Back to Journals » International Journal of General Medicine » Volume 19
Maternal Diabetes and Attention Deficit/Hyperactivity Disorder Association: A Narrative Review on Emerging Evidence, Research Gaps and Future Directions
Received 11 February 2026
Accepted for publication 14 May 2026
Published 22 May 2026 Volume 2026:19 602877
DOI https://doi.org/10.2147/IJGM.S602877
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Satish Nair
Chenyuan Zhao, Yang Liu
Department of Obstetrics and Gynecology, Huludao Central Hospital, Huludao, Liaoning, People’s Republic of China
Correspondence: Yang Liu, Department of Obstetrics and Gynecology, Huludao Central Hospital, No. 28 Haiyue Road, Longgang District, Huludao, Liaoning, People’s Republic of China, Email [email protected]
Abstract: Maternal diabetes includes pre-gestational diabetes mellitus (PGDM) and gestational diabetes mellitus (GDM), with increasing prevalence globally. Attention Deficit Hyperactivity Disorder (ADHD) is a common childhood neurodevelopmental disorder. This narrative review synthesizes epidemiological and mechanistic evidence published mainly since 2023 to explore the association between maternal diabetes and ADHD in offspring. Pooled data show that maternal diabetes increases offspring ADHD risk by approximately 30%, with PGDM showing a stronger association than GDM, and poorly controlled diabetes or diabetes requiring medication conferring higher risk. Mechanistically, intrauterine hyperglycemia induces oxidative stress, inflammatory responses, placental dysfunction, neurotransmitter imbalance, and epigenetic alterations, which may impair fetal neurodevelopment. Inconsistencies remain in diabetes classification, diagnostic criteria, glycemic control level, and offspring assessment age. Most existing studies are observational and cannot confirm causality. This review identifies research limitations and provides a theoretical basis for prenatal glucose management and early intervention. These findings have important public health implications for reducing the burden of neurodevelopmental disorders.
Keywords: ADHD, maternal diabetes, PGDM, GDM, neurodevelopmental disorders, narrative review
Introduction
ADHD is a common neurodevelopmental disorder characterized by inattention, hyperactivity, and impulsivity, affecting 2%-7% of children worldwide and causing substantial educational, social, and economic burdens. Its etiology involves genetic, neurobiological, and environmental factors.
Maternal diabetes comprises two main types: pre-gestational diabetes mellitus (PGDM, including type 1 and type 2 diabetes before pregnancy) and gestational diabetes mellitus (GDM, diabetes first diagnosed during pregnancy). Global prevalence of GDM is about 16%, and both types can disrupt the intrauterine environment and increase risks of adverse pregnancy outcomes and long‑term neurodevelopmental impairments in offspring.
Previous studies have suggested associations between maternal diabetes and offspring ADHD, but findings are inconsistent across diabetes type, glycemic control, medication use, and ADHD subtype. Evidence updated after 2023 has not been systematically summarized.
This narrative review aims to clarify the association between maternal diabetes and offspring ADHD, summarize recent epidemiological and mechanistic evidence, identify research gaps including diagnostic heterogeneity and confounding bias, and highlight the public health importance of prenatal glycemic management for preventing childhood ADHD.
Materials and Methods
This was a narrative review. We searched publications from 2023 to 2026 in PubMed, Embase, and Web of Science. Eligible studies focused on maternal diabetes (PGDM, T1DM, T2DM, GDM) and offspring ADHD. Articles were screened independently by two reviewers. Data including study design, population, exposure definition, outcome assessment, main results, and biological mechanisms were extracted. Evidence was synthesized qualitatively without meta‑analysis.
Overview of Attention Deficit Hyperactivity Disorder
Definition and Diagnostic Criteria for ADHD
Attention deficit hyperactivity disorder (ADHD) is a common neurodevelopmental disorder that is mainly manifested by inattention, hyperactivity, and impulsive behavior that are disproportionate to age and development level. These symptoms can affect patients ‘learning, social and daily life functions. According to the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5), the diagnostic criteria for ADHD mainly include the following aspects:
In terms of inattention, patients often have the following manifestations: they often fail to pay close attention to details, and often make careless mistakes in homework, work or other activities; they have difficulty maintaining attention during study, listening or other activities; when others speak directly to them, they often act as if they are not listening; they often fail to follow instructions to complete tasks and complete homework, housework or work; they often have difficulty organizing tasks and activities; Often avoid, dislike, or be reluctant to engage in tasks that require sustained mental effort; often lose items needed for tasks or activities; often easily distracted by irrelevant external stimuli; often forget daily activities. If a patient develops at least 6 of the above symptoms before the age of 12 and lasts for at least 6 months, the diagnostic criterion for inattention is met.
