Back to Journals » Clinical Interventions in Aging » Volume 21
Loneliness Prevalence and Correlates Among Community-Dwelling Older Adults in Taiwan: Clinical Utility of Brief Screening Measures
Authors Tiunn IT, Tsai KT, Lin YJ, Ho CH ![]()
Received 22 February 2026
Accepted for publication 4 June 2026
Published 10 June 2026 Volume 2026:21 604568
DOI https://doi.org/10.2147/CIA.S604568
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Maddalena Illario
Ing-Tiat Tiunn,1,2 Kang-Ting Tsai,1,3 Ying-Jia Lin,4 Chung-Han Ho4– 6
1Department of Family Medicine, Chi Mei Medical Center, Tainan, Taiwan; 2Department of Philosophy, Fu Jen Catholic University, New Taipei City, Taiwan; 3Department of Geriatrics, Well Clinic, Tainan, Taiwan; 4Department of Medical Research, Chi Mei Medical Center, Tainan, Taiwan; 5Department of Information Management, Southern Taiwan University of Science and Technology, Tainan, Taiwan; 6Cancer Center, Taipei Municipal Wanfang Hospital, Taipei Medical University, Taipei, Taiwan
Correspondence: Chung-Han Ho, Department of Medical Research, Chi Mei Medical Center, No. 901, Zhonghua Road Yongkang Dist, Tainan, 71004, Taiwan, Email [email protected]
Introduction: Loneliness is a growing public health concern among older adults. This study examined the prevalence and correlates of loneliness among community-dwelling older adults in Taiwan and compared the performance of three loneliness measurement tools.
Methods: A cross-sectional survey was conducted among adults aged ≥ 65 years recruited from community centers in Southern Taiwan. Loneliness was assessed using the UCLA-LS-20, UCLA-LS-3, and a single-item direct measure. Psychological and health-related variables included LSNS-6, GDS-15, GAD-7, and EQ-5D-5L. Multivariable logistic regression was used to identify factors associated with loneliness, and ROC analysis was performed to compare the discriminatory performance of the three instruments.
Results: Among 186 participants, the prevalence of loneliness ranged from 18% to 27% depending on the instrument used. Higher GDS-15 scores were consistently associated with loneliness across all models. Other associated factors included social network size, living arrangement, anxiety symptoms, and self-rated health. The models using the UCLA-LS-3 and single-item measure showed high AUC values (0.9005 and 0.8988, respectively), and the model using the UCLA-LS-20 also demonstrated good model-specific predictive performance (AUC=0.8123).
Conclusion: Loneliness is common among older adults in Taiwan. Brief measures, such as the UCLA-LS-3 and single-item question, may be practical for community-based loneliness screening, and the UCLA-LS-20 remains useful for more comprehensive assessment.
Keywords: loneliness, older adult, UCLA-LS-20, UCLA-LS-3, single-item direct measure, Taiwan
Introduction
Loneliness, defined as a subjective feeling of social isolation and lack of connection, is a complex and multifaceted experience. It is conceptually distinct from social isolation, which refers to objective measures of social connectedness, such as the number of social contacts.1 Although social isolation can contribute to loneliness, loneliness is a deeply personal and emotional state that can arise even in the presence of social interactions.2,3 It occurs when individuals feel that their social needs are not being met and depends more on the perceived quality and adequacy of social relationships than on objective social contact.1,4
The prevalence of loneliness varies widely across countries and regions. In the United Kingdom, Germany, and the United States, reported rates range from about 5% to 20%,5–7 and rates of up to 34% have been reported in Australia.8 Globally, estimates differ by age group, from about 5–14% among adolescents and young adults to over 20% among older adults in some regions.9 Despite methodological differences across studies, these findings consistently present loneliness as a global public health concern. The impacts of loneliness on health are multifaceted, encompassing psychological, physiological, behavioral, and neuroendocrine aspects.4 Among older adults, loneliness has been associated with depression and anxiety,10 suicide,11,12 cardiovascular disease,13,14 cognitive decline,12,15 and immune dysfunction.4,16 Loneliness may also promote unhealthy behaviors, such as inactivity, poor diet, substance use, and chronic stress responses, which may further increase health risks.17 Overall, loneliness may reduce life satisfaction and overall well-being.18
The third version of the UCLA Loneliness Scale (UCLA-LS-20) is one of the most used instruments for assessing loneliness. This 20-item self-report questionnaire was developed by Russell in 1996, with total scores ranging from 20 to 80, a higher score reflecting greater loneliness.19,20 Various cut-off values have been used to categorize UCLA-LS-20 scores, and a score of 43 is one of the most common cut-off values to dichotomize loneliness.21,22 To improve use in large surveys, a shorter version of the original 20-item scale was proposed in 2004. The UCLA 3-item loneliness scale (UCLA-LS-3) contains three questions with total scores ranging from 3 to 9.23 Researchers have suggested that score 3–5 indicate “not lonely”, and score 6–9 was “lonely”.24 The previous study has supported the UCLA-LS-3 as an adequate dimensional measure of loneliness that is very similar to the UCLA-LS-20.22
In addition to questionnaire-based indirect measures, another commonly used approach for assessing loneliness is the single-item direct measure.9 This measure directly asks individuals about the degree of loneliness they experience from their own perspective, commonly using wording such as “How often do you feel lonely?” Responses of “Often” and “Always” are classified as chronic loneliness, and a response of “Some of the time” may be defined as transient loneliness.25 Single-item direct measure of loneliness show a moderate correlation with the UCLA Loneliness Scale.26 Although the direct and indirect measures are related and move in similar directions, loneliness appear to under-reported loneliness on the direct measure compared with the indirect measure.27 One possible explanation is that some people may be reluctant to admit to loneliness because of stigma or social desirability concerns. In this case, multi-item measures that do not mention loneliness literally may be helpful.28,29
In Taiwan, a national survey conducted in 2017 revealed that nearly 20% of community-dwelling older adults reported feeling lonely occasionally or frequently.30 Another study conducted during the COVID-19 pandemic indicated that lower self-efficacy, higher social support, and greater socialization were related to increases in loneliness, while satisfaction with family support was identified as a protective factor against loneliness.31 However, evidence remains limited about how different loneliness measures perform among community-dwelling older adults in Taiwan. Based on this context, the present study aimed to investigate the prevalence of loneliness among community-dwelling older adults in Taiwan and to compare three loneliness measures, including the UCLA-LS-20, UCLA-LS-3, and a single-item direct measure. Specifically, we examined the prevalence estimates, associated physical and psychological factors, and model-specific predictive performance across these three measures.
