")
Back to Journals » Psychology Research and Behavior Management » Volume 16
Effects of Wisdom on Mental Health in Old Age: Exploring the Pathways Through Developmental Tasks Attainment and Self-Rated Health
Authors Zadworna M
Received 2 August 2023
Accepted for publication 16 October 2023
Published 3 November 2023 Volume 2023:16 Pages 4541—4554
DOI https://doi.org/10.2147/PRBM.S429918
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Magdalena Zadworna
Institute of Psychology, Faculty of Educational Sciences, University of Lodz, Lodz, Poland
Correspondence: Magdalena Zadworna, Email [email protected]
Purpose: A number of studies indicate a relationship between wisdom and mental health in older adults, which can be explained by different pathways. However, the role of developmental task accomplishment, and of self-rated health in the relationships between wisdom and mental health in later life remain unclear. The aim of the current study is to explore the structure of the relationships between wisdom, developmental task attainment, self-rated health, and positive and negative mental health outcomes (viz. wellbeing and depressive symptoms) in older adults.
Methods: The study included 381 Polish older adults aged 60– 86 (M= 67.33; SD = 5.08). The respondents completed the Personal Wellbeing Index, Geriatric Depression Scale, Three-Dimensional Wisdom Scale, Developmental Tasks Attainment Questionnaire for Seniors, self-rated health scale and sociodemographic survey.
Results: Three-dimensional wisdom, developmental task attainment and self-rated health scores were positive predictors of personal wellbeing and negative predictors of depressive symptoms in older adults. Structural equation modelling revealed that developmental tasks attainment and self-rated health partially mediated the relations between wisdom and mental health in older adults.
Conclusion: It can be assumed that wise older adults implement developmental tasks more efficiently and assess their subjective health more favorably, which may strengthen their personal wellbeing and prevent depression. The findings suggest that wisdom plays an important role in healthy aging.
Keywords: mental health, wisdom, developmental tasks, depression, wellbeing, older adults, healthy aging
Introduction
Due to the growing number of older adults in all societies, caused by aging populations and the rise of longevity, promoting healthy aging is now a significant task. The World Health Organization (WHO), in its World Report on Aging and Health, proposes a person-centered concept of “healthy aging”, defined as more than just the absence of disease, but one that encourages the development and maintenance of functional ability that supports well-being in late-life period.1 Each individual has their own “intrinsic capacity”, resulting from the complex interaction between their genetic, personal, and health characteristics, which affects “healthy aging”. Certain elements, such as persistent physical ailments, may be difficult to alter, whereas other factors, particularly psychological ones, may be more susceptible to modification. Psychosocial models exploring the factors determining healthy aging pay special attention to self-rated general health, health behavior, personal and social resources and mental health.2–10
Wisdom and Mental Health
The field of mental health has recently experienced a growth in interest concerning wisdom, which stems from the longstanding association between wisdom and healthy and successful aging.11–13 One of the most popular models of wisdom is the Three-Dimensional Wisdom Model, comprised of a fusion of cognitive, reflective and compassionate personality traits which are indicative of subjective well-being.14 Cognitive wisdom involves understanding oneself, others, and life’s meaning. Reflective wisdom promotes self-examination and multiple perspectives. Compassionate wisdom entails empathy and care for others. Together, these dimensions can be evaluated using a three-dimensional wisdom scale by Ardelt14, which was employed in the current study. Many studies suggest that wisdom is linked to positive mental health outcomes, such as subjective well-being, happiness, psychological resilience, general positive affect and satisfaction with life in old age.14–19 Wisdom also may prevent negative mental health outcomes like depressive symptoms,14,20,21 but also death avoidance, and fear of death in late life,14 social alienation, loneliness,20 negative affect18 and psychopathological symptoms.22 Wisdom possesses a unique capacity to aid decision-making, interpersonal interactions, and daily tasks among older individuals. Consequently, wisdom may exhibit an inverse association with psychopathological symptoms, serving as a preventive and therapeutic factor for mental well-being.22
According to Weststrate and Glück (2017b), the relationship between wisdom and well-being can be attributed to the coping skills and expertise of wise individuals, their ability to benefit themselves and others, and their capacity to appreciate and savor what they have. However, to date, limited studies have attempted to empirically explain why it is that wise individuals report enhanced well-being and fewer depressive symptoms. A few studies have used a structural modeling approach and mediational analyses to explore e.g. mastery and purpose in life,23 resilience and perceived stress,19 and the sense of meaning and perceived control.18 Wisdom appears to bolster other personal resources in the later stages of life, enabling older adults to maintain a sense of well-being despite the challenges and losses associated with aging.
Wisdom and Developmental Task Attainment
A person with greater wisdom would be able to effectively manage and adapt to stressful life circumstances, typical of the last phase of life; furthermore, wise people learn from negative life experiences, providing greater insight, and are better prepared to future obstacles, accepting the unpredictability of life.24 Therefore, wisdom is suggested to be linked to a positive result of personal development in late life and encompasses a range of psychosocial strengths that enable older adults to effectively adjust to the challenges of later life. Those challenges can be considered as developmental tasks, which individuals of a specific age must face. In late life, confronting those challenges may have significant impacts on healthy aging and the progression of typical development and its consequences.25–27 Havinghurst28,29 identifies common developmental tasks encountered by individuals over 60. These include adjusting to declining physical strength, retirement, reduced financial resources, coping with the loss of friends and a partner, sustaining interpersonal bonds within the same age cohort, accepting and adapting to evolving social roles, and making appropriate housing arrangements to promote physical well-being. In Erikson’s theory of psychosocial development across the lifespan, he underscores the developmental crisis of integrity versus despair that occurs in late adulthood.30 During this stage, individuals are expected to reflect on their lives and find a sense of meaning and purpose. They should be capable of justifying the significance of their life and reconciling with the choices they have made, while also accepting the possibilities and paths they did not pursue. Wisdom, as considered by Erikson31 as “detached concern with life itself in the face of death itself” is connected to the resolution of that last crisis, integrity versus despair.
The key developmental tasks aside from the sociocultural context seem to be universal challenges in old age, such as reflecting on one’s life and accepting it as it is, adapting to aging-related changes, and ultimately coming to terms with the reality of losing friends, relatives, and the inevitability of one’s own mortality.25
Wisdom may strengthen the capacity to manage and adjust to losses associated with the aging process and might also facilitate selection, optimization, and compensation (SOC), which enables older adults to take control of their surroundings.32,33 Wisdom also seems to offer individuals the necessary resources to effectively deal with difficult situations, minimize distress, buffer the negative impact of adversity on well-being in old age and uphold a state of well-being during times of crisis and hardship.32,34,35 Wisdom becomes especially significant for well-being in the later stages of life when confronting the abovementioned tasks.36 Critical life events connected with loss and stress in late life, are a threat to well-being, but also constrain the person to adapt to new circumstances, and develop new roles and lifestyles, which can positively contribute to their mental health.37–41 The accomplishment of positive developmental tasks in late life is related to higher life satisfaction42 and lower depressive symptoms.43 Personal resources may also strengthen wellbeing through developmental tasks attainment.42 Therefore, it may be assumed that wiser older adults may attain developmental tasks more effectively, to enhance wellbeing; however, no research has focused strictly on this issue until now.