In terms of hyperactivity and impulsiveness, patients ‘typical manifestations include: often moving their hands and feet or twisting around in the seat; often leaving the seat and unable to sit for a long time in situations where sitting needs to be maintained; often running around or climbing up and down in inappropriate situations; often unable to play quietly or engage in leisure activities; often “busy”, as if “driven by an engine”; often talking too much; often answering questions first before others have finished; It is often difficult to wait for your turn; often interrupt or interfere with others. Similarly, if at least 6 of the above symptoms appear before the age of 12 and persist for more than 6 months, hyperactivity and impulsiveness can be diagnosed.
ADHD can be diagnosed only if these symptoms occur in multiple settings (such as school, family, social occasions, etc.) and cause significant damage to the patient’s social, academic or professional functioning, and if the symptoms cannot be better explained by other mental disorders. ADHD is mainly divided into three subtypes: inattention-dominant type, which mainly presents with difficulty concentrating, easy distraction, and no end in doing things; hyperactivity/impulse type, which mainly presents with overactivity, restlessness, impulsive behavior, etc.; mixed type, which means having both inattention and hyperactivity/impulse symptoms.
Pathogenesis of ADHD
Genetic Factors
Genetic factors play a crucial role in the development of ADHD. A large number of twin studies and family genetic studies provide strong evidence for this view. A study of twins showed that if one of identical twins (with the same genes) is diagnosed with ADHD, the other has a 79% chance of developing ADHD; while among fraternal twins (with a genetic similarity of about 50%), the probability is only 32%. This fully demonstrates that genes have an important influence in the onset of ADHD. Family genetic research has also found that ADHD has obvious family aggregation. If a child has ADHD, the risk of developing ADHD for parents or siblings is 2–8 times higher than that of normal people.1
Further molecular genetic research has identified multiple genetic loci and genes associated with ADHD. These genes are mainly involved in the dopaminergic neurotransmitter system, the noradrenergic nervous system and the serotonin nervous system. For example, the dopamine D4 receptor gene (DRD4) is closely associated with ADHD. Certain mutations in the DRD4 gene may cause its sensitivity to dopamine to decrease, thereby affecting the transmission of nerve signals in the brain, which in turn triggers symptoms of ADHD. The study also found that a polymorphism in the dopamine transporter gene (DAT1) is also associated with ADHD. DAT1 is responsible for transporting dopamine in the synaptic gap back to presynaptic neurons. Its abnormal function may lead to an imbalance in the concentration of dopamine in the synaptic gap, affecting functions such as attention and impulse control. Although genetic factors dominate the incidence of ADHD, environmental factors cannot be ignored. Genetic and environmental factors interact and jointly affect the occurrence and development of ADHD. The potential mechanism by which maternal diabetes affects attention deficits in offspring is shown in Figure 1.
 |
Figure 1 Schematic diagram of the potential mechanism by which maternal diabetes affects attention deficits in offspring. |
Neurobiological Factors
Neurobiological factors play an important role in the pathogenesis of ADHD, mainly involving brain structure and function abnormalities and neurotransmitter imbalances. Brain imaging research has found that people with ADHD have some characteristic changes in brain structure. Compared with the normal population, ADHD patients have smaller volumes in areas such as the prefrontal cortex, striatum, and cerebellum. The prefrontal cortex plays a key role in advanced cognitive functions such as attention control, behavioral suppression, and decision-making. The reduction in volume of this area may cause patients to experience difficulties in these functions, manifested by symptoms such as inattention, hyperactivity, and impulsiveness. The striatum is involved in processes such as motor control, reward system and habit formation. Its structural abnormalities may affect patients ‘motor coordination and sensitivity to rewards, further exacerbating the symptoms of ADHD.
Functional magnetic resonance imaging (fMRI) studies have shown that when people with ADHD perform tasks such as attention and inhibitory control, the activation patterns of relevant brain areas are different from those of normal people. During attention tasks, areas such as the prefrontal cortex and parietal cortex in ADHD patients have lower levels of activation, indicating that these areas are not functional enough in processing attention-related information. During the inhibitory control task, ADHD patients have abnormal activation in areas such as the anterior cingulate cortex, making it difficult for them to effectively suppress impulsive behavior. These abnormalities in brain function further confirm the dysfunction of brain neural circuits in patients with ADHD.
