Back to Journals » Nature and Science of Sleep » Volume 18

Loop Gain in Obstructive Sleep Apnea: From Physiological Endotype to Clinical Translation
Authors Li C ![]() , Wang C, Zhang Y, Ye J, Guo B, Wu M, Zhang C
, Wang C, Zhang Y, Ye J, Guo B, Wu M, Zhang C ![]() , Huang S
, Huang S ![]() , Yue G
, Yue G ![]()
Received 24 April 2026
Accepted for publication 18 June 2026
Published 9 July 2026 Volume 2026:18 616733
DOI https://doi.org/10.2147/NSS.S616733
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Chaofan Li,1,2,* Chaohua Wang,1,2,* Ying Zhang,1 Juan Ye,1 Bin Guo,1 Min Wu,1 Chun Zhang,1,2 Shaokun Huang,1,2 Guanghao Yue1
1Department of Otorhinolaryngology, Affiliated Hospital of Qinghai University, Xining, Qinghai, 810000, People’s Republic of China; 2Qinghai University School of Medicine, Xining, Qinghai, 810000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guanghao Yue, Department of Otorhinolaryngology, Affiliated Hospital of Qinghai University, Xining, Qinghai, 810000, People’s Republic of China, Email [email protected]
Objective: To define how loop gain can move from a physiological endotype to a clinically actionable metric in obstructive sleep apnea.
Methods: This clinical translational narrative review identified relevant literature from PubMed, Web of Science, Embase, and reference/citation searching, focusing on adult obstructive sleep apnea studies related to loop gain physiology, assessment methods, treatment stratification, and clinical implementation.
Results: Loop gain helps explain why patients with similar apnea-hypopnea index values may show different disease expression and treatment responses. Research-grade perturbation methods remain the physiological reference standard, whereas raw-polysomnography (PSG) modeling currently represents the most practical route for clinical deployment. Simplified screening tools and emerging automated approaches based on polygraphy, photoplethysmography, or respiratory inductance plethysmography may expand access, provided their outputs are interpreted within method-specific contexts. Clinically, elevated loop gain may inform pre-treatment restratification before surgery or oral appliance therapy, selection of oxygen or ventilatory-control-targeted pharmacotherapy, and interpretation of residual instability during continuous positive airway pressure.
Conclusion: Loop gain is most useful as a selective decision-support metric rather than as an isolated physiological number. Staged implementation, method-specific reporting, and outcome-oriented studies are needed to determine when LG-guided stratification improves clinical decisions in obstructive sleep apnea.
Keywords: obstructive sleep apnea, loop gain, polysomnography, endotyping, ventilatory control, precision medicine
Introduction
Although the apnea-hypopnea index (AHI) remains the foundation for diagnosing and grading obstructive sleep apnea (OSA) severity, it does not adequately explain the substantial pathophysiological heterogeneity among patients. Patients with the same AHI may have very different degrees of upper-airway collapsibility, ventilatory control stability, arousal threshold, and treatment responsiveness.1–3 Accordingly, sleep medicine is increasingly moving from simple event counting toward endotyping, with the aim of explaining why disease develops, why it persists, and why the same treatment can produce divergent responses.
Loop gain (LG) occupies a central position in this transition because it describes how strongly ventilatory control amplifies a disturbance. When chemical feedback is excessive, post-obstructive ventilatory overshoot may lower arterial carbon dioxide tension (PaCO2) below the apnea threshold, sustaining recurrent obstruction, overshoot, and renewed instability.2,4 However, LG is only one component of a multifactorial endotype network that also includes pharyngeal collapsibility, arousal threshold, and upper-airway muscle responsiveness.5,6 Arousal threshold determines the level of ventilatory drive that can accumulate before awakening, whereas upper-airway muscle responsiveness determines whether rising drive can be converted into effective airway reopening.5–7 Sleep stage further modifies this interaction through mechanisms that extend beyond the simple distribution of respiratory events. During non-rapid eye movement (NREM) sleep, relatively preserved chemoreflex responsiveness and arousal-dependent recovery drive may allow chemical feedback to amplify post-event ventilatory overshoot and promote ventilatory cycling. During rapid eye movement (REM) sleep, by contrast, state-dependent suppression of upper-airway dilator muscle activity, altered autonomic and chemoreflex behavior, and reduced compensatory neuromuscular responses may increase the importance of anatomical collapsibility even when ventilatory-control instability is not the dominant driver. Therefore, REM- and NREM-predominant OSA should be interpreted as state-specific phenotypic patterns rather than direct surrogates of low or high LG. In clinical interpretation, LG should be considered together with airway collapsibility, arousal threshold, upper-airway muscle responsiveness, arousal dynamics, and the sleep-stage scope of the measurement.2,5,7,8
These scenarios reflect the state- and endotype-dependent expression of LG: ventilatory instability becomes clinically relevant when it interacts with anatomy, arousal behavior, muscle compensation, or treatment response rather than when it is considered as a stand-alone abnormality.Rather than restating the general importance of OSA endotyping, this review focuses on how loop gain can be translated into clinical use. Its specific contribution is to organize current measurement approaches into a deployment-tier framework, ranging from research-grade reference methods to raw-polysomnography modeling, simplified screening tools, and automated or alternative-sensor pathways. The review also proposes a practical reporting logic that links loop gain outputs to their methodological context and to clinical decisions such as treatment restratification, ventilatory-control-targeted therapy, and interpretation of residual instability during CPAP.
Literature Identification and Selection
This clinical translational narrative review was based on literature identified from PubMed, Web of Science, and Embase, supplemented by reference and citation searching of relevant articles. The search covered publications available up to April 2026 and focused on adult obstructive sleep apnea studies related to loop gain physiology, polysomnography-based endotyping, simplified or automated assessment methods, treatment stratification, validation, repeatability, and clinical implementation. Foundational physiological studies, major translational studies, recent reviews, and consensus or research statements were prioritized. No formal systematic-review protocol was registered, and no meta-analysis was performed.