Wisdom and Self-Rated Health
Moreover, wiser individuals, owing to their deep understanding of life, tend to embrace its unpredictability and uncertainties with equanimity.23 This mindset is likely to decrease stress, leading not only to improved subjective well-being but also to the promotion of physical health. Additionally, wiser older adults may demonstrate better self-care by being mindful of the impact of their behaviors on their self-assessed health. Consequently, they are more likely to avoid detrimental habits like smoking and excessive drinking, while engaging in health-promoting activities such as regular exercise, practicing mental relaxation techniques, and maintaining a balanced diet.
Self-rated health (SRH) appears to be a simple and appropriate method to measure a comprehensive and overall objective health status. When individuals are asked to assess their SRH, they have the autonomy to determine which factors they consider relevant,44 making it an inclusive and personalized method for assessing healthy aging. Numerous empirical studies conducted on diverse older adult populations have consistently shown that among older adults, self-assessment of health is a robust predictor of future morbidity and mortality, as it correlates with various objective health outcomes.45–49 The predictive significance of self-rated health remains remarkably strong across various samples, and single-item measures of SRH offer clinically relevant information about health status, surpassing traditional objective health indicators.50 Moreover, the outcomes derived from different measurement approaches yield comparable evaluations of subjective health.51
Previous research has indeed identified a positive relationships between wisdom and self-rated health.13,14,52 Low self-rated health is also negatively related to life satisfaction53–57 and higher numbers of depressive symptoms in old age.58–61 It must be also noted, though, that the relation between variables may also be bidirectional: people who are more satisfied with their lives and less depressed report better self-rated health.9,62–64 The mediational role of subjective health in the relation between wisdom and mental health outcomes has not yet been investigated.
Mental Health in Older Adults
Mental health in older adults is often assessed according to both positive (wellbeing and life satisfaction) and negative outcomes (depression and dementia),65 which may be affected by different pathways.66,67 Subjective well-being can be characterized as the extent to which individuals assess or perceive the quality of their own lives. Life satisfaction represents the cognitive aspect of subjective well-being and arises from an evaluative process where individuals compare their current life circumstances with a perceived standard or expectation.68 Therefore, it refers to some standards of evaluation, which could be related to diverse spheres of life. The Personal Wellbeing Index, used in the present study as the outcome variable, reflects the decomposition of life satisfaction in satisfactions with various areas.69 Moreover, it is not necessary for depression, as a category within the realm of mental health, to be positioned as the direct opposite of well-being. Instead, it could potentially represent a distinct spectrum of depressive experiences, separate from the spectrum of well-being.70 In fact, similar to findings indicating that positive affect and negative affect are two distinct dimensions,71 depressive symptoms are typically inversely correlated with well-being but could also exist as a distinct phenomenon. However, depressive symptoms can significantly affect the well-being and functional abilities of older individuals.53,72 To identify potential ways of helping older individuals lead happier and healthier lives, it is crucial to not only explore the influence of wisdom on mental health challenges, like depressive symptoms, but also on promoting positive mental health.
Notably, both life satisfaction and depressive symptoms can independently serve as predictors of mortality over time in older adults.73 This highlights the importance of identifying individual resources that can serve as protective factors when facing diminished abilities and multiple losses in old age. Such resources have the potential to mitigate depressive symptoms and positively contribute to life satisfaction.74
These factors underscore the essential components of healthy and successful aging. These principles comprise a web of psychological and health factors that serve as a multifaceted backdrop for a personal life. Nevertheless, the specific structural relations between them, as well as the underlying mechanisms influencing these associations and their impact on mental health in late life, remain incompletely understood.
Therefore, the objective of the present study is to evaluate the predictive role of wisdom, self-rated health, and developmental task accomplishment for mental health outcomes (wellbeing and depressive symptoms) among retirees in Poland. Additionally, the study explores the structure of relationships between the variables, after controlling for sociodemographic factors.
Wisdom, developmental task attainment and self-rated health were expected to be related to mental health in late life – positively to personal wellbeing and negatively to depressive symptoms, after controlling for sociodemographic variables (Hypothesis 1). Developmental task attainment and self-rated health were predicted to mediate the association between wisdom and mental health outcomes (Hypothesis 2).
Materials and Methods
Procedure and Data Collection
The study employed a cross-sectional design with a purposeful sample selection. Data were collected through computer-assisted-web-interview (CAWI) between June 2022 and July 2022. Participants were recruited from the Polish National Panel, one of the commercial research panels operating in Poland that comprises voluntary respondents from across the country. They were previously registered in the research panel system, accepted the regulations and consented to participate in social surveys. All respondents received an email invitation from the panel operators, inviting them to participate in the study. Before the survey started, the respondents were given an information letter about the purpose of the study and instructions on test completion, and were assured that their participation was anonymous and voluntary. Participants confirmed their informed consent before starting the survey, but they could also withdraw at any stage. The initial instructions included an e-mail address to the researcher with whom they could contact if they had any questions. Only retired individuals aged 60 and above who gave their informed consent were included in the final sample.
The study adhered to the Helsinki Declaration of Human Rights.75 The research protocol received approval from the Research Ethics Board at the University of Lodz.
Participants
The study was conducted with a sample of 381 participants, comprising 220 women (57.7.8%) and 161 men (42.3%), aged between 60 and 86 years (M = 67.33; SD = 5.08). The majority of participants lived in small towns with populations up to 100,000 (41.5%) or in larger cities with populations over 100,000 (40.2%), completed high school education (50.7%) and reported being married (63.8%). All participants were retired and not currently employed. Table 1 presents more detailed data.
 |
Table 1 Sociodemographic Characteristics in the Study Sample (N = 381) |
Study Tools
The Polish version of the Three-Dimensional Wisdom Scale (3D-WS) by Ardelt14 was used,76 consisting 39 items forming three main dimensions: cognitive, compassionate and reflective. The cognitive dimension (14 items) measures an individual’s ability to comprehensively understand life, including deeper meaning in intrapersonal and interpersonal phenomena and events. The compassionate dimension (13 items) corresponds to the individual’s capacity for positive emotions toward others, improving one’s well-being and overcoming egocentric tendencies. The reflective dimension (12 items) measures an individual’s ability to perceive reality objectively, practice self-distance, and view events from multiple perspectives. Answers are given on a 5-point scale. A composite three-dimensional wisdom score is generated by calculating the average of the three factors. In the current sample, the respective Cronbach’s alpha values were 0.77, 0.69, 0.80, and 0.88 for the overall result.
The Developmental Tasks Questionnaire for Seniors25 measures the general level of developmental task attainment in older people, as defined by Havighurst28,29 and Erikson’s30 general developmental theories. The instrument comprises 15 items, each rated on a 5-point Likert scale. It yields an overall score as well as three distinct categories: (1) acceptance of one’s life – demonstrating an accepting attitude toward one’s past and present experiences, and achieving positive life outcomes, (2) adaptation – adapting to typical age-related changes like physical decline, retirement, reduced income, and accepting help when needed, (3) acceptance of passing – reconciling with the reality of aging and death, for oneself and loved ones. The development and psychometric characteristics of the instrument have been previously detailed.25 The tool is a brief and reliable instrument designed to evaluate fundamental aspects of adjustment to old age. In the current study, the internal consistency was strong (Cronbach’s alpha = 0.87 for the total score, and for factors 0.85, 0.60 and 0.82, respectively).
