")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Lived Experience of People with Type 1 Diabetes in North East Ethiopia; Psycho-Social and Economical Perspective, a Phenomenological Study
Authors Ketema Bogale E , Getachew Desalew E , Tesfa H , Endeshaw D , Guadie Tiruneh M , Ketema Bogale S
Received 24 September 2023
Accepted for publication 28 November 2023
Published 30 November 2023 Volume 2023:16 Pages 3885—3898
DOI https://doi.org/10.2147/DMSO.S431914
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Eyob Ketema Bogale,1 Eyob Getachew Desalew,2 Hiwot Tesfa,3 Destaw Endeshaw,4 Misganaw Guadie Tiruneh,5 Solomon Ketema Bogale6
1Health Promotion and Behavioral Science Department, School of Public Health, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia; 2Health Promotion and Communication Department, School of Public Health, College of Medicine and Health Sciences, Gondar University, Gondar, Ethiopia; 3Public Health Department, Injibara University, Injibara, Ethiopia; 4Department of Adult Health Nursing, School of Health Sciences, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia; 5Department of Health Systems and Policy, Institute of Public Health, University of Gondar, Gondar, Ethiopia; 6Antsokia District Health Office, North Shoa, Debre Birhan, Ethiopia
Correspondence: Eyob Ketema Bogale, Email [email protected]
Objective: To explore lived experience of people with type 1 diabetes in North East Ethiopia; psycho-social and economical perspective.
Methods: A descriptive phenomenological study was conducted to explore the lived experience of people with type 1 diabetes in North East Ethiopia; psycho-social and economical perspective from March 02 to March 25, 2020. A heterogeneous purposive sample method was used to choose the participants. The lead investigator used an in-depth interview to collect data, using an audio recorder and an interview guide. The data were analysed using the thematic analysis method. Atlas. ti software version 7 was used to facilitate the data analysis process.
Results: A total of 13 participants were enrolled in this study. The participants age range were 14 to 70 years and their duration of diabetes since diagnosis were from 8 months to 16 years. The three interconnected themes that emerged from the analysis are: (1) psychological experience with two sub-themes (psychological problems due to diabetes including fear and coping strategies for psychological problems), (2) social experience, which has five categories (influence on intimate relationships, influence on social participation, disclosure status, social isolation and stigma, social support, and influence on education); and (3) economic experience.
Conclusion: Fear was one of the psychological experiences felt by people with type 1 diabetes. Although type 1 diabetes is a biomedical problem, it is also accompanied by other psychological and socio-economic issues, that require a holistic approach to address it. So, health professionals should strengthen health information dissemination programs.
Keywords: lived experience, psychological, socio-economical, type 1 DM, Kemissie General Hospital, Ethiopia
Background
Diabetes is a group of metabolic diseases characterized by hyperglycemia resulting from defects in insulin secretion, insulin action, or both. It is one of the most frequent non-communicable diseases (NCDs) with a growing incidence worldwide is diabetes. Type 1 diabetes mellitus (T1DM), type 2 diabetes mellitus (T2DM), and gestational diabetes are the three main classifications.1
Type 1 diabetes mellitus results from β-cell destruction due to immune mediated or idiopathic, causing absolute insulin deficiency. It is managed in Ethiopia as pharmacologic management including monitoring of blood glucose through insulin injection, and non pharmacologic treatment including self-blood glucose monitoring, physical exercise, follow healthy diet, medication adherence and foot care.2
If blood glucose levels are not sufficiently controlled, the known challenges of people with type 1 diabetes include acute complication such as hypoglycemia, diabetic ketoacidosis, and hyperosmolar hyperglycaemic state are and the long-term complications include micro vascular (nephropathy, retinopathy, and neuropathy) and macro vascular (stroke, myocardial infarction, and coronary artery disease).1
Type 1 diabetes mellitus occurs at any age although it is commonly diagnosed in children and adolescents, which represents around 5–10% of all diabetes cases.3 Although it affects children and adolescents, 42% of type 1 diabetes mellitus cases occur after the age of 30 according to studies from the UK Biobank.4
Patients’ perceptions of their diabetes and their ability to modify their self-care habits over time to match their circumstances are coloured by their lived experiences with the disease. The social framework in which patients’ lived experiences situate medication adherence affects what they deprioritize or prioritise self-care actions in the context of their daily lives.5
Hence, diabetes is a new life experience for the individual. How the individual perceives the disease, the meaning of the disease, treatment compliance, and psychosocial difficulties are some of the issues that need to be addressed. Mental, emotional, social, and psychosexual problems and conflicts arise because this is a lifelong disease and requires a continuously controlled lifestyle.6
According to international Diabetes Federation (IDF) 2021 report, the estimated prevalence of T1DM among children and adolescents is 12.12% in worldwide, 4.5% in South Africa, and 2.4% in Ethiopia.7 According to WHO predictions, over 70% of all fatalities worldwide would be attributable to NCDs by 2025, with 85% of these deaths taking place in developing nations.1 Diabetes was one of the top causes of non-communicable disease fatalities in 2015, accounting for 1.5 million deaths worldwide8 and 321,100 deaths across the continent of Africa.9 Type 1 diabetics have a 20-year reduction in average life expectancy.10
Type 1 diabetes mellitus is a complex disease, and managing it can be difficult in terms of social, emotional, and financial decisions. Several aspects of quality of life were suboptimal in both people living with type 1 diabetes mellitus and their families, such as stigmatisation, short life expectancy due to a poor health care system, low socioeconomic status, health problems (co-morbidity, physical, cognitive, and emotional), and poor social participation.11
Patients with type 1 diabetes mellitus had higher rates of unemployment, more sick days, and a slightly lower level of education.12 Particularly in low- and middle-income countries where diabetes is frequently associated by other diseases, it has broad socioeconomic effects and undermines national productivity and economies.1
According to IDF report, in 2021 diabetes costs 966 billion USD dollars in worldwide, 7200.8 million USD dollars in South Africa and 200.2 million USD dollars in Ethiopia.7 By 2030, the costs of diabetes will reach 1.03 trillion USD dollars in worldwide, 8632.2 million USD dollars in South Africa and 281.2 million USD dollars in Ethiopia.7
Ethiopia is currently facing challenges from the rising prevalence of chronic NCDs including diabetes.9 Diabetes problems are frequently brought on in Ethiopia by non-adherence, a negative attitude towards the condition, a poor diet, and physical inactivity.13
Until now, in 2023, quantitative studies on type 1 DM in Ethiopia have been conducted.14–16 However, there is a scarcity of published qualitative literature and a limited understanding about the psychological and socio-economical experiences of people with type 1 diabetes in Ethiopia.
