Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Leisure Activity Interventions on Cognition in Mild Cognitive Impairment Patients: A Meta-Analysis
Authors He X, Liu C, Li Z, Cai X ![]()
Received 1 May 2025
Accepted for publication 22 July 2025
Published 13 August 2025 Volume 2025:21 Pages 1671—1687
DOI https://doi.org/10.2147/NDT.S536627
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Xueming He,1 Chuming Liu,2 Zhaoyang Li,2 Xiaojun Cai1
1Heilongjiang Academy of Chinese Medicine, Harbin, Heilongjiang, 150036, People’s Republic of China; 2Heilongjiang University of Chinese Medicine, Harbin, Hei longjiang, 150040, People’s Republic of China
Correspondence: Xiaojun Cai, Department of Endocrinology, Heilongjiang Academy of Chinese Medicine, Harbin, Heilongjiang, 150036, People’s Republic of China, Email [email protected]
Abstract: Cognitive impairment has gradually become a serious social problem that endangers the normal life of elderly individuals. Traditional cognitive rehabilitation training (TCRT) is limited by family economic and medical insurance policies, making it difficult to sustain long-term rehabilitation training for patients with cognitive impairments. Leisure activities, as simple, efficient, and convenient intervention therapies, have been used for the rehabilitation of patients with cognitive impairment, but specific effects have not been reported. This meta-analysis of randomized controlled trials evaluated the efficacy of leisure activity intervention versus TCRT control on cognitive function in patients with varying degrees of cognitive impairment. As of December 10, 2024, literature searches were conducted on PubMed, Embase, the Cochrane Controlled Trials Registry, and related databases. The PEDro scale was used to assess the risk of bias. A total of 20 randomized controlled trials (n = 1126) used mahjong, poker, VR, or other games. The results revealed that leisure activity intervention improved overall cognitive function (MOCA, P = 0.012; MMSE, P = 0.013), memory function (DSB, P < 0.0001; DSF, P = 0.015), and quality of life (ADL, P < 0001). In summary, leisure activities can serve as a complementary and alternative therapy to traditional cognitive rehabilitation training to improve some cognitive domains of patients with cognitive impairments (PROSPERO registration: CRD42025639157).
Keywords: leisure activities, mild cognitive impairment, alzheimer’s disease, complementary therapy, cognitive dysfunction, neuropsychological tests
A Letter to the Editor has been published for this article.
Introduction
In recent years, the proportion of people aged 60 years and above has been increasing.1 In 2019, there were 1 billion people aged 60 years or older. By 2030, this number is expected to reach 1.4 billion, and by 2050, it is expected to reach 2.1 billion.2 Cognitive impairment is a stage between normal aging and Alzheimer’s disease. It is a primary symptom of age-related diseases such as Alzheimer’s disease.3–5 Researchers have reported that the overall prevalence of mild cognitive impairment (MCI) is 20.8%, indicating that approximately 23.86 million people aged 65 years or older in China suffer from MCI.6 Without early, active, and effective interventions, MCI can easily progress to dementia. Additionally, cognitive impairment burdens patients, reducing their ability to live independently, increasing hospitalization risk, and increasing medical costs.7
The pathogenesis of MCI has not been fully elucidated, and it may be related to multiple factors, all of which ultimately lead to cognitive impairment.8 Genetic mutations can cause abnormal protein aggregation. Mutations in genes such as amyloid beta precursor protein, presenilin-1, and presenilin-2 promote the increased production, aggregation, and deposition of Aβ amyloid peptides.9 Abnormalities in genes such as ApolipoproteinE affect their metabolic clearance, thereby leading to neuronal death and learning and memory impairments.10 Tau gene mutations cause abnormal phosphorylation of tau protein, loss of normal activity, and neuronal damage, resulting in cognitive impairment.11 The reduction or degeneration of cholinergic neurons in the basal forebrain reduces the content of acetylcholine, affects signal transmission, accelerates Aβ and tau pathology, and exacerbates cognitive deterioration.12 In neuroinflammation, the initial activation of microglia is beneficial, but chronic activation promotes the pathological process.13 Oxidative stress and mitochondrial dysfunction interact with each other, exacerbating Aβ toxicity and apoptosis, and thus participating in the pathogenesis.14
Traditional cognitive rehabilitation training (TCRT) is commonly used to treat elderly patients with cognitive impairments. TCRT positively boosts cognitive and memory functions.15 However, TCRT usually requires professional guidance in medical settings. Patient participation is restricted by factors such as socioeconomic status and health insurance, resulting in a small number of participants.16 Research also demonstrates that while some patients experience short-term improvements after training, these effects often fade over time, and this decline is not solely due to disease progression.17,18 Consequently, there is an urgent demand for a convenient and inexpensive alternative to enhance the cognition and memory of cognitively impaired patients.
