Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Mapping Real-World Data to Self-Reported Information to Explore Determinants of Location Selection for Community Pharmacies in Taiwan
Authors Chen J, Huang YM ![]() , Chan HY
, Chan HY ![]() , Chen MC, Ho YF
, Chen MC, Ho YF ![]()
Received 9 March 2023
Accepted for publication 31 March 2023
Published 7 April 2023 Volume 2023:16 Pages 971—981
DOI https://doi.org/10.2147/JMDH.S409643
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jie Chen,1,* Yen-Ming Huang,1– 3,* Hsun-Yu Chan,4 Mon-Chiao Chen,5 Yunn-Fang Ho1,2
1School of Pharmacy, College of Medicine, National Taiwan University, Taipei, 100025, Taiwan; 2Graduate Institute of Clinical Pharmacy, College of Medicine, National Taiwan University, Taipei, 100025, Taiwan; 3Department of Pharmacy, National Taiwan University Hospital, Taipei, 100229, Taiwan; 4Department of Industrial Education, National Taiwan Normal University, Taipei, 106308, Taiwan; 5Adam’s Drug Store, Taipei, 111049, Taiwan
*These authors contributed equally to this work
Correspondence: Yunn-Fang Ho, Graduate Institute of Clinical Pharmacy, College of Medicine, National Taiwan University, No. 33, Linsen South Road, Zhongzheng District, Taipei, 100025, Taiwan, Tel +886 2 33668794, Fax +886 2 33668780, Email [email protected]
Background: Easy and adequate access to community pharmacies is key to eliminating primary barriers to the utilization of medicines and healthcare services. The location of community pharmacies is important for patients and providers when choosing and opening a pharmacy, but only a handful of studies investigate factors associated with the geographical distribution of pharmacies. This study aimed to identify decisive factors for location selection when starting a pharmacy among districts/townships in Taiwan.
Methods: This cross-sectional mixed mode study employed an explanatory sequential design, beginning with a quantitative analysis of national datasets, and followed by a qualitative analysis of structured interviews. The national data were extracted from the Taiwan government database of 2020, and the qualitative interviews were conducted with 10 community pharmacists through a snowball sampling in 2021. A multiple linear regression was conducted to identify salient predictors of the number of community pharmacies in each of the 368 districts/townships in Taiwan, including population density, median annual household income, number of physician offices, area, and proportion of female residents of each district/township. Ten chief pharmacists were interviewed to share viewpoints on the decision-making process of their selection of current pharmacy practice sites. Inductive thematic analysis was performed to extract factors pertinent to location selection for pharmacy operations and services.
Results: Confirmed by quantitative and qualitative data, population density, numbers of physician offices, median annual household income, pharmacy operation type, and type of retail locations are key determinants for site selection in considering opening a new community pharmacy.
Conclusion: The study uncovers salient factors associated with the choice of community pharmacy location in Taiwan and proposes the adequate number of physician offices that a community pharmacy can collaborate with. In addition, pharmacists should prudently consider if their preferred service features match the needs of residents.
Keywords: community pharmacy, physician office, location, mixed mode
Introduction
Easy access to medicines plays a key role in promoting healthcare for all.1 In recent years, there is a growing interest in utilizing community pharmacies to support holistic care through primary, secondary, and tertiary prevention services.2 In addition to dispensing medications, community pharmacies also offer educational programs,3–5 self-care counseling,6 disease prevention initiatives,7 and wellness programs.8,9 Since 2008, there is a steady growth of community pharmacies in Taiwan, the research site of this study. The number of community pharmacies in Taiwan has risen from 7215 to 8234 between 2008 and 2020, and the 14.1% increase was faster than the population growth (3.5%; Figure 1).10 Providing extended hours of operation, availability of home delivery of medications, and walk-in medication counseling services, community pharmacies are uniquely positioned as more accessible than other healthcare settings.11
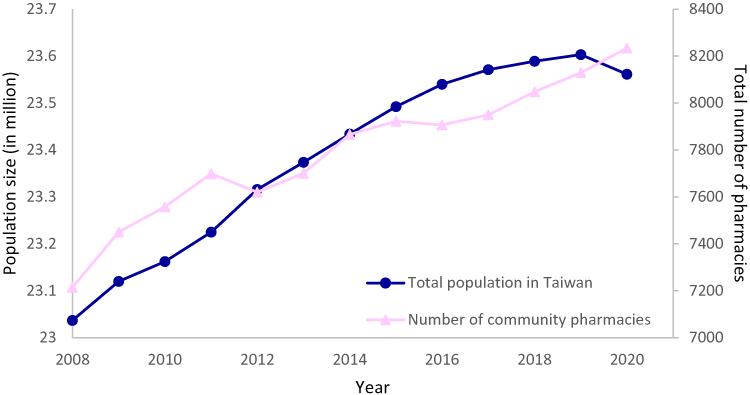 |
Figure 1 Trends of the number of community pharmacies and total population in Taiwan from 2008 to 2020. Notes: Data from the Ministry of Health and Welfare, Taiwan.10 |
