")
Back to Journals » Veterinary Medicine: Research and Reports » Volume 13
Management of Severe Hypomagnesemia as the Primary Electrolyte Abnormality with a Delayed Onset of Clinical Signs as a Result of Refeeding Syndrome in a Cat
Authors Smith B, Hendricks J, Centola S
Received 22 February 2022
Accepted for publication 2 June 2022
Published 5 July 2022 Volume 2022:13 Pages 143—151
DOI https://doi.org/10.2147/VMRR.S358682
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Young Lyoo
Brianna Smith, Jeanette Hendricks, Steven Centola
Advanced Critical Care Emergency and Specialty Services, Culver City, CA, USA
Correspondence: Brianna Smith, Advanced Critical Care Emergency and Specialty Services, 9599 Jefferson Blvd., Culver City, CA, 90232, USA, Tel +1 310 558 6100, Fax +1 310 558 6199, Email [email protected]
Abstract: This case report describes severe hypomagnesemia in a cat attributed to refeeding syndrome with an onset of clinical signs from the magnesium deficiency apparent on the twelfth day following initiation of feeding. The patient initially presented in a state of cachexia from apparent malnutrition after missing from the owners care for five months. The patient was initially discharged five days after the initiation of feeding with only a mild hypokalemia apparent and requiring supplementation and returned for outpatient management. The patient presented through the emergency department on the twelfth day following the onset of feeding with the clinical signs of acute lethargy, vomiting, generalized tremors and a seizure episode and had a severe total hypomagnesemia on diagnostic bloodwork. The patient’s clinical signs resolved following emergency treatment with parenteral magnesium sulfate as a continuous rate infusion and was later managed with oral magnesium hydroxide for a prolonged period of time. Electrolyte abnormalities and associated clinical signs typically occur between two and five days after initiation of feeding and up to ten days after starting food intake in humans with anorexia nervosa. This case report highlights that hypomagnesemia, while not the most common electrolyte disturbance to occur with refeeding syndrome, can occur without other significant electrolyte changes and can cause clinical signs greater than ten days following refeeding to a starving patient. This magnesium deficiency required prolonged treatment, but the patient made a complete recovery.
Keywords: magnesium, starvation, malnutrition, feline
Introduction
Refeeding syndrome is characterized by metabolic and physiologic abnormalities during refeeding after starvation in both people and animals. Refeeding syndrome has been documented to include relative deficiencies in phosphorus, potassium, magnesium and vitamins, as well as glucose and fluid intolerance that occur after initiating feeding following a state of starvation or severe malnutrition.3 The classic electrolyte abnormality associated with refeeding syndrome is hypophosphatemia, which is responsible for most of the clinical consequences reported in human and veterinary patients.4 Refeeding a starved patient will increase utilization of phosphorus, potassium and magnesium to drive metabolic pathways and act as a cofactor for adenosine triphosphate (ATP) synthesis. Increased cellular need, in conjunction with co-transport of potassium and magnesium into the cell with insulin-driven glucose uptake, results in further depletion of these electrolytes.3 Risk factors for refeeding syndrome reported in veterinary patients include patients with chronic malnourishment conditions that result in malabsorption of nutrients such as severe intestinal disease or pancreatic insufficiency, patients that have been anorexic for >7 days, and patients that are obese that have rapid weight loss.17
Refeeding syndrome has rarely been reported in veterinary patients. Hypophosphatemia was reported to occur between 12 and 72 hours after enteral feeding was initiated in 9 chronically malnourished cats.12 Refeeding syndrome was also reported in 2 cats resuscitated and fed after being trapped without access to food for 7 to 12 weeks and another cat with hepatic lipidosis fed through an esophageal feeding tube following a 4-week history of decreased appetite and weight loss.1,3,8,14 Prior to 2017, refeeding syndrome had only been reported in cats in the literature. A case report in 2019 described management of a dog with prolonged starvation and presumptive refeeding syndrome.14 The dog in this study developed a hypophosphatemia and hypomagnesemia on day 1 shortly after refeeding but this resolved with supplementation. The dog never became clinical for those abnormalities.
Patients at risk of developing refeeding syndrome require significant attention, as overlooking these patients can cause life-threatening consequences such as hemolytic anemia, cardiac failure, neurological dysfunction and respiratory failure. When these patients are identified, a comprehensive nutritional plan in addition to a treatment plan for other co-morbidities should be formulated. Currently, there are no evidence-based studies demonstrating the ideal refeeding strategy,8 however, there have been protocols developed in people in which veterinary medicine can extrapolate from. There should be careful assessment of patient risk for refeeding syndrome, restoration of fluid balance without overloading the cardiovascular system, initiation of empirical supplementation of phosphate, potassium and magnesium (unless serum concentrations of these electrolytes are increased), initiation of thiamine and other B vitamins and trace minerals apart from iron.10 Currently, it is recommended that no greater than 20% of RER should be provided on the first day and nutritional support should be increased gradually over 4–10 days.4
The following case report describes a cat that presented cachectic in a state of apparent starvation after missing from its owner’s care for five months. The cat developed a severe hypomagnesemia with clinical signs 12 days after refeeding was initiated. This report highlights the importance of a hypervigilant refeeding strategy, serial electrolyte monitoring and treatment considerations in medical management of refeeding severely malnourished cats.