Because maintaining the sustainability of brain activity is crucial for the recovery of cognition and memory functions in cognitively impaired patients, leisure activities centered on cognitive and memory training have become more popular in recent years as rehab methods.19 Leisure activities are broadly defined.20 Within the context of this study, leisure activities are defined as non-professional, voluntary, and enjoyable activities primarily designed to improve cognitive function through engagement in structured, non-clinical tasks. Specifically, they include three categories:Virtual reality (VR) games: Computer-generated immersive environments that require interactive cognitive tasks (eg, memory puzzles); Board games: Tabletop games involving strategic thinking, rule-based decision-making, and memory (eg, mahjong); Interactive games: Motion-based or rhythm-based activities using dynamic feedback (eg, Xbox Kinect games). This definition emphasizes activities that combine entertainment with cognitive stimulation, distinguishing them from formal cognitive rehabilitation training. VR technology uses computers and other devices to create a lifelike 3D virtual world with visual, tactile, and olfactory experiences, giving users an immersive feeling. VR-based games are used to train and improve cognitive impairment in elderly individuals.21 Studies have shown that VR games enhance cognitive skills in older adults,22,23 although it is unclear whether they are better than TCRT games are. Board games have been in use for thousands of years24 and include games such as mahjong, poker, chess, and Go. Many studies have shown their significance in enhancing elderly individuals’ cognitive function.19,25–27 Interactive games use human motion and dynamic feedback. Players can control in-game characters or operations through physical movements, increasing immersion and interactivity.28 Neuroimaging research has indicated that regular engagement in interactive games for cognitive training can increase resting-state activity in the frontal and temporal lobes, supporting memory and enhancing overall cognition.29,30
Taking part in appropriate leisure activities has numerous advantages. Leisure activities can enhance cognitive function and memory, strengthen executive skills, and increase overall quality of life.31 In fact, these activities are becoming increasingly popular worldwide. They are not just fun hobbies for middle-aged and elderly people but also useful rehabilitation training for those with cognitive impairment.32 Leisure activities are now commonly used in complementary and alternative medicine to improve cognition and memory function.33 Many prospective studies suggest that regularly engaging in leisure activities such as gaming might reduce the risk of dementia and even depression.34,35 Additionally, some cross-sectional studies have revealed a connection between playing games and a lower dementia incidence rate.36 Yates et al reported that people with MCI had better capacity for activity, instrumental daily living skills, and basic motor functions after they participated in leisure activities.37
With leisure activities becoming increasingly popular for improving the health, mobility, and cognitive skills of older adults and the need for comparative assessment and clinical guidance, we conducted a systematic review and meta-analysis of the available evidence. Our aim was to assess how leisure activities affect the cognitive and memory functions of patients with cognitive impairment.
Methods
This study followed the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).38 The protocol for this systematic review has been registered with PROSPERO (number CRD42024563951). This study conducted a meta-analysis by systematically searching and integrating published research data, all of which were sourced from publicly available academic literature and did not involve the collection of raw clinical data or studies on human subjects. Therefore, according to the ethical regulations of Heilongjiang Academy of Chinese Medicine, this study does not require approval from the ethics committee or informed consent from patients.
Search Strategy
The comprehensive search was conducted in the PubMed, Embase, Cochrane Library, Scopus, Web of Science, China National Knowledge Infrastructure, Wanfang, VIP, and Chinese Biomedical Literature Service System databases, with the search time set from the establishment of the databases until October 10, 2024. The search strategies are primarily composed of diseases (“cognitive impairment”, “memory impairment”), interventions (“leisure activities”, “Mahjong”, “poker”, “cards”, “chess”, “Chinese chess”, “digital games”, “jigsaw puzzles”, “virtual reality”), and type of research (“randomized controlled trials”). See Appendix 1. for the detailed search.