Community pharmacies also bring about real and solid changes in patients’ well-being. Previous studies have indicated that pharmacists, when collaborating with other healthcare professionals, can advance medication safety, promote health, prevent disease, reduce healthcare costs, and improve medication adherence and health outcomes.12 For instance, patients with newly diagnosed chronic diseases receiving medication management interventions from a community pharmacy showed a 3% higher medication adherence, 1.8% fewer hospital admissions, 2.7% fewer emergency room visits, and 0.53 fewer mean outpatient visits than their counterparts.13 As a result, access to community pharmacies complements the ultimate care-for-all ideals of a sound healthcare system by providing individuals with assured delivery of healthcare services and securing patients’ appropriate utilization of medications.14
Ensuring equitable access to quality community pharmaceutical services is one of the preemptive goals of public health policy in Taiwan, particularly for residents in rural areas.15 In the UK, the Department of Health and Social Care considers geographical distribution, distance, and availability of healthcare services as the three primary evaluation criteria of community pharmacy access.16 Geographical availability is measured as the geographical distribution of pharmacies within an area and the ratio of the number of pharmacies to the number of residents. However, literature on the geographical distribution of community pharmacies remains sparse.1 In the US, pharmacy dessert has been used to describe the rarity and inaccessibility within a region.14 In Taiwan, the governmental statistics adopts the UK model to define the density of community pharmacies within a region. Such definition is also aligned with the current scale of health equity in Taiwan.
We also argue that the combination of analyzing government datasets and interviewing practitioners provides the best research approach to answer the research questions. Community pharmacies in Taiwan are privately-owned businesses, generally located in commercial areas and contracted by the National Health Insurance to dispense prescriptions, in addition to revenues generated through the provision of over-the-counter medications and other healthcare items. Given the importance of the location, it is surprising that there is a void of empirical research on the start-up of community pharmacies. Choosing the right location for operating a community pharmacy involves multicriteria decision-making processes, which calls for both quantitative and qualitative methodologies to explore.17 Some qualitative studies in Taiwan pointed out that closeness to business areas and population size of an area determined the expansion of community pharmacies.18–20 However, previous literature presents little quantitative evidence to pinpoint salient variables associated with the location selection of starting a pharmacy.21 Moreover, there are other potentially important factors that have received little attention. We know neither the capacity of a pharmacy to serve adjacent residents within a region nor the distribution of community pharmacies nationwide. Given the hiatus of recent data on the location selection of starting a community pharmacy, this study aimed to use a mixed mode approach to exploring determinants of location selection for community pharmacy operations and services in Taiwan.
Materials and Methods
Study Design
This cross-sectional study utilized an explanatory sequential mixed mode design which comprised a quantitative phase and a subsequent qualitative phase (Figure 2).22 This design involved collecting and analyzing government datasets quantitatively first before exploring the nuanced findings complementary to quantitative results through collecting and analyzing interviews of chief pharmacists qualitatively.23 Such design helps answer the research questions the best because exploring the topics of research interest from participants’ insights would enable researchers to use qualitative data and thematic analyses to further elaborate on the statistically significant findings.24
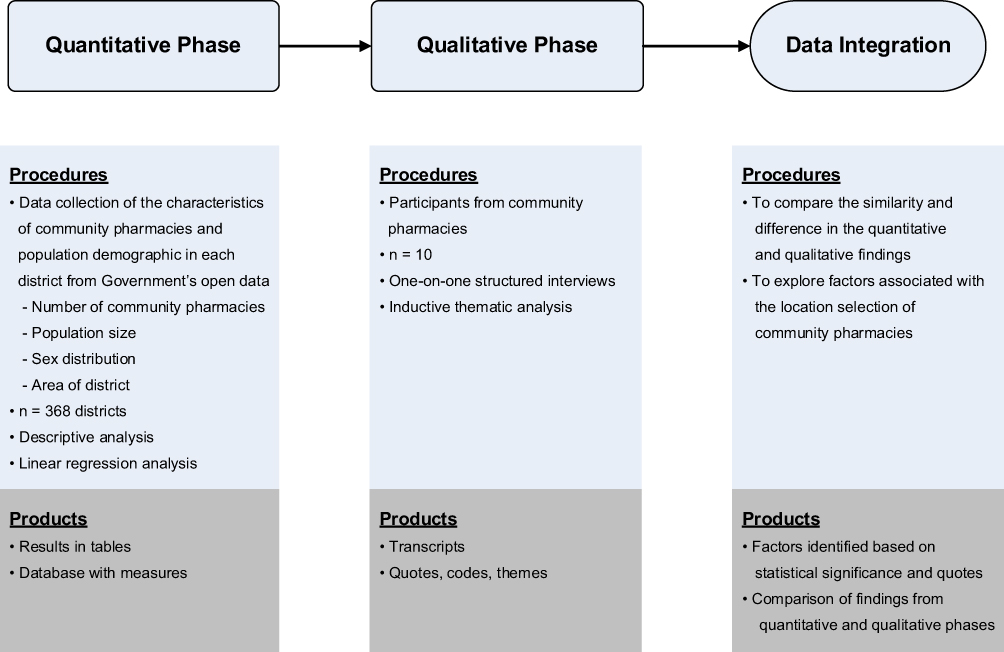 |
Figure 2 Explanatory sequential mixed mode design of the exploration of determinants of the location selection for community pharmacy operations. |
During the quantitative phase of the study, we retrieved public-use data on population demographics and the background information of community pharmacies from the Taiwan Ministry of Health and Welfare 2020 database.25 During the qualitative phase from April to May 2021, we conducted one-on-one interviews to explore the determinants that pharmacists referred to when selecting a practice location in the community setting. Lastly, the findings collected from the qualitative phase were mapped onto the results from the quantitative phase to understand how the findings of the two phases complemented each other. The study protocol was approved by the Research Ethics Committee at the National Taiwan University Hospital (202104014RINC).
