Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Endoscopic Lung Volume Reduction with Valves Improves Cardiovascular Adaptability and 6-MWT Performance in Severely Limited COPD Patients
Authors Farber L ![]() , Pappe E, Sgarbossa T, Neumann K
, Pappe E, Sgarbossa T, Neumann K ![]() , Witzenrath M, Hübner RH, Saccomanno J
, Witzenrath M, Hübner RH, Saccomanno J ![]()
Received 14 January 2026
Accepted for publication 7 May 2026
Published 17 June 2026 Volume 2026:21 592263
DOI https://doi.org/10.2147/COPD.S592263
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Lara Farber,1 Eva Pappe,1 Thomas Sgarbossa,1 Konrad Neumann,2 Martin Witzenrath,1,3,4 Ralf-Harto Hübner,1 Jacopo Saccomanno1
1Department of Infectious Diseases, Respiratory Medicine and Critical Care Medicine, Charité – Universitaetsmedizin Berlin, Corporate Member of Freie Universitaet Berlin and Humboldt-Universitaet Zu Berlin, Berlin, Germany; 2Institute of Biometry and Clinical Epidemiology, Charité – Universitaetsmedizin Berlin, Corporate Member of Freie Universitaet Berlin and Humboldt-Universitaet Zu Berlin, Berlin, Germany; 3CAPNETZ Foundation, Hannover, Germany; 4German Center for Lung Research (DZL), Berlin, Germany
Correspondence: Lara Farber, Department of Infectious Diseases, Respiratory Medicine and Critical Care Medicine, Charité – Universitaetsmedizin Berlin, corporate member of Freie Universitaet Berlin and Humboldt-Universitaet zu Berlin, Hindenburgdamm 30, Berlin, 12203, Germany, Email [email protected]
Background: The 6-minute walk test (6-MWT) assesses exercise capacity in patients with chronic obstructive pulmonary disease. A recent study revealed that selected patients with an advanced emphysema and a baseline walking distance of ≤ 140 m in 6-MWT benefit from endoscopic lung volume reduction with valves (ELVR) with a remarkable improvement in walking distance. However, the reasons for these improvements remain unexplained.
Study Design and Methods: We retrospectively analyzed 54 patients with severe emphysema undergoing ELVR at Charité-Universitaetsmedizin Berlin. Patients were stratified into 2 groups by baseline walking distance: those with 6-MWT ≤ 140 m and those with 6-MWT 140– 450 m. Changes in lung function, quality of life, and 6-MWT parameters (peripheral oxygen saturation (SpO2), heart rate (HR), and walking distance) were evaluated using Generalized Estimating Equations (GEE).
Results: While lung function and quality of life improved comparably in both groups, patients with 6-MWT ≤ 140 m showed a significantly greater improvement in walking distance versus the 6-MWT 140– 450 m group (105.6 ± 123.2 m versus 12.1 ± 80.8 m, p=0.027). GEE analysis indicated that this improvement was accompanied by a significantly greater reduction in ΔHR from baseline to follow-up compared to the 6-MWT 140– 450 m group (p=0.023), while changes in SpO2 were similar.
Conclusion: Patients with very limited exercise capacity (≤ 140 m) improved their walking distance disproportionately after ELVR. The concomitant decrease in HR suggests an associated cardiovascular benefit in this subgroup. Therefore, a 6-MWT of ≤ 140 m should not be considered an exclusion criterion for ELVR, as these patients can achieve meaningful clinical improvements.
Keywords: lung emphysema, endoscopic lung volume reduction with valves, 6-minute walk test, COPD
Introduction
Chronic obstructive pulmonary disease (COPD) plays an important role in public health as the fourth leading cause of death worldwide with an increasing prevalence.1 Lung emphysema is a subtype of COPD that is characterized by air trapping and pulmonary hyperinflation impairing breathing mechanics.2 Lung emphysema in advanced stages is characterized by dyspnea, especially on exertion.
Endoscopic lung volume reduction with valves (ELVR) is a minimally invasive treatment aiming to reduce pulmonary hyperinflation. One-way valves inserted into the bronchi of the target lobe allow air to exit from the target lobe while preventing air influx during inspiration, leading to a lung volume reduction of the target lobe or atelectasis.3 The resulting lung volume reduction improves breathing mechanics, particularly by enabling better diaphragm movement. ELVR is the lung volume reduction procedure with the most supporting evidence. Several randomized controlled trials (RCT) have reported improvements in lung function, quality of life, and exercise capacity in carefully selected patients.4–11
The 6-minute walk test (6-MWT) is a simple and reproducible test evaluating all systems involved in physical activity. It is a submaximal exercise test, where patients walk at a self-selected pace without exertion, taking breaks whenever necessary.12 Walking distance serves as a surrogate parameter for cardiovascular fitness and often correlates with overall disease burden. Therefore, it is commonly used to assess changes in exercise capacity following ELVR. Moreover, walking distance in the 6-MWT correlates with forced expiratory volume in one second (FEV1) and overall survival.13,14
The National Emphysema Treatment Trial (NETT) is a landmark study as the first large RCT of surgical lung volume reduction. It demonstrated a survival benefit in selected patients and identified high-risk groups.15 As a result, NETT significantly influenced treatment guidelines and defined new inclusion criteria for the subsequent studies. According to NETT protocol, patients with a very low walking distance (6-MWT ≤140 m) were excluded from the study due to estimated surgical risks.15 Consequently, this patient cohort was often excluded or underrepresented in later RCTs on ELVR, as their risk of complications—such as pneumothorax—was considered too high, and the potential treatment benefit was deemed limited.9–11,15,16
Own recent work showed in a cohort of 54 patients with a baseline 6-MWT ≤140 m comparable treatment results regarding lung function and quality of life compared to patients with 6-MWT 140–450 m, with a remarkable improvement in walking distance after ELVR, but without an increased risk of complications.17 Data for this analysis were derived from the German Lung Emphysema Registry and did not contain 6-MWT parameters such as peripheral oxygen saturation (SpO2), walking distance, and heart rate (HR) per minute. Therefore, the aim of the present study was to perform an in-depth evaluation of 6-MWT components not captured in the registry data to identify a potential underlying explanation.
