Back to Journals » Nature and Science of Sleep » Volume 15
Longitudinal Findings on the Oneiric Activity Changes Across the Pandemic
Authors Scarpelli S ![]() , Alfonsi V
, Alfonsi V ![]() , Camaioni M
, Camaioni M ![]() , Gorgoni M
, Gorgoni M ![]() , Albano A, Musetti A
, Albano A, Musetti A ![]() , Quattropani MC
, Quattropani MC ![]() , Plazzi G, De Gennaro L
, Plazzi G, De Gennaro L ![]() , Franceschini C
, Franceschini C ![]()
Received 15 March 2023
Accepted for publication 28 May 2023
Published 8 June 2023 Volume 2023:15 Pages 435—447
DOI https://doi.org/10.2147/NSS.S410732
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Serena Scarpelli,1 Valentina Alfonsi,1 Milena Camaioni,1 Maurizio Gorgoni,1,2 Antonio Albano,3 Alessandro Musetti,4 Maria Catena Quattropani,5,6 Giuseppe Plazzi,7,8 Luigi De Gennaro,1,2 Christian Franceschini3
1Department of Psychology, University of Rome Sapienza, Rome, Italy; 2Body and Action Lab, IRCCS Fondazione Santa Lucia, Rome, Italy; 3Department of Medicine and Surgery, Faculty of Medicine and Surgery, University of Parma, Parma, Italy; 4Department of Humanities, Social Sciences and Cultural Industries, University of Parma, Parma, Italy; 5Department of Educational Sciences, University of Catania, Catania, Italy; 6Department of Clinical and Experimental Medicine, University of Messina, Messina, Italy; 7Department of Biomedical, Metabolic and Neural Sciences, University of Modena and Reggio Emilia, Modena, Italy; 8IRCCS Institute of Neurological Sciences, Bologna, Italy
Correspondence: Serena Scarpelli, Department of Psychology, University of Rome Sapienza, Via dei Marsi 78, Rome, 00185, Italy, Tel +39 06 49917508, Email [email protected]
Purpose: COVID-19 pandemic waves have strongly influenced individuals’ behaviors and mental health. Here, we analyzed longitudinal data collected in the Spring 2020 and 2021 from a large Italian sample with the aim of assessing changes in dream features between the first and third wave. Specifically, we evaluated the modifications of pandemic dream activity as a function of the general distress variations over time. Also, we detected the best explanatory variables of nightmare frequency and distress.
Materials and Methods: Participants previously involved in the web survey during the first wave of the pandemic were asked to complete a new online survey on sleep and dream features available in Spring 2021 (N=728). Subjects decreasing their level of psychological general distress in the third (T3) vs the first (T1) pandemic wave were defined as “Improved” (N=330). In contrast, participants with an unchanged or increased level of general distress were defined as “Not Improved” (N=398).
Results: Statistical comparisons revealed that dream recall frequency, nightmare frequency, lucid dream frequency, and emotional intensity show a reduction in T3 than T1. Moreover, the Improved group is characterized by lower nightmare rate and nightmare distress than Not Improved people. Our findings confirmed that beyond the trait-like variables (ie, age, sex), specific sleep-related measures are related to nightmare features. In particular, poor sleep hygiene was one of the best determinants of nightmare distress among Not Improved subjects.
Conclusion: Our findings revealed that people experienced an adaptation to the pandemic during the third wave. We also strengthen the notion that nightmares and their variations over time are strongly related to human well-being, suggesting that specific trait-like and sleep-related factors could modulate the relationship between mental health and nightmare features.
Keywords: nightmare, distress, sleep, pandemic, third wave, clinical psychology
Introduction
Different waves of the Coronavirus disease 2019 (COVID-19) pandemic have occurred in Italy since March 2020, strongly influencing the lifestyle of people.1 During the first wave (T1, Spring 2020), the Italian government, according to other European countries, adopted restrictive measures involving home confinement and social distancing in all Italian regions. During the second and third waves, which occurred, respectively, in Autumn 20202 (T2) and Winter-Spring 20213 (T3), restrictive measures were re-adopted taking into consideration the different levels of contagion risk and pressure on the local healthcare system in each region. Both these periods could be considered a “partial-lockdown”.
Many findings from various countries highlighted that both mental health and sleep have been particularly affected by the pandemic.4–6 Moreover, dream activity has been examined in different moments of the pandemic showing important changes in parallel to sleep alterations and mental health conditions.7 A group of studies compared pandemic-related changes in the oneiric activity with a pre-pandemic condition.7 The most reported result concerned the increased dream recall frequency during the first wave/lockdown period compared with the non-pandemic period in both healthy adults8–12 and COVID-19 patients.13 Even more remarkable, nightmare frequency during the pandemic showed an increase among the general population,11,14,15 COVID-19 patients13 and people affected by persistent COVID-19 symptoms.16,17 In parallel, dream contents during the first wave appeared to be more emotionally intense8 with more negative valence8,9 compared to pre-lockdown period. Moreover, poor sleep11 and psychological symptoms (eg, anxiety, depression or stress) were predictors of greater dream recall and nightmare frequency.11,15
Only a few studies examined the changes during the pandemic by using a longitudinal design.18–21 In particular, Italian studies focused on longitudinal comparison of sleep and dreaming during the first two waves of the COVID-19 pandemic revealing changes in dreaming during the pandemic.18–20 For instance, Scarpelli and colleagues18 showed a reduction in dream recall, lucid dream, and nightmare frequency during the second wave compared with the first wave. Importantly, subjects with increased nightmare and lucid dream frequency in the second wave reported higher sleep disturbances, excessive daytime sleepiness and lower sleep hygiene, along with greater post-traumatic growth and Post-Traumatic Stress Disorder (PTSD)-related nocturnal disruptive behaviors.18 Differently, Conte and co-workers19 found that a reduced proportion of participants reported increased or decreased dream frequency during the partial lockdown.
