Back to Journals » Advances in Medical Education and Practice » Volume 14
Making an Impact with E.M.P.A.C.T. Engage, Mentor Prepare, Advocate, Cultivate, and Teach: An Innovative Pilot Mentoring Program Evaluation for Students Underrepresented in Medicine
Authors Henry TL ![]() , Freeman CD, Sheth A, Jenkins L, Olakunle OE, Adeagbo S, Sanchez-Medina MC, Alcegueire K, Rodríguez J
, Freeman CD, Sheth A, Jenkins L, Olakunle OE, Adeagbo S, Sanchez-Medina MC, Alcegueire K, Rodríguez J ![]()
Received 16 December 2022
Accepted for publication 8 July 2023
Published 21 July 2023 Volume 2023:14 Pages 803—813
DOI https://doi.org/10.2147/AMEP.S400547
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Tracey L Henry,1 Christian D Freeman,2 Anisha Sheth,3 Lauren Jenkins,1 Oreoluwa E Olakunle,1 Segun Adeagbo,1 Mariana C Sanchez-Medina,1 Kara Alcegueire,4 Josué Rodríguez1
1Division of General Medicine, Emory University School of Medicine, Atlanta, GA, USA; 2University of California San Francisco, Department of Obstetrics and Gynecology, San Francisco, CA, USA; 3Emory University Rollins School of Public Health, Atlanta, GA, USA; 4University of Miami, Department of Medicine, Miami, FL, USA
Correspondence: Tracey L Henry, Email [email protected]
Purpose: Medicine has yet to increase the representation of historically excluded persons in medicine to reflect the general population. The lack of support and guidance in the medical training of these individuals is a significant contributor to this disparity. The Engage, Mentor, Prepare, Advocate for, Cultivate, and Teach (EMPACT) Mentoring program was created to address this problem by providing support for learners who are historically underrepresented in medicine (URiM) as they progress through medical school.
Methods: The EMPACT Pilot Program was formed and conducted during the 2019– 2020 academic year. A total of 19 EMPACT mentorship groups were created, each consisting of two mentors and four medical student mentees. Additionally, four professional development workshops were held along with a final Wrap-up and Awards event. Pre and post pilot program surveys along with surveys after each workshop and focus groups were conducted with a random selection of program participants.
Results: When compared to data from before and after the implementation of the EMPACT program, there were statistically significant differences (p < 0.05) in EMPACT mentees reporting they agree or strongly agree they felt ready to handle their clinical rotations (28% to 65%), felt the need to have an advocate (85% to 47%), possessed insight on day-to-day activities of an attending (26% to 56%) and felt a sense of community (79% to 94%). Mentors revealed an increase in their awareness of the concepts of microaggressions and imposter phenomenon. Finally, both groups felt an increase in their support system and sense of community at the school of medicine.
Conclusion: Despite COVID-19 limitations, the EMPACT program met its goals. We effectively supported URiM medical students through mentorship, networking, and community.
Keywords: mentoring, equity, workforce, URiM, medical education
Plain Language Summary
A structured mentoring program can address the unique needs of historically underrepresented in medicine (URiM) learners in undergraduate medical education. Increasing the number of physicians from historically excluded communities requires a careful consideration of the factors that contribute to this problem. EMPACT provides a model of how to create and implement a successful mentorship program that addresses contributors to low retention and increased attrition of URiM students. Mentoring programs such as EMPACT can promote effective mentor training, physician–student relationships, and success in medical school and their medical careers for mentors and mentees.