Materials and Methods
Patient Population
The analyzed data were derived from patients with advanced lung emphysema who underwent ELVR in accordance with the standards of the German Lung Emphysema Registry (https://www.lungenemphysemregister.de) at Charité – Universitaetsmedizin Berlin. All patients provided written informed consent and were enrolled in an open-label clinical trial approved by the local ethics committee (A2/149/17 and EA1/136/13).
Inclusion and Exclusion Criteria
Eligible patients had to present with advanced lung emphysema, defined by a FEV1 <45% predicted and a residual volume (RV) >180% predicted.18 There were no restrictions regarding the diffusing capacity of the lungs for carbon monoxide (DLCO). Partial pressure of carbon dioxide (pCO2) had to be <55 mmHg; otherwise, patients were first evaluated for non-invasive ventilation.18 Additionally, patients required a baseline walking distance of <450 m in the 6-MWT and be on optimal medical therapy for COPD. Dyspnea and reduced physical activity had to be primarily attributed to severe COPD. All patients were required to be non-smokers for at least three months prior to intervention, confirmed by a carboxyhemoglobin (COHb) level <2%.
Evaluation Procedure
Patients underwent a structured evaluation process including body plethysmography, 6-MWT, diffusion capacity test, arterial or capillary blood gas analysis, echocardiography, and ventilation/perfusion lung scan. Additionally, all patients received a non-contrast computed tomography (CT) of the lungs, and a software-based evaluation of fissure integrity and emphysema destruction for each lobe was used to define a potential target lobe for ELVR. Patients completed the COPD Assessment Test (CAT), the Modified Medical Research Council (mMRC), and the St. George`s Respiratory Questionnaire (SGRQ) to assess symptoms, dyspnea, and quality of life. Collateral ventilation of the target lobe was excluded according to current standards by fissure integrity analysis based on computed tomography of the lung. Additionally, bronchoscopic in-vivo measurement of collateral ventilation with the Chartis® assessment system (PulmonX Inc., Redwood City, CA, USA) was performed if fissure integrity showed an intermediate fissure completeness score of 85–95%. Chartis® assessment was part of the baseline evaluation before the emphysema board and was performed under conscious sedation in spontaneous breathing or under high-frequency jet ventilation.19 Chartis® measurements were categorized into conclusive CV-negative or CV-positive phenotypes, or inconclusive phenotypes such as low flow/collapse or low plateau.20 At our center, all patients underwent a ventilation/perfusion lung scan. Since it is not required as a standard work-up at the lung emphysema registry, the results were not available in the RedCap database and are not reported in this study.
Lung Volume Reduction Therapy
Every case was reviewed by the multidisciplinary emphysema board, consisting of at least one thoracic surgeon, one interventional pneumologist, and a radiologist. The target area and type of endoscopic intervention were determined by the board. ELVR was performed in a bronchoscopy session with the Zephyr® valve system (Pulmonx, Redwood City, CA, USA) or Spiration Valve System (Olympus, Center Valley, PA, USA) according to local endobronchial anatomy.
Study Design
This study retrospectively analyzed data available from the RedCAP electronic database and patient files.21 The 6-MWT was conducted according to the American Thoracic Society guidelines, assessing SpO2, HR, walking distance, dyspnea, and muscular fatigue – both evaluated using the Borg scale.12 We considered parameters both at baseline and follow-up data to evaluate treatment response. Follow-up assessments were conducted at 3- and 6-months post-intervention, including lung function tests, 6-MWT, and quality of life measurements. If patients attended only one follow-up appointment (either 3- or 6-months after the intervention), the available data point was used for the follow-up analysis. For patients with a follow-up assessment from both time points, the visit with the highest walking distance was selected for analysis.
Statistical Analysis
Nominal values are presented as counts and percentages, while ordinal and continuous variables are presented as means with standard deviations or standard errors. The mMRC score was analyzed as a categorical variable. Baseline dyspnea was compared between groups using the frequency of patients with a score of ≥3 points. Treatment response was defined as a reduction of ≥1 point in the mMRC scale. Statistical analyses were conducted with SPSS (version 29.0.0.0). We applied paired and unpaired t-tests, the Wilcoxon test, Mann–Whitney U-test, Chi-square test, and McNemar test, as appropriate. Generalized Estimating Equations (GEE) were used to analyze repeated measurements from the same patients during the 6-MWT. This method accounts for the potential correlation among repeated observations and estimates group-level trends over time. We applied GEE to assess HR, SpO2, and walking distance, as well as their changes (ΔHR, ΔSpO2, and Δ walking distance), calculated as the difference between values before and after ELVR. The aim was to determine whether these parameters changed significantly over time and whether the changes differed between groups. P-values ≤ 0.05 were considered statistically significant.
Results
Study Population
A total of 87 patients were treated with ELVR between August 2017 and January 2024 at our center. We excluded 33 patients due to missing 6-MWT assessments: 11 were missing baseline measurements, 12 were missing follow-up measurements, and 10 lacked data at both time points due to either non-participation or unavailable documentation. This resulted in a final cohort of 54 patients included in the analysis. The patients were categorized into two groups based on their walking distance in 6-MWT at baseline: the 6-MWT ≤140 m group (n = 12) and the 6-MWT 140–450 m group (n = 42). Table 1 demonstrates the baseline characteristics. Both groups presented comparable distributions in sex, age, and body mass index (BMI). There were no significant differences in emphysema score, heterogeneity index, or fissure completeness score. Lung function was generally similar, except for a significantly higher vital capacity (VC) in the 6-MWT 140–450 m group. Patients with a 6-MWT ≤140 m had higher levels of dyspnea, with 92% having a mMRC score of ≥3 points compared to 71% in the 6-MWT 140–450 m group. However, this difference did not reach a statistical significance (p=0.148). Patients with a 6-MWT ≤140 m reported a significantly worse quality of life based on the SGRQ score. Since the groups were stratified by their walking distance in 6-MWT at baseline, a statistical comparison of these values was considered non-applicable as this difference was expected by study design.