Case Report
History
A 2-year-old female spayed domestic short-haired cat was initially presented to our emergency service for poor appetite and severe weight loss upon returning to her owners care after reportedly missing for the previous 5 months. Prior to her disappearance, the patient was reported to be healthy and had an appropriate Body Condition Score (BCS). On initial admission, the patient was quiet, alert and responsive, ~8% dehydrated, cachectic and had a large flea burden. She was hypotensive on indirect blood pressure measurement at 78mmHg (reference range 120–170mmHg)5 with an initial body weight of 1.49 kg. Her BCS was assessed as 1–2/9 and muscle condition score (MCS) of 1/3. Initial bloodwork included a venous blood gas, complete blood count (CBC), serum chemistry panel, and in-house FeLV/FIV test (Siemens, IDEXX Procyte Dx, IDEXX Catalyst One, IDEXX Snap FIV/FeLV Combo). These diagnostics revealed a mild hyperlactatemia (2.34 mmol/L, reference 0.5–2 mmol/L), mild hyperkalemia (5.24 mEq/L, reference range 3.5–4.8 mEq/L), mild ionized hypocalcemia (0.95 mmol/L, reference range 1.23–1.4 mmol/L), mild hypochloremia (108 mmol/L, reference range 116–126 mEq/L), a normocytic, normochromic, non-regenerative anemia (Hct 19.7%, reference range 31.7–48.0) (Table 1). The patient was viral negative on in-house infectious screen. A total magnesium level was not measured at initial presentation and an ionized magnesium level was not available on the in-house blood gas analyzer (Siemens Rapid 500). Initial treatments for stabilization included an intravenous (IV) bolus of 13 mL/kg of Normosol-R with a recheck blood pressure measurement post-bolus of 110mmHg. Once stable, the cat was placed on crystalloid fluids (Normosol-R) at 3mL/kg/hr IV and was administered oral nitenpyram (Capstar, Elanco). The patient was initially fed a commercial maintenance diet and ate with a large appetite before transfer to the Intensive Care Unit (ICU) at the beginning of the second day of hospitalization
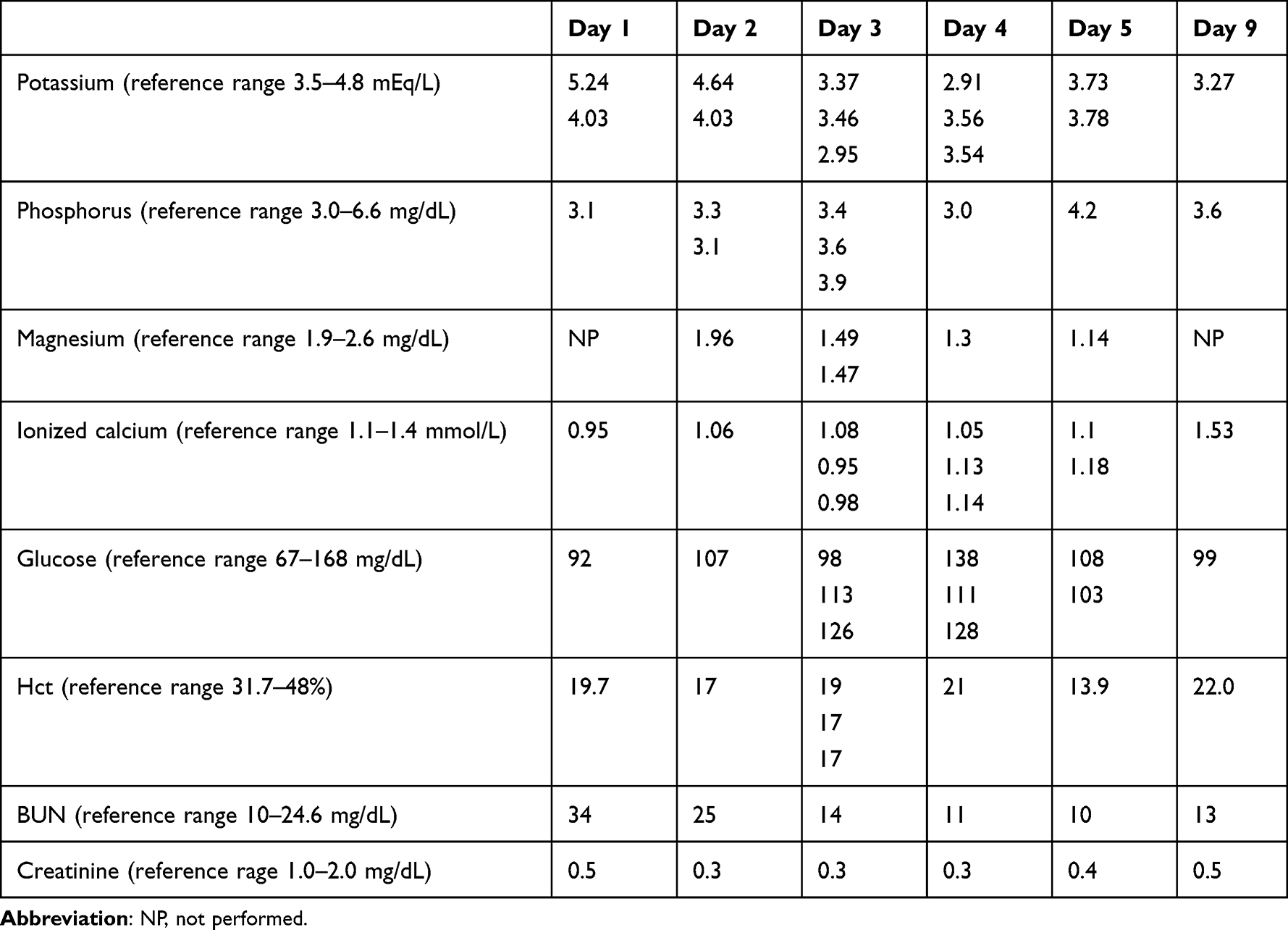 |
Table 1 Pertinent labwork findings after refeeding was started on Day 1 |
In the ICU, the patient received additional diagnostics and treatments starting on the second day of hospitalization. Further diagnostic testing included a recheck of her venous blood gas and a total magnesium measurement along with abdominal and thoracic imaging. On recheck venous blood gas, she had a persistent hyperlactatemia with a normalized potassium level (Table 1). Her total magnesium measurement was normal at 1.96 mg/dL (reference range 1.5–3.0 mg/dL). Thoracic radiographs were unremarkable. An abdominal ultrasound was performed that showed hyperechoic hepatic parenchyma, mild jejunal lymphadenopathy, and gall bladder sludge. Diagnostic tests were also submitted to the commercial laboratory (IDEXX Reference Laboratories) including further infectious testing for additional underlying causes of her anemia by screening for Cytauxzoon felis, Bartonella, Anaplasma, Ehrlichia, Mycoplasma haemofelis, Mycoplasma haemominutum, Mycoplasma turicensis, Feline Leukemia and Feline Immunodeficiency Virus via polymerase chain reaction (PCR). Fecal testing including giardia antigen testing and a urinalysis with culture were also submitted to the reference laboratory. Ultimately, results did not reveal any underlying infectious cause for her anemia and no intestinal parasites. Her urinalysis showed rare bacteriuria, but the urine culture was negative for growth.
