Back to Journals » International Journal of Women's Health » Volume 18
Maternal Profiles and Associated Outcomes in Preeclampsia: A Five-Year Retrospective Study in a Tertiary Care Center in Saudi Arabia
Authors Aljebeli S, Alshalan R ![]() , Alarfaj RK
, Alarfaj RK ![]() , Alsalamah N, AlHarbi RA, Basha EA, Alkharouf F
, Alsalamah N, AlHarbi RA, Basha EA, Alkharouf F ![]()
Received 19 March 2026
Accepted for publication 20 May 2026
Published 10 June 2026 Volume 2026:18 607378
DOI https://doi.org/10.2147/IJWH.S607378
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Shahad Aljebeli,1,2 Renad Alshalan,1,3 Rwan K Alarfaj,1,3 Noura Alsalamah,1,3 Rozanna Abdullah AlHarbi,1,3 Ehssan Ashraf Basha,1,3 Feras Alkharouf1,2
1King Abdullah International Medical Research Center (KAIMRC), Riyadh, Saudi Arabia; 2Department of Obstetrics and Gynecology, King Abdulaziz Medical City, Riyadh, Saudi Arabia; 3College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia
Correspondence: Renad Alshalan, Email [email protected]
Introduction: Hypertensive disorders, encompassing chronic hypertension, gestational hypertension, preeclampsia (PE), eclampsia, and superimposed preeclampsia, impact up to 10% of pregnancies globally and contribute to significant maternal and neonatal morbidity and mortality.
Aim: This study aimed to compare the clinical characteristics of women with preeclampsia and evaluate the associated maternal and neonatal outcomes across different subtypes of preeclampsia.
Patient and Methods: This retrospective study was conducted among patients diagnosed with preeclampsia at the Maternal-Fetal Medicine department in National Guard Health Affairs, Riyadh, Saudi Arabia, between January 2019 and January 2024 (5 years). All pregnant females diagnosed with preeclampsia were involved. Data collected include age, gravity, parity, BMI, antihypertensive medication use, Magnesium sulfate use, type of preeclampsia, history of preeclampsia, length of hospital stay, and neonatal outcomes.
Results: Two hundred and seventy-one patients were analyzed and classified into 4 groups: Mild preeclampsia (N=117; 43.2%), severe preeclampsia (N=102; 37.6%), postpartum preeclampsia (N=42; 15.5%), and superimposed preeclampsia (N=10; 3.7%). The mean maternal age was 32 years, and the mean BMI was 31.2 kg/m2. Superimposed preeclampsia was associated with early preterm delivery (p=0.029), and emergency cesarean section (p=0.010). Stillbirth prevalence among PE patients was 5.5% (N=15).
Conclusion: Superimposed preeclampsia was associated with adverse maternal outcomes, including lower gestational age at delivery and increased emergency cesarean section rates. However, these findings should be interpreted carefully due to the small sample size of the superimposed preeclampsia subgroup. Stillbirth occurred in 5.5% of cases and was observed among patients with severe preeclampsia; however, no statistically significant difference was identified between groups. Further prospective studies are warranted to better understand these associations and improve maternal and neonatal outcomes.
Plain Language Summary: Preeclampsia is a serious condition that can occur during pregnancy. It poses significant risks to both the mother and the neonate. This study reviewed medical records of 271 pregnant women diagnosed with preeclampsia over a period five years. Patients were grouped based on the type of preeclampsia: mild, severe, postpartum, or superimposed preeclampsia. The results showed that women with superimposed preeclampsia had more complications, including lower gestational age at delivery and higher chance of emergency cesarean section. Stillbirth occurred in 5.5% of all cases and was more frequently observed in severe preeclampsia. Understanding how different types of preeclampsia affect outcomes can help guide better monitoring and care for women with this condition.
Keywords: pregnancy, preeclampsia, stillbirth
Introduction
Hypertensive disorders, encompassing chronic hypertension, gestational hypertension, preeclampsia, eclampsia, and superimposed preeclampsia, impact up to 10% of pregnancies globally and contribute to roughly 10% of maternal deaths in the United States. Over the past few decades, there has been a rise in the occurrence of preeclampsia, leading to increased health risks for both mothers and newborns.1 An overlooked epidemiological aspect of hypertensive disorders of pregnancy (HDPs) is their prevalence and mortality rates, which vary significantly based on race and ethnicity.2,3 These variations highlight the importance of understanding risk factors associated with maternal hypertension, such as advanced maternal age (over 40 years), pre-pregnancy obesity, excessive weight gain during pregnancy, and the development of gestational diabetes.2
Preeclampsia is described as new onset hypertension after 20 weeks of gestation, defined by systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg, accompanied by proteinuria and/or malfunctioning of vital organs like the kidneys, liver, central nervous system, lungs, or decreased platelet count. This definition aligns with established diagnostic criteria reported in the literature.1,4
Eclampsia is a severe complication of preeclampsia characterized by the occurrence of generalized tonic-clonic seizures. These seizures can occur before childbirth (antepartum), during labor (intrapartum), or after delivery (postpartum). While uncommon before 20 weeks of gestation, documented cases associated with gestational trophoblastic disease have been reported.4,5