There are many neurotransmitter imbalances in the brain of patients with ADHD, among which neurotransmitters such as dopamine, norepinephrine and serotonin are most closely related to ADHD. Dopamine plays an important role in regulating attention, motivation, reward and exercise control. Dopamine levels in the brain of people with ADHD may be reduced, or dopamine receptors may function abnormally, resulting in impaired dopamine signaling, which may affect the patient’s attention and behavioral control. The noradrenergic system is closely related to attention, vigilance and executive function. Abnormal function of the noradrenergic system in patients with ADHD may lead to impairment of these cognitive functions, manifested as symptoms such as inattention and hyperactivity. 5-The serotonin system is involved in processes such as emotion regulation, sleep and cognitive function. 5-Abnormal serotonin levels may be related to symptoms such as emotional instability and attention deficit in ADHD patients.2
Environmental Factors
Environmental factors also play an important role in the pathogenesis of ADHD, mainly including prenatal, perinatal and postpartum environmental factors. Maternal diabetes, as an important prenatal environmental factor, has attracted increasing attention. Maternal diabetes can cause the fetus to be in a hyperglycemic environment in the mother, which may affect the normal development of the fetal brain. Hyperglycemia can cause increased insulin secretion in the fetus, leading to excessive fetal growth, increasing the risk of neonatal hypoglycemia, hypoxemia, etc. These factors may have adverse effects on the proliferation, migration and differentiation of fetal brain neurons, thereby increasing the risk of children suffering from ADHD. A follow-up study of the offspring of pregnant women with GDM found that the incidence of ADHD in children in the GDM group at the age of 7 was significantly higher than that in the normal control group, further confirming the association between maternal diabetes and ADHD in the offspring.3
Premature labor is also an important risk factor for ADHD. Because the brain development is not yet fully mature, premature infants may face various complications and environmental stimuli after birth. These factors may affect the normal development of the brain. Studies have shown that children born prematurely have 2–3 times the risk of developing ADHD than full-term babies.4 White matter damage and abnormal development of the neurotransmitter system caused by premature birth may be important mechanisms that increase the risk of ADHD. The family environment after childbirth also has an impact on the incidence of ADHD. Tense family atmosphere, improper parental education methods, parents suffering from mental illness or behavioral problems are all related to the occurrence of ADHD. Parents over-pampering or being too strict with their children and lack of effective communication and guidance may lead to children’s emotional instability, loss of control, and increase the risk of ADHD.
The Prevalence of ADHD
ADHD is a common neurodevelopmental disorder worldwide, and its incidence varies among different regions and populations. Globally, the incidence of ADHD is approximately 2%-7%. In some developed countries, such as the United States, the incidence of ADHD is relatively high, about 5%-7%. In developing countries, the incidence of ADHD cannot be ignored. For example, the incidence of ADHD among children and adolescents in China is about 6.26%. The incidence of ADHD fluctuates to some extent in different countries and regions, but it is generally within a relatively stable range. There are many reasons for this difference. Differences in diagnostic criteria and methods may lead to different incidence statistics. Different countries and regions may adopt different diagnostic standards, such as DSM5, International Classification of Diseases, 10th Edition (ICD-10), etc. These standards have certain differences in symptom descriptions and diagnostic thresholds, which affects the incidence statistics. Cultural and social factors may also have an impact on the diagnosis and incidence of ADHD. In some cultural settings, people’s perceptions and tolerances of behavioral problems in children are different, which may lead to some ADHD patients being not diagnosed and identified in a timely manner.5
In recent years, with the improvement of people’s awareness of ADHD and the continuous improvement of diagnostic techniques, the incidence of ADHD has shown an upward trend. This upward trend may not only be due to the increase in real incidence, but may also be related to the increased awareness of diagnosis and the expansion of the scope of diagnosis. More and more parents and doctors have a deeper understanding of ADHD and are able to detect and diagnose ADHD patients in a timely manner, resulting in an increase in the calculated incidence of ADHD.
In addition to the diagnostic factors mentioned above, the reason for the increase in the incidence rate is also related to changes in environmental factors. With the development of industrialization and urbanization, factors such as environmental pollution, the popularization of electronic products, and the accelerated pace of life may have an impact on children’s neurodevelopment and increase the risk of ADHD. Studies have found that children who are exposed to high-lead, high-mercury and other pollutants for a long time have an increased risk of developing ADHD. Excessive use of electronic products may also lead to behavioral problems such as inattention and hyperactivity in children.