Clinical Scenarios in Which Loop Gain Deserves Particular Attention
There is currently no realistic pathway by which LG could be quantified routinely in every patient with OSA. Its greatest value lies in patients for whom pathophysiological explanation is incomplete or treatment stratification remains uncertain. The first group includes patients with a high AHI and marked event-to-event variability whose upper-airway anatomy seems insufficient to fully explain disease severity. The second includes patients with NREM-predominant OSA, conspicuous post-event ventilatory overshoot, or residual central/complex events during continuous positive airway pressure (CPAP), all of which suggest greater involvement of ventilatory control instability.8–10 The third includes patients being considered for upper-airway surgery, oral appliance therapy, or other anatomical interventions in whom non-anatomical factors may limit treatment efficacy.11–13 The fourth includes patients in whom oxygen therapy, carbonic anhydrase inhibition, or combination therapy is being considered and better physiological matching is desirable.14–16
Thus, the most useful clinical role of LG is not to replace routine diagnostic workflows, but to serve as a tool for pre-treatment restratification and post-treatment reinterpretation. It is especially relevant when there is a mismatch between disease mechanism and treatment choice—that is, when anatomical information does not adequately explain severity or when clinicians need to judge whether strategies beyond anatomy should be considered (Supplementary Table S1)(Figure 1).
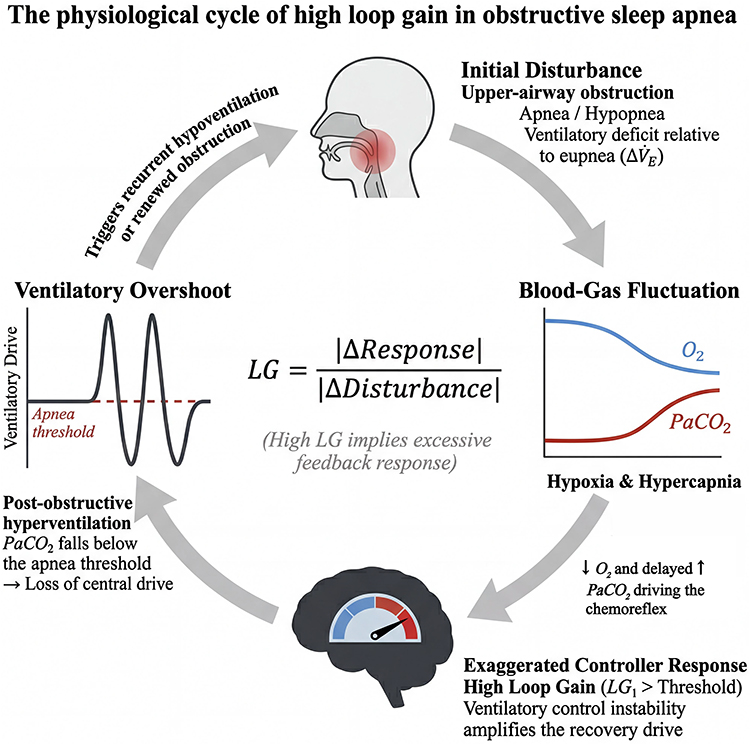 |
Figure 1 The physiological cycle of high loop gain in obstructive sleep apnea. Upper-airway obstruction produces a ventilatory deficit, causing hypoxia and hypercapnia. In patients with high loop gain, an exaggerated chemoreflex response drives post-obstructive ventilatory overshoot; when PaCO2 falls below the apnea threshold, ventilatory drive transiently decreases, predisposing to recurrent hypoventilation or renewed obstruction and perpetuating instability. |
From Research Measurement to Clinical Deployment: Translational Pathways for Loop Gain Assessment
To make LG assessment clinically interpretable, we propose a deployment-tier framework that classifies available methods according to physiological fidelity, workflow burden, and readiness for implementation. Research-grade perturbation methods provide reference physiology; PSG modeling represents the most realistic current pathway for clinical translation; simplified screening tools identify patients with a likely high-LG tendency; and automated or alternative-sensor approaches aim to extend endotyping into lower-burden settings. This tiered structure is intended to avoid false equivalence across methods: each LG output should be interpreted within the implementation that generated it, including the signal source, experimental paradigm, algorithm, and quality-control rules17–22 (Supplementary Methods S1).
Research-Grade Reference Methods: Defining the Physiological Framework of Loop Gain
Methods such as CPAP dial-down/dial-up, proportional assist ventilation (PAV), and pseudorandom binary sequence CO2 stimulation are physiologically closest to reference measurements of LG. CPAP dial-down creates a controlled disturbance by briefly lowering pressure and then quantifies ventilatory overshoot after obstruction is relieved. PAV can infer intrinsic stability by progressively amplifying the ventilatory control loop until instability emerges. Pseudorandom binary sequence carbon dioxide (PRBS-CO2) system identification helps separate controller gain from plant gain and thus clarifies why LG is elevated.5,23–30 Their common importance is that they establish LG as a measurable, calibratable, and decomposable physiological construct.
These methods, however, are not suitable as routine tests in ordinary sleep laboratories. They usually require additional equipment or active intervention, demand stable sleep and technical expertise, and their outputs are influenced by sleep stage, body position, arousal, and stimulus parameters. In a clinically oriented review, they are therefore best regarded as reference methods and anchors for algorithm calibration rather than realistic deployment pathways (Supplementary Methods S2).
PSG-Based Modeling: The Most Realistic Main Pathway at Present
PSG-based modeling is the pivotal step in the clinical translation of LG. Terrill and colleagues first showed that routinely acquired PSG signals can quantify the contribution of ventilatory control to OSA and can detect LG changes induced by oxygen therapy and acetazolamide.18 Sands and colleagues, Finnsson and colleagues, and Dutta and colleagues subsequently advanced the reconstruction of ventilatory drive from raw PSG, the quantification of key pathophysiological traits, and scalable implementation for larger datasets or standard clinical inputs.7,31,32 Compared with research-grade reference methods, the chief advantage of this pathway is that it does not require building a new measurement platform; instead, it extracts more interpretable physiological stratification directly from signals that sleep laboratories already collect, including nasal pressure, effort belts, respiratory events, and arousals.
For clinical translation, the implementation details define the result. PSG-derived LG1 depends on the model structure, frequency-domain assumptions, optimization strategy, analyzable windows, sleep architecture, and signal quality. Recent optimization and repeatability studies therefore support transparent reporting of the software version, parameter settings, window inclusion rules, and quality-control limitations with every LG estimate20,33 (Supplementary Methods S3 and S4).