Introduction
Diversity in the physician workforce should mirror our nation’s diversity.1 Racial and ethnic minorities, specifically Blacks or African Americans, American Indian or Indigenous peoples, and Hispanic and/or Latinx/o/a total over 30% of the US population; however, they represent around 12% of the physician workforce.2–4 Given that health disparities and inequitable access to health-care services are pervasive in resource poor ethnic minority communities,5 a diverse physician workforce is a necessary step toward eradicating these inequities by increasing cultural humility and cost-effective care for all.5,6 For example, black patients with black doctors were 72% more likely to get a cholesterol test and 47% more likely to get diabetes screening compared to a black patient seeing a white doctor.7 A diverse physician workforce increases trust between patients and doctors, while mitigating biases in the clinical setting, leading to better outcomes.8 Of note, students of marginalized communities are subsequently more likely to return to work in medically underserved marginalized communities after training.9
However, once some students who are historically underrepresented in medicine (URiMs) enter undergraduate medical education (UME) as a part of increasing diversity, other obstacles exist: lack of mentorship and support, awareness of URiM unique needs, engagement with faculty members of color, in addition to experiencing biases, microaggressions and/or even racism in educational settings. URiMs face distinctive barriers at all stages of their education and professional development leading to disproportionate feelings of isolation, self-doubt, and fear in comparison to their counterparts thus affecting their performance and academic success.10
Yet, most of the barriers begin before they begin their professional journey. Often URiM students grow up in settings with fewer opportunities for career development and limited social mobility. In some cases, food and housing instability, as well as physical safety, play a role in their upbringing.10 Dealing with trauma, lack of exposure to different positive experiences, and stress of new environments with uncertainty due to fear and racism can be detrimental to future and current medical students.10 After medical students have matriculated, an additional host of barriers exist including: adapting to the culture of medicine, resource disparities, stigmatization of seeking help, and lack of institutional accountability.10
It is essential to acknowledge that URiM students come from a diverse range of cultures with unique values, norms, and traditions that play a role in their professional development. For example, research shows that Hispanic and/or Latinx/o/a, American Indian or Indigenous American, and Black or African American cultures often value communal goals more than individualist goals. Disregard for some of these unique cultural values, combined with resource disparities, and stigmatization of seeking help, can lead to more URiMs to struggle.11 Additionally, institutions do not always offer culture-specific help due to lack of resources, awareness of need, URiM faculty and/or dedicated faculty or staff to address these needs.12–15
In order to mitigate the unique challenges of URiM students, innovative evidence-based solutions are needed. Mentorship programs posit a possible solution to ensuring the success of URiM students in medical school. As such, in the fall of 2019, we piloted a structured mentorship program, EMPACT. The mission of EMPACT is to Engage, Mentor, Prepare, Advocate for, Cultivate, and Teach URiM medical students in a supportive and inclusive learning environment. EMPACT provides students who self-identify as underrepresented in medicine and/or come from disadvantaged backgrounds with experiences that foster timely and successful progress through medical school and graduation.
EMPACT builds upon previous research and seeks to increase URiM faculty mentorship and peer-to-peer support, thus creating a pathway that can help URiM medical students succeed.10,16 The program goals for EMPACT are to address their unique needs, strengthen social support with structured mentoring relationships, cultivate a sense of community, help mitigate barriers adapting to the culture of medicine, and promote personal and professional growth for URiMs.
EMPACT was designed to address the needs of URiM students and trainees. The short-term goal for this mentoring program is to support underrepresented minorities in medicine in ways that are sensitive to their unique backgrounds, challenges, values, and goals. The long-term goal is to not only increase diversity within medical schools and the physician workforce but also to maximize equity, inclusion and ultimately belonging whereby maximizing success of URiMs. Although there is an abundance of evidence on becoming a mentor,17,18 there is still a lack of research demonstrating how to develop a robust mentoring program. The EMPACT program helps fill in these gaps by showing the impact of direct guided mentorship on mentees, while providing consistent educational resources for both sides of the relationship.19
Methods
Basic Framework of the Program
A needs assessment was conducted and completed by URiM medical student learners in 2017 at the school of medicine. See Appendix 1. We created 19 groups of 3–4 medical school students (M1-M4) with two overarching faculty (attending and resident/fellow physicians). See Table 1. Students filled out a survey at the end of the initial introductory EMPACT mentoring event ranking the top three mentors they desired to be paired with in a mentoring group along with selection of their choice of peer mentors as well. Students had three options: to be randomly paired with a mentor and peer mentee group, be paired based upon their specialty of interest and/or simply be paired based on their organic interaction with the potential mentors and peers that evening of the introductory EMPACT mentoring event. In most cases, per students, it was a combination of organic interactions and interest in the specialty of the mentor.
 |
Table 1 Demographics of Medical Students and Mentors in the Program |
The goals for these groups were to promote peer mentoring, leadership, accountability, and networking among its members. A trickle-down effect of mentoring was expected, as the more senior medical student mentee (M3 or M4) would also mentor the junior medical students (M1 or M2) enabling participants to learn about the culture of medicine and strategies to handle potential pitfalls more common to their own demographic and medical school cohort.
The EMPACT Program Director led the mentorship program, facilitated the mentorship pairings, recruited faculty and resident/fellow participants, conducted check-ins regularly with the program participants to ensure it is accomplishing its goals, and ultimately organized programing where all URiM faculty and students could interact and cultivate relationships. Additional administrative support was required to help with flyers, reserving rooms, inputting events on the school calendars and ordering food.