Results
Epidemiological Evidence of Maternal Diabetes and ADHD Association
Cohort Study
A retrospective birth cohort study conducted at Kaiser Medical Institution in Southern California included 333182 births born at the institution from 1995 to 2012, and prospectively followed up with electronic medical records on children aged 4. The study used Cox regression analysis to estimate the relative risk of ADHD associated with intrauterine diabetes exposure through hazard ratios (HRs) and adjusted for potential confounding factors. The results showed that a total of 37878 (11.4%) children were exposed to diabetes (522 exposed to T1D, 7822 exposed to T2D, and 29534 exposed to GDM). During an average of 4.9 years of follow-up (interquartile range 2.2, 9.6) after 4 years of age, 17415 (5.2%) children were diagnosed with ADHD. Compared with children not exposed to diabetes, the adjusted HRs for ADHD exposed to T1D were 1.57 (95% CI 1.09 −2.25), the adjusted HRs for ADHD exposed to T2D were 1.43 (1.29–1.60), the adjusted HRs for GDM requiring antidiabetic medication were 1.26 (1.141.41), and the adjusted HRs for GDM not requiring medication were 0.93 (0.86–1.01). Overall, the risk of ADHD was not associated with GDM overall (P=0.50) or with gestational age (P=0.16), however, the risk of GDM requiring antidiabetic drugs was much greater than that of GDM not requiring antidiabetic drugs (P<0.001). This suggests that the severity of a mother’s diabetes affects the child’s risk of ADHD, and that GDM requiring antidiabetic medication is associated with an increased risk of ADHD in the offspring.6
A study of more than 200,000 pairs of maternal and infant data from 10 birth cohorts based on the European Union Child Cohort Network (EUCCN) explored the relationship between maternal pre-pregnancy and pregnancy diabetes and children’s neurodevelopment, cognitive and behavioral outcomes. Studies have found that children aged 7–10 born to GDM mothers have more obvious ADHD symptoms. Among children aged 11–13, maternal GDM was not significantly associated with ADHD.3 Type 1 or 2 diabetes in a mother before pregnancy is associated with ADHD symptoms in children aged 4–6. This further confirms the association between maternal diabetes and ADHD in offspring, and this association may differ among different age groups. Table 1 shows the association between different types of maternal diabetes and the risk of ADHD in offspring.
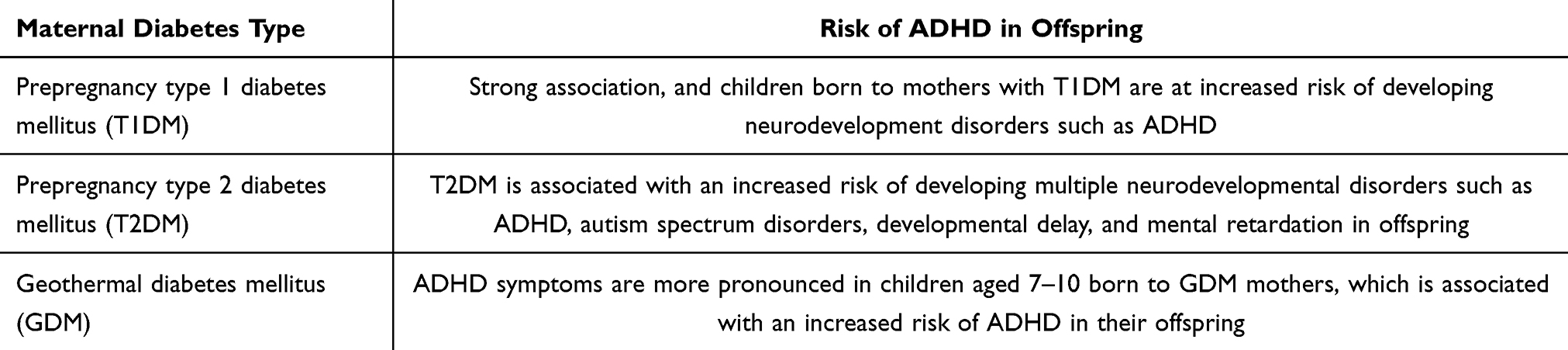 |
Table 1 Association Between Different Types of Maternal Diabetes and Risk of ADHD in Offspring |
Case-Control Study
In a case-control study, the researchers selected children with ADHD as the case group, and healthy children matched for age and sex as the control group. The exposure of their mothers to diabetes during pregnancy was compared between the two groups. See Table 2. The results showed that the proportion of mothers with diabetes in the case group was significantly higher than that in the control group. After adjusting for confounding factors such as mother’s age, education level, and family income, the OR value was 1.35 (95% CI 1.12 −1.63), indicating that there is a significant association between maternal diabetes during pregnancy and ADHD in the offspring.7
 |
Table 2 Diabetes Prevalence of Mothers in Case Group and Control Group |
Another case-control study on children in a certain area collected detailed information on the mother’s health during pregnancy, including diagnosis and treatment of diabetes, as well as children’s development and diagnosis of ADHD. It was found that children whose mothers had GDM and had poor blood sugar control had a 2.1 times higher risk of developing ADHD than children whose mothers had normal blood sugar. This suggests that the control of maternal diabetes may also be an important factor affecting the incidence of ADHD in offspring.8
Case-control studies can obtain research results in a short period of time and are of great significance for exploring disease risk factors. However, this research method also has certain limitations, such as being susceptible to recall bias and selection bias. When recalling health conditions during pregnancy, mothers in the case group and the control group may have different recall accuracy, resulting in inaccurate exposure information. When selecting study subjects, if the selection criteria for the case group and the control group are not strict, it may lead to differences in other important factors between the two groups, thus affecting the reliability of the study results. Therefore, when interpreting the results of case-control studies, these limitations need to be fully considered and combined with the results of other research methods for comprehensive analysis.
