Back to Journals » Clinical Epidemiology » Volume 14
Maternal Cigarette Smoking During Pregnancy and Genital Anomalies in Boys: A Register-Based Cohort and Sibling-Matched Design Study
Authors Lindbo D ![]() , Arendt LH, Ernst A, Lunddorf LLH
, Arendt LH, Ernst A, Lunddorf LLH ![]() , Brix N
, Brix N ![]() , Ramlau-Hansen CH
, Ramlau-Hansen CH ![]()
Received 31 March 2022
Accepted for publication 27 June 2022
Published 23 July 2022 Volume 2022:14 Pages 901—910
DOI https://doi.org/10.2147/CLEP.S368826
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lars Pedersen
Daniel Lindbo,1 Linn Håkonsen Arendt,1,2 Andreas Ernst,1,3 Lea Lykke Harrits Lunddorf,1 Nis Brix,1,4 Cecilia Høst Ramlau-Hansen1
1Department of Public Health, Research Unit for Epidemiology, Aarhus University, Aarhus, Denmark; 2Department of Obstetrics and Gynecology, Horsens Region Hospital, Horsens, Denmark; 3Department of Urology, Aarhus University Hospital, Aarhus, Denmark; 4Department of Clinical Genetics, Aarhus University Hospital, Aarhus, Denmark
Correspondence: Daniel Lindbo, Department of Public Health, Research Unit for Epidemiology, Aarhus University, Bartholins Allé 2, Aarhus, 8000, Denmark, Tel +45 21950102, Email [email protected]
Purpose: Cryptorchidism and hypospadias share several prenatal risk factors. However, in published studies, boys exposed to cigarette smoking during pregnancy have a higher risk of cryptorchidism and a lower risk of hypospadias. Using Danish register-based data, we revisited these findings with a cohort and sibling-matched design to investigate the potential effect of shared time-stable factors.
Patients and Methods: For the cohort study, we included 823,670 live-born, singleton boys born from 1991 to 2016. Crude and adjusted hazard ratios (HRs) with 95% confidence intervals (CIs) were estimated using Cox regression models for each genital anomaly according to maternal cigarette smoking during pregnancy. For the sibling-matched design, we included 399,258 brothers and used a stratified Cox regression model creating family-adjusted results.
Results: In the cohort study, we found a higher risk of cryptorchidism (aHR = 1.18, 95% CI: 1.12, 1.24) and a lower risk of hypospadias (aHR = 0.84, 95% CI: 0.76, 0.93) when comparing boys exposed to cigarette smoking with non-exposed, and for increasing numbers of cigarettes smoked. In comparison, the sibling-matched analyses suggested a slightly weaker association for cryptorchidism and an association of similar magnitude for hypospadias, both in the same direction as in the cohort study.
Conclusion: Shared, familial confounding does not seem to explain earlier findings of higher risk of cryptorchidism and lower risk of hypospadias.
Keywords: cryptorchidism, hypospadias, epidemiology, fetal development
Introduction
Cryptorchidism (uni- or bilaterally undescended testis) and hypospadias (urethral meatus displacement) are the two most common genital anomalies in boys,1,2 but their etiologies remain unclear.3,4 However, they share several prenatal risk factors, including being born small for gestational age and preterm delivery,5,6 and studies suggest multifactorial mechanisms.7,8
Several predominantly small studies show no association between maternal cigarette smoking during pregnancy and cryptorchidism.9,10 However, large-scale epidemiological studies and three meta-analyses report a higher risk of cryptorchidism in boys exposed to cigarette smoking in fetal life compared to unexposed boys.9–12 Although some studies report no association between maternal cigarette smoking and hypospadias,9,13,14 several studies show lower risk among boys exposed to cigarette smoking in fetal life than unexposed.15–17 This was also supported by a large meta-analysis from 2011.9 These findings remain puzzling, as the many, shared risk factors for cryptorchidism and hypospadias suggest a common etiology. Since maternal smoking has been associated with most common birth complications,18 it raises the important question of whether the observed inverse association for hypospadias is causal or a result of confounding from time-stable familial factors such as social, genetic, and environmental factors.19
We hypothesized that maternal cigarette smoking during pregnancy increases the risk of both cryptorchidism and hypospadias and that the opposing associations previously found are due to confounding, possibly from time-stable familial factors.
Using large Danish register-based data, we performed a cohort and sibling-matched design study to explore the associations between maternal cigarette smoking cryptorchidism and hypospadias, and to investigate the potential confounding from time-stable familial factors.
Methods
Study Population and Data Sources
The study population consisted of all live-born, singleton boys born in Denmark between January 1st, 1991, and December 31st, 2016 (N = 823,670). They were identified in the Danish Medical Birth Register (MBR) which contains information on all births in Denmark.20 All Danish residents are given a unique Civil Registration (CPR) number at birth or immigration.21 This allowed for individual-level linkage between the MBR and The Danish National Patient Registry (DNPR), which holds data on all hospital admissions and visits in Denmark including surgical codes22 and The Integrated Database for Labor Market Research (IDA) at Statistics Denmark, which includes information on educational level.23
Ascertainment of Exposure
From 1991 to 1996, cigarette smoking during pregnancy was registered in the MBR by midwives, either as non-smoker or smoker based on self-reports by the pregnant woman at the first antenatal care visit during week 16 or 17 of gestation. From 1997, smoking status registration changed to several categories: non-smoker, smoking cessation in 1st trimester, smoking cessation after 1st trimester, ≤5 cigarettes/day, 6–10 cigarettes/day, 11–20 cigarettes/day, ≥21 cigarettes/day and amount unknown.24 Based on these data, we created two main exposure variables of interest. First, using data for the whole study period (1991–2016), we divided the exposure status into three categories: non-smoker, stopped during pregnancy, and smoker. Smoking cessation during pregnancy was only available from 1997 onwards, but we included this category in all analyses to broaden the exposure contrast. Second, using data from 1997–2016, we divided the exposure status into six categories: non-smoker, stopped during pregnancy, ≤5cigarettes/day, 6–10cigarettes/day, 11–20cigarettes/day, and ≥21cigarettes/day. Throughout the manuscript, we will refer to these as “the 3-categorized exposure variable” and “the 6-categorized exposure variable”.