Self-rated health was evaluated using the numeric version of the scale. This scale, created by the author, ranges from 1 to 10 and is commonly used in medical research due to its strong discriminatory ability and minimal language skill requirements.49,77,78 The measurement of self-rated health involved asking respondents the question, “In my opinion, my general health status is”, and providing response options ranging from 1 (very bad) to 10 (very good). Participants were instructed to select the point on the scale that best corresponded to their current state of health.
Geriatric Depression Scale (GDS) was used, in the Polish language 15-item form.79,80 In the measure, the respondent indicates the presence of depressive symptoms within the previous two weeks (Yes/No). The number of points obtained shows a lack of depressive symptoms (0–5 points) or a risk of depression (6–15 points). The tool demonstrated good internal consistency in the current study (Cronbach’s alpha was 0.88).
The eight-item Personal Wellbeing Index69 was used to measure satisfaction with various life spheres, including standard of living, health, life achievements, personal relationships, personal safety, community connectedness, future security, and religion and spirituality. Participants rate their level of satisfaction on an 11-point scale, ranging from 0 (indicating no satisfaction at all) to 10 (representing complete satisfaction). The total score is derived by computing the average from individual domains. The tool was examined across 26 countries, indicating good psychometric properties in the simple and short measurement of general life satisfaction. The Polish language version of the tool was employed in the study.81 The reliability of the tool was excellent in the current study (Cronbach’s alpha 0.89).
Sociodemographic status was evaluated using a questionnaire specifically designed for this study, which gathered data on sex (1=men, 2=woman), age (number of years), education level (1=primary, 2=basic vocational, 3=secondary, 4=higher), marital status (1=single, 2=married), place of living (1=village, 2=town with less than 100000 residents, 3=city with more than 100000 residents).
Statistical Analysis
A descriptive analysis was conducted by computing the means and standard deviations. The normality assumption was examined by assessing Shapiro–Wilk test, plots, histograms and the kurtosis and skewness. Scores of kurtosis and skewness close to zero indicate the normal distribution;82,83 however, the scores between −2 and +2 are considered acceptable in terms of the normality assumption.84 After calculating bivariate Pearson’s correlations, a linear multiple regression analysis was performed to examine the relationship between wisdom, developmental task attainment and self-rated health (independent variables), and depressive symptoms and wellbeing (outcome variables); the calculation was performed after controlling for sociodemographic factors. Statistical diagnostic analyses checked an absence of collinearity and heteroscedasticity, and distributions of residuals. The presence of outliers was detected using the Mahalanobis and Cook’s distance. The results were analyzed with SPSS Version 28.0. Additionally, the complex structure of relationships between variables was calculated using structural equation modeling (path analysis) in AMOS 28, using the maximum likelihood method. The path analyses aimed to assess both the direct and indirect effects of independent variables on the outcome variables.83 To determine the goodness of fit between data and model, a combination of different fit indices was used.83,85,86
After conducting a priori power analysis with G*Power 3.1 software,87 considering a medium effect size (alpha of 0.05, a standard power level of 0.95), the minimum sample size required was found to be 161. Additionally, the minimum sample size of 200 respondents for SEM, as suggested by Kenny86 and Kline,83 was also met.
Results
Descriptive statistics and correlation matrix for the variables in the study were computed (see Table 2).
 |
Table 2 Descriptive Statistics and Correlation Matrix for the Variables in the Study |
Results concerning the distribution of variables showed that the Shapiro–Wilk test yielded significant results, indicating non-normality. However, considering the sample size, plots and histograms of the factors, and the values of skewness and kurtosis (< |2|), it was assumed that all followed a normal distribution. The results indicate that general wisdom and all its dimensions, general level of developmental tasks achievement and all its dimensions as well as self-rated health level correlated negatively with depressive symptoms. Positive significant correlations were observed for those variables and personal wellbeing level.
The results of the multiple regression analysis with well-being and depressive symptoms as the outcome variables are presented in Table 3.
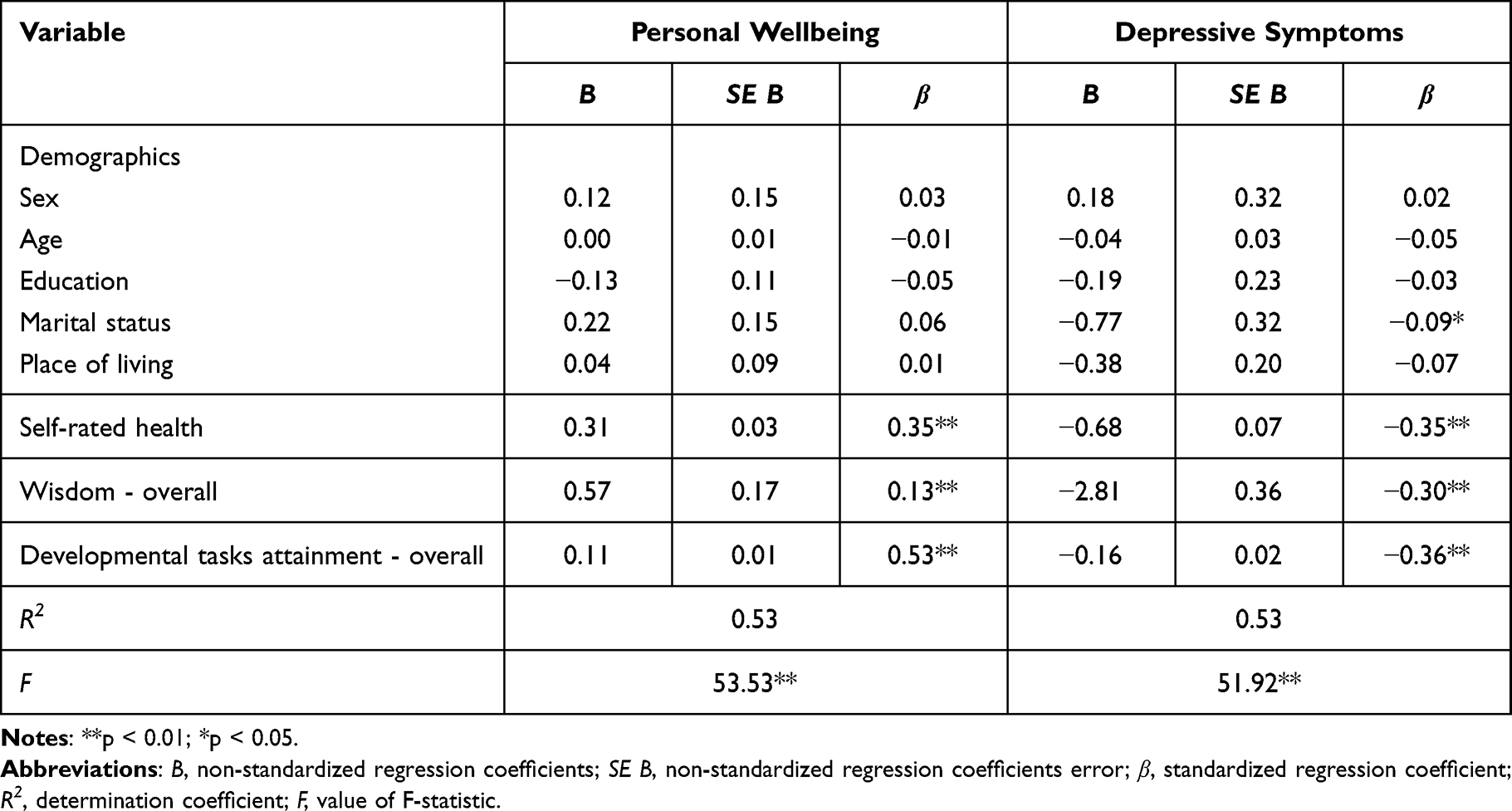 |
Table 3 Summary of the Multiple Regression Analysis for Variables Predicting Personal Wellbeing and Depressive Symtoms |
No evidence of multicollinearity was found based on the variance inflation factor (VIF ranged from 1.04 to 1.21), and tolerance (ranged from 0.81 to 0.96). The Durbin-Watson scores, ranging from 1.90 to 2.01, suggest the absence of autocorrelation in the residuals. The Mahalanobis and Cook’s distance excluded the presence of significant outliers.88
Regarding confounders, the results showed that the demographic variables included in the regression analyses, both for wellbeing and depressive symptoms, did not predict outcome variables in a significant way. For depressive symptoms, only a weakly significant relationship was observed for marital status. Self-rated health, overall level of wisdom and developmental task attainment were significant positive predictors for personal wellbeing and negative – for depressive symptoms. The model accounted for 53% of the variance in personal well-being and 53% of depressive symptoms.