Biological Mechanisms Underlying Maternal Diabetes and Offspring ADHD
In order to deeply explore the potential mechanism between maternal diabetes and attention deficit in offspring, many scholars have carried out a series of animal experiments. In an animal experiment, researchers induced diabetes by injecting pregnant rats with streptozotocin (STZ), thereby simulating the maternal diabetes environment. After the offspring rats were born, they were subjected to a series of behavioral tests and neurodevelopment-related indicators.9
Behavioral test results showed that compared with the control group, offspring rats exposed to diabetes performed worse in attention-related tests. For example, in the eight-arm maze experiment, they were more prone to making wrong choices and having difficulty concentrating. Find the right path. In the open-field experiment, these offspring rats showed hyperactivity, significantly increased movement distance, and shorter stays in the central area, indicating that they had behavioral characteristics of hyperactivity and inattention, similar to human ADHD.
In terms of neural development, studies have found that neurotransmitter imbalances and neuronal structure abnormalities occurred in areas of the brain of offspring rats related to attention and behavioral control, such as the prefrontal cortex and striatum. This is reflected in reduced levels of neurotransmitters such as dopamine and norepinephrine, as well as reduced dendritic branches and reduced synaptic density of neurons in these areas. These changes may lead to abnormal neural signal transmission in the brain, which in turn affects the attention and behavioral regulation ability of offspring rats.
Another animal experiment used high-sugar and high-fat diet to feed pregnant mice to establish a mouse model of gestational diabetes. It was found that the offspring mice developed abnormalities in glucose metabolism and lipid metabolism after adulthood, and also showed attention deficit and hyperactivity behavior in behavioral tests. Histological examination found that the islet tissue structure of the offspring mice was abnormal, fat tissue accumulated increased, and neurons in the hippocampus in the brain related to learning, memory and attention were damaged. This further suggests that maternal diabetes may increase the risk of behavioral problems such as attention deficits in offspring by affecting fetal metabolism and neurodevelopment.10
Animal experiments can strictly control experimental conditions and conduct in-depth research on the mechanism of the impact of maternal diabetes on the neural development and behavior of offspring. By simulating different types of maternal diabetes environments and observing the changes of offspring at different stages of development, it provides important experimental basis for understanding the relationship between the two. However, animal experiments also have certain limitations. The physiological and pathological processes of animal models and humans are different, and the experimental results cannot be completely directly extrapolated to humans. Therefore, it is necessary to combine animal experimental results with epidemiological and clinical studies to more comprehensively reveal the relationship between maternal diabetes and attention deficits in offspring.
Discussion on the Influence Mechanism
Changes in Intrauterine Environment
Hyperglycemia and Hyperinsulinemia
In the pathological state of maternal diabetes, the intrauterine environment changes significantly, among which hyperglycemia and hyperinsulinemia have many effects on fetal neural development. In a hyperglycemic state, glucose in the maternal blood enters the fetus in large quantities through the placenta, causing the fetal blood sugar level to increase. In order to maintain blood sugar balance, the fetus’s pancreatic beta cells compensatory proliferation and secrete large amounts of insulin, causing hyperinsulinemia.
Hyperglycaemia and hyperinsulinemia interfere with the normal proliferation, migration and differentiation of fetal nerve cells. During the proliferation stage of neural cells, a hyperglycemic environment can lead to abnormal cell cycle regulation and affect the division and proliferation speed of neural stem cells. Studies have found that neural stem cells cultured in a hyperglycemic environment have significantly reduced their proliferation ability and the expression of cyclins has also changed. This may be due to metabolic disorders caused by high blood sugar, which leads to insufficient energy supply within cells and affects the normal division activities of cells.11
During nerve cell migration, hyperinsulinemia may hinder the normal migration of nerve cells by affecting the composition of extracellular matrix and signaling pathways. Nerve cells need to migrate to the right location along a specific path to form a normal neural network. Hyperinsulinemia may change the expression of adhesion molecules on the cell surface, abnormal the interaction between nerve cells and extracellular matrix, resulting in the inability of nerve cells to accurately migrate to the target location, which in turn affects the normal structure and function of the brain.