More recently, in an Italian sample reporting moderate level of depression, stress, anxiety and poor sleep, Sommantico et al22 found that, during the third wave, a high proportion of individuals remembered their dreams and nightmares that were, respectively, characterized by high emotional intensity and nightmare distress. Sommantico et al22 showed that people affected by COVID-19 have a higher nightmare distress and more negative emotions in their most recent dreams. Consistently, individuals who knew someone who died of COVID-19 reported greater nightmare distress along with higher anxiety, stress and sleep disturbances during the wakefulness.22
To the best of our knowledge, this represents the only study investigating the sociodemographic, COVID-19-related variables, mood, sleep quality, and oneiric activity during the third wave of the pandemic in Italy.22 However, no longitudinal data including within-subject analyses are available concerning dream changes from the first to the third large waves.
Here, we compared data collected in the third vs first wave from a quite large healthy sample consisting of Italians from all over regions (age range 18–75 years). We aimed to evaluate changes in self-reported dream features between the first and third wave. We also assessed the differences in dreaming taken into account the variation in the general distress among individuals, an index of mental health conditions. Specifically, we hypothesized that all dream variables changed between first and third waves, in the direction of reduced recall of dreams and nightmares. Also, since the well-established relationship between dreaming and mood variables, we expected that the condition of reduced psychological distress during the third wave was associated with a lower unpleasant oneiric activity.
Considering that nightmares are relevant indicators of individual well-being,17 we aimed to identify predictors of nightmare frequency and the associated distress during the third wave (T3). In light of previous findings,8,11,15 we hypothesized that specific trait-like variables (eg, age, sex), COVID-19-related variables, and sleep measures may be determinants of the altered oneiric features in the third wave of pandemic.
Materials and Methods
Protocol and Participants
The current study is part of a more comprehensive project having different aims on the effect of the pandemic in Italy. Part of the data from healthy subjects included in the present study have been reported elsewhere.11,18,23,24
We carried out a follow-up study during the third wave of the pandemic. Italian participants previously involved in the web survey investigating the dream and sleep features during the first wave of the pandemic (please see11,23) were asked to complete a new online survey on the Microsoft Azure platform available from 12 April to 20 May 2021.
The survey was advertised through academic websites (eg, Facebook, Instagram and Twitter accounts of Italian universities) and social networks, and it took approximately 30 min to complete. Subjects were required to fill out self-administered questionnaires to collect socio-demographic and COVID-19-related information, psychological measures, sleep, and dream features.
All subjects filled out the survey after mandatorily accepting the informed consent stating a clear agreement to participate in the study by checking an appropriate box. Conversely, the subject could not access the questionnaires. No monetary compensation was given, and the participation was completely voluntary. After providing written permission, all participants generated a personal identification code to bridge their data between the two time points. Individuals could withdraw from the protocol without justification, and no data was stored. No individually identifiable information was required to guarantee anonymity.
The protocol was carried out following the Declaration of Helsinki, and the approval was granted by the local ethics committee of the University of Messina (protocol #12106, 4 March 2021).
Eight hundred and sixteen individuals included in the first survey (T1) completed the follow-up survey (T3). The response rate at T3 was about 13%. The inclusion criteria were being Italian and being resident in Italy at the time of the survey completion, and being at least 18 years old. To account for potential effects of current or recent COVID-19 infection on oneiric, sleep, or psychological variables, all participants who reported having had COVID-19 within the last 3 months were excluded from the study. In brief, eighty-eight subjects were excluded for the following reasons: 77 reported to have recently had COVID-19 (last three months), 5 subjects were under 18, 6 subjects were living outside Italy. The final sample consisted of 728 participants.
Measures
Socio-Demographic and COVID-19-Related Information
Firstly, socio-demographic and COVID-19-related information were requested: age, sex, Italian area, education level, marital status, occupation, job loss, having friends or relatives infected by COVID-19; having friends or relatives dead due to COVID-19, and changes in physical or online relationships.
Depression Anxiety Stress Scale-21
The short form of the Italian version of the Depression Anxiety Stress Scale-21 (DASS-21)25 was used to assess the mental health status of each participant. Individuals evaluated through 21 items the frequency and severity of depression, anxiety and stress symptoms. Each subscale score corresponds to the sum of the responses to the 7 items multiplied by two. The total score indicates the General Distress, calculated as the sum of the three subscales. The General Distress index (GDI) was considered for further analyses in the current study and used as an index of general psychopathology and mood problems, according to the literature.25
The Italian version of the DASS-21 scale seems to have good psychometric properties. Cronbach’s alpha was between 0.88 and 0.92 for the three scales and the total general distress.25
Sleep Hygiene Index (SHI)
The Sleep Hygiene Index (SHI)26 is a subjective questionnaire including 13 items to assess specific habits associated with sleep hygiene. Subjects rate the frequency of each behavior on a 5-point Likert scale (from “never” to “always”). A total score (13–65) is calculated by summing items and was considered for further analysis in the present study. A greater score represents poor sleep hygiene. The Italian version of SHI showed high internal consistency with a Cronbach’s alpha of 0.91.26
Medical Outcomes Study—Sleep Scale (MOS-SS)
Sleep parameters were evaluated through the Italian adaptation of the Medical Outcomes Study-sleep scale (MOS-SS),27 a self-administered questionnaire assessing the quantity and quality of sleep within a month by 12 items. The questionnaire allows us to obtain six outcomes: sleep disturbance, snoring, awakening short of breath or with headache, sleep adequacy, sleepiness, and sleep duration/optimal sleep. Moreover, a Sleep Problem Index (SPI) can be calculated as a synthetic measure of sleep quality. Specifically, the SPI represents an aggregate measure of responses in the following areas: sleep disturbance, awakening with shortness of breath or headache, sleep adequacy, and sleepiness. In the current investigation, the SPI was considered for further analyses. Internal consistency of the scale is good to excellent, with Cronbach’s alpha values ranging from 0.63 to 0.83 for the subscales.28
Mannheim Dream Questionnaire (MADRE)
Dream characteristics were measured by the Italian adaptation of the Mannheim Dream Questionnaire (MADRE),29 a self-administered questionnaire including 20 items. Different outcomes concerning dreaming features were obtained through this instrument. In the current investigation, we considered for further analyses the following state-like dream measures with the reference to the last month: (a) item 1 evaluating the dream-recall frequency (DRF) from “0 = never” to “6 = almost every morning”; (b) item 2 assessing the dream emotional intensity (EI) from “0 = not at all intense” and “4 = very intense”; (c) item 4 evaluating the nightmare frequency (NMF) from “0 = never” to “8 = several times a week”; (d) item 5 assessing the nightmare distress (NMD) from “0 = not at all distressing” to “4 = very distressing”; and (e) item 10 assessing the lucid-dream frequency (LDF) from “0 = never” to “8 = several times a week”. The Italian version of the MADRE has been shown to have good internal consistency with Cronbach’s alpha values ranging from 0.74 to 0.91.29
Statistical Analysis
Descriptive analyses were performed to show the socio-demographic features of the final sample.