Quantitative Phase
Data Source and Collection
There are 22 counties/municipalities, composed of 368 districts/townships, in Taiwan (Table 1). All registered community pharmacies were indexed on the government’s websites and included in the quantitative phase.25 We collected the number of community pharmacies located in each district/township nationwide from the Taiwan Ministry of Health and Welfare.25 The number of physician offices located in each district/township was extracted from the website of the Taiwan Medical Association.26 In addition, the national sociodemographic information of the population (ie, population size, sex distribution, proportion of senior citizens [individuals of 65 years of age and beyond], and size of district) of each district/township was collected from the Department of Household Registration, Ministry of the Interior, Taiwan.27 The median annual household income was retrieved from the website of the Financial Data Center of the Ministry of Finance, Taiwan.28 All data were collected from the latest information reported during study execution.
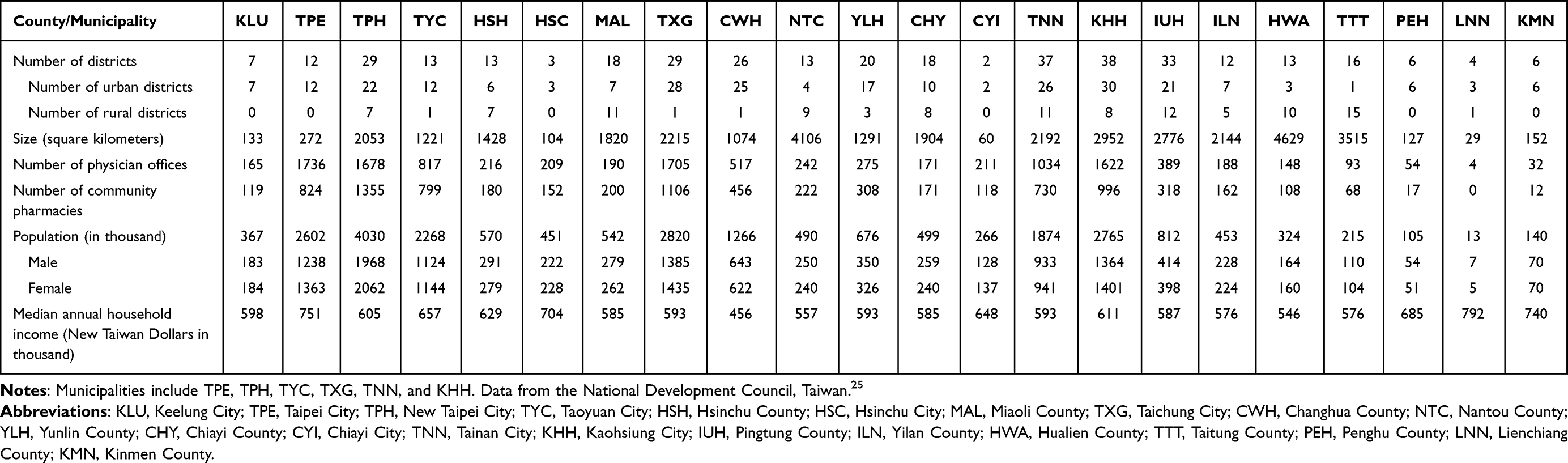 |
Table 1 Descriptive Statistics of the 22 Counties or Municipalities in Taiwan in 2020 |
Data Analysis
Descriptive analysis was used to summarize the population sociodemographics and community pharmacy characteristics. A multiple linear regression model was estimated to identify salient factors that predict the number of community pharmacies in each district. Each district/township was treated as an analytic unit for operating a community pharmacy. We assumed the number of community pharmacies in each district/township as the pharmacists’ preference of location selection for pharmacy operations. In the regression model (n = 368), the outcome variable was the sum of community pharmacies operated in each district/township. The independent variables included the population size, proportion of females, proportion of senior citizens, total number of physician offices located in each district/township, and if the district/township belonged to an urban area. A district/township was defined as urban if it had more than 20,000 individuals registered as residents and a population density of more than 300 residents per square kilometer, otherwise defined as rural.29 All statistical analyses were carried out using SPSS version 28, with the statistical significance level at a two-sided p < 0.05.