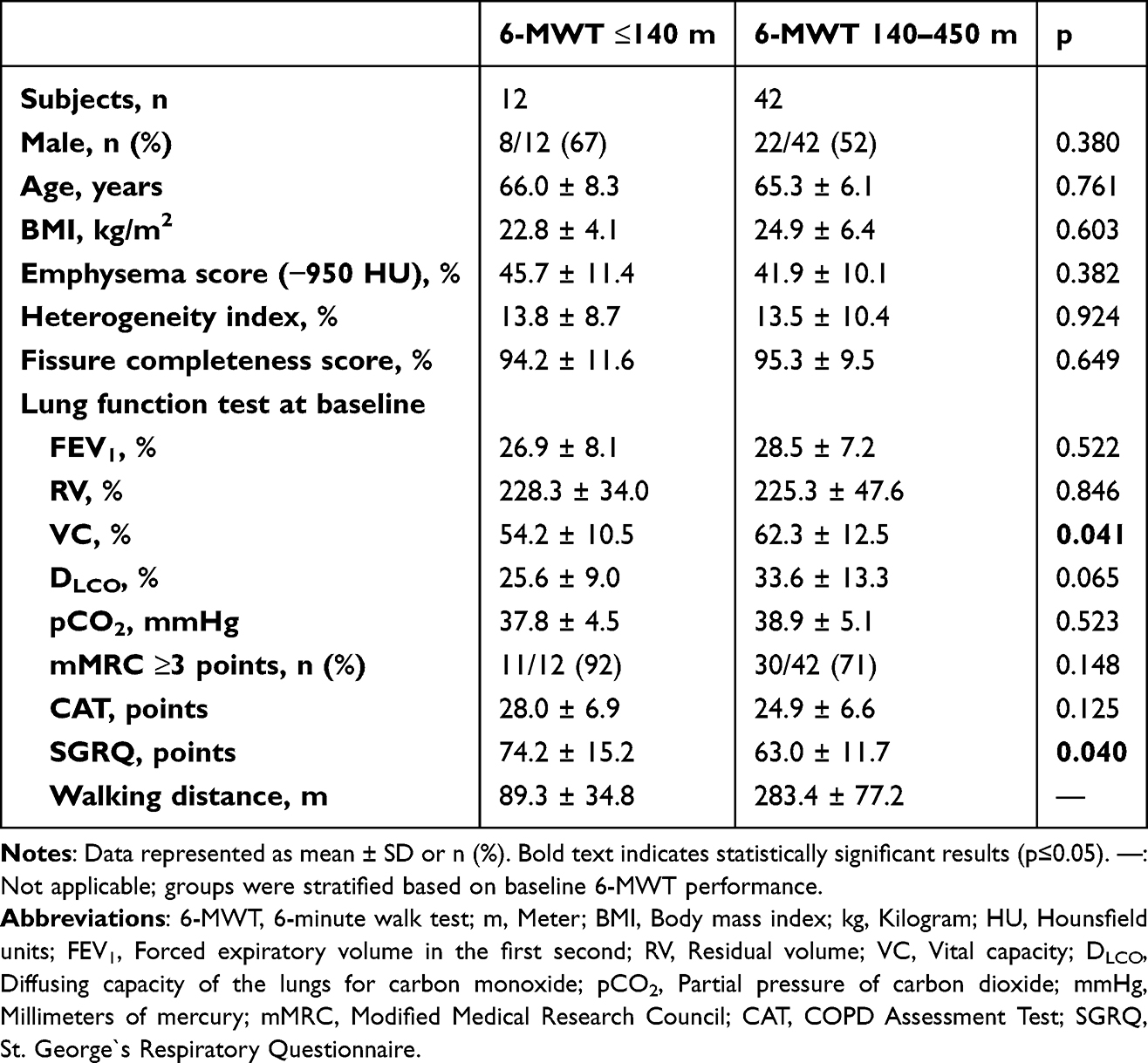 |
Table 1 Baseline Parameters of Study Population |
Comparison of Treatment Outcome After ELVR Between Both Groups
Table 2 summarizes treatment outcomes between baseline and follow-up. Both groups showed comparable improvements in lung function and quality of life after ELVR. However, patients with 6-MWT ≤140 m experienced a significantly greater increase in walking distance, with an average improvement of 105.6 ± 123.2 m compared to 12.1 ± 80.8 m in the 6-MWT 140–450 m group (p=0.027).