Simplified Screening Tools: Identify a High-LG Tendency Before Detailed Quantification
In many real-world settings, clinicians do not first need a precise continuous LG value; they need to know whether a patient is likely to have a high-LG phenotype. Point-of-care models derived from routine PSG report variables suggest that predicted LG rises as AHI increases and as the proportion of hypopneas falls.21 At the group level, NREM-predominant OSA also more often points to a meaningful contribution from ventilatory control instability.8 The main value of these tools is to identify potentially high-LG patients at low cost and thereby determine whether more detailed endotyping from raw PSG is warranted.
Daytime voluntary breath-holding and treatment-response clues belong to the same tier. A shorter breath-hold duration and a stronger recovery-breath response may suggest a higher sleep LG.33,34 Likewise, a clearer reduction in respiratory-event burden with oxygen therapy supports a greater contribution of ventilatory instability to disease expression.14–16 These methods should therefore be treated as screening or referral signals that indicate when raw-PSG endotyping may be warranted (Supplementary Methods S5).
Automation and Alternative Sensors: Expanding Access to Loop Gain Assessment
Automation and alternative-sensor approaches represent the newest direction in moving LG assessment from the laboratory toward scalable deployment. The phenotyping using polysomnography (PUP)/PUPpy platform has operationalized PSG endotyping for large retrospective datasets and cross-center replication.32 Respiratory self-similarity algorithms can identify a manifest high-loop-gain surrogate and predict the risk of residual central events during CPAP.10 PPG-derived autonomic-arousal surrogates further support estimation of key endotypic traits in EEG-free polygraphy.22 More recent dynamic-modeling work suggests that automated LG quantification may also be achievable using respiratory inductance plethysmography (RIP) signals alone and can distinguish different phenotypes of ventilatory instability in multi-source datasets including 465 patients.19
The true value of these newer methods is not that they redefine the physiology of LG, but that they lower barriers to access, broaden deployment settings, and improve the feasibility of repeated assessment. Because current evidence still treats conventional PSG endotyping as the principal reference standard, these approaches are better understood as extensions of the deployment pathway rather than direct replacements for research-grade reference methods or standard PSG-based endotyping (Table 1) (Supplementary Methods S6).
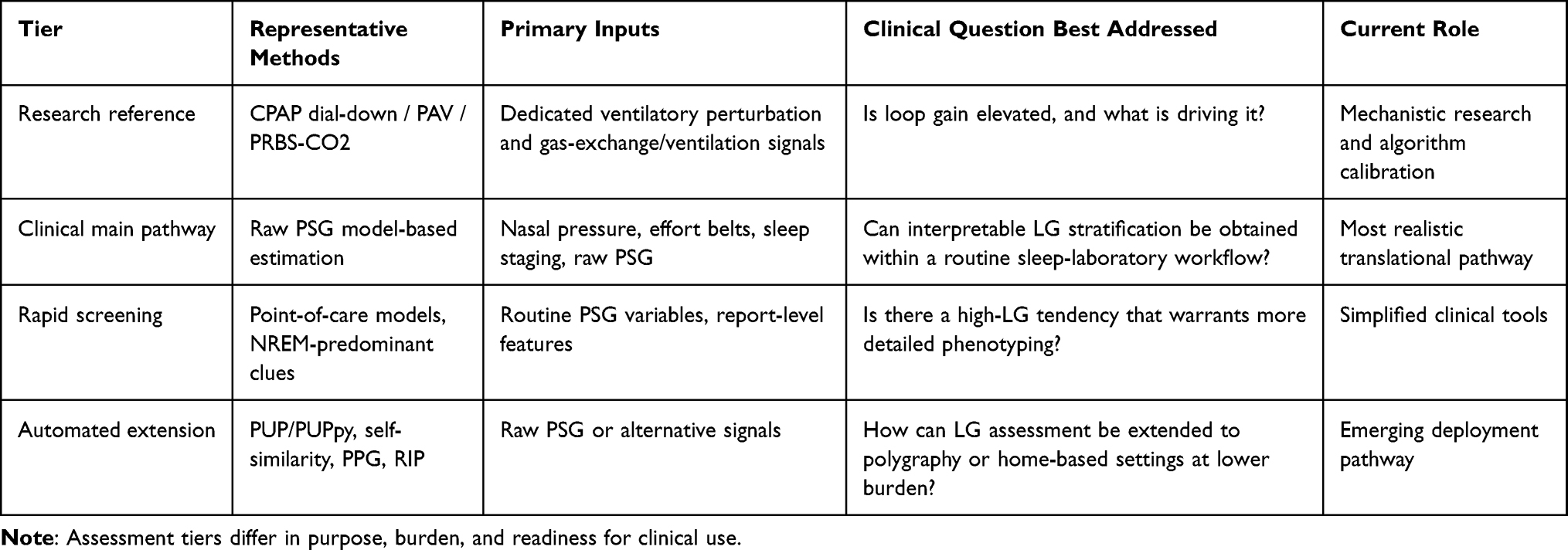 |
Table 1 Proposed Deployment-Tier Framework for Loop Gain Assessment in Obstructive Sleep Apnea |
When Loop Gain Changes the Next Step: Clinical Value for Treatment Stratification
LG only becomes truly translational when it changes the clinical pathway. Although the current evidence base still relies heavily on single-center studies, retrospective analyses, and secondary analyses of clinical trials, four high-value applications have already emerged: judging whether purely anatomical therapy is likely to be sufficient; identifying patients more likely to benefit from oxygen therapy or pharmacotherapy; explaining residual central instability during CPAP; and indicating who may derive greater cardiovascular outcome benefit from treatment.9,11,14–16,35–37
For this reason, LG1 values should be interpreted as implementation-specific decision-support metrics rather than universal physiological constants. In PSG/PUP-style adult OSA studies, reported LG1 values commonly occupy an approximate range of 0.3–1.2, with many clinical cohorts clustering around 0.4–0.8. Lower LG1 values have been associated with a more favorable response to anatomical interventions, whereas higher values may indicate that ventilatory control instability continues to amplify OSA despite correction of upper-airway anatomy.11,16,37 A cutoff around 0.7 has been used in selected PSG-based implementations to define a high-LG tendency, but this threshold should be reported with its measurement method, algorithmic source, and study context rather than treated as a universal treatment threshold.1,3,37
Restratification Before Anatomical Therapy
One of the most direct clinical uses of LG is to determine, before upper-airway surgery or other anatomy-directed interventions, whether OSA is still being materially amplified by ventilatory control instability. Joosten and colleagues showed that a lower baseline LG was associated with a better response to upper-airway surgery, and related work indicates that a lower loop gain together with a more favorable collapsibility profile predicts a better response to oral appliance therapy.11–13 This does not mean that patients with high LG should not receive anatomical therapy; rather, it suggests that they are better served by more complete mechanistic evaluation before treatment, earlier discussion of combined strategies, and more cautious expectations regarding efficacy.