Additional therapeutics added during the second day of hospitalization included the administration of B complex vitamins (2 mL/L, VetOne), thiamine (25 mg SQ every 24 hours, VetOne), Cerenia (1 mg/kg IV every 24 hours, Zoetis), pantoprazole (1 mg/kg IV q24 hours, Pfizer), Unasyn (40 mg/kg IV every 8 hour, Pfizer), praziquantel/pyrantel pamoate (Drontal, Bayer) per os once with the dose repeated in three weeks.
The patient was fed a large amount of a commercial diet once at intake through the emergency service (referenced as day 1 of feeding). Further feedings were initially withheld until a nutrition plan was formulated and planned nutritional intake was started on the second day of hospitalization at 25% of the patients calculated resting energy requirement (RER). A diet of Emeraid Intensive Care HDN (EmerAidVet) was offered for refeeding every 6 hours and the patient ate with a ravenous appetite. Nutrition was increased daily by 25% until reaching 100% calculated RER on the fifth day of hospitalization/refeeding.
The patient was hospitalized for a total of 5 days. While hospitalized, serial electrolyte levels were monitored every 6 to 12 hours with daily chemistry bloodwork. Overnight during the second day of hospitalization, the patient developed a mild hypokalemia and potassium chloride supplementation (Hospira) at 20meq/L was added to her crystalloid fluids. This progressed through day 4 of hospitalization warranting an increase in parenteral potassium supplementation to 60meq/L crystalloid fluids IV. She was started on oral potassium gluconate supplementation (RenaPlus, VetOne) on the fourth day of hospitalization at 1.6meq PO every 8 hours and her parenteral supplementation was weaned. She was progressively anemic on the fifth day of hospitalization warranting a packed red blood cell transfusion (pRBC, Blood Type A) at a dose of 15mL/kg IV. The owner elected discharge from the ICU on the fifth day of hospitalization given that the patient was stable following transfusion. The patient was discharged from the hospital with amoxicillin-Clavulanate (Zoetis) and potassium gluconate at 1.6meq PO q12 hours (RenaPlus, VetOne). A nutrition plan was formulated for the owner to continue at no more than 100% calculated RER with a Hill’s m/d diet. At the time of discharge, the patient’s weight was 1.5kg.
The patient presented for a recheck on day 9 following initial presentation/refeeding and was reported to be doing well at home with the owner adhering to the feeding and medication plan. The patient was stable on physical examination and her weight was 1.65kg. Recheck labwork was performed and showed a stable potassium and hematocrit with a continued normal phosphorous level (Table 1). A total magnesium level was not performed due to lack of sample and patient temperament. Given the patients clinical improvements and stable bloodwork 9 days following refeeding, the owner was instructed to increase feedings to 1.2 times the calculated RER. Oral potassium gluconate supplementation was continued as prescribed, and antibiotics were discontinued given negative urine culture results. The owner was instructed to recheck in one week or sooner with concerns.