This phenomenological study’s aim was to explore the psychological and socio-economical experiences of type 1 DM patients to fill the previously indicated gap in the area. Additionally, it was intended to giving type 1 DM patients a voice to express their individual experiences, to better comprehend the essence of what it means to live with type 1 diabetes and describe their lived experience.
Methodology
Approach and Setting
From March 2 to March 25, 2020, a descriptive phenomenological study was carried out. Phenomenological research is a qualitative research methodology that aids in portraying the lived experiences of an individual. The phenomenological approach concentrates on examining the phenomena that have affected a person. Phenomenological research is a potent tool for comprehending subjective perceptions. Because it emphasizes giving meaning to events while they are being lived, we use the hermeneutic branch of phenomenology.17 The phenomenological approach was thus deemed appropriate for this study.
The study was carried out at Kemisse General Hospital, which is in the Amhara area of Ethiopia, 325 kilometers from Addis Ababa, the country’s capital city. The hospital provides an outpatient follow-up department (OPD) for chronic diseases, including hypertension and diabetes. According to data from Kemisse General Hospital’s OPD registration, there are 217 diabetic patients, 63 of them have type 1 DM.
Inclusion Criteria
People with type 1 diabetes who had been getting care in the study clinic for at least six months following their diagnosis eligible as participants in the study.
Exclusion Criteria:
- Seriously ill people with type 1 diabetes who are unable to communicate at the time of data collection.
- Children less than 12 years old since this is qualitative study which need in depth interview for data collection process in whom children less than 12 years old considered to be not giving adequate information.
Study Participants
We recruited a total of 13 type 1 diabetes mellitus patients from Kemisse General Hospital. Patients who met the study’s inclusion criteria were identified with the aid of the healthcare professionals at Kemisse General Hospital’s follow-up clinics and admitting wards. When the participant agreed to take part in the study, a meeting was planned for a time and day that suited for the individual being interviewed.
The participants were identified through the use of a purposive sampling technique. Age, sex, marital status, and duration of diagnosis and follow-up were taken into account to retain the participants’ diverse traits. The participant’s age category comprises adolescents (14 years through 17 years), adults (18 years or older), and older adults (65 and older). The authors considered age variety during data collection, and analysis and used quotes as supportive evidence from each age category of participants. This was done in order to be able to view many different aspects of type 1 diabetic patients’ living experiences from different points of view.
Data Collection
Data were collected by the first author using a semi-structured, in-depth interview guide (Supplementary File). The interview guide contains eight socio demographic question and 10 lived experience (psycho - social and economical perspective) related questions. First of all, we made a list of the heterogeneous characteristics that our study participants should have. Then we Identified and sampled every person with type 1 diabetes who meets the sample criteria. The nurses and doctors who are working in the admission ward and follow up clinics at Kemissie General Hospital helped in identifying patients that fulfill the inclusion criteria of the study.
After giving consent, all of the interviews carried out in Amharic language. Between 40 and 60 minutes were spent on each interview. The collection of data was carried out until saturation was attained in each heterogeneous category. Data saturation was attained when all questions were answered, responses were completed and no further new information was obtained from many participants. In this study, the total sample size was 13, the data saturation was achieved in eleventh interview and the additional two interviews were conducted for confirmation of data saturation.
Recall bias may be introduced at the time of the in-depth interview due to the chronic nature of the disease. To minimise recall bias, we used probing, which leads to more clarity on interview questions, and furthermore, by following an ordered sequence of events, backwards recall can help with memory recall. Start in the present and consider a specific moment in the past.
Rigor and Trustworthiness of the Study
This study was trustworthy based on Lincoln and Guba’s criteria of dependability, credibility, transferability and confirmability.17
Dependability
It is the assessment of the data collection and data analysis process. Dependability was attained through accurate documentation including all documents in the final report such as including the notes were taken during the interview and ensure that the details of the procedures were described to allow the readers to see the basis upon which conclusions was made18 each of which was considered at all times.
Credibility
It means ensuring the results are believable, consistent with reality and that the interpretations are true.17 Credibility was assured by keeping the consistency of procedures and the neutrality of the investigator about findings or decisions. Data collection sessions involved only those who are voluntary to participate and to offer data freely. Probing was employed during data collection process in order to dig contextual rich data. We also invited seven participants to review the ideas for transcription verification, which they think the investigator would provide us the reality from the participant point of view.
Transferability
It means showing that the findings have applicability in other contexts.17 To allow judgments about transferability by the reader appropriate probes had been used to obtain detailed information on responses. Data analysis, interpretations, and conclusions were continuously peer-debriefed by health promotion experts.
