Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Limited Benefit of Additional Chartis® Assessments for Collateral Ventilation Evaluation in Patients with Software Quantified Intact Target Lobe Fissure – Results from a Retrospective Analysis of the German Lung Emphysema Registry
Authors Saccomanno J ![]() , Sgarbossa T, Neumann K
, Sgarbossa T, Neumann K ![]() , Stanzel F, Andreas S, Eisenmann S
, Stanzel F, Andreas S, Eisenmann S ![]() , Schmidt B, Gesierich W, Witzenrath M, Hübner RH
, Schmidt B, Gesierich W, Witzenrath M, Hübner RH
Received 6 May 2025
Accepted for publication 15 October 2025
Published 4 December 2025 Volume 2025:20 Pages 3939—3950
DOI https://doi.org/10.2147/COPD.S538587
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Jacopo Saccomanno,1 Thomas Sgarbossa,1 Konrad Neumann,2 Franz Stanzel,3 Stefan Andreas,4,5 Stephan Eisenmann,6 Bernd Schmidt,7 Wolfgang Gesierich,8 Martin Witzenrath,1,5,9 Ralf Harto Hübner1 On behalf of the Lung Emphysema study group
1Department of Infectious Diseases, Respiratory Medicine and Critical Care, Charité – Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität Zu Berlin, Berlin, Germany; 2Institute of Biometry and Clinical Epidemiology, Charité - Universitätsmedizin Berlin, Berlin, Germany; 3Department of Respiratory Medicine, Lungenklinik Hemer, Hemer, Germany; 4Zentrum für Pneumologie, Lungenfachklinik Immenhausen, Immenhausen, Germany; 5German Center for Lung Research (DZL), Berlin, Germany; 6Department of Respiratory Medicine, Universitätsklinikum Halle, Halle, Germany; 7Department of Internal Medicine – Respiratory and Sleep Medicine, DRK Kliniken Berlin Mitte, Berlin, Germany; 8Department of Respiratory Medicine, Asklepios Lungenklinik Gauting, Gauting, Germany; 9Capnetz Foundation, Hannover, Germany
Correspondence: Jacopo Saccomanno, Department of Infectious Diseases, Respiratory Medicine and Critical Care, Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Hindenburgdamm 30, Berlin, 12203, Germany, Email [email protected]
Background: Endoscopic lung volume reduction (ELVR) with valves is a treatment option for selected patients with emphysema. Collateral Ventilation (CV) is measured directly with the Chartis® bronchoscopic assessment system (PulmonX Inc. Redwood City, CA, USA) and indirectly via fissure completeness score (FCS) on computed-tomography (CT). It remains unclear, whether the additional Chartis® assessment improves treatment outcome when the target lobe shows intact fissure (FCS ≥ 95%).
Study Design and Methods: This retrospective analysis used data from the German Lungenemphysemregister e.V. a prospective multicenter trial on lung volume reduction therapy. Patients with an intact fissure (FCS ≥ 95%) of the target lobe undergoing ELVR were included. Treatment outcomes were compared between patients who had a Chartis® measurement prior to ELVR and those who did not.
Results: A total of 262 patients were analyzed: 175 with Chartis® and 87 without. Baseline parameters were comparable between groups. At 3-month follow-up significant improvements in lung function parameters (FEV1, RV, DLCO, pCO2), exercise capacity (6-MWT) and quality of life parameters (SGRQ, mMRC and CAT) were seen in both groups. Treatment efficacy at 3-month follow-up was comparable in patients regardless of previous Chartis® measurements. Furthermore, there was no difference in treatment outcome, when comparing improvements for the right and left lung separately. Responder rates were similar between the groups, with a comparable MCID in both. Complication rates were also largely comparable, except for a higher pneumothorax rate in the no-Chartis group (7% vs 22%).
Discussion: This analysis did not find evidence that a Chartis® assessment provided additional benefit to the treatment response after ELVR at 3-month follow-up in patients with an intact fissure of the target lobe with an FCS ≥ 95%. These findings may be clinically relevant as they suggest that additional invasive Chartis® measurement might be dispensable in this subgroup.
Keywords: Lung emphysema, endoscopic lung volume reduction with valves, collateral ventilation, COPD
Introduction
Chronic obstructive pulmonary disease (COPD) is increasing in prevalence worldwide with significant morbidity and mortality.1 Severe lung emphysema is a debilitating form of COPD presenting with severe dyspnea. Lung emphysema is characterized by destruction of alveolar walls and remodeling of airway walls reducing elastic recoil of the lung, due to chronic inflammation often linked to smoking. The resulting air trapping at alveolar level leads to hyperinflation limiting breathing mechanics in particular due to reduced diaphragmatic mobility.2–4
Endoscopic lung volume reduction (ELVR) with endobronchial and intrabronchial one-way valves addressing hyperinflation is an established therapy for carefully selected patients with advanced lung emphysema improving lung function, exercise capacity and life quality parameters and is potentially reversible.5–7 For treatment response of ELVR with valves, prior exclusion of collateral ventilation (CV) between the target lobe and its adjacent lobe is mandatory.8 Software-based fissure quantification of computed tomography (CT) scans assesses CV with the fissure completeness score (FCS). An in vivo assessment of CV is the bronchoscopic measurement of airflow in the target lobe, called Chartis® (PulmonX Inc., Redwood City, CA, USA) assessment.9,10 Diagnostic accuracies of 74–83.3% for Chartis® assessment and 78.8–96.4% for fissure completeness score (FCS) have been reported.11–14 The exact diagnostic algorithm still remains to be elucidated since randomized controlled studies employed different study protocols, variable cut-off values or different software tools for the FCS.6,8,15–20 A study by Koster et al, which analyzed pooled data from four prospective studies, recommended performing a Chartis® assessment of collateral ventilation (CV) in cases of intermediate fissure integrity (FCS 80–95%), and proceeding directly with ELVR when fissure completeness is ≥95%.11 However, a more recent publication focusing on anatomical differences in fissure formation between the right and left lung suggested a fissure-dependent approach for assessing CV. The authors recommended always performing a confirmatory Chartis® assessment in the right lung, since several cases with CV-positive measurements were found even when fissure completeness was ≥95%.20 Although a fissure-dependent approach may seem logical when considering the more complex fissure anatomy in the right lung, this study did not report treatment outcomes after ELVR. This is clinically relevant, since a Chartis® assessment is an invasive and time intensive procedure that requires occluding the target lobe with a balloon catheter and measuring the change in airflow over a longer time period.
The German Lung Emphysema Registry is a large, prospective, multi-center national trial involving over 40 centers in Germany, aimed at improving medical care for patients with lung emphysema. In this study, we first surveyed centers within the registry to determine whether Chartis® assessment is routinely performed in patients with an FCS ≥95%. Second, using data from the registry and the survey results, we analyzed whether Chartis® assessment provided any additional benefit in treatment outcomes for patients with an intact fissure in the target lobe.