The overall prevalence of preeclampsia and eclampsia among adolescent women is 6.7%.6 The pathogenesis of preeclampsia is unpredictable; no exam or test can predict its development. However, potential risk factors for developing preeclampsia include history of preeclampsia, obesity, chronic high blood pressure or kidney disease before pregnancy, age more than 40, multiple gestation, African American ethnicity, and family history.7–9 Preeclampsia is also more common among women who have history of lupus, rheumatoid arthritis, urinary tract infections, polycystic ovary syndrome, and gestational diabetes.10–13 Several acute maternal complications of preeclampsia and eclampsia including liver rupture, hypertensive emergency, renal failure, pulmonary edema, disseminated intravascular coagulopathy (DIC), hypertensive encephalopathy, cortical blindness, and HELLP syndrome.14 The study by Baha M. Sibai found that 53 pregnancies complicated by eclampsia 13% of the pregnancies could be considered to have severe preeclampsia prior to seizure.15 A study in the United Kingdom reported similar findings in which high blood pressure (≥120 mmHg diastolic) was recorded in 20% of patients with eclampsia.16 A form of hypertensive encephalopathy where an acute rise in blood pressure causes loss of cerebral blood flow (CBF) autoregulation and hyperperfusion of the brain that results in vasogenic edema formation and subsequent seizure is considered to be the pathogenesis of eclamptic seizure.17 Three categories are important for effective preeclampsia management; prevention of preeclampsia, early detection, and treatment. Magnesium sulfate (MgSO4) is the drug of choice for prevention of eclampsia while other anticonvulsant agents such as diazepam are not appropriate treatments in the prevention of convulsions.18
Several risk factors were identified for preeclampsia. For example, a cross sectional study conducted at King Abdulaziz University Hospital in Jeddah, Saudi Arabia, studied 370 pregnant women between March to May 2016. Higher risk of preeclampsia was associated with older age (≥35 years), smoking, multiple pregnancies, family history of diabetes mellitus, and chronic hypertension.19 In correlation with these findings, studies in Nigeria and Pakistan also reported significant associations with advanced maternal age, obesity, parity, smoking, and family history of diabetes mellitus and hypertension.20,21
Moreover, according to the American College of Obstetricians and Gynecologists, the common clinical manifestations of preeclampsia include persistent elevated blood pressure, proteinuria, edema, visual disturbances, epigastric pain, decreased platelet count, elevated liver enzymes, and impaired renal function.22 Additionally, North Western Armed Forces Hospital Program in Tabuk, Saudi Arabia, has reported similar clinical manifestations of preeclampsia among Saudi women.23 With this information in hand, it is important to review and understand the charactretics of preeclamptic patients and aid in preventing complications that may arise. Despite the extensive literature describing the epidemiology, risk factors, and complications of preeclampsia, there remains limited comparative data on maternal and neonatal outcomes across different subtypes of preeclampsia, particularly in Middle Eastern populations. In addition, variations in clinical presentation and outcomes across these subtypes are not fully understood. Building on this need, this study aimed to compare the clinical characteristics and maternal and neonatal outcomes across different subtypes of preeclampsia in a tertiary care center in Saudi Arabia. We hypothesized that outcomes may differ between preeclampsia subtypes, with more severe forms being associated with worse maternal and neonatal outcomes.
Methods
This study was conducted in the Maternal-Fetal Medicine Department at National Guard Health Affairs (NGHA) in Riyadh, Saudi Arabia, a tertiary care center. This is a retrospective chart review utilizing the BESTCare electronic health record (EHR) system at NGHA to analyze medical records of pregnant patients diagnosed with preeclampsia who received care between January 2019 and January 2024. All pregnant women diagnosed with preeclampsia during the study period were included. Missing data were reported where present and were not included in the statistical analysis for the affected variables.
Data collection was performed using a structured checklist that extracted key details from patient records, including demographic information (age, BMI, gravida, parity), type of preeclampsia (mild preeclampsia, severe preeclampsia, postpartum preeclampsia, superimposed preeclampsia), obstetric outcomes (mode of delivery, gestational age at delivery, fetal outcomes, complications), hospital course (length of stay) and neonatal outcomes.
Preeclampsia was defined as new-onset hypertension after 20 weeks of gestation accompanied by proteinuria and/or end-organ dysfunction, according to established diagnostic criteria reported in the literature. Superimposed preeclampsia was defined as preeclampsia occurring in patients with pre-existing chronic hypertension. The classification of preeclampsia subtypes was based on these definitions.
Data analysis was conducted using SPSS software (version 28), with categorical variables summarized using frequencies and percentages, and continuous variables presented as means, ranges, and standard deviations. The Chi-square test (or Fisher’s Exact test) was used to assess categorical associations, while the Student’s t-test was employed to compare continuous variables, with a significance level set at p-value < 0.05.
Results
This study analyzed two hundred and seventy-one patients. As seen in Table 1, patients’ mean age was slightly higher in postpartum preeclamptic patients (mean: 33.8 years) but were not significantly different across the groups (p=0.165). The mean BMI was higher in the superimposed preeclamptic group (mean: 33.9 kg/m2; p=0.166), (80%; p=0.751) being obese. The number of gravidities (p=0.672) and parity (p=0.398) were almost similar across the groups. Further, the mean gestational age was statistically significantly lower among superimposed preeclamptic patients (mean: 31.7 weeks; p=0.004), and early preterm was also more frequently observed in this group (p=0.029). Additionally, the number of gestation (p=0.754) and history of preeclampsia in previous pregnancy (p=0.150) were similar across the groups.