Inclusion and Exclusion Criteria
We limited our evidence to studies published in peer-reviewed journals, and we applied the PICOS principles to establish the inclusion and exclusion criteria for this study. Additionally, manuscripts published exclusively online were also included in our review.
P (participant): The subjects in the study met the diagnostic criteria for cognitive impairment and were at least 18 years old. There were no restrictions on the sex or race of the subjects.
I (intervention): The subjects included in the study will receive leisure activity interventions, with the primary rehabilitation treatment methods including Go, poker, mahjong, VR games, and interactive games. There will be no restrictions on the stimulation site, duration, or frequency.
C (control): The control group received a nonleisure activity intervention or a lower frequency leisure activity intervention.
O (outcome): Efficacy of intervention on (1) the Montreal Cognitive Assessment (MoCA) and Mini-Mental State Examination (MMSE), (3) the digit span forward (DSB), (4) the digit span backward (DSF), (5) the trail-making test-A (TMT-A), (6) the trail-making test-B (TMT-B), and (7) activities of daily living (ADL).
S (Study Design): All the included studies were randomized controlled trials.
The exclusion criteria included duplicate studies, animal studies, reviews, conference papers, and studies with incomplete data. Due to resource constraints, non-Chinese or English studies (eg, Korean) were excluded. While attempts were made to retrieve data via author contact, language barriers may have resulted in potential omissions. In order to maintain consistency in the measurement results, studies using alternative tests that are inconsistent with our predefined diagnostic framework were excluded. This study only included studies using specific tests such as MMSE, MoCA, DSF, DSB, TMT-A, TMT-B, and ADL to diagnose cognitive impairment.
Data Extraction
Two assessors (HXM and LCM) extracted data from the eligible articles, covering details such as publication year, data source, participant demographics (gender, age, education level), intervention methods, and outcome measures. For any missing or inaccessible data, we contacted the authors via phone or email. The outcomes from each study are reported as the means with standard deviations (means ± SDss). In cases where data were presented in different formats (eg, quartiles, means ± standard errors, or confidence intervals), we converted them according to the guidelines in the Cochrane Handbook while noting any potential errors that might result from this conversion process. All included studies declared ethical approval by institutional review boards and adherence to the Declaration of Helsinki. During data extraction, we verified ethical compliance.
Risk of Bias Assessment
Two review authors (HEM and LCM) independently evaluated the risk of bias in the selected studies using the Physical Therapy Evidence Database (PEDro) scale.39,40 This scale comprises 11 criteria, with each criterion being awarded a score of 1 (note that the first criterion, related to eligibility, is not scored). The total score ranges from 0 to 10, where higher scores reflect better experimental quality. Any disagreements were resolved through discussions with a third author (LZY).
Statistical Analyses
All meta-analyses were performed using R studio. For continuous outcome data, we used the mean ± standard deviation (SD) or standardized mean difference (SMD) along with the 95% confidence interval (CI) for analysis. The I² statistic was used to assess the degree of heterogeneity, with I² values of 25%, 50%, and 75% indicating low, moderate, and high heterogeneity, respectively. In cases of significant heterogeneity, we identified its source through sensitivity analysis, which was conducted on the basis of the type of intervention. If the I² value exceeds 50%, a random effects model will be applied; otherwise, a fixed effects model will be used for data evaluation. Publication bias was assessed using Egger’s regression test.41
Results
Results of the Database Search
As shown in Figure 1, a total of 8,185 articles were retrieved from 9 different databases. Following the application of the inclusion and exclusion criteria, 4,310 references were initially screened. Among these, 343 articles were selected for full-text analysis, but 323 were subsequently excluded. In the end, this study included a total of 20 randomized controlled trials (RCTs), which were analyzed to evaluate the relevant outcomes.
