Back to Journals » International Medical Case Reports Journal » Volume 19
Synchronous Video-Assisted Thoracoscopic Fissure Closure and Endoscopic Lung Volume Reduction Using Endobronchial Valves in a Patient with Less Than 20% Fissure Completeness: A Case Report
Authors Di Campli MP ![]() , Vander Kuylen M, Perez Bogerd S
, Vander Kuylen M, Perez Bogerd S ![]() , Etienne I, Knoop C, Taton O
, Etienne I, Knoop C, Taton O ![]()
Received 12 September 2025
Accepted for publication 2 February 2026
Published 20 March 2026 Volume 2026:19 567072
DOI https://doi.org/10.2147/IMCRJ.S567072
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Maria-Pia Di Campli,1,* Maarten Vander Kuylen,1,* Silvia Perez Bogerd,2 Isabelle Etienne,2 Christiane Knoop,2 Olivier Taton2
1Department of Thoracic Surgery, Erasme University Hospital, Brussels, Belgium; 2Department of Pulmonology, Erasme University Hospital, Brussels, Belgium
*These authors contributed equally to this work
Correspondence: Maria-Pia Di Campli, Department of Thoracic Surgery, Erasme University Hospital, Route de Lennik 808, Anderlecht, Brussels, 1070, Belgium, Tel +32 2 555 6582, Email [email protected]
Abstract: Endoscopic lung volume reduction (ELVR) using endobronchial valves (EBV) is an effective treatment for selected patients with severe emphysema and hyperinflation. However, its success relies on the absence of collateral ventilation (CV), typically requiring complete interlobar fissures. We report a unique case of a single-session combined surgical and ELVR approach in a patient with severe homogeneous emphysema fissure completeness below 20% on the left side. Intraoperative Pulmonary Assessment System (Chartis®, Pulmonx, Redwood City, CA, USA) confirmed the presence of CV before, and its absence after surgical stapling of the interlobar fissure by video-assisted thoracoscopic surgery (VATS). The immediate postoperative course was uneventful. Postoperative chest imaging revealed atelectasis of the left lower lobe, resulting in improved quality of life, pulmonary function, and exercise capacity. This case suggests the potential feasibility and clinical benefit of a combined VATS-ELVR approach in well-selected patients with markedly incomplete fissures, when performed in experienced centers.
Keywords: COPD, combined VATS-ELVR, VATS inter-lobar fissure completion, collateral ventilation, case report
Introduction
A successful endoscopic lung volume reduction (ELVR) with endobronchial valves (EBVs) in patients with severe emphysema and hyperinflation can lead to a clinically significant improvement in lung function, exercise capacity, and quality of life.1–3 However, patients with fissure completeness <80% are typically excluded due to the high likelihood of collateral ventilation (CV).4
Recent studies have evaluated the role of video-assisted thoracoscopic surgery (VATS) fissure completion to enable EBV therapy in patients with CV or as rescue treatment after failed ELVR.5,6 However, no cases have been reported in the literature involving fissure completeness below 20%, likely due to the increased technical difficulty of stapling severely incomplete or fused fissures during VATS.7 Here we present a unique case of a single-session VATS-ELVR procedure in a patient with 19% fissure integrity.
Case Report
A 48-year-old woman with a 70 pack-year smoking history presented with dyspnea and limited exercise capacity. Of note, her medical history included cardiac pacemaker implantation at age 2 following interatrial septal defect closure. Despite optimal medical management, pulmonary function tests showed severe hyperinflation and significant self-reported health-impairment (Table 1).