Confirmability
It is a measure of how well the study’s discoveries are supported by the data collected and reflects the objectivity of the data. This means that the researcher’s bias should not alter the result.17 Confirmability of the study was ensured by the recording of every activity of the participants during the time of the interview. In addition, the audio-taped interviews were not destroyed until publication process completed which can enable others to track the process. Moreover, peer debriefing also ensured confirmability. It was also achieved by using quotes which means linking the words of the participants with the discoveries.17
Ethics Approval and Consent to Participate
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and Bahir Dar University College of Medicine and Health Sciences’ Instructional Review Board (IRB) granted ethical approval under the reference number CHMS 215/2020. Caretakers of participants under the age of 18 were requested for their agreement and consent for their child’s participation. Permission was obtained at all levels to conduct the investigation. During the permission process, carers received thorough explanations of the study’s objectives, data gathering methods, potential hazards, discomforts, and advantages of participating. All guardians of study participants’ children provided written informed permission. The families in this instance were portrayed as guardians. Only when the guardians agreed with the youngster were they allowed to participate in the study. A child’s option not to participate in the study was honoured even without their guardians’ agreement.
Participants who could not read or write had their consent forms read to them by the data collector, so they were aware of all the terms.Prior to the start of data collection, each study participant provided written informed consent. Data collecting procedures used codes rather than participant names to ensure the confidentiality of the information collected from study participants.In addition, participants provided signed informed agreement to share their data anonymously for scientific research only.
Data Analysis
After data collection, the first lead author transcribed the audio-recorded data in the participant’s local language in Amharic, then back-translated to English by the second author, and the other authors verified the accuracy of the translated data independently. The data were analysed using the thematic analysis method. The six thematic analysis steps were followed to analyze the data such as; step 1: become familiar with the data, step 2: generate initial codes, step 3: search for categories, Step 4: search for sub-themes and themes, step 5: review and define themes and step 6: report writing.19
In step 1, the principal investigator hears the audio-recorded data repeatedly, reads and rereads the transcribed data multiple times to maintain a sense of integrity and comprehend the significance of the experiences from the participant’s perspective. In step 2 and 3, the first and second authors assigned a code to each meaning unit that represented its content, and then related codes were grouped together into categories. The analysis of data was facilitated by the usage of Atlas.ti software version 7. In step 4 and 5, final categories, sub-themes and themes were developed after peer review and verification by the co-lead author. Finally in step 6, in order to present the study’s findings, the report was produced using categories and emerged themes. Quotes were utilised to draw attention to each category and demonstrate how it relates to each theme.
Results
Characteristics of the Study Participant: Thirteen in-depth interviews were done at all. There were 13 respondents, and 8 of them were males, and 2 were divorced. Concerning their educational backgrounds, five participants could not read and write. (See Table 1).
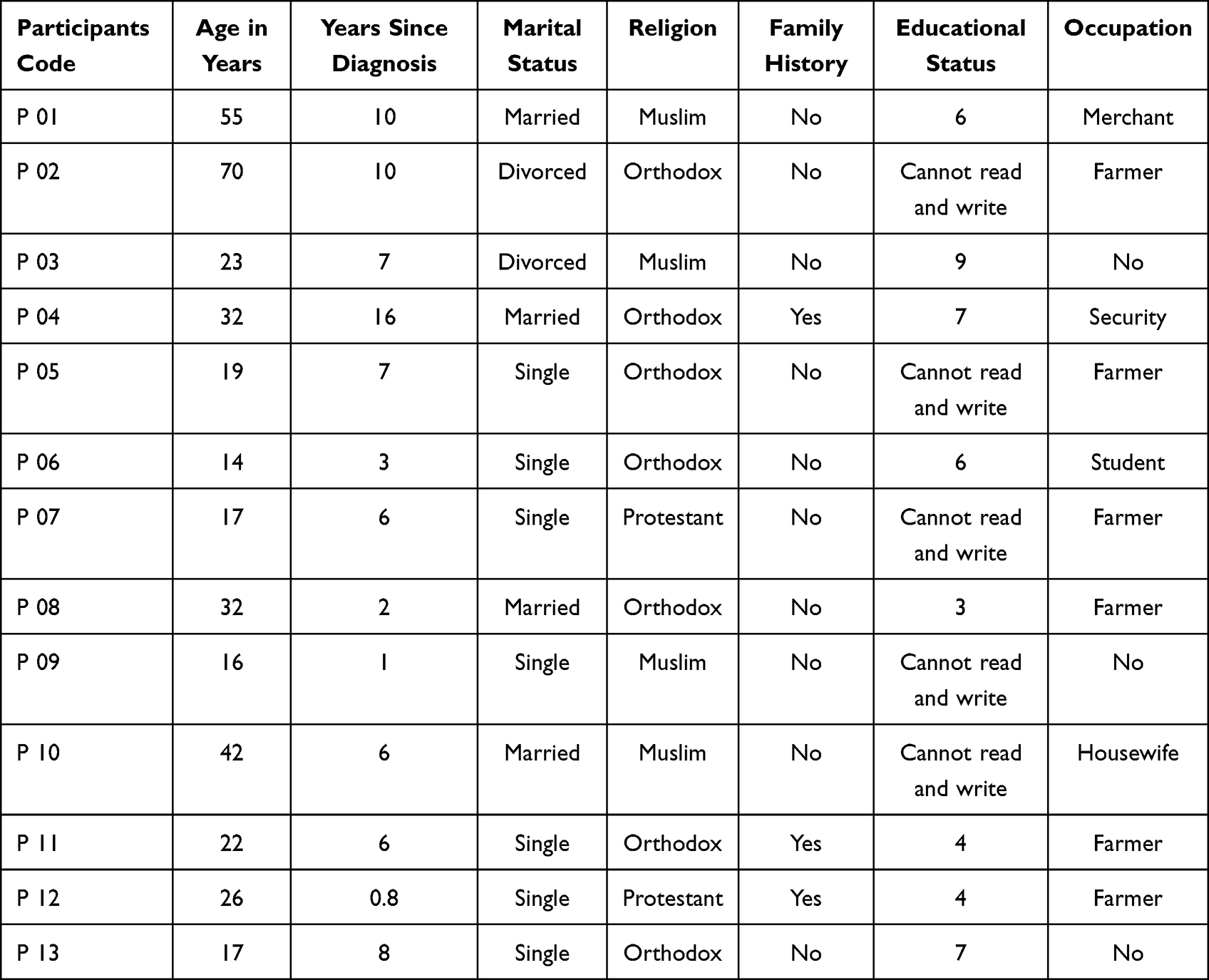 |
Table 1 Description of Study Participant Profile |
Themes, sub-themes, and categories are used to present and organise the conclusions that resulted from the study of the in-depth interview. Data analysis has revealed three interconnected themes that express the lived experiences of type 1 diabetes mellitus patients. The themes are (1) psychological experience, with two sub-themes such as psychological problems due to diabetes and coping strategies for psychological problems, (2) economic experience, and (3) social experience, which has five categories such as influence on intimate relationships, influence on social participation, disclosure status, social isolation and stigma, social support, and influence on education. See Figure 1.