Materials and Methods
Data from patients who received ELVR with valves according to the standards of the Lungenemphysemregister e.V. were included. Lungenemphysemregister e.V. (www.lungenemhysemregister.de) is a German national, multicentric, prospective, producer independent, open label clinical trial significantly supported in terms of centralized and quality-assured data collection by CAPNETZ foundation. The trial was approved by the local ethics committees of the study centers (A2/149/17 and EA1/136/13). All patients provided informed consent. Data was centrally managed by REDCap electronic data capture tools located at Charité – Universitätsmedizin Berlin.21
Inclusion and Exclusion Criteria
Patients with advanced lung emphysema who received optimal medical therapy were included in case they presented with the following lung function parameters: Forced expiratory volume in 1 second (FEV1) <45%, Residual Volume (RV) ≥180%. They had to be a non-smoker for at least three months confirmed by a carboxyhemoglobin (HbCO) <2% and/or negative urine cotininetest. Exercise capacity was assessed using the 6-Minute Walk Test (6-MWT); a distance of less than 450 m was required, without a defined lower limit.22 A partial pressure of carbon dioxide <55mmHg was required, otherwise patients were evaluated for non-invasive ventilation first. If possible, patients needed to establish a physical activity program prior to ELVR. Patients were excluded if dyspnea was not primarily due to lung emphysema and hyperinflation.
Evaluation Procedure
All patients underwent a standardized evaluation procedure. A bodyplethysmography, diffusion capacity test, blood arterial/capillary gas analysis, 6-MWT and optional echocardiography were performed. In some centers a ventilation perfusion scintigraphy is part of the baseline assessment. Additionally, quality of life questionnaires including the COPD Assessment Test (CAT), modified Medical Research Council Dyspnea Scale (mMRC) and Saint George´s Respiratory questionnaire (SGRQ) were also collected.
Assessment of Collateral Ventilation and Emphysema Quantification
For fissure integrity analysis and emphysema quantification a CT scan of the lung without contrast media was obtained and a software analysis was performed. The most frequently used software tools are StratX (Pulmonx), Apollo (Vida) and YACTA. Usually, FCS is expressed in percentages, whereby a FCS ≥95% is considered as an intact fissure. In the left lung FCS values for left upper lobe and left lower lobe correspond since only the left oblique fissure is separating both lobes. Fissure anatomy in the right lung is more complex. The right upper lobe is separated from the middle lobe by the upper horizontal fissure. The right oblique fissure separates the middle and upper lobe from the lower lobe. Values for fissure integrity for the right upper lobe, middle lobe, right lower lobe and right upper lobe including right middle lobe together are presented.
Chartis® measurements were performed under general anesthesia and mechanical ventilation or in procedural sedation and spontaneous breathing patients depending on the standards of the centers.23 CV status was visually classified according to the previously described four Chartis® phenotypes: CV positive, CV negative, Low Flow and Low Plateau.10,24–26 However, Chartis® assessment was only recorded in the registry as CV negative, CV positive and inconclusive Chartis® assessment.
To picture current standards of the evaluation of CV in the lung emphysema registry we sent a questionnaire to the 20 most experienced centers with more than five ELVR procedures per year and asked whether a Chartis® assessment in case of FCS ≥95% is routinely performed.
To assess the emphysema score per lobe based on CT data, the percentage of voxels with an attenuation value below −950 Hounsfield Units (HU) was calculated. The heterogeneity index (HI), used to differentiate heterogeneous from homogeneous emphysema, was defined as the absolute difference in emphysema score between the target lobe and its ipsilateral adjacent lobe. An HI ≥15% is commonly applied as the threshold to classify emphysema as heterogeneous.6,17,19
Endoscopic Lung Volume Reduction
Prior to ELVR with valves every case was discussed by a local multidisciplinary emphysema board consisting of interventional pulmonologists, thoracic surgeons, radiologists to identify the target area for lung volume reduction and optimal treatment methods. Patients recommended for ELVR with valves underwent valve implantation with Zephyr® valve system (Pulmonx, Redwood City, CA, USA) or Spiration Valve System (Olympus, Center Valley, PA, USA) in the target lobe. The valves system was selected by the interventional pulmonologist according to endobronchial anatomy and local availability of valve types.
Study Design
Patient data were obtained from the lung emphysema registry and were included if they presented for 3-month follow-up and had an FCS ≥95%. Patients were divided into two groups based on whether a Chartis® measurement (CV positive, CV negative and CV unevaluable) was performed. A retrospective analysis was conducted to evaluate overall treatment outcomes, treatment outcomes for the left and right lung, MCID, and complication rates.27–30 It is important to note that, due to the nature of the registry, only patients who underwent ELVR were included. Therefore, the number of patients with a CV positive Chartis® result may be underreported, as these patients might not have been treated and thus were not included in the analysis.
Statistical Analysis
For categorical variables, absolute and relative frequencies were reported for all levels. Continuous variables were summarized as means and standard deviations for both groups. Baseline characteristics were compared between the patient groups with and without Chartis® using independent samples t-tests. Changes in lung function parameters, quality of life questionnaire scores, and exercise capacity were analyzed using Wilcoxon’s signed-rank test. Differences in changes in lung function parameters (denoted by the prefix Δ) between baseline and the 3-month follow-up were compared between the Chartis® and non-Chartis® groups using independent samples t-tests. Statistical analyses were conducted using SPSS software (version 24.0.0.0; IBM, Armonk, NY, USA). As this study is non-confirmatory, all p-values are considered exploratory.
Results
Questionnaire
The 20 most experienced centers in the Lung Emphysema Registry were asked whether an additional Chartis® measurement was performed, if the target lobe was considered to have an intact fissure. 19/20 centers used quantitative FCS analysis, while one center relied on visual assessment. Additional Chartis® assessment was only performed in 8/20 centers when FCS showed fissure integrity ≥95%.
Study Population
Table 1 represents the baseline characteristics of 175 patients with Chartis® and 87 patients without Chartis® assessment. All of them had a FCS of 95% or higher. In the Chartis® group 159 (90.9%) patients were CV negative, one (0.4%) was reported CV positive and 15 (8.7%) had an unevaluable Chartis phenotype. The age range, gender distribution, body mass index (BMI), heterogeneity index, lung function parameters, exercise capacity and life quality parameters were comparable in both groups. The emphysema score of the target lobe was higher in the no Chartis® group (p=0.011) and there was a slightly higher mMRC in patients with Chartis® measurement compared to no Chartis® measurement at baseline. In the Chartis® group, ELVR was performed in the right upper lobe (7.4%), middle lobe (3.4%), right lower lobe (20.0%), left upper lobe (27.4%) and left lower lobe (27.4%). In the no-Chartis® group, the respective rates were 10.3% in the right upper lobe, 4.6%, in the middle lobe, 16.1% in the right lower lobe, 27.6% in the left upper lobe and 42.5% in the left lower lobe. There was no difference between the two groups.