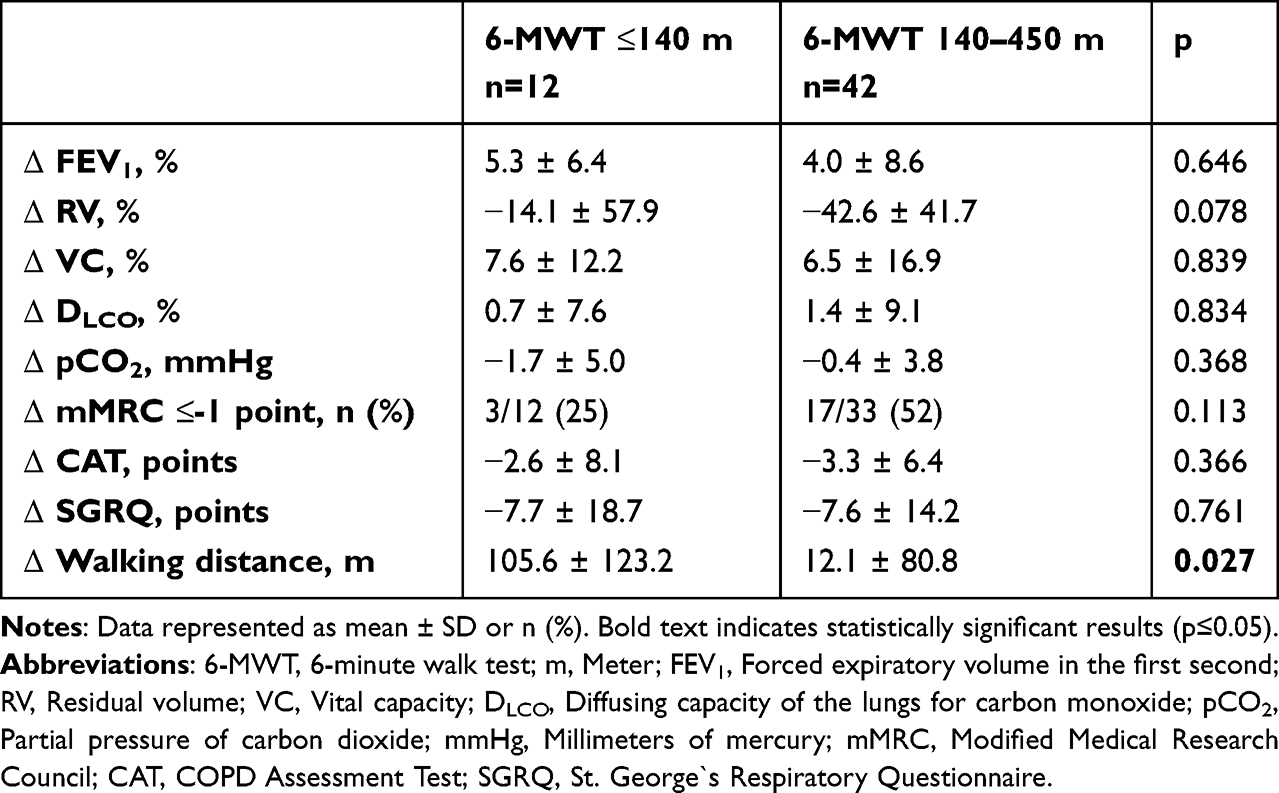 |
Table 2 Comparison of Outcome Between Both Groups |
Trajectories of 6-MWT Parameters (Walking Distance, SpO2 and HR)
Figure 1 illustrates trajectories of walking distance at baseline (Figure 1a), follow-up (Figure 1b) and changes after ELVR (Figure 1c) for both groups. GEE analysis was used to detect parameter differences between groups and to assess parameter changes over time. At both time points, walking distance per minute declined progressively over the course of the 6-MWT in each group (both p<0.001). This decrease was more pronounced in patients with 6-MWT ≤140 m, particularly at baseline. Patients with a 6-MWT 140–450 m walked statistically farther per minute at baseline and follow-up (p<0.001). However, the improvement in walking distance after ELVR was significantly higher for patients with a 6-MWT ≤140 m (p=0.038).
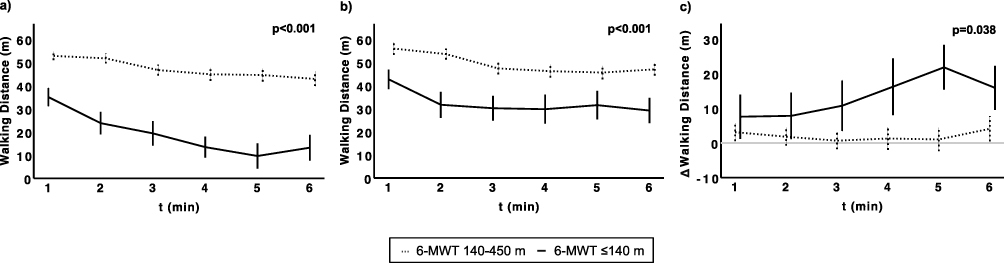 |
Figure 1 Trajectories of walking distance per minute after endoscopic lung volume reduction with valves (ELVR) in patients with 6-MWT ≤140 m (solid line) and patients with 6-MWT 140–450 m (dotted line). (a) Baseline: Patients with 6-MWT ≤140 m had statistically lower walking distance. (b) Follow-up: Patients with 6-MWT ≤140 m had statistically lower walking distance. (c) Changes between Baseline and Follow-up: Patients with 6-MWT ≤140 m had a higher increase in Δ walking distance than patients with 6-MWT 140–450 m. The grey horizontal line at y=0 in panel indicates the reference line. P-values from the Generalized Estimating Analysis (GEE) assessing differences between the groups are shown within panels. Bolded p-values indicate statistically significant results (p≤0.05). Data are presented as mean values with error bars representing standard error. Abbreviations: t, Time; min, Minute; ELVR, Endoscopic lung volume reduction with valves; 6-MWT, 6-minute walk test. m: Meter. |
Figure 2 presents trajectories of SpO2 at baseline (Figure 2a), follow-up (Figure 2b) and changes after ELVR (Figure 2c). In both groups, SpO2 declined significantly over the course of the 6-MWT at baseline and follow-up (both p<0.001). No difference between the groups was observed in the magnitude of SpO2 at either time point, and ΔSpO2 did not differ significantly between the groups.
