Back to Journals » Vascular Health and Risk Management » Volume 22
Low Toe-Brachial Indices are Associated with Saccular Intracranial Aneurysms
Authors Kangas E ![]() , Rantasalo V, Korpisalo P, Kuusela AM, Hakovirta E, Korhonen PE, Rahi M, Kivelev J, Rinne J, Venermo M, Hirvonen J, Hakovirta H
, Rantasalo V, Korpisalo P, Kuusela AM, Hakovirta E, Korhonen PE, Rahi M, Kivelev J, Rinne J, Venermo M, Hirvonen J, Hakovirta H ![]() , Laukka D
, Laukka D
Received 4 July 2025
Accepted for publication 6 January 2026
Published 8 February 2026 Volume 2026:22 547932
DOI https://doi.org/10.2147/VHRM.S547932
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Essi Kangas,1,2 Ville Rantasalo,1,2 Petra Korpisalo,3 Aino M Kuusela,4 Eelis Hakovirta,5 Päivi Elina Korhonen,1,6 Melissa Rahi,4,7 Juri Kivelev,4,7 Jaakko Rinne,4,7 Maarit Venermo,8 Jussi Hirvonen,9,10 Harri Hakovirta,1,2 Dan Laukka4,7
1Department of Surgery, University of Turku, Turku, Finland; 2Department of Vascular Surgery, Turku University Hospital, Turku, Finland; 3Heart Center, Kuopio University Hospital, Kuopio, Finland; 4Clinical Neurosciences, University of Turku, Turku, Finland; 5Department of Business and Administration, University of Vaasa, Vaasa, Finland; 6Department of General Practice, University of Turku, Turku, Finland; 7Department of Neurosurgery, Neurocenter, Turku University Hospital, Turku, Finland; 8Department of Vascular Surgery, University of Helsinki and Helsinki University Hospital, Helsinki, Finland; 9Department of Radiology, Turku University Hospital and University of Turku, Turku, Finland; 10Department of Radiology, University of Tampere, Tampere, Finland
Correspondence: Essi Kangas, Department of Vascular Surgery, Turku University Hospital, Hämeentie 10, Turku, 20520, Finland, Email [email protected]
Purpose: Peripheral artery disease (PAD) is a manifestation of systemic atherosclerosis. Non-invasive lower-limb pressure indices, such as the ankle-brachial index (ABI) and toe-brachial index (TBI), are widely used in the diagnostic evaluation of PAD and are strongly associated with atherosclerotic cardiovascular diseases. Intracranial aneurysms (IAs) share common risk factors with atherosclerotic cardiovascular diseases, particularly smoking and hypertension. In previous research, we found that a low ABI is associated with a higher prevalence of unruptured IAs. The objective of the present study is to examine whether low TBI is similarly associated with a prevalence if IAs.
Patients and Methods: This retrospective cohort study included patients (n=2751) who underwent a TBI assessment at a tertiary hospital between January 2011 and December 2013. The patients with available cerebrovascular imaging or a confirmed diagnosis of ruptured saccular IA (n = 776) were included into the study. The potential association between TBI and the prevalence of saccular IAs was the main outcome of interest.
Results: Patients were stratified according to their TBI values as follows: low TBI (< 0.5; n=473), borderline TBI (0.50– 0.69; n=180), and normal TBI (≥ 0.7; n=123).The prevalence of unruptured IAs was 16.3% in the low TBI group, 8.3% in the borderline TBI group, and 4.1% in the normal TBI category (p< 0.001). Sex- and age-adjusted multinomial regression including clinically relevant variables revealed that low TBI (odds ratio [OR], 3.59; 95% confidence interval [CI], 1.39– 9.27), female sex (OR, 1.68; 95% CI, 1.06– 2.673), and smoking history (OR, 2.56; 95% CI, 1.393– 4.695) were associated with the prevalence of unruptured IAs.
Conclusion: Low TBI was associated with a fourfold higher prevalence of unruptured IAs compared with normal TBI. In this retrospective cohort, the strongest association remained between low TBI and unruptured IAs after adjustment for established IA risk factors. These finding support a potential role of atherosclerosis in IA formation. Prospective studies are warranted to clarify the temporal relationship and to evaluate whether TBI could contribute to risk stratification in patients at risk of intracranial aneurysms.
