Back to Journals » Clinical Interventions in Aging » Volume 20
Malnutrition and Muscle Loss Mediate the Association Between NT-proBNP and Mortality in Hospitalized Older Adults
Authors Tao J ![]() , Zhang X, Wang N, Cheng D
, Zhang X, Wang N, Cheng D
Received 8 April 2025
Accepted for publication 18 August 2025
Published 23 August 2025 Volume 2025:20 Pages 1349—1357
DOI https://doi.org/10.2147/CIA.S523073
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Jun Tao,1,2 Xiaoyan Zhang,2 Niansong Wang,1 Dongsheng Cheng1
1Department of Nephrology, Shanghai Sixth People’s Hospital Affiliated to Shanghai JiaoTong University School of Medicine, Shanghai, People’s Republic of China; 2Department of Geriatrics, Shanghai Sixth People’s Hospital Affiliated to Shanghai JiaoTong University School of Medicine, Shanghai, People’s Republic of China
Correspondence: Dongsheng Cheng, Department of Nephrology, Shanghai Sixth People’s Hospital Affiliated to Shanghai JiaoTong University School of Medicine, No. 600, Yi Shan Road, Shanghai, 200233, People’s Republic of China, Tel +86-021-64369181, Email [email protected] Niansong Wang, Department of Nephrology, Shanghai Sixth People’s Hospital Affiliated to Shanghai JiaoTong University School of Medicine, No. 600, Yi Shan Road, Shanghai, 200233, People’s Republic of China, Tel +86-021-64369181, Email [email protected]
Background & Aims: Elevated N-terminal pro-B-type natriuretic peptide (NT-proBNP), a biomarker of cardiac stress, predicts mortality in heart failure. Its association with outcomes in older hospitalized patients without overt heart failure, and potential mediation by malnutrition and muscle loss, remains unclear. The purpose of this study was to assess the association between NT-proBNP and mortality in hospitalized oldest-old adults (≥ 80 years) and to explore the mediating role of malnutrition and muscle loss.
Methods: This prospective cohort study was conducted among 360 hospitalized patients ≥ 80 years of age (median age 87 years, 24.4% women) in the Department of Geriatrics (Shanghai, China), between August 2017 and January 2018. The Geriatric Nutritional Risk Index (GNRI) and Mini Nutritional Assessment Short Form (MNA-SF) were used for nutritional assessment, while calf circumference was used as a measure of muscle mass. A Cox proportional hazard model was used to assess the relationship between NT-proBNP levels and mortality. Mediation analysis was used to explore the mediating effects of malnutrition and muscle loss.
Results: The median follow-up was 4.1 years with 159 (44.1%) deaths. Mortality risk increased by 32% per 2-fold increase in NT-proBNP levels (full adjusted hazard ratio: 1.32 [95% Confidence Interval (CI), 1.20– 1.46]). A mediation analysis showed that a lower GNRI score and decreased calf circumference partially mediated the effects of high NT-proBNP and mortality risk, with an estimated relative effect size of 28.9%, while MNA-SF and calf circumference mediated with an estimated relative effect size of 25.3%.
Conclusion: NT-proBNP levels were associated with increased mortality in hospitalized older patients. Moreover, the detrimental effects of NT-proBNP on survival were partly mediated by malnutrition and muscle loss. Consequently, preventive and nutritional strategies should be required for these patients.
Plain Language Summary: Hospitalization poses greater risks with aging. Research shows elevated NT-proBNP—a cardiac biomarker—predicts higher mortality in hospitalized older adults. Assessments revealed increased mortality risk with rising NT-proBNP levels, significantly mediated by malnutrition and muscle loss. These findings indicate NT-proBNP reflects broader physiological decline, highlighting the critical need to evaluate nutritional and muscle status. Screening enables targeted interventions like dietary support and physical activity to improve outcomes.
Keywords: natriuretic peptide, sarcopenia, malnutrition, hospitalization, oldest-old
Introduction
Older hospitalized patients often suffer from malnutrition (an imbalance of nutrients impairing health and body function) and muscle loss, which is associated with a poor quality of life and an increased mortality risk.1–3 Notably, lower limb muscles - particularly those measured by calf circumference - show prominent depletion in this population. Many factors, including reduced food intake, the burden of chronic disease, systemic inflammation, and insulin resistance, are responsible for malnutrition and muscle loss in hospitalized older patients. Nutritional intervention combined with exercise training can help improve prognosis in older patients, the underlying mechanisms linking cardiac biomarkers to outcomes warrant exploration.
