Back to Journals » Infection and Drug Resistance » Volume 16
Lumbar Spine Infection with Eikenella corrodens Presented as Abdominal Pain: A Case Report and Literature Review
Authors Cheng H ![]() , Tan N, Lu Y, Wu H, Liu Z, Zhang D, Xu Z, Li C
, Tan N, Lu Y, Wu H, Liu Z, Zhang D, Xu Z, Li C
Received 7 December 2022
Accepted for publication 8 February 2023
Published 13 March 2023 Volume 2023:16 Pages 1407—1417
DOI https://doi.org/10.2147/IDR.S400451
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Hanwen Cheng,1,* Ni Tan,2,* Yiwen Lu,3,* Haoyu Wu,1 Zhuojie Liu,1 Di Zhang,1 Zixin Xu,4 Chunhai Li1,5
1Department of Orthopaedics, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangzhou, Guangdong Province, People’s Republic of China; 2Cellular & Molecular Diagnostics Center, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, Guangdong Province, People’s Republic of China; 3Breast Cancer Center, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangzhou, Guangdong Province, People’s Republic of China; 4Department of Urology, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangzhou, Guangdong Province, People’s Republic of China; 5Teaching and Research Bureau of Surgery, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangzhou, Guangdong Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chunhai Li, Department of Orthopaedics, Sun Yat-sen Memorial Hospital, Sun Yat‐sen University, Guangzhou, Guangdong Province, 510000, People’s Republic of China, Tel +86-18602079796, Fax +86-2081332523, Email [email protected]
Background: Eikenella corrodens is a part of the inherent flora on the surface of human mucosa. It usually does not cause disease unless the patient has been bitten, injured or surgically infected. Lumbar spine infection caused by Eikenella corrodens usually presents with conventional symptoms such as low back pain and fever. Herein, we report a case of lumbar intervertebral space infection with Eikenella corrodens presented as abdominal pain.
Case Presentation: A 38-year-old man with no medical history of note presented with abdominal pain. Initially, local doctors suspected that the patient had abdominal disease. However, abdominal diseases were ruled out and only lumbar spine infection was confirmed. Then, the patient was misdiagnosed as lumbar tuberculosis. Finally, anaerobic culture and metagenomic next-generation sequencing confirmed the Eikenella corrodens, which was rarely involved in lumbar intervertebral space infection. The patient recovered after operation and antibiotic therapy.
Conclusion: This case indicated a rare symptom of lumbar spine infection, abdominal cramping, which is caused by Eikenella corrodens. Blood culture had low sensitivity as a diagnostic method for Eikenella corrodens, but lesion sample culture or metagenomic next-generation sequencing had high sensitivity for early diagnosis.
Keywords: non-specific spinal infection, lumbar intervertebral space infection, metagenomic next-generation sequencing, misdiagnosis
Introduction
Non-specific spinal infection (NSI), a rare and challenging entity, represents as intervertebral space infection and vertebral osteomyelitis. Due to its non-specific clinical symptoms, imaging examinations and laboratory examinations, it is often misdiagnosed as spinal tuberculosis or tumor.1,2
Eikenella corrodens is a part of the inherent flora on the surface of human mucosa. It is often isolated from specimens of upper respiratory tract, gastrointestinal tract or urogenital tract.3 However, it usually does not cause disease unless the patient has been bitten, injured or surgically infected. This kind of bacteria can lead to endocarditis, NSI, osteomyelitis, perirenal abscess and so on.4–8 For the past several decades, there were 16 cases of orthopaedic-related infections caused by Eikenella corrodens (Table 1 and Table 2). In these cases, since the blood culture was hard to confirm Eikenella corrodens, clinicians faced great challenges in early diagnosis.
 |
Table 1 The Basic Information of Patients and the Method of Diagnosis |
 |
Table 2 Antibiotic Use and Surgical Records of Patients |
Herein, a healthy middle-aged man with an unexplained lumbar intervertebral space infection (LISI) had been presented. This was the first case of LISI of Eikenella corrodens presented as abdominal pain. Based on the present case and other 16 orthopaedic-related cases, the characteristics of Eikenella corrodens were analyzed to provide more clinical practice experiences for the diagnosis and treatment.