Events and Programming
The EMPACT Pilot Program was conducted between October 2019 and May 2020. A total of 19 EMPACT mentorship groups were created from the October Mentoring Mixer. The Mentoring Mixer event enabled students to meet and engage with URiM faculty via dinner, speed mentoring activity and networking opportunities with guided questions. Furthermore, four workshops were held for EMPACT student mentees and mentors between March 2020 and May 2020: Addressing Microaggressions and Upstander Training, Maintaining Wellness during COVID-19, Overcoming the Imposter Phenomenon, and a CV Building Workshop. A final EMPACT Wrap-up event was held in May 2020 in which outstanding mentors and mentees were recognized. See Table 2 for themes with illustrative quotes from EMPACT participants on impact of programming and lessons learned.
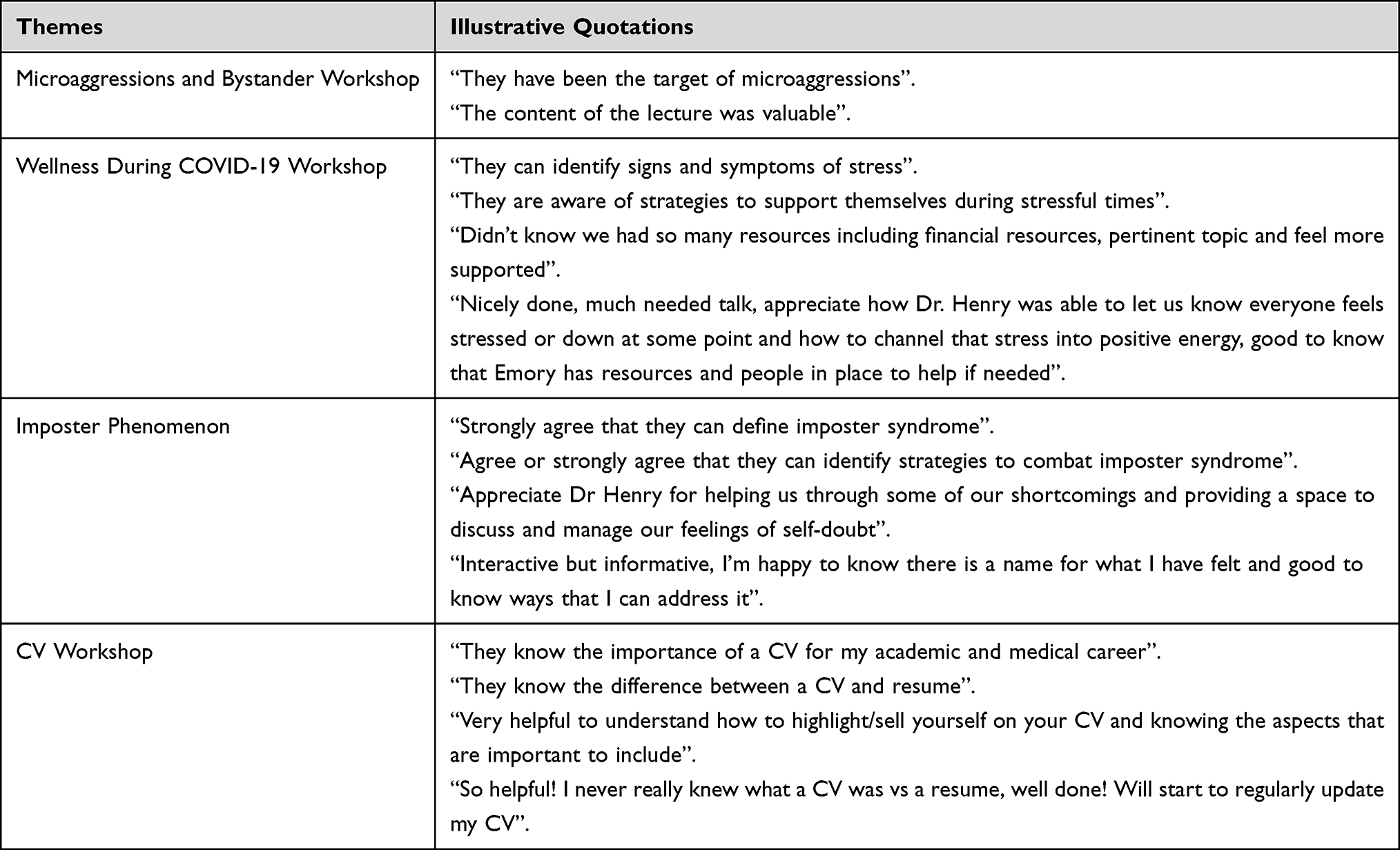 |
Table 2 Themes with Illustrative Quotations |
Data Collection
Pre and post surveys were administered at the start of the EMPACT Program (October 2019) and at the end of the year (May 2020) See Appendix 2. The EMPACT Program Survey consisted of 30 questions along with additional demographics. Out of 69 students, 40 students completed the pre-survey (58.0%) and 34 students completed the post-survey (49.3%). Out of 38 mentors, 15 mentors completed the pre-survey (39.5%) and 16 mentors completed the post-survey (42.1%).