Brain natriuretic peptide (BNP) and NT-proBNP are important in the diagnosis and management of patients with heart failure.4 Higher BNP levels predicted a higher risk of death in heart failure patients as well as in general populations.4 Circulating natriuretic peptides released from the heart respond to cardiac wall stress and have diuretic, natriuretic, and vasodilatory effects.5 However, the mechanisms by which elevated BNP levels increase the risk of premature death, especially in general population, remain unclear. Proposed pathways include increased energy expenditure via adipose tissue browning and promotion of catabolic states6–8 This aligns with observed associations between natriuretic peptides and muscle loss in healthy individuals.9 Thus, we hypothesized that malnutrition and muscle loss may mediate the association between NT-proBNP levels and mortality.
Therefore, the purpose of this study was to evaluate the association between NT-proBNP and mortality in hospitalized oldest-old adults and to explore the mediating role of malnutrition and muscle loss.
Materials and Methods
Patient Selection
This was a prospective cohort study conducted in the Department of Geriatrics of an academic teaching hospital (Shanghai, China). As this study is part of a larger cohort, a post-hoc power analysis was conducted using Cox regression in PASS 2015 (NCSS LLC).10 Based on the overall mortality rate of 44.1% (159/360) and the minimal detectable hazard ratio of 1.32 (from Table 1), with α=0.05 and R²=0.4415 between NT-proBNP and covariates (age, sex, CCI, eGFR), the achieved power was 99.67% - substantially exceeding the conventional 80% threshold. This confirms the adequacy of our sample size (N=360) to detect clinically significant associations. Patients ≥80 years of age were screened between August 2017 and January 2018. Exclusion criteria were participants with terminal carcinomatous cachexia (clinical history), inability to communicate, bedridden or in wheelchairs, those receiving hemodialysis or peritoneal dialysis, acute severe infection, acute gastrointestinal bleeding, severe respiratory, liver, or heart failure, and those with incomplete comprehensive geriatric assessment data. For individuals with more than one admission to the geriatric unit, only the first admission during the study period was considered. A total of 381 participants were screened, and 21 participants were excluded (acute severe infection [n = 8]; severe respiratory, liver, or heart failure [n = 5]; acute gastrointestinal bleeding [n = 3]; incomplete data [n = 5]). Ultimately, 360 participants were included in the final analysis (as shown in Figure 1). This study was approved by the Ethics Committee of the Shanghai Jiao tong University Affiliated Sixth People’s Hospital [approval number, 2016-141-(1)]. Written informed consent was obtained from all participants and in accordance with the principle of the Helsinki Declaration. All participants provided written informed consent.
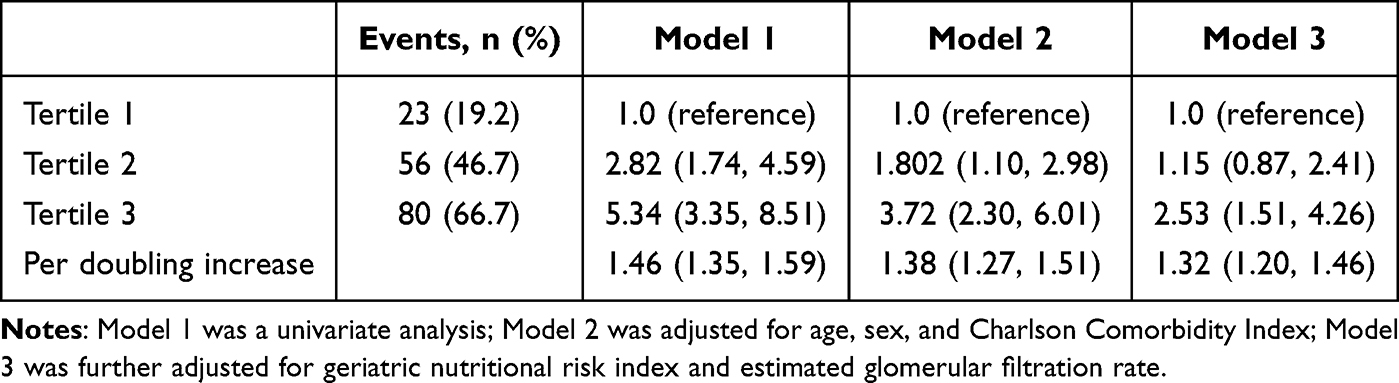 |
Table 1 Associations of NT-proBNP and Mortality in Hospitalized Oldest-Old Patients |
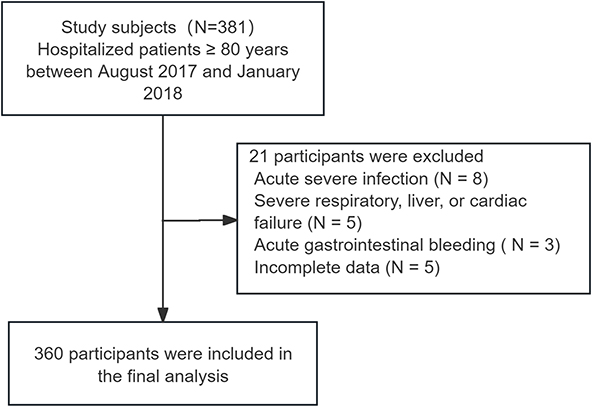 |
Figure 1 Participant flowchart. |
Data Collection and Measurements
In-hospital patients underwent a comprehensive geriatric assessment. Demographic data, comorbid conditions and clinical data were extracted from the hospital’s EMR system with standardized data entry protocols for critical parameters. Charlson comorbidity index (CCI) was calculated.11 Baseline laboratory measurements during admission included serum albumin, prealbumin, serum creatinine, and NT-proBNP levels. The estimated glomerular filtration rate (eGFR) was calculated using CKD-EPI formula.12