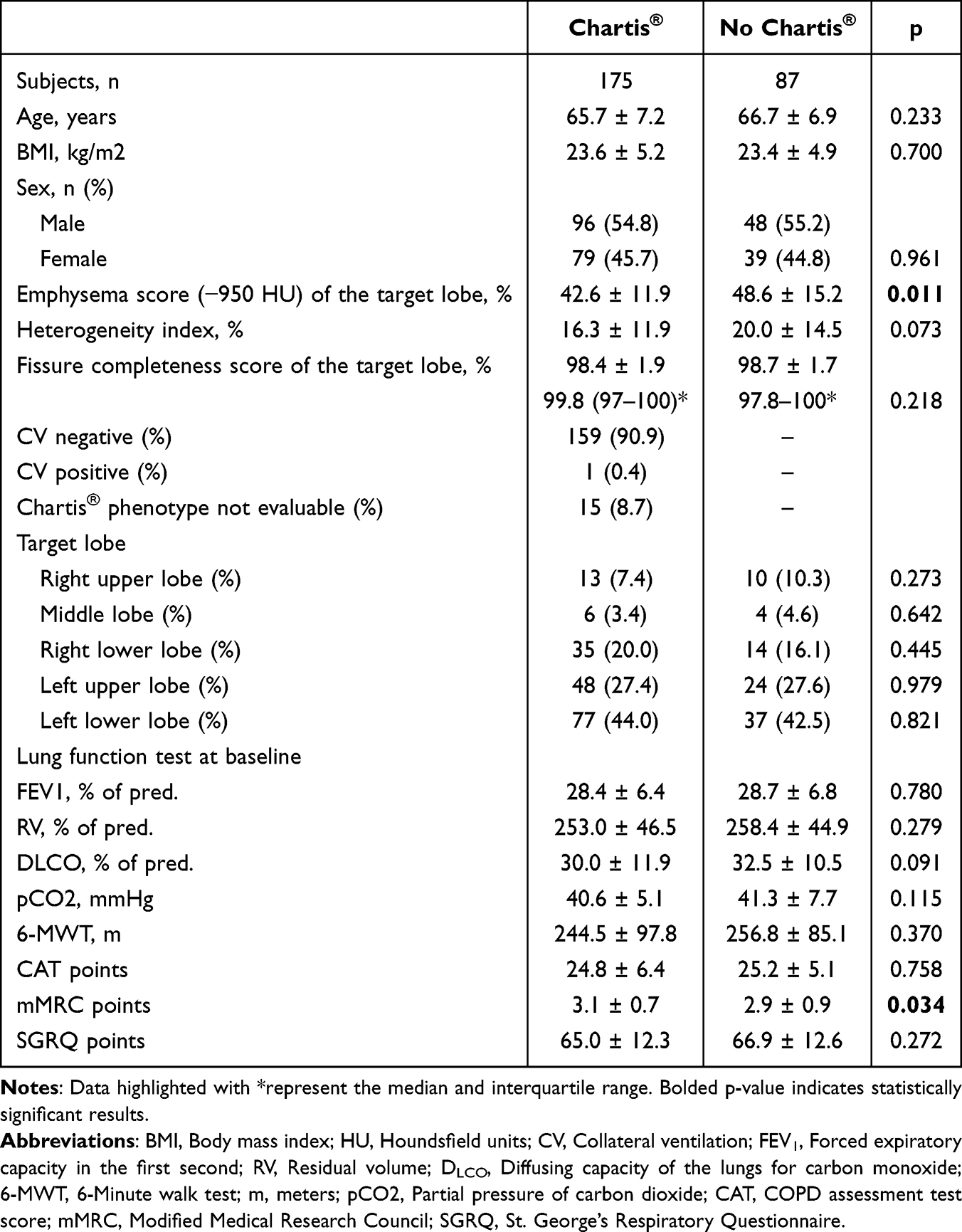 |
Table 1 Baseline Parameters of Study Population |
Clinical Trajectories in Patients with or Without Chartis®
Patients with Chartis® showed significant improvements in lung function parameters (FEV1, RV, DLCO), 6-MWT, CAT, mMRC and SGRQ were seen between baseline and 3-month follow-up (Table 2). The patient with a CV positive Chartis® assessment presented with an improvement in FEV1 of 4% and a reduction in RV of 39%. Additionally, the 6-MWT improved by 60m for follow-up. Similarly, significant improvements were seen in the no Chartis® group for the above-mentioned parameters, while there were also no changes in DLCO (Table 2).
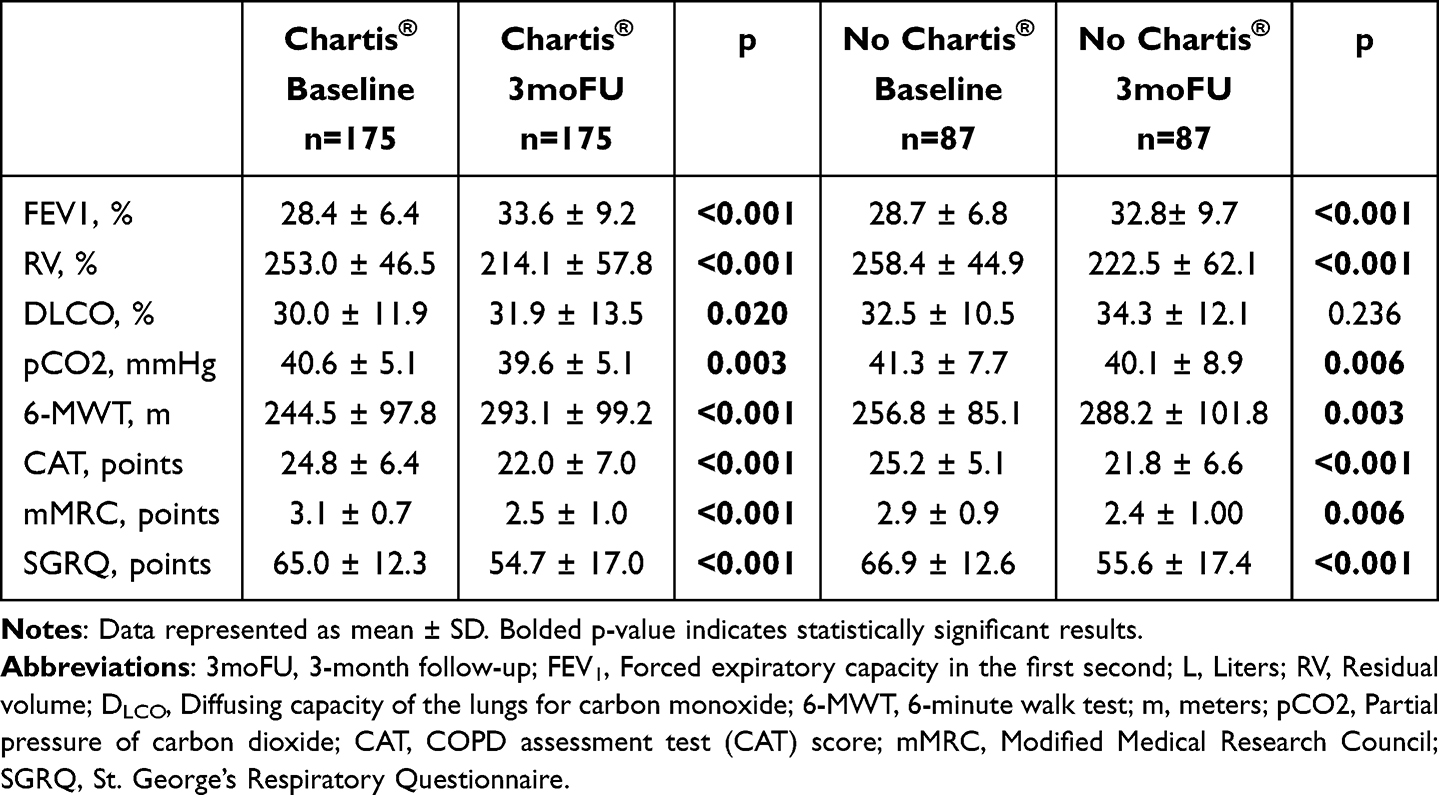 |
Table 2 Changes Between Baseline and 3-month Follow up in Patients with an Intact Fissure with and Without Chartis |
Comparison of 3-month Outcome in Patients with or Without Chartis®
No differences in the overall treatment response at 3-month follow-up were observed with regards to FEV1, RV, DLCO, pCO2, 6-MWT, CAT, mMRC and SGRQ (Table 3).