After each of the four EMPACT workshops, post-surveys were administered to workshop participants. Additionally, students and mentors were randomly selected for a phone call to ask about their experiences with the EMPACT program and gauge participation. Statistical significance was measured using 2×2 chi square analysis for the survey results. Qualitative data from phone interviews were reviewed for thematic analysis.
Results
EMPACT Mentorship Group Meetings
There was a total of 69 medical students and 38 mentors in the inaugural EMPACT mentoring program. Of the mentors and students who were randomly selected for a phone call to inquire about their level of engagement and satisfaction with their EMPACT mentoring group, 15 mentors and 34 students completed the phone interview. Students and mentors both reported an average of meeting three times after being matched in mentoring groups after the introductory mentoring mixer. Among those who met with their mentoring group, the most common mode of communication was email (37%), followed by in-person (25%) and video-based virtual platform (eg, Zoom) (25%). They were also asked the reason, content or topic(s) of their EMPACT mentoring group meeting(s). Among those who met with their mentoring group, the most common topics were introductions (29%), career advice (21%), general content (18%), and academic advice (14%). See Figure 1.
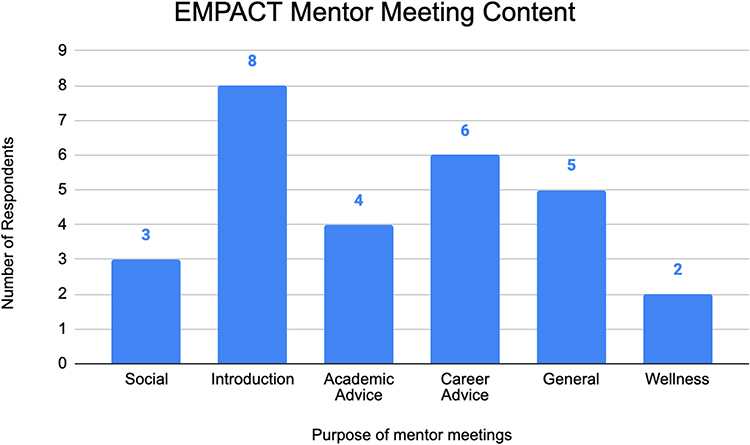 |
Figure 1 Purpose of EMPACT Mentor Meetings. |
Impact of Educational Workshops
Surveys were administered to workshop attendees upon completion of each workshop. The median attendance for these workshops was 30 (SD = 3.65) and the median survey responses was 17.5 (SD = 2.38).
Pre and Post EMPACT Mentoring Program Survey Results
The vast majority of EMPACT students and mentors 95% and 82%, respectively, were aware of the term microaggressions prior to the EMPACT program. There was a clear increase trend (but not statistically significant) in mentors’ awareness of the term microaggressions (82 to 100%) and how to address microaggressions (45 to 69%), as well as students’ knowledge of how to address microaggressions (54% to 65%) when reviewing responses from before and after the EMPACT program.
Most EMPACT students were aware of the term imposter phenomenon (98%) prior to the EMPACT program and there was no significant difference in feelings of having imposter phenomenon (60–50%) before and after the program for medical students. For mentors, there was a statistically significant increase in awareness of the term imposter phenomenon (70% to 100%, p < 0.05) after the program and a statistically significant increase in mentors reported feeling they have imposter phenomenon (10% to 56%, p < 0.05) when compared to responses prior to starting the EMPACT program.
There was a statistically significant increase in the number of medical students that feel ready to handle their clinical education and/or clinical rotations (28% to 65%, p < 0.05), as well as having an insight into the day-to-day activities of attending (26% to 56%, p < 0.05) when comparing before and after the EMPACT Program. See Table 3.