Case Presentation
On September 25th, 2021, a 38-year-old Chinese man went to a local hospital for his left lower abdominal pain (Figure 1). The patient was hospitalized and given symptomatic treatment such as fasting, antispasmodic, analgesic, enema and nutritional support. Subsequently, the abdominal diseases were ruled out by examinations. On October 2nd, 2021, after one week of empirically treated with levofloxacin intravenously (unknown dose), his abdominal pain was relieved and he was discharged.
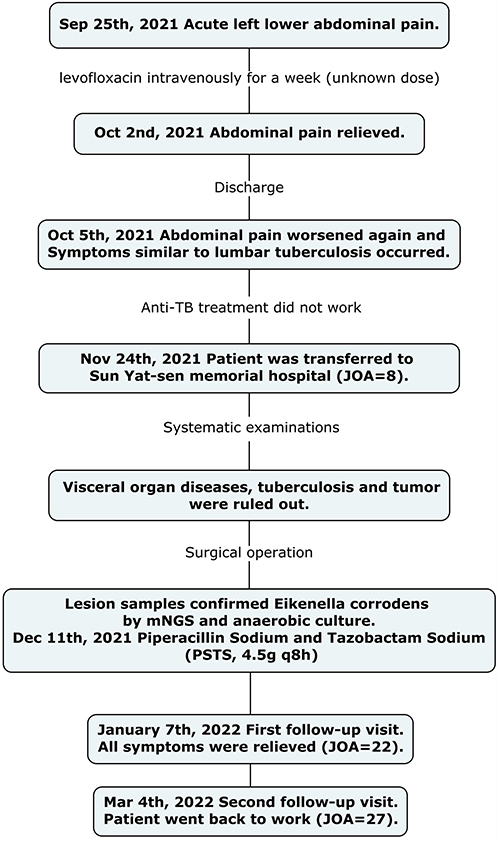 |
Figure 1 Flow chart of the entire procedures from onset to cure in the present case. |
However, on October 5th, 2021, the patient complained of left lower abdominal pain again, which could spread to the entire abdomen quickly. Meanwhile, he began to suffer from continuous low back pain and a low-grade fever in the afternoon (fluctuations at 37–38 degrees Celsius). Based on the symptoms and the lumbar spine magnetic resonance (MR) images (Supplementary Figure 1) of the patient, the local doctors thought there was a possibility of lumbar (L3/4) tuberculosis (TB). After receiving anti-TB treatment, the patient was discharged.
On November 24th, 2021, the patient was transferred to Sun Yat-sen memorial hospital as his condition continued to deteriorate. His vital signs were within normal limits, his body weight dropped 10% in two months and he went without a bowel movement for a week. On detailed consultation, the history of underlying diseases, bites, surgery, betel nut addiction and oral uncleanness were excluded. Then, a systematic physical examination confirmed that he had lower abdominal pain, especially in his left lower abdomen. Apart from that, he had percussion pain in the spinous process of the lumbar spine (L3, L4) and limited lumbar mobility. The patient reported his visual analogue scale (VAS) score of lower abdominal pain was 8, the VAS score of low back pain was 6 and the lumbar spine Japanese Orthopaedic Association Scores (JOA) was 8.