Ascertainment of Male Genital Anomalies
Information on cryptorchidism and hypospadias was available through the DNPR, using the International Classification of Disease (ICD) codes. ICD-8 was in use from 1978 to 1993, and ICD-10 has been in use from 1994 onwards. Boys were considered to have cryptorchidism if one of the following ICD codes were registered: ICD-8: 75210, 75211, or 75219 or ICD-10: Q53, Q531, Q531A, Q532, Q532A, or Q539, who also received a code for relevant corrective surgery (Surgery and Treatment Classification of the National Board of Health: 55600 or 55640, or Nordic Classification of Surgical Procedures: KFH100, KFH01, or KFH10).25 Boys were considered to have hypospadias if one of the following ICD codes were registered: ICD-8: 75220, 75221, 75222, 75228, 75229, or ICD-10: Q54, Q540, Q541, Q542, Q543, Q548, or Q549.
Ascertainment of Covariates
Based on existing literature, we made decisions on potential confounders to be included in our models for both study designs by drawing directed acyclic graphs (DAGs)26, (Supplementary Figures 1 and 2. Information on maternal diabetes was available from the DNPR and was defined as type 1 diabetes (ICD−8: 249; ICD−10 E10, O240), type 2 diabetes (ICD−8: 25; ICD−10: E11, O241), or gestational diabetes (ICD−8: 63474, Y6449; ICD−10: O244, O240). Information on maternal age, gestational age, birth weight, and parity was available within the MBR. Information on pre-pregnancy body mass index (BMI, kg/m2) was available from 2004 in the MBR.24 Maternal nationality was available from Statistics Denmark. Information on years of education was available from IDA at Statistics Denmark. The categorization of variables included in the cohort design is presented in Table 1. Birthweight z-scores were created for a sensitivity analysis based on relevant intrauterine growth curves.27
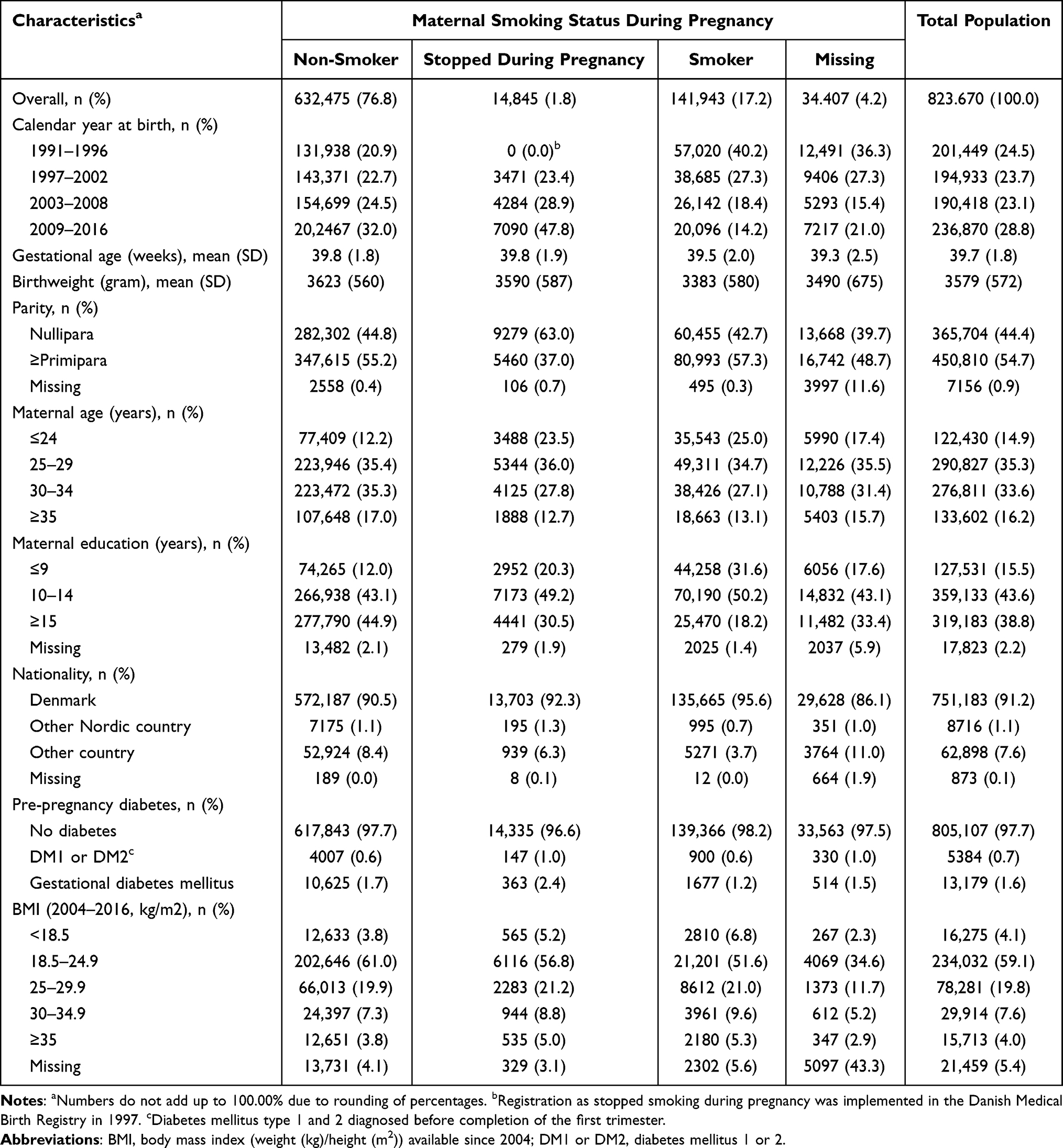 |
Table 1 Maternal and Infant Characteristics According to Maternal Smoking During Pregnancy Among 823,670 Danish Singleton Boys Born in Denmark, 1991–2016 |
Statistical Analyses
We applied multiple imputations with chained equations to account for missing data on covariates and imputed 20 datasets28, (Supplementary file 1). In the cohort design, we accounted for time to diagnosis with a Cox proportional model, estimating both crude and adjusted hazard ratios (HRs) with 95% confidence intervals (CIs) across levels of exposure for both the 3-categorized and the 6-categorized exposure variable. We used the boys’ age as the underlying time scale and followed them until a diagnosis of cryptorchidism or hypospadias, death, emigration, or end of follow-up (December 31st, 2016). The following variables were included in the regression model: calendar year at birth, maternal years of education, parity, maternal age at birth, nationality, and maternal diabetes. Robust standard errors were applied to account for the clustering of siblings. In the sibling-matched design, we used stratified Cox regression, creating separate strata for all sibling pairs of two or more brothers by the unique maternal identifier. This design makes within-family comparisons of exposure and outcome, accounting for shared familial factors, both observed and unobserved.29 Thus, we adjusted only for calendar year at birth, parity, maternal age at birth, and maternal diabetes. We assessed the proportional hazards assumptions with adjusted log-log plots for all models, and the data were compatible with these assumptions (data not shown).
Sensitivity Analyses