Oxygen Therapy and Ventilatory-Control-Targeted Pharmacotherapy
When high LG contributes substantially to disease expression, the most direct intervention is to reduce ventilatory control instability. Randomized crossover trials and subsequent systematic reviews indicate that nocturnal oxygen can reduce AHI in some patients, but with marked interindividual heterogeneity.14–16 That heterogeneity is entirely consistent with the clinical meaning of LG: oxygen is not a universal therapy for OSA, but may be most relevant for patients in whom ventilatory instability is a major pathogenic driver.
Pharmacologic evidence reinforces the same concept. Earlier work showed that acetazolamide can reduce PSG-estimated LG,18 and a dedicated physiological study further showed that acetazolamide lowered loop gain without materially improving the other major OSA traits.6 Early randomized clinical data with sulthiame showed acceptable short-term safety and tolerability in OSA,35 mechanistic work has shown that sulthiame can modify OSA endotypic traits including loop gain,38 and the subsequent multicentre FLOW Phase 2 trial reported dose-dependent reductions in AHI together with improvements in nocturnal hypoxaemia, sleep quality, and excessive daytime sleepiness with sulthiame.36 These data do not yet support routine LG-guided drug selection, but they do show that ventilatory-control instability is becoming a therapeutic target rather than remaining only an explanatory biomarker.
Residual Instability During CPAP and Complex Sleep Apnea
Another high-value application of LG is to explain why some patients continue to exhibit residual central events or complex sleep apnea during CPAP treatment. A high LG suggests that, even after upper-airway obstruction is removed, the patient may continue to cycle between overshoot and undershoot because the chemical drive response remains excessive. Pilot studies and subsequent automated-algorithm work both support the explanatory and predictive value of LG-related information for residual central instability during CPAP.10 In this setting, LG may not change the initial decision to use CPAP, but it can markedly improve the mechanistic explanation of why instability persists and help guide individualized follow-up adjustments (Supplementary Methods S7).
Potential Value at the Outcome Level
Sleep medicine is increasingly concerned not only with the extent to which AHI falls, but with which patients actually benefit from treatment. A secondary analysis of the HeartBEAT trial showed that a higher LG was associated with a larger reduction in 24-hour mean blood pressure after CPAP, whereas this relationship was not evident in the oxygen-therapy arm.37 Although this remains a secondary analysis and cannot yet be translated directly into clinical rules, it suggests that LG may influence not only disease formation and treatment selection, but also the direction and magnitude of downstream outcome benefit. For a clinically translational review, this link from mechanism to outcome is especially important (Table 2).
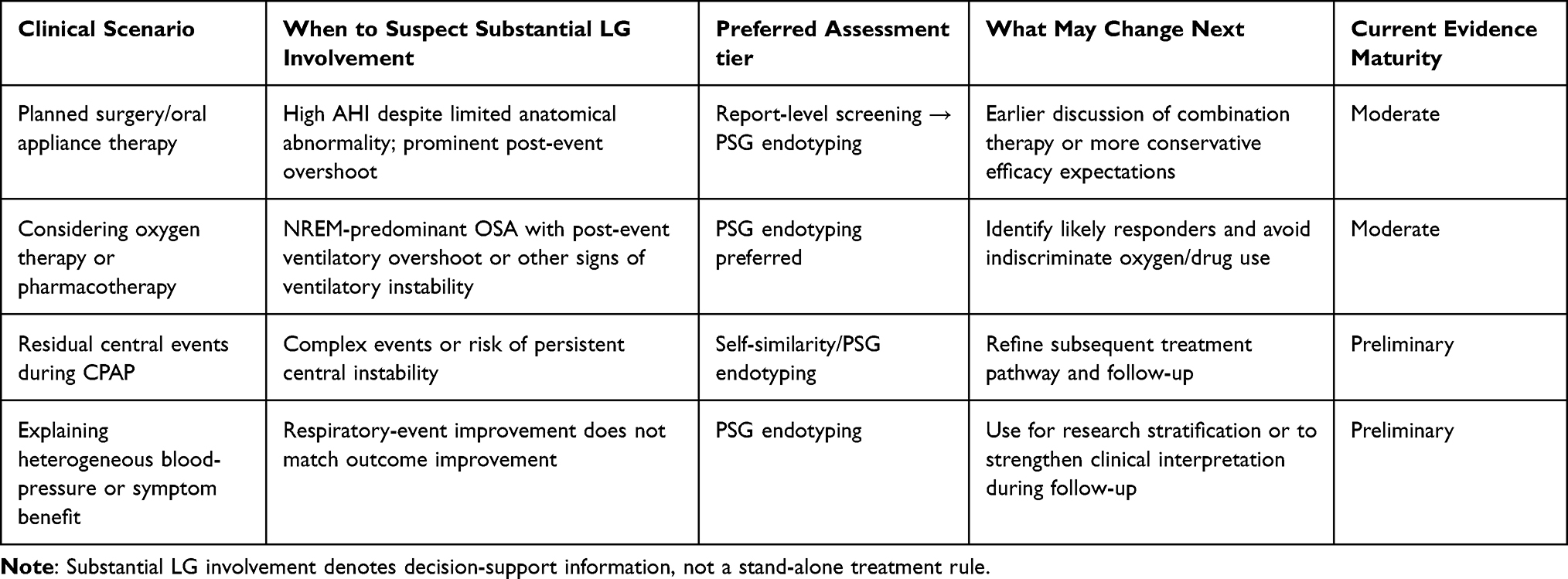 |
Table 2 Potential Clinical Applications of Loop Gain for Treatment Stratification in Obstructive Sleep Apnea |
From Research Output to Clinical Reporting: Implementation Pathways and Real-World Challenges
If LG is to enter clinical workflows, the report should communicate not only a number, but also how that number was obtained and what level of clinical confidence it supports. Building on the deployment-tier framework, we propose a pragmatic reporting logic with three components: first, the LG output itself, preferably as a continuous value and, where appropriate, an implementation-specific category; second, the methodological context, including assessment tier, signal source, software or algorithm version, analyzable windows, signal-quality limitations, and the sleep-stage or positional scope of the estimate; and third, a cautious clinical interpretation explaining whether ventilatory control instability is likely to contribute to OSA maintenance and whether additional endotyping or ventilatory-control-targeted strategies should be considered.