Qualitative Phase
Data Source and Collection
Study participants in the qualitative phase were eligible if they were at least 20 years of age, presently being the chief pharmacist in the community pharmacy he or she served, and able to speak Mandarin. Snowball sampling was used to recruit community pharmacists to participate in the study. We also collaborated with the Taichung City New Pharmacist Association to refer community pharmacists to voluntarily partake in the qualitative phase. A one-on-one, in-person structured interview with each participant was conducted to elicit his or her experiences of selecting the location for pharmacy operations. For qualitative interviews, there is no rigid rule of how large the sample size should be.30 A sample size of 9 to 17 is considered sufficient to reach saturation with well-defined study populations.31 A protocol was developed to guide the interview process. The interview questions (Box 1) were developed based on relevant literature and revised by three professionals with expertise in pharmacy practice to ensure the questions were pertinent to the research. The interview questions focused on the participants’ experiences of choosing the location for starting and managing a community pharmacy. All interviews were conducted in quiet office spaces at the community pharmacies, and the interviewer took field notes during each interview.
 |
Box 1 Questions for the Structured Interview of Chief Pharmacists |
Data Analysis
Inductive thematic analysis was conducted to analyze interview transcripts. By using an inductive approach, researchers are not bound to pre-existing theoretical frameworks or preconceptions before data analyses, and the flexibility of this method allows for broader and more extensive analyses of the entire body of data.32,33 Thematic analysis is appropriate to use when seeking to understand a set of thoughts across different individuals and illustrate the commonality related to research questions.33 Hence, researchers are able to find nuances in light of the research questions that go beyond unique experiences from one single individual.33 The analyses were conducted in the following steps: 1) reading and rereading the transcripts three times to be familiar with the data; 2) reading the data line by line to capture key thoughts; 3) generating initial codes to perform coding schemes to search for themes; 4) reviewing, organizing, defining, and naming the themes that were mapped onto the research questions.34,35 The coding process (step 3) consisted of two stages. First, the researchers assigned data chunks to generate main codes and then used both descriptive coding and in vivo coding.36 At this stage, we first summarized the segments of data and condensed large amounts of data into fewer analytic units. At the second stage, pattern coding was used to group these units into a smaller number of categories or themes linking to research questions. We used investigator triangulation to develop an overall coding taxonomy and ensure the trustworthiness of the results.37 For all transcripts, two researchers independently coded the transcripts and came to a consensus on each code and the interpretation to ensure the findings were grounded in the texts. Data saturation was evaluated until no other themes emerged. MAXQDA 12 was used to help organize and categorize the themes.
Results
Quantitative Findings
Of the 368 districts, 8421 community pharmacies and 11,696 physician offices were extracted from the government’s open data, totaling 23,561,236 residents (49.55% males and 50.45% females). The average size and population density of the districts were 98.35 square kilometers and 2748 people per square kilometer, respectively. Appendix 1 presents the population size, sex distribution, area size, median household annual income, and the number of community pharmacies and physician offices in each district.
The number of community pharmacies was positively associated with the number of residents (β = 0.746, p < 0.001) and physician offices (β = 0.272, p < 0.001) in districts/townships after controlling for the covariates (Table 2). The median annual household income (β = −0.068, p < 0.001) showed a negative association with the number of community pharmacies in districts/townships. However, the size of districts/townships (β = −0.021, p = 0.191), proportion of elder adults (β = −0.021, p = 0.216), proportion of female residents (β = −0.008, p = 0.664), and whether the district/township was an urban area (β = 0.009, p = 0.591) was negligible to predict the number of community pharmacies in districts/townships. The predictors included in the regression model can explain 94.2% of the variance in the number of community pharmacies in a district/township (p < 0.001).