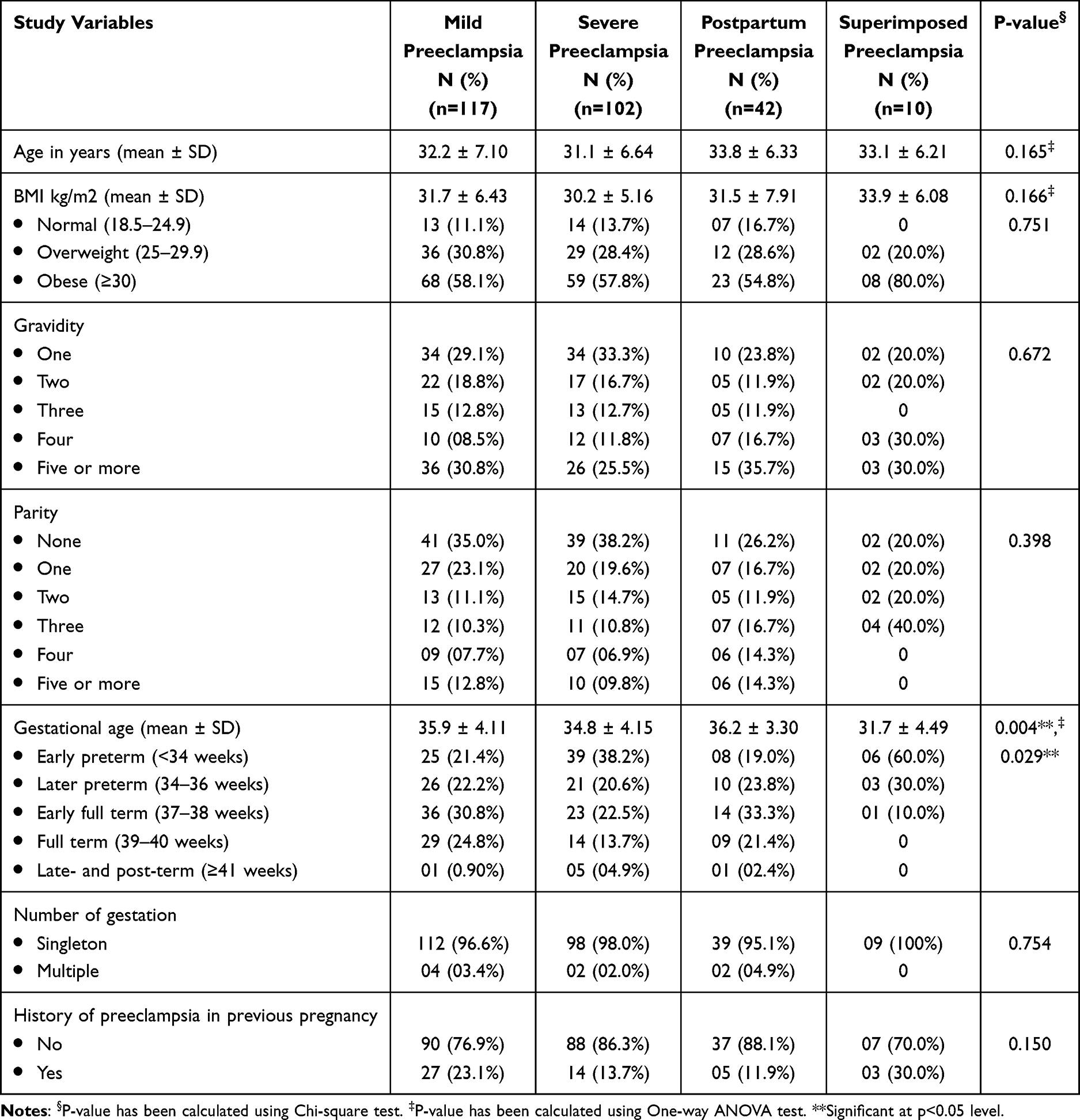 |
Table 1 Maternal Characteristics in Relation to Diagnosis (n=271) |
Regarding the maternal outcomes of preeclamptic patients (Table 2), superimposed preeclamptic patients were associated with emergency caesarean section (p=0.010). However, the use of analgesia/anesthesia (p=0.059) was not significantly different across the groups (p=0.059). Also, the mean duration of hospital stay among preeclamptic patients did not differ significantly across the groups (p=0.267).