We performed five sensitivity analyses. First, we repeated all cohort design analyses with restriction to boys with complete data to compare the results with those obtained from the imputed data used in the main cohort design. Second, we further adjusted for maternal BMI in the cohort design with both exposures, as maternal BMI has been associated with an increased risk of cryptorchidism and hypospadias30 and may act as a potential confounder. Maternal BMI was only available and valid from 2004 in the MBR,24 thus, we adjusted for maternal BMI in the subset of all boys born from 2004 to 2016. Third, we further adjusted the cohort design analyses with the 3-categorized exposure for birthweight z-scores, as being born small for gestational age has been strongly associated with both genital anomalies19 and may act as an important mediator. However, conditioning on birth weight might create severe collider stratification bias.31 Thus, we decided a priori to only adjust for birthweight z-scores in a sensitivity analysis. Fourth, for the 3-categorized exposure, we restricted the cohort to siblings to explore potential selection problems in the sibling-matched design. Fifth, the sibling-matched design assumes no carry-over effects, ie, the outcome of the first sibling does not affect the exposure of the next sibling. Therefore, we tested for carry-over effect between genital anomalies of the firstborn sibling (independent variable: yes, no) and maternal cigarette smoking during the subsequent pregnancy (dependent variable: non-smoker, smoker), using logistic regression models.29 We adjusted for maternal cigarette smoking during the first pregnancy, calendar year of birth of both siblings, maternal age, nationality, and years of education. All statistical analyses were performed in STATA/MP 15.1 (StataCorp LLC, College Station, Texas).
Results
Between 1991 and 2016, 823,670 singleton boys of 607,999 mothers were born in Denmark and included in this study. The average (range) follow-up time was 12.7 (0–25.9) years. Of the participants, 141,943 (18.0%) had mothers, who smoked cigarettes during pregnancy, whereas 14,845 (1.9%) had mothers, who stopped smoking during pregnancy. In total, 20,870 (2.5%) boys were diagnosed with cryptorchidism. Among these, 11,509 boys (1.4%) were also registered with a surgical code for orchiopexy with a mean (range) age of 4.0 (0–23.0) years at first diagnosis. A total of 4296 boys (0.6%) were diagnosed with hypospadias with a mean age (range) of 1.8 (0–25.0) years at first diagnosis. Characteristics of the study population are presented in Table 1.
The total population for the sibling-matched design consisted of 399,258 brothers. In total, 18,480 sibling pairs were discordant for their mother’s smoking status. Further, 5036 and 2007 sibling pairs were discordant for cryptorchidism and hypospadias. For cryptorchidism, 324 sibling pairs were discordant for both smoking status and cryptorchidism. For hypospadias, 105 sibling pairs were discordant for both smoking status and hypospadias.
Cohort Design
Using the 3-categorized exposure variable, fetal cigarette smoking exposure was associated with a higher risk of cryptorchidism (aHR = 1.18, 95% CI: 1.12, 1.24) and a lower risk of hypospadias (aHR = 0.84, 95% CI: 0.76, 0.93) compared to boys of non-smoking mothers (Tables 2 and 3). Using the 6-categorized exposure variable, an increasing number of cigarettes smoked was generally associated with an increased risk of cryptorchidism and decreasing risk of hypospadias. For cryptorchidism, those exposed to the highest level of cigarettes per day (≥21), had the highest risk of cryptorchidism (aHR = 1.34, 95% CI: 1.04, 1.73). For hypospadias, those exposed to ≥21 cigarettes/day had the lowest risk (aHR = 0.65, 95% CI: 0.37, 1.16), however with wide 95% CIs overlapping the null for all exposure groups.