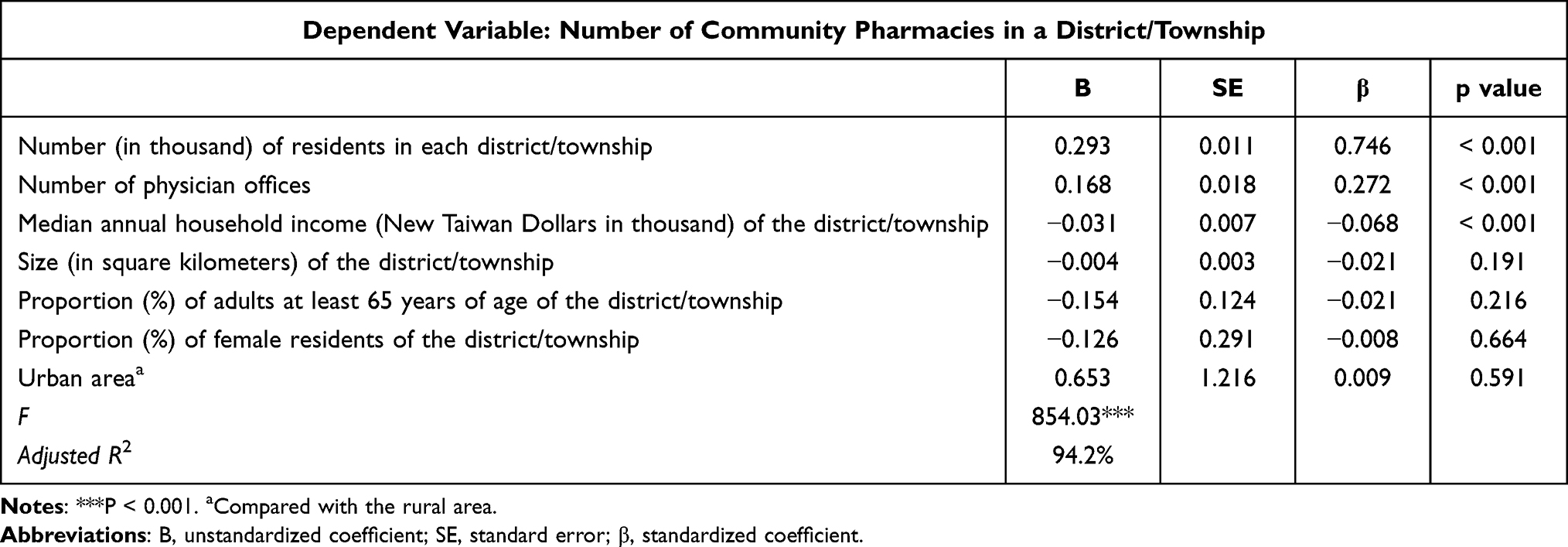 |
Table 2 Predicting Number of Community Pharmacies by Characteristics of Each District (n = 368) |
Qualitative Findings
Ten chief community pharmacists consented to participate and completed the interviews. They were 7 males and 3 females, with the age range of 30 to 60 years old. The mean length of practice at the current community pharmacies was 15.3 (SD: 6.4) years. We present beneath participants’ responses about the most important factors when making decisions on location selection for pharmacy operations in the community.
Theme 1: Population size matters for pharmacy operations and services.
Most of the participants indicated that the population size is a prominent factor influencing their site selection for starting a pharmacy operation. Community pharmacies located in a business district with a high population density are more likely to have more customers to serve. In turn, they can earn adequate income to offset the operating cost. The provision of pharmaceutical care to a broader population would generate more revenues to sustain pharmacy operations.
Where there are crowds, there is business. More customers bring more income to compensate for the rentals. We are not worried about high rentals in a populous area if more people come in and out. The place with cheaper rental may have lower pedestrian flow.
A pharmacy located in a mixed-use neighborhood can serve a diverse population. In the morning, people from the residential communities come to the pharmacy for help. In the evening, people from the commercial facilities can present their needs to pharmacists for help. Busy pedestrian flow brings business to support pharmacy operations.
Theme 2: The type of pharmacy operation and personal attributes determine where the pharmacy should be located.
Some participants mentioned that the type of pharmacy operation greatly impacts the location selection for pharmacy operations. In aging residential areas, the provision of medications and healthcare products and collaboration with allied healthcare professionals may better meet resident’s needs. Pharmacies focusing on beauty products and counseling may consider targeting the younger population in commercial and industrial areas. Pharmacists’ personal characteristics are also bound to the type of pharmacy operation. Pharmacies specializing in medication dispensing and refill may work with nearby physician offices or hospitals to consolidate rapport. Pharmacists providing services for one-time consumers in urban areas ought to be more eloquent and skillful in communication, especially in such a swift timeframe.
To operate a community pharmacy is a human-centered profession, and you can decide which type of operation works for you. Prescription dispensing may be the main task for pharmacists whose pharmacies are adjacent to hospitals. Those who are good at getting along with the elderly may decide to operate pharmacies in senior communities and provide long-term care services. Commercial areas may be a good idea if you want to serve a younger population or white-collar workers.
Theme 3: Types of retail locations play a double-edged sword for pharmacy operations and services.
Most participants pointed out that types of retail locations are important factors when choosing the site for starting a pharmacy. Pharmacies near physician offices, supermarkets, and convenience stores are easy to attract customers who plan to visit physicians or need to replenish daily supplies. Cross-industry alliances can be developed with allied professions or enterprises to provide integrated one-stop services to attentively fulfill customers’ needs. Transportation is deemed a critical factor of pharmacy operations as convenient transportation offers customers easy access to pharmacies. Pharmacies near bus stops may become a gathering place for public transporters, bringing in better revenue. However, the visibility of the pharmacy may be hindered by too many excessive billboards from nearby shops. In addition, convenient transportation without enough parking space may deter customers from stopping by.