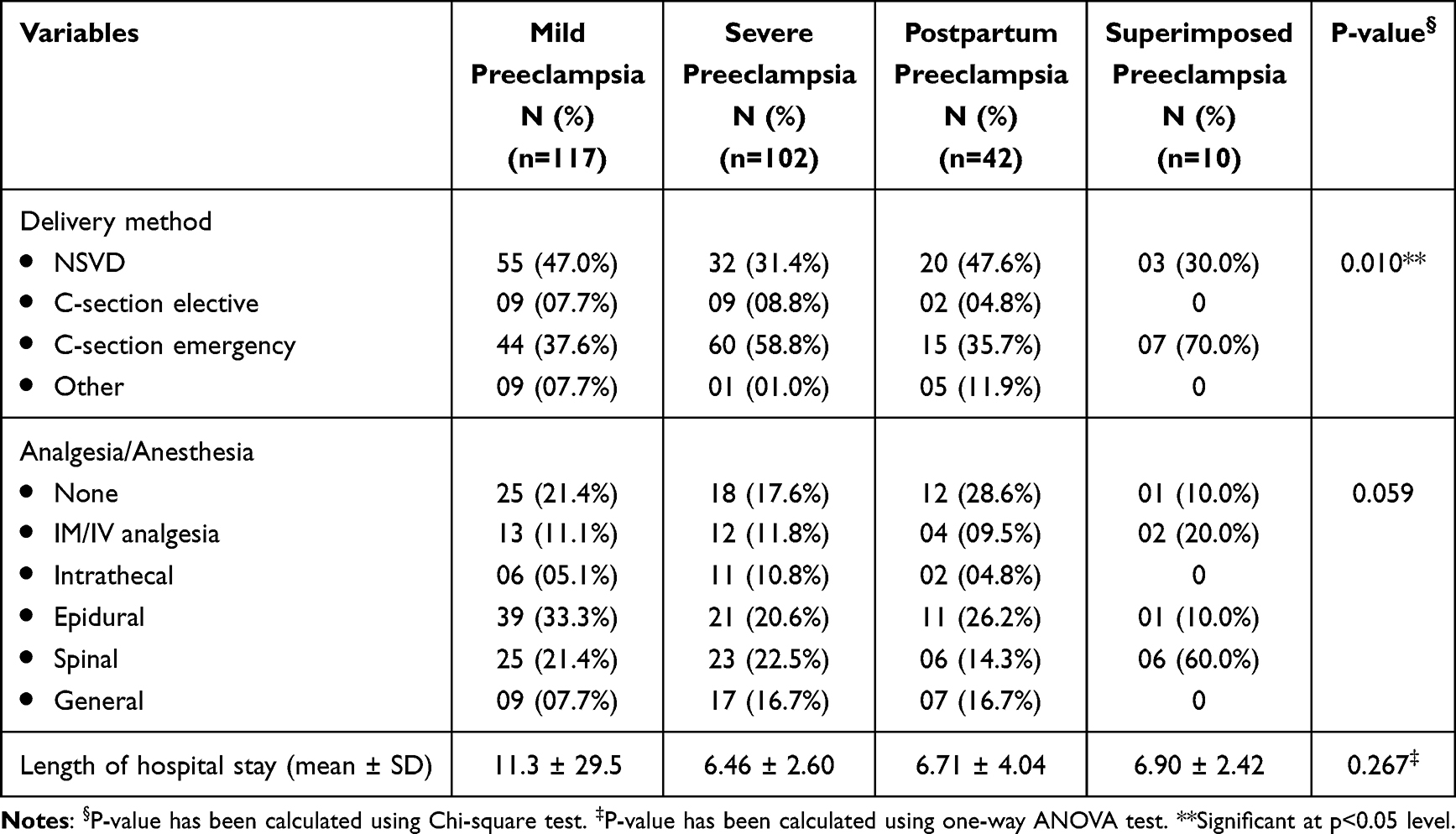 |
Table 2 Maternal Outcome in Relation to Diagnosis (n=271) |
Regarding neonatal outcomes of preeclamptic patients (Table 3), the birth weight level was similar among preeclamptic patients (p=0.207), while neonate resuscitations were less associated with mild preeclampsia (p=0.001).
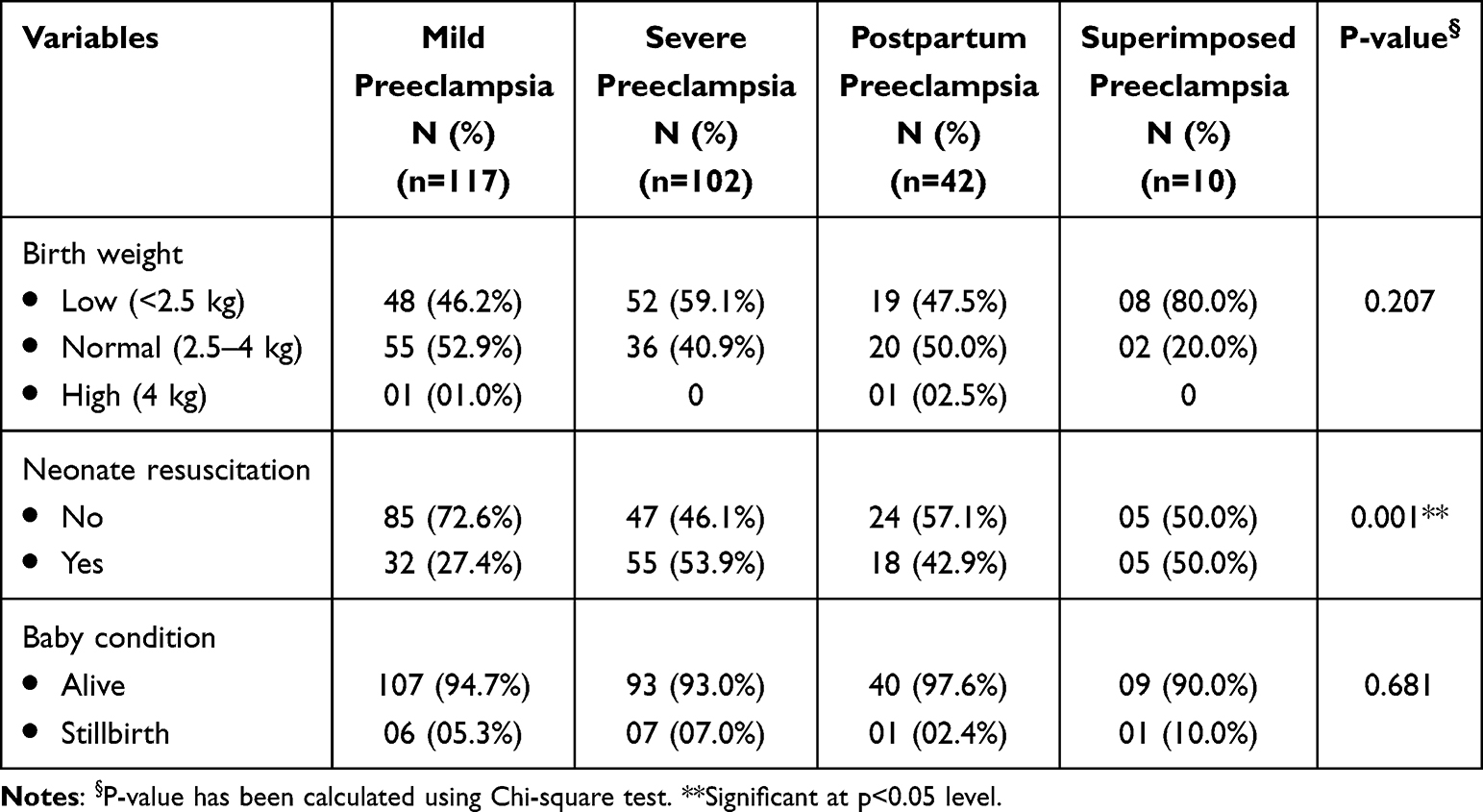 |
Table 3 Neonatal Outcome in Relation to Diagnosis (n=271) |
Regarding medications used among preeclamptic patients (Table 4), it was observed that the use of methyldopa (p=0.804), Nifedipine (p=0.462), and Labetalol (p=0.263) were similar across the groups, while the use of Hydralazine was significantly higher in severe preeclamptic patients (p=0.032). Also, superimposed patients were associated with the usage of MgSO4 (p<0.001).