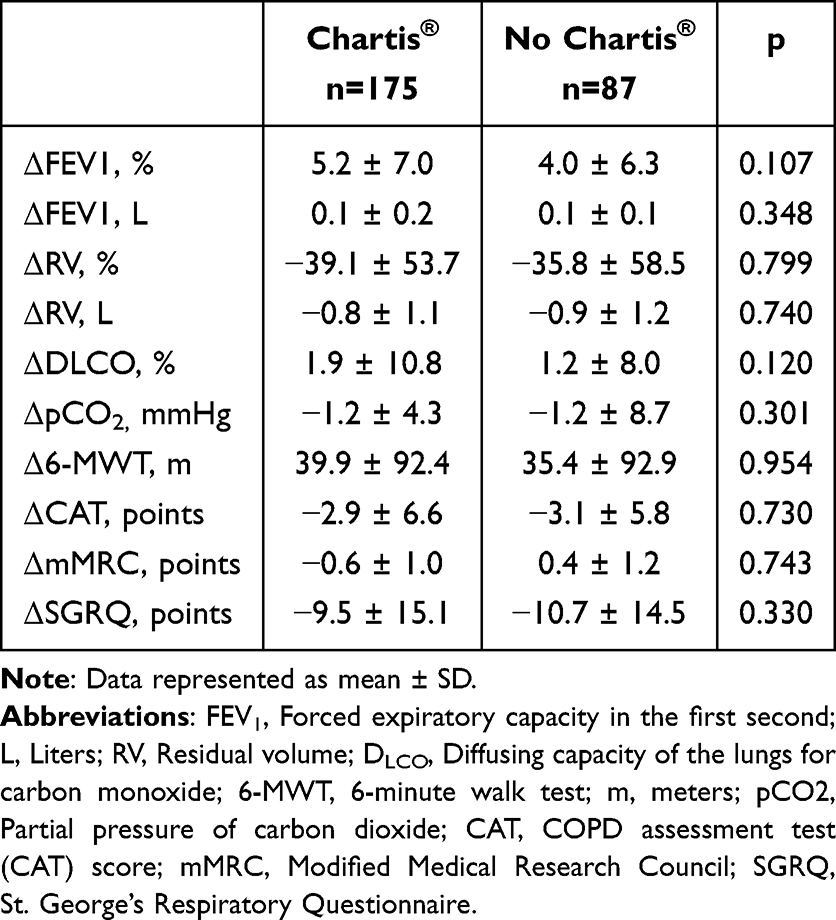 |
Table 3 Comparison of 3-month Follow-up in Patients with an Intact Fissure with and Without Chartis |
Due to the small number of patients treated in the right upper lobe and right middle lobe, an analysis of treatment outcomes for each lung lobe separately was not possible. However, a subgroup analysis of the treatment response at the 3-month follow-up, comparing the right and left lung separately, showed similar improvements in lung function parameters (FEV1, RV, DLCO, pCO2), 6-minute walk test (6-MWT), and quality of life measures (CAT, mMRC, and SGRQ) (Table 4).
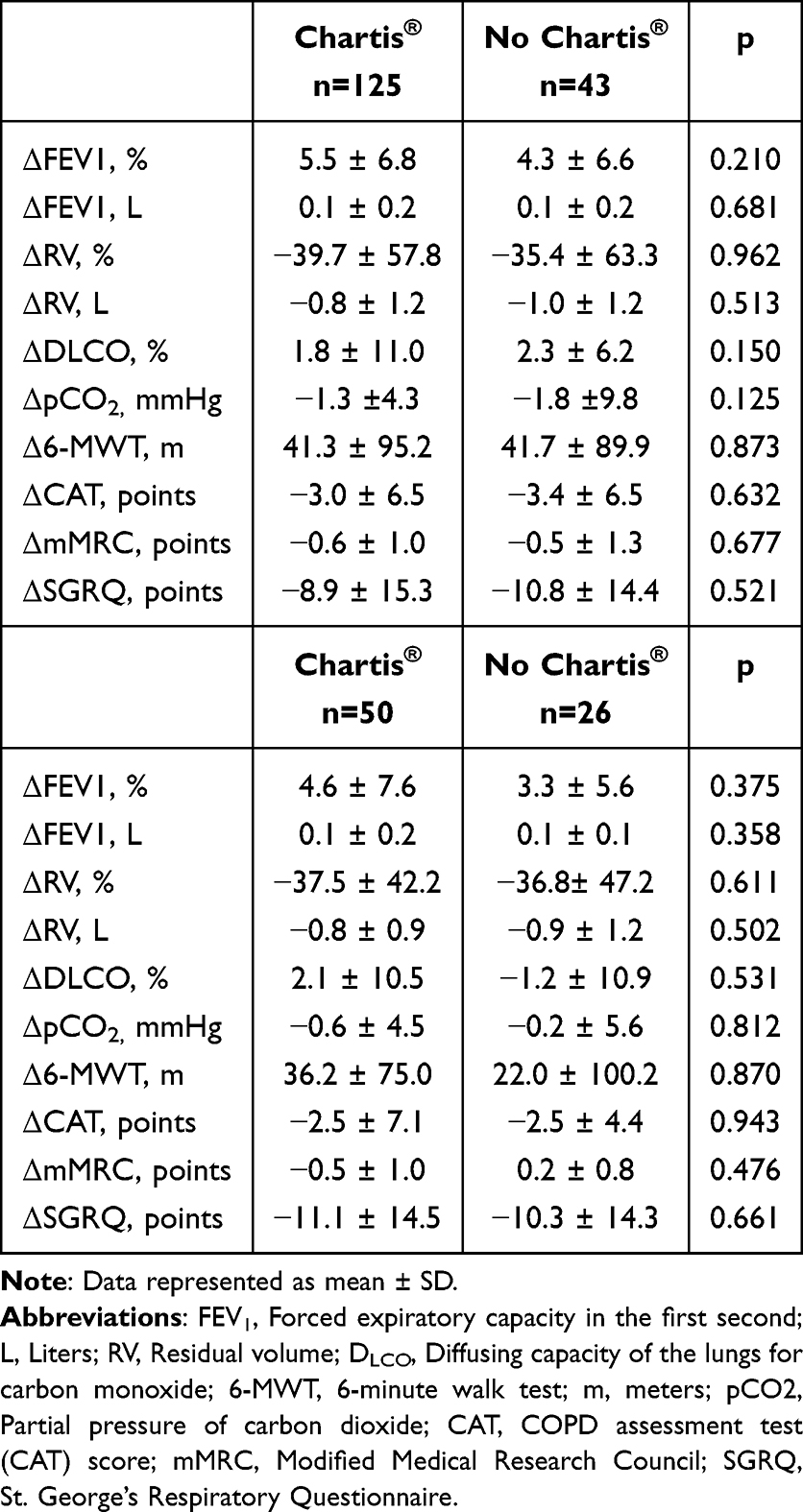 |
Table 4 Comparison of 3-month Follow-up Between Both Groups in the Left Lung and Right Lung |
The MCID Showed Similar Results for FEV1, RV, 6-MWT and SGRQ in Both Groups (Table 5)
Adverse Events During the 3-month Follow-up Period in Patients with or Without Chartis®
The only notable difference in adverse events between the groups was a higher pneumothorax rate in the no-Chartis® group (22% vs 7%). All other complications, including ICU admissions, mechanical ventilation, sepsis, bleeding, pneumonia, COPD exacerbations, and valve removal, occurred in less than 10% of patients. Notably, no patient died during the follow-up period (Table 6).