Materials and Methods
Study Design and Participants
The study was conducted in multiple community centers in a major city in southern Taiwan, targeting community residents. In Taiwan, community centers are local public venues where older adults can join social, educational, health promotion, and recreational activities. Although these centers are not only for older adults, many regular participants are older community residents. Participants were recruited voluntarily. The inclusion criteria were as follows (a) adults aged 65 or older; (b) those who could understand the purpose and risks of the study and were willing to participate. The exclusion criteria were (a) major physical or mental disabilities that prevented participation; (b) difficulty communicating verbally or in writing.
The researchers explained the purpose, methods, and procedures of the study to eligible participants. After obtaining informed consent, participants completed a hard-copy paper questionnaire. Those capable of reading and answering the questionnaire did so independently, while those unable to read it themselves had the questionnaire administered orally by the researchers, who recorded their responses. This study was approved by the Institutional Review Board of Chi-Mei Medical Center (approval code: 11203–004).
Questionnaire and Measurements
Loneliness Measures
The UCLA-LS-20 is a 20-item scale designed to measure subjective feelings of loneliness and social isolation. Participants rated each item on a scale from 1 (never), 2 (rarely), 3 (sometimes) to 4 (often). The Mandarin translation of the UCLA-LS-20 is available,32 and its psychometric properties have also been evaluated among older adults.21 Higher scores indicate greater loneliness, and a score ≥43 was used to define higher loneliness in this study.
The UCLA-LS-3 comprises three questions that measure three dimensions of loneliness: relational connectedness, social connectedness, and self-perceived isolation. Each question is rated from 1 (hardly ever), 2 (some of the time) to 3 (often). Previous research among older adults has provided supporting evidence for the use of the UCLA-LS-3 in community-based settings.33 A score of 6–9 was used to classify participants as lonely.
The direct measure of loneliness uses a single question “How often do you feel lonely?”, with five response categories: 1 (never), 2 (hardly ever), 3 (occasionally), 4 (some of the time), and 5 (often/always).34 Participants scoring ≥3 were classified as feeling lonely occasionally or more often.
Psychological Distress, Social Network, and Quality-of-Life Measures
The Lubben Social Network Scale (LSNS-6), Geriatric Depression Scale (GDS-15), Generalized Anxiety Disorder Assessment (GAD-7), and EuroQol instrument (EQ-5D-5L) were used to evaluate participants’ degree of social isolation, depression, anxiety, and quality of life, respectively. All these instruments have established Mandarin translations, and reliability and validity evidence has been reported for the LSNS-6, GDS-15, and GAD-7 in older adult populations.35–38 The EQ-5D-5L is a common measure of health-related quality of life, and utility scores were calculated using the established Taiwanese value set.39,40 The EQ-5D-5L consists of two parts. The first part assesses respondents’ quality of life in five dimensions, and the second part consists of a visual analogue scale (EQ-VAS) on which respondents rate their perceived health. For interpretation, LSNS-6 scores <12 indicate risk of social isolation, GDS-15 scores ≥5 suggest possible depression, and GAD-7 scores of 5, 10, and 15 indicate mild, moderate, and severe anxiety symptoms, respectively. Higher EQ-5D-5L utility and EQ-VAS scores indicate better health-related quality of life and self-rated health.
Demographic Variables
Multiple demographic variables, including sex, age, religious affiliation, education level, marital status, living arrangement, social media use, perceived financial sufficiency, and employment status were collected to describe the characteristics of participants. Perceived financial sufficiency was assessed by self-report and categorized according to whether participants perceived their financial condition as sufficient or insufficient for daily living.
Statistical Analysis
Descriptive statistics were used to summarize participants’ demographic, psychosocial, and health-related characteristics. Continuous variables were expressed as means with standard deviations, and categorical variables were presented as frequencies and percentages.
The prevalence of loneliness was reported separately according to the UCLA-LS-20, UCLA-LS-3, and the single-item direct measure. Candidate covariates were selected a priori based on prior literature and conceptual relevance to loneliness, including sociodemographic, psychosocial, and health-related factors. Multivariable logistic regression analyses were performed separately for each loneliness measure to identify associated factors. All selected covariates were entered simultaneously into the multivariable logistic regression models, and the odds ratios (ORs) and 95% confidence intervals (CIs) were also presented for these selected covariates. To further examine the relative contribution of different associated factors, additional block-wise multivariable logistic regression models were used. Model 1 included basic demographic and social characteristics, including age, sex, religion, education, marital status, living status, social media use, perceived financial sufficiency, and work status. Model 2 further added scale-based psychosocial and health-related measures, including LSNS-6, GDS-15, GAD-7, EQ-5D-5L, and EQ-VAS. This block-wise approach was used to assess whether the associations observed in Model 1 were decreased or remained robust after further adjustment for psychosocial and health-related measures. Multicollinearity among covariates was assessed using variance inflation factors (VIFs), with VIF values >5 considered indicative of potential multicollinearity.
Receiver operating characteristic (ROC) curve analysis was used to evaluate the model-specific predictive performance of the multivariable logistic regression models after covariate adjustment. The area under the curve (AUC) was calculated for models using the UCLA-LS-20, UCLA-LS-3, and the single-item direct measure as outcome definitions. Because these models were based on different operational definitions of loneliness, AUC values were interpreted as model-specific performance rather than direct evidence of superiority of one loneliness measure over another. To further evaluate the comparability of the three loneliness classifications, agreement among dichotomized classifications was assessed using Cohen’s kappa statistics. A two-tailed p-value < 0.05 was considered statistically significant. All analyses were conducted using SAS 9.4 (SAS Institute, Cary, NC, USA).
Results
A total of 186 participants were included in this study. The mean age was 72.66 ± 6.98 years, and the majority of participants were female (66.67%). Most participants reported having religious affiliation (89.25%), were married (67.74%), and lived with a spouse and/or descendants (65.59%). Nearly half of the participants had an education level of elementary school or below (46.77%), and 52.69% were unemployed. The mean LSNS-6 score was 18.90±6.05, suggesting that the overall level of social connectedness was above the commonly used threshold for social isolation risk. The mean GDS-15 and GAD-7 scores were 2.85±2.79 and 2.56±3.46, respectively, indicating generally low levels of depressive and anxiety symptoms. The mean EQ-5D-5L and EQ-VAS scores were 0.87±0.23 and 83.48±13.31, respectively, suggesting relatively favorable health-related quality of life and self-rated health (Table 1).