Based on the difference between T3 and T1 on the GDI (from DASS-21), the participants were divided into two subgroups: 1) Improved subjects, ie, participants with a GDI score lower at T3 than T1, and 2) Not Improved subjects, ie, participants with a GDI score equal or higher at T3 than T1. Then, intending to explore differences in dream features between the first (T1) and third (T3) wave of the COVID-19 pandemic, we performed a two-way mixed multivariate analysis of variance (MANOVA), with “Time” (T1 versus T3) as the within-subject factor, and “GDI condition” (Improved vs Not Improved subjects) as the between-subject factor. DRF, NMF, LDF, EI and NMD were considered dependent variables. Partial eta-squared (η2) was calculated as a measure of effect size. Effect sizes between 0.01 and 0.05 were considered small or low, between 0.06 and 0.13 were moderate, and ≥0.14 were large.
Finally, to assess the best explanatory variables of the dream measures discriminating Improved and Not Improved groups, we performed multiple linear regressions separately in the two groups (Not Improved and Improved) considering the following socio-demographic, COVID-19-related, and sleep-related measures as independent variables: age, sex, having friends or relatives infected by or dead due to COVID-19, changes in physical or online relationships, SPI, SHI. We entered the variables at the same time into the model. We also checked the multicollinearity between the predictors (ie, independent variables) prior to performing the regressions by calculating variance inflation factors (VIF <3). The Statistical Package for Social Sciences (SPSS) version 25.0 and MATLAB version R2019 were used for computing statistical analyses. The significance level for all analyses was α = 0.05.
Results
Characteristics of Participants
The features of the sample are detailed in Table 1.
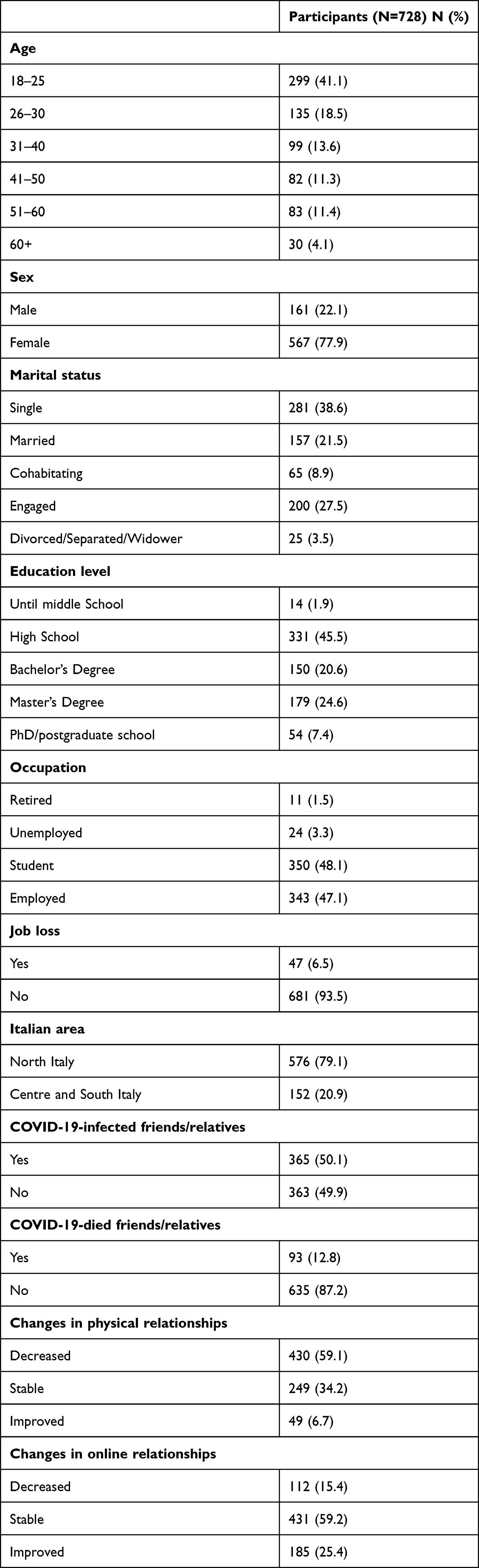 |
Table 1 Characteristics of the Sample During the Third Wave of the Pandemic |
Briefly, more than 40% of participants were young (18–25 years). Most of the participants were females (77.9%). Individuals were mainly single (38.6%), but a significant proportion of subjects was involved in a stable relationship (27.5%) or married (21.5%). Participants most often indicated that they had a high-school education (45.5%). Also, a great percentage of individuals had a job (47.1%) or were students (48.1%). Few subjects had lost (6.5%) their job during the third wave of the pandemic. Moreover, the most represented Italian area was the North (79.1%). Slightly more than half of the sample had COVID-19-infected friends or relatives (50.1%), and a small proportion of people had a close person who died for the COVID-19 infection (around 12%). Finally, more than half of the sample reduced their physical relationships (59.1%) and maintained stable online relationships (59.2%).
Dreams and Nightmares Changes During the Third Wave
In this section, we report the results of the two-way mixed MANOVA (Time X GDI condition) comparing the self-reported dream features between the first and third wave of the pandemic, considering the modifications of the GDI as a criterion to divide the sample in Improved (N = 330) and Not Improved (N = 398) people. We showed significant differences between the two time points (Wilk’s λ = 0.935, F5,722 = 9.977, p < 0.001, η2 = 0.065), but not between the two groups based on GDI scores (Wilk’s λ = 0.994, F5,722 = 0.907, p = 0.476, η2 = 0.006). We also found a significant interaction between the two factors “Time” and “GDI condition” (Wilk’s λ = 0.960, F5,722 = 6.038, p < 0.001, η2 = 0.040).