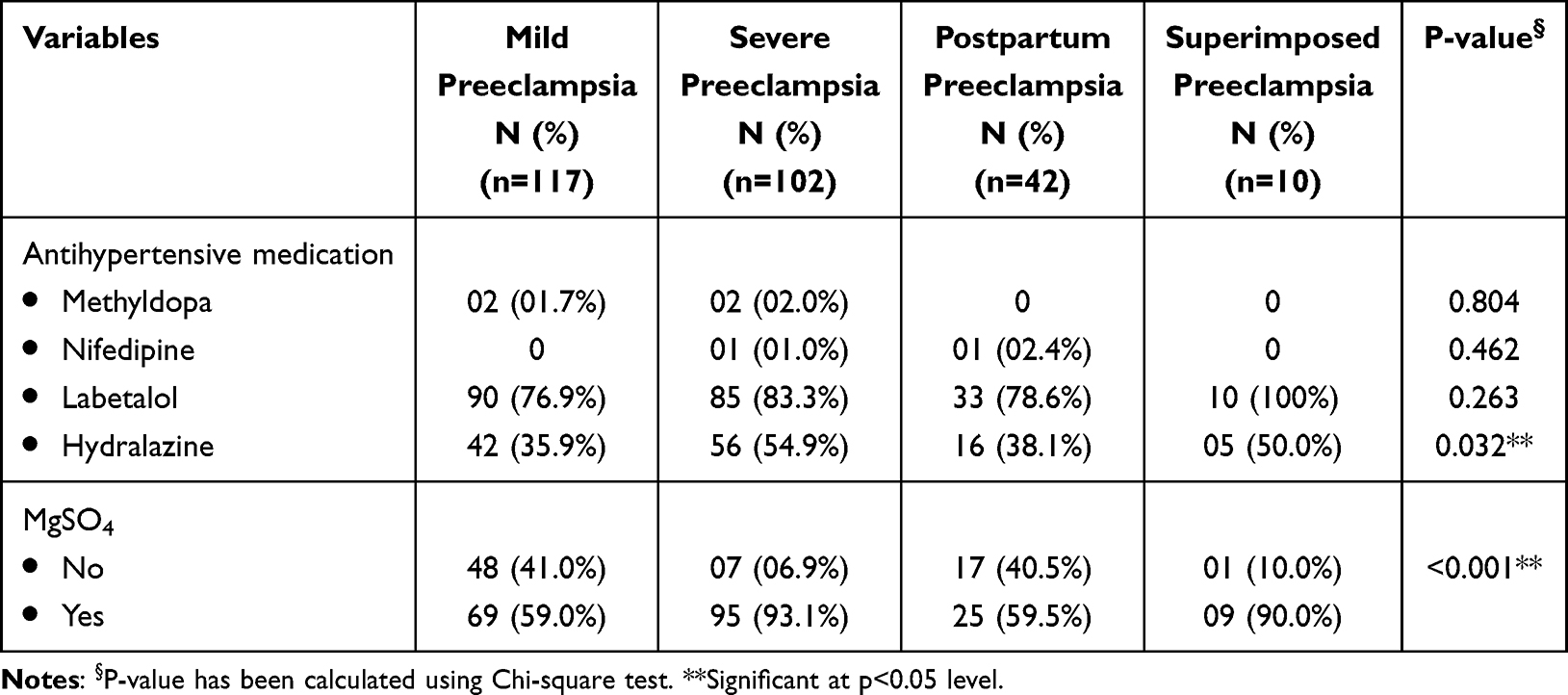 |
Table 4 Medications in Relation to Diagnosis (n=271) |
The characteristics of the stillbirth babies have been described in Table 5. Baby #7 had the highest maternal age (44 years), while baby #5 showed the lowest (20 years). Seven of the stillbirths were born by mothers with severe preeclampsia. Also, 7 of them were delivered by normal vaginal delivery (NVD) and 5 of them by Emergency C-section. The highest birth weight was recorded by baby #3 (3.49 kg), while baby #12 recorded the lowest (0.34 kg). Only baby #1 had neonate resuscitation.