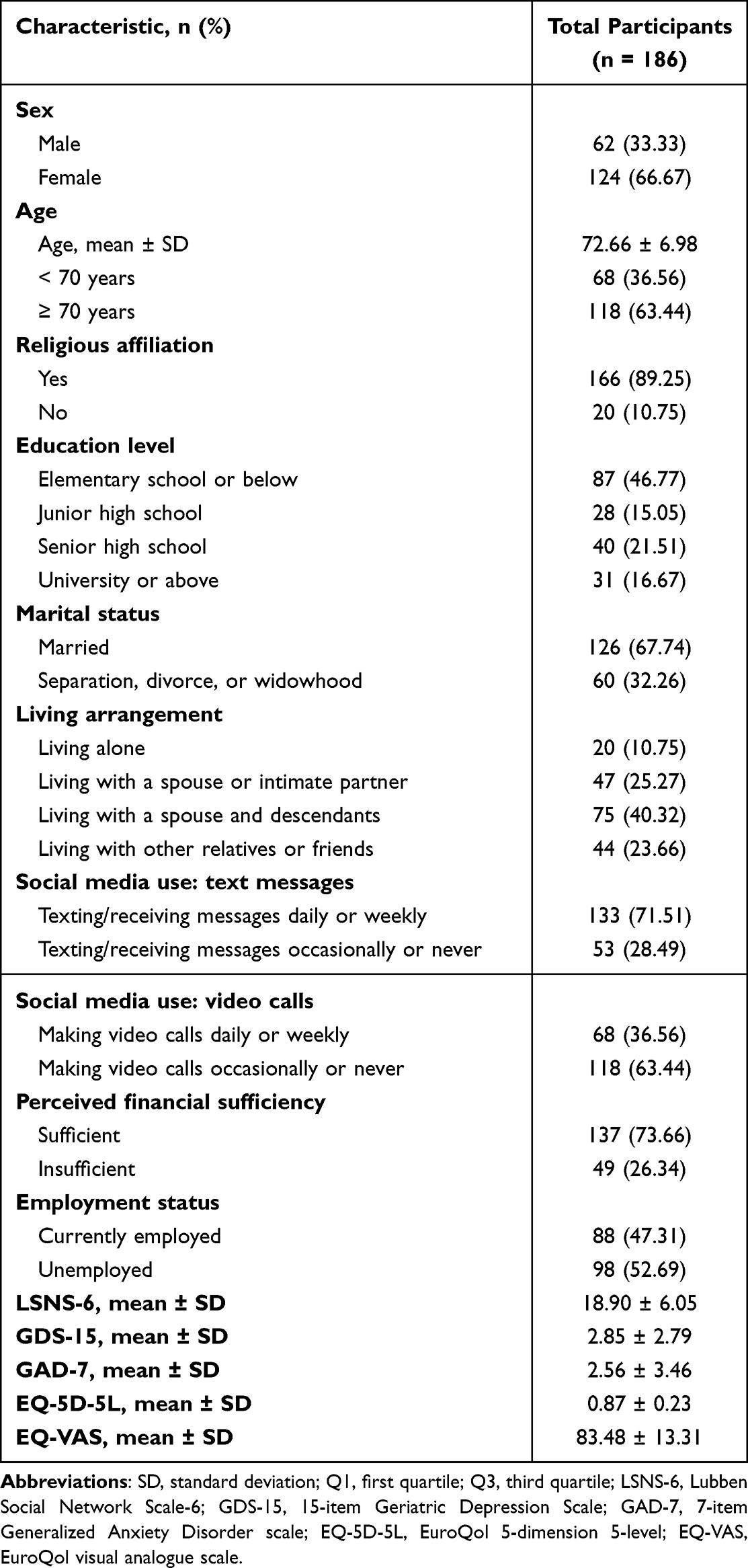 |
Table 1 Characteristics of Participants |
The distribution of loneliness levels across the three measurement tools is presented in Table 2. Based on the predefined cut-off values, the prevalence of loneliness was 27.42% using the UCLA-LS-20 and 18.28% using the UCLA-LS-3. For the single-item direct measure, 26.88% of participants reported feeling lonely occasionally or more often. The distributions of scores for the UCLA-LS-20, UCLA-LS-3, and single-item direct measure are further illustrated using box plots in Supplementary Figure 1.
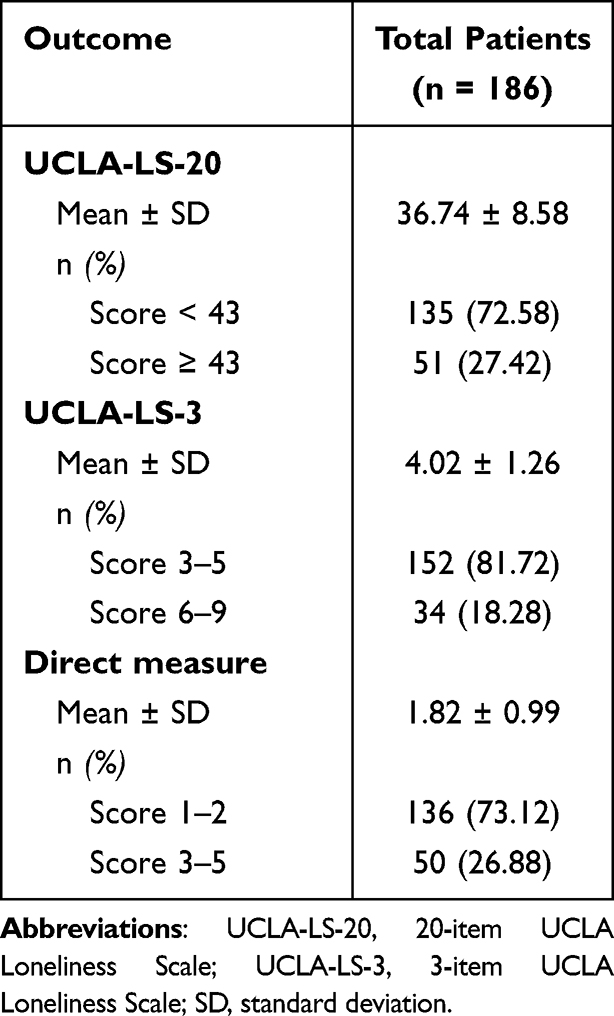 |
Table 2 Outcomes of the Three Loneliness Measurements |
The results of the full multivariable logistic regression models for the three loneliness measures are shown in Table 3. In the model using the UCLA-LS-20, factors significantly associated with being classified into the high-loneliness group (score ≥43) included the absence of religious affiliation (OR = 3.75, 95% CI: 1.01–13.92, p = 0.049), lower scores on the LSNS-6 (OR = 0.90, 95% CI: 0.83–0.97, p = 0.008), higher scores on the GDS-15 (OR = 1.33, 95% CI: 1.09–1.62, p = 0.006), and lower scores on the EQ-5D-5L (OR = 0.74, 95% CI: 0.59–0.92, p = 0.008).