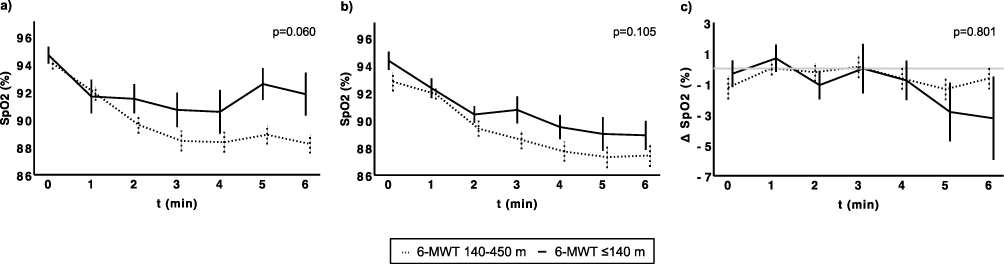 |
Figure 2 Trajectories of peripheral oxygen saturation (SpO2) per minute after endoscopic lung volume reduction with valves (ELVR) in patients with 6-MWT ≤140 m (solid line) and patients with 6-MWT 140–450 m (dotted line). (a) Baseline: There was no significant difference in SpO2 between the two groups. (b) Follow-up: There was no significant difference in SpO2 between the two groups. (c) Changes between Baseline and Follow-up: There was no significant difference in ΔSpO2 between the two groups. The grey horizontal line at y=0 in panel indicates the reference line. P-values from the Generalized Estimating Analysis (GEE) assessing differences between the groups are shown within panels. Data are presented as mean values with error bars representing standard error. Abbreviations: t, Time; min, Minute; ELVR, Endoscopic lung volume reduction with valves; 6-MWT, 6-minute walk test; m, Meter; SpO2, Peripheral oxygen saturation. |
Figure 3 illustrates trajectories of HR at baseline (Figure 3a), follow-up (Figure 3b) and the changes after ELVR (Figure 3c). In both groups, HR increased significantly over the course of the 6-MWT at baseline and follow-up (p<0.001 for both). No between-group differences in HR were observed at baseline or follow-up. However, patients with a 6-MWT ≤140 m showed a significantly higher reduction in ΔHR after ELVR compared with the 6-MWT 140–450 m group (p=0.023). Using McNemar test, the change in the use of heart rate lowering medications between baseline and follow-up was assessed for each group separately. The change was not significant in the group with 6-MWT ≤140 m (p=1.000) or the group with 6-MWT 140–450 m (p=0.063).
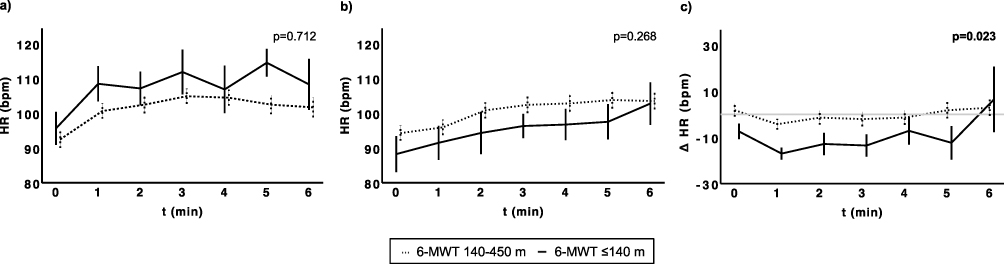 |
Figure 3 Trajectories of heart rate (HR) per minute after endoscopic lung volume reduction with valves (ELVR) in patients with 6-MWT ≤140 m (solid line) and patients with 6-MWT 140–450 m (dotted line). (a) Baseline: There was no significant difference in HR between the two groups. (b) Follow-up: There was no significant difference in HR between the two groups. (c) Changes between Baseline and Follow-up: Patients with 6-MWT ≤140 m had a higher decrease in ΔHR than patients with 6-MWT 140–450 m. The grey horizontal line at y=0 in panel indicates the reference line. P-values from the Generalized Estimating Analysis (GEE) assessing differences between the groups are shown within panels. The bolded p-value indicates a statistically significant result (p≤0.05). Data are presented as mean values with error bars representing standard error. Abbreviations: t, Time; min, Minute; ELVR, Endoscopic lung volume reduction with valves; 6-MWT, 6-minute walk test; HR, Heart rate; m, Meter; bpm, Beats per minute. |
Discussion
This is the first study evaluating cardiovascular response, assessed by HR, during the 6-MWT in lung emphysema patients treated with ELVR. Severe emphysema patients benefitted from ELVR with comparable improvements in lung function and quality of life, regardless of their baseline 6-MWT. While the improvements in lung function were statistically similar across both groups, a notable discrepancy was observed regarding the reduction in RV. Table 2 highlights a three-fold greater reduction in RV in the 6-MWT 140–450 m group compared to the 6-MWT ≤140 m group (−42.6 ± 41.7% vs −14.1 ± 57.9%, p=0.078). Although this difference in  RV between the groups was not statistically significant, likely due to the small sample size, the magnitude of this change is substantial. Despite this more pronounced RV reduction in the 6-MWT 140–450 m group, the improvement in VC remained nearly the same between the two groups (6.5 ± 16.9% vs 7.6 ± 12.2%, p=0.839). This suggests that in patients with 6-MWT ≤140m, even a modest reduction in RV can result in a comparable improvement in VC. This may be explained by the profound hyperinflation of these patients, where even a low reduction in RV may enhance the mechanical efficiency of the respiratory system.
RV between the groups was not statistically significant, likely due to the small sample size, the magnitude of this change is substantial. Despite this more pronounced RV reduction in the 6-MWT 140–450 m group, the improvement in VC remained nearly the same between the two groups (6.5 ± 16.9% vs 7.6 ± 12.2%, p=0.839). This suggests that in patients with 6-MWT ≤140m, even a modest reduction in RV can result in a comparable improvement in VC. This may be explained by the profound hyperinflation of these patients, where even a low reduction in RV may enhance the mechanical efficiency of the respiratory system.
However, GEE analysis revealed a different effect on exercise capacity after ELVR between the groups. Patients with a baseline 6-MWT ≤140 m exhibited a significantly greater reduction in HR at follow-up and showed a disproportionately larger improvement in walking distance compared with those walking 140–450 m at baseline. This reduction in HR suggests that ELVR not only enhances respiratory mechanics in the most severely limited patients but may also modify their cardiovascular response to physical exertion.