For PSG-based modeling, LG1 is commonly reported because it reflects dynamic feedback gain near the oscillatory frequency of sleep-related breathing instability. The reporting items listed above should accompany any categorical LG1 label so that readers can understand the basis for the interpretation.
A clinically useful LG report should separate decision support from treatment prescription. A high-LG tendency may justify more careful evaluation before purely anatomical therapy, consideration of ventilatory-control-targeted strategies in appropriate specialist or research settings, or closer interpretation of residual central or complex events during CPAP. These interpretations should not be framed as automatic treatment rules. Any mock clinical report card or example LG1 value shown in this review is illustrative only.
Key Issues That Still Limit Routine Adoption
First, implementation transparency remains a prerequisite for clinical validation. Future studies should prespecify the LG assessment method, input signals, software or algorithm version, analysis-window rules, and quality-control criteria before testing whether LG-guided decisions improve outcomes.5,7,19–22,28–30,32
Second, algorithms and optimization strategies can change the stratification result. A technical study published in 2025 showed that changing the optimization method alters model error, the number of boundary solutions, and high-versus-low LG classification.20 At the current stage, standardization, version transparency, and external validation are therefore more urgent than continued proliferation of new algorithms.
Third, repeatability and decision thresholds remain insufficiently established. Although PUP-derived LG1 has shown some night-to-night reliability,33 the clinically relevant questions are how much LG must change to justify a different treatment pathway and which thresholds can be transported across centers. These issues remain inadequately resolved.
Fourth, the evidence base still needs to move from mechanistic association to decision benefit. The 2025 American Thoracic Society research statement explicitly identified technical standards and data sharing, external and prospective validation, clinical-trial design, and knowledge translation and impact assessment as prerequisites for bringing OSA endotyping into clinical care.17 The key question for the next phase is therefore no longer whether LG can be measured, but whether it can be measured in a stable and interpretable way that improves patient-important outcomes(Supplementary Table S2) (Figure 2).
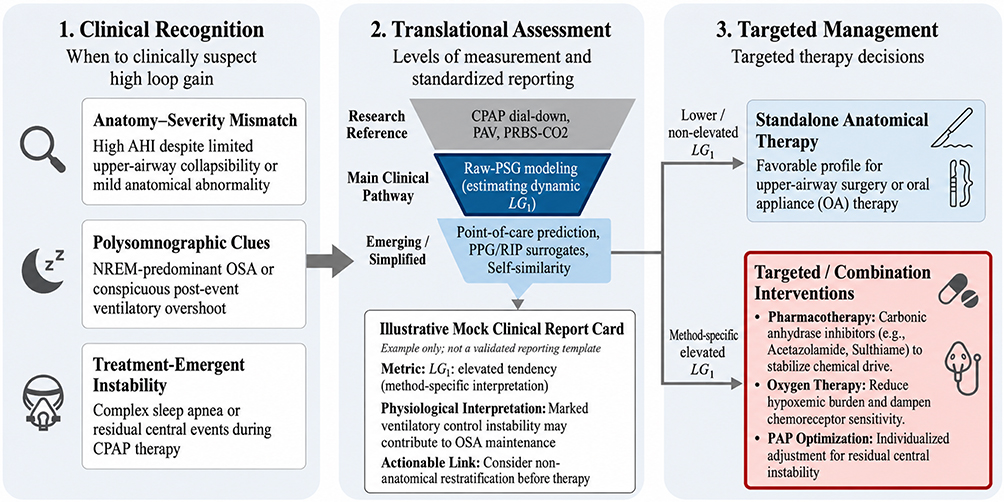 |
Figure 2 Clinical translation framework for loop gain in obstructive sleep apnea. Proposed framework for integrating loop gain into OSA care, from clinical recognition and translational assessment to targeted management. Raw polysomnography-based modelling is presented as the main clinical pathway, with simplified or alternative-sensor approaches as extensions. The mock clinical report card and example LG1 categories are illustrative only and should not be interpreted as a validated reporting standard, recommended clinical template, universal clinical cutoff, or treatment threshold. Lower or non-elevated LG1 may support predominantly anatomical therapy when anatomy is favorable, whereas method-specific elevated LG1 may favor non-anatomical restratification or combination approaches. Note: LG1 denotes dynamic loop gain at approximately 1 cycle/min. The example LG1 categories and mock clinical report card are illustrative only and should not be interpreted as a validated reporting standard or recommended clinical template.LG1 interpretation depends on the measurement method, signal source, algorithm/sofware version, sleep-stage scope, and qualit-control information; oupus from iferent modeling platforms and surrogate sensors are no strictly interchangeable without methodological cos-clibration. |