Anthropometric parameters included body weight, height, body mass index (BMI), mid arm circumference, waist circumference, abdominal skinfold thickness, calf circumference, and handgrip strength. Waist circumference was measured at the midpoint between the rib cage and the iliac crest. Mid arm circumference was measured with millimeter tape at the midpoint of the arm, between olecranon and acromion. Abdominal skinfold thickness was measured at the junction of the horizontal line of the umbilicus and the midline of the right clavicle using a skinfold caliper (SYNTEK Electronic Digital Fat Caliper, China). Calf circumference refers to the measurement taken at the widest part of the right calf, typically at the fullest area below the knee, using a soft measuring tape. All these parameters were measured twice to obtain mean values. The maximum grip strength of the dominant hand (WCS-100 electronic vibrometer, China) was measured three times, and each time after the measurement, the rest was taken for 1min. Anthropometric measurements were performed by two board-certified geriatric nurses with specialized training in geriatric assessment, using calibrated instruments and standardized positioning techniques.
Definitions of Exposure, Mediator, and Outcome
Serum NT-proBNP was measured using an electrochemiluminescence immunoassay (Elecsys proBNP II, Roche Diagnostics GmbH). Nutritional status was also assessed using the Geriatric Nutritional Risk Index (GNRI)13 and Mini Nutritional Assessment S.nb, jkhort Form (MNA-SF; score 0–14)14 (see Reference 14 for full scale details). GNRI is derived from serum albumin, height, and weight, while MNA-SF assesses dietary intake, weight loss, mobility, acute illness, cognitive problems, and BMI. Calf circumference (CC) was also recorded (Supplementary Table S1).
The primary outcome was long-term all-cause mortality. Mortality data were ascertained through two sources: in-hospital deaths were captured via real-time documentation in the EMR system by attending physicians; out-of-hospital deaths were identified through quarterly structured telephone follow-ups conducted by research coordinators, with validation using local medical records when available. Follow-up completed on January 1, 2022.
GNRI and CC, key indices linked to nutritional status and muscle mass, are important determinants of mortality. Studying these variables deepens understanding of the relationship between admission serum NT-proBNP levels and mortality risk, contributing to more nuanced patient stratification.
Statistical Analyses
Continuous data were summarized as mean ± standard deviation or median (interquartile range), while categorical data was presented as percentages. To explore the potential nonlinear relationship between NT-proBNP and mortality, restricted cubic splines were used for survival analysis, and Cox regression was employed to assess the association between NT-proBNP levels and mortality. Before entering the Cox regression model, log-transformed NT-proBNP values were evaluated as a continuous variable and in different tertiles. Hazard ratios (HRs) and 95% confidence intervals (95% CIs) were determined through Cox proportional hazard models, considering baseline variables including age, sex, Charlson Comorbidity Index, geriatric nutritional risk index and estimated glomerular filtration rate (eGFR). Subgroup analysis was conducted based on sex, BMI, diabetes mellitus history, stage of chronic kidney disease (CKD), and severity of heart failure. Sensitivity analyses were also carried out by excluding participants with events occurring in the first 1–2 years or patients with cancer at baseline.
In order to understand the mediating roles of the GNRI and CC in the relationship between NT-proBNP and mortality, we established a two-part regression analysis framework, which includes mediator and outcome models (as shown in Figure 1). The mediator model regressed potential mediating factors (GNRI and CC) against NT-proBNP, while the outcome model estimated the association of mortality with NT-proBNP alongside the mediators in a Cox proportional hazard model. Regression coefficients reflecting the relationship of NT-proBNP with each mediator were obtained from these models. Indirect effects of NT-proBNP on mortality through each mediator were defined, and the total mortality effect attributable to NT-proBNP was calculated.