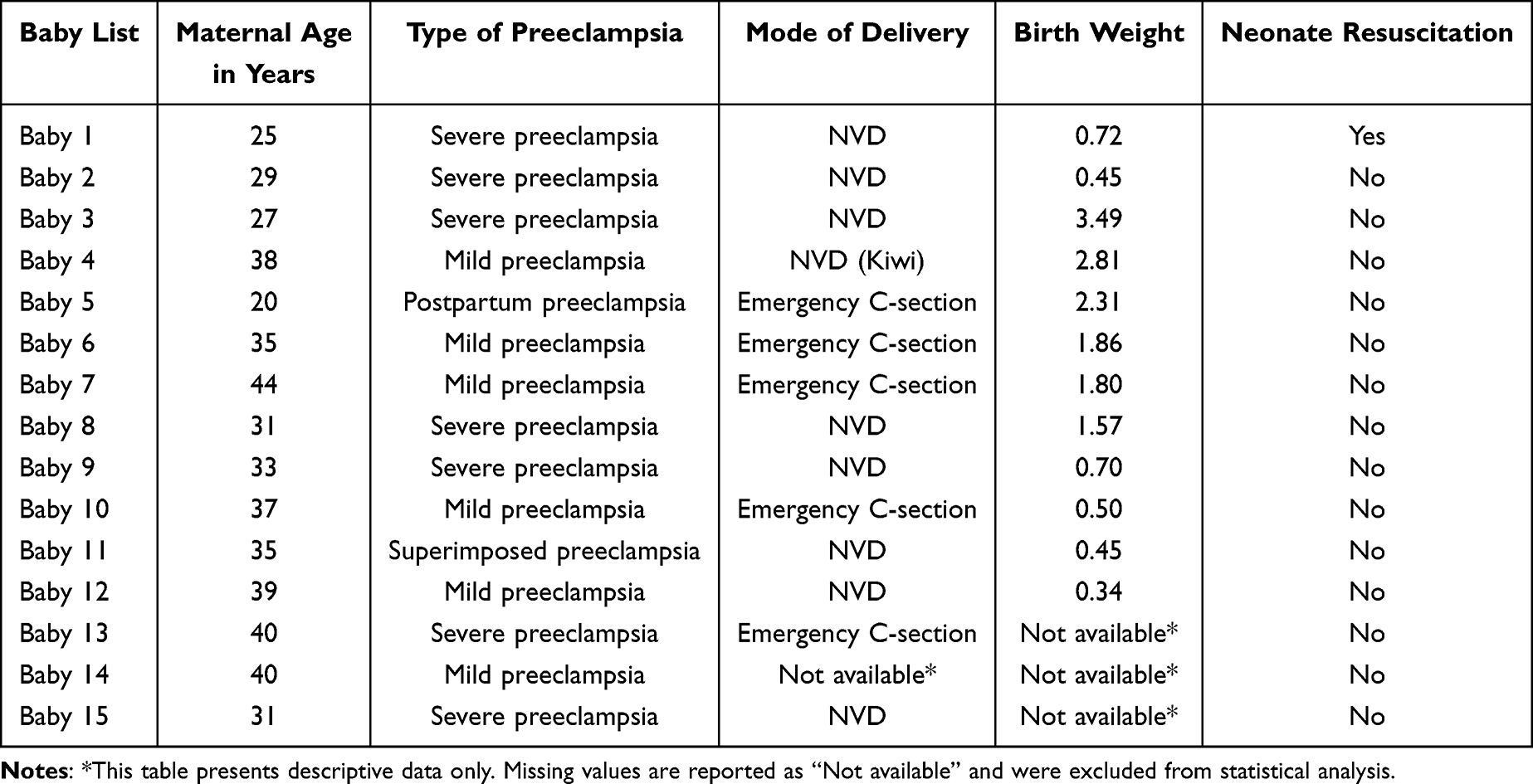 |
Table 5 Descriptive Characteristics of Stillbirth Babies |
Discussion
This study investigated the characteristics of preeclampsia during pregnancy. Evidence suggests that mild preeclampsia showed the highest prevalence among preeclamptic types (43.2%), followed by severe (37.6%) and postpartum (15.5%), while superimposed preeclampsia was the least common (3.7%). Early recognition, careful monitoring, and medical intervention could prevent preeclamptic complications during pregnancy. Hence, regular prenatal check-ups are necessary to monitor blood pressure, protein in the urine, and other signs of preeclampsia during pregnancy.
Compared with preeclampsia, superimposed preeclampsia confounds approximately 20% of pregnancies in patients with chronic hypertension and is correlated with a higher risk of maternal and perinatal morbidity.24 In our study, patients with superimposed preeclampsia were associated with lower gestational age at delivery and and emergency cesarean section. Notwithstanding these reports, several studies documented risk factors associated with preeclampsia. For example, according to the reports of Alalem and Aldukkan, preeclampsia was associated with twin pregnancies, terminated pregnancies, diabetes, family history of diabetes mellitus, women having a family history of hypertension, women with severe to mild anemia, tobacco smoking, asthma, and age 35 years or higher.19 Corroborating these reports, Anorlu et al revealed that the factors that increased the risk of preeclampsia include nulliparity, stressful work, stressful home environment, previous history of preeclampsia, previous history of chronic hypertension, elevated body weight (>80 kg) and multiple pregnancies.20 However, a previous report enunciated in Tanzania revealed that risk factors associated with severe preeclampsia include maternal age between 15 to 20 years, pregnancy from a new partner/husband, diabetes prior to conception, family history of high blood pressure, having high blood pressure in a previous pregnancy, multifetal gestation and paternal age over 45 years.25 In our study, we found no significant relationships between preeclampsia in terms of maternal age, BMI, gravidity, parity, number of gestation, and history of preeclampsia in a previous pregnancy (p>0.05). These findings may be attributed to population diversity, study design, sample size, definitions, and diagnostic criteria.