Basing on the regression analysis results, the path analysis was performed to examine the structural relations between variables. The final model (see Figure 1) indicated good data–model fit statistics (χ2= 0.29; df= 1; p= 0.59; RMSEA= 0.095 [90% CI for RMSEA: 0.021–0.193],; NFI=0.993; CFI=0.995; GFI =0.995; AGFI=0.930; SRMR = 0.031). All standardized path coefficients of the model were statistically significant (p < 0.01). Wisdom (β=0.13, p<0.01), developmental tasks attainment (β=0.53, p<0.01) and subjectively perceived health (β=0.36, p<0.01) were found to directly positively influence personal wellbeing (R2=0.51, p<0.01). Moreover, wisdom (β=−.31, p<0.01), developmental tasks attainment (β=−.37, p<0.01) and self-rated health (β=−.36, p<0.01) were found to have a direct negative influence on depressive symptoms (R2=0.49, p<0.01). A negative significant correlation between personal wellbeing and depressive symptoms was also established (r=.-36, p<0.01). Wisdom was also positively related to developmental tasks attainment (β=0.31, p<0.01) and self-rated health (β=0.18, p<0.01).
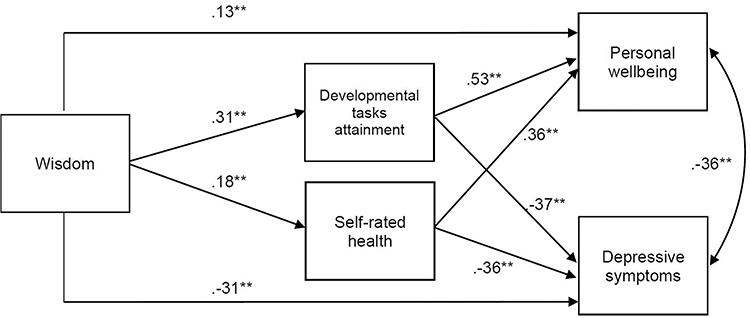 |
Figure 1 Results of Structural Equation Modelling. Note: **p <0.01. |
In addition, mediation analyses found wisdom to have a significant indirect effect on personal wellbeing and depression through developmental task attainment and self-rated health. The initial path from wisdom to depressive symptoms was reduced from β=−.49 to β=−.31 and from wisdom to personal wellbeing from β=0.36 to 0.13 (p<0.01). All total and direct effects of wisdom on personal wellbeing and on depression were significant (p<0.05). Therefore, it may be supported that there is a significant partial mediation in the effect of wisdom on mental health outcomes.
Discussion
The aim of the current study was to assess whether developmental task attainment and self-rated health might be another possible pathway between wisdom and mental health among retired older individuals in Poland. Both positive (personal wellbeing) and negative aspects (depressive symptoms) of mental health were assessed, as different pathways may affect distinct negative and positive mental health outcomes.66,67,70
As expected, wisdom, developmental task attainment and self-rated health were positively related to personal wellbeing and negatively to depressive symptoms, after controlling for sociodemographic variables (Hypothesis 1). Those results are consistent with prior studies indicating positive relationships between wisdom and subjective wellbeing and negative associations between wisdom and depressive symptoms.14,19–21,89 Chen and Wang20 suggest that a significant level of wisdom can play a crucial role in mitigating social alienation and loneliness among older adults, thereby serving as a protective factor against depression. In a study conducted by Etezadi and Pushkar18 on retirees, it was discovered that perceived control and life engagement played a mediating role in the relation between wisdom and negative and positive affect. The authors put forward the hypothesis that wisdom could facilitate engagement in meaningful activities. By actively selecting personally significant and enjoyable activities, individuals with higher levels of wisdom may be able to avoid circumstances that lead to unfavorable experiences. In the longitudinal study, Ardelt52 tried to answer the question whether personal wisdom, might be more likely to positively predict wellbeing, than the other way around. The study’s results supported this hypothesis, suggesting that developing three-dimensional wisdom may help to maintain or even improve subjective well-being.
Also, developmental task attainment in the late-life period and higher subjectively-perceived health are typical indicators of healthy and successful aging.3,9,28,42 Effectively adapting to deteriorating health, retirement phase with lower financial resources and evolving social roles, as well as reconciling with the loss of relatives and friends while also reflecting on one’s life, may strengthen wellbeing and prevent depressive symptoms. Havinghurst28 postulates that while maintaining a behavioral style consistent with earlier stages of life and pursuing personal plans and needs are crucial objectives in staying active, it is equally important to effectively cope with losses in retirement. Successfully navigating these challenges, along with subjective factors, lifestyle, health and social support, can form the foundation for aging well and adapting to old age.90,91
Self-rated health was also associated with mental health in the current study – positively with wellbeing, and negatively with depressive symptoms. Self-assessed health frequently aligns with objective health status,92 being strongly related to life satisfaction.53,54,56 Low self-rated health is also associated with higher numbers of depressive symptoms in old age.58–61 Experiencing physical health issues increases the likelihood of experiencing depression in older people and can contribute to its persistence over time.93 The old age is commonly marked by a deterioration in health, and other critical events such as retirement, the loss of a partner and a decline in independence can have an adverse impact on life satisfaction, potentially leading to depressed mood.94,95
Finally, the findings reveal that developmental task attainment and self-rated health partially mediated the relationship between wisdom and mental health outcomes (Hypothesis 2). While this relationship has not been explored to date, some studies have focused on similar areas of interest. Previous studies using structural equation modeling have shown that attainment of developmental tasks in old age plays a mediating role between personal resources, such as resiliency, and satisfaction with life.42 Dezutter et al90 indicate that Erikson’s developmental task of integrity versus despair mediates the relationship between a sense of coherence, depression, and life satisfaction. According to Brudek,96 life balance, measured as late-life developmental tasks from the perspective of Erikson’s theory, acts as the mediator between personality traits and the overall quality of life in older individuals. These results are supported by the present structural modeling equation data. The achievement of developmental tasks, including the establishment of life balance, acts as a partial mediator between wisdom and mental health.
Wiser older adults would more easily accept their past and present life and the inevitability of passing. In this process, a special role may be played by reflective wisdom, which refers to the ability to observe and perceive things, events, and oneself from different perspectives, engaging in introspection, mindful awareness and contemplation. This dimension of wisdom allows individuals to develop a profound understanding of themselves, others, and life as a whole. It also involves a gradual reduction of subjectivity, projections, and self-centeredness, while fostering the growth of tolerance and empathy towards others.