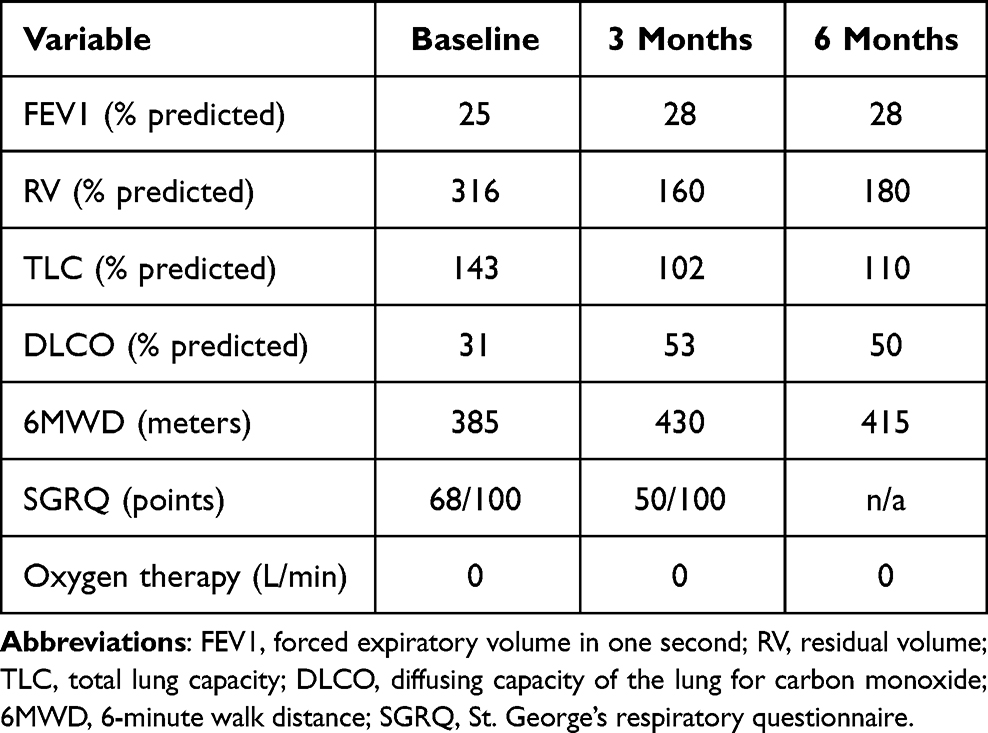 |
Table 1 Pulmonary Function Test, Exercise Capacity Assessment, Oxygen Requirements and Quality of Life Evaluation Before and After the Combined VATS-ELVR Procedure |
CT scan revealed homogeneous emphysema without potential targets for lung volume reduction surgery (LVRS) (Figure 1). Perfusion scan (StratX® Lung Analysis Platform, Pulmonx, Redwood City, CA, USA) showed predominant parenchymal destruction in the left lower lobe, with fissure integrity below 20% (Figure 2). After multidisciplinary evaluation and detailed discussion involving pulmonologists, transplant specialists, radiologists and thoracic surgeons, a single-session approach combining VATS fissure closure and ELVR of the left lower lobe was proposed to the patient who gave her informed consent.
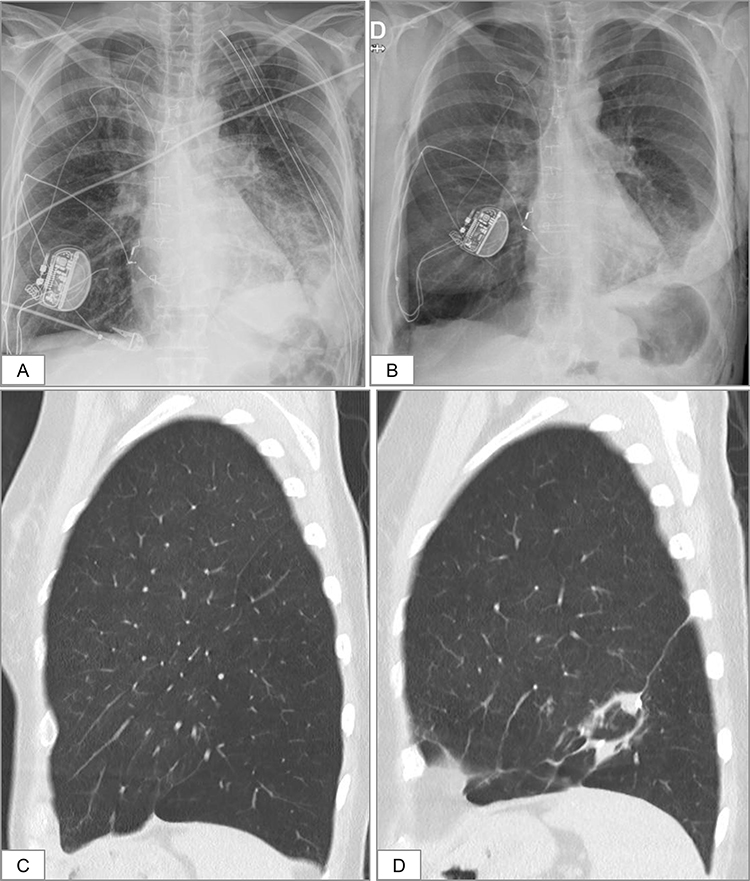 |
Figure 1 (A) Chest X-ray at POD 1 and (B) upright chest X-ray at POD 6 after chest tube removal, showing atelectasis of the left lower lobe (LLL); Chest CT scan at baseline (C) and at 3 months postoperative (D) demonstrating homogeneous emphysema and atelectasis of the LLL after the VATS-ELVR procedure, respectively; D upright chest X-ray; POD: postoperative day. |
 |
Figure 2 Perfusion scan (StratX® Lung Analysis Platform, Pulmonx, Redwood City, CA, USA) revealing predominant parenchymal destruction in the left lower lobe (gray highlighting indicating 60% voxel density less than −910 HU in the LLL versus 50% in the RLL), with only 19% fissure completeness. Abbreviations: RUL, right upper lobe; RLM, middle lobe; RLL, right lower lobe; LUL, left upper lobe; LLL, left lower lobe; HU, Hounsfield units. |
Intraoperative Pulmonary Assessment System (Chartis®, Pulmonx, Redwood City, CA, USA) evaluation demonstrated the presence of CV (Figure 3). Pleural adhesiolysis and interlobar fissure stapling using the tunnel technique, as described by Decaluwé et al for fissure-first anatomical lung resections, were performed via a triportal VATS approach under general anesthesia using a single-lumen endotracheal tube with a bronchial blocker8 Stapling of the fissure was performed using a 60-mm powered Echelon Flex stapler with blue cartridges. No air leaks were detected at the end of the procedure. Two chest tubes were inserted through the trocars incisions. Three Zephyr® endobronchial valves (Pulmonx, Redwood City, CA, USA) were placed in the left lower lobe after confirming the absence of residual CV.
 |
Figure 3 Intraoperative Pulmonary Assessment before (A) and after (B) surgical stapling of the interlobar fissure via video-assisted thoracoscopic surgery (VATS), confirming the presence of collateral ventilation (CV) prior to fissure closure and its absence following stapling. The horizontal axis represents time (seconds), and the vertical axis represents expiratory volume (mL). The white asterisk (*) indicates Pulmonary Assessment System (Chartis®, Pulmonx, Redwood City, CA, USA) balloon deflation. |