Women with mild PE were less likely to require neonate resuscitation (p=0.001) and were less frequently treated with Hydralazine (p=0.032). In our study, MgSO4 prescriptions were common in patients with more serious maternal PE, including severe and superimposed PE. Literature suggests that patients with superimposed PE could exhibit worse maternal outcomes than those with mild PE. Despite the fact that both cases could have similar neonatal outcomes, superimposed PE had increased maternal complications compared to PE alone.26
Examining the details of stillbirth among PE patients showed that cases were distributed across different preeclampsia subtypes, with severe PE (7/15) and mild PE (6/15), without statistically significant differences between the groups (p=0.681). Maternal age ranged from 20 years to 44 years, reflecting a broad age distribution and indicating that stillbirth among preeclamptic patients is not limited to a specific maternal age group. Regarding mode of delivery, normal delivery (8 out of 15 cases) and emergency cesarean section (5 out of 15 cases). The highest birthweight being recorded was 3.49 kg, while 0.34 kg was the lowest. Only one patient had neonate resuscitation. Overall, the prevalence of stillbirth among PE patients was 5.5%. This prevalence is consistent with the study of Ngwenya et al,27 reporting a prevalence of stillbirth among severe PE patients at 9.8%. Timely intervention, careful monitoring, and patient education are keys to preventing stillbirth among PE’s population.
Conclusion
This study provides evidence that superimposed preeclampsia was associated with lower gestational age at delivery and increased emergency cesarean section rates. Further, the use of MgSO4 was more frequent among this group of patients. Nevertheless, stillbirth was observed among patients with severe preeclampsia. These findings highlight the importance of careful monitoring and individualized management of patients with different subtypes of preeclampsia to reduce maternal and fetal complications. However, the findings should be interpreted with caution, particularly given the relatively small sample size of the superimposed preeclampsia group. Further prospective studies are warranted to better understand these associations and improve maternal and neonatal outcomes.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, S.J., upon reasonable request. The data are not publicly available due to institutional restrictions and the presence of information that could compromise patient confidentiality. The data were obtained from the Maternal-Fetal Medicine Department at the National Guard Health Affairs – Riyadh, Saudi Arabia.
Ethical Approval Statement
Ethical approval for this study was obtained from the Institutional Review Board (IRB) of the King Abdullah International Medical Research Center (KAIMRC), Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia (IRB Approval No: 000005924; Study Number: NRR24/008/5; Approval Date: 26 May 2024). The study was reviewed under expedited review and conducted in accordance with the principles of the Declaration of Helsinki. This retrospective chart review utilized anonymized patient records obtained from the BESTCare electronic medical record system. As the study involved secondary analysis of de-identified data, the requirement for informed consent was waived by the Institutional Review Board.
Disclosure
All authors have no conflicts of interest to declare for this work.
References
1. Sutton ALM, Harper LM, Tita ATN. Hypertensive disorders in pregnancy. Obstet Gynecol Clin North Am. 2018;45(2):333–8. doi:10.1016/j.ogc.2018.01.012
2. Singh GK, Siahpush M, Liu L, Allender M. Racial/ethnic, nativity, and sociodemographic disparities in maternal hypertension in the United States, 2014–2015. Int J Hypertens. 2018;2018:7897189. doi:10.1155/2018/7897189
3. Petersen EE, Davis NL, Goodman D, et al. Vital signs: pregnancy-related deaths, United States, 2011–2015, and strategies for prevention, 13 states, 2013–2017. MMWR. 2019;68(18):423–429. doi:10.15585/mmwr.mm6818e1
4. Wilkerson RG, Ogunbodede AC. Hypertensive disorders of pregnancy. Emerg Med Clin North Am. 2019;37(2):301–316. doi:10.1016/j.emc.2019.01.008
5. Leeman L, Dresang LT, Fontaine P. Hypertensive disorders of pregnancy. Am Fam Physician. 2016;93(2):121–127.
6. Macedo TC, Montagna E, Trevisan CM, et al. Prevalence of preeclampsia and eclampsia in adolescent pregnancy: a systematic review and meta-analysis of 291,247 adolescents worldwide since 1969. Eur J Obstetrics Gynecol Reprod Biol. 2020;248:177–186. doi:10.1016/j.ejogrb.2020.03.043
7. Duckitt K, Harrington D. Risk factors for preeclampsia at antenatal booking: systematic review of controlled studies. Br Med J. 2005;330(7491):565. doi:10.1136/bmj.38380.674340.E0
8. Boghossian NS, Yeung E, Mendola P, et al. Risk factors differ between recurrent and incident preeclampsia: a hospital-based cohort study. Ann Epidemiol. 2014;24(12):871–877.e3. doi:10.1016/j.annepidem.2014.10.003
9. Lim KH, Steinberg G, Ramus RM. Preeclampsia. 2016. Available from: http://emedicine.medscape.com/article/1476919-overview.