6-MWT is an important clinical tool for assessing exercise capacity in COPD patients. Although clinical trials for ELVR show consistent improvements in lung function parameters, the response in 6-MWT was found to be more heterogeneous. STELVIO and TRANSFORM trials demonstrated a significant mean increase in walking distance from baseline of 60 m and 36 m, respectively, which were both above the minimal clinically important difference of 25 m.6,16,22 In contrast, the BeLieVeR-HIFi trial observed a statistically significant but more modest improvement in walking distance of ELVR groups (median 25 m) compared to the control group, whereas the EMPROVE trial found no significant differences between the groups.5,11 This variability suggests that not all patients improve their physical capacity to the same extent after ELVR, but the reasons for that are still unknown. The present study offers an explanation for this heterogeneity by demonstrating that a very low baseline walking distance may serve as a predictor of gains in exercise capacity after ELVR.
Physiologically, increases in physical activity, reflected by longer walking distance during the 6-MWT, are achieved by a rise in cardiac output and HR. However, this response also depends on adequate breathing mechanics and physical fitness. In this study, patients with 6-MWT ≤140 m walked significantly farther after ELVR, while exhibiting -or possibly because of- a lower HR at follow-up compared with baseline. This pattern suggests a regained HR reserve, indicating that patients recovered the ability to increase their HR as a response to physical activity. GEE analysis confirmed that HR rose significantly over time during the 6-MWT. Thus, it is tempting to speculate that the lower starting HR allowed more efficient use of the restored reserve to support higher levels of physical activity. However, functional analyses are warranted to provide evidence for this concept. Although these are the first data describing cardiovascular changes in an ELVR cohort, analogous findings have been documented after lung volume reduction surgery (LVRS). For instance, Armstrong et al reported a significant decrease in resting HR (89 ± 12 bpm vs 85 ± 12 bpm) as well as decreasing HR at exercise (118 ± 15 bpm vs 114 ± 18 bpm).23 Similarly, a study by Benditt et al found a significant decrease in HR during exercise (from 115 bpm to 111 bpm) and observed a significant increase in oxygen pulse at maximal exercise, suggesting an improvement in stroke volume.24
Both groups in the present study showed a comparable decline in SpO2 during the 6-MWT after ELVR as compared to baseline, indicating that all patients performed the test at the required submaximal intensity and were respiratorily exhausted during the procedure. This suggests that the substantial improvement in walking distance observed in the 6-MWT ≤140 m group is not primarily attributable to enhanced oxygenation or lung function but rather to improved exercise capacity linked to changes in HR.
The improvement in HR regulation may reflect a rebalancing of the autonomic nervous system function.23 Patients with severe lung emphysema commonly develop sympathetic nervous system abnormalities due to impaired breathing mechanics, driven by increased intrathoracic pressure, hypoxemia, hypercapnia, inflammation, and increased respiratory effort.25,26 These pathological processes elevate pulmonary vascular resistance and pulmonary artery pressure, ultimately reducing right ventricular function.27–29 This results in an imbalance of the autonomic nervous system with an increase in sympathetic nerve activity with a higher resting HR to maintain cardiac output against the high resistance.25,30 ELVR appears to disrupt this vicious cycle. By reducing lobar volume and hyperinflation, lung volume reduction lowers intrathoracic pressure, improves right ventricular preload and afterload, and increases stroke volume.24,31 Consequently, the sympathetic tone required for cardiac function is reduced, which leads to a recovery of the autonomic nervous system, contributing to the observed HR reduction.
Lung function parameters at baseline and their improvement after ELVR were comparable in both groups and therefore do not explain the observed differences in HR and walking distance. Other factors not assessed in this study, such as emphysema heterogeneity and pulmonary perfusion distribution, may also play a role. Previous research highlights the importance of disease pattern for ELVR outcome. Roodenburg et al found that patients with heterogeneous emphysema have greater improvements in walking distance compared to patients with homogeneous emphysema.32 Thomsen et al demonstrated that preserved perfusion in the ipsilateral non-target lobe is associated with superior gains in exercise capacity.33
Following the NETT trial, patients with a very low walking distance were frequently excluded from volume reduction trials because of an assumed higher risk for complications and limited therapy benefit.15 Of note, the findings of this study suggest a reversible physiological mechanism in this subgroup. The data indicate that this severe limitation in exercise capacity may be due to a cardiovascular strain, which is reduced by ELVR. For this reason, 6-MWT ≤140 m should not be viewed as an absolute exclusion criterion. As shown here and in prior work from this study group, these patients benefit substantially from ELVR without an increased risk of complications.17 Instead, a reduced walking distance combined with elevated HR may help identifying patients with the greatest need for intervention.
The clinical significance of these findings extends beyond symptom improvement. Physical activity and exercise capacity are strong predictors of mortality in COPD.34 A meta-analysis by Fermont et al demonstrated that both shorter walking distance and elevated resting HR are associated with a higher risk of early mortality.35 In this study, ELVR favorably influenced both factors in the 6-MWT ≤140 m group, increasing walking distance by more than 100 m and significantly reducing HR. Thus, ELVR may offer a survival benefit in this particularly vulnerable population.
Strengths of this study include the detailed minute-by-minute analysis of HR and SpO2 throughout the 6-MWT and the use of GEE to effectively compare repeated measurements. Nevertheless, several limitations should be acknowledged. First, the study is retrospective with a small sample size of patients, especially in the subgroup of patients with 6-MWT ≤140 m, limiting generalizability. Second, the study did not include direct measurements of cardiac output, such as right heart catheterization, or direct assessments of the autonomic nerve system, such as heart rate variability analysis. Third, patients were recruited from a single center, and the follow-up period was relatively short, precluding assessment of long-term outcomes.