After admission to Sun Yat-sen memorial hospital, MR, computed tomography (CT), ultrasonography and endoscopy ruled out visceral organ diseases. X-ray images showed the intervertebral space height between L3 and L4 was decreased (Figure 2). His lumbar spine CT images showed a large vertebral bone defect at L3 (Figure 3A and D). Subsequent MR imaging revealed disc inflammation and osteomyelitis at L3 and L4 (Figure 3B and C). Due to the unclear diagnosis of bacterial infection, we initially let him continue to use anti-TB drugs (Isoniazid 300 mg qm, Rifampicin 450mg qm, Ethambutol 750mg qm, Pyrazinamide 500mg tid) until the TB-related tests confirmed negative. In addition, considering the possibility of his potential gastrointestinal bacterial infection, we empirically used levofloxacin (0.5 g qd) intravenously since admission. However, the patient’s condition gradually deteriorated while taking anti-TB drugs and levofloxacin, and the patient had a low-grade fever (Figure 4). In the following days, the results of TB-related and tumor marker-related test were confirmed to be negative and the patient stopped taking anti-TB drugs. In a series of preoperative cultures, no bacteria were found in his blood.
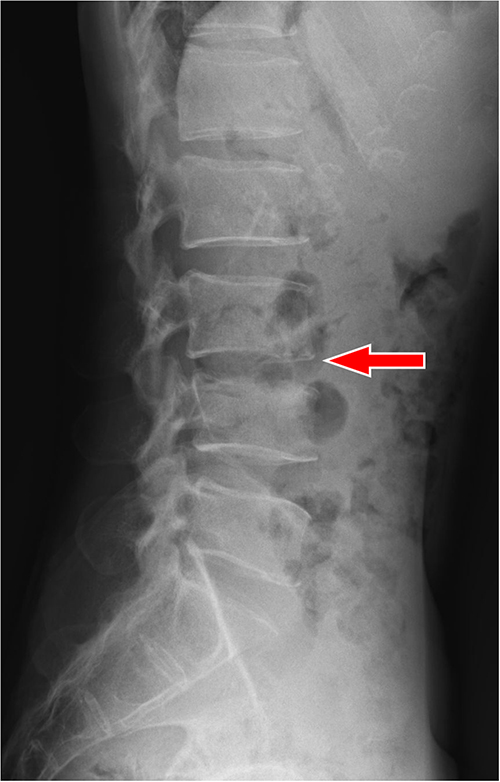 |
Figure 2 X-ray image of pre-operative. Notes: The red arrow points to the lesion site. Pre-operative X-ray image shows: the intervertebral space height between L3 and L4 is decreased. |
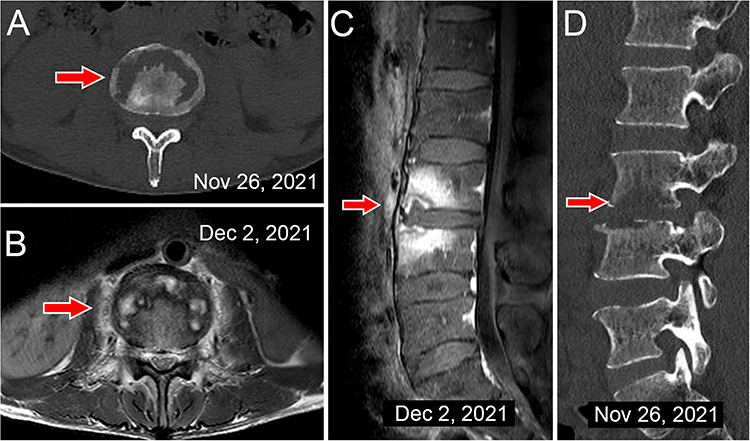 |
Figure 3 CT and MR images of lesion site. Notes: The red arrow points to the lesion site. (A) A CT image of L3 shows: severe bone destruction at the edge of the vertebral body. (B) An enhanced T1-weighted MR image shows: abnormal signals can be seen in the vertebral body and the soft tissue around the vertebral body. (C) An enhanced T1-weighted MR image shows: abnormal signals can be seen in the vertebral body of L3 and L4. (D) The 3-month follow-up CT image shows: bone grafting and internal fixation were stable and the intervertebral space height was restored. |
 |
Figure 4 Record of the patient’s armpit temperature during hospitalization and followed-up. Abbreviations: LF, levofloxacin; PSTS, Piperacillin Sodium and Tazobactam Sodium. |
On December 7th, 2021, considering the large vertebral bone defect and high-intensity activity required for his job could lead to spinal instability, an operation was performed (Supplementary surgical Technique and Supplementary Figure 2).9 After the operation, his abdominal symptoms disappeared and vital signs were stable. Then, his intraoperative samples were sent for pathological examination, culture and metagenomic next-generation sequencing (mNGS). Of all the intraoperative lesion samples submitted, only mNGS (Supplementary Figure 3) and anaerobic culture confirmed the presence of Eikenella corrodens. The procedure and quality control of mNGS records are in Supplementary Material Method. On the first postoperative day, his wound drainage fluid was re-cultured and no bacteria was found.