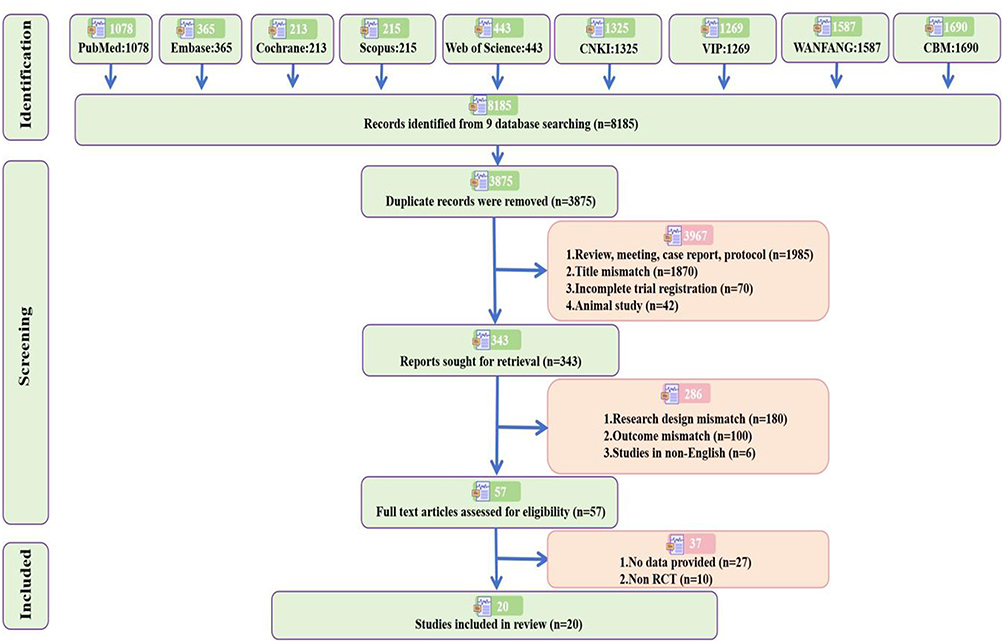 |
Figure 1 PRISMA flowchart of the literature search and screening. |
Characteristics of the Included Studies
Table 1 offers a comprehensive summary of the studies included in this analysis. Among the 20 studies, 19 were RCTs, and 1 was a cluster RCT. The studies were geographically diverse, with 13 originating from China (including 2 from Taiwan, China), 3 from Korea, and 1 each from Pakistan, Türkiye, Iran, and Japan.
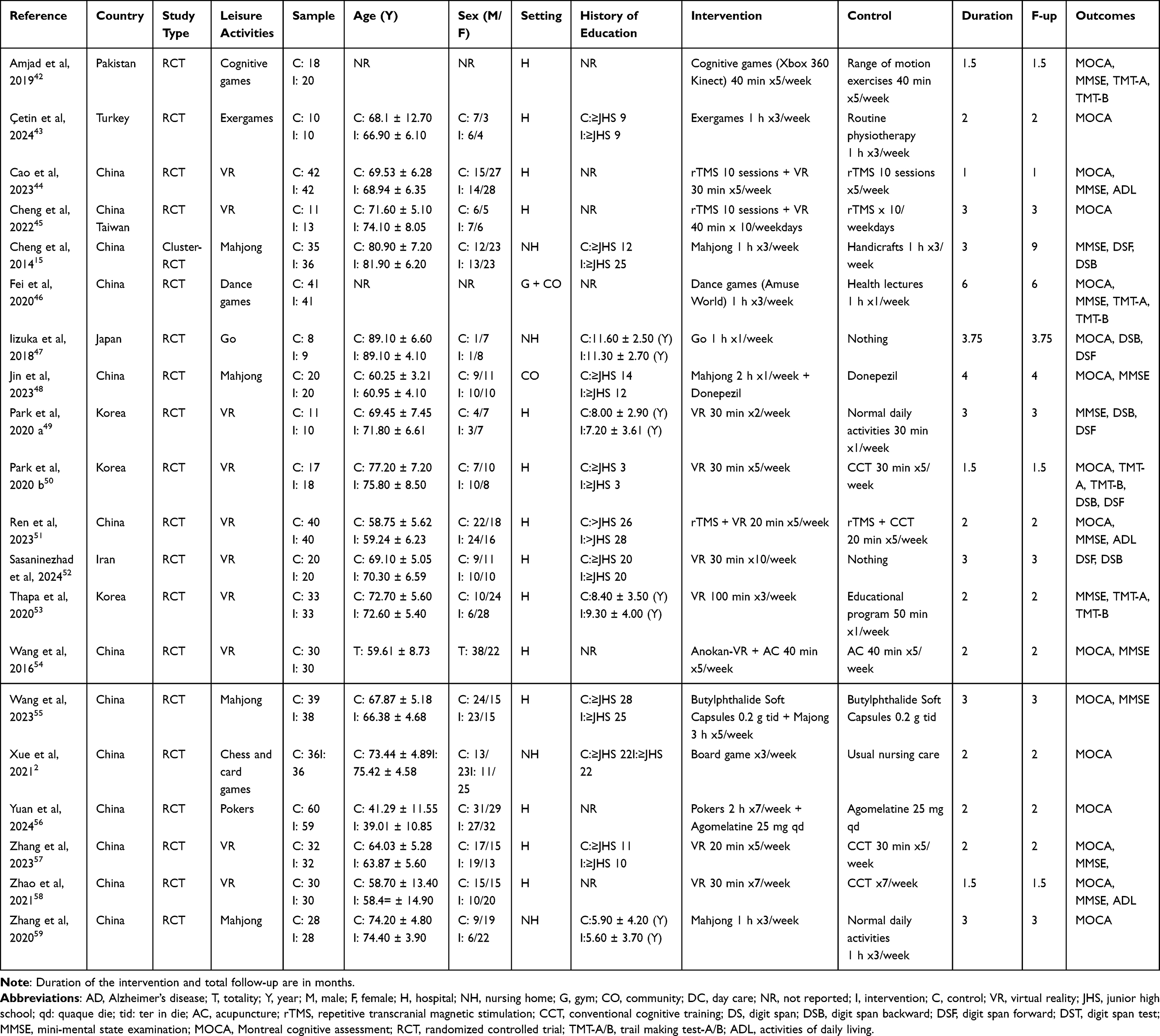 |
Table 1 Characteristics of the Included Studies |
The sample size ranged from 17 to 119 elderly people with cognitive impairment, with a total of 1126 elderly people with cognitive impairment participating in these studies. In all the studies, 565 elderly individuals with cognitive impairments were assigned to leisure activities (intervention group), whereas 561 elderly individuals with cognitive impairments participated in traditional nursing routine training (control group). After 3 surveys that did not indicate the gender ratio of participants were excluded, the overall gender ratio in this study was comparable, with 51.9% of males in the intervention group and 55.4% in the control group. Seven studies did not report the education level of the participants. Nine studies categorized education level as a categorical variable, whereas the remaining studies treated it as a continuous variable. All participants in the studies exhibited some form of cognitive impairment. Specifically, MCI was identified in fourteen studies, cognitive problems following stroke in one study, severe depression with cognitive impairment in one study, vascular cognitive impairment in one study, dementia in another study, and MCI associated with Parkinson’s disease in two studies.