More people pass by community pharmacies because physician offices and grocery stores are nearby. The 24-hour lighting billboard of the convenience stores makes the pharmacies noticed, too.
It is convenient to go to the pharmacies around bus stops where customers can take buses with ease. However, pharmacies may be left out if temporary parking lots are unavailable.
Discussion
Confirmed by quantitative and qualitative data, population density, number of physician offices, annual household income, type of pharmacy services, and surrounding environments are determinants for decision-making in site selection for pharmacy operations in the community setting.
Similar to previous literature, the distribution of community pharmacies within a region is associated with population density, local health needs, and median income of the community.14,16,17,38 The identified demographic factors (ie, number of residents and annual household income) associated with the number of community pharmacies in the areas can inform policy-making to improve access to prescription medications and community pharmacies. Caring pharmacists can target specific regions where pharmaceutical services are underserved. Besides, adding one additional community pharmacy was associated with an increase of 3413 residents and 6 physician offices in each district/township, indicating the capacity of a pharmacy can serve residents and collaborate with physician offices in the community setting. As such, these objective indicators provide pharmacists and health authorities with a better understanding of how to allocate appropriate pharmaceutical care resources in society.
This study reveals that mapping types of pharmacy services onto characteristics of pharmacists and regions may inform the decision-making of the location of community pharmacies. Through the lens of pharmacy practitioners, providing pharmaceutical care that fulfills local health needs and integrates surrounding resources tends to make a successful pharmacy and strengthen the community healthcare network. For example, pharmacists are appropriate candidates to connect the public to general practitioners (GPs) through cardiovascular risk screening. Trained pharmacists can engage community residents in getting a screening, refer those at risk to the GPs nearby, and promote interprofessional primary-care collaboration.39 As such, the rapport between the public and healthcare professionals can be teamed up to develop a seamless health promotion process in the community.
In contrast to previous research, which indicated a higher density of pharmacies was found in urban areas,1 our study showed no significant difference in the number of community pharmacies between rural and urban areas. It is possible that on the populous island of Taiwan (13,826 square miles, approximately 245 miles long and 90 miles wide), one district is not far away from another. As a result, there is a stark difference in the notion of pharmacy dessert in the United States which is defined as 10 miles away from a pharmacy.40 What concerns us more is limited accessibility to essential services offered by community pharmacies in rural areas. For example, the access to certain prescribed medications may be a problem in rural areas since most prescribed medications are not allowed to be substituted with generic ones in Taiwan.41 As such, when these prescription drugs are unavailable at their neighborhood pharmacies, patients need to refill their prescriptions from pharmacies in urban areas or the prescribing hospital. The inequitable access to necessary medical care should be addressed sooner than later.
Limitations
Though this study explored pertinent factors to the number of community pharmacies across districts/townships in Taiwan, the findings need to be interpreted cautiously with some limitations. First, this study used aggregate data to calculate population density per pharmacy to represent spatial access to pharmacies but did not calculate the distance between the household address of each individual in the population and the corresponding closest pharmacy. This may introduce an error because it is possible that the actual distance that an individual needs to reach a pharmacy is farther than the distance between the centroid and one’s nearest pharmacy. Future studies may consider using other approaches (eg, geographic information system, space-distance approach) that consider actual distances to validate our findings. Due to the nature of the data property, we did not account for the impact of each community pharmacy’s size and the type of service on the pharmacy operation. For example, patients may go to a large pharmacy with more pharmaceutical products to fulfill their needs rather than a small pharmacy that is short of medications or associated supplies. Further research may collect data about pharmacy size and type of services provided in the pharmacy to understand if and how rural-urban disparity in pharmaceutical care exists in Taiwan. Lastly, the unique healthcare system (ie, universal, mandatory, and public single-payer system) and geographic characteristics in Taiwan restrict the generalizability of the study findings.
Conclusions
Quantitative and qualitative data demonstrate that population density, numbers of physician offices, median annual household income, pharmacy operation type, and type of retail locations are key determinants for site selection of opening a new community pharmacy in Taiwan. The findings help health authorities understand the average number of physician offices that a community pharmacy can collaborate with in the community setting after accounting for relevant covariates. In addition, pharmacists may consider matching their characteristics and local health needs when making decisions for starting up pharmacy operations and services.
Abbreviations
GP, general practitioner.
Data Sharing Statement
The study materials and the details of all analyses are available from the corresponding author upon reasonable request. The characteristics of community pharmacies in Taiwan can be assessed at https://data.gov.tw/dataset/6134.