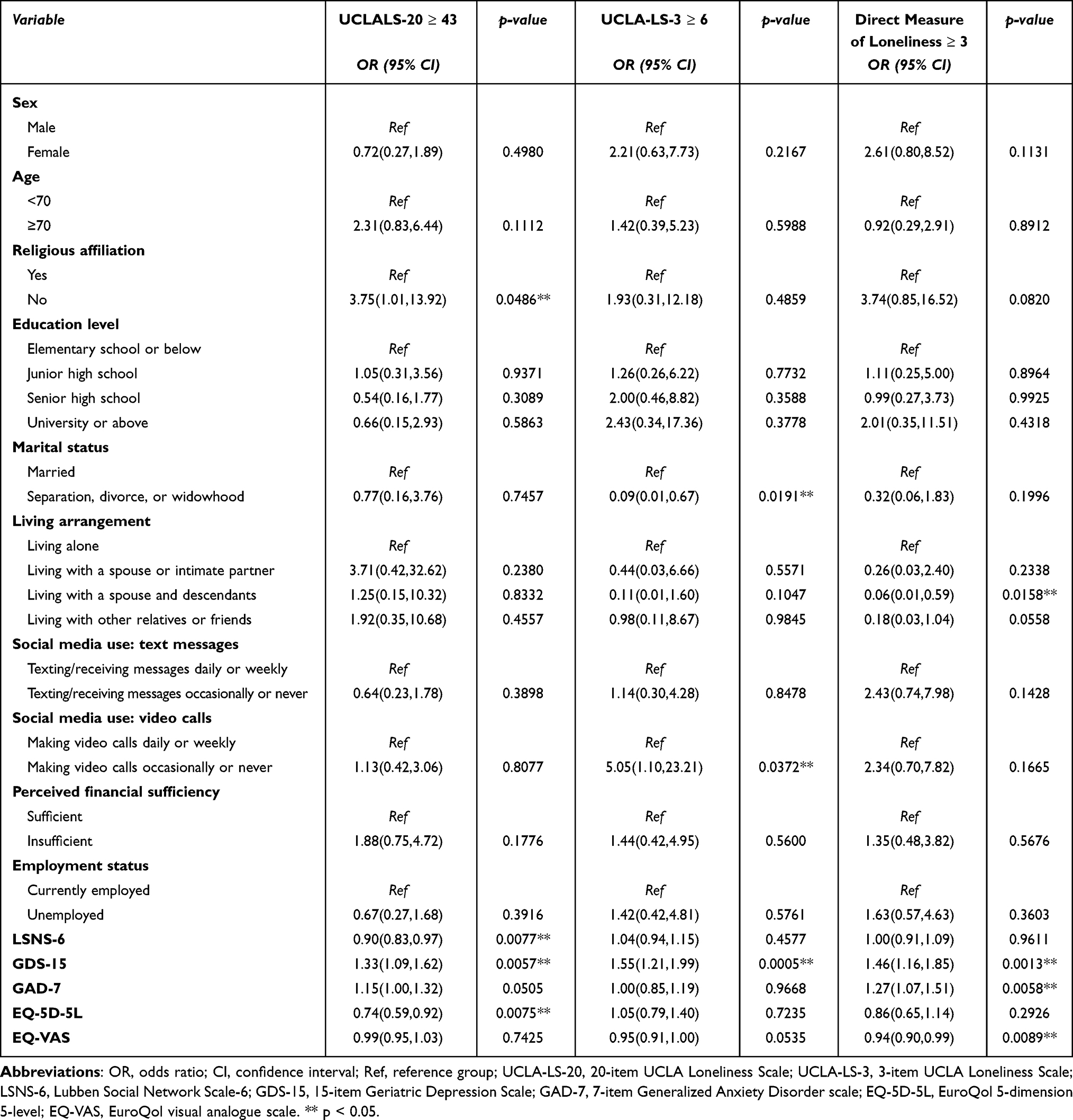 |
Table 3 Multivariable Logistic Regression Analysis of Factors Associated with Loneliness by Different Measurements |
In the model using the UCLA-LS-3, factors significantly associated with loneliness (score ≥6) were marital status, frequency of video calls, and GDS-15 scores. Compared with married participants, those with other marital statuses (separated, divorced, widowed) were inversely associated with loneliness (OR = 0.09, 95% CI: 0.01–0.67, p = 0.019). Participants who occasionally or never used video calls had a significantly higher risk of loneliness compared to those who used them daily or weekly (OR = 5.05, 95% CI: 1.10–23.21, p = 0.037). A higher GDS-15 score was associated with an increased risk of loneliness (OR = 1.55, 95% CI: 1.21–1.99, p = 0.001).
In the model for the direct measure of loneliness (score ≥3), living arrangement, GDS-15, GAD-7, and EQ-VAS were significantly associated with loneliness. Compared to living alone, living with a spouse and children was inversely associated with loneliness (OR = 0.06, 95% CI: 0.01–0.59, p = 0.016). Higher scores on the GDS-15 (OR = 1.46, 95% CI: 1.16–1.85, p = 0.001) and GAD-7 (OR = 1.27, 95% CI: 1.07–1.51, p = 0.006) increased the risk of loneliness. Conversely, better self-rated health was associated with a lower risk of loneliness (OR = 0.94, 95% CI: 0.90–0.99, p = 0.009). In the block-wise analyses, the associations of several demographic and social variables observed in Model 1 were decreased after adding scale-based psychosocial and health-related measures in Model 2 (Supplementary Table 1).