Specifically, subsequent univariate ANOVAs on each dependent variable (Table 2, and see also Figure 1) revealed that both Improved and Not Improved groups reported in T3 lower scores on the following oneiric variables: DRF (F1,726 = 23.001, p < 0.001, η2 = 0.031), NMF (F1,726 = 14.093, p < 0.001, η2 = 0.019), LDF (F1,726 = 8.996, p = 0.003, η2 = 0.012), EI (F1,726 = 23.778, p < 0.001, η2 = 0.032). Moreover, the significant “Time” vs “GDI condition” interaction points to reduced NMF (F1,726 = 19.734, p < 0.001, η2 = 0.026) and NMD (F1,726 = 4.549, p = 0.033, η2 = 0.006) during the third wave in Improved compared with Not Improved subjects. Accordingly, post-hoc (paired t-tests) showed that Improved subjects significantly reduced their NMF (t = 5.424; p < 0.001) and NMD (t = 2.095; p = 0.037) in T3 compared to T1.
 |
Table 2 Univariate Test of the Two-Way Mixed MANOVA with “Time” and “General Distress Condition” as Within and Between Factors, Respectively |
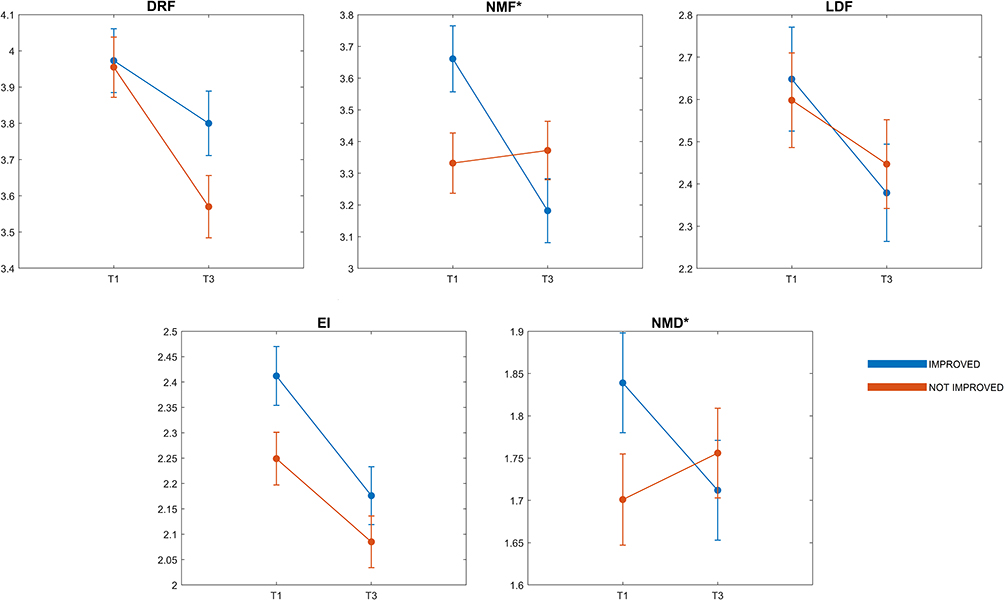 |
Figure 1 Mean (and SE) across the two time periods (T1: first wave; T3: third wave) in the two groups (N = 330 Improved and N = 398 Not Improved) for the following variables: Dream Recall Frequency (DRF), Nightmare Frequency (NMF), Lucid Dream Frequency (LDF), Emotional Intensity (EI), and Nightmare Distress (NMD). *Asterisks indicate statistical significance. |
Predictors of Nightmare Frequency and Nightmare Distress During the Third Wave
Considering socio-demographic, COVID-19-related factors and sleep measures as predictors, multiple linear regressions have been carried out on the oneiric variables in which we detected an interaction effect in the previous analyses, ie, NMF and NMD. Results of the multiple regressions conducted separately on Not Improved and Improved group were reported in Table 3 and 4.
 |
Table 3 Results of the Multiple Linear Regressions Considering Nightmare Frequency and Nightmare Distress During the Third Wave as Dependent Variables in Improved People (N = 330) |
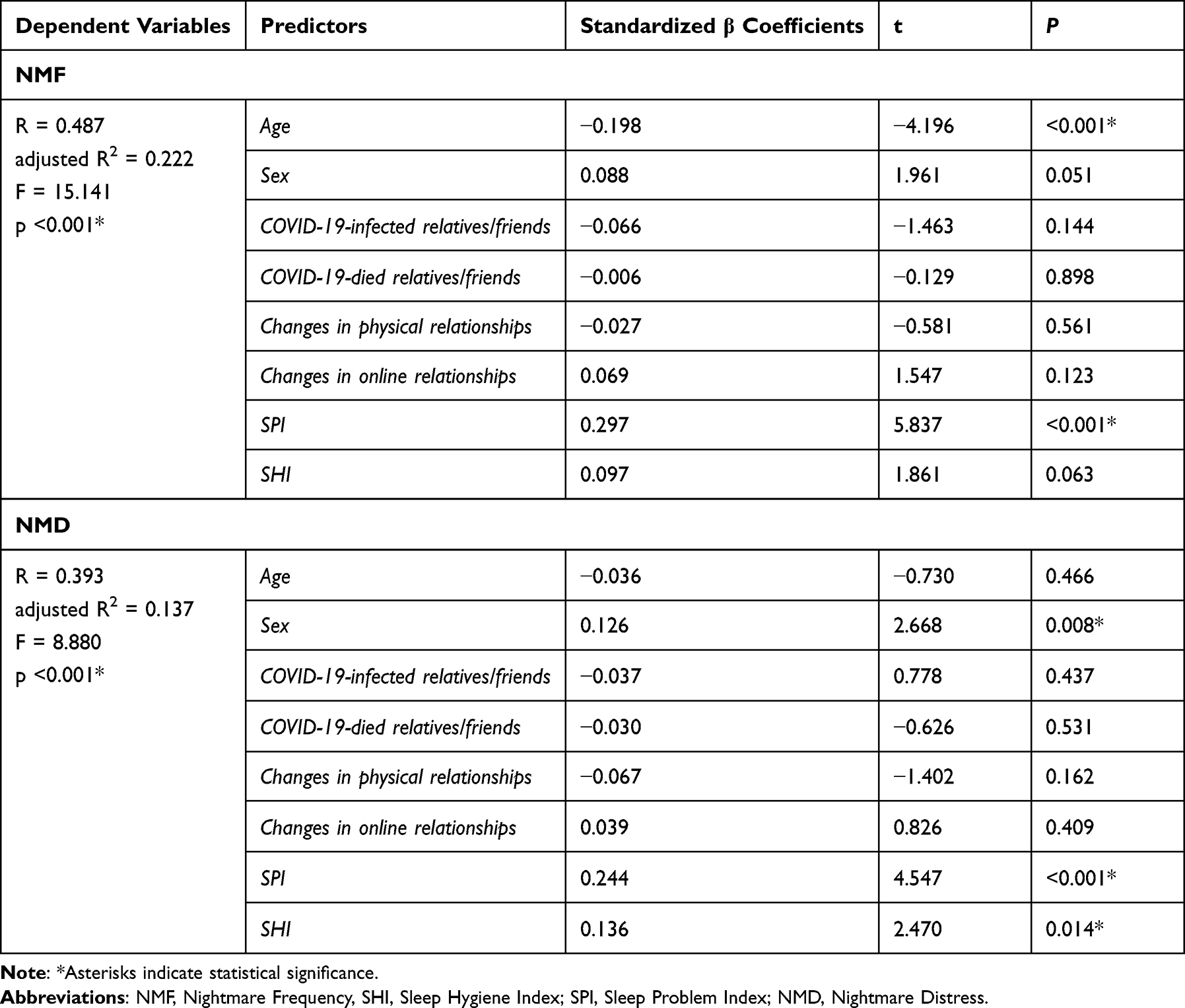 |
Table 4 Results of the Multiple Linear Regressions Considering Nightmare Frequency and Nightmare Distress During the Third Wave as Dependent Variables in Not Improved People (N = 398) |
Concerning Improved participants, both the regression models were statistically significant (NMF: adjusted R2 = 0.179, p < 0.001; NMD: adjusted R2 = 0.090, p < 0.001). The partial correlations show that younger age (β = −0.266; t = −4.931; p < 0.001), female sex (β = 0.135; t = 2.626; p = 0.009), and higher scores on SPI (β = 0.251; t = 4.325; p < 0.001) predict higher NMF. Also, the partial correlations reveal that female sex (β = 0.141; t = 2.590; p = 0.010), and higher scores on SPI (β = 0.199; t = 3.264; p = 0.001) predict higher NMD.
Concerning Not Improved participants, both the regression models were statistically significant (NMF: adjusted R2 = 0.222, p < 0.001; NMD: adjusted R2 = 0.137, p < 0.001). Specifically, the partial correlations show that younger age (β = −0.198; t = −4.196; p < 0.001), and higher scores on SPI (β = 0.297; t = 5.847; p < 0.001) predict higher NMF. Additionally, the partial correlations reveal that female sex (β = 0.126; t = 2.668; p = 0.008), higher scores on SPI (β = 0.244; t = 4.547; p < 0.001), and poor sleep hygiene (β = 0.136; t = 2.470 0; p = 0.014) predict higher NMD.
As control analyses, we performed the regressions on the whole sample to verify potential changes in the predictors of NMF and NMD (see Supplementary Data, Table S1). No other variable was associated with these two oneiric features.
Since the Sleep Hygiene shows a significant relationship with NMD only among Not Improved participants, we checked potential differences of SHI score between T1 and T3 in the Improved and Not Improved groups. Actually, the two-way mixed ANOVA “Time x GDI condition” shows no main effect for Time (F1,726 = 1.327, p = 0.250, η2 = 0.002) and GDI Condition (F1,726 = 1.273, p = 0.260, η2 = 0.002) was found. Differently, the interaction Time x GDI condition was significant (F1,726 = 57.895, p < 0.001, η2 = 0.074) and reveals that the Improved group have greater scores in SHI (poorer sleep hygiene) at T1 than T3. Conversely, Not Improved people report higher scores in SHI at T3 than T1 (see Figure 2).
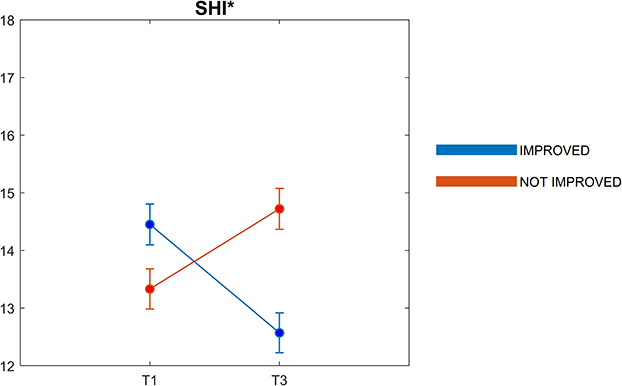 |
Figure 2 Mean (and SE) across the two time periods (T1: first wave; T3: third wave) in the two groups (N = 330 Improved and N = 398 Not Improved) for the Sleep Hygiene Index (SHI). *Asterisks indicate statistical significance. |