Mediation Analysis Framework
The causal relationships were conceptualized through a directed acyclic graph (DAG, Figure 2) specifying: NT-proBNP as the primary exposure (E), Malnutrition (M1, assessed by GNRI) and muscle loss (M2, assessed by calf circumference) as sequential mediators, All-cause mortality as the outcome (O), Age, sex, Charlson Comorbidity Index (CCI), and eGFR as essential confounders (C). This framework hypothesizes: 1. Malnutrition mediates the NT-proBNP → mortality pathway (E→M1→O) 2. Muscle loss mediates the NT-proBNP → mortality pathway (E→M2→O) 3. Malnutrition influences muscle loss (M1→M2) 4. Confounders (C) potentially affect all variables.
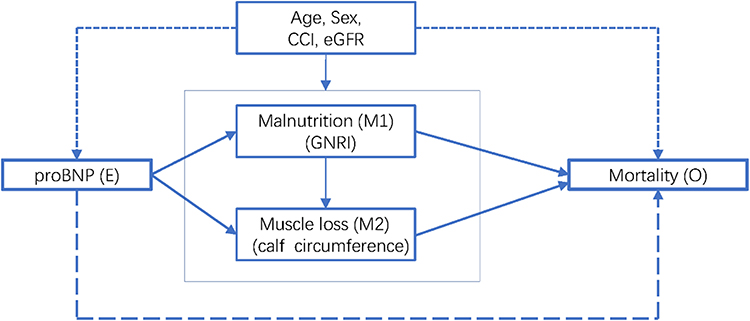 |
Figure 2 Underlying causal framework of the relationship between NT-proBNP and mortality (The directed acyclic graph outlines a conceptual schema involving NT-proBNP (E), Malnutrition (M1), and Muscle Loss (M2) as indicated by GNRI and calf circumference, leading to Mortality (O). It includes key confounders such as age, sex, Charlson Comorbidity Index (CCI), and estimated Glomerular Filtration Rate (eGFR). Dotted arrows suggest potential confounding, while solid arrows and dashed arrows represent indirect and direct effects of NT-proBNP, respectively. The schema also includes a vector from GNRI to calf circumference, reflecting the impact of malnutrition on muscle loss. All statistical analyses are based on this framework, with adjustments for variables such as age, sex, CCI and eGFR. |
All data were analyzed using SPSS version 22.0 software, the PROCESS plugin was employed to enhance this analytical method. Statistical significance was defined as a P-value <0.05.
Results
Baseline Characteristics
Table 2 presents baseline patient characteristics by NT-proBNP tertiles. The study included 360 participants (median age: 87 [IQR 84–90] years), 88 (24.4%) of whom were women. Overall, 33.1% of patients had diabetes mellitus, and 85.0% had hypertension. NT-proBNP ranged from 12.6 pg/mL to 11930.0 pg/mL.
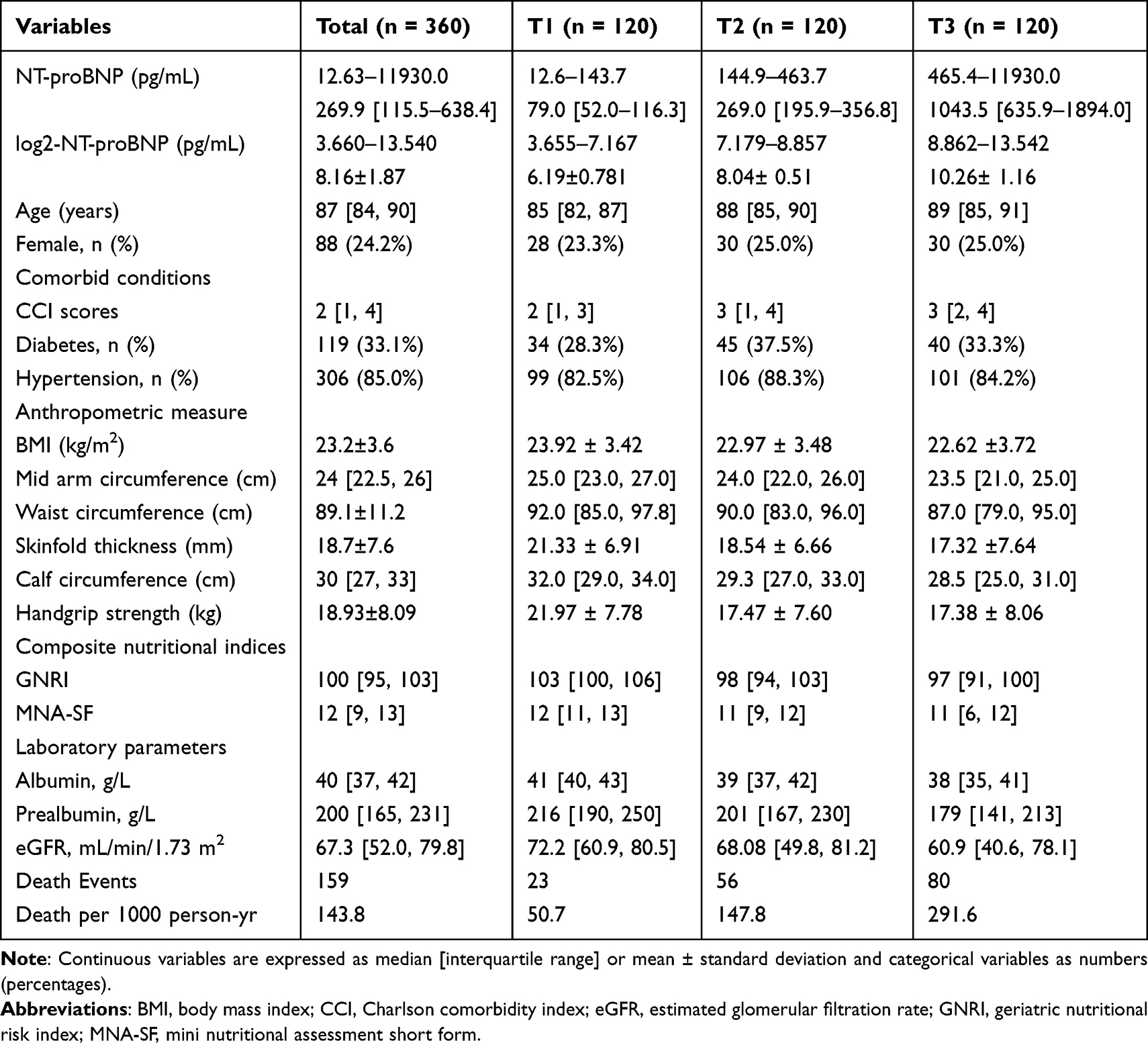 |
Table 2 Baseline Characteristics of Hospitalized Oldest-Old Patients According to NT-proBNP Tertiles |