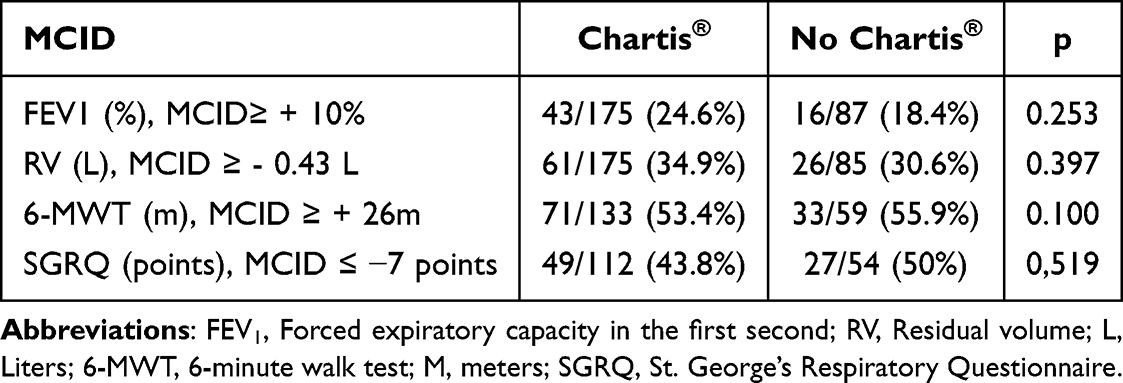 |
Table 5 Minimal Clinically Important Difference (MCID) in Patients with an Intact Fissure with and Without Chartis |
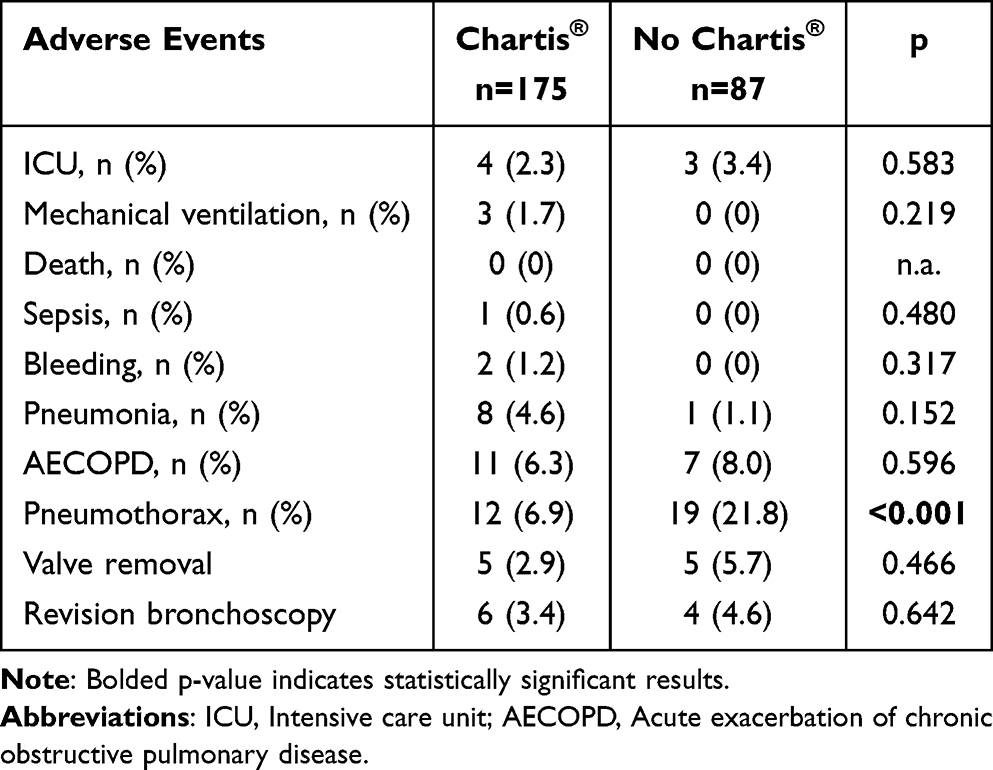 |
Table 6 Adverse Events During the 3-month Follow-up Period |
Discussion
The aim of this study was to quantify the impact of Chartis® assessment in addition to CT-based fissure quantification with a FCS ≥95%. This impact was quantified as clinical treatment response 3-month follow-up after ELVR as compared to baseline. This analysis identified, that in the majority of emphysema centers a fissure with an FCS≥95% is considered complete and that in 12/20 of these centers ELVR with valves is performed without additional Chartis® measurement. This study showed no impact on treatment outcome at 3-month follow-up after ELVR with valves in patients with intact fissure of the target lobe regardless whether Chartis® assessment was performed or not. Furthermore, this study did not find differences in treatment outcome at 3-month follow-up for the right or left lung separately. Noteworthy that treatment response at 3-month follow-up was in line with previously published data from this cohort.22,31–34
The exact diagnostic algorithm to assess CV remains controversial, and randomized controlled trials approached CV differently. In the BeLieVeR-HIFi and VENT trial study fissure integrity was visually assessed and if deemed intact an ELVR with valves was performed. In the STELVIO trial Chartis® was always performed and additionally the fissure was evaluated visually and if exceeding ≥90% it was considered intact. In EMPROVE, and REACH, patients with an FCS of ≥90% were treated. The LIBERATE, IMPACT and TRANSFORM study did not use the FCS and relied only on Chartis® measurement for CV assessment.6,8,15–19,35
A few studies investigated the diagnostic value of FCS and tried to identify the optimal cut-off for FCS to predict significant treatment approach. Gompelmann et al used a visually assessed FCS ≥90% and found a 77% treatment success defined by a significant target lobe reduction of ≥350mL.36 However, several studies proved interrater reliability for fissure integrity analysis to be only moderate so that more precise quantitative software based fissure analysis is currently considered to be the standard.37 Schumann et al compared quantitative imaging software with FCS to Chartis® in retrospective analysis and found a comparable accuracy of 75.5%.12 In a large retrospective analysis, where data from four large prospective studies was pooled, Koster et al challenged the previously widely used cut-off of ≥90% and suggested an FCS of 95% as optimal cut-off with a higher positive predictive value of 88.1% in predicting a CV negative status and significant treatment response after ELVR.11 Considering these results, it seems reasonable that most consulted centers of the lung emphysema registry use FCS≥95% to define an intact fissure.