Clinical Findings
Twelve days following refeeding and initial hospitalization, the patient presented through the Emergency service for acute anorexia, vomiting, panting, generalized tremors, and a tonic-clonic seizure. In-house venous blood gas, CBC and chemistry were performed (Siemens Rapid 500, Procyte dx, Catalyst One) revealed a markedly low total magnesium level (<0.5 mg/dL, reference range 1.9–2.6 mg/dL) as well as low-normal potassium (3.5 mEq/L, reference range 3.504.8 mEq/L) (Table 2). Her weight at presentation was 1.6kg. Emergent therapeutics included administration of midazolam 0.5 mg/kg IV (Almaject) pending labwork and a magnesium sulfate (Fresenius USA) continuous rate infusion (CRI) at 1 mEq/kg/day IV as well as one oral dose of magnesium hydroxide (320 mg PO, Phillips Milk of Magnesia) once the patient mentation could support oral medication administration. Continuous telemetry monitoring was started and the patient maintained a normal sinus rhythm throughout hospitalization. The clinical signs of tremoring resolved with supplementation of magnesium as described above. The magnesium sulfate CRI led to normalization of total magnesium levels within 9 hours following initiation of treatment (see Table 2). Additional treatments for the patient included potassium supplementation intravenously at 30meq/L of crystalloid fluids (Normosol-R). On the thirteenth day following initial refeeding, the patient was found to be severely anemic again and received a second pRBC transfusion (Blood type A, 15mL/kg IV dose administered over 4 hours). Given her stable magnesium levels, she was started back on enteral nutrition at 25% of calculated RER. The magnesium sulfate CRI was tapered and discontinued on day 14 following initial refeeding given normal total magnesium levels (Table 2). On day 15 following initial refeeding, she was stable but her total magnesium levels had decreased so she was started on oral supplementation with magnesium hydroxide (Phillips Milk of Magnesia, Bayer 240 mg PO q12 hours) which stabilized then increased her total magnesium levels leading to the discontinuation of oral therapy by day 16 (Table 2). Her nutritional supplementation was increased from 25% to 100% RER by day 15 and she was again eating with a ravenous appetite. She was discharged from the hospital on day 16 following initial refeeding with a plan for outpatient monitoring and treatments. Her body weight was 1.62kg at the time of discharge and the only medication that she required was oral potassium gluconate (RenaPlus, VetOne) supplementation at a dose of 0.8meq PO q12 hours. The owner was instructed to continue to only feed the Hill’s m/d diet at 100% of calculated RER per day.
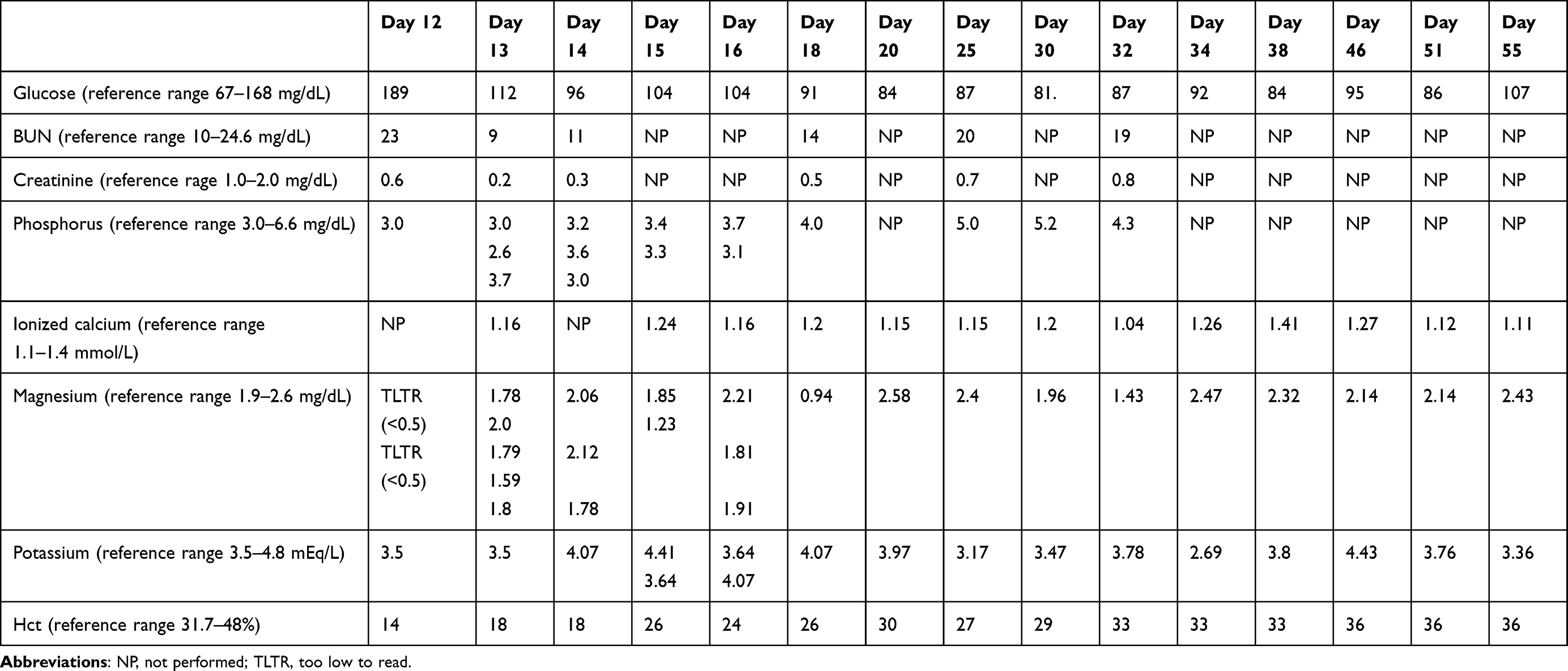 |
Table 2 Lab work findings during second hospitalization and rechecks following discharge |
The patient presented for a recheck examination 18 days following initial refeeding and hospitalization. She was doing well with no concerns expressed by the owner with the exception of a single episode of apparent melena. The owner was adhering to the strict nutritional guidelines established and noted that the patient was eating with a ravenous appetite. Recheck labwork showed a progressive total hypomagnesaemia (0.94mg/dL, reference range 1.9–2.6 mg/dL) without any of the previously noted clinical signs (Table 2). She was treated as an outpatient with sucralfate (Par Pharmaceuticals 100mg PO q8 hours) for the apparent melena as well as magnesium hydroxide (Phillips Milk of Magnesia 3mL (240 mg) PO q12 hours. On subsequent rechecks, the patient’s total magnesium levels were stable on oral therapy and the melena had improved to resolve according to the owner. Her nutrition plan was adjusted to allow her 1.2x calculate RER. Her oral magnesium hydroxide