Conclusion
In conclusion, this study defines a subgroup of highly symptomatic patients with advanced emphysema and severely impaired exercise capacity (6-MWT of ≤140 m) who improve their walking distance disproportionately well after ELVR. The concomitant significant reduction in HR from baseline to follow-up suggests an associated cardiovascular benefit and recovery in this subgroup. Therefore, a baseline walking distance of ≤140 m should not be considered an exclusion criterion for ELVR, as these highly symptomatic patients can derive substantial clinical benefit.
Data Sharing Statement
Data can be made available on request to the corresponding author.
Ethics Approval and Informed Consent
The presented study was conducted according to the standards of the World Medical Association Declaration of Helsinki and the appropriate guidelines for human studies. Ethical approval was obtained from the Ethics Committee of the Charité Universitaetsmedizin Berlin, Germany (approval number EA2/149/17 and EA1/136/13). Each patient consented to participate in the study. Inability to sign the consent form was an exclusion criterion.
Acknowledgments
The authors sincerely thank Antje Geldmeyer for her excellent support in collecting the data and patient coordination. We also express our gratitude to the patients who consented to participate and provided their data for inclusion in the registry. Gemini 3 (Google) was used to assist with language refinement and grammar to improve the readability of the manuscript. AI was not used to generate content. The authors reviewed and approved all AI-assisted content.
Funding
No funding was received for this study.
Disclosure
L. Farber, E. Pappe, T. Sgarbossa, K. Neumann, R. H. Hübner, J. Saccomanno have nothing to disclose. M. Witzenrath received funding for research from Deutsche Forschungsgemeinschaft (DFG; German Research Foundation), Bundesministerium für Forschung, Technologie und Raumfahrt (BMFTR; Federal Ministry of Research, Technology and Space), Gemeinsamer Bundesausschuss (G-BA; The Federal Joint Committee), Bundesministerium für Gesundheit (BMG; Federal Ministry of Health), Deutsches Zentrum für Lungenforschung (DZL; German Center for Lung Research), Biotest, Pantherna, Aptarion, and for lectures and advisory from Astra Zeneca, Chiesi, Insmed, Gilead, Pfizer, Boehringer, Biotest, Pantherna and Aptarion. The authors report no other conflicts of interest int his work.
References
1. GBD 2021 Causes of Death Collaborators. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2100–10. doi:10.1016/S0140-6736(24)00367-2
2. Kemp SV, Polkey MI, Shah PL. The epidemiology, etiology, clinical features, and natural history of emphysema. Thorac Surg Clin. 2009;19(2):149–158. doi:10.1016/j.thorsurg.2009.03.003
3. Shah PL, Herth FJ, van Geffen WH, Deslee G, Slebos DJ. Lung volume reduction for emphysema. Lancet Respir Med. 2017;5(2):147–156. doi:10.1016/S2213-2600(16)30221-1
4. Patel M, Chowdhury J, Zhao H, et al. Meta-analysis and systematic review of bronchoscopic lung volume reduction through endobronchial valves in severe emphysema. J Bronchology Interv Pulmonol. 2022;29(3):224–237. doi:10.1097/LBR.0000000000000872
5. Davey C, Zoumot Z, Jordan S, et al. Bronchoscopic lung volume reduction with endobronchial valves for patients with heterogeneous emphysema and intact interlobar fissures (the BeLieVeR-HIFi study): a randomised controlled trial. Lancet. 2015;386(9998):1066–1073. doi:10.1016/S0140-6736(15)60001-0
6. Klooster K, ten Hacken NHT, Hartman JE, Kerstjens HAM, van Rikxoort EM, Slebos DJ. Endobronchial valves for emphysema without interlobar collateral ventilation. N Engl J Med. 2015;373(24):2325–2335. doi:10.1056/NEJMoa1507807
7. Hopkinson NS, Toma TP, Hansell DM, et al. Effect of bronchoscopic lung volume reduction on dynamic hyperinflation and exercise in emphysema. Am J Respir Crit Care Med. 2005;171(5):453–460. doi:10.1164/rccm.200407-961OC
8. Toma TP, Hopkinson NS, Hillier J, et al. Bronchoscopic volume reduction with valve implants in patients with severe emphysema. Lancet. 2003;361(9361):931–933. doi:10.1016/S0140-6736(03)12762-6
9. Sciurba FC, Ernst A, Herth FJF, et al. A randomized study of endobronchial valves for advanced emphysema. N Engl J Med. 2010;363(13):1233–1244. doi:10.1056/NEJMoa0900928
10. Valipour A, Slebos DJ, Herth F, et al. Endobronchial valve therapy in patients with homogeneous emphysema. Results from the IMPACT study. Am J Respir Crit Care Med. 2016;194(9):1073–1082. doi:10.1164/rccm.201607-1383OC
11. Criner GJ, Delage A, Voelker K, et al. Improving lung function in severe heterogenous emphysema with the spiration valve system (EMPROVE). A multicenter, open-label randomized controlled clinical trial. Am J Respir Crit Care Med. 2019;200(11):1354–1362. doi:10.1164/rccm.201902-0383OC
12. ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111–117. doi:10.1164/ajrccm.166.1.at1102
13. Celli B, Tetzlaff K, Criner G, et al. The 6-minute-walk distance test as a chronic obstructive pulmonary disease stratification tool. Insights from the COPD biomarker qualification consortium. Am J Respir Crit Care Med. 2016;194(12):1483–1493. doi:10.1164/rccm.201508-1653OC
14. Butland RJ, Pang J, Gross ER, Woodcock AA, Geddes DM. Two-, six-, and 12-minute walking tests in respiratory disease. Br Med J Clin Res Ed. 1982;284(6329):1607–1608. doi:10.1136/bmj.284.6329.1607