Discussion
The current investigation had the main objective to longitudinally evaluate the changes in the oneiric activity during the third wave of the COVID-19 pandemic. In line with the available literature,18,19 we showed that both quantitative (DRF, NMF, LDF) and emotional (EI) oneiric features had lower scores in the third than the first wave. We substantially confirmed the reduced oneiric production and emotional load of dreams after more than one year of the pandemic according to the hypothesis of an adaptation to the situation.19,20,22 Indeed, most of the studies found higher dream recall and nightmare rate among healthy subjects during the period characterized by greater restrictive measures (lockdown/first pandemic wave).8,10,11,30 Consistently, these effects appeared to change over the course of the pandemic, with the reduction of dream recall and lucid dreams immediately after the end of the lockdown31 and lower DRF and NMF during the second wave than the first wave.18
Moreover, for the first time, we assessed the modifications of pandemic dream activity as a function of the general distress variations over time. Although we identified that almost all dream features decreased during the third wave, we revealed that nightmare rate and distress are reduced in the third than first wave only among Improved subjects. Namely, subjects that reduced their level of general (psychological) distress during the third wave reported a decreased rate of nightmare and lower nightmare-related consequences. This is partly in line with the several findings suggesting that changes in the oneiric activity could inform us about the individual psychological conditions.13,32,33 Actually, frequent nightmares are strongly associated with mental illness.34 For instance, anxiety symptoms and mood alterations are often accompanied by nightmares32,35,36 and nightmare sufferers seem to have more suicidal ideations.37,38 More directly, recent studies revealed people more impacted by COVID-19 had greater NMF13,17 or greater emotional load in their dreams.9,29,39,40 Moreover, anxiety symptoms were associated with higher NMF in people who have contracted the infection.13 Also, subjects with long-term COVID-19 consequences showed more nightmares associated with greater number of persistent symptoms and anxiety.17 On the one hand, the reduction of NMF and NMD among Improved is consistent with the continuity hypothesis postulating that dream activity mirror the individual’s current concerns, thoughts and waking experiences.41,42 On the other hand, the absence of any decreasing in NMF and NMD among Not Improved could reflect the effort – still ongoing – of metabolizing, downregulating, and coping with emotions elicited by adverse pandemic events.43
Moreover, we identified the explanatory variables of NMF and NMD in each group. Consistently to the well-known literature on dreaming,44,45 it is not surprising that stable individual features are related with nightmare characteristics. Aging seems to prevent the oneiric production likely because older adults are lower interested in their dreams.46 Additionally, female sex is associated with both high nightmare frequency and nightmare distress in both group, consistently to several COVID-19 studies revealed that women experiencing more dreams and nightmares and an increase in negative dreams during the COVID-19 pandemic.11,15,39,40,47
According to our expectation, Improved and Not Improved people showed higher nightmare frequency and distress in relation to greater sleep problems as evaluated by the MOSS. In other words, having more sleep disorders, intra-sleep awakenings and sleepiness – included in the synthetic index SPI – was associated with greater NMF and NMD. This is in line with previous pandemic studies suggesting that dream rate is influenced by the level of arousal/activation during sleep.7 More in general, the results are coherent with the current frameworks explaining dream recall (eg, arousal-retrieval model48) and also confirmed by electrophysiological studies49–51 emphasizing that fragmentation and lower deep sleep promote the retrieval of oneiric traces.