dose was slowly tapered and was discontinued 30 days following initial refeeding as was her potassium supplementation. Her weight at that recheck was 2.03kg (day 30) and she was reported to be doing well by the owner but continued to act ravenous while eating at home. Her feedings were increased to 1.8xRER at that time. On recheck evaluation 32 days following initial refeeding, the owner reported a new onset diarrhea and recurrent melena. Recheck labwork at that time showed progressively hypokalemia (2.7 mEq/L, reference range 3.5–4.8 mEq/L) and mild total hypomagnesemia (1.43 mg/dL reference range 1.9–2.6 mg/dL) (Table 2). The patient was started back on potassium supplementation(RenaPlus, VetOne, at 0.8meq PO every 12 hours), magnesium hydroxide 80 mg PO q12 (Philips Milk of Magnesia, Bayer) at 80 mg PO q12 hours), metronidazole (MixLab compounding pharmacy) and sucralfate (Par pharmaceutical) Given the persistence of her apparent hypomagnesemia and gastrointestinal signs, she had a gastrointestinal malabsorption blood panel (Texas Agricultural and Mechanical University to measure serum B12, folate, TLI and PLI as well as a repeated abdominal ultrasound. She was found to be mildly hyperfolatemic (30.6 mcg/L, reference range 9.7–21.6 mcg/L) and on repeated ultrasound she had a new multifocal small intestinal functional ileus with resolution of the hyperechoic hepatic parenchyma and jejunal lymphadenopathy. On subsequent recheck examinations, the patient was discontinued from oral potassium gluconate supplementation 51 days following initial refeeding and hospitalization. The last recheck performed on the patient was 55 days post-initial refeeding at which time her magnesium levels had remained stable on supplementation (Table 2). Her weight at that recheck was 2.68kg. Further dose adjustments were not pursued at that time because the owner was moving out of state. Seventy-five days following initial hospitalization, a recheck through a new veterinary provider revealed a normal magnesium level so her oral magnesium supplementation started another taper. Further communication with the owner revealed that the patient was successfully tapered off of oral magnesium supplementation and is clinically healthy. The patient received the best practice of veterinary care and all diagnostics and treatments performed were consented by the owners.
Discussion
To our knowledge, this is the first case report describing hypomagnesemia as the primary electrolyte disturbance attributed to refeeding syndrome in a cat following prolonged starvation as well as an apparent delay in onset of clinical signs compatible with hypomagnesemia. The electrolyte derangements characteristic of refeeding syndrome are usually clinically apparent within two to five days following initiation of feeding with clinical consequences not suspected greater than 10 days following feeding.1,4,10 This patient developed a mild, total hypomagnesemia on the fifth day following refeeding without clinical signs and only a mild hypokalemia, which stabilized on oral potassium supplementation. She developed anorexia, vomiting, generalized tremors and seizure activity on the twelfth day following initiation of refeeding and intake to our hospital. These clinical signs were attributed to total body magnesium depletion as noted by the markedly low total magnesium levels on in-house bloodwork. The clinical signs of her hypomagnesemia improved with both parenteral and enteral supplementation leading to the termination of her clinical signs. This patient was serially monitored and required long-term electrolyte supplementation without another potential cause of her hypomagnesemia. This patient responded well to treatment and has recovered completely and has not required permanent supplementation of magnesium.