On December 11th, 2021, according to the mNGS and drug susceptibility results, we switched the patient’s levofloxacin to Piperacillin Sodium and Tazobactam Sodium (PSTS, 4.5g q8h). PSTS was administered intravenously until the patient was discharged on December 25th, 2021, during which time his infection-related indicators gradually improved (Figures 4 and 5). After discharge, the patient continued to take amoxicillin and clavulanate potassium tablets (457mg bid) orally for four weeks.
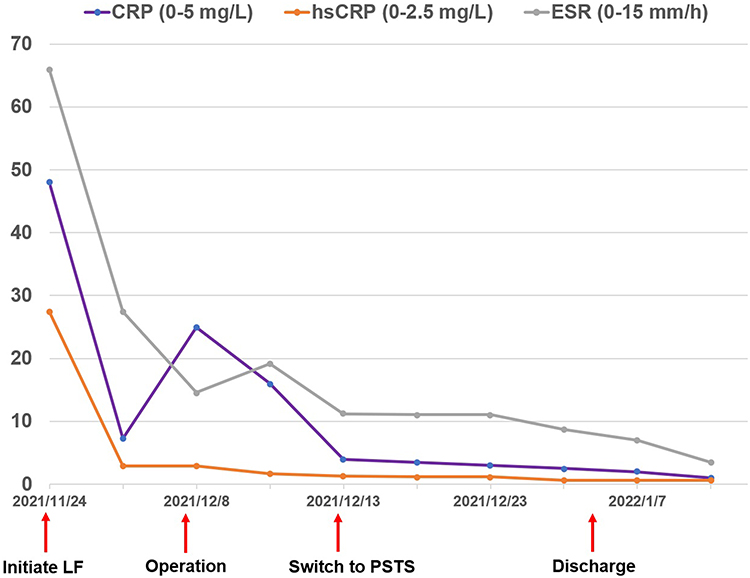 |
Figure 5 Record of the patient’s inflammatory indicators during hospitalization and followed-up. Abbreviations: CRP, C-reactive protein; hsCRP, high-sensitivity c-reactive protein; ESR, erythrocyte sedimentation rate; LF, levofloxacin; PSTS, Piperacillin Sodium and Tazobactam Sodium. |
On January 7th, 2022, the patient returned to our hospital for the first follow-up visit. His inflammatory indicators were normal and nutritional status had improved significantly (Figure 6). X-ray examination of lumbar showed that the lumbar spine (L3/4) had recovered well (Figure 7A and B). At this time, he could gradually extend his standing and walking time to about 2 hours and his lumbar spine JOA score was 22. Except for his wound pain, symptoms of lower abdominal pain, lumbar pain and other discomfort were relieved.