 |
Figure 1 Themes and categories for lived experience of people with type 1 diabetes in north east Ethiopia; psycho-social and economical perspective, in Kemisse General Hospital, Ethiopia, 2020. |
Psychological Experience
Psychological Problems Due to Diabetes
Negative emotion was one of the psychological problems felt by the majority of the respondents during their first diagnosis of diabetes. Some of them felt shocked, cried, and scared during the initial diagnosis. The reasons for negative emotions reported by some respondents were that they considered diabetes a disease only for the rich. Assuming that it has influences on their fertility and consider it a sexually transmittable disease like HIV/AIDS. However, few of the respondents had suicidal attempts during their diagnosis. They considered diabetes a serious disease that prevented them from leading a joyful life.
When the doctor told me that I have diabetes, whether you believe it or not, I touched the electric light cord to kill myself, but while I scratched the cord with scissors to touch the electric light cord, I survived when the lights had gone off suddenly. (he said with astonishment) male respondent
When I was diagnosed with diabetes, I was shocked and screamed by saying Eyeye. Because I thought that the disease was transmitted as HIV / AIDS, and I was shocked to find out if I had never had sex outside of my husband. I was calmed down when the doctors told me that it was not an infectious disease caused by sexual contact. In fact, when my daughter went to Saudi Arabia, I became very frustrated and worried, so much so that I thought I had diabetes due to this. female respondent
All adolescent respondents felt nothing or gave no reaction when they said that they had diabetes because they were little children who did not know about diabetes and were not considered to have diabetes as a lifelong disease. When they knew diabetes was an incurable disease, some of them felt angry and stressed.
When the first time I heard that I had diabetes, I didn’t feel anything because I was a child, I didn’t know anything about the illness. Now, as I grow older and when I know diabetes is an incurable disease, my head gets stressed. female respondent
When I first had diabetes, I was young, and I didn’t know anything, so I felt nothing. male respondent
After the initial diagnosis, the majority of respondents reported that they mentally felt bad when they thought about living with diabetes, but only a few respondents did not face any negative emotions. Some of them faced angriness, crying, aggressiveness, living without patience, worrying, and giving up because they did not want to stay home alone without work. Few of them stated that they preferred to die rather than live with diabetes; they lost their joy in life and did not have any desire for life. In addition, a few of the respondents reported that they felt stressed, anxious, despaired, and depressed.
There is no need to live with diabetes, it is better to die (he spoke in a desperate voice). Eee. eree. ende. how much can I tolerate it? It made me highly angry. I have never experienced anything worse than this. male respondent
When I knew that the pain would not be healed immediately and what would be done for it, I decided to accept and tolerate it to live by controlling the pain. Now I’m living by controlling it. male respondent
Some of the respondents feared when they thought the disease could cause serious complications in their future lives, such as hypoglycemia, blindness, foot ulcers, and mental illnesses like being crazy.
They [doctors] said that it will cause blindness in the future, and I am worrying about it all the time. female respondent
Living with diabetes is very stressful. Living with diabetes is just like when a person protects grain from a wild animal such as a zoo monkey; I live suspiciously if the disease makes me drop and comes with other complications, male respondent.
Coping Strategy for Psychological Problems: To cope with psychological problems, some of the respondents adapted situations to live harmoniously with the disease, but a few respondents did not do anything to manage negative feelings. Other respondents tried to manage the situation by participating in entertainment activities, being alone at home, and seeking support from family and health professionals.
I like mental relaxation. My family makes me entertained when I get stressed, but my friends consider it difficult, and they make me ill. When they consider the disease difficult, they make me stressed, and at that time I stay at home. male respondent
When I am getting angry, my mother reassures me to keep quiet about what is going on, and she says why I am worried since she and my brothers are here for me. My brothers take care of me and keep me from becoming angry. female respondent
Performing religious activities like praying and seeking solutions from God was a common strategy mentioned by the majority of participants. They trust God to simplify their condition. Only one respondent had not the notion to perform a spiritual activity because he thought going to church without fasting was valueless since he can’t fast due to diabetes.