A positive association was observed between greater wisdom and subjective well-being (SWB), along with the finding that wisdom acted as a protective factor against the detrimental effect of unfavorable life events on present well-being.32 This indicates that wisdom is crucial in enhancing the ability to cope with the losses associated with aging. This results seem to correspond with predictive role of wisdom for developmental tasks attainment, such as adaptation to age-related loses, retirement and declining health, acceptance of passing and positive life outcome.
Wise older individuals have the capability and composure to handle adversity without compromising their overall sense of well-being. This is especially true for individuals who have acquired wisdom by successfully navigating past adversities.97 In a study conducted with terminally ill older patients, a considerably stronger correlation between wisdom and well-being was observed among nursing home and hospice residents compared to the community sample.35 Nursing home residency or the diagnosis of a terminal illness did not seem to have a significant impact on the well-being of wiser older patients. Wisdom appeared to compensate for the end-of-life losses.33 It may be assumed that wisdom stimulates wellbeing and prevents geriatric depression by enhancing developmental task accomplishment in later life. This is also corroborated by other results indicating negative relationships between wisdom and fear of death.14
Also, self-rated health acted as a partial mediator in the relationship between wisdom and mental health. According to previous research, wisdom also affects self-rated health in older adult samples.13,15,21 Wisdom can have a positive effect on physical health in older individuals, which can be caused by their greater likelihood of following a healthy lifestyle.52 Wisdom provides a deep understanding of life, which can lead to stress reduction and foster physical and mental health. Wise older adults may undertake health-promoting behavior by being aware of how their lifestyle influences health.23 A prior study found that both wisdom and subjective assessed physical health may have an impact on satisfaction with life; however, wisdom had the strongest influence on well-being and reduced the positive impact of physical health.15 One longitudinal study found the association between wisdom and self-rated health to be one-directional (i.e. the role of physical health on wisdom was not significant): older adults with greater wisdom not only experienced higher life satisfaction but also better overall health.13 It can also be postulated that wiser individuals demonstrate higher accuracy in assessing their health, which can affect the relationship between self-rated health and well-being.57
Other longitudinal studies13 indicated a positive association between wisdom and successful aging. Older individuals who scored higher on wisdom measures experienced greater satisfaction in their later years of life. Additionally, they exhibited better overall subjective health and stronger familial relationships than individuals with lower wisdom scores.19
The impact of self-assessed health on depressive symptoms can be understood through psychological mechanisms. Specifically, when individuals perceive a risk to their self-integrity due to health-related concerns, it can result in emotional stress. This includes an increased likelihood of experiencing negative affective outcomes.98 SRH may be related to mental health outcomes in bidirectional ways.9,62–64 However, a study conducted by Peleg and Nudelman59 found that self-assessed health had a greater longitudinal influence on depressive symptoms compared to the effect of depressive symptoms on SRH, especially among younger-older adults. The authors conclude that particular emphasis should be given to the impact of SRH on depressive symptoms in the years after retirement. This observation aligns with the idea that as individuals age, their health becomes increasingly significant in shaping their overall well-being.99 Consequently, lower SRH has a more pronounced effect on depressive symptoms during later stages of life.
Among the young-old age group, health-related changes tend to be more noticeable and impactful. This stage of life becomes a critical period for functional abilities and engagement in various activities.100 Individuals may place greater emphasis on their health due to the significant life challenges and losses they experience.101 The transition from the pre-retirement phase, where people typically enjoy relative health and are occupied with work, family, and social connections, to this new and more challenging stage can intensify health-related concerns. Additionally, the increased available time in this phase allows for more focus on these issues. Consequently, these factors can contribute to heightened negative emotions, including depressive symptoms.
It must also be noted that, in the current study, path analyses found positive and negative mental health outcomes found to be negatively associated with each other (r=−0.36, p<0.01). This result is consistent with previous findings examining similar variables in older adults.90 Taking action to address various aspects of life satisfaction can result in better mental well-being and reduced psychological distress in older individuals in the future.102
The structural model appears to show the complexity of the relationships between the determinants of mental health in old age. The novelty of the study is its main strength, insofar that it employs health and developmental variables to understand the wisdom-related aspects of healthy aging. The study results have valuable implications for enhancing health promotion policies targeting older adults. In Poland, where it is widely recognized the necessity to raise awareness of social and healthcare issues pertaining to the aging population, this is especially relevant.103 The research provides novel avenues for creating prevention-oriented initiatives by incorporating psychological and developmental factors as crucial goals for mental health promotion. While wisdom can be developed through training in human development and interventions,104,105 also developmental task attainment and healthy aging processes can also be effectively supported in late life.3,9,42,106 In order to successfully complete developmental tasks during retirement, it may be helpful to encourage people to reflect on challenging life experiences in a way that promotes a “wise” perspective on both the present and past experiences.107
However, it is important to acknowledge the limitations of this study. The research design is susceptible to selection bias, and the study itself is cross-sectional in nature. It relied on the use of computer-assisted-web-interview (CAWI) in a group of relatively healthy and well-educated retired volunteers from the community in Poland. In the study, quantitative self-reported measures were utilized, and self-rated health was assessed using a single item created by the author. Consequently, any causal relationships inferred from the findings should be interpreted cautiously, as well as any attempts to generalize the results to different populations or cultural settings. To gain a more comprehensive understanding, future research should explore additional factors related to mental health among older adults in diverse populations. Additionally, longitudinal studies would provide valuable insights into the changes and developments over time in this field.
Conclusion
This study contributes to our understanding of why wiser individuals tend to age well and has implications for social interventions aimed at promoting mental health among older adults. By identifying potential psychological mechanisms, this study broadens the scope of wisdom research and sheds light on the factors that may underlie the positive association between wisdom and mental health in later life.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Statement
The study protocol was approved by the Research Ethics Board at the University of Lodz.
Participants Consent Statement
All participants provided informed consent statement.
Funding
The study was funded by University of Lodz, as part of the increased by 2% subsidy for the universities participating in “The Excellence Initiative – Research University” competition (grant no. 106/2021).
Disclosure
The author reports no conflicts of interest in this work.
References
1. World Health Organization. World report on ageing and health; 2015. Available from: https://apps.who.int/iris/bitstream/handle/10665/186463/9789240694811_eng.pdf?sequence=1.