The hypomagnesemia in this patient is consistent with refeeding a starved or malnourished patient. The pathophysiology of starvation can be divided into an acute response (occurring within the first 2 weeks of starvation) and delayed response (occurring 10 days after the onset of starvation). In the acute phase of starvation, there are metabolic alterations that occur such as decreases in insulin and triiodothyronine (T3) and increases in glucagon, growth hormone, catecholamines and plasma cortisol. The end result of these hormonal alterations is enhanced by hepatic glycogenolysis, gluconeogenesis and skeletal muscle proteolysis thereby facilitating lipolysis. The brain is surviving on glucose generated from protein catabolism and gluconeogenesis in the liver. During the delayed response to starvation there is a major shift from using carbohydrate to using fat as the main energy source. Gluconeogenesis is reduced during this period and protein catabolism is minimized. Ketone bodies from hepatic oxidation of fatty acids are used by most of the tissues for energy. At this stage, the brain is reliant on ketone bodies as an energy substrate.17 During starvation, depletion of electrolytes occurs from lack of dietary intake with additional electrolyte losses from the catabolism of fat and muscle.1 During refeeding, intake of carbohydrate stimulates insulin release, resulting in conversion from a catabolic to an anabolic state, which increases cellular demand for phosphorus, potassium and water. Newly synthesized cells require potassium for maintenance of electrical gradients and translocate serum potassium intracellularly. Glycolysis and protein synthesis resume following refeeding which require the cellular uptake of phosphorus and magnesium. The insulin released during refeeding increases cellular activities thus increasing the cellular requirement for magnesium.17
Hypophosphatemia is the primary electrolyte abnormality characteristic of refeeding syndrome.4,14,16 Hypophosphatemia has been a prominent feature of refeeding syndrome in all previously reported feline cases and was often associated with hemolysis.1,3,8,14 Our patient did not develop a hypophosphatemia on bloodwork throughout any of her evaluations, but her primary electrolyte abnormality was a total hypomagnesemia. Hypomagnesemia is a variable finding in patients with refeeding syndrome.3,14 In a previous study, low serum total magnesium was only detected in one of the cats reported with refeeding syndrome but was not measured in every case.1,3,8,14 Hypomagnesemia developed on day 3 and improved to a low-normal value with supplementation. The mechanism for hypomagnesemia in refeeding syndrome is not clear and is likely multifactorial, resulting from intracellular movement of magnesium ions into cells with carbohydrate feeding and poor dietary intake of magnesium.7 Upregulation of carbohydrate metabolism may also explain the increased demand for magnesium and thiamine, which then leads to neurological and neuromuscular complications.5 Many cases of hypomagnesemia do not appear clinically significant, but severe hypomagnesemia can result in clinical complications, some of which were noted in this patient.7 Severe hypomagnesemia can result in cardiac dysrhythmias, gastrointestinal ileus/abdominal discomfort, anorexia and neuromuscular features such as tremors, paresthesia, tetany, seizures, irritability, confusion, weakness and ataxia.7 Our patient presented with vomiting, weakness, generalized tremors and a tonic-clonic seizure on day 12 following initial refeeding.
Total body magnesium concentration is affected by dietary intake, gastrointestinal function, hormonal balance, redistribution of the magnesium cation, and excretion into a third body space or urine.12 A large amount of magnesium is absorbed in the small intestine and gastrointestinal disease (inflammatory bowel diseases, malabsorptive syndromes) can lead to a hypomagnesemia.11 This patient was screened for an underlying enteropathy through serial ultrasound examinations and through a malabsorption panel (completed through Texas Agricultural and Mechanical University) without convincing evidence for an enteropathy and she was prophylactically treated for intestinal parasites and fecal negative. Her renal function remained adequate throughout hospitalization making renal losses of magnesium less likely. An underlying cause of hypomagnesemia was not identified in this patient; therefore, her hypomagnesemia was attributed solely to refeeding syndrome. The patient in this case report had persistent, mild hypokalemia and ionized hypocalcemia. All reports of cats with refeeding syndrome had documented hypokalemia14 Magnesium is an important mediator of both hypocalcemia and refractory hypokalemia.1 Low magnesium impairs potassium reuptake in the nephron resulting in excess losses and may also impair the cellular transport of potassium all through the impact on magnesium-dependent enzymes such as the Na-K-ATPase.2,15 The hypokalemia secondary to hypomagnesemia may be refractory to parenteral potassium supplementation but is generally responsive once magnesium is corrected.9 While our patient was initially hypokalemic starting the second day following refeeding, she stabilized with potassium supplementation alone and remained stable on oral potassium supplementation at a recheck nine days following refeeding. Magnesium deficiency may also lead to refractory hypocalcemia. Approximately one-third of human patients with low serum magnesium may concurrently have low serum calcium.11 Factors contributing to this include impaired release of parathyroid hormone, diminished parathyroid hormone synthesis, and skeletal resistance to the action of parathyroid hormone, all resulting from impaired magnesium-dependent adenylate cyclase function.9 The cat in this report had a mild ionized hypocalcemia which never required supplementation.