 |
Figure 6 Record of the patient’s albumin during hospitalization and followed-up. Abbreviations: LF, levofloxacin; PSTS, Piperacillin Sodium and Tazobactam Sodium. |
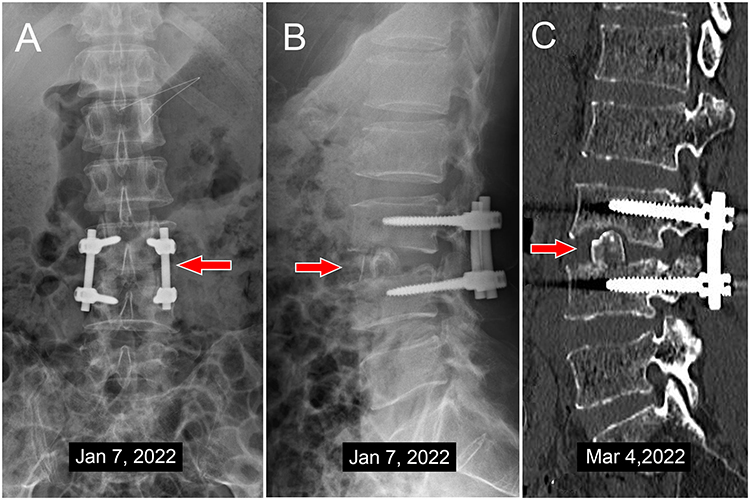 |
Figure 7 The follow-up X-ray and CT images. Notes: (A) Post-operative X-ray image shows: the internal fixation is in the correct position and keeps the spine stable. (B) Post-operative X-ray image shows: the bone graft is in place and restores the intervertebral space height. (C) The 3-month follow-up CT image shows: bone grafting and internal fixation were stable and the intervertebral space height was restored. |
On March 4th, 2022, the patient finished his second follow-up visit. Three months after the operation, the patient could go back to his work and live a completely normal life. Under the protection of the waist brace (Supplementary Figure 4B), the bone fusion and spinal stability were good (Figure 7C). His lumbar spine JOA score was 27 and all relevant test indicators had returned to normal (Figures 4–6).
On December 25th, 2022, the patient had completed a 12-month follow-up. During multiple telephone follow-up visits, the patient did not report any pain, fever or other discomfort.
Discussion
Identification of Abdominal Pain
The causes of abdominal pain are broad, clinicians usually first consider visceral disease in the abdomen. If all abdominal examinations reveal nothing, attention should be paid to potential spinal infections. Thus, checking the infection infiltration around the spine is important for patients with unexplained abdominal pain.
Abdominal MR, abdominal puncture, gastroscopy, and colonoscopy ruled out abdominal diseases, when the patient was admitted to Sun Yat-sen Memorial Hospital with abdominal pain as the main symptom. Only spinal infection was confirmed when he finished all examinations. Later, his abdominal pain recovered as soon as he underwent surgery. Thus, we guessed that the displaced pus from the lumbar vertebral lesions stimulated the retroperitoneal part of the descending colon causing left abdominal pain (Figure 8). For his abdominal tenderness, it was actually from the vicinity of the vertebral body. Firstly, his vertebral lesions were located in the anterior part of the vertebral body and the pus near the vertebral body irritated the soft tissue (Figure 3B). Secondly, he was thin (Supplementary Figure 4A) and the abdominal wall was concave close to the vertebral body in the supine position. Abdominal tenderness occurred when the lesions around the vertebral body were compressed.