Hyperglycaemia and hyperinsulinemia can also adversely affect the differentiation of nerve cells. They may interfere with the expression of genes related to neural differentiation and hinder the differentiation of neural stem cells into neurons and glial cells. Studies have shown that in a hyperglycemia environment, the expression of some transcription factors closely related to neural differentiation is down-regulated, resulting in a decrease in the proportion of neural stem cells that differentiate into neurons and an increase in the proportion of neural stem cells that differentiate into glial cells. This may affect synaptic connections and signal transmission between neurons, which in turn affects the brain’s cognitive and behavioral functions.12
Oxidative Stress and Inflammatory Response
Maternal diabetes can trigger oxidative stress and inflammatory reactions, which can damage fetal brain development. In a hyperglycemic environment, glucose metabolism in the body is abnormal and a large number of reactive oxygen species (ROS) are produced, such as superoxide anions, hydrogen peroxide and hydroxyl free radicals. The production of these ROS exceeds the body’s antioxidant defense capabilities, leading to the occurrence of oxidative stress. Oxidative stress can cause damage to biological macromolecules in the fetal brain, such as DNA, proteins and lipids. In terms of DNA, ROS can cause DNA strand breaks, base modifications, and gene mutations, affecting the normal expression and replication of genes. Studies have found that levels of 8-hydroxydeoxyguanosine (8-OHdG), a marker of oxidative DNA damage, are significantly elevated in the brains of fetuses with maternal diabetes. In terms of proteins, oxidative stress can lead to protein carbonylation, sulfhydryl oxidation and disulfide bond formation, which changes the structure and function of the protein. This may affect signal transduction pathways and metabolic processes within nerve cells, leading to nerve cell dysfunction. Oxidative stress can also cause peroxidation of lipids on cell membranes, destroy the integrity and mobility of cell membranes, and affect material exchange and signal transmission in nerve cells.13
Maternal diabetes can also trigger an inflammatory response. Hyperglycemia activates the immune system in the mother and fetus, leading to the release of multiple inflammatory factors, such as tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), and C-reactive protein (CRP). These inflammatory factors can enter the fetus through the placenta and affect the development of the fetal brain. TNF-α can induce apoptosis of nerve cells and inhibit proliferation and differentiation of nerve cells. Studies have shown that in nerve cells cultured in vitro, after adding TNF-α, the apoptosis rate of nerve cells is significantly increased and the cell proliferation ability is decreased. IL-6 interferes with the synthesis and release of neurotransmitters and affects the transmission of neural signals.14 In animal experiments, injecting IL-6 antibodies into diabetic rats during pregnancy can partially improve neurobehavioral abnormalities in offspring rats. The inflammatory response can also lead to damage to the blood-brain barrier, making it easier for harmful substances to enter the brain, further exacerbating the damage to the fetal brain.15
In an animal experiment, researchers injected streptozotocin into pregnant rats to induce diabetes. The results showed that ROS levels in the brains of the offspring rats were significantly increased, antioxidant enzyme activities were reduced, and the inflammatory factors TNF-α and IL-6 increased expression. These offspring rats showed significant cognitive and behavioral deficits in behavioral tests, such as decreased learning and memory abilities, hyperactivity and inattention. In clinical studies, placental and cord blood of maternal diabetic patients were tested, and abnormalities in indicators related to oxidative stress and inflammatory response were also found. Analysis of placental tissues of pregnant women with GDM found that the level of oxidative stress marker malondialdehyde (MDA) increased, the activity of the antioxidant enzyme superoxide di*ase (SOD) decreased, and the expression of the inflammatory factors IL-6 and CRP also increased significantly. These results all suggest that oxidative stress and inflammatory responses caused by maternal diabetes play an important role in neurodevelopment abnormalities in offspring.16
Epigenetic Regulation
