the student volunteers and their role as part of our volunteer organization (through better communication between academic and hospital staff), in addition to altering the possible visitation hours for the students themselves.
Study limitations
We recognize a number of limitations to the current study. The students in the study group experienced real patient contact before their SP encounter. This may have influenced their view of a more “restrictive” experience in the formal teaching setting. Relatedly, this also introduces the possibility of self-selection bias as the study group students, having already committed to extra-curricular activities, are possibly more motivated than the majority of the Year 1 cohort. The actual delivery of each modality was also different. In the real patient setting, learning was supported by peer learners whereas in the SP setting learning was supported by faculty staff. The contact time in each setting also differed with more interaction time allocated in the real patient setting.
The study was also limited by a small sample size and a short exposure time to the intervention. Students attended a minimum of six sessions totaling a combined 12 hours of real patient exposure and this may be considered insufficient to see significant benefits, especially in SP interview performance. Following up students who continue to volunteer throughout later academic years would be useful to account for this.
Moreover, the findings are heavily reliant on self-reported measures of learning benefit since no statistical significance was found between the control and study group in their respective SP interviews. In addition, because of the timing between teaching and exams, we were only able to conduct one focus group and only half of the original study group participated in this. As a first-year cohort, this group has comparatively limited experience of both types of encounters.
Additionally, only first-year medical students were included in the study (to control for the effect of previous experience), which may reduce the generalizability of findings to older students. Real patients whom students were exposed to were mostly in-patients aged over 70 years, which may further confound a lack of transferability to the SP setting (where the SPs were generally younger and healthier). Finally, time and resource constraints of the study meant that the design was limited to one simulated interview as a means of assessment.
Conclusion
Our quantitative analysis showed no significant improvement in attainment of skills by incorporating real patient contact. This may have been partly due to the limitations of our study and the small sample size.
Nevertheless, the focus group findings from 57% of our study group indicate that that regular real patient contact is beneficial in building confidence with patients and naturalizing the acquisition of clinical communication skills. The findings hold some implications for the design of medical curricula toward effectively harnessing the benefits of real patient contact alongside SP contact to ensure that the learning strengths from both modalities are maximized. One possibility would be to organize teaching with real patients in the early years alongside follow-up focussed educational activities with SPs to reinforce or explore further the learning with real patients. More research into real patient contact as a method of learning may identify further possibilities for creating a stronger pedagogical dialogue between the two modes of training in a way that would benefit students’ learning.
Disclosure
The authors report no conflicts of interest in this work.
References
1. General Medical Council (GMC). Good Medical Practice: Working with Doctors for Patients. London: GMC; 2014.
2. General Medical Council (GMC). Outcomes for Graduates (tomorrow’s Doctors). London: GMC; 2015.
3. Brown J. How clinical communication has become a core part of medical education in the UK. Med Educ. 2008;42(3):271–278. doi:10.1111/j.1365-2923.2007.02955.x
4. Kneebone R, Nestel D, Wetzel C, et al. The human face of simulation: patient-focused simulation training. Acad Med. 2006;81(10):919–924. doi:10.1097/01.ACM.0000238323.73623.c2
5. Nestel D, Kneebone R. Perspective: authentic patient perspectives in simulations for procedural and surgical skills. Acad Med. 2010;85(5):889–893. doi:10.1097/ACM.0b013e3181d749ac
6. Bokken L, Rethans JJ, Jobsis Q, Duvvier R, Scherpbier A, van der Vleuten C. Instructiveness of real patients and simulated patients in undergraduate medical education: a randomized experiment. Acad Med. 2010;85(1):148–154. doi:10.1097/ACM.0b013e3181c48130
7. Nestel D, Bentley L. The role of patients in surgical education. In: Fry H, Kneebone R, editors. Surgical Education: Theorising an Emerging Domain. London: Springer; 2011:151–165.