10. Lin HC, Chen SF, Lin HC, Chen YH. Increased risk of adverse pregnancy outcomes in women with rheumatoid arthritis: a nationwide population-based study. Ann Rheumatic Dis. 2010;69:715–717. doi:10.1136/ard.2008.105262
11. Clowse MEB. Lupus activity in pregnancy. Rheum Dis Clin North Am. 2007;33:237–252. doi:10.1016/j.rdc.2007.01.002
12. Conde-Agudelo A, Villar J, Lindheimer M. Maternal infection and risk of preeclampsia: systematic review and meta-analysis. Am J Clin Exp Obstet Gynecol. 2008;198(1):7–22. doi:10.1016/j.ajog.2007.07.040
13. Veltman-Verhulst SM, van Rijn BB, Westerveld HE, et al. Polycystic ovary syndrome and early-onset preeclampsia: reproductive manifestations of increased cardiovascular risk. Menopause. 2010;17(5):990–996. doi:10.1097/gme.0b013e3181ddf705
14. Norwitz ER, Hsu CD, Repke JT. Acute complications of preeclampsia. Clin Obstet Gynecol. 2002;45(2):308–329. doi:10.1097/00003081-200206000-00004
15. Sabai BM. Eclampsia: VI. Maternal-perinatal outcome in 254 consecutive cases. Am J Clin Exp Obstet Gynecol. 1990;163:1049–1055. doi:10.1016/0002-9378(90)91123-T
16. Douglas KA, Redman CWG. Eclampsia in the United Kingdom. BMJ. 1994;309:1395–1400. doi:10.1136/bmj.309.6966.1395
17. Cipolla MJ, Kraig RP. Seizures in women with preeclampsia: mechanisms and management. Fetal Maternal Med Rev. 2011;22(2):91–108. doi:10.1017/S0965539511000040
18. Altman D, Carroli G, Duley L, Farrell B. Do women with preeclampsia, and their babies, benefit from magnesium sulphate? The Magpie Trial: a randomised placebo-controlled trial. Lancet. 2002;359(9321):1877–1890.
19. Alalem DH, Aldukkan LB. Prevalence and associated risk factors for preeclampsia among pregnant women attending antenatal care in King Abdulaziz University Hospital in Jeddah, Saudi Arabia: a hospital-based study. Ann Int Med Dent Res. 2017;4(1). doi:10.21276/aimdr.2018.4.1.me8
20. Anorlu R, Iwuala NC, Odum CU. Risk factors for preeclampsia in Lagos, Nigeria. Aust N Z J Obstetrics Gynaecol. 2005;45(4):278–282. doi:10.1111/j.1479-828X.2005.00411.x
21. Shamsi U, Saleem S, Nishtar N. Epidemiology and risk factors of preeclampsia: an overview of observational studies. ResearchGate; 2013. Available from: https://www.researchgate.net/publication/261027618.
22. American College of Obstetricians and Gynecologists. Hypertension in pregnancy. Obstet Gynecol. 2013;122(5):1122–1131. doi:10.1097/01.AOG.0000437382.03963.88
23. Al-Ghamdi S, Al-Harbi AS, Khalil A, et al. Hypertensive disorders of pregnancy: prevalence, classification and adverse outcomes in Northwestern Saudi Arabia. Ann Saudi Med. 1999;19(6):557–560. doi:10.5144/0256-4947.1999.557
24. Kametas NA, Nzelu D, Nicolaides KH. Chronic hypertension and superimposed preeclampsia: screening and diagnosis. Am J Clin Exp Obstet Gynecol. 2022;226(2):S1182–S1195. doi:10.1016/j.ajog.2020.11.029
25. Machano MM, Joho AA. Prevalence and risk factors associated with severe preeclampsia among postpartum women in Zanzibar: a cross-sectional study. BMC Public Health. 2020;20(1):1–10. doi:10.1186/s12889-020-09384-z
26. Valent AM, DeFranco EA, Allison A, et al. Expectant management of mild preeclampsia versus superimposed preeclampsia up to 37 weeks. Am J Clin Exp Obstet Gynecol. 2015;212(4):515–e1. doi:10.1016/j.ajog.2014.10.1090
27. Ngwenya S, Jones B, Mwembe D, Nare H, Heazell AE. The prevalence of and risk factors for stillbirths in women with severe preeclampsia in a high-burden setting at Mpilo Central Hospital, Bulawayo, Zimbabwe. J Perinat Med. 2022;50(6):678–683. doi:10.1515/jpm-2022-0080
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Diagnostic Value of Hepatic and Renal Biochemical Tests for the Detection of Preeclampsia Among Pregnant Women Attending the Antenatal Care Clinic at the University of Gondar Comprehensive Specialized Hospital, Gondar, Northwest Ethiopia
Walle M, Getu F, Gelaw Y, Getaneh Z
International Journal of General Medicine 2022, 15:7761-7771
Published Date: 10 October 2022
Investigating Serum and Placental Levels of IGF-1 and IGF-1R in Preeclampsia Patients and Their Clinical Implications
Su J, Huang X, Meng S, Wang S
International Journal of Women's Health 2025, 17:729-738
Published Date: 13 March 2025
A Comparative Cross-Sectional Study Between Gestational Diabetes Mellitus and Preeclampsia: Medication Adherence, Depression and Quality of Life
Noor R, Abbas G, Khurram H, Aslam A, Randhawa FA, Assiri A, Shah S
International Journal of Women's Health 2026, 18:565083
Published Date: 8 January 2026
Red Cell Distribution Width-to-Albumin Ratio as a Predictor of Preeclampsia in Advanced Maternal Age: A Retrospective Cohort Study
Wang N, Liu S, Zhou W, Ge L, Huang S
International Journal of Women's Health 2026, 18:596658
Published Date: 25 April 2026