The patient had an uneventful recovery with atelectasis confirmed radiologically on postoperative days (POD) 1 and 6 (day of discharge) (Figure 1). Subsequently, she showed significant improvements in quality of life (3-month follow-up), lung function and exercise capacity (3- and 6-month follow-up) (Table 1). Unfortunately, she resumed smoking a few months after the procedure and an unexpected sudden death occurred at 7 months postoperative. Post-arrest chest CT showed no pulmonary abnormalities attributable to the VATS-ELVR procedure. Despite multiple atrial fibrillation episodes recorded by her pacemaker, the exact cause of death remains unclear, though a cardiac origin is favored due to her medical history.
Discussion
This is the first reported case of a single-session VATS fissure closure and ELVR in a patient with only 19% fissure completeness. Although this combined procedure has been used as rescue therapy post EBV placement in patients with ≥80% major fissure integrity, our case suggests that even patients with severely incomplete fissures may benefit from a synchronous hybrid approach.5
This strategy could offer several physiological and technical advantages: endotracheal intubation with target lung isolation enables controlled lobar collapse, while VATS adhesiolysis—if needed—can promote faster atelectasis while reducing the risk of parenchymal tearing post-EBV placement. Additionally, chest tube placement decreases the risk of life-threatening pneumothorax, a complication seen in up to 30% of stand-alone ELVR procedures.9
This combined approach could expand the pool of patients eligible for lung volume reduction, particularly those who are not candidates for either LVRS or ELVR alone. While current evidence supports this combined strategy mainly as salvage therapy after failed ELVR, the ongoing COMPLETE-1 trial is evaluating its efficacy as an upfront treatment in patients with <95% fissure completeness, with EBV placed during the same session or within 48 hours of VATS fissure closure.5,10
Limitations of this approach include longer procedural time compared to ELVR or LVRS alone, and VATS-specific complications such as bleeding or prolonged air leak. These can be minimized when the procedure is performed by surgical teams experienced in minimally invasive fissure-first, hilum-last lung resections, particularly in safely stapling incomplete interlobar fissures without injuring pulmonary arteries, veins, or airways, as described in the thoracoscopic tunnel technique for anatomical fissure-first lung resections.8 Although chest tubes may contribute to postoperative pain, they might help reduce the morbidity and mortality associated with pneumothorax following EBV placement. Given the limited follow-up period of this case, further studies with longer follow-up are warranted to assess the safety and efficacy of this combined procedure.