A Proposed Clinical Implementation Pathway for Loop Gain–Guided Stratification
The immediate translational goal is not to report LG routinely in every patient with OSA, but to define when LG can reasonably change classification, counseling, or management. On the basis of the current evidence and the limitations of available methods, we propose a staged clinical implementation pathway for LG-guided stratification (Table 3). This pathway begins with identifying patients in whom AHI and anatomy are insufficient to explain disease expression, then selects an assessment tier according to clinical burden and required physiological confidence, standardizes reporting, maps the result to a management-relevant category, and finally evaluates whether the LG-informed pathway improves patient-important outcomes.11–15,17,18,39–41
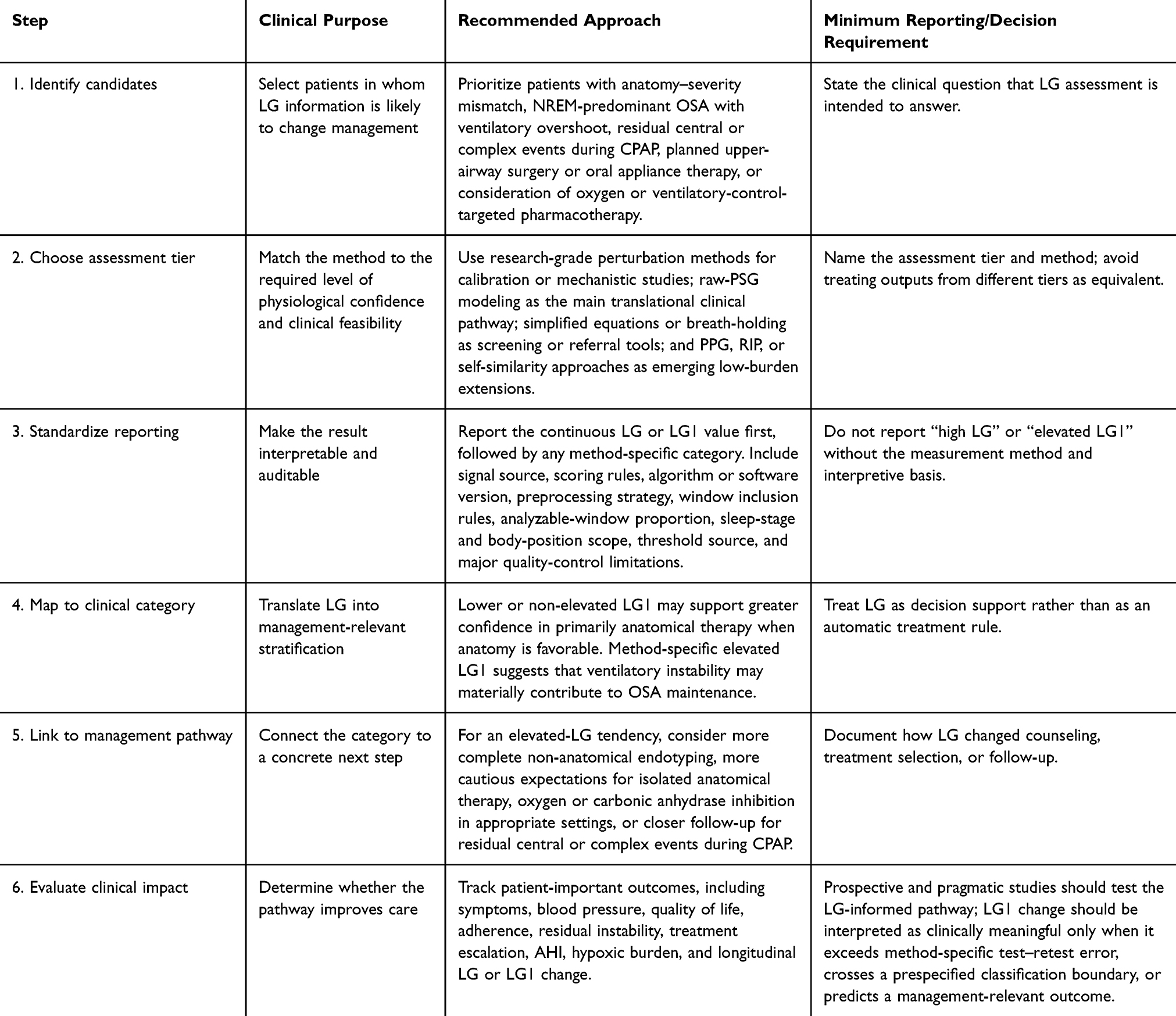 |
Table 3 Proposed Clinical Implementation Pathway for Loop Gain–Guided Stratification in Obstructive Sleep Apnea |
No universal minimal clinically important difference has yet been established for LG or LG1. Existing consecutive-night PUP data suggest that LG1 has good relative reliability but limited individual-level agreement, with an smallest real difference (SRD) of approximately 0.20, or about 24% of the observed LG1 range. Therefore, a candidate clinically meaningful LG1 change should exceed method-specific test–retest error, ideally cross a prespecified high-versus-low classification boundary, and be linked to a management-relevant outcome rather than interpreted as an isolated numerical change.33
This pathway intentionally separates measurement from action. A simplified screening result may justify referral for raw-PSG endotyping, but should not be used as a stand-alone treatment rule. A raw-PSG LG1 result may support clinical restratification, but only when the report specifies the method, threshold source, sleep-stage scope, and quality-control limitations. Similarly, an elevated-LG tendency should not automatically exclude anatomical therapy; rather, it should prompt more complete mechanistic counseling, consideration of combination strategies, and more cautious expectations regarding isolated anatomy-directed treatment.21,33,37,39–41
The final step is to evaluate the pathway rather than only the metric. Future pragmatic studies should ask whether LG-guided stratification changes decisions and improves outcomes compared with usual care. A feasible design would enroll adults with OSA in whom treatment selection is uncertain, perform baseline raw-PSG LG assessment using a prespecified algorithm and reporting template, and compare usual care with an LG-informed pathway. The LG-informed pathway could include non-anatomical endotyping, individualized expectations for surgery or oral appliance therapy, consideration of oxygen or carbonic anhydrase inhibition when clinically appropriate, and targeted follow-up for residual central or complex events during CPAP. Primary outcomes should be patient-important endpoints such as symptoms, blood pressure, quality of life, adherence, treatment escalation, and residual instability, with AHI, hypoxic burden, and LG or LG1 change as secondary mechanistic outcomes. External validation remains necessary, but it should ultimately test the whole LG-informed pathway—measurement, reporting, classification, and decision impact—rather than the transportability of an isolated number alone.