In a recently published study, Klooster et al evaluated a fissure-dependent approach using an FCS-only assessment for patients with an intact fissure integrity of ≥95% in the left lung. However, for the right lung, they recommended an additional Chartis® assessment in patients with an FCS of ≥90%. These recommendations were based on Receiver Operating Characteristic (ROC) curves, which predicted Chartis® outcomes based on FCS. The analysis estimated a 26.8% likelihood of a CV-positive result in cases with an FCS ≥95% in the right upper lobe fissure and 18.8% when FCS was 100%. For the right lower lobe, the predicted likelihood of a CV-positive result was 26.3% for an FCS≥95% and 14.3% for an FCS of 100%. The most likely reason for the lower number of CV-positive patients is that only those who underwent ELVR were included in the registry, and therefore CV positive patients who were not treated may have been excluded. However, the key difference between this study and our analysis is that treatment outcomes after ELVR were not evaluated and that our analysis focuses exclusively on patients with a FCS≥95% making it a more specific representation of this subgroup. The authors hypothesized that FCS might be less precise in the right lung, as fissure defects are often centrally located due to the more complex anatomy, potentially affecting the accuracy of software-based analysis.20 When describing the rationale to perform Chartis® in patients with intact fissures based on CT-assessment, the centers of the lung emphysema registry mainly quoted differences in diagnostic accuracy of the FCS between the right and left lung as described by Klooster et al. However, this study did not find a difference in treatment response after ELVR between the groups, even when analyzing treatment outcome for the right and left lung separately, and questions the benefit of an additional Chartis® measurement in case of an intact fissure. Compared to the aforementioned publication, the main strength of our analysis is the inclusion of treatment outcomes after ELVR in patients with intact fissures. Notably, treatment outcomes in the Chartis® group where all patients but one were CV negative on Chartis® assessment were comparable to those in the group selected based on FCS alone. This is particularly noteworthy given that, according to the Klooster study, up to 26% of patients in the no-Chartis® group for the right lung may have been CV positive had they undergone Chartis® measurement—and might not have been treated as a result.
Chartis® is a technically complex and time-intensive procedure, that was developed to identify patients suitable for ELVR with valves in a time where quantitative fissure analysis was not readily available.9 Even though the new VT20 software feature reduces the measurement duration in CV negative patients, Chartis® outcome depends on factors such as endobronchial secretion, sedation and it is more demanding in the right lung.10 Additionally, we previously found discordant Chartis® results in up to 13% of cases when the same lobe was assessed twice during the same procedure, independently of FCS values or ventilation mode.23 However, today quantitative fissure analysis is widely used and the patients included in this analysis had very high FCS values in both groups, so that additional benefit of Chartis® assessment is questionable.
When comparing the outcomes of this analysis with the EMPROVE and REACH studies, in which patients with FCS ≥90% underwent ELVR, similar improvements were observed: FEV1 increased by approximately 100 mL, RV decreased by around 450 mL, and SGRQ improved by approximately −8 points. The only notable difference was in the 6-MWT: while EMPROVE reported a mean decrease of −4.4 ± 76.7 m, the REACH study showed an increase of 27.2 ± 80 m. In our study, the FEV1 improvement of approximately 100 mL aligns with these randomized controlled trials. However, the observed changes in RV (−800 mL), 6-MWT (+40 m), and SGRQ (−10 points) suggest slightly greater improvements in our study population. This indicates that an FCS ≥95% is an excellent discriminator for treatment response alone.15,16
Limitations of this study might be selection bias due the retrospective nature. However, all patients undergoing LVR were prospectively included in this large multicentric registry. The most significant limitation of this study is the potential selection bias that patients with a CV positive result on Chartis® assessment might not have been treated and were therefore not included in this study meaning that an incomplete dataset in regards to Chartis® outcome was reported. Considering that with additional Chartis® were almost exclusively CV negative and still treatment results were comparable in the no Chartis® groups at follow-up supports the interpretation that an additional Chartis assessment adds little information. A potentially interesting information would have been atelectasis rates of the target lobe in patients with FCS≥95% and evidence of CV in Chartis® assessment. However, the fact that treatment outcome for both groups was comparable renders this unlikely. Another interesting question would have been the impact of Chartis® assessment on treatment outcome in case of an intermediate FCS. Unfortunately, our registry could not provide insights in these cases because scientific and clinical standards recommend Chartis® assessment of CV in patients with an intermediate FCS. Accordingly, in patients with an intermediate FCS do not undergo ELVR without prior Chartis® assessment. Potentially, a RCT would help answer this question. A separate analysis comparing the two groups for each lobe separately would have been interesting, however the number of cases receiving ELVR simultaneously in the middle lobe and right lower lobe was too small. Nevertheless, treatment results at 3-month follow-up were comparable between the right and left lung and in line with previous publications. Therefore, an analysis of treatment outcome for each pulmonary lobe separately might add little information. Another potential bias could arise from variations in CV assessment among centers. The lung emphysema registry aims to generate data that reflect real-world clinical practice, where variations in assessment are expected. The inclusion of data from more than 40 specialized emphysema centers, along with a large patient population, may help mitigate potential bias.
This study suggests of whether Chartis® assessment can be omitted in cases where the fissure is intact and FCS ≥95%, allowing ELVR with valves to be performed if recommended by the emphysema board. However, further research—ideally comparing treatment outcomes after ELVR in patients with an intact fissure alone versus those with an intact fissure plus Chartis® assessment, regardless of the Chartis® phenotype—is needed to confirm these findings.
Data Sharing Statement
Data can be made available on request to the corresponding author.