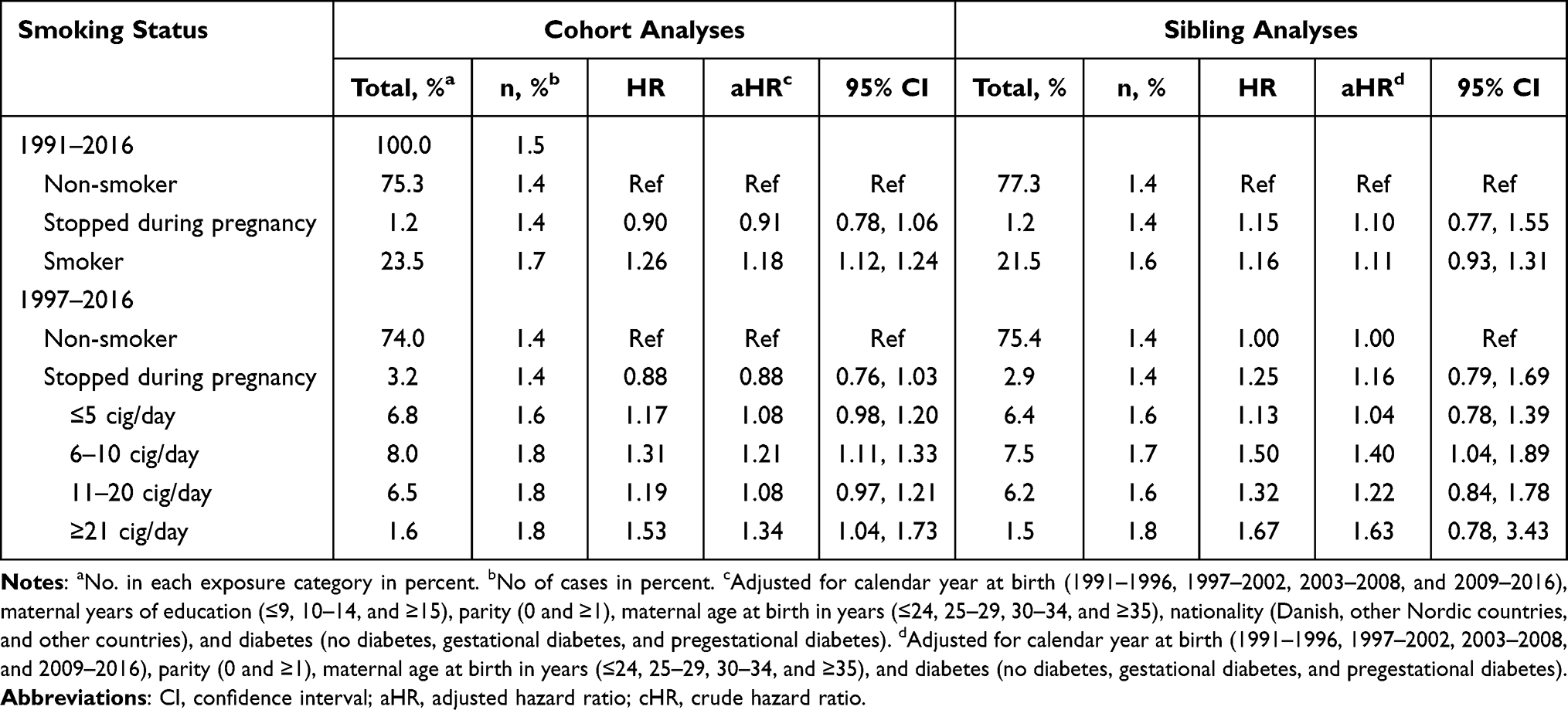 |
Table 2 Hazard Ratios with 95% Confidence Intervals for Cryptorchidism According to Maternal Cigarette During Pregnancy Among 823,670 Danish Singleton Boys Born in Denmark, 1991–2016 |
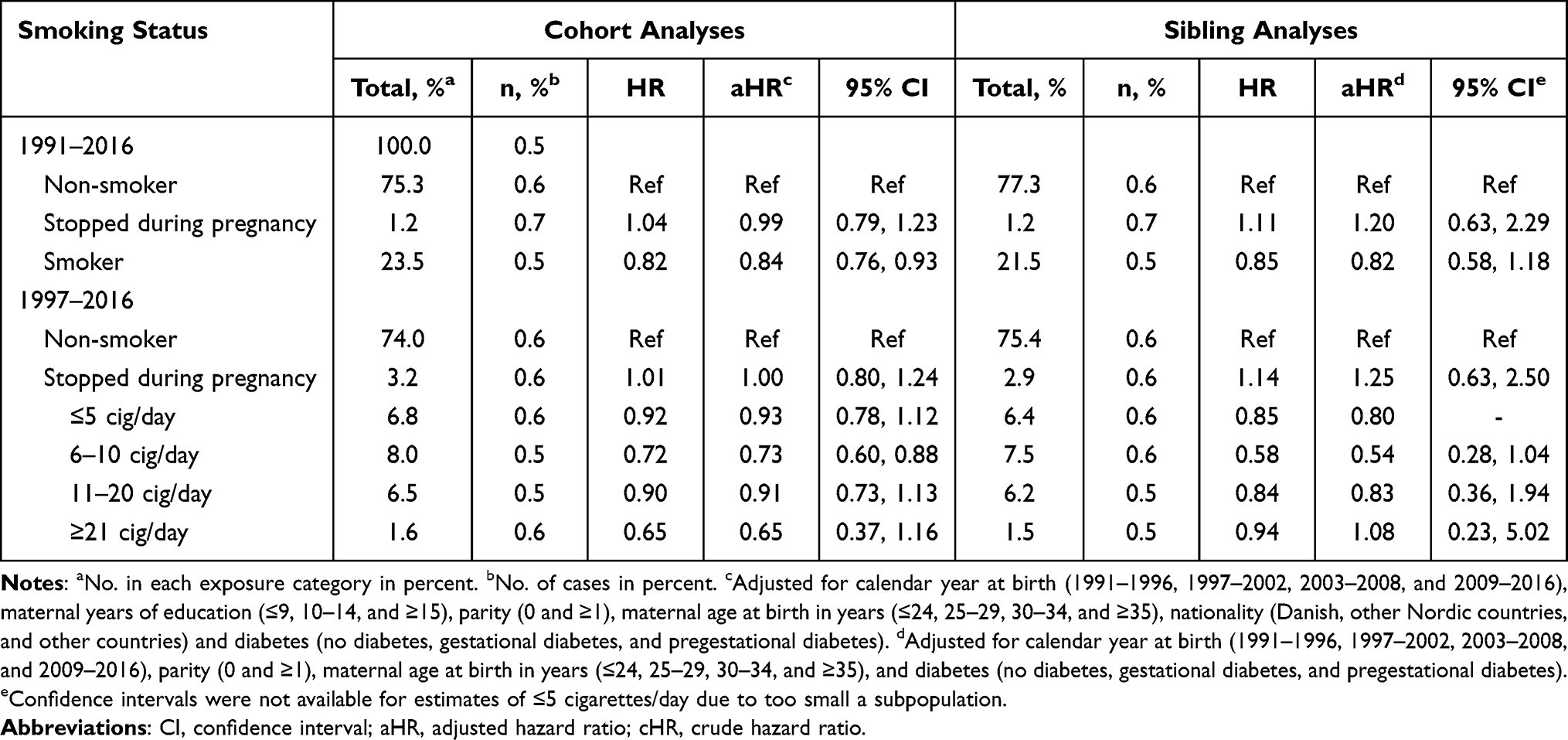 |
Table 3 Hazard Ratios with 95% Confidence Intervals for Hypospadias According to Maternal Cigarette During Pregnancy Among 823,670 Danish Singleton Boys Born in Denmark, 1991–2016 |
Sibling Design
For the 3-categorized exposure, we found a tendency toward a higher risk of cryptorchidism (aHR = 1.11, 95% CI: 0.77, 1.55), and a lower risk of hypospadias (aHR = 0.82, 95% CI: 0.58; 1.18) among those, whose mothers smoked during pregnancy, compared to those unexposed (Tables 2 and 3). The analyses with the 6-categorized exposure variable showed the same tendency of a dose-response relationship; however, most 95% CIs overlapped the null. The highest risk of cryptorchidism was observed among those, whose mothers smoked ≥21 cigarettes/day (aHR = 1.63, 95% CI: 0.78, 3.43). For hypospadias, the risk decreases with levels of exposure up until 6–10 cigarettes per day (aHR = 0.54, 95% CI: 0.28, 1.04) and increases for higher levels of exposure. However, all estimates had 95% CIs overlapping the null for all exposure groups.
Sensitivity Analyses
First, the complete case analyses yielded similar results compared to the main cohort design (Supplementary Table 1). Second, adjusting for maternal BMI in the years 2004–2016 attenuated the results, most notably for cryptorchidism, where the aHR for smoking ≥21 cigarettes/day was 1.15 (95% CI: 0.77, 1.72) (Supplementary Table 2). Third, adjusting for birthweight z-scores with the 3-categorized exposure resulted in slightly lower HRs for cryptorchidism (aHR = 1.11, 95% CI: 1.05, 1.16) and for hypospadias (aHR = 0.74, 95% CI: 0.67, 0.82) (Supplementary Table 3). Fourth, when restricting the cohort to only include siblings, we found comparable results (Supplementary Table 3). Finally, when investigating the presence of a carry-over effect, we obtained adjusted odds ratios (ORs) approximate to 1 for both cryptorchidism and hypospadias, indicating no carry-over effect (Supplementary Table 4).