Conclusions
Loop gain provides a clinically meaningful pathophysiological dimension of OSA beyond the AHI, helping explain heterogeneity in disease expression, treatment response, and residual instability. Its most realistic clinical role is not routine measurement in all patients, but selective, staged use when LG information may change classification, counseling, or management. Raw-PSG modeling currently represents the main translational pathway, with simplified screening and automated or alternative-sensor approaches serving as lower-burden extensions. Future work should test whether LG-guided stratification—identifying appropriate candidates, standardizing reporting, and linking results to concrete management decisions—improves patient-important outcomes.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. Access to the data will be granted for legitimate academic or scientific purposes, subject to applicable ethical, institutional, and privacy restrictions.
Author Contributions
Chaofan Li: Conceptualization, Methodology, Investigation, Data curation, Formal analysis, Visualization, Writing – original draft.
Chaohua Wang: Conceptualization, Methodology, Investigation, Data curation, Formal analysis, Visualization, Writing – original draft.
Ying Zhang: Investigation, Data curation, Writing – review and editing.
Juan Y E: Investigation, Data curation, Writing – review and editing.
Bin Guo: Investigation, Data curation, Writing – review and editing.
Min Wu: Investigation, Data curation, Writing – review and editing.
Chun Zhang: Methodology, Visualization, Writing – review and editing.
Shaokun Huang: Methodology, Writing – review and editing.
Guanghao Yue: Conceptualization, Supervision, Project administration, Funding acquisition, Writing – review and editing.
All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Qinghai Province Kunlun Talents Program for High-End Innovation and Entrepreneurship Top-Notch Talents and the Young and Middle-Aged Research Fund Project of the Affiliated Hospital of Qinghai University.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Deacon-Diaz N, Malhotra A. Inherent vs. induced loop gain abnormalities in obstructive sleep apnea. Front Neurol. 2018;9:896. doi:10.3389/fneur.2018.00896
2. Dempsey JA, Smith CA. Pathophysiology of human ventilatory control. Eur Respir J. 2014;44(2):495–12. doi:10.1183/09031936.00048514
3. Antonaglia C, Citton GM, Soave S, et al. Deciphering loop gain complexity: a primer for understanding a pathophysiological trait of obstructive sleep apnea patients. Respir Med. 2024;234:107820. doi:10.1016/j.rmed.2024.107820
4. Naughton MT. Loop gain in apnea: gaining control or controlling the gain? Am J Respir Crit Care Med. 2010;181(2):103–105. doi:10.1164/rccm.200909-1449ED
5. Wellman A, Edwards BA, Sands SA, et al. A simplified method for determining phenotypic traits in patients with obstructive sleep apnea. J Appl Physiol. 2013;114(7):911–922. doi:10.1152/japplphysiol.00747.2012
6. Edwards BA, Sands SA, Eckert DJ, et al. Acetazolamide improves loop gain but not the other physiological traits causing obstructive sleep apnoea. J Physiol. 2012;590(5):1199–1211. doi:10.1113/jphysiol.2011.223925
7. Sands SA, Edwards BA, Terrill PI, et al. Phenotyping pharyngeal pathophysiology using polysomnography in patients with obstructive sleep apnea. Am J Respir Crit Care Med. 2018;197(9):1187–1197. doi:10.1164/rccm.201707-1435OC
8. Joosten SA, Landry SA, Wong AM, et al. Assessing the physiologic endotypes responsible for REM- and NREM-based OSA. Chest. 2021;159(5):1998–2007. doi:10.1016/j.chest.2020.10.080
9. Stanchina M, Robinson K, Corrao W, Donat W, Sands S, Malhotra A. Clinical use of loop gain measures to determine continuous positive airway pressure efficacy in patients with complex sleep apnea. A pilot study. Ann Am Thorac Soc. 2015;12(9):1351–1357. doi:10.1513/AnnalsATS.201410-469BC
10. Oppersma E, Ganglberger W, Sun H, Thomas RJ, Westover MB. Algorithm for automatic detection of self-similarity and prediction of residual central respiratory events during continuous positive airway pressure. Sleep. 2020;44(4):zsaa215. doi:10.1093/sleep/zsaa215
11. Joosten SA, Leong P, Landry SA, et al. Loop gain predicts the response to upper airway surgery in patients with obstructive sleep apnea. Sleep. 2017;40(7). doi:10.1093/sleep/zsx094
12. Edwards BA, Andara C, Landry S, et al. Upper-a4 irway collapsibility and loop gain predict the response to oral appliance therapy in patients with obstructive sleep apnea. Am J Respir Crit Care Med. 2016;194(11):1413–1422. doi:10.1164/rccm.201601-0099OC
13. Bamagoos AA, Cistulli PA, Sutherland K, et al. Polysomnographic endotyping to select patients with obstructive sleep apnea for oral appliances. Ann Am Thorac Soc. 2019;16(11):1422–1431. doi:10.1513/AnnalsATS.201903-190OC
14. Sands SA, Edwards BA, Terrill PI, et al. Identifying obstructive sleep apnoea patients responsive to supplemental oxygen therapy. Eur Respir J. 2018;52(3):1800674. doi:10.1183/13993003.00674-2018
15. Phyu SL, Ercan S, Harriss E, Turnbull C. Nocturnal oxygen therapy in obstructive sleep apnoea: a systematic review and meta-analysis. Eur Respir Rev. 2024;33(171):230173. doi:10.1183/16000617.0173-2023
16. Joosten SA, Tan M, Wong AM, et al. A randomized controlled trial of oxygen therapy for patients who do not respond to upper airway surgery for obstructive sleep apnea. J Clin Sleep Med. 2021;17(3):445–452. doi:10.5664/jcsm.8920
17. Tolbert TM, Schmickl CN, Gell LK, et al. Research priorities for translating endophenotyping of adult obstructive sleep apnea to the clinic: an official American thoracic society research statement. Am J Respir Crit Care Med. 2025;211(9):1562–1583. doi:10.1164/rccm.202507-1574ST
18. Terrill PI, Edwards BA, Nemati S, et al. Quantifying the ventilatory control contribution to sleep apnoea using polysomnography. Eur Respir J. 2015;45(2):408–418. doi:10.1183/09031936.00062914
19. Nassi T, Amidi Y, Oppersma E, et al. Unraveling sleep apnea dynamics: quantifying loop gain using dynamical modeling of ventilatory control. Sleep. 2026;49(2):zsaf213. doi:10.1093/sleep/zsaf213
20. Heuker Of Hoek TA, Cerina L, de Jongh FHC, Fonseca P, Overeem S, Fabius TM. Loop gain quantification from polysomnography in obstructive sleep apnea is impacted by the model optimization technique. Ann Am Thorac Soc. 2025;22(8):1273–1276. doi:10.1513/AnnalsATS.202501-083RL
21. Schmickl CN, Orr JE, Kim P, et al. Point-of-care prediction model of loop gain in patients with obstructive sleep apnea: development and validation. BMC Pulm Med. 2022;22(1):158. doi:10.1186/s12890-022-01950-y
22. Strassberger C, Hedner J, Sands SA, Zou D, Grote L. From pulse to phenotype: sleep apnea endotyping for polygraphy via oximeter-derived autonomic arousal. Chest. 2025;S0012-3692(25):05925.