The patient in this study developed diarrhea 12 days after refeeding during her emergency presentation for severe hypomagnesemia. Diarrhea can develop solely from low magnesium, however this occurred shortly after treatment with parenteral magnesium sulfate and continued intermittently in the patient history when magnesium levels had improved. While diarrhea is a known adverse effect of oral magnesium hydroxide,16 it has not been noted as an effect of parenteral magnesium sulfate. The patient’s diarrhea may have initially developed as a result of hypovolemic shock or a result of enterocyte-damage from a functional ileus due to her hypomagnesemia.9,11 On recheck abdominal ultrasound, a functional ileus was noted in this patient. Hypomagnesemia has been reported in horses after colic surgery, suggesting a potential causal relationship between the hypomagnesemia and strangulating lesions and ileus of the bowel.11 Starvation is known to lead to reduction in enterocyte formation and nutrient absorption. Gut atrophy with decreased crypt cell proliferation, reduced villous height, intestinal mass reduction, thickening and coarsening of the intestinal mucosal folds, reduced gastric acidity, reduced gastric and intestinal motility are also noted in patients that have been starved.17 Diarrhea occurs in these starved patients due to impaired absorptive ability, bacterial overgrowth, presence of unconjugated bile salts, hypoalbuminemia and gut edema.3,17 While starvation is a potential mechanism, given the timing of the onset of diarrhea (12 days following refeeding), this is not suspected for our patient. In addition to diarrhea, this patient also developed melena, consistent with GI bleeding. Her melena improved with gastrointestinal protectants (sucralfate). Part of this patient’s anemia was attributed to melena later in her care, but, initially, her anemia was attributed to her heavy flea burden and from the need for survey phlebotomy for monitoring her electrolytes. She required two pRBC transfusions throughout the duration of her care.
This patient was fed unrestricted once at initial presentation (day 1) and ate with a large appetite. Further feedings were withheld following the understanding for nutritional restriction given her clinical picture. Her nutritional management for refeeding syndrome was structured starting on the second day of her initial hospitalization at 25% calculated RER and gradually increased to 100% RER over the course of four days. Refeeding syndrome has been reported in a cat started a 6 Kcal/kg/day.1,4 In humans, the NICE guidelines recommend refeeding should commence at a maximum of 5 kcal/kg/day in severely malnourished patients.6 In our case, a more conservative plan for the patient’s initial nutritional supplementation could have been implemented with a slower increase in supplemented nutrition. In humans, the NICE Guidelines (National Institute for Health and Care Excellence) identify risk factors and recommendations for refeeding in malnourished patients. In these guidelines, initial refeeding should not exceed 20 kcal/kg/day or no more than 20% RER on the first day. These guidelines also recommend that <50% RER total should be fed during the first 3 days. Nutritional support should be increased gradually over 4 to 10 days. However, despite these recommendations, there is no universal recommendation of how quickly to advance the nutritional regimen, particularly in veterinary medicine. This study highlights that a cautious approach to nutrition should be practiced in feline patients.
Nutritional strategies in starved patients should consist of a low level of digestible (soluble) carbohydrates, contain high fat and protein content, and adequate electrolytes. This patient was fed Emeraid Intensive Care HDN (EmerAidVet). This formula is appropriate as it is high in crude protein (8.61 grams/100 kcals), crude fat (6.05 grams/100 kcals) and contains adequate electrolytes, vitamins and minerals that exceed the National Research Council guidelines. It is recommended to provide the most calories as fat and protein because carbohydrates stimulate insulin release and may result in more severe metabolic derangement.8 Consequently, when a diet used for refeeding is composed of a high proportion of carbohydrate, the cessation of natriuresis is abrupt and can lead to the development of peripheral edema and fluid overload. Refeeding with fat or protein alone will allow for natriuresis to continue and may prevent fluid overload or edema formation from occurring in these patients.17 In veterinary medicine, if refeeding syndrome is suspected then it is recommended to stop refeeding immediately and aggressively treat electrolyte abnormalities.17 The refeeding nutritional formula can also be adjusted to contain a lower amount of carbohydrate. There should be no attempt to achieve weight gain during the first week of treatment and any weight gain that does occur should be considered to be due to fluid retention rather than addition of lean body mass.17 Not all starved patients who are refed develop refeeding syndrome. It is important to be aware of the condition and anticipate problems to help minimize its occurrence. It is important to closely monitor at-risk patients, in particular their vital functions, fluid balance and electrolytes.7
Prior to refeeding, the patient should have complete bloodwork and any electrolyte abnormalities should be corrected prior to initiation of nutritional support. Electrolyte trends should be evaluated several times per day depending on the patient. If electrolyte values are not increasing, it may be necessary to slow or stop nutrition completely until they are improved. High risk patients should be empirically supplemented for the first 24 hours of therapy. Before initiating feeding, thiamine should also be administered and followed by daily injections until day 3 of treatment. Additionally, the patient’s body weight and urine output should be monitored for fluid overload. A PCV/TS should also be performed to evaluate for presence of hemolysis. The patient’s cardiovascular and respiratory function ought to be monitored. This can be done using telemetry and placing the patient on a respiratory watch. Serial neurological exams should also be performed as electrolyte and thiamine deficiencies can cause neurological signs in these patients.