2. Wang H. Wisdom in healthy aging research: starting from measurement. Int Psychogeriatrics. 2022;34(7):593–596. doi:10.1017/S1041610222000540
3. Zadworna M. Healthy aging and the University of the Third Age – health behavior and subjective health outcomes in older adults. Arch Gerontol Geriatr. 2020;90:104126. doi:10.1016/j.archger.2020.104126
4. Kim ES, James P, Zevon ES, Trudel-Fitzgerald C, Kubzansky LD, Grodstein F. Optimism and healthy aging in women and men. Am J Epidemiol. 2019;188(6):1084–1091. doi:10.1093/AJE/KWZ056
5. Klusmann V, Gow AJ, Robert P, Oettingen G, Freund A. Using theories of behavior change to develop interventions for healthy aging. Journals Gerontol Ser B. 2021;76(Supplement_2):S191–S205. doi:10.1093/GERONB/GBAB111
6. Lu W, Pikhart H, Sacker A. Domains and measurements of healthy aging in epidemiological studies: a review. Gerontologist. 2019;59(4):e294–e310. doi:10.1093/geront/gny029
7. Peel NM, McClure RJ, Bartlett HP. Behavioral determinants of healthy aging. Am J Prev Med. 2005;28(3):298–304. doi:10.1016/j.amepre.2004.12.002
8. Sowa A, Tobiasz-Adamczyk B, Topór-Mądry R, Poscia A, Ignazio D, Milia L. Predictors of healthy ageing: public health policy targets. BMC Health Serv Res. 2016. doi:10.1186/s12913-016-1520-5
9. Zadworna M. Pathways to healthy aging – exploring the determinants of self-rated health in older adults. Acta Psychol. 2022;228. doi:10.1016/j.actpsy.2022.103651
10. Michel JP, Sadana R. “Healthy Aging” concepts and measures. J Am Med Dir Assoc. 2017;18(6):460–464. doi:10.1016/j.jamda.2017.03.008
11. Staudinger UM, Glück J. Psychological wisdom research: commonalities and differences in a growing field. Ann Rev Psychol. 2010;62(1):215–241. doi:10.1146/ANNUREV.PSYCH.121208.131659
12. Webster JD, Bohlmeijer ET, Westerhof GJ. Time to flourish: the relationship of temporal perspective to well-being and wisdom across adulthood. Aging Ment Heal. 2014;18(8):1046–1056. doi:10.1080/13607863.2014.908458
13. Ardelt M. Antecedents and effects of wisdom in old age: a longitudinal perspective on aging well. Res Aging. 2000;22(4):360–394. doi:10.1177/0164027500224003
14. Ardelt M. Empirical assessment of a three-dimensional wisdom scale. Res Aging. 2003;25(3):275–324. doi:10.1177/0164027503025003004
15. Ardelt M. Wisdom and life satisfaction in old age. Journals Gerontol Ser B. 1997;52(1):5–27. doi:10.1093/geronb/52B.1.P15
16. Zacher H, Staudinger UM. Wisdom and Well-Being. In: Diener E, Oishi S, Tay L, editors. Handbook of Well-Being. DEF Publishers; 2018:1–15.
17. Webster JD, Westerhof GJ, Bohlmeijer ET. Wisdom and mental health across the lifespan. Journals Gerontol Ser B. 2014;69(2):209–218. doi:10.1093/geronb/gbs121
18. Etezadi S, Pushkar D. Why are wise people happier? An explanatory model of wisdom and emotional well-being in older adults. J Happiness Stud. 2013;14(3):929–950. doi:10.1007/s10902-012-9362-2
19. Ardelt M, Jeste DV. Wisdom as a resiliency factor for subjective well-being in later life. Psychosoz und Medizinische Rehabil. 2022;118:13–28.
20. Chen H, Wang F. Wisdom in old age. Adv Psychol Sci. 2021;29(5):885–893. doi:10.3724/sp.j.1042.2021.00885
21. Mikaeili N, Hedayat S. Depression in the elderly: investigating the role of self-compassion and wisdom. Knowl Res Appl Psychol. 2020;21(2):54–63. doi:10.30486/jsrp.2019.1865286.1770
22. Roháriková V, Špajdel M, Cviková V, Jagla F. Tracing the relationship between wisdom and health. Act Nerv Super Rediviva. 2013;55(3):95–102.
23. Ardelt M, Ferrari M. Effects of wisdom and religiosity on subjective well-being in old age and young adulthood: exploring the pathways through mastery and purpose in life. Int Psychogeriatrics. 2019;31(04):477–489. doi:10.1017/S1041610218001680
24. Ardelt M. How wise people cope with crises and obstacles in life. ReVision. 2005;28(1):7–19. doi:10.3200/REVN.28.1.7-19
25. Zadworna-Cieślak M. Psychometric properties of the developmental tasks questionnaire for seniors. Curr Psychol. 2020;39(4):1172–1180. doi:10.1007/s12144-019-00380-0
26. Zauszniewski JA, Martin MH. Developmental task achievement and learned resourcefulness in healthy older adults. Arch Psychiatr Nurs. 1999;13(1):41–47. doi:10.1016/S0883-9417(99)80016-8
27. Hutteman R, Hennecke M, Orth U, Reitz AK, Specht J. Developmental Tasks as a Framework to Study Personality Development in Adulthood and Old Age. Eur J Pers. 2014;28(3):267–278. doi:10.1002/per.1959
28. Havighurst RJ. Successful Aging. Gerontologist. 1961;1(1):8–13. doi:10.1093/geront/1.1.8
29. Havighurst RJ. Developmental Tasks and Education. Addison-Wesley Longman; 1972.
30. Erikson E. The Life Cycle Completed. New York: Norton; 1982.
31. Erikson EH. Insight and Responsibility: Lectures on the Ethical Implications of Psychoanalytic Insight. New York, NY, US: W W Norton & Co; 1964.
32. Ardelt M, Jeste DV. Wisdom and hard times: the ameliorating effect of wisdom on the negative association between adverse life events and well-being. Journals Gerontol Ser B. 2018;73(8):1374–1383. doi:10.1093/geronb/gbw137
33. Baltes PB, Freund AM. The intermarriage of wisdom and selective optimization with compensation: two meta-heuristics guiding the conduct of life. In: Keyes CLM, Haidt J, editors. Flourishing: Positive Psychology and the Life Well-Lived. Washington, DC, US: American Psychological Association; 2003:249–273. doi:10.1037/10594-011
34. Choi NG, Landeros C. Wisdom from life’s challenges: qualitative interviews with low- and moderate-income older adults who were nominated as being wise. J Gerontol Soc Work. 2011;54(6):592–614. doi:10.1080/01634372.2011.585438
35. Ardelt M, Edwards CA. Wisdom at the end of life: an analysis of mediating and moderating relations between wisdom and subjective well-being. Journals Gerontol Ser B. 2016;71(3):502–513. doi:10.1093/geronb/gbv051
36. Clémence A, Karmaniola A, Green EGT, Spini D. Disturbing life events and wellbeing after 80 years of age: a longitudinal comparison of survivors and the deceased over five years. Ageing Soc. 2007;27(2):195–213. doi:10.1017/S0144686X06005630
37. Finogenow M, Zadworna-Cieślak M. Wydarzenia krytyczne w okresie późnej dorosłości [Critical life events in late adulthood]. Przedsiebiorczosc i Zarzadzanie. 2013;14(5):97–115.