Interestingly, sleep hygiene was the only determinant related to nightmare distress among Not Improved but not among Improved participants. Our additional analysis revealed two opposite directions for SHI scores in Improved and Not Improved groups between the two different pandemic waves, with a significant amelioration of sleep hygiene among Improved and significant worsening among Not Improved in T3. Notably, some randomized clinical trial showed that including a section that specifically focuses on improving dysfunctional sleep habits appeared to be effective in the treatment of chronic nightmares (eg,52). Moreover, better sleep hygiene by improving overall sleep quality could also reduce the perceived discomfort associated with nightmares.53 In light of this, we can speculate that a good sleep hygiene may represent a protective factor for nightmare-related consequences.
Limitations
The present study has some important limitations. First, likely most of web-survey on the COVID-19 pandemic in the field of sleep research8,23,54,55 we have a sex imbalance in our sample. Importantly, the response rate at T3 was very low (13%). We are aware that people during T1 were probably more willing to fill out online questionnaires and participate in research on pandemic. However, the low response rate can give rise to sampling bias. Both these issues lead to a relative difficulty in generalizing the current results.
Moreover, the protocol did not evaluate the presence of potential long-COVID symptoms that could contribute to modulate the oneiric activity as suggested by previous findings.17
Our investigation has the great advantage of longitudinally comparing oneiric activity between first and third wave in a large Italian sample taking under account the general distress condition. However, it should be noted that we were unable to address the same research objective also considering the second wave since the data on psychological status (DASS) were not collected in that step.
Finally, intrinsic flows of the retrospective questionnaires should be considered since memory biases could stem for the use of self-reported instrument to assess dream and sleep patterns without any support from polysomnographic or actigraphic measures.56
Conclusion
Our investigation represents the first longitudinal assessment of dreaming across the first and third wave of the pandemic. In brief, we found that most of the dream features, with the exception of nightmare distress, decreased in the third wave as compared to the first. Notably, we revealed that subjects that reduced their level of general distress in the third vs first pandemic (ie, Improved people) wave are characterized by lower nightmares rate and nightmare distress.
Additionally, our findings confirmed that beyond the trait-like variables (ie, age, sex), also specific sleep-related measures are related to nightmare features. Importantly, poor sleep hygiene was one of the best determinants of nightmare distress among individuals with unchanged or increased level of general distress (ie, Not Improved people).
Overall, our results strengthen the available pandemic literature emphasizing that nightmares and their variations over time are strongly related to human well-being. Moreover, we suggest that specific factors could modulate the relationship between mental health and nightmares along with their consequences. Therefore, our results suggest that clinicians should assess the role of nightmares to better direct clinical psychological interventions. Future studies should focus on protective and risk factors eliciting nightmares to increase the efficacy of treatments and prevent the development of chronic nightmare disorder.
Abbreviations
COVID-19, coronavirus disease 2019; T1, first wave; T2, second wave; T3, third wave; PTSD, Post-Traumatic Stress Disorder; DASS-21, Depression Anxiety Stress Scale-21; GDI, General Distress index; SHI, Sleep Hygiene Index; MOS-SS, Medical Outcomes Study—Sleep Scale; SPI, Sleep Problem Index; MADRE, Mannheim Dream Questionnaire; DRF, Dream Recall Frequency; NMF, Nightmare Frequency; LDF, Lucid Dream Frequency; EI, Emotional Intensity; NMD, Nightmare Distress; MANOVA, multivariate analysis of variance; VIF, variance inflation factor; SPSS, Statistical Package for Social Sciences.
Disclosure
Giuseppe Plazzi is a consultant and participated in advisory board for Jazz, Bioprojet, Takeda, Idorsia. Luigi De Gennaro reports personal fees from Idorsia, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Altena E, Baglioni C, Espie CA, et al. Dealing with sleep problems during home confinement due to the COVID-19 outbreak: practical recommendations from a task force of the European CBT-I Academy. J Sleep Res. 2020;29(4):e13052. doi:10.1111/jsr.13052
2. Decreto del Presidente del Consiglio dei Ministri 3 Novembre 2020. Available from: https://www.gazzettaufficiale.it/eli/id/2020/11/04/20A06109/sg.