23. Meza S, Younes M. Ventilatory stability during sleep studied with Proportional Assist Ventilation (PAV). Sleep. 1996;19(suppl_10):164–166. doi:10.1093/sleep/19.suppl_10.164
24. Younes M, Ostrowski M, Thompson W, Leslie C, Shewchuk W. Chemical control stability in patients with obstructive sleep apnea. Am J Respir Crit Care Med. 2001;163(5):1181–1190. doi:10.1164/ajrccm.163.5.2007013
25. Younes M. Proportional assist ventilation, a new approach to ventilatory support. Theory. Am Rev Respir Dis. 1992;145(1):114–120. doi:10.1164/ajrccm/145.1.114
26. Wellman A, Malhotra A, Fogel RB, Edwards JK, Schory K, White DP. Respiratory system loop gain in normal men and women measured with proportional-assist ventilation. J Appl Physiol. 2003;94(1):205–212. doi:10.1152/japplphysiol.00585.2002
27. Gederi E, Nemati S, Edwards BA, Clifford GD, Malhotra A, Wellman A. Model-based estimation of loop gain using spontaneous breathing: a validation study. Respir Physiol Neurobiol. 2014;201:84–92. doi:10.1016/j.resp.2014.07.002
28. Ghazanshahi SD, Khoo MC. Estimation of chemoreflex loop gain using pseudorandom binary CO2 stimulation. IEEE Trans Biomed Eng. 1997;44(5):357–366. doi:10.1109/10.568911
29. Deacon-Diaz NL, Sands SA, McEvoy RD, Catcheside PG. Daytime loop gain is elevated in obstructive sleep apnea but not reduced by CPAP treatment. J Appl Physiol. 2018;125(5):1490–1497. doi:10.1152/japplphysiol.00175.2018
30. Qian Y, Tong H, Cao P, et al. Automatic measurement of loop gain based on pseudorandom binary sequence CO2 stimulation. IEEE Trans Biomed Eng. 2025;72(1):256–263. doi:10.1109/TBME.2024.3449410
31. Dutta R, Delaney G, Toson B, et al. A novel model to estimate key obstructive sleep apnea endotypes from standard polysomnography and clinical data and their contribution to obstructive sleep apnea severity. Ann Am Thorac Soc. 2021;18(4):656–667. doi:10.1513/AnnalsATS.202001-064OC
32. Finnsson E, Ólafsdóttir GH, Loftsdóttir DL, et al. A scalable method of determining physiological endotypes of sleep apnea from a polysomnographic sleep study. Sleep. 2021;44(1):zsaa168. doi:10.1093/sleep/zsaa168
33. Tolbert TM, Schoenholz RL, Parekh A, et al. Night-to-night reliability and agreement of obstructive sleep apnea pathophysiologic mechanisms estimated with phenotyping using polysomnography in cognitively normal elderly participants. Sleep. 2023;46(8):zsad058. doi:10.1093/sleep/zsad058
34. Wang D, Martins RT, Rowsell L, et al. Comparison of awake respiratory control versus sleep obstructive sleep apnea endotypes. J Appl Physiol. 2024;137(6):1524–1534. doi:10.1152/japplphysiol.00138.2024
35. Hedner J, Stenlöf K, Zou D, et al. A randomized controlled clinical trial exploring safety and tolerability of sulthiame in sleep apnea. Am J Respir Crit Care Med. 2022;205(12):1461–1469. doi:10.1164/rccm.202109-2043OC
36. Randerath W, Grote L, Stenlöf K, et al. Sultiame once per day in obstructive sleep apnoea (FLOW): a multicentre, randomised, double-blind, placebo-controlled, dose-finding, phase 2 trial. Lancet. 2025;406(10514):1983–1992. doi:10.1016/S0140-6736(25)01196-1
37. Schmickl CN, Orr JE, Sands SA, et al. Loop gain as a predictor of blood pressure response in patients treated for obstructive sleep apnea: secondary analysis of a clinical trial. Ann Am Thorac Soc. 2024;21(2):296–307. doi:10.1513/AnnalsATS.202305-437OC
38. Hoff E, Strassberger C, Zou D, Grote L, Stenlöf K, Hedner J. Modification of endotypic traits in OSA by the carbonic anhydrase inhibitor sulthiame. Chest. 2024;165(3):704–715. doi:10.1016/j.chest.2023.09.022
39. Quan SF, Ward SLD, Gozal D, et al. AASM scoring manual version 2.2. 2015.
40. Bossuyt PM, Reitsma JB, Bruns DE, et al. STARD 2015: an updated list of essential items for reporting diagnostic accuracy studies. BMJ. 2015;351:h5527. doi:10.1136/bmj.h5527
41. Collins GS, Moons KGM, Dhiman P, et al. TRIPOD+AI statement: updated guidance for reporting clinical prediction models that use regression or machine learning methods. BMJ. 2024;385:e078378. doi:10.1136/bmj-2023-078378
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
New Metrics from Polysomnography: Precision Medicine for OSA Interventions
Guo J, Xiao Y
Nature and Science of Sleep 2023, 15:69-77
Published Date: 9 March 2023
Awareness and Predictors of the Use of Bioinformatics in Genome Research in Saudi Arabia
Alomair L, Abolfotouh MA
International Journal of General Medicine 2023, 16:3413-3425
Published Date: 11 August 2023