Discussion
In the cohort design, we replicated the earlier findings of a higher risk of cryptorchidism and a lower risk of hypospadias among boys exposed to cigarette smoking during pregnancy. In the sibling-matched design, we found comparable but attenuated results for cryptorchidism, suggesting that previous findings may be slightly overestimated, but not largely affected by confounding from familial time-stable factors. For hypospadias, results from the sibling-matched design also showed a lower risk among boys of mothers, who smoked during pregnancy. This suggests that shared, time-stable familial factors do not explain the observed inverse association between smoking and hypospadias. However, almost all estimates in the sibling-matched design had CIs overlapping the null.
The majority of existing studies show no association between maternal cigarette smoking and cryptorchidism,10,32–34 which could be due to their predominantly small study populations. However, three meta-analyses have found a small increased risk.9,10,12 In 2018, Yu et al included only crude estimates from 20 studies and found a pooled OR of 1.18 (95% CI: 1.12; 1.24),10 but the two earlier studies included adjusted estimates whenever possible and found similar results.9,12 Further, both performed sensitivity analyses testing their estimates with pooled ORs of only adjusted estimates and found similar results.
Most studies on maternal cigarette smoking during pregnancy and hypospadias report no association.13,14,35,36 However, our findings are consistent with those of four large case-control studies.15,16,37,38 A meta-analysis by Hackshaw et al included 15 studies on hypospadias, and reported a lower risk of hypospadias (pooled OR 0.90, 95% CI: 0.85; 0.95).9
A Danish study on hypospadias by Leite et al in 2014 found no association (aOR = 0.94, 95% CI: 0.83, 1.06).39 The study used the same registers and case definitions but registered all women as either never smokers or ever smokers and included fewer observations, which could explain this finding.