I am not going to church because I am eating in the early morning, how can I still go to church while I eat frequently? male respondent
Every person does not want to have the disease, but it is forced on them by the will of God, so I accept and tolerate it. I perform spiritual activities like giving a gift to the poor, showing sorrow to others, and praying to cope with those negative feelings. I can get psychological support from my family, friends, and health professionals by giving advice. I can’t see a bad face from a health professional during care. Nothing is coming despite sorrow due to illness. male respondent
Social Experience Related to Diabetes
Influence on Intimate Relationships
The distraction of intimate relationships was one of the major social problems reported by some of the participants. Some of the married respondents reported that diabetes had influenced their marital status, especially their sexual activity. Two of the respondents were divorced due to diabetes, and another one faced divorce only for three months because of illness but returned to his marriage through negotiation. The major reasons for divorce were sexual dysfunction and being unable to participate in income-generating work.
I am divorced due to diabetes. The first thing that broke my marriage was that I didn’t work since I had diabetes. The second thing that broke my marriage was a reduction in sexual activity. Even if I performed it occasionally, it reduced my pleasure during sexual activity. male respondent
I am divorced from my wife because of my pain (diabetes), and she is tired of my pain (diabetes), as a result, she keeps quiet when I drop in front of her. It is only now that I know my condition, and it makes me feel crazy because I don’t know anything when it (hypoglycemia) comes up. male respondent
The majority of single male respondents fear having a partner for marriage or a girlfriend because some of them think that they will face problems during sex and consider it a sexually transmittable disease. All adolescent female respondents do not have the idea of marriage in the future because of social stigma and are unable to do the routine activities that husbands expect from housewives. The following quotations serve as examples:
I don’t have a girlfriend. I am thinking of getting a girlfriend, but I am afraid because I think it is going to take my energy when I perform sex. male respondent
At the present time, I have no boyfriend and no idea of marriage. I don’t think about marriage anymore for the future because I can’t work on what I see and what I want to do. female respondent
Influence on Social Participation
Being diabetic has a great influence on social participation, as reported by the majority of the respondents. They did not attend social gatherings such as wedding ceremonies, funeral ceremonies, and Kire (Iddir). The most common reasons mentioned by respondents were fear of hypoglycemia, feeling tired during the journey, and the food prepared for those special events not being suitable for them.
I stopped participating in social activities like wedding ceremonies, funeral ceremonies, and Iddir (kire) because the disease [diabetes] dropped me in front of others due to low blood glucose. male respondent
I don’t participate in social life because of diabetes. I don’t go to the wedding ceremony because I am going to get lost in a direction to pass in the middle of a lot of people going to the wedding party (mass of people), and I suspect diabetes will drop me in front of another person. Also, if I go to the wedding party, I don’t eat food because the meal is not suitable for diabetics. male respondent
Disclosure Status, Social Isolation, and Stigma
The majority of respondents disclosed their diabetes status to their family, relatives, friends, and neighbours. Disclosing their status was beneficial for some respondents to get social support. Few of the respondents did not disclose their status to another person except their family, and they performed selective disclosure depending on the situation. The reported reasons for not disclosing their status were fear of stigma, isolation, and dissemination of their diabetic status as secret information to another person.
I told my friends, brothers, and family about how the disease hurts me, what I need, and if I am hungry, it (hypoglycemia) will drop me. I didn’t talk about my diabetes status with her [my girlfriend]. If I am going to get married to her in the future, I will let her know that I have diabetes in time, but now I won’t tell her because I do not want to disseminate the news. male respondent
Some of the respondents reported that people they meet every day felt angry and sad at them when they knew he or she is diabetic. Some other people did not feel anything and few of them were supportive. In addition, few participants reported the negative reactions of other people when they disclose their diabetes status and their need for lifelong daily insulin injections.
When the people I meet every day know that I am diabetic…they said that having AIDS is better than having sugar [diabetes]…They considered that I had a serious illness, an irreversible, always injecting the drug and they get bored when I am not tired of the needle. female respondent
Some of the respondents reported that people they meet every day felt angry and sad at them when they knew he or she was diabetic. Some other people did not feel anything, and a few of them were supportive. In addition, a few participants reported the negative reactions of other people when they disclosed their diabetes status and their need for lifelong daily insulin injections.
When the people I meet every day know that I am diabetic, they said that having AIDS is better than having sugar [diabetes]…They considered that I had a serious illness, an irreversible one, and I was always injecting the drug, and they got bored when I was not tired of the needle. female respondent
Social isolation and stigma were among the reported social problems of participants. Few participants faced social isolation imposed by others. Besides this, some participants reported that they withdrew from social contacts due to self-imposed social isolation after they were diagnosed with diabetes. The major reasons for social isolation reported by participants were lack of financial income, lack of creating fun with friends, being unable to drink and eat food together, being unable to work together, and even not being able to discuss things with them.
I am isolated from social life. If I ask them [friends] to approach me, they don’t approach me because I have nothing to talk to them, nothing to give them, I couldn’t work, and I didn’t discuss with them this [some idea]. Why did they approach me because I was out of action? My friends hate me to say good morning…. male respondent
There is something to isolate me. My friends were isolated when they discovered it was sugar (diabetes). Now that I have no friends, I am alone, female respondent.
Social stigma was another problem faced by participants. Some participants verbalized that they kept their diagnosis a secret from neighbours and friends in order to avoid diabetes-related stigma. Participants were very secretive about their health. They told only the closest family members whom they could trust. They thought it was not their fault to get the disease; rather, it was God’s will. The participants feared that disclosure would result in losing friends or becoming socially isolated. They just wanted to be alone to avoid being confronted with stigma.
I didn’t tell my neighbour that I had diabetes, because I am afraid that if I told them they couldn’t understand the condition since we live in a rural area. As a result, they will tell another person that I have diabetes. It compromises me. My friends didn’t know I have diabetes, but only my family knows. male respondent
Social Support
Social support is crucial to people with chronic illnesses. The majority of the participants had supportive family members who knew about their illnesses. The majority of respondents stated that support from family or friends may also play a significant role in managing diabetes. Through the support, they took medicine, ate an appropriate diet, and the support helped them not to be busy with a lot of work to manage their way of life regularly. The majority of patients claimed that receiving social support inspired them to lead healthy lifestyles and reduce psychological issues. In addition to the family, some respondents received support from friends, neighbors, and health professionals.