ROC analysis was performed to evaluate the model-specific predictive performance of the three models after adjusting for all covariates. The AUC was 0.8123 for the model using the UCLA-LS-20 definition, 0.9005 for the model using the UCLA-LS-3 definition, and 0.8988 for the model using the single-item direct measure. According to the commonly accepted AUC interpretation criteria, AUC of 0.8–0.9 had good discrimination, and AUC≥0.9 indicated excellent discrimination. Therefore, all three models demonstrated good to excellent model-specific predictive performance. The models using the UCLA-LS-3 and the single-item direct measure as outcome definitions showed higher AUC than the model using the UCLA-LS-20 definition (Figure 1). Agreement analyses were performed to further compare the dichotomized loneliness classifications across the three measures. Agreement was moderate between the UCLA-LS-3 and the single-item direct measure (kappa=0.665), but fair between the UCLA-LS-20 and the single-item direct measure (kappa=0.334), and between the UCLA-LS-20 and the UCLA-LS-3 (kappa=0.352).
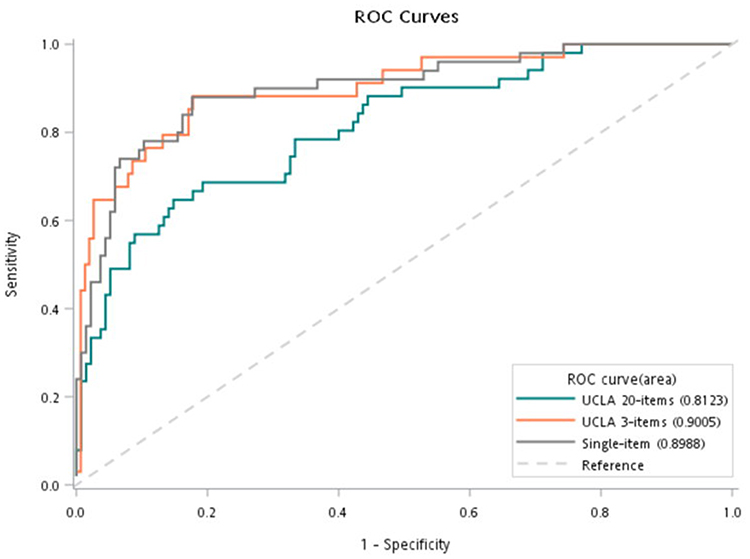 |
Figure 1 ROC curves among three different Loneliness measurements. |
Discussion
This study investigated the factors associated with loneliness among community-dwelling older adults in Southern Taiwan and compared three different loneliness measurement tools. Our findings indicate that loneliness is an important issue, with prevalence rates ranging from 18% to 27% depending on the instrument used. These estimates are comparable to Taiwan’s nationwide survey which reported nearly 20% of community-dwelling older adults felt lonely occasionally or frequently.30 A key finding is that depressive symptomatology (GDS-15) was a robust and consistent factor associated with loneliness across all three models. Furthermore, the brief UCLA-LS-3 and single-item direct measure demonstrated good model-specific predictive performance, and the UCLA-LS-20 remains useful for a more comprehensive assessment of loneliness.
The strong, consistent association between higher GDS-15 scores and loneliness across all three models aligns with a large body of existing literature, confirming the close relationship between depression and loneliness in older adult.41 This relationship is likely bidirectional; longitudinal studies have demonstrated that loneliness can predict the onset of depression, and depression may similarly lead to social withdrawal, thus intensifying loneliness.42,43 While this link is robust, some researchers have argued that the association may be partially confounded by underlying personality traits, such as neuroticism, which predispose individuals to both depression and loneliness.44,45 However, the consistency of the association across diverse populations and its persistence after controlling for clinical covariates suggests that loneliness and depression are distinct, albeit overlapping, constructs.41 This underscores the need for integrated mental health screening. Given this overlap, our finding suggest that brief loneliness measures may be useful as preliminary tools for identifying older adults who require further emotional or psychosocial assessment in busy clinical settings.46
A key contribution of this study is the comparison of loneliness assessment approaches among current sample of community-dwelling older adults in Taiwan. The models using the UCLA-LS-3 and the single-item direct measure showed high AUC values, and the model using the UCLA-LS-20 also demonstrated good model-specific predictive performance. However, these AUC values should be interpreted cautiously because these three models were based on different operational definitions of loneliness. Additionally, these findings suggest that brief measures may have practical value for identifying older adults who may require further assessment in community or clinical settings. Our findings are consistent with previous studies supporting the reliability and construct validity of the UCLA-LS-3 as a proxy for the full scale,23 and a large-scale cohort study also indicated that single-item loneliness measures could be used to predict major health outcomes, including mortality.24
Theoretically, longer scales may better capture the complex and multidimensional nature of loneliness, such as distinctions between social and emotional loneliness.47 Although the UCLA-LS-20 demonstrated good model-specific predictive performance in our study, its observed AUC was numerically lower than those of the models using the two brief measures. A possible explanation is that the 20-item scale may induce greater respondent burden or cause confusion, especially among older populations or those with lower educational attainment.48 This may introduce response variability or measurement noise. Therefore, brief measures are easier to administer and may be more feasible for use in busy primary care settings or large-scale community health surveys, facilitating broader screening and earlier intervention of individuals who may benefit from further evaluation.46 Nevertheless, the UCLA-LS-20 remains valuable with a more comprehensive assessment of loneliness.
Cultural context may also affect how loneliness is experienced, reported, and measured. In Taiwan and other East Asian societies, which are often characterized by family-centered values and collective interdependence, loneliness may be perceived and regulated differently than in Western individualistic cultures. For older adults In Taiwan, loneliness is frequently intertwined with traditional concepts of filial piety and family structure. As personal identity and well-being are often embedded in family and social relationships, loneliness may be experienced not only as an individual emotional state but also as a perceived relational deficiency or unmet expectation of family companionship.49 In addition, East Asian cultures tend to favor emotion suppression and avoidant coping strategies, whereas Western cultures often prioritize active, problem-focused coping and the reappraisal of stressful situations. This suppression can make loneliness more difficult to identify or disclose in clinical or social settings in East Asia.50 Therefore, Western-developed instruments, such as the UCLA-LS, should be interpreted with attention to cultural context.
The different models also revealed unique sets of factors, highlighting the multifaceted nature of loneliness. The UCLA-LS-20 model identified lack of religious affiliation and weaker social networks, measured by the LSNS-6, as factors associated with loneliness. This supports a vast literature emphasizing the protective role of social capital against loneliness.51 In contrast, the single-item direct measure linked loneliness with more direct indicators of health and environment, such as living alone and poorer self-rated health. This finding is also consistent with previous studies identifying living alone as a primary risk factor for social isolation and poor self-rated health as a strong correlate of emotional distress and mortality.52,53
This divergence suggests that different instruments may capture different facets of the loneliness construct. The UCLA-LS-20, with items focused on companionship and social integration, may be more sensitive to deficits in social network. In contrast, the single-item question, as a direct inquiry about emotional state, may capture subjective distress arising from objective, adverse circumstances, such as poor health or domestic isolation. These findings reinforce the idea that the choice of instrument should be guided by the specific aspect of loneliness that researchers or clinicians intend to assess.