Keywords: intracranial aneurysm, peripheral artery disease, risk factors, screening, toe-brachial index
Introduction
Peripheral artery disease (PAD) is an atherosclerotic condition associated with increased cardiovascular morbidity and mortality. Patients with PAD are likely to have generalized atherosclerosis; 46–68% of PAD patients have disease in one or more vascular beds.1 Ankle-Brachial Index (ABI) and Toe-Brachial Index (TBI) are widely used in the diagnosis of PAD. According to current guidelines, ABI <0.9 and TBI <0.7 are diagnostic of PAD.2,3 Similar to low ABI, a low TBI has been associated with an increased risk of cardiovascular and all-cause mortality.4,5 However, this association has been less extensively studied than that of ABI. In the presence of medial arterial calcification (MAC) the tibial arteries become incompressible leading to falsely elevated ABI measurements and may underestimate the prevalence of PAD.6,7 Small arteries in toes are less susceptible to MAC changes and making TBI a more sensitive method for diagnosing PAD in a presence of MAC.8,9 Furthermore, patients with normal ABI but low TBI have been demonstrated to exhibit similar cardiovascular comorbidities to those observed in patients with a low ABI.10
The global prevalence of unruptured intracranial aneurysms (IA) among individuals aged 50 years and over is 3%, while the global incidence of aneurysmal subarachnoid haemorrhage (SAH) is 6 per 100 000 person-years.11,12 A considerable proportion of IAs demonstrate stability over the course of an individual’s lifetime, however, a proportion of IAs demonstrate a tendency towards expansion and rupture, which can result in severe consequences.13 It is estimated that 25% of patients suffering from aneurysmatic SAH die before reaching the hospital or the emergency room.14 Furthermore, the 1-year mortality rate is 50%, which serves to illustrate the severity of this condition. It is estimated that one third of individuals who successfully complete the acute phase of recovery are unable to resume their usual daily activities.15
Smoking and hypertension are well established risk factors for both conditions PAD and IAs.15 Moreover, a plausible association has been observed between an increased atherosclerotic burden and the prevalence of IAs.16,17 However, there is a paucity of consensus regarding the association between coronary artery disease (CAD) and the increased prevalence of IAs.18,19 Furthermore, research has demonstrated that the prevalence of IA appears to be elevated among patients with carotid artery stenosis when compared to the general population.20
In a prior retrospective study, we established a notable an association between a low ABI and the prevalence of unruptured IAs.21 The objective of the present study is to investigate the association between TBI and the prevalence of IAs, thereby aiming to find a method to identify these patients and investigate the possible association between atherosclerotic diseases and the prevalence of IAs. To the authors’ knowledge, low TBI has not previously been reported to be associated with the prevalence of IAs.
Material and Methods
Study Cohort
Turku University Hospital, located in Southwest Finland, provides secondary care to 480,000inhabitants and functions as a tertiary referral center for 860 000 individuals. The Vascular Laboratory of The University of Turku performed peripheral pressure measurements on 2,757 patients between January 1, 2011, and 31 December 31, 2013, which constituted the initial research cohort comprising 2,757 patients. The date of the first peripheral pressure measurement was considered the index date for the study. Only the value of index measurement was considered in the analyses. The patients for whom cerebral artery imaging or data on previously treated ruptured IA were available from electronic patient records since 2003 were included in the study (766 patients). Patients for whom such data were not available were excluded. The study population was observed until January 1st, 2023. Imaging modalities included magnetic resonance angiography (MRA), computed tomography angiography (CTA), or digital subtraction angiography.21
The retrospective registry design of the present study was reviewed and approved in September 2017 by the Turku University Hospital Institutional Review Board (IRB) (IRB# T344/2017). According to the Finnish Act on the Secondary Use of Health and Social Data (552/2019), informed consent is not required for scientific research in the context of retrospective registry studies.
The data collection and review of electronic medical records was collected using the patient’s personal identity number. The dataset was fully pseudonymised prior to analysis, and no personally identifiable information was available to the research team during the analysis phase. All data used in this study were handled in accordance with applicable data protection and privacy regulations, including the EU General Data Protection Regulation (GDPR), and institutional data handling policies.
Baseline Measurement
Electronic medical records were retrospectively reviewed, and comorbidities were recorded by ICD codes: coronary artery disease (CAD) (I20.0 – I25.9), chronic heart failure (CHF) (I50.0 – I50. 9), hypertension (HTA) (I10.0 – I10.9), atrial fibrillation (AF) (I48.0 – I48.9), diabetes mellitus (DM) (E10.0 – E11.9), chronic obstructive pulmonary disease (COPD) (J44.8), hypercholesterolemia (HTC) (E78.0) and chronic kidney disease (CKD) (N18.1 – N18.9). Smoking data were also collected retrospectively. Previously identified IA risk factors, such as smoking, HTA, CKD, and CAD, which represent the burden of atherosclerotic diseases, were considered clinically significant variables.
All ankle and toe pressure measurements were conducted by vascular technicians in a standardized environment in the vascular laboratory of Turku University Hospital. Measurements were performed by using PeriFlux 6000 Laser Doppler system. Cuffs were placed bilaterally on the upper arms (brachial artery), ankles and toes to register the systolic pressures, and the TBI value was subsequently calculated by dividing the systolic pressure in the toe by the systolic pressure in the brachial artery. The report from the vascular laboratory included the absolute ankle and toe pressures of both legs, in addition to the ABI and TBI indices. The lower TBI value were included in the study.
All cerebrovascular imaging studies were reviewed to screen for intracranial aneurysms by a neurosurgeon. An experienced neuroradiologist evaluated each IA imaging finding to confirm the diagnosis. Any discrepancies that may have emerged in the assessments between the neurosurgeon and the neuroradiologist were resolved by consensus.
Aneurysms that were intracranial, saccular type, and at least 2 mm in size were considered IAs and included in the study.22,23 Internal carotid artery (ICA) aneurysms were classified as intradural or extradural according to the Bouthillier classification.24 Intradural aneurysms were located distal to the clinoid segment (C5), and extradural aneurysms in the intracavernous segment (C4) or on its proximal side. Extradural aneurysms were not included in the analysis. Intradural aneurysms were further classified according to anatomical location into four main groups: ICA and its two terminal branches, middle cerebral artery and anterior cerebral artery, and posterior circulation artery. IAs were further divided into subgroups to indicate more precise location.