Ethics Approval and Consent to Participate
This study protocol received approval from the Research Ethics Committee at the National Taiwan University Hospital (202104014RINC). The data accessed from the Taiwan Ministry of Health and Welfare database are open for public use and comply with relevant data protection and privacy regulations. Participants were informed of the research purpose and assured of the anonymity of their participation. Each eligible participant was required to provide oral informed consent prior to data collection, which was approved by the Research Ethics Committee at the National Taiwan University Hospital. All procedures were performed in accordance with the Declaration of Helsinki.
Acknowledgments
Jie Chen and Yen-Ming Huang shared first authorship. The authors would like to acknowledge Dr. David Yu-Shen Lai and Ms. Amy Huei-Mei Lin for their support for the improvement of access to quality pharmaceutical services in Taiwan. We are grateful to the Taichung City New Pharmacist Association and pharmacists who took part in this study.
Funding
The study was supported by the Ministry of Science and Technology (MOST), Executive Yuan, Taipei, Taiwan, R.O.C. (MOST 109-2511-H-002-002-MY2 and MOST 110-2320-B-002-079-MY3) and the National Taiwan University School of Pharmacy Alumni Association in North America (NTUSPAA-NA). The MOST and the NTUSPAA-NA had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclosure
The authors declare that they have no competing interests.
References
1. Tharumia Jagadeesan C, Wirtz VJ. Geographical accessibility of medicines: a systematic literature review of pharmacy mapping. J Pharm Policy Pract. 2021;14(1):28. doi:10.1186/s40545-020-00291-7
2. Goode J-V, Owen J, Page A, Gatewood S. Community-based pharmacy practice innovation and the role of the community-based pharmacist practitioner in the United States. Pharmacy. 2019;7(3):106. doi:10.3390/pharmacy7030106
3. Huang YM, Wang HP, Yang YHK, et al. Effects of a national health education program on the medication knowledge of the public in Taiwan. Ann Pharmacother. 2006;40(1):102–108. doi:10.1345/aph.1G312
4. Chang FC, Chi HY, Huang LJ, Lee CH, Yang JL, Yeh MK. Developing school–pharmacist partnerships to enhance correct medication use and pain medication literacy in Taiwan. J Am Pharm Assoc. 2015;55(6):595–602. doi:10.1331/JAPhA.2015.15053
5. Huang YM, Chen LJ, Hsieh LL, Chan HY, Chen‐Liu KC, Ho YF. Evaluation of use, comprehensibility and clarity of over‐the‐counter medicine labels: consumers’ perspectives and needs in Taiwan. Health Soc Care Community. 2022;30(2):753–761. doi:10.1111/hsc.13190
6. Huang YM, Wang YH, Chan HY, et al. Engaging consumers in wise use of over-the-counter medications in Taiwan: development and evaluation of a structured medication counseling approach. Patient Educ Couns. 2022;105(4):942–948. doi:10.1016/j.pec.2021.08.009
7. Ou HT, Yang YHK. Community pharmacists in Taiwan at the frontline against the novel coronavirus pandemic: gatekeepers for the rationing of personal protective equipment. Ann Intern Med. 2020;173(2):149–150. doi:10.7326/M20-1404
8. Huang YM, Yang YHK, Lin SJ, Chen KCS, Kuo CC, Wu FLL. Medication knowledge to be improved in participants in community universities in Taiwan: outcome of a nationwide community university program. J Formos Med Assoc. 2015;114(12):1267–1279. doi:10.1016/j.jfma.2014.12.001
9. Ho YF, Hsieh LL, Chao WK, Huang YC. Orientation to community pharmacy by online education amid the COVID-19 pandemic: teaching and learning reflections. JAASP. 2020;9:53–59.
10. Ministry of Health and Welfare. 10522-01-01 Pharmacy administration; 2021. Available from: https://dep.mohw.gov.tw/dos/cp-1729-2939-113.html.
11. Kelling SE. Exploring accessibility of community pharmacy services. Inov Pharm. 2015;6(3). doi:10.24926/iip.v6i3.392
12. Lin HW, Lin CH, Chang CK, et al. Economic outcomes of pharmacist-physician medication therapy management for polypharmacy elderly: a prospective, randomized, controlled trial. J Formos Med Assoc. 2018;117(3):235–243. doi:10.1016/j.jfma.2017.04.017
13. Akinbosoye OE, Taitel MS, Grana J, Hill J, Wade RL. Improving medication adherence and health care outcomes in a commercial population through a community pharmacy. Popul Health Manag. 2016;19(6):454–461. doi:10.1089/pop.2015.0176
14. Pednekar P, Peterson A. Mapping pharmacy deserts and determining accessibility to community pharmacy services for elderly enrolled in a State Pharmaceutical Assistance Program. PLoS One. 2018;13(6):e0198173. doi:10.1371/journal.pone.0198173
15. Huang YM, Chan HY, Lee PI, et al. Exploration of changes in pharmacy students’ perceptions of and attitudes towards professionalism: outcome of a community pharmacy experiential learning programme in Taiwan. BMC Med Educ. 2022;22(1):195. doi:10.1186/s12909-022-03261-6
16. Wagner A, Hann M, Noyce P, Ashcroft D. Equity in the distribution of community pharmacies in England: impact of regulatory reform. J Health Serv Res Policy. 2009;14(4):243–248. doi:10.1258/jhsrp.2009.008167
17. Kahraman C, Ruan D, Doǧan I. Fuzzy group decision-making for facility location selection. Inf Sci. 2003;157:135–153. doi:10.1016/S0020-0255(03)00183-X