38. James JB, Matz-Costa C, Smyer MA. Retirement security: it’s not just about the money. Am Psychol. 2016;71(4):334–344. doi:10.1037/A0040220
39. Grünwald O, Damman M, Henkens K. Does retirement change what individuals value in life? Results from a 3-year panel study. Journals Gerontol Ser B. 2022;77(9):1699–1709. doi:10.1093/GERONB/GBAC014
40. Fisher GG, Chaffee DS, Sonnega A. Retirement timing: a review and recommendations for future research. Work Aging Retire. 2016;2(2):230–261. doi:10.1093/WORKAR/WAW001
41. Denton FT, Spencer BG. What is retirement? A review and assessment of alternative concepts and measures. Can J Aging. 2009;28(1):63–76. doi:10.1017/S0714980809090047
42. Zadworna-Cieślak M, Ogińska-Bulik N. Satisfaction with life in old age – the role of developmental tasks attainment and resiliency. Educ Stud Rev. 2019;1(28):23–35. doi:10.12775/pbe.2019.002
43. Reed PG, Boyd M, Buckwalter KC. Mental health of older adults. West J Nurs Res. 1989;11(2):143–163. doi:10.1177/019394598901100202/ASSET/019394598901100202.FP.PNG_V03
44. Bryant LL, Beck A, Fairclough DL. Factors that contribute to positive perceived health in an older population. J Aging Health. 2000;12(2):169–192. doi:10.1177/089826430001200202
45. Wuorela M, Lavonius S, Salminen M, Vahlberg T, Viitanen M, Viikari L. Self-rated health and objective health status as predictors of all-cause mortality among older people: a prospective study with a 5-, 10-, and 27-year follow-up. BMC Geriatr. 2020;20(1). doi:10.1186/s12877-020-01516-9
46. Lyyra TM, Leskinen E, Jylhä M, Heikkinen E. Self-rated health and mortality in older men and women: a time-dependent covariate analysis. Arch Gerontol Geriatr. 2009;48(1):14–18. doi:10.1016/j.archger.2007.09.004
47. Kusumastuti S, Gerds TA, Lund R, Mortensen EL, Westendorp RGJ. Discrimination ability of comorbidity, frailty, and subjective health to predict mortality in community-dwelling older people: population based prospective cohort study. Eur J Intern Med. 2017;42:29–38. doi:10.1016/j.ejim.2017.05.016
48. Meng Q, Xie Z, Zhang T. A single-item self-rated health measure correlates with objective health status in the elderly: a survey in suburban Beijing. Front Public Heal. 2014;2:27. doi:10.3389/fpubh.2014.00027
49. Szybalska A, Broczek K, Puzianowska-Kuznicka M, et al. Self-rated health and its association with all-cause mortality of older adults in Poland: the PolSenior project. Arch Gerontol Geriatr. 2018;79:13–20. doi:10.1016/j.archger.2018.07.016
50. Christian LM, Glaser R, Porter K, Malarkey WB, Beversdorf D, Kiecolt-Glaser JK. Poorer self-rated health is associated with elevated inflammatory markers among older adults. Psychoneuroendocrinology. 2011;36(10):1495–1504. doi:10.1016/j.psyneuen.2011.04.003
51. Eriksson I, Undén A-L-L, Elofsson S. Self-rated health. Comparisons between three different measures. Results from a population study. Int J Epidemiol. 2001;30(2):326–333. doi:10.1093/ije/30.2.326
52. Ardelt M. Disentangling the relations between wisdom and different types of well-being in old age: findings from a short-term longitudinal study. J Happiness Stud. 2016;17(5):1963–1984. doi:10.1007/S10902-015-9680-2/TABLES/3
53. Puvill T, Lindenberg J, de Craen AJM, Slaets JPJ, Westendorp RGJ. Impact of physical and mental health on life satisfaction in old age: a population based observational study. BMC Geriatr. 2016;16(1):194. doi:10.1186/s12877-016-0365-4
54. Borim FSA, Neri AL, Francisco PMSB, de Azevedo Barros MB, Barros MB, de Ade A. Dimensions of self-rated health in older adults. Rev Saude Publica. 2014;48(5):714–722. doi:10.1590/S0034-8910.2014048005243
55. Smith JL, Bryant FB. The benefits of savoring life: savoring as a moderator of the relationship between health and life satisfaction in older adults. Int J Aging Hum Dev. 2016;84(1):3–23. doi:10.1177/0091415016669146
56. Tavares AI. Health and life satisfaction factors of Portuguese older adults. Arch Gerontol Geriatr. 2022;99:104600. doi:10.1016/j.archger.2021.104600
57. Bak W, Dutkiewicz D, Brudek P. Relationship between self-assessed health and life satisfaction in older adults: the moderating role of ego-resiliency. Ageing Soc. 2021. doi:10.1017/S0144686X21001689
58. Mulsant BH, Ganguli M, Seaberg EC. The relationship between self-rated health and depressive symptoms in an epidemiological sample of community-dwelling older adults. J Am Geriatr Soc. 1997;45(8):954–958. doi:10.1111/j.1532-5415.1997.tb02966.x
59. Peleg S, Nudelman G. Associations between self-rated health and depressive symptoms among older adults: does age matter? Soc Sci Med. 2021;280:114024. doi:10.1016/j.socscimed.2021.114024
60. Ambresin G, Chondros P, Dowrick C, Herrman H, Gunn JM. Self-rated health and long-term prognosis of depression. Ann Fam Med. 2014;12(1):57–65. doi:10.1370/afm.1562
61. Kosloski K, Stull DE, Kercher K, Van Dussen DJ. Longitudinal analysis of the reciprocal effects of self-assessed global health and depressive symptoms. Journals Gerontol Ser B. 2005;60(6). doi:10.1093/geronb/60.6.P296
62. Siahpush M, Spittal M, Singh GK. Happiness and life satisfaction prospectively predict self-rated health, physical health, and the presence of limiting, long-term health conditions. Am J Heal Promot. 2008;23(1):18–26. doi:10.4278/ajhp.061023137
63. Kim ES, Delaney SW, Tay L, Chen Y, Diener E, Vanderweele TJ. Life satisfaction and subsequent physical, behavioral, and psychosocial health in older adults. Milbank Q. 2021;99(1):209–239. doi:10.1111/1468-0009.12497
64. Han B. Depressive symptoms and self-rated health in community-dwelling older adults: a longitudinal study. J Am Geriatr Soc. 2002;50(9):1549–1556. doi:10.1046/j.1532-5415.2002.50411.x
65. Okabayashi H, Liang J, Krause N, Akiyama H, Sugisawa H. Mental health among older adults in Japan: do sources of social support and negative interaction make a difference? Soc Sci Med. 2004;59(11):2259–2270. doi:10.1016/J.SOCSCIMED.2004.02.024
66. Goodwin TC, Williams GA. Testing the roles of perceived control, optimism, and gratitude in the relationship between general/personal belief in a just world and wellbeing/depression. Soc Justice Res. 2023;36(1):40–74. doi:10.1007/S11211-023-00405-X
67. Elliot AJ, Mooney CJ, Douthit KZ, Lynch MF. Predictors of older adults’ technology use and its relationship to depressive symptoms and well-being. Journals Gerontol Ser B. 2014;69(5):667–677. doi:10.1093/GERONB/GBT109
68. Diener E, Oishi S, Lucas RE, Subjective well-being: the science of happiness and life satisfaction. In: Lopez SJ, Snyder CR, editors. The Oxford Handbook of Positive Psychology.