A major limitation in this case report is the measurement of serum magnesium, which has been reported as total serum magnesium here rather than an ionized magnesium level. Magnesium measurements in veterinary patients are often limited by the availability and ability of point-of-care monitoring for ionized magnesium levels. Ionized magnesium is the preferred measurement to total magnesium as it is the physiological active form in serum.2,11 Severe total body magnesium depletion may exist in the face of normal serum magnesium concentration13 and may have been the case early in the care in our patient. Measurement of low total serum magnesium levels suggests that the intracellular magnesium balance has been disturbed and implies a moderate to severe total body magnesium deficiency.13 The total hypomagnesemia measured in our patient likely represents total body depletion given her clinical signs, but these levels may have been detected sooner with the availability of ionized magnesium measurement. The true incidence of hypomagnesemia in refeeding syndrome in veterinary medicine is unknown; however, it is likely higher than suggested by the intermittent case reports and small case series.1,3,12
In conclusion, this case demonstrates a delayed, severe, and persistent life-threatening hypomagnesemia with clinical signs in a patient in the absence of other severe electrolyte abnormalities attributed to refeeding syndrome. This patient demonstrated a delay in the severity of her electrolyte abnormalities with persistent deficiencies warranting chronic supplementation. This case illustrates the necessity of magnesium measurement regardless of other electrolyte alterations, most notably in the absence of a hypophosphatemia, and outlines the need for magnesium supplementation in the acute and chronic setting. This case report also provides a description of the compatible clinical signs observed in a feline patient with hypomagnesemia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Armitage-Chan EA, O’Toole T, Chaj DL. Management of prolonged food deprivation, hypothermia, and refeeding syndrome in a cat. JVECCS. 2006;16(2):S34–S41.
2. Barerra R, Fleischer MJ, Groeger J, Groeger J. Ionized magnesium supplementation in critically ill patients: comparing ionized and total magnesium. J Crit Care. 2000;15(1):36–40. doi:10.1053/jcrc.2000.0150036
3. Brenner K, KuKanich KS, Smee NM. Refeeding syndrome in a cat with hepatic lipidosis. J Feline Med Surg. 2011;13:614–617. doi:10.1016/j.jfms.2011.05.001
4. Chan DL. Refeeding syndrome in small animals. In: Nutritional Management of Hospitalized Small Animals. Wiley Blackwell; 2015:159–164.
5. Cooper E. Hypotension. In: Silverstein DC, Hoper K, editors. Small Animal Critical Care Medicine.
6. Crook MA. Refeeding syndrome: problems with definition and management. Nutrition. 2014;30:1448–1455. doi:10.1016/j.nut.2014.03.026
7. Crook MA, Hally V, Panteli JV. The importance of the refeeding syndrome. Nutrition. 2001;17:632–637. doi:10.1016/S0899-9007(01)00542-1
8. DeAvilla MD, Leech EB. Hypoglycemia associated with refeeding syndrome in a cat. JVECCS. 2016;26(6):798–803.
9. Duhpa N, Proulx J. Hypocalcemia and hypomagnesemia. Advances in fluid and electrolyte disorders. Vet Clin North Am. 1998;28(3):587–602. doi:10.1016/S0195-5616(98)50057-5
10. Hofer M, Pozzi A, Joray M, et al. Safe refeeding management of anorexia nervosa inpatients: an evidence-based protocol. Nutrition. 2013;30:524–530. doi:10.1016/j.nut.2013.09.019
11. Humphrey S, Kirby R, Rudloff E. Magnesium physiology and clinical therapy in veterinary critical care. JVECCS. 2015;25(2):210–225.
12. Justin RB, Hohenhaus AE. Hypophosphatemia associated with enteral alimentation in cats. J Vet Intern Med. 1995;9(4):228–233. doi:10.1111/j.1939-1676.1995.tb01072.x
13. Khanna C, Lund EM, Rafee M, Armstrong PJ. Hypomagnesemia in 188 dogs: a hospital population-based prevalence study. J Vet Intern Med. 1998;12:304–309. doi:10.1111/j.1939-1676.1998.tb02126.x
14. Khoo WSA, Taylor SM, Owens TL. Successful management and recovery following prolonged starvation in a dog. JVECCS. 2019;29:1–7.
15. Martin LG, Matteson VL, Van Pelt DR, Hacket TB. Abnormalities of serum magnesium in critically ill dogs: incidence and implications. JVECCS. 1994;4(1):17–20.
16. Martin M, Diaz-Rubio E, Casado A, Lopez Vega JM, Sastre J, Almenarez J. Intravenous and oral magnesium supplementation in the prophylaxis of cisplatin-induced hypomagnesemia. Am J Clin Oncol. 1992;15(4):348–351. doi:10.1097/00000421-199208000-00016
17. Peterson N. Refeeding syndrome: how to avoid, recognize and treat.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.