18. Kuo PW. The Study of the Key Successful Factors of the Chain Pharmacies [thesis]. National Taiwan University; 2004.
19. Kung SW. A Research of Expansion Strategy of Chain Drugstore [thesis]. Chaoyang University of Technology; 2012.
20. Huang CY. A Study on the Expansion Strategy of Chain Pharmacies [thesis]. Ling Tung University; 2014.
21. Chen WH, Lee PC, Chiang SC, et al. Pharmacist workforce at primary care clinics: a nationwide survey in Taiwan. Healthcare. 2021;9(7):863. doi:10.3390/healthcare9070863
22. Creswell JW. A Concise Introduction to Mixed Methods Research.
23. Clark VLP, Ivankova NV. Mixed Methods Research: A Guide to the Field. California: Sage Publications; 2016.
24. Johnson RB, Schoonenboom J. Adding qualitative and mixed methods research to health intervention studies: interacting with differences. Qual Health Res. 2016;26(5):587–602. doi:10.1177/1049732315617479
25. National Development Council. Characteristics of community pharmacies in Taiwan; 2021. Available from: https://data.gov.tw/dataset/6134.
26. Taiwan Medical Association. Statistics of the licensed physicians and medical institutions in Taiwan - 2020 report. Available from: https://www.tma.tw/stats/index_NYearInfo.asp?/2020.html.
27. Department of Household Registration, Ministry of the Interior. Statistics of population demographic by age and gender. Available from: https://www.ris.gov.tw/app/portal/346.
28. Financial Data Center, Ministry of Finance. 2018 Preliminary approved statistics booklet of annual comprehensive income tax declaration; 2020. Available from: https://www.fia.gov.tw/WEB/fia/ias/isa107/107%E5%B9%B4%E5%BA%A6%E7%B6%9C%E5%90%88%E6%89%80%E5%BE%97%E7%A8%85%E7%94%B3%E5%A0%B1%E5%88%9D%E6%AD%A5%E6%A0%B8%E5%AE%9A%E7%B5%B1%E8%A8%88%E5%B0%88%E5%86%8A.html.
29. National Statistics. Definition of urbanized areas. Available from: https://www.stat.gov.tw/ct.asp?xItem=954&ctNode=1313.
30. Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies: guided by information power. Qual Health Res. 2016;26(13):1753–1760. doi:10.1177/1049732315617444
31. Hennink M, Kaiser BN. Sample sizes for saturation in qualitative research: a systematic review of empirical tests. Soc Sci Med. 2022;292:114523. doi:10.1016/j.socscimed.2021.114523
32. Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis: striving to meet the trustworthiness criteria. Int J Qual Methods. 2017;16(1):160940691773384. doi:10.1177/1609406917733847
33. Joffe H. Thematic analysis. In: Qualitative Research Methods in Mental Health and Psychotherapy: A Guide for Students and Practitioners. John Wiley & Sons; 2011:209–223.
34. Savin-Baden M, Howell-Major C. Qualitative Research: The Essential Guide to Theory and Practice
35. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
36. Saldaña J. Coding and Analysis Strategies.
37. Archibald MM. Investigator triangulation: a collaborative strategy with potential for mixed methods research. J Mix Methods Res. 2016;10(3):228–250. doi:10.1177/1558689815570092
38. Kelly ET, Rodowskas CA, Gagnon JP. An examination of the effect of market demographic and competitive characteristics on gross margins of prescription drugs. Med Care. 1975;13:956–965. doi:10.1097/00005650-197511000-00008
39. Mc Namara KP, Krass I, Peterson GM, et al. Implementing screening interventions in community pharmacy to promote interprofessional coordination of primary care–a mixed methods evaluation. Res Social Adm Pharm. 2020;16(2):160–167. doi:10.1016/j.sapharm.2019.04.011
40. Qato DM, Daviglus ML, Wilder J, Lee T, Qato D, Lambert B. ‘Pharmacy deserts’ are prevalent in Chicago’s predominantly minority communities, raising medication access concerns. Health Aff. 2014;33(11):1958–1965. doi:10.1377/hlthaff.2013.1397
41. Hsu CC, Chou CL, Chiang SC, Chen TJ, Chou LF, Chou YC. Urban-rural disparity of generics prescription in Taiwan: the example of dihydropyridine derivatives. Sci World J. 2014;2014:905213. doi:10.1155/2014/905213
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.