Neighbors who are old people and they are infirmly called me to check whether I was raised up to eat food. When the pain dropped me, they shout like wu.ou.ou, ou.rey… and they called someone for help. Then they [neighbors] came over and bring me injera, and this is my mouth that is closed (showing his mouth) and they feed me while they mingle my mouth by spoon (showing by poking his teeth) … Social support is very soulful… male respondent
I get help from health professionals and they even treat me like their brother, they make me feel very welcome, advice, and explained to me about diabetes. male respondent
Influence on Education
Diabetes had a great influence on education, as was reported by some of the respondents. It made them stressed when they took the exams. Few of them dropped from school because of diabetes. A few participants reported that the reasons for dropping out were frequent hypoglycemia, traveling long distances on foot to reach schools, and tiredness during the journey. Currently, only one respondent is in education, while the rest are not.
It has an effect on my education because it made me stressed when I took an exam test. When they went on a long journey for educational competition, I stayed away because I was afraid it would throw me if I went on a long journey. female respondent
Now I am no longer in school. I learned until I was in 7th grade and dropped out because of the illness, but I knew I had diabetes when I was in 3rd grade. I dropped out of school four years after my diabetes started because I am tired while traveling since I live far away from school, I am not walking the same route as my friends, and at that time, being a diabetic put a strain on my education. When I went through a test, I got stressed, but it didn’t make me think about answering the test. Now I can write and read well, but I have no desire to start school again. female respondent
Economical Experience
Regarding occupation, six of the respondent’s livelihoods were agriculture, 1 merchant, 1 security, and 1 housewife, and the rest four respondents lived with their families dependently. Most of the respondents stated that their working lives were adversely affected and they had financial problems because of their conditions. They faced difficulty in participating income generating work because of diabetes. The reasons reported by most participants were the occurrence of the hypoglycemic episode while they were working for a long period of time and fear of sun heat which exacerbate their illness.
… when I get busy with the workload I have a diabetic tendency to feel like an electric city contact. If I work a little and stop it, I will be fine, but if I keep working, I will be sweaty and the pain will drop me. it tends to get like crazy, I don’t know what to say or do, I can’t control my body… male respondent.
The majority of the respondents expressed their difficulty to get money to fulfill their basic needs. Most of the respondents were in good living conditions before being diagnosed with diabetes, but their life was changed dramatically including economical crises since they were diabetic. Almost all of them lost their money for treatment that they had before they were diagnosed with diabetes. They sold all their property because of their diabetes to attend life long treatment regimen.
Ohoooy…(the laughter of surprise) I was rich before I got sick of diabetes….My condition wonders to other people and they said he was a good man empiiempiii (Express sympathy)…all those who know me before would be very sorry to see me. …today I seem like a dead donkey (the laughter of surprise), I have nothing…. male respondent
Living with dependency on the family was one of the problems reported by some of the participants. All respondents who were dependent never thought to live independently because of diabetes, and their family livelihood depends upon agriculture. Family support did not end with social and psychological support; rather, it extended financially too.
Now I live with family by looking into their eyes [to express dependency] because I sat down. I am looking for them (financial support), but I am finished with my own (money). I am living in an asylum (dependent on) with my family. I have no idea if I can afford it because I have no money. I couldn’t work because of the pain. female respondent
All respondents reported that they had health insurance for their follow-up treatment. Most of them paid for health insurance on a yearly basis, but few of them were supported by the government to treat for free by covering the fee for health insurance. Few of them mention the anticipated fear of interruption of taking insulin injections in the future because they will not be able to afford to pay for treatment if the government either increases the fee or stops health insurance.
When I have a hard time paying for health insurance, my family helps me. I am worried that either the government will increase the amount paid for health insurance or that the health insurance will stop, and that the illness is on me until death because I will spend the rest of my life on drugs, so I am worried that health insurance will not interrupt for me. male respondent
As explained by some of the respondents, first of all, the government should start to gather diabetes patients and form associations to help them by creating opportunities for income-generating work since most diabetic patients cannot participate in work due to an uncomfortable working environment.
If there are people like me who have diabetes and we don’t have a good job of managing our lives, It will be good if the government gathers us together for discussion and creates a joint venture. male respondent
Discussion
In this study, people with type 1 diabetes had fear as one of their main issues, which arises from fear of chronic complications such as amputation, heart disease, and blindness. This finding was similar to studies conducted in Ireland,20 Netherlands,18 and United Kingdom 21 in which participants worried not only about day-to-day complications, but also about long-term complications like blindness and having problems with their circulation.
Fear also arises from acute complications, such as the fear of hypoglycemic episodes. This result is similar to studies conducted in Netherlands,18 Sweden,22 and Boston,23 which revealed the potential for adverse consequences and harm to oneself or others when experiencing hypoglycemia. This might be due to the proper understanding of diabetic patients about the impact of chronic and acute complications of diabetes, which may restrict their social participation and limit routine activities that can reduce the quality of life of people with type 1 diabetes.