Statement of Ethics
The research presented in this article was conducted according to the standards of the World Medical Association Declaration of Helsinki and the appropriate guidelines for human studies. All data were derived from prospective open-label clinical studies in our institution which were approved by the Ethics Committee of the Charité Universitätsmedizin Berlin, Germany (EA2/149/17 and EA1/136/13). All patients consented to participation. Inability to sign the consent form was an exclusion criterion.
Acknowledgment
The authors sincerely thank CAP NETZ, Berlin Institute of Health (BIH), data management: Laura Grebe and Andreas Hetey for editing support. We would like to thank Monika Rummenholl from the Lungenemphysemregister e.V.
Collaborators
Members of the Lung Emphysema Registry study group:
Nicolas Dickgreber1, Christian Geltner2, Joachim H. Ficker3, Angelique Holland4, Björn Schwick5, Stephan Eggeling6, Ralf Eberhardt7, Christian Grah8, Christoph Hünermann9, Urte Sommerwerck10, Andreas Fertl11, Sylke Kurz112, Peter Schramm113, Joanna Krist14, Grit Barten-Neiner 141 Department of Respiratory Medicine and Thoracic Oncology – Klinikum Rheine – Matthias Spital – Rheine, Germany
2 Department of Respiratory Medicine – Donauisar Klinikum Deggendorf – Landau an der Isar - Germany
3 Department of Internal Medicine 3 / Respiratory Medicine, Klinikum Nuernberg, Paracelsus Medical University, Nuernberg, Germany
4 Department of Respiratory Medicine, Universitätsklinikum Gießen und Marburg GmbH, Marburg, Germany
5 Department of Respiratory Medicine, Luisenhospital Aachen, Germany
6 Department of Thoracic Surgery, Vivantes-Klinikum Neukölln, Berlin, Germany
7 Department of Pneumology and Critical Care Medicine, Asklepios Klinik Barmbek, Hamburg, Germany
8 Department of Respiratory Medicine, Klinik Havelhöhe Berlin, Berlin, Germany
9 Department of Respiratory Medicine – St. Raphael Hospital – Niels-Stensen Kliniken, Ostercappeln Germany
10 Department of Respiratory Medicine, Allergology, Sleeping Medicine – Krankenhaus der Augusterinnen – Cellitinnen Severinsklösterchen, Cologne, Germany
11 Department of Internal Medicine and Respiratory Medicine, Krankenhaus Martha-Maria München, München, Germany
12 Department of Respiratory Medicine – Evangelische Lungenklinik Berlin – Johannesstift Diakonie, Berlin, Germany
13 Department of Respiratory Medicine and Thoracic Oncology, München Klinik Bogenhausen, Munich, Germany
14 Department of Respiratory Medicine, Lungenklinik Heckeshorn, Helios Klinikum Emil von Behring, Berlin, Germany
15 Capnetz Foundation, Hannover, Germany
Funding
No funding was received for this study. The support provided by the CAPNETZ STIFTUNG was free of charge.
Disclosure
Jacopo Saccomanno reports Payment or honoraria for lectures, presentations from PulmonX, Support for attending meetings and/or travel Medtronic. Member of Lungenemphysemregister e.V.
Stefan Andreas reports Consulting fees from Sanofi. Payment/honoraria for lectures from Boehringer Ingelheim, Novartis, AstraZeneca, GSK, Chiesi, Merini. Support for attending meetings and/or travel from Boehringer Ingelheim. He is speaker of the Section “Tabakentwöhnung” at DGP and board member of the ABNR.
Stephan Eisenmann reports Consulting fees for Acceleron, Boehringer, Astra Zeneca, Bess. Payment or honoraria for lectures and presentation fpr PulmonX, Travel Support from Boehringer and Astra Zeneca. Participation on data safety monitoring ´board / advisory board for Astra Zeneca and Zanofi
Dr Wolfgang Gesierich reports personal fees from Astra Zeneca, outside the submitted work.
Prof. Dr. Martin Witzenrath reports grants from Bundesministerium für Forschung, Technologie und Raumfahrt (BMFTR; Federal Ministry of Research, Technology and Space), grants from Deutsche Forschungsgemeinschaft (DFG; German Research Foundation), grants from Gemeinsamer Bundesausschuss (G-BA; The Federal Joint Committee), grants from Bundesministerium für Gesundheit (BMG; Federal Ministry of Health), grants, personal fees from Biotest, Pantherna and Aptarion, personal fees from Astra Zeneca, Chiesi, Insmed, Gilead, Pfizer and Boehringer, outside the submitted work.
Ralf Harto Hübner: Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events by Pulmonx, Astra Zeneca, GSK, Berlin Chemie, Olympus, Chiesi GmbH. Support for attending meetings and/or travel from Medtronic, Astra Zeneca, Boehringer Ingelheim. Head of Lungenemphysemregister.
The authors report no other conflicts of interest in this work.
References
1. Stolz D, Mkorombindo T, Schumann DM, et al. Towards the elimination of chronic obstructive pulmonary disease: a lancet commission. Lancet. 2022;400(10356):921–972. doi:10.1016/S0140-6736(22)01273-9
2. Hogg JC, Chu F, Utokaparch S, et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(26):2645–2653. doi:10.1056/NEJMoa032158
3. Agustí A, Hogg JC. Update on the pathogenesis of chronic obstructive pulmonary disease. N Engl J Med. 2019;381(13):1248–1256. doi:10.1056/NEJMra1900475
4. Rennard SI. COPD: overview of definitions, epidemiology, and factors influencing its development. Chest. 1998;113(4 Suppl):235S–241S. doi:10.1378/chest.113.4_Supplement.235S
5. Herth FJF, Eberhardt R, Gompelmann D, et al. Radiological and clinical outcomes of using Chartis™ to plan endobronchial valve treatment. Eur Respir J. 2013;41(2):302–308.
6. Criner GJ, Sue R, Wright S, et al. A multicenter randomized controlled trial of zephyr endobronchial valve treatment in heterogeneous emphysema (LIBERATE). Am J Respir Crit Care Med. 2018;198(9):1151–1164.
7. Hübner RH, Gloesenkamp C, Saccomanno J, et al. Endoscopic lung volume reduction: can endobronchial valves be safely removed? Respiration. 2020;99:1–2.
8. Sciurba FC, Ernst A, Herth FJF, et al. A randomized study of endobronchial valves for advanced emphysema. N Engl J Med. 2010;363(13):1233–1244. doi:10.1056/NEJMoa0900928
9. Aljuri N, Freitag L. Validation and pilot clinical study of a new bronchoscopic method to measure collateral ventilation before endobronchial lung volume reduction. J Appl Physiol. 2009;106(3):774–783. doi:10.1152/japplphysiol.91075.2008
10. Saccomanno J, Hübner RH, Witzenrath M, et al. Bronchoscopic measurement of collateral ventilation: state of the art. Respiration. 2023;102(4):296–307. doi:10.1159/000528419
11. Koster TD, van Rikxoort EM, Huebner RH, et al. Predicting lung volume reduction after endobronchial valve therapy is maximized using a combination of diagnostic tools. Respiration. 2016;92(3):150–157. doi:10.1159/000448849
12. Schuhmann M, Raffy P, Yin Y, et al. Computed tomography predictors of response to endobronchial valve lung reduction treatment. comparison with Chartis. Am J Respir Crit Care Med. 2015;191(7):767–774. doi:10.1164/rccm.201407-1205OC
13. de Oliveira HG, de Oliveira SM, Rambo RR, de Macedo Neto AV. Fissure integrity and volume reduction in emphysema: a retrospective study. Respiration. 2016;91(6):471–479. doi:10.1159/000446288
14. Fiorelli A, Poggi C, Anile M, et al. Visual analysis versus quantitative CT analysis of interlobar fissure integrity in selecting emphysematous patients for endobronchial valve treatment. Interactive CardioVascul Thoracic Surg. 2019;28(5):751–759.