Statistics
The primary outcome was the prevalence of IAs in the different TBI categories. We further analyzed separately the prevalence of ruptured and unruptured IAs.
All statistical analyses were conducted using SPSS version 27 (IBM, Armonk, NY, USA). Descriptive statistics were utilized to compare the demographics of the patients. For variables that followed a normal distribution, mean values and standard deviations (SD) were calculated. The normality of continuous variables was assessed using the Shapiro–Wilk test, while the homogeneity between the groups was evaluated with Levene’s test. The Fisher’s exact test was employed to compare categorical variables, while the Student’s t-test and ANOVA were used for comparing continuous variables that were normally distributed. The Kruskall-Wallis test was used to analyze non-normally distributed continuous variable.
The optimal threshold for predicting the occurrence of intracranial aneurysms (IA) was identified by determining the cutoff value for TBI using Youden’s J-index. The J-index was calculated from the ROC curve derived from a binary logistic regression model, where TBI was the predictor variable and the occurrence of IA was the outcome variable. The cutoff value for TBI was determined as the TBI value that corresponded to the highest J-index and maximised both sensitivity and specificity. The TBI value corresponding to the highest J-index value, which maximises both sensitivity and specificity, was 0.5. This value was utilised as the TBI cutoff value for low TBI group (<0.5). TBI 0.5–0.69 was employed to categorise patients into the borderline TBI group, where the value of 0.7 was suggested in the guidelines.2,3 TBI values of 0.7 and above were considered normal TBI. According to aneurysm findings, patients were classified into three groups: unruptured, ruptured and no intracranial aneurysm.
Regression analyses were performed first to detect statistically significant variables for IA utilizing univariate analysis. We then conducted two multinomial regression analyses to evaluate associations between the TBI and the IA groups; all analyses were age and sex adjusted. For the first analysis, statistically significant variables at univariate analyses were used, and in the second analysis, we used clinically significant variables.
Because this was a retrospective observational study including all eligible patients during the study period, no formal a priori sample size or power calculation was performed.
Results
Altogether 2751 patients with TBI were identified, of whom 776 had available brain MRA and/or CTA or a confirmed diagnosis of ruptured IA. Among these 473 (60.9%) had a low TBI (<0.5), 180 (23.2%) had a borderline TBI (0.5–0.69), and 123 (15.9%) had a normal TBI (≥ 0.7). The flow chart detailing the patient’s selection process is presented in Figure 1.
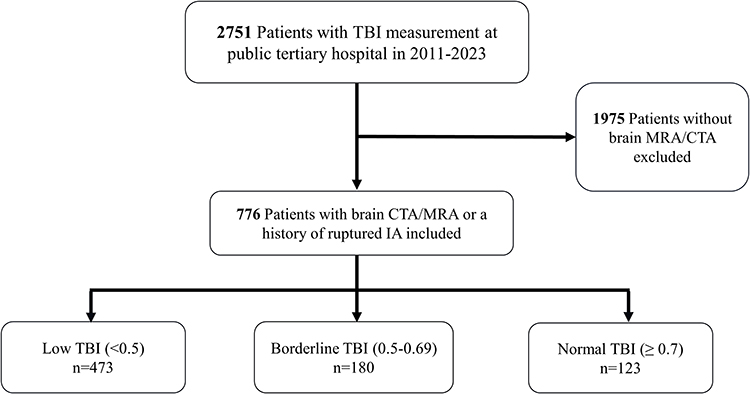 |
Figure 1 Flow chart of patient selection. Bold numbers indicate the number of patients at each step of inclusion and exclusion. |
A J-index of 0.5 was calculated for the ROC curve of binary regression for IA presence in a model with TBI as the only variable. The J-index of 0.5 had the best predictive value for IA presence. Based on Youdens index, 0.5 was therefore set as a cut-off value for categorization to low TBI cohort.
Demographic characteristics stratified by TBI category for the study cohort are presented in Table 1. Significant differences were observed across TBI categories in age, hypertension, type II diabetes, CAD and smoking history. The prevalence of unruptured IAs differed across TBI categories as shown in Figure 2: 16.3% in the low TBI (< 0.5) category, 8.3% in the borderline TBI (0.5–0.69) category, and 4.1% in the normal TBI (≥ 0.7) category (p < 0.001). Within the low TBI (< 0.5) category, 1.5% had ruptured IAs; in the borderline TBI (0.5–0.69) category, 1.1% exhibited ruptured IAs; and in the normal TBI (≥ 0.7) category, 3.3% showed ruptured IAs (p = 0.307).
 |
Table 1 Comparison of Baseline Characteristics According to TBI Category. Patients with Both Ruptured IA and Unruptured IA Were Categorized as Ruptured IA |
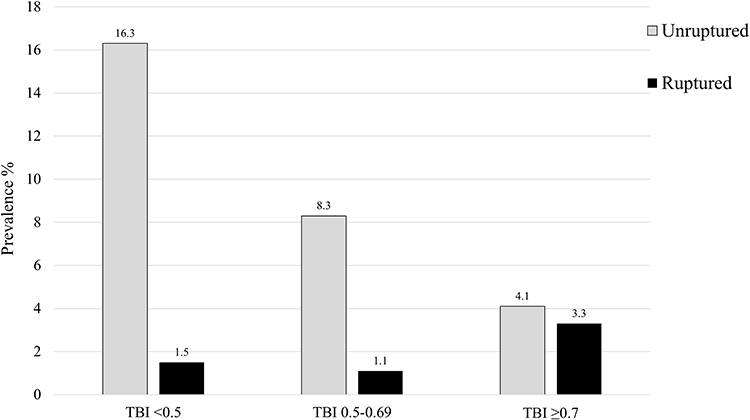 |
Figure 2 Presents the prevalence of unruptured and ruptured IAs by TBI categories. |
Table 2 presents a summary of the main baseline demographic characteristics of the patient cohort, classified according to IA presentation. The mean TBI was 0.36 (SD ± 0.180) in patients with unruptured IAs, 0.49 (SD ± 0.269) in patients with ruptured IAs, and 0.46 (SD ± 0.241) in patients without IAs (p<0.001).