In this study, aggressiveness was one of the psychological problems faced by diabetes patients who mostly live with no patience and quarrel with most people that they meet. The same results were reported in the studies conducted in Ireland,20 Netherlands,18 and Sweden 22 participants described irritable and aggressive behavior, which sometimes left family members feeling unsafe and vulnerable to attack from the person with type 1 diabetes. This might be due to the psychological and the physiological factors which are responsible for diabetic aggression. The psychological component of diabetic aggression comes from the stress of living with this disease and physiological component of diabetic aggression is due to diabetes is a disorder characterized by the inability to metabolize glucose since glucose is a brain food that increases self-control, those who have difficulty metabolizing glucose should have less self-control. Low levels of self-control are linked to high levels of aggression.24
In this study, diabetes has a negative impact on the social aspects of the patient, which include isolation and stigma, which is similar to studies conducted in Zambia,11 New York,25 Finland,26 and in four countries (US, UK, Germany, and France).27 This might be due to a lack of community understanding of diabetes in developing countries. Additionally, patients also isolate themselves from society. This might be due to their desire to protect themselves and their families from stigma.
Inability to participate in regular social activities like wedding ceremonies, which were similar to studies conducted at Ireland20 and San Antonio.28 This might be due to fear of hypoglycemia in front of other people, isolation, stigma, and the fact that the food prepared for the special social events was not suitable for diabetic patients, which inhibits their participation in the social events.
In this study, participants feel bad about disclosing their diabetic status. Fear of social stigma was one of the major reasons for not disclosing diabetes status due to personal fear of being judged, especially for women who may not be married due to the stigma imposed by society. This result was similar to studies conducted in studies conducted at Ireland,20 in four countries (US, UK, Germany, and France),27 and Central England,28 in which some unmarried participants described a more inhibited approach towards disclosure. This might be due to their interest in protecting themselves and their families from stigmatization by either isolating themselves or not disclosing their diabetes status to society.
All students in this study disclosed their diabetes status to their friends, and they got good support from their peers. However, the study conducted in Canada,29 revealed the opposite results: students hid their diseases for a variety of reasons, such as not wanting empathy from others and not wanting being labelled as different from their peers. This difference might be due to all student peers coming from the same living environment in this study, which leads to ease of disclosure. In contrast, the study participants in Canada were university students, in which they faced a difficult environment to disclose their status since most students gather from a different background perspective.
Diabetes also prevents patients from participating in income-generating work. This result was similar to other studies conducted at Ireland,20 Briston,23 Finland,26 and South East England,30 in which diabetes patients did not participate in work that could endanger them or others, such as operating heavy machinery, driving, or caring for a young kid alone. This might be due to fear of hypoglycemic episodes during work, and the absence of a comfortable working environment to comply with insulin injections and follow recommended dietary plans, which might lead to an economic crisis. Additionally, due to safety concerns, the danger of hypoglycemia may prevent specific work kinds from being pursued.
Strengths and Limitations of the Study
In this study, a phenomenological type of approach is best suited to the title psychological and socio-economical experiences of people with type 1 diabetes. We recruited the study participants using a heterogeneous purposive sampling strategy, which enabled the authors to view the data from a different angle.
The one of the limitation of this phenomenological study is linked with the emphasis on subjectivity and difficulty to have generalizable research findings, which means the result of the study can not be generalized to population, settings, and contexts other than the sample being studied.
This study also prone to bias, and one of biases introduced due to use of purposive sampling which is non probability sampling to recruit study participant does not yield external validity. Recall bias may be introduced at the time of the in-depth interview due to the chronic nature of the disease. To minimise recall bias, we used probing, which leads to more clarity on interview questions, and furthermore, by following an ordered sequence of events, backwards recall can help with memory recall. Start in the present and consider a specific moment in the past. Because recent occurrences are simpler to remember, recalling earlier ones is aided. Moreover, despite the precautions taken during the interviews, social desirability bias may still be present.
Conclusions
In this study, the lived experience of people with type 1 Diabetes in North East Ethiopia was addressed in terms of the psychological, social and economical experience of people with type 1 Diabetes. The psychological experiences were psychological problems due to diabetes (fear, aggressiveness, anger, stress, and giving up) and coping strategy (participating in entertainment activities, being alone at home, family support, health professionals support and stick with religious activity). Identified social experiences were influence on intimate relationships, influence on social participation, disclosure status, social isolation, stigma, social support and influence on education. The economical experiences were difficulty in participating income generating work, difficulty of earning money to buy medication and other basic needs. Although type 1 diabetes is a biomedical problem, it is also accompanied by other psycho-social and economical issues, that require a holistic approach to address it. So, health professionals should strengthen health information dissemination programs.
Abbreviation
ADA, American Diabetes Association; BDU, Bahir Dar University; CVDs, Cardio Vascular Diseases; DM, Diabetes Mellitus; IDF, International Diabetes Federation; IRB, Institutional Review Board; NCD, Non-Communicable Disease; NGOs, Non-Governmental Organizations; NHS, National Health Survey; QOL, Quality Of Life; SDG, Sustainable Development Goal; T1DM, Type 1 Diabetes Mellitus; T2DM, Type 2 Diabetes Mellitus; UK, United Kingdom; UNGA, United Nations General Assembly; US, United States; WHO, World Health Organization.
Data Sharing Statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Consent for Publication
The authors affirm that they have given their consent to be published in this journal. In addition, participants provided signed informed agreement to share and publish their data anonymously for scientific research only.
Acknowledgments
We would like to give our special thanks to study participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no funding from any funding agency.
Disclosure
The authors declare that they have no competing interest.
References
1. WHO. Classification of Diabetes Mellitus; 2019.
2. FDRE-MOH. Guidelines on clinical and programmatic management of major non communicable diseases, Addis Ababa, Ethiopia; 2016:37.