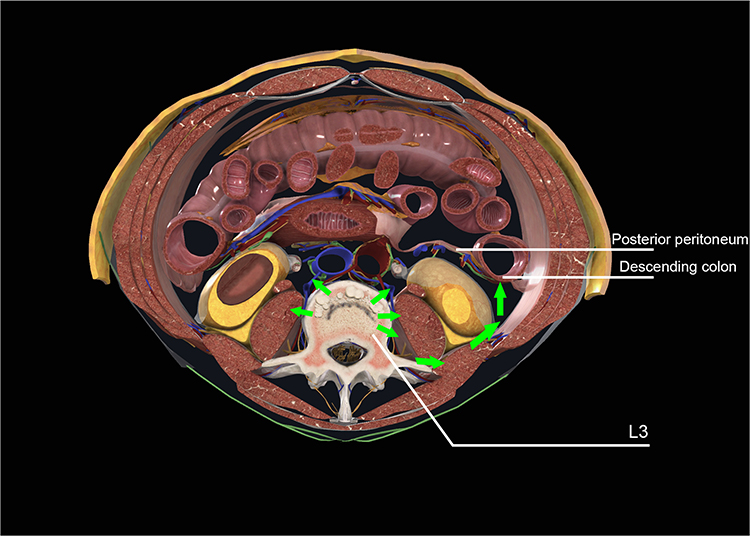 |
Figure 8 Cross-section of the lesion in the third lumbar vertebra. Notes: Green arrows indicate the direction of pus transfer; the green area indicates the extent of the pus invasion. |
Unusual Eikenella corrodens
Eikenella corrodens is a part of the inherent flora on the surface of human mucosa and it is a microaerophilic, slow-growing, nonmotile, gram-negative rod.3 Eikenella corrodens usually does not cause disease, but according to the literature, in the case of bites, trauma, surgery, etc., it may transfer through the bloodstream and cause infections.3,10 Infections caused by Eikenella corrodens are diverse, with documented cases of thigh abscess,11 lung abscess,4 purulent pericarditis,5 and osteomyelitis.12
Although LISI is relatively common, infections caused by Eikenella corrodens are rare. In previous cases of orthopaedic-related Eikenella corrodens infection, a particular risk of infection was identified in most patients, and the infection symptoms were absolutely different from TB. Fishbone stabbing caused a cervical spine infection,12 toothpick stabbing caused a foot infection,13 surgical pollution caused a knee joint infection,14 licking injury fingers caused a finger bone infection,8 dental infection caused a hip infection,15 and severe periodontitis (regularly chewing betel quid) caused a lumbar infection.16 However, some healthy individuals without potential risks also developed Eikenella corrodens infections (Table 1), and it was difficult to achieve a definite diagnosis at initial presentation. Therefore, the present patient had been misdiagnosed as lumbar TB at the local hospital due to the similar symptoms of TB, imaging findings and missed biopsy.
Diagnosis and Treatment
In the absence of clear potential risks, Eikenella corrodens is usually overlooked by doctors and aggravates the patient’s condition. Through the analysis of the existing orthopaedic-related literature (Table 1), the diagnostic efficiency of blood culture was low. Eikenella corrodens was an opportunistic pathogen with strict requirements on the growth environment, resulting in a low success rate of blood culture. According to the previous literature, when blood cultures were negative, lesions should be identified and biopsied for culture or mNGS.17
In the present case, the patient was initially treated with intravenous levofloxacin (0.5 g qd) for two weeks. Then, drug susceptibility test indicated that Eikenella corrodens was sensitive to β-lactams antibiotics. Thus, the patient received two weeks of intravenous PSTS (4.5g q8h) and four weeks of oral amoxicillin and clavulanate potassium tablets (457mg bid). Finally, a good clinical outcome was obtained. In our literature review (Table 2), improvements were seen in patients treated with β-lactams antibiotics, but not in patients treated with non-β-lactams antibiotics. Clinical outcomes of these cases were consistent with the present case. However, two patients were not cured after receiving sensitive antibiotic treatment. The reason for the failure of the first case18 was insufficient time for medication, and the second8 was that oral antibiotics did not reach the therapeutic concentration in the body (Table 2). In addition, it was particularly important to drain and clear the lesions after locating the lesions. For patients, lesion debridement combined with continuous β-lactams antibiotics for at least four weeks could reach the best clinical outcomes. In the present case, lesion debridement was performed and a total of six weeks of sensitive antibiotics was used. Compared with admission, the patient’s self-care ability and clinical symptoms were significantly improved at discharge.
Etiology Analysis
Reviewing these orthopaedic-related infection cases, only five cases11,19–22 had not found clear potential causative factors and 11 cases7,8,12–16,18,23–25 had revealed clear potential risks of patients. In the present case, the patient did not report any underlying diseases, fishbone stuck, invasive treatment, licking of wounds, and trauma. However, the patient reported that he occasionally ate betel nuts and had a tooth extraction in June 2021, all of which were possible potential risk factors. Besides, other potential risks should also be considered, such as oral conditions, toothpick stab wounds, skin damage caused by diabetes and fishbone stab wounds. These potential risks were responsible for serious Eikenella corrodens infections.