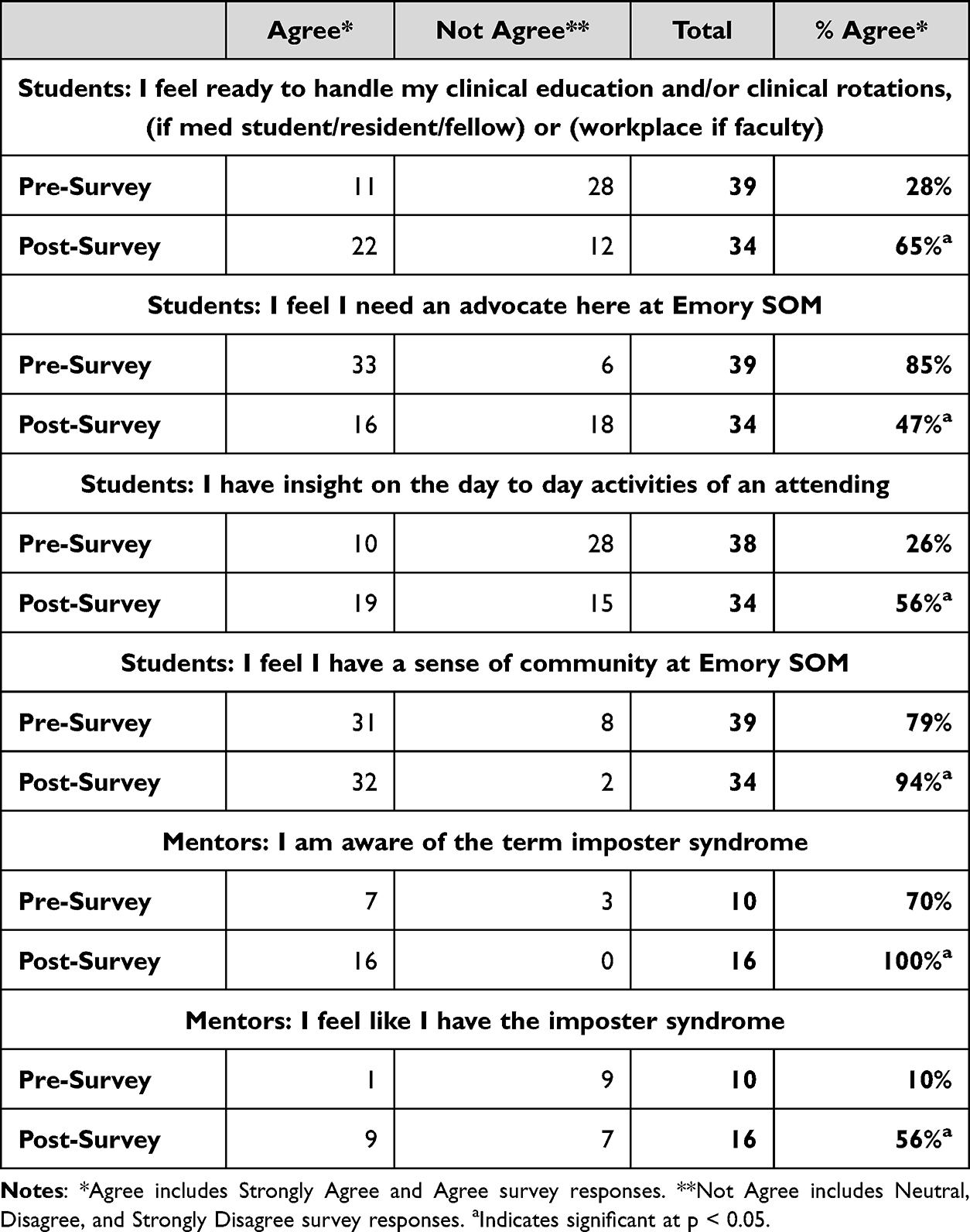 |
Table 3 Participant Attitudes Toward Their Experience at Emory Pre and Post Involvement in the EMPACT Pilot Mentoring Program |
There was a statistically significant increase for mentors and students in feeling that there is a good social support system and in feeling that they have a good sense of community at Emory SOM (79% to 94%, p < 0.05) when comparing before and after the EMPACT program. There was also a significant decrease in feeling the need to have an advocate at Emory (85% to 47%, p < 0.05). See Table 3.
In addition, although not statistically significant, there was a noticeable trend with an increase in the amount of student awareness of resources available if experiencing academic or personal difficulty and in feelings of confidence in having the resources needed to excel at Emory SOM for both students and mentors when comparing the responses before and after the EMPACT program.
Finally, EMPACT mentors and mentees were randomly selected for a phone interview to inquire about their experience in the EMPACT program and to gauge participation. Thirty-four (49.3%) EMPACT student mentees and 15 (39.5%) EMPACT mentors completed the phone interview. Of those students who completed the phone interview, 94% of students would recommend the EMPACT program to other students. The majority of mentors and mentees were satisfied or very satisfied with the EMPACT educational experience (93% and 79%, respectively) and the program overall (87% and 85%, respectively). See Figure 2.
 |
Figure 2 EMPACT Mentee and Mentor Satisfaction. |
Discussion
Overall, the EMPACT program was successful in its goals to support URiM medical students. Success was defined as an increase in perceived professional and social development, support from community, and wellness for URiM mentees. Our data demonstrated that 94% of mentees would recommend the EMPACT program to other mentees with 93% of mentors recommending the program to future mentors.