3. Decreto del Presidente del Consiglio dei Ministri 2 Marzo 2021. Available from: https://www.gazzettaufficiale.it/eli/id/2021/03/02/21A01331/sg.
4. Scarpelli S, Zagaria A, Ratti PL, et al. Subjective sleep alterations in healthy subjects worldwide during COVID-19 pandemic: a systematic review, meta-analysis and meta-regression. Sleep Med. 2022;100:89–102. doi:10.1016/j.sleep.2022.07.012
5. Jahrami HA, Alhaj OA, Humood AM, et al. Sleep disturbances during the COVID-19 pandemic: a systematic review, meta-analysis, and meta-regression. Sleep Med Rev. 2022;62:101591. doi:10.1016/j.smrv.2022.101591
6. Merikanto I, Dauvilliers Y, Chung F, et al. Disturbances in sleep, circadian rhythms and daytime functioning in relation to coronavirus infection and long‐COVID– a multinational ICOSS study. J Sleep Res. 2022;31:e13542. doi:10.1111/jsr.13542
7. Gorgoni M, Scarpelli S, Alfonsi V, et al. Dreaming during the COVID-19 pandemic: a narrative review. Neurosci Biobehav Rev. 2022;138:104710. doi:10.1016/j.neubiorev.2022.104710
8. Gorgoni M, Scarpelli S, Alfonsi V, et al. Pandemic dreams: quantitative and qualitative features of the oneiric activity during the lockdown due to COVID-19 in Italy. Sleep Med. 2021;81:20–32. doi:10.1016/j.sleep.2021.02.006
9. Schredl M, Bulkeley K. Dreaming and the COVID-19 pandemic: a survey in a US sample. Dreaming. 2020;30(3):189–198. doi:10.1037/drm0000146
10. Fränkl E, Scarpelli S, Nadorff MR, et al. How our dreams changed during the COVID-19 pandemic: effects and correlates of dream recall frequency-a multinational study on 19,355 adults. Nat Sci Sleep. 2021;13:1573–1591. doi:10.2147/NSS.S324142
11. Scarpelli S, Alfonsi V, Mangiaruga A, et al. Pandemic nightmares: effects on dream activity of the COVID‐19 lockdown in Italy. J Sleep Res. 2021;30(5):e13300. doi:10.1111/jsr.13300
12. Solomonova E, Picard-Deland C, Rapoport IL, et al. Stuck in a lockdown: dreams, bad dreams, nightmares, and their relationship to stress, depression and anxiety during the COVID-19 pandemic. PLoS One. 2021;16(11):e0259040. doi:10.1371/journal.pone.0259040
13. Scarpelli S, Nadorff MR, Bjorvatn B, et al. Nightmares in people with COVID-19: did Coronavirus infect our dreams? Nat Sci Sleep. 2022;14:93–108.
14. Guerrero-Gomez A, Nöthen-Garunja I, Schredl M, et al. Dreaming in adolescents during the COVID-19 health crisis: survey among a sample of European school students. Front Psychol. 2021;12:652627. doi:10.3389/fpsyg.2021.652627
15. Pesonen AK, Lipsanen J, Halonen R, et al. Pandemic dreams: network analysis of dream content during the COVID-19 lockdown. Front Psychol. 2020;11:2569. doi:10.3389/fpsyg.2020.573961
16. Davis HE, Assaf GS, McCorkell L, et al. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClin Med. 2021;38:101019. doi:10.1016/j.eclinm.2021.101019
17. Scarpelli S, De Santis A, Alfonsi V, et al. The role of sleep and dreams in long‐COVID. J Sleep Res. 2022c;18:e13789. doi:10.1111/jsr.13789
18. Scarpelli S, Alfonsi V, Gorgoni M, et al. Dreams and nightmares during the first and second wave of the covid-19 infection: a longitudinal study. Brain Sci. 2021b;11(11):1375. doi:10.3390/brainsci11111375
19. Conte F, Rescott ML, De Rosa O, et al. Changes in dream features across the first and second waves of the Covid‐19 pandemic. J Sleep Res. 2022;31(1):e13425. doi:10.1111/jsr.13425
20. Gorgoni M, Scarpelli S, Alfonsi V, et al. The oneiric activity during and after the COVID-19 total lockdown in Italy: a longitudinal study. Int J Environ Res Public Health. 2022b;19(7):3857. doi:10.3390/ijerph19073857
21. Alfonsi V, Gorgoni M, Scarpelli S, et al. Changes in sleep pattern and dream activity across and after the COVID‐19 lockdown in Italy: a longitudinal observational study. J Sleep Res. 2022;31(2):e13500. doi:10.1111/jsr.13500
22. Sommantico M, Iorio I, Parrello S. Mood, sleep quality, and dreaming during the third wave of the COVID-19 pandemic in Italy. Int J Dream Res. 2021;14(2):309–319. doi:10.11588/ijodr.2021.2.82109
23. Franceschini C, Musetti A, Zenesini C, et al. Poor sleep quality and its consequences on mental health during the COVID-19 lockdown in Italy. Front Psychol. 2020;11:3072. doi:10.3389/fpsyg.2020.574475
24. Musetti A, Soffer-Dudek N, Imperato C, et al. Longitudinal associations between maladaptive daydreaming and psychological distress during the COVID-19 health crisis. J Behav Addict. 2023;1:34.
25. Bottesi G, Ghisi M, Altoè G, et al. The Italian version of the Depression Anxiety Stress Scales-21: factor structure and psychometric properties on community and clinical samples. Compr. 2015;60:170–181. doi:10.1016/j.comppsych.2015.04.005
26. Zagaria A, Ballesio A, Musetti A, et al. Psychometric properties of the Sleep Hygiene Index in a large Italian community sample. Sleep Med. 2021;84:362–367. doi:10.1016/j.sleep.2021.06.021
27. Palagini L, Manni R. Misurare il sonno: repertorio delle scale di valutazione dei disturbi del sonno. Minerva Med. 2016;3–4.