69. Cummins RA, Eckersley R, Pallant J, Van Vugt J, Misajon R. Developing a national index of subjective wellbeing: the Australian Unity Wellbeing Index. Soc Indic Res. 2003;64(2):159–190. doi:10.1023/A:1024704320683/METRICS
70. Diehl M, Hay EL, Berg KM. The ratio between positive and negative affect and flourishing mental health across adulthood. Aging Ment Heal. 2011;15(7):882–893. doi:10.1080/13607863.2011.569488
71. Kercher K. Assessing subjective well-being in the old-old: the PANAS as a measure of orthogonal dimensions of positive and negative affect. Res Aging. 1992;14(2):131–168. doi:10.1177/0164027592142001
72. Beekman ATF, Penninx BWJH, Deeg DJH, de Beurs E, Geerlings SW, Tilburg WV. Tilburg W van. The impact of depression on the well-being, disability and use of services in older adults: a longitudinal perspective. Acta Psychiatr Scand. 2002;105(1):20–27. doi:10.1034/J.1600-0447.2002.10078.X
73. Collins AL, Glei DA, Goldman N. The role of life satisfaction and depressive symptoms in all-cause mortality. Psychol Aging. 2009;24(3):696–702. doi:10.1037/a0016777
74. Zadworna-Cieślak M. Spirituality, satisfaction with life and health-related behavior of older residents of long-term care institutions—a pilot study. Explore. 2020;16(2):123–129. doi:10.1016/j.explore.2019.07.016
75. World Medical Association. World Medical Association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
76. Steuden S, Brudek P, Izdebski P. A Polish adaptation of Monika Ardelt’s Three-Dimensional Wisdom Scale (3D-WS). Ann Psychol. 2016;19(4):769–792. doi:10.18290/RPSYCH.2016.19.4-4EN
77. Hjermstad MJ, Fayers PM, Haugen DF, et al. Studies comparing numerical rating scales, verbal rating scales, and visual analogue scales for assessment of pain intensity in adults: a systematic literature review. J Pain Symptom Manage. 2011;41(6):1073–1093. doi:10.1016/J.JPAINSYMMAN.2010.08.016
78. Wierucki Ł, Kujawska-Danecka H, Mossakowska M, et al. Health status and its socio-economic covariates in the older population in Poland – the assumptions and methods of the nationwide, cross-sectional PolSenior2 survey. Arch Med Sci. 2020;18(1):92–102. doi:10.5114/AOMS.2020.100898
79. Albiński R, Kleszczewska-Albińska A, Bedyńska S; Geriatryczna Skala Depresji (GDS). Trafność i rzetelność różnych wersji tego narzȩdzia - Przegld badań [Geriatric Depression Scale (GDS). Validity and reliability of different versions of the scale – review]. Psychiatr Pol. 2011;45(4):555–562.
80. Yesavage JA, Brink TL, Rose TL, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. 1982;17(1):37–49. doi:10.1016/0022-3956(82)90033-4
81. Żemojtel-Piotrowska M, Piotrowski JP, Cieciuch J, et al. Measurement invariance of Personal Well-Being Index (PWI-8) Across 26 countries. J Happiness Stud. 2017;18(6):1697–1711. doi:10.1007/s10902-016-9795-0
82. Tabachnick BG, Fidell LS. Using Multivariate Statistics. Pearson; 2019.
83. Kline R. Principles and Practice of Structural Equation Modelling.
84. George D, Mallery P. IBM SPSS Statistics 26 Step by Step. Routledge; 2019; doi:10.4324/9780429056765
85. Hooper D, Coughlan J, Mullen M. Structural equation modelling: guidelines for determining model structural equation modelling: guidelines for determining model fit fit. Electron J Bus Res Methods. 2008;6(1):53–60. doi:10.21427/D7CF7R
86. Kenny D. Measuring model fit; 2020. Available from: http://davidakenny.net/cm/fit.htm.
87. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/BF03193146
88. Field A. Discovering Statistics Using SPSS.
89. Bergsma A, Ardelt M. Self-reported wisdom and happiness: an empirical investigation. J Happiness Stud. 2012;13(3):481–499. doi:10.1007/s10902-011-9275-5
90. Dezutter J, Wiesmann U, Apers S, Luyckx K. Sense of coherence, depressive feelings and life satisfaction in older persons: a closer look at the role of integrity and despair. Aging Ment Heal. 2013;17(7):839–843. doi:10.1080/13607863.2013.792780
91. Westerhof GJ, Bohlmeijer ET, McAdams DP. The relation of ego integrity and despair to personality traits and mental health. J Gerontol B Psychol Sci Soc Sci. 2017;72(3):400–407. doi:10.1093/geronb/gbv062
92. Wu S, Wang R, Zhao Y, et al. The relationship between self-rated health and objective health status: a population-based study. BMC Public Health. 2013;13(1):320. doi:10.1186/1471-2458-13-320
93. Geerlings SW, Beekman ATF, Deeg DJH, Van Tilburg W. Physical health and the onset and persistence of depression in older adults: an eight-wave prospective community-based study. Psychol Med. 2000;30(2):369–380. doi:10.1017/S0033291799001890
94. Wilkinson P, Ruane C, Tempest K. Depression in older adults. BMJ. 2018;363. doi:10.1136/BMJ.K4922
95. Dang L, Ananthasubramaniam A, Mezuk B. Spotlight on the challenges of depression following retirement and opportunities for interventions. Clin Interv Aging. 2022;17:1037–1056. doi:10.2147/CIA.S336301
96. Brudek P. Mediacyjna rola bilansu życiowego w związkach cech osobowości i jakości życia osób starszych [The mediating role of life review in the relations between personality traits and life satisfaction among elderly people]. Gerontol Pol. 2017;2017:168–175.
97. Linley PA. Positive adaptation to trauma: wisdom as both process and outcome. J Trauma Stress. 2003;16(6):601–610. doi:10.1023/B:JOTS.0000004086.64509.09
98. Cohen GL, Sherman DK. The psychology of change: self-affirmation and social psychological intervention. Ann Rev Psychol. 2014;65(1):333–371. doi:10.1146/annurev-psych-010213-115137
99. Schüz B, Wurm S, Warner LM, Wolff JK, Schwarzer R. Health motives and health behaviour self-regulation in older adults. J Behav Med. 2014;37(3):491–500. doi:10.1007/s10865-013-9504-y
100. Schindler I, Staudinger UM, Nesselroade JR. Development and structural dynamics of personal life investment in old age. Psychol Aging. 2006;21(4):737–753. doi:10.1037/0882-7974.21.4.737
101. Alpass FM, Neville S. Loneliness, health and depression in older males. Aging Ment Heal. 2003;7(3):212–216. doi:10.1080/1360786031000101193
102. Nakamura JS, Delaney SW, Diener E, VanderWeele TJ, Kim ES. Are all domains of life satisfaction equal? Differential associations with health and well-being in older adults. Qual Life Res. 2022;31(4):1043–1056. doi:10.1007/S11136-021-02977-0/TABLES/3
103. Arsenijevic J, Groot W. Health promotion policies for elderly—Some comparisons across Germany, Italy, the Netherlands and Poland. Health Policy. 2020;126(1):69–73. doi:10.1016/J.HEALTHPOL.2020.01.013
104. Sternberg RJ. Wisdom, foolishness, and toxicity in human development. Res Hum Dev. 2018;15(3–4):200–210. doi:10.1080/15427609.2018.1491216
105. Lee EE, Bangen KJ, Avanzino JA, et al. Outcomes of randomized clinical trials of interventions to enhance social, emotional, and spiritual components of wisdom: a systematic review and meta-analysis. JAMA Psychiatry. 2020;77(9):925–935. doi:10.1001/JAMAPSYCHIATRY.2020.0821
106. Urbaniak B, Chałas M, Szukalski P, et al. Trwałość i Zmienność Procesów Starzenia Się i Starości [Durability and variability of aging processes and old age]. Wydawnictwo Uniwersytetu Łódzkiego; 2021.
107. Kadri A, Leddy A, Gracey F, Laidlaw K. Wisdom enhancement and life skills to augment CBT outcomes for depression in later life: a series of N-of-1 trials. Behav Cogn Psychother. 2022;50(5):508–527. doi:10.1017/S1352465822000224
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.