Conclusion
Although spinal infection is rarely presented as abdominal pain, checking the infection infiltration around the spine is important for patients with unexplained abdominal pain. Due to the low sensitivity of using blood culture as a diagnostic method for Eikenella corrodens, lesion sample culture or mNGS may better avoid misdiagnosis. In addition, when Eikenella corrodens was confirmed, lesion debridement combined with continuous β-lactams antibiotics for at least six weeks could achieve good clinical outcomes.
Data Sharing Statement
If necessary, data can be obtained from e-mail: [email protected].
Ethical Approval and Consent to Participate
All procedures were performed in compliance with relevant laws and institutional guidelines and that the medical ethics committee of Sun Yat-Sen Memorial Hospital of Sun Yat-sen University has approved them (SYSKY-2022-199-01). The patient agreed to participate.
Consent for Publication
The patient agreed to publication and we obtained written consent from him.
Acknowledgments
Thanks for the cooperation of the patient in the present case, and for the relevant academic guidance.26
Funding
Professor Li has received funding from Guangzhou Science and technology projects (Grant numbers [202102010259]).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Babic M, Simpfendorfer CS. Infections of the spine. Infect Dis Clin North Am. 2017;31(2):279–297. doi:10.1016/j.idc.2017.01.003
2. Schwab JH, Shah AA. Spinal epidural abscess: diagnosis, management, and outcomes. J Am Acad Orthop Surg. 2020;28(21):e929–e938. doi:10.5435/JAAOS-D-19-00685
3. Muhlhauser M. [Eikenella corrodens]. Rev Chilena Infectol. 2013;30(2):163–164. Spanish. doi:10.4067/S0716-10182013000200007
4. Hu L, Lin J, Li J, Cao Y, Lin L. Lung abscess secondary to lung cancer with Eikenella corrodens and Streptococcus anginosus: a case report. BMC Infect Dis. 2020;20(1):351. doi:10.1186/s12879-020-05054-y
5. Wei W, Nie H. Severe purulent pericarditis caused by invasive Eikenella corrodens: case report and literature review. BMC Infect Dis. 2019;19(1):657. doi:10.1186/s12879-019-4256-0
6. Dhaese S, De Wilde V, Snauwaert C, Orlent H. Eikenella corrodens perirenal abscess resulting from a pancreatic fistula in a patient with chronic pancreatitis. Case report and literature review. Acta Gastroenterol Belg. 2018;81(2):323–326.
7. Ranabhat K, Bhatta S, Bhatta RK, Acharya Y. Eikenella corrodens vertebral osteomyelitis in a young patient with type i diabetes mellitus. Cureus. 2020;12(8):e9553. doi:10.7759/cureus.9553
8. Cuenca-Estrella M, Ramos JM, Esteban J, Soriano F, Vallejo JV. Eikenella corrodens thumb osteomyelitis. Postgrad Med J. 1996;72(845):188. doi:10.1136/pgmj.72.845.188
9. Berbari EF, Kanj SS, Kowalski TJ, et al. 2015 Infectious Diseases Society of America (IDSA) clinical practice guidelines for the diagnosis and treatment of native vertebral osteomyelitis in adults. Clin Infect Dis. 2015;61(6):e26–e46. doi:10.1093/cid/civ482
10. Revest M, Egmann G, Cattoir V, Tattevin P. HACEK endocarditis: state-of-the-art. Expert Rev Anti Infect Ther. 2016;14(5):523–530. doi:10.1586/14787210.2016.1164032
11. Zhiyong Z, Xiufang L, Jiajie L. Thigh abscess caused by Eikenella corrodens and Streptococcus intermedius: a case report. J Infect. 2007;54(1):e17–e19. doi:10.1016/j.jinf.2006.03.021
12. Lehman CR, Deckey JE, Hu SS. Eikenella corrodens vertebral osteomyelitis secondary to direct inoculation: a case report. Spine. 2000;25(9):1185–1187. doi:10.1097/00007632-200005010-00022
13. Melton KS, DeRosa DC, Agee WA, Pires VL, Yim DG, Ngauy V. Mouth in foot disease. Hawaii J Med Public Health. 2015;74(9 Suppl 2):30–32.