Some findings warrant further exploration. In the UCLA-LS-3 model, participants with a marital status other than married, including those who were widowed or divorced, had a lower risk of loneliness. This counterintuitive result may suggest that marital quality, rather than marital status alone, is the more critical factor, or that these individuals have developed more resilient alternative support networks over time.54 In addition, participants who used video calls occasionally or never had a higher likelihood of loneliness than those who used them daily or weekly. This finding may reflect the role of digital communication in maintaining social connection. Social Internet use has been proposed to reduce loneliness when it could help reconnection and increase existing social relationships.55 Video-mediated communication may be particularly suitable for older adults because it makes interaction with family members and friends across geographical distance.56,57 However, evidence regarding the effectiveness of video calls for reducing loneliness among older adults remains limited.58 Alternatively, frequent video-call users may already have stronger social networks, which could partly explain their lower loneliness. Future studies are needed to clarify whether digital communication reduces loneliness or simply reflects pre-existing social connectedness.
Limitations
This study has several limitations. Firstly, the cross-sectional design precludes the establishment of causal relationships between the identified factors and loneliness. To elucidate these causal pathways, future research employing a longitudinal study design should be helpful. Secondly, no a priori power calculation was conducted, and the sample size was determined by the number of eligible participants recruited during the study period. Although the sample size was considered reasonable for estimating loneliness prevalence in this exploratory study, it may have limited statistical power to detect modest associations and to compare model-specific predictive performance across the three loneliness measures. Thirdly, the reliance on self-report measures is subject to potential recall and social desirability biases. Future studies could reduce this limitation by using validated instruments, standardized administration procedures, and complementary qualitative approaches to better capture participants’ subjective experiences of loneliness. Finally, because the participants were recruited from community centers, selection bias should be concerned. Older adults who actively participate in community center activities are likely to be healthier, more functionally independent, and more socially engaged than those who are homebound, frail, or socially isolated. Previous studies in Taiwan have shown that social participation and active engagement in social groups are associated with better mental and physical health among older adults.59,60 Community-based programs are also often designed to support older adults in maintaining independence.61 Therefore, participants may not be fully representative of the broader community-dwelling older population in Taiwan, and the prevalence of loneliness may have been underestimated. Moreover, although participants were recruited from multiple community centers, between-center differences were not examined. This may limit the generalizability of our findings. To improve generalizability, future studies should utilize stratified random sampling combined with a multi-site recruitment strategy, drawing participants from diverse settings such as home care services or residential facilities.
Conclusion
In conclusion, loneliness is a prevalent concern among community-dwelling older adults in Southern Taiwan and is associated with depression, anxiety, social disconnectedness, and poorer health. The UCLA-LS-3 and single-item direct measure may be practical tools for loneliness screening, and the UCLA-LS-20 remains useful for providing a more comprehensive assessment of loneliness. In the absence of a gold standard or common external criterion, our findings should be interpreted as supporting the practical utility of brief measures in community settings. Future research should employ longitudinal designs to elucidate causal pathways and further explore nuanced relationships, such as the roles of marital quality and digital social interaction on loneliness. Clinically, these findings support routine attention to loneliness and the development of multifactorial interventions that address mental health, promote social engagement, and support well-being in older adults.
Abbreviations
UCLA-LS-20, UCLA Loneliness Scale; UCLA-LS-3, UCLA 3-item loneliness scale; LSNS-6, Lubben Social Network Scale; GDS-15, Geriatric Depression Scale; GAD-7, Generalized Anxiety Disorder Assessment; EQ-5D-5L, EuroQol instrument; VAS, visual analogue scale; ORs, odds ratios; Cis, confidence intervals; ROC, Receiver operating characteristic; AUC, area under the curve.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the institutional review board of Chi-Mei Medical Center (IRB: 11203-004), which was conducted in accordance with the Declaration of Helsinki. All participants provided written informed consent.
Acknowledgments
The authors would like to thank the participants for giving freely of their time and effort in supporting our study.
Author Contributions
I.T.T., K.T.T., and C.H.H. conceived and designed the study. Y.J.L. and C.H.H. curated the data and performed the formal analyses. Methodology was developed collaboratively by I.T.T., K.T.T., and C.H.H. Project administration and resource provision were led by I.T.T., who also secured the funding. I.T.T. and K.T.T. conducted validation procedures. The original draft was written by I.T.T., Y.J.L., and C.H.H., and all authors contributed to the review and editing of the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The preparation of this article was supported from grants from the Chi Mei Medical Center (CMFHR112021).
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Perlman D, Peplau LA. Toward a Social Psychology of Loneliness. Academic Press; 1981:31–12.
2. Cacioppo S, Grippo AJ, London S, Goossens L, Cacioppo JT. Loneliness: clinical import and interventions. Perspectives Psychol Sci. 2015;10(2):238–249.
3. Holt-Lunstad J, Smith TB, Baker M, Harris T, Stephenson D. Loneliness and social isolation as risk factors for mortality: a meta-analytic review. Perspectives Psychol Sci. 2015;10(2):227–237.
4. Hawkley LC, Cacioppo JT. Loneliness matters: a theoretical and empirical review of consequences and mechanisms. Ann Behav Med. 2010;40(2):218–227.
5. Office for National Statistics. Loneliness - What characteristics and circumstances are associated with feeling lonely? 2018. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/wellbeing/articles/lonelinesswhatcharacteristicsandcircumstancesareassociatedwithfeelinglonely/2018-04-10.
6. Beutel ME, Klein EM, Brähler E, et al. Loneliness in the general population: prevalence, determinants and relations to mental health. BMC Psychiatry. 2017;17(1):97. doi:10.1186/s12888-017-1262-x
7. Mullen RA, Tong S, Sabo RT, et al. Loneliness in primary care patients: a prevalence study. Ann Fam Med. 2019;17(2):108–115. doi:10.1370/afm.2358
8. Lim MH, Manera KE, Owen KB, Phongsavan P, Smith BJ. The prevalence of chronic and episodic loneliness and social isolation from a longitudinal survey. Sci Rep. 2023;13(1):12453. doi:10.1038/s41598-023-39289-x
9. Surkalim DL, Luo M, Eres R, et al. The prevalence of loneliness across 113 countries: systematic review and meta-analysis. BMJ. 2022;376:e067068. doi:10.1136/bmj-2021-067068
10. Donovan NJ, Blazer D. Social isolation and loneliness in older adults: review and commentary of a national academies report. Am J Geriatric Psychiatry. 2020;28(12):1233–1244.