Patients in the higher tertiles of NT-proBNP were significantly older, and had higher CCI scores, lower BMI, calf circumference, poorer handgrip strength and reduced serum albumin compared to patients in the lower tertiles. They were more likely to have lower GNRI and MNA-SF scores and an increased risk of death when NT-proBNP was higher.
Association Between NT-ProBNP and Mortality
During a median 4.1 years (IQR 2.4–5.5) accumulating 1106 person-years of observation, 159 deaths occurred. In total, 29 patients died during hospital admission. Compared to the first tertile (as a reference group), fully adjusted HRs for mortality were 2.82 (95% CI, 1.74–4.59) and 5.34 (95% CI, 3.35–8.51) for the second and third tertiles, respectively (Table 1). A restricted multivariable cubic spline plot clearly showed a linear association between NT-proBNP levels and long mortality (Figure S1). Mortality risk increased by 32% when per doubling increase in NT-proBNP (adjusted hazard ratio [HR], 1.32 [95% CI, 1.20–1.46]).
A significant association between NT-proBNP level and mortality was observed in all subgroups (Supplementary Table S2). There was a substantial subgroup interaction for sex (P = 0.008), whereby the association was more evident in women than that in men (per doubling increase in NT-proBNP (HR 1.57 [95% CI, 1.23–2.02] and 1.27 [95% CI, 1.13–1.42], respectively).
The exclusion of participants with events occurring during the first 1–2 years, or excluding participants with cancer at baseline, did not affect the relationship between NT-proBNP levels and mortality risk (Supplementary Table S3).
Malnutrition and Muscle Loss Mediated the Association Between NT-proBNP and Mortality
The potential mediation effects of malnutrition and muscle loss on the associations between NT-proBNP and mortality are described in Figure 3. A mediation analysis was performed, controlling for multiple confounders, including age, sex, BMI, CCI, and eGFR. The indirect effects of the GNRI score and calf circumference were 0.097 (95% CI, 0.026–0.188) and 0.061 (95% CI, 0.008–0.134), respectively (Figures 3A). Lower GNRI scores and a smaller calf circumference largely explained the effects of high proBNP levels as a predictor of increased mortality risk, with an estimated relative effect of 28.9% (17.7% and 11.2%, respectively). Significant results were also obtained when using the MNA-SF scores as nutritional assessment tools, with an estimated relative effect of 25.3% (Figure 3B).