A major strength of our study is the use of Danish health care registers. Since the Danish Health Care System is free and accessible to all Danish residents,40 selection bias due to non-participation is minimal. The outcome definitions used were based on recent Danish validations studies, showing high positive predictive values for both genital anomalies.25,41
The study also had limitations. Since only live births were included and maternal cigarette smoking is well-known to increase the risk of miscarriage,18 different fetal survival rates between exposure groups may have resulted in selection bias, ie, live-birth bias.42 Information on maternal cigarette smoking was based on self-reports, which may have been affected by underreporting. Further, information on second-hand smoking and other smoking habits was not available. However, since the information was reported before the outcome, the potential misclassification would most likely be non-differential. A large, Norwegian cohort study compared self-reported smoking information from pregnant women with plasma cotinine levels (a sensitive marker of tobacco smoking) and indicated that self-reported smoking is a valid marker for tobacco exposure.43 Still, other studies have reported misclassification among occasional smokers when comparing self-reports with serum-cotinine levels.44,45
The Danish Health Care Authority recommends all health care staff pay extra attention to children exposed to prenatal smoking,46 which might result in earlier detection of genital anomalies in boys of smoking mothers. However, we found no evidence of such detection bias in our model-based log-log plots. Further, with the long follow-up time available, it is unlikely that detection bias can explain our findings, as previously described.47
We lacked information on alcohol intake during pregnancy, which was a priori identified as a potential confounder, and any resulting confounding cannot be excluded. Maternal BMI has been associated with a higher risk of both genital anomalies and was a priori identified as a possible confounder.17,30 However, the information was only available and valid in the MBR from 2004 onwards.24 Adjusting for maternal BMI in the subpopulation with available data resulted in attenuated associations, suggesting that BMI might have confounded our results to some extent. We used maternal educational level as a proxy for socioeconomic status and thus, we cannot rule out the possibility of residual confounding. We considered growth restriction as an intermediate factor. Adjusting for birthweight z-scores in the sensitivity analyses lowered the aHRs of both cryptorchidism and hypospadias, supporting this assumption.
Our sensitivity analyses showed that the sibling population was representative of the whole cohort and showed no sign of carry-over effects. However, the sibling-matched design risks amplification of confounding bias from unadjusted, non-shared factors.48 While we did adjust for several measured, non-shared covariates, we cannot exclude that important, non-shared confounders were not accounted for. Further, the possible non-differential misclassification of smoking status may cause an even stronger bias towards the null in the sibling-matched design than in the cohort design.
We replicated the findings from previous studies of a higher risk of cryptorchidism and a lower risk of hypospadias among boys exposed in utero to cigarette smoking compared to unexposed boys. The diverging findings for cryptorchidism and hypospadias in our and previous studies are puzzling, as the two anomalies share many prenatal risk factors, suggesting a partly common etiology. Our results do not support our hypothesis that these diverging results are due to unadjusted, familial confounding, but it remains unknown, whether the association between maternal smoking during pregnancy and hypospadias is causal.
A possible explanation can be derived from the different effects of cigarette smoking on the in utero environment. Cigarette smoking inhibits the enzyme placental aromatase, which converts testosterone into estrogen.49 This will decrease the fetal bioavailability of estrogen while increasing the bioavailability of testosterone,50 which may lower the risk of both anomalies.3,51 However, cigarette smoking also increases the risk of preterm delivery and induces fetal growth restriction,18 which are well-known risk factors for cryptorchidism. Hence, cigarette smoking may increase the risk of cryptorchidism through this mechanism. On the other, fetal growth restriction induced by cigarette smoking probably occurs later in pregnancy well after the fusion of the urethral folds has ended. Hence, cigarette smoking may have a protective effect on hypospadias owing to its inhibition of placental aromatase. To further investigate the possible association between smoking during pregnancy and both anomalies, future studies should investigate the possible anti-estrogenic effects and interactions of maternal lifestyle factors on the risk of cryptorchidism and hypospadias to better understand their exact etiology.
Conclusion
In this large, register-based study cohort and sibling-matched design study, maternal cigarette smoking during pregnancy was associated with a higher risk of cryptorchidism and a lower risk of hypospadias. Based on the results from the sibling-matched design, the apparently opposing associations for cryptorchidism and hypospadias cannot be explained by time-stable, familial confounding. Future studies should explore this and other possible causal mechanisms further to disentangle the causal links of this research area.
Abbreviations
MBR, Danish Medical Birth Register; CPR, Civil Registration; DNPR, Danish National Patient Registry; IDA, Integrated Database for Labor Market Research; ICD, International Classification of Disease; DAG, directed acyclic graphs; BMI, body mass index; HR, hazard ratios; CI, confidence interval; aHR, adjusted hazard ratio; OR, odds ratio.
Data Sharing Statement
The dataset analyzed in the study is not publicly available due to national data security legislation on sensitive personal data.
Ethics Approval
The study was conducted after approval by the Danish Data Protection Agency (No.2013-41-1964). According to Danish legislation, informed consent or approval by an independent review board is not necessary for register-based research on encrypted data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Novo Nordisk Foundation (grant reference number NNF19OC0058463).