11. McClelland H, Evans JJ, Nowland R, Ferguson E, O’Connor RC. Loneliness as a predictor of suicidal ideation and behaviour: a systematic review and meta-analysis of prospective studies. J Affect Disord. 2020;274:880–896. doi:10.1016/j.jad.2020.05.004
12. Guarnera J, Yuen E, Macpherson H. The impact of loneliness and social isolation on cognitive aging: a narrative review. J Alzheimer’s Dis Reports. 2023;7(1):699–714.
13. Paul E, Bu F, Fancourt D. Loneliness and risk for cardiovascular disease: mechanisms and future directions. Curr Cardiol Rep. 2021;23(6):68. doi:10.1007/s11886-021-01495-2
14. Christensen AV, Juel K, Ekholm O, et al. Significantly increased risk of all-cause mortality among cardiac patients feeling lonely. Heart. 2020;106(2):140–146. doi:10.1136/heartjnl-2019-315460
15. Karska J, Pszczołowska M, Gładka A, Leszek J. Correlations between dementia and loneliness. Int J Mol Sci. 2023;25(1). doi:10.3390/ijms25010271
16. Smith KJ, Gavey S, Ne RI, Kontari P, Victor C. The association between loneliness, social isolation and inflammation: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2020;112:519–541. doi:10.1016/j.neubiorev.2020.02.002
17. Christiansen J, Lund R, Qualter P, Andersen CM, Pedersen SS, Lasgaard M. Loneliness, social isolation, and chronic disease outcomes. Ann Behav Med. 2021;55(3):203–215. doi:10.1093/abm/kaaa044
18. Park C, Majeed A, Gill H, et al. The effect of loneliness on distinct health outcomes: a comprehensive review and meta-analysis. Psychiatry Res. 2020;294:113514. doi:10.1016/j.psychres.2020.113514
19. Russell DW. UCLA Loneliness Scale (Version 3): reliability, validity, and factor structure. J Pers Assess. 1996;66(1):20–40. doi:10.1207/s15327752jpa6601_2
20. Banerjee A, Kaur Chawla S, Kohli N. The 100 top-cited studies on loneliness: a bibliometric analysis. Cureus. 2023;15(4):e37246. doi:10.7759/cureus.37246
21. Lee C, Cho B, Yang Q, et al. A psychometric analysis of the 20-item revised university of california los angeles loneliness scale among korean older adults living alone. Res Gerontol Nurs. 2021;14(6):306–316. doi:10.3928/19404921-20210924-03
22. Gosling CJ, Colle R, Cartigny A, Jollant F, Corruble E, Frajerman A. Measuring loneliness: a head-to-head psychometric comparison of the 3- and 20-item UCLA Loneliness Scales. Psychol Med. 2024;54(14):1–7. doi:10.1017/s0033291724002083
23. Hughes ME, Waite LJ, Hawkley LC, Cacioppo JT. A short scale for measuring loneliness in large surveys: results from two population-based studies. Res Aging. 2004;26(6):655–672. doi:10.1177/0164027504268574
24. Steptoe A, Shankar A, Demakakos P, Wardle J. Social isolation, loneliness, and all-cause mortality in older men and women. Proc Natl Acad Sci U S A. 2013;110(15):5797–5801. doi:10.1073/pnas.1219686110
25. Department for Digital C, Media and Sport. Investigating factors associated with loneliness in adults in England. 2022. Available from: https://www.gov.uk/government/publications/factors-associated-with-loneliness-in-adults-in-england/investigating-factors-associated-with-loneliness-in-adults-in-england.
26. Russell D. The measurement of loneliness. 1982;81–104.
27. Shiovitz-Ezra S, Ayalon L. Use of direct versus indirect approaches to measure loneliness in later life. Research Aging. 2012;34(5):572–591.
28. Office for National Statistics. Testing of loneliness questions in surveys. 2018. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/wellbeing/compendium/nationalmeasurementofloneliness/2018/testingoflonelinessquestionsinsurveys.
29. Van den Broek T, Lam J, Potente C. Do middle-aged and older people underreport loneliness? Experimental evidence from the Netherlands. Eur J Ageing. 2024;21(1):29.
30. Ministry of Health and Welfare. Report of the senior citizen condition survey. 2017. Available from: https://dep.mohw.gov.tw/DOS/lp-5095-113-xCat-y106.html.
31. Hsu HC, Chao SF. Loneliness, loneliness literacy, and change in loneliness during the COVID-19 pandemic among older adults: a cross-sectional study. BMC Geriatr. 2022;22(1):707. doi:10.1186/s12877-022-03396-7
32. Chang SH, Yang MS. The relationships between the elderly loneliness and its factors of personal attributes, perceived health status and social support. Kaohsiung J Med Sci. 1999;15(6):337–347.
33. Liu T, Lu S, Leung DK, et al. Adapting the UCLA 3-item loneliness scale for community-based depressive symptoms screening interview among older Chinese: a cross-sectional study. BMJ open. 2020;10(12):e041921.
34. Statitics OfN. Measuring loneliness: guidance for use of the national indicators on surveys. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/wellbeing/methodologies/measuringlonelinessguidanceforuseofthenationalindicatorsonsurveys.
35. Chang Q, Sha F, Chan CH, Yip PSF. Validation of an abbreviated version of the Lubben Social Network Scale (“LSNS-6”) and its associations with suicidality among older adults in China. PLoS One. 2018;13(8):e0201612. doi:10.1371/journal.pone.0201612
36. Chang C-J, Chen C-Y. Loneliness in elderly patients: evaluation and management. Taiwan Geriat Gerontol. 2021.
37. Shin C, Park MH, Lee SH, et al. Usefulness of the 15-item geriatric depression scale (GDS-15) for classifying minor and major depressive disorders among community-dwelling elders. J Affect Disord. 2019;259:370–375. doi:10.1016/j.jad.2019.08.053
38. Wild B, Eckl A, Herzog W, et al. Assessing generalized anxiety disorder in elderly people using the GAD-7 and GAD-2 scales: results of a validation study. Am J Geriatric Psychiatry. 2014;22(10):1029–1038.