 |
Table 2 Baseline Characteristics of Unruptured and Ruptured Intracranial Aneurysms and Patients Without IAs |
After adjusting for age, sex, and clinically relevant variables as outlined in Table 3 (Model 1), the multinomial regression analysis revealed a statistically significant correlation between low TBI (<0.5) and unruptured IAs. (odds ratio [OR], 3.75; 95% confidence interval [CI], 1.448–9.708; p=0.006). Furthermore, female sex (OR, 1.63; 95% CI, 1.03–2.60) and smoking history (OR, 2.59; 95% CI, 1.41–4.76; p=0.002) exhibited significant associations with unruptured IAs. The second multinomial regression analysis was conducted, including the statistically significant variables identified in the univariate analysis and adjusted for age and sex (Table 3, Model 2). The results were found to be consistent with those of the previous analysis.
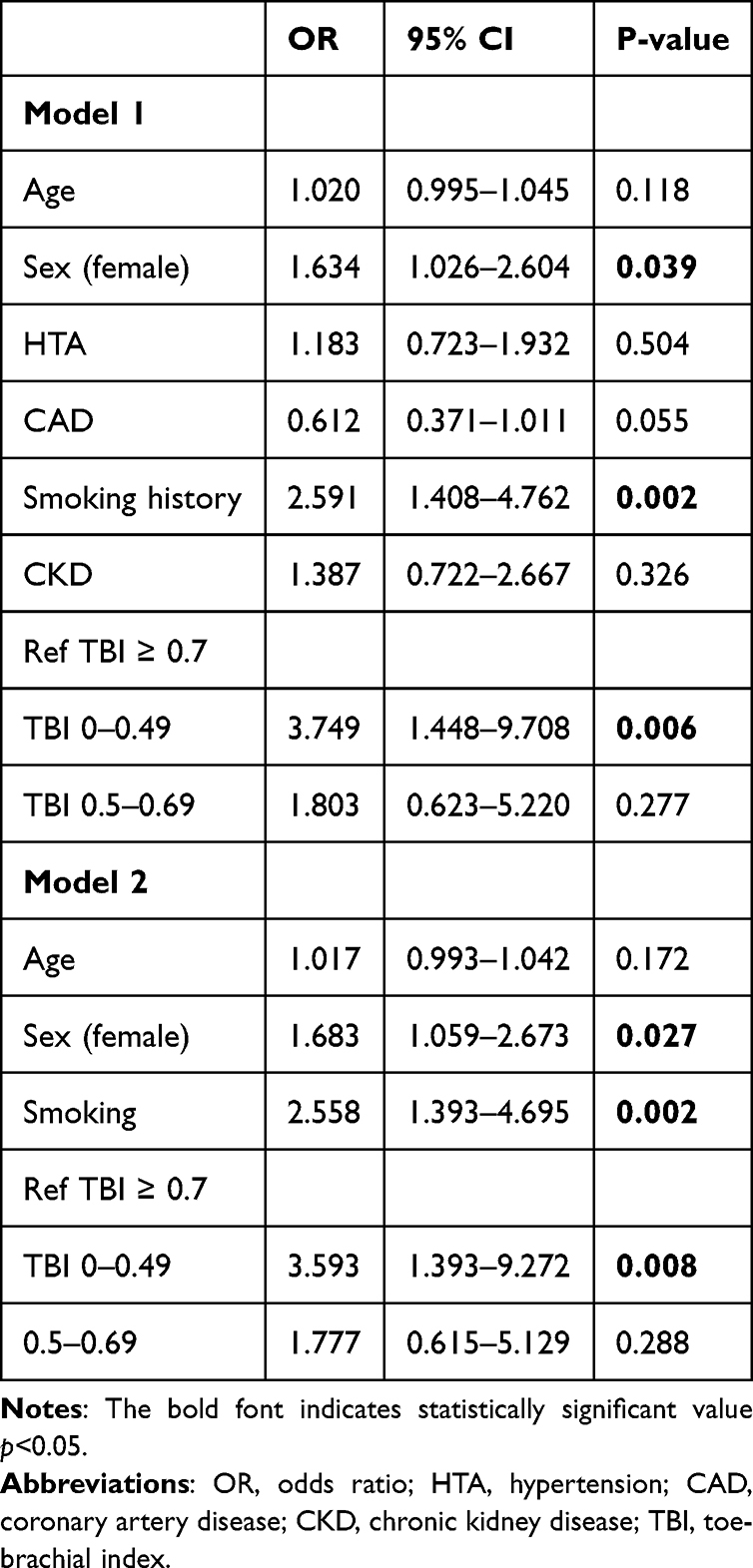 |
Table 3 Multinomial Regression Models for Unruptured Intracranial Aneurysms Adjusted for Sex- and Age. Model 1 Included Clinically Significant Variables. Model 2 Included Variables That Were Statistically Significant in the Univariate Analysis |
Discussion
Present data suggest a strong association between low TBI (< 0.5) and the prevalence of unruptured IAs. Our results show a 4-fold prevalence of unruptured IAs in the low TBI groups (< 0.5) compared to those with normal TBI (≥ 0.7). The prevalence of unruptured IAs in the low TBI category (< 0.5) was 16.3%, and the corresponding value in the normal TBI category (≥ 0.7) was 4.1%. In addition, the borderline TBI category (0.5–0.69) had a higher prevalence of unruptured IAs compared to the normal TBI category, although the difference was not statistically significant. The prevalence of unruptured IAs in this borderline TBI category (0.5–0.69) was 8.3%. The prevalence of unruptured IAs in the normal TBI category (4.1%) was marginally higher than that reported in the general population.12 To the best of our current knowledge, this is the first study to investigate the potential correlation between TBI and intracranial aneurysms.