This pilot mentoring program demonstrates not only the viability of evidence-based structured mentoring programs but also the positive impact on mentees. Furthermore, it shines a light on the necessity to engage URiM students in structured mentoring programs that build and maintain sustainable mentorship engagement. As seen in our intervention, such programs have the potential to greatly impact readiness for clinical clerkships, insight on specialties, and sense of community. Notably, structured mentorship programs give mentees readily accessible and experienced advocates. Prior research has shown that racial/ethnic concordance between the mentor and mentee inspires students and provides positive influences towards their possibilities and alleviates concerns about explaining the context and nuances associated with their demographic.20 Having a designated mentor equips students to handle the unforeseen circumstances they might experience as URiMs, while providing a space for professional relationships to flourish. Moreover, dedicated mentors provided and assisted students with opportunities such as other networking events (eg, specialty-specific), scholarships, research, shadowing, and leadership positions.
Unique to our program is the joint faculty and near peer mentoring which allowed the trickle-down effect of mentoring and for learners to have a glimpse of the future through more senior students, residents/fellows, or faculty. As opposed to physician-student mentorship, there is less impedance from a hierarchical framework in peer-to-peer mentorship between academic years and thus has the added benefit of fostering collaboration, trust, and empowerment at a faster rate.21 There was a concerted effort to dedicate time and resources for intentional networking and targeted career development throughout the academic year along with clear expectations and responsibilities outlined for mentors and mentees.
Our data also revealed some surprising differences between mentors and mentees concerning knowledge of certain realities experienced in medicine. For example, mentees were more aware and knowledgeable of microaggressions than mentors and some of our mentors initially did not understand the concept of impostor phenomenon. Before the start of the program, 10% of mentors reported they felt they had the impostor phenomenon, while 60% of mentees reported they felt they had the impostor phenomenon. At the end of the program, 56% of mentors felt like they had imposter syndrome while only 50% of mentees felt like they possessed it. The decreasing trend in how mentees felt could have been attributed to the increased confidence in their self-efficacy and additional support from faculty and peers, which would further support the success of the EMPACT program. Particularly, more mentors may have felt they had the imposter phenomenon at the end of the program because over 60% of mentors were junior faculty, residents, or fellows who likely experience similar issues as our UriMs mentees (ie, microaggressions and work-life integration) and could possibly now map their experience onto a studied sensation. These results illustrate the importance of mentor training and faculty development before serving as a mentor as the concept of imposter phenomenon is not exclusive to newer generations, yet it is discussed more in current medical education.
Mentors must understand the changing environment of medical education to create opportunities for personal and professional growth, particularly necessary for the unique needs of URiM students. Thus, we incorporated educational activities and workshops into our mentorship program with resources on how to succeed in medicine to promote discussion and knowledge sharing. Workshops (eg, note writing and mock patient interviews) provide medical students direct supervision in preparation for clinical rotations and provide further insight into the information pertinent to each medical specialty prior to their patient presentations.22 In this regard, our EMPACT mentees build rapport with their mentor and gain an enhancement in their confidence both personally and professionally.
Limitations
There were several limitations that could have affected the impact of the program. One major limitation was the COVID-19 pandemic because it prevented the program from being executed as intended. This may have affected the number of meetings mentoring groups held and decreased the feelings of connectedness and satisfaction with the program. Aside from COVID-19, there were some challenges with the surveys that could have affected the data. The pre and post surveys may have been completed by different respondents since the data was collected anonymously. In addition, the survey did not ask respondents whether they attended the workshops, which may have provided more insight into tracking pre and post outcomes for those who attended the workshops. The EMPACT pre and post survey also did not evaluate the one-on-one mentoring URiM students likely underwent, which included study strategies, assistance with scholarships and manuscripts, or facilitated connections to other mentors and programs. Lastly, schedules of medical students by academic year (M1-M4) are not aligned, making it difficult to find mutual times where all four classes could meet and provide additional barriers to participation and further peer-to-peer support.