39. Lin HW, Li CI, Lin FJ, et al. Valuation of the EQ-5D-5L in Taiwan. PLoS One. 2018;13(12):e0209344. doi:10.1371/journal.pone.0209344
40. Chang T-J, Tarn Y-H, Hsieh C-L, Liou W-S, Shaw JW, Chiou XG. Taiwanese version of the EQ-5D: validation in a representative sample of the Taiwanese population. JFormos Med Assoc. 2007;106(12):1023–1031.
41. Owczarek M, Nolan E, Shevlin M, et al. How is loneliness related to anxiety and depression: a population-based network analysis in the early lockdown period. Int J Psychol. 2022;57(5):585–596. doi:10.1002/ijop.12851
42. Wang Y, Liu M, Yang F, Chen H, Wang Y, Liu J. The associations of socioeconomic status, social activities, and loneliness with depressive symptoms in adults aged 50 years and older across 24 countries: findings from five prospective cohort studies. Lancet Healthy Longev. 2024;5(9):100618. doi:10.1016/j.lanhl.2024.07.001
43. Van As BAL, Imbimbo E, Franceschi A, Menesini E, Nocentini A. The longitudinal association between loneliness and depressive symptoms in the elderly: a systematic review. Int Psychogeriatr. 2022;34(7):657–669. doi:10.1017/s1041610221000399
44. Schutter N, Koorevaar L, Holwerda TJ, Stek ML, Dekker J, Comijs HC. ‘Big Five’ personality characteristics are associated with loneliness but not with social network size in older adults, irrespective of depression. Int Psychogeriatr. 2020;32(1):53–63. doi:10.1017/s1041610219000231
45. Ormstad H, Eilertsen G, Heir T, Sandvik L. Personality traits and the risk of becoming lonely in old age: a 5-year follow-up study. Health Qual Life Outcomes. 2020;18(1):47. doi:10.1186/s12955-020-01303-5
46. Gerst-Emerson K, Jayawardhana J. Loneliness as a public health issue: the impact of loneliness on health care utilization among older adults. Am J Public Health. 2015;105(5):1013–1019. doi:10.2105/ajph.2014.302427
47. Weiss RS. Loneliness: the experience of emotional and social isolation.
48. Rolstad S, Adler J, Rydén A. Response burden and questionnaire length: is shorter better? A review and meta-analysis. Value Health. 2011;14(8):1101–1108. doi:10.1016/j.jval.2011.06.003
49. Yen C-M, Huang W-L. Exploring social detachment among older adults in non-urban Southern Taiwan: a qualitative study. Int J Qualitat Studies Health Well Being. 2025;20(1):2560166.
50. Hirano H, Ishii K. Exploring emotion regulation and coping across cultures: implications for happiness and loneliness. Asian J Soc Psychol. 2024;27(4):613–625.
51. Holt-Lunstad J, Smith TB, Layton JB. Social relationships and mortality risk: a meta-analytic review. PLoS Med. 2010;7(7):e1000316. doi:10.1371/journal.pmed.1000316
52. Dahlberg L, McKee KJ. Correlates of social and emotional loneliness in older people: evidence from an English community study. Aging Mental Health. 2014;18(4):504–514. doi:10.1080/13607863.2013.856863
53. Luo Y, Hawkley LC, Waite LJ, Cacioppo JT. Loneliness, health, and mortality in old age: a national longitudinal study. Soc Sci Med. 2012;74(6):907–914. doi:10.1016/j.socscimed.2011.11.028
54. de Jong Gierveld J, Broese van Groenou M, Hoogendoorn AW, Smit JH. Quality of marriages in later life and emotional and social loneliness. J Gerontol SerB. 2009;64(4):497–506.
55. Nowland R, Necka EA, Cacioppo JT. Loneliness and social internet use: pathways to reconnection in a digital world? Perspect Psychol Sci. 2018;13(1):70–87. doi:10.1177/1745691617713052
56. Kim YK, Fingerman KL. Daily social media use, social ties, and emotional well-being in later life. J Soc Pers Relat. 2022;39(6):1794–1813.
57. Hutto CJ, Bell C, Farmer S, et al. Social Media Gerontology: Understanding Social Media Usage Among Older Adults. London, England: SAGE Publications Sage UK; 2015:69–87.
58. Noone C, McSharry J, Smalle M, et al. Video calls for reducing social isolation and loneliness in older people: a rapid review. Cochrane Database Syst Rev. 2020;5(5):Cd013632. doi:10.1002/14651858.Cd013632
59. Chiao C, Weng L-J, Botticello AL. Social participation reduces depressive symptoms among older adults: an 18-year longitudinal analysis in Taiwan. BMC Public Health. 2011;11(1):292.
60. Lee K-L, Wu C-H, Chang C-I, Weng L-J, Wu Y-C, Chen C-Y. Active engagement in social groups as a predictor for mental and physical health among Taiwanese older adults: a 4-year longitudinal study. Int J Gerontol. 2015;9(1):1–6.
61. Crocker TF, Ensor J, Lam N, et al. Community based complex interventions to sustain Independence in older people: systematic review and network meta-analysis. BMJ. 2024;384.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Spotlight on the Challenges of Depression following Retirement and Opportunities for Interventions
Dang L, Ananthasubramaniam A, Mezuk B
Clinical Interventions in Aging 2022, 17:1037-1056
Published Date: 7 July 2022
Effects of a Multi-Component Psychological Intervention to Cultivate Mental Health in Older Adults
Sarrionandia S, Gorbeña S, Gómez I, Penas P, Macía P, Iraurgi I
Clinical Interventions in Aging 2022, 17:1493-1502
Published Date: 11 October 2022
Potential Mobile Health Applications for Improving the Mental Health of the Elderly: A Systematic Review
Chou YH, Lin C, Lee SH, Chang Chien YW, Cheng LC
Clinical Interventions in Aging 2023, 18:1523-1534
Published Date: 14 September 2023
Effects of Wisdom on Mental Health in Old Age: Exploring the Pathways Through Developmental Tasks Attainment and Self-Rated Health
Zadworna M
Psychology Research and Behavior Management 2023, 16:4541-4554
Published Date: 3 November 2023
The Impact of Stigma of Loneliness on Psychological Distress in Older Adults: The Chain Mediating Effect
Fan Z, Shi X, Leng J, Cui D, Li D
Psychology Research and Behavior Management 2025, 18:25-38
Published Date: 8 January 2025