In the present study, female sex was associated with an increased risk for unruptured IAs, which aligns with prior research that show a 1.5–2-fold prevalence of unruptured IA in females than in males.12,25,26 Both smoking and hypertension are recognized and established risk factors for IA and PAD.15,27,28 Notably, our multinomial regression analysis revealed that smoking history emerged as a significant independent risk factor for unruptured IAs alongside low TBI and female sex categories. However, the association of smoking history and female sex in relation to IAs appeared to be relatively weaker when compared to the influence of low TBI. It may be hypothesized that an alternative mechanism is responsible for the relationship between IA and low TBI, possibly through a common vascular pathophysiology.29 Interestingly, hypertension did not emerge as a significant risk factor for IA. This may be attributable to the high prevalence of cardiovascular disease within the study cohort, which may diminish the statistical significance of the independent effect of hypertension.
The TBI has been demonstrated to be associated with an increased cardiovascular risk and is therefore linked to an increased atherosclerotic burden.4,5 The findings of this study indicate that patients with a higher atherosclerotic burden also exhibited a higher prevalence of IAs. The pathophysiological link between atherosclerosis and IA is not yet established, however, according to histological studies, there are often present lipid accumulation and calcification in IA wall.29,30 Notably, these both conditions exhibit common pathophysiological mechanisms involving hemodynamic stress, endothelial dysfunction and chronic inflammation to promote arterial wall degeneration and augment the risk of IA formation and atherosclerosis.31,32 It has been hypnotized that atherosclerosis may result in the weakening of blood vessel walls and the predisposition of individuals to IA development.33
The significance of TBI in the detection of PAD and, consequently, generalized atherosclerosis has become increasingly apparent. In certain conditions ABI measurements may be misleadingly elevated and TBI has been demonstrated to have superior sensitivity compared to ABI for diagnosing PAD.34–36 Moreover, TBI encompasses a more comprehensive range of PAD phenotypes than ABI, thereby enhancing its utility in clinical practice.37 In our prior publication, we observed that the prevalence of unruptured IA was up to 9-fold for the low ABI group compared to the normal ABI group.21 The present study demonstrates a similar, albeit less pronounced results across the TBI categories. A vascular profile characterized by a normal ABI but reduced TBI may indicate isolated distal small artery disease (SAD), in which occlusive lesions are limited to pedal arteries distal to malleoli. Low TBI values are likewise associated with MAC when affecting the pedal arteries.38 MAC occurs independently of atherosclerosis and do not necessary have direct arterial obstructive effect, but it has been noted to have hemodynamic irruptions leading to decreased perfusion.39 Moreover, MAC can artefactually elevate ABI measurements in conditions where the calcified tibial arteries become non-compressible. Ageing, chronic kidney disease and diabetes are primary risk factors for MAC, whereas diabetes and chronic kidney disease have also been associated with SAD.38,40,41 However, these risk factors have not been shown to be associated with an increased risk for IAs.12 Although atherosclerotic PAD of great arteries, SAD and MAC may present with similar clinical manifestations, their underlying pathophysiological mechanisms and associated risk factors differ.40,42 In contradistinction to atherosclerotic PAD, SAD and MAC do not demonstrate atherosclerotic changes, such as lipid deposits. SAD is characterized by endothelial dysfunction and arterial wall remodeling, while MAC is typified by the calcification of the arterial media without luminal narrowing.40,43 PAD affecting large arteries reflects the classical atherosclerotic pathway and risk factor profile, and it shares similar risk factors associated with IAs.44 In the present study, the population in the low and borderline TBI group were significantly older and had a more often diabetes compared to normal TBI cohort. Decreased TBI values are indicative of more distally manifested PAD, and the risk factors associated with distal PAD differ from those linked to IA formation. This distinction may provide a valuable insight into the observed differences in the prevalence of unruptured IAs across the categories of TBIs and ABIs.