15. Fishman A, Martinez F, Naunheim K, et al. A randomized trial comparing lung-volume-reduction surgery with medical therapy for severe emphysema. N Engl J Med. 2003;348(21):2059–2073. doi:10.1056/NEJMoa030287
16. Kemp SV, Slebos DJ, Kirk A, et al. A multicenter randomized controlled trial of zephyr endobronchial valve treatment in heterogeneous emphysema (TRANSFORM). Am J Respir Crit Care Med. 2017;196(12):1535–1543. doi:10.1164/rccm.201707-1327OC
17. Saccomanno J, Kilic L, Sgarbossa T, et al. Clinical improvements after endoscopic lung volume reduction with valves in patients with advanced emphysema and a 6-min walk test ≤140 m at baseline. ERJ Open Res. 2025;11(1):00410–02024. doi:10.1183/23120541.00410-2024
18. Sgarbossa T, Lenga P, Stanzel F, et al. Assessment of efficacy and safety of endoscopic lung volume reduction with one-way valves in patients with a very low FEV1. ERJ Open Res. 2023;9(4):00190–02023. doi:10.1183/23120541.00190-2023
19. Saccomanno J, Sgarbossa T, Pappe E, et al. VT20 method for Chartis assessment of collateral ventilation with flexible bronchoscopy under procedural sedation. ERJ Open Res. 2024;10(4):00945–02023. doi:10.1183/23120541.00945-2023
20. Herzog D, Thomsen C, Poellinger A, et al. Outcomes of endobronchial valve treatment based on the precise criteria of an endobronchial catheter for detection of collateral ventilation under spontaneous breathing. Respiration. 2016;91(1):69–78. doi:10.1159/000442886
21. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
22. Holland AE, Hill CJ, Rasekaba T, Lee A, Naughton MT, McDonald CF. Updating the minimal important difference for six-minute walk distance in patients with chronic obstructive pulmonary disease. Arch Phys Med Rehabil. 2010;91(2):221–225. doi:10.1016/j.apmr.2009.10.017
23. Armstrong HF, Gonzalez-Costello J, Jorde UP, et al. The effect of lung volume reduction surgery on chronotropic incompetence. Respir Med. 2012;106(10):1389–1395. doi:10.1016/j.rmed.2012.06.011
24. Benditt JO, Lewis S, Wood DE, Klima L, Albert RK. Lung volume reduction surgery improves maximal O2 consumption, maximal minute ventilation, O2 pulse, and dead space-to-tidal volume ratio during leg cycle ergometry. Am J Respir Crit Care Med. 1997;156(2 Pt 1):561–566. doi:10.1164/ajrccm.156.2.9611032
25. Alqahtani JS, Aldhahir AM, Alghamdi SM, et al. A systematic review and meta-analysis of heart rate variability in COPD. Front Cardiovasc Med. 2023;10:1070327. doi:10.3389/fcvm.2023.1070327
26. Van Gestel AJR, Kohler M, Steier J, Teschler S, Russi EW, Teschler H. Cardiac autonomic dysfunction and health-related quality of life in patients with chronic obstructive pulmonary disease. Respirology. 2011;16(6):939–946. doi:10.1111/j.1440-1843.2011.01992.x
27. Mahler DA, Brent BN, Loke J, Zaret BL, Matthay RA. Right ventricular performance and central circulatory hemodynamics during upright exercise in patients with chronic obstructive pulmonary disease. Am Rev Respir Dis. 1984;130(5):722–729. doi:10.1164/arrd.1984.130.5.722
28. Light RW, Mintz HM, Linden GS, Brown SE. Hemodynamics of patients with severe chronic obstructive pulmonary disease during progressive upright exercise. Am Rev Respir Dis. 1984;130(3):391–395. doi:10.1164/arrd.1984.130.3.391
29. Matthay RA, Berger HJ, Davies RA, et al. Right and left ventricular exercise performance in chronic obstructive pulmonary disease: radionuclide assessment. Ann Intern Med. 1980;93(2):234–239. doi:10.7326/0003-4819-93-2-234
30. Spiesshoefer J, Regmi B, Ottaviani MM, et al. Sympathetic and vagal nerve activity in COPD: pathophysiology, presumed determinants and underappreciated therapeutic potential. Front Physiol. 2022;13:919422. doi:10.3389/fphys.2022.919422
31. Mineo TC, Pompeo E, Rogliani P, et al. Effect of lung volume reduction surgery for severe emphysema on right ventricular function. Am J Respir Crit Care Med. 2002;165(4):489–494. doi:10.1164/ajrccm.165.4.2108129
32. Roodenburg SA, Klooster K, Slebos DJ, Hartman JE. The impact of emphysema heterogeneity on treatment response after endobronchial valve treatment. ERJ Open Res. 2023;9(4):00279–02023. doi:10.1183/23120541.00279-2023
33. Thomsen C, Theilig D, Herzog D, et al. Lung perfusion and emphysema distribution affect the outcome of endobronchial valve therapy. Int J Chron Obstruct Pulmon Dis. 2016;11:1245–1259. doi:10.2147/COPD.S101003
34. Waschki B, Kirsten A, Holz O, et al. Physical activity is the strongest predictor of all-cause mortality in patients with COPD: a prospective cohort study. Chest. 2011;140(2):331–342. doi:10.1378/chest.10-2521
35. Fermont JM, Masconi KL, Jensen MT, et al. Biomarkers and clinical outcomes in COPD: a systematic review and meta-analysis. Thorax. 2019;74(5):439–446. doi:10.1136/thoraxjnl-2018-211855
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Limited Benefit of Additional Chartis® Assessments for Collateral Ventilation Evaluation in Patients with Software Quantified Intact Target Lobe Fissure – Results from a Retrospective Analysis of the German Lung Emphysema Registry
Saccomanno J, Sgarbossa T, Neumann K, Stanzel F, Andreas S, Eisenmann S, Schmidt B, Gesierich W, Witzenrath M, Hübner RH
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:3939-3950
Published Date: 4 December 2025