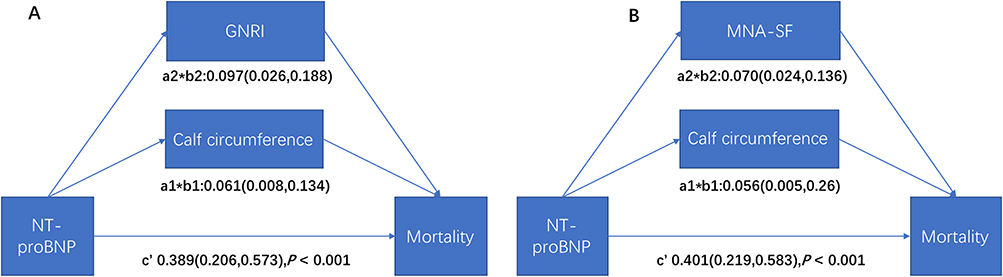 |
Figure 3 Mediation analysis exploring malnutrition ((A) GNRI; (B) MAN-SF) and muscle loss (calf circumference) as mediators of NT-proBNP induced high mortality in hospitalized oldest-old patients, adjusted for age, gender, Charlson comorbidity index, and estimated glomerular filtration rate. |
Discussion
The major findings of our analysis were as followings: 1) increased NT-proBNP levels were associated with high mortality in hospitalized older patients; 2) demonstrated that the detrimental effects of NT-proBNP on survival were partly mediated by malnutrition and muscle loss. By synthesizing these results, clinicians could better understand NT-proBNP levels and determine which patients face a greater risk; moreover, nutritional screening and intervention should be required for these patients with high circulating NT-proBNP level.
Circulating NT-proBNP is a well-established prognostic marker in patients with heart failure.15 Additionally, the measurement of NT-proBNP could help identify individuals at high risk for cardiovascular disease.15 In this study, NT-proBNP levels (median: 269.9 pg/mL, IQR: 115.5–638.4 pg/mL) upon admission were associated with mortality in hospitalized oldest-old adults. Moreover, these associations persisted after stratification by sex, BMI, history of diabetes mellitus, CKD stage, and heart failure severity. For example, York et al demonstrated progressive risk escalation starting from >100 pg/mL in non-heart failure status.5 Thus, our findings support the role of NT-proBNP not only a diagnostic and prognostic biomarker for patients with heart failure, but also a good indicator of health status and prognosis in hospitalized oldest-old patients. Nevertheless, the findings bring to light further essential questions regarding the treatment strategies for patients who have raised plasma NT-proBNP levels but do not have heart failure.
Natriuretic peptides are released from the heart in response to cardiac wall pressure and ventricular volume overload.16 Natriuretic peptides are vital biomarkers and play an important regulatory role by opposing vasoconstriction, sodium retention, and antidiuretic effects.16 However, the mechanism underlying the detrimental effects of elevated BNP levels on mortality risk remain poorly understood. Recently, cardiac natriuretic peptides have been recognized as activators of browning in white adipose tissue and contribute to protein-energy wasting.6,17 Among 5300 consecutively enrolled asymptomatic Asian participants, individuals with malnourishment had substantially higher NT-proBNP levels (median 167.0 pg/mL, IQR 68.7–501.8) than the well-nourished group (median 77.9 pg/mL, IQR 35.3–180.4), regardless of lean mass or the presence of obesity.18 This aligns with our cohort’s median NT-proBNP of 269.9 pg/mL (IQR 115.5–638.4) in high-risk patients. Natriuretic peptides are associated with muscle loss in apparently healthy middle-aged to elderly subjects.9 This association may stem from BNP’s involvement in inducing mitochondrial dysfunction within skeletal muscle and disrupting adipokine signaling pathways, potentially signaling subclinical cardiovascular stress even in non-clinical populations.7 Furthermore, these peptides are linked to protein-energy wasting in patients undergoing hemodialysis.8
In this study, of hospitalized oldest-old adults, increased NT-proBNP levels were associated with a poor nutritional status, as indicated by anthropometric measures, composite nutritional indices, and nutritional laboratory parameters. Participant with increased NT-proBNP levels also had lower with muscle mass (lower CC) and poorer handgrip strength. Based on the harmful effects of malnutrition and muscle loss on survival, we first tested their mediating role in the relationship between NT-proBNP levels and mortality risk. Mediation analysis showed that the association between NT-proBNP and mortality was mediated by malnutrition (lower GNRI scores) and muscle mass loss (smaller calf circumference). Moreover, these effects remained when the GNRI scores were replaced by the MNA-SF scores for nutritional assessment. These findings may have significant clinical implications. Considering the mediating roles of malnutrition and muscle loss, preventive and treatment strategies, such as malnutrition screening, nutritional therapy, and exercise intervention, are required for hospitalized oldest-old patients with high NT-proBNP levels. Further prospective studies are required to clarify whether these strategies can improve patient outcomes. From a societal value perspective, both indicators demonstrate high cost-effectiveness: NT-proBNP testing ($20-45/test) is routinely covered in hospital panels, while calf circumference measurement requires only a tape measure (<$1/assessment), imposing negligible burden on patients or healthcare systems. This dual approach optimizes resource allocation without compromising risk stratification.