Screening recommendations for IAs are aimed at high-risk populations, including patients with connective tissue disorders, autosomal dominant polycystic kidney disease, or those with one or more first-degree relatives with IAs.43 The prevalence of IAs in these targeted populations ranges from 10% to 19%.43 The present study demonstrates that the prevalence of IA in the low TBI category (< 0.5) aligns closely with the prevalence in groups recommended for IA screening. This suggests that TBI measurements could serve as an additional screening tool for identifying individuals at an elevated risk of IA. Developing an IA risk prediction model would aid physicians in comprehensive risk assessment, with TBI measurement offering a potential complementary aspect to other risk factors. The simplicity, cost-effectiveness, and widespread availability of TBI measurements make them a feasible candidate for integration into an IA risk assessment model.
Despite the unclear precise mechanism linking low TBI to the prevalence of IAs, the findings of these studies suggest that the risk factor profile of IA patients is broader than previously recognized. The present study demonstrates a significant correlation between diminished pressure measurements and the prevalence of IA, thus suggesting that cardiovascular risk factors may potentially exert a more substantial influence on the development of IA than previously hypothesized. These findings support the necessity for a more extensive approach to IA risk assessment, incorporating markers of systemic atherosclerosis in addition to traditional IA risk factors.
Limitations
The present study has limitations, including the retrospective nature of data collection, which may lead to selection bias. The study population underwent non-invasive pressure measurements due to the presence of lower limb symptoms. Consequently, patients with PAD are over-represented in this cohort, which also explains the high proportion of smokers. Of the original cohort of 2,757 patients, only 28% underwent cerebrovascular imaging or had ruptured IA and were therefore included in this study. The reasons for performing imaging varied, which could introduce selection bias. Additionally, despite the fact that each TBI group contained a sufficient number of patients for statistical analysis, it should be noted that unequal sample sizes may have a detrimental effect on statistical power, particularly in the smallest group. Additionally, the high prevalence of IAs in patients with low TBI suggests that selection bias alone may not account for these findings. However, the sample size is too small to definitively determine whether differences exist between TBI groups regarding ruptured IAs. In this study, imaging was performed for neurological symptoms or suspected symptoms, with only five patients undergoing imaging for IA screening. Thus, our findings do not determine the utility of the TBI in patients with IA screening indications. These patients should continue to follow current guidelines, regardless of normal TBI results. A prospective study is needed to evaluate whether TBI can be used for IA screening.
Patients in the cohort of this study reported experiencing lower limb symptoms. A significant proportion of these symptoms are likely due to PAD or to spinal etiologies. PAD is thus probably over-represented in this cohort. Therefore, patients in this cohort are likely to have more atherosclerotic changes than the general population.
Although the study data were collected retrospectively, we were able to obtain data on smoking history from 94% of the patients. Missing data on smoking history were similarly distributed across the TBI groups. Due to the retrospective nature of this study, more comprehensive information on smoking status, such as pack years, may be impossible to obtain from electronic health records. The data on alcohol consumption was not available in the medical records and therefore could not be included as a variable.
Conclusion
Based on the present observational study, the prevalence of IAs was 16.8% in the low TBI category, which represents a 4-fold increase compared to the normal TBI. This finding underscores the potentially heightened accumulation of cardiovascular risk factors in IA patients and underscores the possible association between atherosclerosis and the development of IAs. However, no causal conclusions can be drawn from our results; prospective research is needed in this regard. These findings emphasise the potential value of TBI as a marker for identifying individuals at an elevated risk of unruptured IAs and thus offering valuable insights for further prospective research.
Data Sharing Statement
Data cannot be shared publicly because of patient identification. Data access requests may be submitted to Turku Clinical Research Centre (Turku CRC). If the access is granted, the data will be provided from the Turku CRC ([email protected]).
Ethics Approval and Informed Consent
This retrospective study was reviewed and approved by the Turku University Hospital Institutional Review Board (IRB# T344/2017). Informed consent was not required due to the retrospective design of the study. All procedures were conducted in accordance with relevant guidelines and regulations, including the Declaration of Helsinki.
Acknowledgments
We thank Auria Clinical Informatics for assisting in data collection. We thank Tiia Rissanen for evaluating the statistical analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Preset study was funded by Federal Grant Satasairaala and Finnish Culture Foundation Satakunta fund, grant numbers: 75212239 and 75221501.
Disclosure
The authors report no financial or non-financial conflicts of interest in this work.