Conclusion
Our case suggests that a synchronous VATS–ELVR strategy can effectively eliminate collateral ventilation in carefully selected patients with severe homogeneous emphysema and markedly incomplete fissures who are not considered candidates for standard endoscopic or surgical treatments after thorough multidisciplinary evaluation. When performed in high-volume centers with surgical expertise in thoracoscopic fissure closure, this approach might enable successful lung volume reduction with endobronchial valves even in the setting of less than 20% fissure completeness, leading to meaningful improvements in pulmonary function, exercise capacity, and quality of life.
Declaration of AI-Assisted Technology
Artificial intelligence technology (ChatGPT, GPT-5, OpenAI, 2025) was used solely to assist with improving the medical English and overall readability of the manuscript, as none of the authors are native English speakers. All content edited with AI was carefully reviewed and revised by the authors to ensure accuracy, clarity, and fidelity to the original meaning.
Abbreviations
CT, computed tomography; CV, collateral ventilation; ELVR, endoscopic lung volume reduction; EBV, endobronchial valve; LVRS, lung volume reduction surgery; POD, postoperative day; VATS, video-assisted thoracoscopic surgery.
Consent for Publication
The patient’s family provided consent for publication of this manuscript. Institutional approval was not required to publish this case.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
Olivier Taton and Maarten Vander Kuylen received consultancy fees from PulmonX. The other authors have no conflict of interest to declare for this work.
References
1. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2025 report. Fontana, WI: GOLD; 2025. Available from: https://goldcopd.org/2025-gold-report/.
2. Taton O, Gevenois PA, Van Muylem A, et al. Improvements of the shape and strength of the diaphragm after endoscopic lung volume reduction. Thorax. 2024;79:
3. Labarca G, Uribe JP, Pacheco C, et al. Bronchoscopic lung volume reduction with endobronchial Zephyr valves for severe emphysema: a systematic review and meta-analysis. Respiration. 2019;98:
4. Klooster K, Koster TD, Ruwwe-Glösenkamp C, et al. An integrative approach of the fissure completeness score and Chartis® Pulmonary Assessment System (Pulmonx, Redwood City, CA, USA) assessment in endobronchial valve treatment for emphysema. Int J Chron Obstruct Pulmon Dis. 2020;15:
5. Shafiq M, Polhemus E, Perkins R, et al. Bilateral bronchoscopic lung volume reduction after surgical fissure completion. Chest. 2022;162:
6. Majid A, Ospina-Delgado D, Kheir F, et al. Thoracoscopic surgical stapling as salvage therapy for failed endobronchial valve treatment in patients with incomplete lobar fissures: initial experience. J Bronchol Interv Pulmonol. 2022;29:
7. Lee S, Lee JG. The significance of pulmonary fissure completeness in video-assisted thoracoscopic surgery. J Thorac Dis. 2019;11(Suppl 3):
8. Decaluwé H, Sokolow Y, Deryck F, et al. Thoracoscopic tunnel technique for anatomical lung resections: a ‘fissure first, hilum last’ approach with staplers in the fissureless patient. Interact Cardiovasc Thorac Surg. 2015;21:
9. Lee M, Dhanji AR, Perikleous P, et al. Bronchoscopic lung volume reduction as the treatment of choice versus robotic-assisted lung volume reduction surgery in similar patients with emphysema: an initial experience of the benefits and complications. Int J Chron Obstruct Pulmon Dis. 2024;19:
10. ClinicalTrials.gov. Combined Zephyr Valve System with inter-lobar fissure completion for lung volume reduction in emphysema (COMPLETE-1) [ongoing clinical trial]. NCT04801108. Available from: https://clinicaltrials.gov/study/NCT04801108.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Misdiagnosis of Chronic Heart Failure in Patients with Type 2 Diabetes Mellitus in Primary Care: A Report of Two Cases and Literature Review

Yeshniyazov N, Posokhov IN, Medovchshikov VV, Kurmanalina G, Sartayeva A
Vascular Health and Risk Management 2024, 20:479-485
Published Date: 3 November 2024
Limited Benefit of Additional Chartis® Assessments for Collateral Ventilation Evaluation in Patients with Software Quantified Intact Target Lobe Fissure – Results from a Retrospective Analysis of the German Lung Emphysema Registry
Saccomanno J, Sgarbossa T, Neumann K, Stanzel F, Andreas S, Eisenmann S, Schmidt B, Gesierich W, Witzenrath M, Hübner RH
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:3939-3950
Published Date: 4 December 2025