15. Criner GJ, Delage A, Voelker K, et al. Improving lung function in severe heterogenous emphysema with the spiration valve system (EMPROVE). A multicenter, open-label randomized controlled clinical trial. Am J Respir Crit Care Med. 2019;200(11):1354–1362.
16. Li S, Wang G, Wang C, et al. The REACH trial: a randomized controlled trial assessing the safety and effectiveness of the spiration® valve system in the treatment of severe emphysema. Respiration. 2019;97(5):416–427. doi:10.1159/000494327
17. Valipour A, Slebos DJ, Herth F, et al. Endobronchial valve therapy in patients with homogeneous emphysema. results from the IMPACT study. Am J Respir Crit Care Med. 2016;194(9):1073–1082. doi:10.1164/rccm.201607-1383OC
18. Davey C, Zoumot Z, Jordan S, et al. Bronchoscopic lung volume reduction with endobronchial valves for patients with heterogeneous emphysema and intact interlobar fissures (the BeLieVeR-HIFi trial): study design and rationale. Thorax. 2015;70(3):288–290. doi:10.1136/thoraxjnl-2014-205127
19. Kemp SV, Slebos DJ, Kirk A, et al. A multicenter randomized controlled trial of zephyr endobronchial valve treatment in heterogeneous emphysema (TRANSFORM). Am J Respir Crit Care Med. 2017;196(12):1535–1543. doi:10.1164/rccm.201707-1327OC
20. Klooster K, Koster TD, Ruwwe-Glösenkamp C, et al. An integrative approach of the fissure completeness score and Chartis assessment in endobronchial valve treatment for emphysema. Int J Chron Obstruct Pulmon Dis. 2020;15:1325–1334. doi:10.2147/COPD.S242210
21. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Informat. 2019;95:103208.
22. Saccomanno J, Kilic L, Sgarbossa T, et al. Clinical improvements after endoscopic lung volume reduction with valves in patients with advanced emphysema and a 6-minute-walk-test ≤140 m at baseline. Erjor. 2024;11:00410–2024.
23. Saccomanno J, Ruwwe-Glösenkamp C, Neumann K, et al. Impact of ventilation modes on bronchoscopic Chartis assessment outcome in candidates for endobronchial valve treatment. Respiration. 2022;101(4):408–416. doi:10.1159/000520082
24. Herzog D, Thomsen C, Poellinger A, et al. Outcomes of endobronchial valve treatment based on the precise criteria of an endobronchial catheter for detection of collateral ventilation under spontaneous breathing. Respiration. 2016;91(1):69–78. doi:10.1159/000442886
25. Saccomanno J, Sgarbossa T, Pappe E, et al. VT20 method for Chartis® assessment of collateral ventilation with flexible bronchoscopy under procedural sedation. Erjor. 2024;10:00945–2023.
26. Koster TD, Klooster K, McNamara H, et al. An adjusted and time-saving method to measure collateral ventilation with Chartis. ERJ Open Res. 2021;7(3):00191–2021.
27. Jones PWS. George’s respiratory questionnaire: MCID. COPD. 2005;2(1):75–79. doi:10.1081/COPD-200050513
28. Donohue JF. Minimal clinically important differences in COPD lung function. COPD. 2005;2(1):111–124. doi:10.1081/COPD-200053377
29. Hartman JE, Ten Hacken NHT, Klooster K, Boezen HM, de Greef MHG, Slebos DJ. The minimal important difference for residual volume in patients with severe emphysema. Eur Respir J. 2012;40(5):1137–1141. doi:10.1183/09031936.00219111
30. Puhan MA, Chandra D, Mosenifar Z, et al. The minimal important difference of exercise tests in severe COPD. Eur Respir J. 2011;37(4):784–790. doi:10.1183/09031936.00063810
31. Lenga P, Ruwwe-Glösenkamp C, Grah C, et al. Endoscopic lung volume reduction with endobronchial valves in very low D (LCO) patients: results from the german registry - lungenemphysemregister e.V. ERJ Open Res. 2021;7(1):00449–2020. doi:10.1183/23120541.00449-2020
32. Lenga P, Grah C, Ruwwe-Glösenkamp C, et al. Endoscopic lung volume reduction with one-way valves in patients with severe chronic obstructive pulmonary disease with hypercapnia. Respiration. 2022; 101.
33. Sgarbossa T, Lenga P, Stanzel F, et al. Assessment of efficacy and safety of endoscopic lung volume reduction with one-way valves in patients with a very low FEV1. erjor. 2023;9(4):00190–2023.
34. Sgarbossa T, Borchers P, Saccomanno J, et al. Comparison of efficacy and safety of different types of one-way valves in endoscopic lung volume reduction in patients with severe lung emphysema. Respiration. 2024; 2024:1–16.
35. Klooster K, ten Hacken NHT, Hartman JE, Kerstjens HAM, van Rikxoort EM, Slebos DJ. Endobronchial valves for emphysema without interlobar collateral ventilation. N Engl J Med. 2015;373(24):2325–2335. doi:10.1056/NEJMoa1507807
36. Gompelmann D, Eberhardt R, Slebos DJ, et al. Diagnostic performance comparison of the Chartis system and high-resolution computerized tomography fissure analysis for planning endoscopic lung volume reduction. Respirology. 2014;19(4):524–530. doi:10.1111/resp.12253
37. Hartman JE, Criner GJ, Moore WH, et al. HRCT characteristics of severe emphysema patients: interobserver variability among expert readers and comparison with quantitative software. Eur J Radiol. 2021;136:109561. doi:10.1016/j.ejrad.2021.109561
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Synchronous Video-Assisted Thoracoscopic Fissure Closure and Endoscopic Lung Volume Reduction Using Endobronchial Valves in a Patient with Less Than 20% Fissure Completeness: A Case Report
Di Campli MP, Vander Kuylen M, Perez Bogerd S, Etienne I, Knoop C, Taton O
International Medical Case Reports Journal 2026, 19:567072
Published Date: 20 March 2026
Endoscopic Lung Volume Reduction with Valves Improves Cardiovascular Adaptability and 6-MWT Performance in Severely Limited COPD Patients
Farber L, Pappe E, Sgarbossa T, Neumann K, Witzenrath M, Hübner RH, Saccomanno J
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:592263
Published Date: 17 June 2026