Future Directions
We plan to incorporate a more diverse URiM population by actively reaching out to members of other URiM groups to encourage participation. Some students from other AAMC-defined URiM groups expressed assumptions that the program was only for one demographic. Also prudent is to track data for EMPACT mentee participants’ academic performance, professional satisfaction, and feelings of inclusivity and belonging over time. As it relates to educational performance (pass, fail, time to graduate, match rates) of the URiM students in the mentoring program and compare to profiles of prior URiMs before the mentoring program was implemented. We will seek additional support for regular check-ins to ensure mentoring groups are meeting regularly, determine the effectiveness of their meetings and to address any challenges that arise. Also, we aim to determine the feasibility and accessibility of a website or in-person location to contain our academic resources.
Even though all EMPACT participants were highly encouraged to attend all EMPACT events (workshops, panels, mixer, etc.), some did not due to competing demands. Nonetheless, given many, including junior faculty, often experience issues with microaggressions, imposter phenomenon, and work life integration, our data suggest that educational career building sessions in our program would have benefitted them.
Conclusion
EMPACT was designed to address the unique needs of URiM students in a systematic structured fashion. Programs like this best work when a needs assessment is conducted before spearheading a new structured mentoring program. These needs assessments serve as a blueprint for which events, workshops or panels are necessary to maximize success for your students. Planning of workshops, mentoring events, and recruitment requires engaged faculty, staff, and students that can effectively communicate and work as a team to provide a program that is attentive to needs of the mentees, mentors, and the changing educational environment. Institutional buy–in and resources such as a mentoring program director and program coordinator are paramount. EMPACT opens the door to the dramatic impact that educational institutions can have on URiM learner professional development and academic success via a well-guided structured mentoring program. Our program attempted to maximize impact via regular and consistent feedback to adapt to the changing needs of both mentors and mentees.
Increasing the number of physicians from historically excluded communities requires a careful consideration of the factors that contribute to this problem. EMPACT provides a model of how to create and implement a successful mentorship program that addresses contributors to low retention and increased attrition of URiM students. Mentoring programs such as EMPACT can promote effective mentor training, physician–student relationships, and success in medical school and their medical careers for mentors and mentees.
Ethics Statement
The Emory University School of Medicine’s Institutional Review Board (IRB) determined this quality improvement study was exempt from further review in May 2020. Additionally, the IRB policy states that our category of human subjects research is exempt from additional informed consent, as it is, “Research that only includes interactions involving tests (cognitive, diagnostic, aptitude, achievement), survey procedures, interview procedures, or observation of public behavior (including visual or auditory recording) since the following criteria met: The information obtained is recorded by the investigator in such a manner that the identity of the human subjects cannot readily be ascertained, directly or through identifiers linked to the subject; and that any disclosure of the human subjects’ responses outside the research would not reasonably place the subjects at risk of criminal or civil liability or be damaging to the subjects’ financial standing, employability, educational advancement, or reputation”.
Acknowledgments
The authors wish to thank Bernice Fokum, MD, MPP University of Chicago, Department of Emergency Medicine. Mojibade Hassan, MD, PhD, University of Florida, College of Medicine. Yolanda Hood, PhD, Director, Office of Multicultural Affairs, Emory University School of Medicine, Marilane B. Bond, EdD, MEd, MBA, Associate Dean, Medical Education, UME, GME, CME and Health Professions, Emory University School of Medicine and Sheryl L. Heron, MD, MPH, FACEP, Associate Dean – Community Engagement, Equity & Inclusion/Chief Diversity Officer, Professor and Vice-Chair of Faculty Equity, Engagement & Empowerment, Department of Emergency Medicine, Emory University School of Medicine.
Disclosure
The authors have no conflicts of interest to report.
References
1. Laveist TA, Nuru-Jeter A. Is doctor-patient race concordance associated with greater satisfaction with care? J Health Soc Behav. 2002;43(3):296–306. doi:10.2307/3090205
2. U.S. Census Bureau QuickFacts: United States. United States Census Bureau. Available from: https://www.census.gov/quickfacts/fact/table/US/PST045221.
3. AAMC. Diversity in medicine facts and figures 2019: figure 18-Percentage of all active physicians by race/ethnicity; 2018. Available from: https://www.aamc.org/data-reports/workforce/interactive-data/figure-18-percentage-all-active-physicians-race/ethnicity-2018.
4. AAMC. Underrepresented in medicine definition; 2021. Available from: www.aamc.org/what-we-do/diversity-inclusion/underrepresented-in-medicine.
5. Saha S, Komaromy M, Koepsell TD, Bindman AB. Patient-physician racial concordance and the perceived quality and use of health care. Arch Intern Med. 1999;159(9):997–1004. doi:10.1001/archinte.159.9.997
6. Association of American Medical Colleges. Diversity in Medical Education: Facts & Figures 2016. Washington DC: Association of American Medical Colleges; 2016.