References
1. Bhatt DL, Steg PG, Ohman EM. et al. International prevalence, recognition, and treatment of cardiovascular risk factors in outpatients with atherothrombosis. JAMA. 2006;295(2):180–11. doi:10.1001/jama.295.2.180
2. Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). J Vasc Surg. 2007;45(Suppl S):S5–67. doi:10.1016/j.jvs.2006.12.037
3. Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation. 2006;113(11):e463–654. doi:10.1161/circulationaha.106.174526
4. Wickström JE, Laivuori M, Aro E, et al. Toe Pressure and Toe Brachial Index are Predictive of Cardiovascular Mortality, Overall Mortality, and Amputation Free Survival in Patients with Peripheral Artery Disease. Eur J Vasc Endovasc Surg. 2017;53(5):696–703. doi:10.1016/j.ejvs.2017.02.012
5. Hyun S, Forbang NI, Allison MA, Denenberg JO, Criqui MH, Ix JH. Ankle-brachial index, toe-brachial index, and cardiovascular mortality in persons with and without diabetes mellitus. J Vasc Surg. 2014;60(2):390–395. doi:10.1016/j.jvs.2014.02.008
6. Suominen V, Uurto I, Saarinen J, Venermo M, Salenius J. PAD as a risk factor for mortality among patients with elevated ABI--a clinical study. Eur J Vasc Endovasc Surg. 2010;39(3):316–322. doi:10.1016/j.ejvs.2009.12.003
7. Emanuele MA, Buchanan BJ, Abraira C. Elevated leg systolic pressures and arterial calcification in diabetic occlusive vascular disease. Diabetes Care. 1981;4(2):289–292. doi:10.2337/diacare.4.2.289
8. Leskinen Y, Salenius JP, Lehtimäki T, Huhtala H, Saha H. The prevalence of peripheral arterial disease and medial arterial calcification in patients with chronic renal failure: requirements for diagnostics. Am J Kidney Dis. 2002;40(3):472–479. doi:10.1053/ajkd.2002.34885
9. Young MJ, Adams JE, Anderson GF, Boulton AJ, Cavanagh PR. Medial arterial calcification in the feet of diabetic patients and matched non-diabetic control subjects. Diabetologia. 1993;36(7):615–621. doi:10.1007/bf00404070
10. Høyer C, Høgh AL, Sandermann J, Zacho HD, Petersen LJ. Risk factors and haemodynamic variables in patients with low toe-brachial index but normal ankle-brachial index. Atherosclerosis. 2019;289:21–26. doi:10.1016/j.atherosclerosis.2019.08.005
11. Etminan N, Chang HS, Hackenberg K, et al. Worldwide Incidence of Aneurysmal Subarachnoid Hemorrhage According to Region, Time Period, Blood Pressure, and Smoking Prevalence in the Population: a Systematic Review and Meta-analysis. JAMA Neurol. 2019;76(5):588–597. doi:10.1001/jamaneurol.2019.0006
12. Vlak MH, Algra A, Brandenburg R, Rinkel GJ. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: a systematic review and meta-analysis. Lancet Neurol. 2011;10(7):626–636. doi:10.1016/S1474-4422(11)70109-0
13. Etminan N, Rinkel GJ. Unruptured intracranial aneurysms: development, rupture and preventive management. Nat Rev Neurol. 2016;12(12):699–713. doi:10.1038/nrneurol.2016.150
14. Korja M, Lehto H, Juvela S, Kaprio J. Incidence of subarachnoid hemorrhage is decreasing together with decreasing smoking rates. Neurology. 2016;87(11):1118–1123. doi:10.1212/wnl.0000000000003091
15. Karhunen V, Bakker MK, Ruigrok YM, Gill D, Larsson SC. Modifiable Risk Factors for Intracranial Aneurysm and Aneurysmal Subarachnoid Hemorrhage: a Mendelian Randomization Study. J Am Heart Assoc. 2021;10(22):e022277. doi:10.1161/jaha.121.022277
16. Cho BH, Kim JH, Suh SH, et al. Characteristics of Intracranial Aneurysms According to Levels of Coronary Artery Calcium. Stroke. 2019;50(6):1403–1408. doi:10.1161/strokeaha.119.024726
17. Rantasalo V, Gunn J, Kiviniemi T, et al. Intracranial aneurysm is predicted by abdominal aortic calcification index: a retrospective case-control study. Atherosclerosis. 2021;334:30–38. doi:10.1016/j.atherosclerosis.2021.08.027
18. Kang HG, Kim BJ, Lee J, et al. Risk Factors Associated With the Presence of Unruptured Intracranial Aneurysms. Stroke. 2015;46(11):3093–3098. doi:10.1161/strokeaha.115.011351
19. Uehara T, Tabuchi M, Mori E. High frequency of unruptured intracranial aneurysms in female patients with ischaemic heart disease. J Neurol Neurosurg Psychiatry. 1998;64(4):536–538. doi:10.1136/jnnp.64.4.536
20. Yang X, Lu J, Wang J, et al. A clinical study and meta-analysis of carotid stenosis with coexistent intracranial aneurysms. J Clin Neurosci. 2018;52:41–49. doi:10.1016/j.jocn.2018.02.021
21. Laukka D, Kangas E, Kuusela A, et al. Low and Borderline Ankle-Brachial Index Is Associated With Intracranial Aneurysms: a Retrospective Cohort Study. Neurosurgery. 2024. doi:10.1227/neu.0000000000002837
22. Johnsen LH, Herder M, Vangberg T, et al. Prevalence of unruptured intracranial aneurysms: impact of different definitions - the Tromsø Study. J Neurol Neurosurg Psychiatry. 2022;93(8):902–907. doi:10.1136/jnnp-2022-329270
23. Li MH, Chen SW, Li YD, et al. Prevalence of unruptured cerebral aneurysms in Chinese adults aged 35 to 75 years: a cross-sectional study. Ann Intern Med. 2013;159(8):514–521. doi:10.7326/0003-4819-159-8-201310150-00004