Disclosure
Mr Daniel Lindbo reports grants from Novo Nordisk, during the conduct of the study. Professor Cecilia Høst Ramlau-Hansen reports grants from Novo Nordisk Foundation, during the conduct of the study; grants from Independent Research Fund Denmark, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Sijstermans K, Hack WW, Meijer RW, van der Voort-Doedens LM. The frequency of undescended testis from birth to adulthood: a review. Int J Androl. 2008;31(1):1–11. doi:10.1111/j.1365-2605.2007.00770.x
2. Springer A, van den Heijkant M, Baumann S. Worldwide prevalence of hypospadias. J Pediatr Urol. 2016;12(3):152 e151–157. doi:10.1016/j.jpurol.2015.12.002
3. van der Horst HJ, de Wall LL. Hypospadias, all there is to know. Eur J Pediatr. 2017;176(4):435–441. doi:10.1007/s00431-017-2864-5
4. Lee PA, Houk CP. Cryptorchidism. Curr Opin Endocrinol Diabetes Obes. 2013;20(3):210–216. doi:10.1097/MED.0b013e32835ffc7d
5. Akre O, Lipworth L, Cnattingius S, Sparen P, Ekbom A. Risk factor patterns for cryptorchidism and hypospadias. Epidemiology. 1999;10(4):364–369. doi:10.1097/00001648-199907000-00005
6. Jensen MS, Wilcox AJ, Olsen J, et al. Cryptorchidism and hypospadias in a cohort of 934,538 Danish boys: the role of birth weight, gestational age, body dimensions, and fetal growth. Am J Epidemiol. 2012;175(9):917–925. doi:10.1093/aje/kwr421
7. Main KM, Skakkebaek NE, Virtanen HE, Toppari J. Genital anomalies in boys and the environment. Best Pract Res Clin Endocrinol Metab. 2010;24(2):279–289. doi:10.1016/j.beem.2009.10.003
8. van der Zanden LF, van Rooij IA, Feitz WF, Franke B, Knoers NV, Roeleveld N. Aetiology of hypospadias: a systematic review of genes and environment. Hum Reprod Update. 2012;18(3):260–283. doi:10.1093/humupd/dms002
9. Hackshaw A, Rodeck C, Boniface S. Maternal smoking in pregnancy and birth defects: a systematic review based on 173 687 malformed cases and 11.7 million controls. Hum Reprod Update. 2011;17(5):589–604. doi:10.1093/humupd/dmr022
10. Yu C, Wei Y, Tang X, et al. Maternal smoking during pregnancy and risk of cryptorchidism: a systematic review and meta-analysis. Eur J Pediatr. 2018;178:287–297. doi:10.1007/s00431-018-3293-9
11. Kjersgaard C, Arendt LH, Ernst A, et al. Lifestyle in pregnancy and cryptorchidism in sons: a study within two large Danish birth cohorts. Clin Epidemiol. 2018;10:311–322. doi:10.2147/CLEP.S150657
12. Zhang L, Wang XH, Zheng XM, et al. Maternal gestational smoking, diabetes, alcohol drinking, pre-pregnancy obesity and the risk of cryptorchidism: a systematic review and meta-analysis of observational studies. PLoS One. 2015;10(3):e0119006. doi:10.1371/journal.pone.0119006
13. Kovalenko AA, Brenn T, Odland JO, Nieboer E, Krettek A, Anda EE. Risk factors for hypospadias in Northwest Russia: a Murmansk County birth registry study. PLoS One. 2019;14(4):e0214213. doi:10.1371/journal.pone.0214213
14. Xu LF, Liang CZ, Lipianskaya J, et al. Risk factors for hypospadias in China. Asian J Androl. 2014;16(5):778–781. doi:10.4103/1008-682X.131704
15. Winston JJ, Meyer RE, Emch ME. Geographic analysis of individual and environmental risk factors for hypospadias births. Birth Defects Res a Clin Mol Teratol. 2014;100(11):887–894. doi:10.1002/bdra.23306
16. Rodriguez-Pinilla E, Mejias C, Prieto-Merino D, Fernandez P, Martínez-Frías, ML. Risk of hypospadias in newborn infants exposed to valproic acid during the first trimester of pregnancy: a case-control study in Spain. Drug Saf. 2008;31(6):537–543. doi:10.2165/00002018-200831060-00008
17. Carmichael SL, Shaw GM, Laurent C, Olney RS, Lammer EJ; National Birth Defects Prevention Study. Maternal reproductive and demographic characteristics as risk factors for hypospadias. Paediatr Perinat Epidemiol. 2007;21(3):210–218. doi:10.1111/j.1365-3016.2007.00809.x
18. Cnattingius S. The epidemiology of smoking during pregnancy: smoking prevalence, maternal characteristics, and pregnancy outcomes. Nicotine Tob Res. 2004;6(Suppl 2):S125–140. doi:10.1080/14622200410001669187
19. Hakonsen LB, Ernst A, Ramlau-Hansen CH. Maternal cigarette smoking during pregnancy and reproductive health in children: a review of epidemiological studies. Asian J Androl. 2014;16(1):39–49. doi:10.4103/1008-682X.122351