Key strengths of this study include its focus on the underrepresented hospitalized oldest-old (≥80 years), the use of validated tools (GNRI, MNA-SF, calf circumference) for mediation analysis, and the identification of actionable clinical targets (nutrition/muscle preservation).
However, our study had several limitations. First, NT-proBNP was only recorded at baseline, while dynamic monitoring could better capture its relationship with evolving nutritional status and mortality trajectories. Second, nutritional status was not evaluated using with comprehensive assessment tools, such as the full Mini Nutritional Assessment or Subjective Global Assessment. However, the assessment tools used, including MNA-SF and GNRI, are common in clinical settings, align with a full assessment, and effectively predict clinical outcomes in hospitalized patients.13,14,19 Third, muscle mass was not assessed via calf circumference rather than gold-standard techniques (dual-energy X-ray absorptiometry or computed tomography). Nonetheless, calf circumference is a recommended surrogate measure for muscle loss and independently predicted outcomes.20 Fourth, residual confounding may persist despite adjustments. Finally, single-center recruitment limits generalizability across healthcare systems and ethnicities, particularly regarding NT-proBNP threshold applicability.
Conclusion
In hospitalized oldest-old patients, high NT-proBNP levels were significantly associated with poor survival. Moreover, malnutrition and muscle loss partly mediate the detrimental effects of NT-proBNP on survival. Nutritional screening and intervention may improve the prognosis of hospitalized oldest-old adults with high NT-proBNP level. Future research should prioritize: validating findings in multi-center studies across diverse populations; assessing whether tailored nutrition/exercise interventions reduce mortality in patients with elevated NT-proBNP; monitoring longitudinal trends in NT-proBNP, nutrition, and muscle mass to pinpoint optimal intervention timepoints.
Abbreviations
BMI, Body mass index; BNP, Brain natriuretic peptide; CCI, Charlson comorbidity index; CKD, Chronic kidney disease; GNRI, Geriatric nutritional risk index; HR, Hazard ratio, NT-proBNP, Pro-B-type natriuretic peptide.
Acknowledgment
This paper has been uploaded to ResearchSquare as a preprint: https://www.researchsquare.com/article/rs-3863523/v1.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was sponsored by the Shanghai municipal health commission (grant number 20194y0347), and the Interdisciplinary Program of Shanghai Jiao Tong University (grant number YG2019QNB14).
Disclosure
The authors declare that they have no competing interests for this work.
References
1. Martone AM, Bianchi L, Abete P. et al. The incidence of sarcopenia among hospitalized older patients: results from the Glisten study. J Cachexia Sarcopenia Muscle. 2017;8:907–914. doi:10.1002/jcsm.12224
2. Hu X, Zhang L, Wang H, Hao Q, Dong B, Yang M. Malnutrition-sarcopenia syndrome predicts mortality in hospitalized older patients. Sci Rep. 2017;7:3171. doi:10.1038/s41598-017-03388-3
3. Xie L, Jiang J, Fu H, Zhang W, Yang L, Yang M. Malnutrition in relation to muscle mass, muscle quality, and muscle strength in hospitalized older adults. J Am Med Dir Assoc. 2022;23:722–728. doi:10.1016/j.jamda.2021.11.025
4. Mueller C, McDonald K, de Boer RA, et al; Heart Failure Association of the European Society of C. Heart Failure Association of the European Society of Cardiology practical guidance on the use of natriuretic peptide concentrations. Eur J Heart Fail. 2019;21:715–731. doi:10.1002/ejhf.1494
5. York MK, Gupta DK, Reynolds CF, et al. B-type natriuretic peptide levels and mortality in patients with and without heart failure. J Am Coll Cardiol. 2018;71:2079–2088. doi:10.1016/j.jacc.2018.02.071
6. Luce M, Barba C, Yi D, et al. Accumulation of natriuretic peptides is associated with protein energy wasting and activation of browning in white adipose tissue in chronic kidney disease. Kidney Int. 2020;98:663–672. doi:10.1016/j.kint.2020.03.027
7. Ikeda M, Honda H, Takahashi K, Shishido K, Shibata T. N-Terminal Pro-B-type natriuretic peptide as a biomarker for loss of muscle mass in prevalent hemodialysis patients. PLoS One. 2016;11:e0166804. doi:10.1371/journal.pone.0166804
8. Luce M, Bres E, Yi D, et al. Natriuretic peptides as predictors of protein-energy wasting in hemodialysis population. J Ren Nutr. 2021;32:234–242. doi:10.1053/j.jrn.2021.03.002
9. Yamashita T, Kohara K, Tabara Y, et al. Muscle mass, visceral fat, and plasma levels of B-type natriuretic peptide in healthy individuals (from the J-SHIPP Study). Am J Cardiol. 2014;114:635–640. doi:10.1016/j.amjcard.2014.05.050