14. Hurley RK, Maranich AM, Schmitz MR. Postoperative septic arthritis with Eikenella corrodens and Streptococcus mitis following arthroscopic anterior cruciate ligament reconstruction in an adolescent: a case report and review of the literature. Int J Pediatr Adolesc Med. 2016;3(4):184–186. doi:10.1016/j.ijpam.2016.08.007
15. Tricard T, Bund L, Alhefzi A, et al. Eikenella corrodens bone and Hip joint infection. A case report and literature review. Arch Pediatr. 2016;23(11):1146–1149. doi:10.1016/j.arcped.2016.08.011
16. Tsai J, Huang TJ, Huang CC, Li YY, Hsu RW. Eikenella corrodens discitis in a habitual betel quid chewer: a case report. Spine. 2009;34(9):E333–E336. doi:10.1097/BRS.0b013e31819b2283
17. Ranjbar R, Behzadi P, Najafi A, Roudi R. DNA microarray for rapid detection and identification of food and water borne bacteria: from dry to wet lab. Open Microbiol J. 2017;11:330–338. doi:10.2174/1874285801711010330
18. Yetimoglu C, Rafeiner P, Engel D, Fournier JY. Spinal infections due to Eikenella corrodens: case report and literature review. Neurochirurgie. 2014;60(4):197–200. doi:10.1016/j.neuchi.2014.03.002
19. Arana E, Vallcanera A, Santamaria JA, Sanguesa C, Cortina H. Eikenella corrodens skull infection: a case report with review of the literature. Surg Neurol. 1997;47(4):389–391. doi:10.1016/S0090-3019(96)00192-9
20. Sayana MK, Chacko AJ, Mc Givney RC. Unusual cause of infective discitis in an adolescent. Postgrad Med J. 2003;79(930):237–238. doi:10.1136/pmj.79.930.237
21. Zeifang F, Haag M, Lill CA, Sabo D. Eikenella-corrodens-induzierte Spondylitis Nachweis mittels 16s-RNA-Polymerasekettenreaktion [Eikenella corrodens-induced spondylitis. Detection with 16s-RNA polymerase chain reaction]. Orthopade. 2002;31(6):591–593. German. doi:10.1007/s001320100215
22. Farrington M, Eykyn SJ, Walker M, Warren RE. Vertebral osteomyelitis due to coccobacilli of the HB group. Br Med J. 1983;287(6406):1658–1660. doi:10.1136/bmj.287.6406.1658
23. Johnson SM, Pankey GA. Eikenella corrodens osteomyelitis, arthritis, and cellulitis of the hand. South Med J. 1976;69(5):535–539, 549. doi:10.1097/00007611-197605000-00018
24. Ang BS, Ngan CC. Eikenella corrodens discitis after spinal surgery: case report and literature review. J Infect. 2002;45(4):272–274. doi:10.1053/jinf.2002.1050
25. Patel K, Park C, Memon Z, Ilyas N. Eikenella Corrodens and Streptococcus anginosus co-infection causing skull base osteomyelitis and internal carotid artery lesion. IDCases. 2020;20:e00740. doi:10.1016/j.idcr.2020.e00740
26. Behzadi P, Gajdacs M. Writing a strong scientific paper in medicine and the biomedical sciences: a checklist and recommendations for early career researchers. Biol Futur. 2021;72(4):395–407. doi:10.1007/s42977-021-00095-z
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.