20. Knudsen LB, Olsen J. The Danish medical birth registry. Dan Med Bull. 1998;45(3):320–323.
21. Pedersen CB. The Danish civil registration system. Scand J Public Health. 2011;39(7 Suppl):22–25. doi:10.1177/1403494810387965
22. Lynge E, Sandegaard JL, Rebolj M. The Danish national patient register. Scand J Public Health. 2011;39(7 Suppl):30–33. doi:10.1177/1403494811401482
23. Petersson F, Baadsgaard M, Thygesen LC. Danish registers on personal labour market affiliation. Scand J Public Health. 2011;39(7 Suppl):95–98. doi:10.1177/1403494811408483
24. Bliddal M, Broe A, Pottegard A, Olsen J, Langhoff-Roos J. The Danish medical birth register. Eur J Epidemiol. 2018;33(1):27–36. doi:10.1007/s10654-018-0356-1
25. Jensen MS, Snerum TM, Olsen LH, et al. Accuracy of cryptorchidism diagnoses and corrective surgical treatment registration in the Danish national patient registry. J Urol. 2012;188(4):1324–1329. doi:10.1016/j.juro.2012.06.045
26. Robins JM, Hernán MA, Brumback B. Marginal structural models and causal inference in epidemiology. Epidemiology. 2000;11(5):550–560. doi:10.1097/00001648-200009000-00011
27. Maršál K, Persson P-H, Larsen T, Lilja H, Selbing A, Sultan B. Intrauterine growth curves based on ultrasonically estimated foetal weights. Acta Paediatr. 1996;85(7):843–848. doi:10.1111/j.1651-2227.1996.tb14164.x
28. Sterne JA, White IR, Carlin JB, et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ. 2009;338:b2393. doi:10.1136/bmj.b2393
29. Sjolander A, Frisell T, Kuja-Halkola R, Oberg S, Zetterqvist J. Carryover effects in sibling comparison designs. Epidemiology. 2016;27(6):852–858. doi:10.1097/EDE.0000000000000541
30. Arendt LH, Ramlau-Hansen CH, Lindhard MS, et al. Maternal overweight and obesity and genital anomalies in male offspring: a population-based Swedish cohort study. Paediatr Perinat Epidemiol. 2017;31(4):317–327. doi:10.1111/ppe.12373
31. Wilcox AJ, Weinberg CR, Basso O. On the pitfalls of adjusting for gestational age at birth. Am J Epidemiol. 2011;174(9):1062–1068. doi:10.1093/aje/kwr230
32. McGlynn KA, Graubard BI, Klebanoff MA, Longnecker MP. Risk factors for cryptorchism among populations at differing risks of testicular cancer. Int J Epidemiol. 2006;35(3):787–795. doi:10.1093/ije/dyl024
33. Shiono PH, Klebanoff MA, Berendes HW. Congenital malformations and maternal smoking during pregnancy. Teratology. 1986;34(1):65–71. doi:10.1002/tera.1420340109
34. Zakaria M, Azab S, El Baz M, Fawaz L, Bahagat A. Cryptorchidism in Egyptian neonates. J Pediatr Urol. 2013;9(6Pt A):815–819. doi:10.1016/j.jpurol.2012.10.024
35. Akre O, Boyd HA, Ahlgren M, et al. Maternal and gestational risk factors for hypospadias. Environ Health Perspect. 2008;116(8):1071–1076. doi:10.1289/ehp.10791
36. Carmichael SL, Shaw GM, Laurent C, Lammer EJ, Olney RS; National Birth Defects Prevention Study. Hypospadias and maternal exposures to cigarette smoke. Paediatr Perinat Epidemiol. 2005;19(6):406–412. doi:10.1111/j.1365-3016.2005.00680.x
37. Carmichael SL, Ma C, Shaw GM; National Birth Defects Prevention Study. Maternal smoking, alcohol, and caffeine exposures and risk of hypospadias. Birth Defects Res. 2017;109(14):1127–1133. doi:10.1002/bdr2.1044
38. Kallen K. Role of maternal smoking and maternal reproductive history in the etiology of hypospadias in the offspring. Teratology. 2002;66(4):185–191. doi:10.1002/tera.10092
39. Leite M, Albieri V, Kjaer SK, Jensen A. Maternal smoking in pregnancy and risk for congenital malformations: results of a Danish register-based cohort study. Acta Obstet Gynecol Scand. 2014;93(8):825–834. doi:10.1111/aogs.12433
40. Schmidt M, Schmidt SAJ, Adelborg K, et al. The Danish health care system and epidemiological research: from health care contacts to database records. Clin Epidemiol. 2019;11:563–591. doi:10.2147/CLEP.S179083
41. Arendt LH, Ernst A, Lindhard MS, et al. Accuracy of the hypospadias diagnoses and surgical treatment registrations in the Danish national patient register. Clin Epidemiol. 2017;9:483–489. doi:10.2147/CLEP.S143118
42. Liew Z, Olsen J, Cui X, Ritz B, Arah OA. Bias from conditioning on live birth in pregnancy cohorts: an illustration based on neurodevelopment in children after prenatal exposure to organic pollutants. Int J Epidemiol. 2015;44(1):345–354. doi:10.1093/ije/dyu249
43. Kvalvik LG, Nilsen RM, Skjærven R, et al. Self-reported smoking status and plasma cotinine concentrations among pregnant women in the Norwegian mother and child cohort study. Pediatr Res. 2012;72(1):101–107. doi:10.1038/pr.2012.36
44. Klebanoff MA, Levine RJ, Morris CD, et al. Accuracy of self-reported cigarette smoking among pregnant women in the 1990s. Paediatr Perinat Epidemiol. 2001;15(2):140–143. doi:10.1046/j.1365-3016.2001.00321.x
45. Nafstad P, Kongerud J, Botten G, et al. Fetal exposure to tobacco smoke products: a comparison between self-reported maternal smoking and concentrations of cotinine and thiocyanate in cord serum. Acta Obstet Gynecol Scand. 1996;75(10):902–907. doi:10.3109/00016349609055025
46. Danish Health Authority (2013). Recommendations for Maternity Care.
47. Arendt LH, Lindhard MS, Henriksen TB, et al. Maternal diabetes mellitus and genital anomalies in male offspring: a nationwide cohort study in 2 Nordic countries. Epidemiology. 2018;29(2):280–289. doi:10.1097/EDE.0000000000000781
48. Frisell T, Oberg S, Kuja-Halkola R, Sjolander A. Sibling comparison designs: bias from non-shared confounders and measurement error. Epidemiology. 2012;23(5):713–720. doi:10.1097/EDE.0b013e31825fa230
49. Marom-Haham L, Shulman A. Cigarette smoking and hormones. Curr Opin Obstet Gynecol. 2016;28(4):230–235. doi:10.1097/GCO.0000000000000283
50. Toriola AT, Vaarasmaki M, Lehtinen M, et al. Determinants of maternal sex steroids during the first half of pregnancy. Obstet Gynecol. 2011;118(5):1029–1036. doi:10.1097/AOG.0b013e3182342b7f
51. Agoulnik AI. Cryptorchidism–an estrogen spoil? J Clin Endocrinol Metab. 2005;90(8):4975–4977. doi:10.1210/jc.2005-1290
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.