7. Alsan M, Garrick O, Graziani G, et al. Does diversity matter for health? Experimental Evidence from Oakland. NBER. Available from: www.nber.org/papers/w24787.
8. Hoffman KM, Trawalter S, Axt JR, Oliver MN. Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between blacks and whites. Proc Natl Acad Sci. 2016;113(16):4296–4301. doi:10.1073/pnas.1516047113
9. Walker KO, Moreno G, Grumbach K, et al. The association among specialty, race, ethnicity, and practice location among California physicians in diverse specialties. J Natl Med Assoc. 2012;104(1–2):46–52. doi:10.1016/s0027-9684(15)30126-7
10. Taylor SM. The health care career pipeline: a program director’s reflection on extending the resources of the University to the minority student community. National Academy of Medicine. Available from: nam.edu/the-health-care-career-pipeline-A-program-directors-reflection-on-extending-The-resources-of-The-university-to-The-minority-student-community/.
11. Estrada M, Burnett M, Campbell AG, et al. Improving Underrepresented Minority Student Persistence in STEM. CBE Life Sciences Education, American Society for Cell Biology; 2016. Available from: www.ncbi.nlm.nih.gov/pmc/articles/PMC5008901/.
12. Carnes M, Schuler L, Sarto GE, Lent SJ, Bakken L. Increasing sex and ethnic/racial diversity of researchers in aging: some promising strategies at the postdoctoral level. J Am Geriatr Soc. 2006;54(6):980–985. doi:10.1111/j.1532-5415.2006.00739.x
13. Johnson JC, Jayadevappa R, Taylor L, Askew A, Williams B, Johnson B. Extending the pipeline for minority physicians: a comprehensive program for minority faculty development. Acad Med. 1998;73(3):237–244. doi:10.1097/00001888-199803000-00011
14. Palepu A, Carr PL, Friedman RH, Amos H, Ash AS, Moskowitz MA. Minority faculty and academic rank in medicine. JAMA. 1998;280(9):767–771. doi:10.1001/jama.280.9.767
15. Fang D, Moy E, Colburn L, Hurley J. Racial and ethnic disparities in faculty promotion in academic medicine. JAMA. 2000;284(9):1085–1092. doi:10.1001/jama.284.9.1085
16. Nellis JC, Eisele DW, Francis HW, Hillel AT, Lin SY. Impact of a mentored student clerkship on underrepresented minority diversity in otolaryngology-head and neck surgery. Laryngoscope. 2016;126(12):2684–2688. doi:10.1002/lary.25992
17. Kurré J, Bullinger M, Petersen-Ewert C, Guse A. [Pdf] differential mentorship for medical students: development, implementation and initial evaluation: semantic scholar; 1970. Available from: https://www.semanticscholar.org/paper/Differential-mentorship-for-medical-students%3A-and-Kurr%C3%A9-Bullinger/e3ac434d867ae7c2c9ac5d894d0d09c654919160.
18. Wingard DL, Garman KA, Reznik V. Facilitating faculty success: outcomes and cost benefit of the UCSD national center of leadership in academic medicine. Acad Med. 2004;79(10 Suppl):S9–11. doi:10.1097/00001888-200410001-00003
19. Bussey-Jones J, Bernstein L, Higgins S, et al. Repaving the road to academic success: the IMeRGE approach to peer mentoring. Acad Med. 2006;81(7):674–679. doi:10.1097/01.ACM.0000232425.27041.88
20. Yehia BR, Cronholm PF, Wilson N, et al. Mentorship and pursuit of academic medicine careers: a mixed methods study of residents from diverse backgrounds. BMC Med Educ. 2014;14:26. doi:10.1186/1472-6920-14-26
21. Maloof PS. Mentoring: an evidence-based strategy to increase diversity among students and faculty from racial and ethnic groups underrepresented in maternal and child health training programs. National Center for Cultural Competence. Center for Child and Human Development. Georgetown University; 2012.
22. Griffith E, McGowan H, Wilson A. A department-wide mentoring initiative to encourage URM student success in statistics; 2017. Available from https://diversity.ncsu.edu/wp-content/uploads/2017/09/Griffith-and-Gowen-Final-Report.pdf.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
How Do Medical Students Perceive Their Research Experiences and Associated Challenges?
Alyousefi N, Alnojaidi J, Almohsen A, Alghanoum S, Alassiry G, Alsanad L, Alzeer S
Advances in Medical Education and Practice 2023, 14:9-20
Published Date: 6 January 2023