10. PASS 15 power analysis and sample size software. Kaysville, UT: NCSS LLC.; 2015. ncss.com/software/pass.
11. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–383. doi:10.1016/0021-9681(87)90171-8
12. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150:604–612. doi:10.7326/0003-4819-150-9-200905050-00006
13. Bouillanne O, Morineau G, Dupont C, et al. Geriatric nutritional risk index: a new index for evaluating at-risk elderly medical patients. Am J Clin Nutr. 2005;82:777–783. doi:10.1093/ajcn/82.4.777
14. Rubenstein LZ, Harker JO, Salva A, Guigoz Y, Vellas B. Screening for undernutrition in geriatric practice: developing the short-form mini-nutritional assessment (MNA-SF). J Gerontol a Biol Sci Med Sci. 2001;56:M366–72. doi:10.1093/gerona/56.6.M366
15. Hussain A, Sun W, Deswal A, et al. Association of NT-ProBNP, blood pressure, and cardiovascular events: the ARIC study. J Am Coll Cardiol. 2021;77:559–571. doi:10.1016/j.jacc.2020.11.063
16. Daniels LB, Maisel AS. Natriuretic peptides. J Am Coll Cardiol. 2007;50:2357–2368. doi:10.1016/j.jacc.2007.09.021
17. Bordicchia M, Liu D, Amri EZ, et al. Cardiac natriuretic peptides act via p38 MAPK to induce the brown fat thermogenic program in mouse and human adipocytes. J Clin Invest. 2012;122:1022–1036. doi:10.1172/JCI59701
18. Chien SC, Chandramouli C, Lo CI, et al. Associations of obesity and malnutrition with cardiac remodeling and cardiovascular outcomes in Asian adults: a cohort study. PLoS Med. 2021;18:e1003661. doi:10.1371/journal.pmed.1003661
19. Raslan M, Gonzalez MC, Dias MC, et al. Comparison of nutritional risk screening tools for predicting clinical outcomes in hospitalized patients. Nutrition. 2010;26:721–726. doi:10.1016/j.nut.2009.07.010
20. Chen LK, Woo J, Assantachai P, et al. Asian working group for sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Am Med Dir Assoc. 2020;21:300–307e2. doi:10.1016/j.jamda.2019.12.012
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Interprofessional Treatment of Malnutrition and Sarcopenia by Dietitians and Physiotherapists: Exploring Attitudes, Interprofessional Identity, Facilitators, Barriers, and Occurrence
Reinders JJ, Hobbelen JSM, Tieland M, Weijs PJM, Jager-Wittenaar H
Journal of Multidisciplinary Healthcare 2022, 15:1247-1260
Published Date: 31 May 2022
Cutoff Value of Psoas Muscle Area as Reduced Muscle Mass and Its Association with Acute Pancreatitis in China
Fu H, Li P, Xing Q, Jiang H, Sui H
International Journal of General Medicine 2023, 16:2733-2751
Published Date: 30 June 2023
Interprofessional Management of (Risk of) Malnutrition and Sarcopenia: A Grounded Theory Study from the Perspective of Professionals
Boxum SD, van Exter SH, Reinders JJ, Koenders N, Drenth H, van den Berg MGA, Tieland M, Spoorenberg SLW, Finnema EJ, van der Wees PJ, Jager-Wittenaar H
Journal of Multidisciplinary Healthcare 2024, 17:4677-4692
Published Date: 9 October 2024
Understanding the Needs and Wishes of Older Adults in Interprofessional Treatment for Malnutrition and Sarcopenia: A Grounded Theory Study
Boxum SD, Van Exter SH, Reinders JJ, Drenth H, Van den Berg MG, Tieland M, Geluk-Bleumink A, Spoorenberg SL, Finnema E, Van der Wees PJ, Koenders N, Jager-Wittenaar H
Journal of Multidisciplinary Healthcare 2025, 18:1433-1444
Published Date: 11 March 2025