3. Kalyva E, Malakonaki E, Eiser C, Mamoulakis D. Health-related quality of life (HRQoL) of children with type 1 diabetes mellitus (T1DM): self and parental perceptions. Pediatr Diabet. 2011;12(1):34–40. PMID: 20546163. doi:10.1111/j.1399-5448.2010.00653.x
4. Thomas NJ, Jones SE, Weedon MN, Shields BM, Oram RA, Hattersley AT. Frequency and phenotype of type 1 diabetes in the first six decades of life: a cross-sectional, genetically stratified survival analysis from UK Biobank. Lancet Diabet Endocrinol. 2018;6(2):122–129. PMID: 29199115; PMCID: PMC5805861. doi:10.1016/S2213-8587(17)30362-5
5. Onwudiwe NC, Mullins CD, Winston RA, et al. Barriers to self-management of diabetes: a qualitative study among low-income minority diabetics. Ethn Dis. 2011;21(1):27–32. PMID: 21462726.
6. Celik S, Kelleci M, Avcı D, et al. Psychosocial adaptation and strategies for coping with stress of adolescents with type 1 diabetes (in Turkish) . Florence Nightingale J Nur. 2015;23(2):105–115.
7. IDF, International Diabetes Federation. Diabetes atlas 10 edition; 2021. Available from: https://diabetesatlas.org/idfawp/resourcefiles/2021/07/IDF_Atlas_10th_Edition_2021.pdf.
8. Wang H, Naghavi M, Allen C, et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388(10053):1459–1544.
9. International Diabetes Federation. (IDF) Diabetes Atlas. 7th Edition, International Diabetes Federation, Brussels, Belgium; 2015. Available from: http://www.diabetesatlas.org.
10. UK Department of Health. National Service Framework for Diabetes; 2016.
11. Hapunda G, Abubakar A, van de Vijver F, Pouwer F. Living with type 1 diabetes is challenging for Zambian adolescents: qualitative data on stress, coping with stress and quality of care and life. BMC Endocr Disord. 2015;15(1):20. PMID: 25928592; PMCID: PMC4411790. doi:10.1186/s12902-015-0013-6
12. Nielsen HB, Ovesen LL, Mortensen LH, Lau CJ, Joensen LE. Type 1 diabetes, quality of life, occupational status and education level - A comparative population-based study. Diabet Res Clin Pract. 2016;121:62–68. PMID: 27662040. doi:10.1016/j.diabres.2016.08.021
13. Agalu A, Zeleke A, Woldie M. Diabetic complications among adult diabetic patients of a tertiary hospital in northeast Ethiopia. Adv Public Health. 2015;1–7. doi:10.1155/2015/290920
14. Habtewold TD, Tsega WD, Wale BY. Diabetes mellitus in outpatients in debre berhan referral hospital, Ethiopia. J Diabet Res. 2016;2016:3571368. PMID: 26881245; PMCID: PMC4736777. doi:10.1155/2016/3571368
15. Abebe N, Kebede T, Addise D Diabetes in Ethiopia 2000–2016 – prevalence and related acute and chronic complications; a systematic review; 2017.
16. Alemu F. Prevalence of diabetes mellitus disease and its association with level of education among adult patients attending at dilla referral hospital, Ethiopia. J Diabet Metab. 2015;6(521):1.
17. Lincoln Y, Guba E. Handbook of Qualitative Research. Thousand Oaks, CA: Sage; 2000.
18. Hortensius J, Kars M, Wierenga W, et al. Perspectives of patients with type 1 or insulin-treated type 2 diabetes on self-monitoring of blood glucose: a qualitative study. BMC Public Health. 2012;12(167). doi:10.1186/1471-2458-12-167
19. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
20. Balfe M, Doyle F, Smith D, et al. What’s distressing about having type 1 diabetes? A qualitative study of young adults’ perspectives. BMC Endocr Disord. 2013;13:14.
21. King K, Nayar R, Wilkes S. Perceptions of adolescent patients of the “lived experience” of type 1 diabetes. Am Diabet Ass. 2017;30(1):23–35.
22. Garmo A, Hornsten A, Leksell J. The pump was a saviour for me.’ Patients’ experiences of insulin pump therapy. Diabet Med. 2013;30(6):717–723. doi:10.1111/dme.12155
23. Ryninks K, Sutton E, Thomas E, et al. Attitudes to exercise and diabetes in young people with type 1 diabetes mellitus: a qualitative analysis. PLoS One. 2015;10(10):e0137562. doi:10.1371/journal.pone.0137562
24. DeWall CN, Deckman T, Gailliot MT, Bushman BJ. Sweetened blood cools hot tempers: physiological self-control and aggression. Aggress Behav. 2011;37(1):73–80. doi:10.1002/ab.20366
25. Trief P, Sandberg J, Dimmock J, et al. Personal and relationship challenges of adults with type 1 diabetes: a qualitative focus group study. Diabet Care. 2013;36(9):2483–2488. doi:10.2337/dc12-1718
26. Rintala T, Paavilainen E, Åstedt-Kurki P. Everyday life of a family with diabetes as described by adults with type 1 diabetes. Eur Diabet Nurs. 2013;10(3):86–90. doi:10.1002/edn.234
27. Brod M, Pohlman B, Wolden M, et al. Non-severe nocturnal hypoglycemic events: experience and impacts on patient functioning and well-being. Qual Life Res. 2013;22(5):997–1004. doi:10.1007/s11136-012-0234-3
28. Sourav A, Arijit S, Uttam K, et al. A qualitative study on the thoughts of diabetics against initiation of insulin therapy. Int J Sci Stud. 2017;5(2):21.
29. Hill S, Gingras J, Gucciardi E. The lived experience of Canadian University students with type 1 diabetes mellitus. Can J Diabet. 2013;37(4):237–242. doi:10.1016/j.jcjd.2013.04.009
30. Ruston A, Smith A, Fernando B. Diabetes in the workplace, diabetic’s perceptions and experiences of managing their disease at work: a qualitative study. BMC Public Health. 2013;13(10). doi:10.1186/1471-2458-13-386
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.