24. Bouthillier A, van Loveren HR, Keller JT. Segments of the internal carotid artery: a new classification. Neurosurgery. 1996;38(3):425–432. doi:10.1097/00006123-199603000-00001
25. Cras TY, Bos D, Ikram MA, et al. Determinants of the Presence and Size of Intracranial Aneurysms in the General Population: the Rotterdam Study. Stroke. 2020;51(7):2103–2110. doi:10.1161/strokeaha.120.029296
26. Laukka D, Kivelev J, Rahi M, et al. Detection Rates and Trends of Asymptomatic Unruptured Intracranial Aneurysms From 2005 to 2019. Neurosurgery. 2024;94(2):297–306. doi:10.1227/neu.0000000000002664
27. Sun X, Liu B, Chen Y, Lv L, Ye D, Mao Y. Modifiable risk factors for intracranial aneurysms: evidence from genetic studies. Int J Stroke. 2022;17(10):1107–1113. doi:10.1177/17474930211065640
28. Conte MS, Bradbury AW, Kolh P, et al. Global vascular guidelines on the management of chronic limb-threatening ischemia. J Vasc Surg. 2019;69(6s):3S–125S. doi:10.1016/j.jvs.2019.02.016
29. Frösen J, Tulamo R, Paetau A, et al. Saccular intracranial aneurysm: pathology and mechanisms. Acta Neuropathol. 2012;123(6):773–786. doi:10.1007/s00401-011-0939-3
30. Gade PS, Tulamo R, Lee KW, et al. Calcification in Human Intracranial Aneurysms Is Highly Prevalent and Displays Both Atherosclerotic and Nonatherosclerotic Types. Arterioscler Thromb Vasc Biol. 2019;39(10):2157–2167. doi:10.1161/atvbaha.119.312922
31. Signorelli F, Sela S, Gesualdo L, et al. Hemodynamic Stress, Inflammation, and Intracranial Aneurysm Development and Rupture: a Systematic Review. World Neurosurg. 2018;115:234–244. doi:10.1016/j.wneu.2018.04.143
32. Libby P. The changing landscape of atherosclerosis. Nature. 2021;592(7855):524–533. doi:10.1038/s41586-021-03392-8
33. Pan T, Shi Y, Yu G, Mamtimin A, Zhu W. Intracranial Aneurysms and Lipid Metabolism Disorders: from Molecular Mechanisms to Clinical Implications. Biomolecules. 2023;13(11):1652. doi:10.3390/biom13111652
34. Herraiz-Adillo Á, Cavero-Redondo I, Álvarez-bueno C, Pozuelo-Carrascosa DP, Solera-Martínez M. The accuracy of toe brachial index and ankle brachial index in the diagnosis of lower limb peripheral arterial disease: a systematic review and meta-analysis. Atherosclerosis. 2020;315:81–92. doi:10.1016/j.atherosclerosis.2020.09.026
35. Tehan PE, Santos D, Chuter VH. A systematic review of the sensitivity and specificity of the toe–brachial index for detecting peripheral artery disease. Vascular Medicine. 2016;21(4):382–389. doi:10.1177/1358863x16645854
36. Dachun X, Jue L, Liling Z, et al. Sensitivity and specificity of the ankle--brachial index to diagnose peripheral artery disease: a structured review. Vasc Med. 2010;15(5):361–369. doi:10.1177/1358863x10378376
37. Martelli E, Enea I, Zamboni M, et al. Focus on the Most Common Paucisymptomatic Vasculopathic Population, from Diagnosis to Secondary Prevention of Complications. Diagnostics. 2023;13(14):2356. doi:10.3390/diagnostics13142356
38. Sundaram S, Barksdale C, Rodriguez S, Wooster MD. The Impact of Small Artery Disease (SAD) and Medial Arterial Calcification (MAC) Scores on Chronic Wound and Amputation Healing: can It Tell Us More? Ann Vasc Surg. 2025;110(Pt B):260–275. doi:10.1016/j.avsg.2024.07.089
39. Lanzer P, Boehm M, Sorribas V, et al. Medial vascular calcification revisited: review and perspectives. Eur Heart J. 2014;35(23):1515–1525. doi:10.1093/eurheartj/ehu163
40. Ferraresi R, Ucci A, Pizzuto A, et al. A Novel Scoring System for Small Artery Disease and Medial Arterial Calcification Is Strongly Associated With Major Adverse Limb Events in Patients With Chronic Limb-Threatening Ischemia. J Endovasc Ther. 2021;28(2):194–207. doi:10.1177/1526602820966309
41. Lanzer P, Ferraresi R. Medial Sclerosis-Epidemiology and Clinical Significance. Dtsch Arztebl Int. 2023;120(21):365–372. doi:10.3238/arztebl.m2023.0066
42. Ho CY, Shanahan CM. Medial Arterial Calcification: an Overlooked Player in Peripheral Arterial Disease. Arterioscler Thromb Vasc Biol. 2016;36(8):1475–1482. doi:10.1161/atvbaha.116.306717
43. Lanzer P, Hannan FM, Lanzer JD, et al. Medial Arterial Calcification: JACC State-of-the-Art Review. J Am Coll Cardiol. 2021;78(11):1145–1165. doi:10.1016/j.jacc.2021.06.049
44. Diehm N, Shang A, Silvestro A, et al. Association of Cardiovascular Risk Factors with Pattern of Lower Limb Atherosclerosis in 2659 Patients Undergoing Angioplasty. Eur J Vasc Endovascular Surg. 2006;31(1):59–63. doi:10.1016/j.ejvs.2005.09.006
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Screening for Abdominal Aortic Aneurysm in Elderly Male Patients with Coronary Artery Disease During Standard Transthoracic Echocardiography
Lei Y, Zhang L, Wang M, Wang L, Su J, Zhou M, Wang X, Qi X, Xue Y
International Journal of General Medicine 2026, 19:616767
Published Date: 25 June 2026