28. Hays RD, Martin SA, Sesti AM, et al. Psychometric properties of the medical outcomes study sleep measure. Sleep Med. 2005;6:41–44. doi:10.1016/j.sleep.2004.07.006
29. Settineri S, Frisone F, Alibrandi A, et al. Italian adaptation of the Mannheim Dream Questionnaire (MADRE): age, gender and dream recall effects. Int J Dream Res. 2019;12(1):119–129. doi:10.11588/ijodr.2019.1.59328
30. Iorio I, Sommantico M, Parrello S. Dreaming in the time of COVID-19: a quali-quantitative Italian study. Dreaming. 2020;30(3):199–215. doi:10.1037/drm0000142
31. Scarpelli S, Gorgoni M, Alfonsi V, et al. The impact of the end of COVID confinement on pandemic dreams, as assessed by a weekly sleep diary: a longitudinal investigation in Italy. J Sleep Res. 2022d;31(1):e13429. doi:10.1111/jsr.13429
32. Blagrove M, Farmer L, Williams E. The relationship of nightmare frequency and nightmare distress to well‐being. J Sleep Res. 2004;13(2):129–136.
33. Carr M, Matthews E, Williams J, et al. Testing the theory of Differential Susceptibility to nightmares: the interaction of Sensory Processing Sensitivity with the relationship of low mental wellbeing to nightmare frequency and nightmare distress. J Sleep Res. 2021;30(3):e13200. doi:10.1111/jsr.13200
34. Bishop TM, Walsh PG, Ashrafioun L, et al. Sleep, suicide behaviors, and the protective role of sleep medicine. Sleep Med. 2020;66:264–270. doi:10.1016/j.sleep.2019.07.016
35. Levin R, Fireman G. Nightmare prevalence, nightmare distress, and self-reported psychological disturbance. Sleep. 2002;25(2):205–212.
36. Van Schagen A, Lancee J, Swart M, et al. Nightmare disorder, psychopathology levels, and coping in a diverse psychiatric sample. J Clin Psychol. 2017;73(1):65–75. doi:10.1002/jclp.22315
37. Sjöström N, Hetta J, Waern M. Persistent nightmares are associated with repeat suicide attempt: a prospective study. Psychiatry Res. 2009;170(2–3):208–211. doi:10.1016/j.psychres.2008.09.006
38. Nadorff MR, Nazem S, Fiske A. Insomnia symptoms, nightmares, and suicidal ideation in a college student sample. Sleep. 2011;34:93–98. doi:10.1093/sleep/34.1.93
39. Barrett D. Dreams about COVID-19 versus normative dreams: trends by gender. Dreaming. 2020;30(3):216–221. doi:10.1037/drm0000149
40. Parrello S, Sommantico M, Lacatena M, et al. Adolescents’ dreams under COVID-19 isolation. Int J Dream Res. 2021;14(1):10–20. doi:10.11588/ijodr.2021.1.73858
41. Hall CS, Nordby VJ. The Individual and His Dreams. New York, NY: NAL; 1972.
42. Scarpelli S, Alfonsi V, Gorgoni M, et al. What about dreams? State of the art and open questions. J Sleep Res. 2022e;31(4):e13609. doi:10.1111/jsr.13609
43. Picchioni D, Goeltzenleucher B, Green DN, et al. Nightmares as a coping mechanism for stress. Dreaming. 2002;12:155–169.
44. Scarpelli S, Bartolacci C, D’Atri A, et al. Mental sleep activity and disturbing dreams in the lifespan. Int J Environ Res Public Health. 2019a;16(19):3658. doi:10.3390/ijerph16193658
45. Schredl M, Reinhard I. Gender differences in dream recall: a meta-analysis. J Sleep Res. 2008;17:125–131. doi:10.1016/j.smrv.2010.06.002
46. Cohen DB. Remembering and forgetting dreaming. In: Kihlstrom J, Evans F, editors. Functional Disorders of Memory. Hillsdale, NY, USA: Erlbaum; 1979:239–274. doi:10.1177/000306516301100404
47. Holzinger B, Nierwetberg F, Chung F, et al. Has the COVID-19 Pandemic Traumatized Us Collectively? The Impact of the COVID-19 Pandemic on Mental Health and Sleep Factors via Traumatization: a Multinational Survey. Nat Sci Sleep. 2022;14(August):1469–1483. doi:10.2147/NSS.S368147
48. Koulack D, Goodenough DR. Dream recall and dream recall failure: an arousal-retrieval model. Psychol Bull. 1976;83(5):975–984. doi:10.1037/0033-2909.83.5.975
49. Scarpelli S, D’Atri A, Mangiaruga A, et al. Predicting dream recall: EEG activation during NREM sleep or shared mechanisms with wakefulness? Brain Topogr. 2017;30:629–638. doi:10.1007/s10548-017-0563-1
50. Siclari F, Baird B, Perogamvros L, et al. The neural correlates of dreaming. Nat Neurosci. 2017;20(6):872–878. doi:10.1038/nn.4545
51. D’Atri A, Scarpelli S, Schiappa C, et al. Cortical activation during sleep predicts dream experience in narcolepsy. Ann Clin Transl Neurol. 2019;6(3):445–455. doi:10.1002/acn3.718
52. Davis JL, Wright DC. Randomized clinical trial for treatment for chronic nightmares in trauma-exposed adults. J Trauma Stress. 2007;202:123–133. doi:10.1002/jts.20199
53. Krakow B, Johnston L, Melendrez D, et al. An open-label trial of evidence-based cognitive behavior therapy for nightmares and insomnia in crime victims with PTSD. Am J Psychiatry. 2001;158(12):2043–2047. doi:10.1176/appi.ajp.158.12.2043
54. Cellini N, Canale N, Mioni G, et al. Changes in sleep pattern, sense of time and digital media use during COVID‐19 lockdown in Italy. J Sleep Res. 2020;29(4):e13074. doi:10.1111/jsr.13074
55. Casagrande M, Favieri F, Tambelli R, et al. The enemy who sealed the world: effects quarantine due to the COVID-19 on sleep quality, anxiety, and psychological distress in the Italian population. Sleep Med. 2020;75:12–20. doi:10.1016/j.sleep.2020.05.011
56. Scarpelli S, Gorgoni M, D’Atri A, et al. Structural and functional differences in brain mechanisms of dream recall. Handb Behav Neurosci. 2019;30:269–281.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Once-Nightly Pregabalin for Co-Occurring Nightmares, Poor Sleep, and Headaches: A Case Series
Bates JH, Rosin SB, Tobin JA
Nature and Science of Sleep 2026, 18:600495
Published Date: 17 July 2026