8. Salmon P, Young B. Creativity in clinical communication: from communication skills to skilled communication. Med Educ. 2011;45(3):217–226. doi:10.1111/j.1365-2923.2010.03801.x
9. Littlewood S, Ypinazar V, Margolis SA, Scherpbier A, Spencer J, Dornan T. Early practical experience and the social responsiveness of clinical education: systematic review. BMJ. 2005;331:387–391. doi:10.1136/bmj.331.7513.387
10. Skelton J. The impact of training. In: Brown J, Noble LM, Papageorgiou A, Kidd J, editors. Clinical Communication in Medicine. Oxford: Wiley Blackwell; 2006:49–56.
11. Spencer J, Blackmore D, Heard S, et al. Patient-oriented learning: a review of the role of the patient in the education of medical students. Med Educ. 2000;34(10):851–857. doi:10.1046/j.1365-2923.2000.00779.x
12. Bokken L, Rethans JJ, Scherpbier AJ, van der Vleuten CP. Strengths and weaknesses of simulated and real patients in the teaching of skills to medical students: a review. Simul Healthc. 2008;3(3):161–169. doi:10.1097/SIH.0b013e318182fc56
13. Kirkpatrick DL, Kirkpatrick JD. Evaluating Training Programs: The Four Levels.
14. Bokken L, Rethans JJ, van Heurn L, Duvivier R, Scherpbier AJ, van der Vleuten CP. Students’ views on the use of real patients and simulated patients in undergraduate medical education. Acad Med. 2009;84(7):958–963. doi:10.1097/ACM.0b013e3181a814a3
15. Norman G. RCT = results confounded and trivial: the perils of grand educational experiments. Med Educ. 2003;37(7):582–584. doi:10.1046/j.1365-2923.2003.01586.x
16. Kaufman DM, Laidlaw TA, Macleod H. Communication skills in medical school: exposure, confidence and performance. Acad Med. 2000;75(10):s90–s92.
17. Morgan PJ, Cleave-Hogg D. Comparison between medical students’ experience, confidence and competence. Med Educ. 2002;36(6):534–539. doi:10.1046/j.1365-2923.2002.01228.x
18. Hampshire AJ. Providing early clinical experience in primary care. Med Educ. 1998;32(5):495–501. doi:10.1046/j.1365-2923.1998.00243.x
19. Eagles JM, Calder SA, Nicoll KS, Walker LG. A comparison of real patients, simulated patients and videotaped interview in teaching medical students about alcohol misuse. Med Teach. 2001;23(5):490–493. doi:10.1080/01421590120075733
20. Simek-Downing L, Quirk ME, Letendre AJ. Simulated versus actual patients in teaching medical interviewing. Fam Med. 1986;18(6):358–360.
21. Clever SL, Dudas RA, Barry S, et al. Medical student and faculty perceptions of volunteer outpatients versus simulated patients in communication skills training. Acad Med. 2011;86(11):1437–1442. doi:10.1097/ACM.0b013e3182305bc0
22. Vaz R, Gona O. Undergraduate education in rural primary health care: evaluation of a first-year field attachment programme. Med Educ. 1992;26(1):27–33. doi:10.1111/j.1365-2923.1992.tb00118.x
23. Quinby PM, Papp KK. Adopt-A-Student: early mentoring in family medicine. Med Teach. 1995;17(1):47–52. doi:10.3109/01421599509008288
24. Rooks L, Watson RT, Harris JO. A primary care preceptorship for first-year medical students coordinated by an Area Health Education Center program: a six-year review. Acad Med. 2001;76(5):489–492. doi:10.1097/00001888-200105000-00024
25. Kent GC. Medical student’s reactions to a nursing attachment scheme. Med Educ. 1991;25(1):23–32. doi:10.1111/j.1365-2923.1991.tb00022.x
26. Orbell S, Abraham C. Behavioural sciences and the real world: report of a community interview scheme for medical students. Med Educ. 1993;27(3):218–229. doi:10.1111/j.1365-2923.1993.tb00260.x
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.