Epigenetic regulation plays a pivotal role in modulating the impact of maternal diabetes on offspring neurodevelopment, primarily through mechanisms involving DNA methylation and histone modifications. DNA methylation occurs through the action of DNA methyltransferases, which add methyl groups to specific regions of the DNA (usually CpG islands) in cytosine bases, thereby influencing gene expression. In the context of maternal diabetes, the DNA methylation patterns within the fetal organism may undergo significant alterations. Research has revealed that in offspring of women with gestational diabetes mellitus (GDM), the DNA methylation levels in certain gene promoter regions have shown notable changes compared to those in offspring from normal pregnant women. When studying cord blood from GDM offspring, it has been found that the promoter regions of genes associated with neurodevelopment, such as the brain-derived neurotrophic factor (BDNF) gene, exhibit elevated levels of methylation. BDNF plays crucial roles in the survival, differentiation, synaptogenesis, and plasticity of neural cells. An increase in the methylation levels within the promoter region of the BDNF gene leads to a suppression of BDNF expression, thereby impacting the neurodevelopmental process. The alteration in DNA methylation patterns might be attributed to the intrauterine environment changes caused by maternal diabetes, including high blood glucose levels and oxidative stress, which may affect the activity or expression of DNA methyltransferases, thereby altering the methylation status of genes.17
Histone modification is also an important epigenetic regulatory mechanism, including methylation, acetylation, phosphorylation, and other modification types. These modifications can change the interaction between histones and DNA, affect the structure of chromatin and the accessibility of genes, thus regulating gene expression. In the study of maternal diabetes, it was found that histone modification also participates in the regulation of offspring neurodevelopment. The methylation level of histone H3 lysine 9 (H3K9) in offspring of diabetic mothers is altered in the brain. H3K9 methylation is usually associated with gene silencing, and its level changes may affect the expression of genes related to neurodevelopment. Studies have shown that in a high-glucose environment, the activity of histone deacetylase increases, leading to a decrease in histone acetylation levels, and the chromatin structure becomes tighter, thereby inhibiting gene expression. This may affect the processes of differentiation, migration, and synapse formation of neurons, ultimately leading to abnormal neurodevelopment in offspring.18
In a study involving animal models, by establishing a gestational diabetes mouse model, it was found that the histone modification states of genes related to learning and memory in the offspring mouse brains were significantly altered. Compared to the control group, the level of trimethylation of histone H3 lysine 27 (H3K27) in the hippocampus of the experimental group mice increased, and this modification is associated with gene silencing. Further research revealed that these genes’ expression levels were significantly reduced, and the offspring mice also performed significantly worse in learning and memory tests. This suggests that gestational diabetes may affect the expression of genes related to neurodevelopment by altering histone modifications, thereby exerting adverse effects on the neurobehavior of offspring. In human studies, similar abnormalities in histone modifications were also found in the brain tissue or peripheral blood of offspring of pregnant diabetic patients. These research findings provide important clues for a deeper understanding of the mechanisms by which gestational diabetes affects offspring neurodevelopment.19
Controversies and Research Gaps
There are still inconsistencies in the definition and diagnosis of maternal diabetes (PGDM vs GDM), glycemic control level, ADHD diagnostic criteria, and age at assessment across studies. Most current evidence comes from observational research, which cannot fully confirm a causal relationship between maternal diabetes and ADHD in offspring. Confounding factors such as family genetics, socioeconomic status, and maternal lifestyle may also affect the authenticity of the results.
Strengths and Limitations of This Review
The major strength of this narrative review is that it integrates the latest epidemiological and mechanistic evidence published since 2023, systematically clarifies the association between maternal diabetes and offspring ADHD, and summarizes potential biological pathways. The main limitation is that this is a narrative review without a systematic search, quality assessment, or meta-analysis; thus, potential selection bias and heterogeneity cannot be quantitatively evaluated.
Public Health Implications
This review suggests that standardized prenatal glycemic screening and tight glucose control in diabetic pregnancies may help reduce the risk of neurodevelopmental disorders such as ADHD in offspring. For offspring exposed to maternal diabetes, early neurodevelopmental monitoring and timely intervention are of great significance to reduce the long-term public health burden.
Conclusions
Based Maternal diabetes is associated with an increased risk of ADHD in offspring, especially PGDM and poorly controlled or medication-treated GDM. Intrauterine hyperglycemia, oxidative stress, inflammation, neurotransmitter imbalance, and epigenetic modifications contribute to fetal neurodevelopmental impairment. However, most existing studies are observational and cannot confirm causality, and heterogeneity exists in diabetes type, diagnostic criteria, glycemic control, and offspring follow-up age. Future large-scale, long-term prospective cohort studies with strict adjustment for confounders and standardized definitions are needed. Prenatal glucose monitoring and management are critical to reduce the risk of neurodevelopmental disorders such as ADHD in offspring.
Data Sharing Statement
No datasets were generated or analysed during the current study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Faraone SV, Larsson H. Genetics of attention deficit hyperactivity disorder. Mol Psychiatry. 2019;24(4):562–10. doi:10.1038/s41380-018-0070-0
2. Tang W, Jiang J, Wang H. Brain functional differences among ADHD subtypes in children revealed by phase-amplitude coupling analysis of resting-state EEG. Int J Psychophysiol. 2025;215:113222. doi:10.1016/j.ijpsycho.2025.113222
3. Pretorius RA, Avraam D, Guxens M, et al. Is maternal diabetes during pregnancy associated with neurodevelopmental, cognitive and behavioural outcomes in children? Insights from individual participant data meta-analysis in ten birth cohorts. BMC Pediatric. 2025;25(1). doi:10.1186/s12887-024-05365-y
4. Mitha A, Chen R, Razaz N, et al. Neurological development in children born moderately or late preterm: national cohort study. BMJ. 2024;384:e075630. doi:10.1136/bmj-2023-075630
5. Getinet A, Sileshi D, Yitbarek G, et al. The global prevalence of attention deficit hyperactivity disorder in children and adolescents: an umbrella review of meta-analyses. J Affect Disord. 2023;339:860–866. doi:10.1016/j.jad.2023.07.071
6. Xiang AH, Wang X, Martinez MP, et al. Maternal gestational diabetes mellitus, type 1 diabetes, and type 2 diabetes during pregnancy and risk of ADHD in offspring. Diabetes Care. 2018;41(12):2502–2508. doi:10.2337/dc18-0733
7. Ye W, Luo C, Zhou J, et al. Association between maternal diabetes and neurodevelopmental outcomes in children: a systematic review and meta-analysis of 202 observational studies comprising 56·1 million pregnancies. Lancet Diab Endocrinol. 2025;13(6):494–504. doi:10.1016/S2213-8587(25)00036-1
8. Zhan-kui L, Rui-miao B. Effects of gestational hyperglycemia exposure on neurodevelopmental outcomes in offspring. Chin J Children’s Health. 2022;30(10):1045–1048.
9. Ghasemi A, Jeddi S. Streptozotocin as a tool for induction of rat models of diabetes: a practical guide. EXCLI J. 2023;22:274–294. doi:10.17179/excli2022-5720
10. Evans MV, Mejia EM, Zulk JJ, et al. Gestational diabetes augments group B Streptococcus infection by disrupting maternal immunity and the vaginal microbiota. Nat Commun. 2024;15(1):1035. doi:10.1038/s41467-024-45336-6
11. Zheng Y, Zhang F, Deng C, Wei Z. Research progress on effects of high glucose microenvironment on biological activity of adipose-derived stem cells. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2020;34(12):1602–1606. doi:10.7507/1002-1892.202003094
12. Zhang Y, Zhou H. Hyper-reactive platelets and type 2 diabetes. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2022;47(3):374–383. doi:10.11817/j.issn.1672-7347.2022.210271
13. Huan C, Jiawen C, Ailing L, et al. Advances in the study of the correlation between oxidative stress and gestational diabetes mellitus. Chin J Sexuality. 2021;(04):35–38.
14. Min Y. Molecular mechanism of tmTNF-α mediating apoptosis through TNFR1 and study on the reverse signaling pathway of tmTNF-α. Huazhong University of Science and Technology; 2012.
15. Zipp F, Bittner S, Schafer DP, et al. Cytokines as emerging regulators of central nervous system synapses. Immunity. 2023;56(5):914–925. doi:10.1016/j.immuni.2023.04.011
16. Kyeong EL, Mi EK, Na YK, et al. Immunomodulatory effect of hispolon on LPS-induced RAW264.7 cells and mitogen/alloantigen-stimulated spleen lymphocytes of mice. Pharmaceutics. 2022;14(7):1423. doi:10.3390/pharmaceutics14071423
17. Briana DD, Maria P, Maria B, et al. Differential expression of cord blood neurotrophins in gestational diabetes: the impact of fetal growth abnormalities. J Maternal-Fetal Neonatal Med. 2018;31(3):278–283. doi:10.1080/14767058.2017.1281907
18. Qian Y, Li Y, Zheng C, et al. High methylation levels of histone H3 lysine 9 associated with activation of hypoxia-inducible factor 1α (HIF-1α) predict patients’ worse prognosis in human hepatocellular carcinomas. Cancer Genetics. 2020;245(prepublish):17–26. doi:10.1016/j.cancergen.2020.04.077
19. Wanyi H, Youxiang Z, Lina W, Meijuan L, Yuhua L, Jiaqi H. Morphological changes and gene differential expression in hippocampus tissue of newborn mice from pregnant diabetic rats. Guangdong Med J. 2023;44(3):271–277.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Orexin/Hypocretin System Dysfunction in ESSENCE (Early Symptomatic Syndromes Eliciting Neurodevelopmental Clinical Examinations)
Knez R, Stevanovic D, Fernell E, Gillberg C
Neuropsychiatric Disease and Treatment 2022, 18:2683-2702
Published Date: 15 November 2022