Intervention Characteristics
The frequency of interventions ranged from once to ten times per week, with the overall treatment duration varying between 4 and 24 weeks. Each intervention session lasted from 20 to 120 minutes. The intervention group utilized several methods, including VR games (used in 10 studies), board games (used in 7 studies), and interactive games (used in 3 studies). The VR game interventions involved immersive VR experiences or games. The interactive game interventions included various rhythmic activities, such as cognitive games, exergames, and dance-based games. In contrast, the control group used nonleisure activities, including conventional cognitive training, health lectures, acupuncture, medication treatment, and other methods.
Risk of Bias
In this review, we employed the Cochrane risk assessment tool to comprehensively evaluate the risk levels of the studies included in our analysis. According to,60 studies that achieve a PEDro score of 6 or higher are considered high-quality or excellent-quality studies, reflecting their reliability and rigor. On the basis of these criteria, the 23 studies included in our analysis were all rated as high quality, with PEDro scores ranging from 6 to 9 (Table 2). We conducted Egger tests and generated funnel plots for studies with more than 10 entries (Supplementary Figures 1 and 2). The results revealed MOCA (t = 1.95, df = 14, P = 0.072) and MMSE (t = 1.76, df = 10, P = 0.108) scores. Overall, these studies were assessed as having low risk in terms of intergroup performance differences at baseline, evaluator blinding, dropout rates, and reporting of intergroup differences.
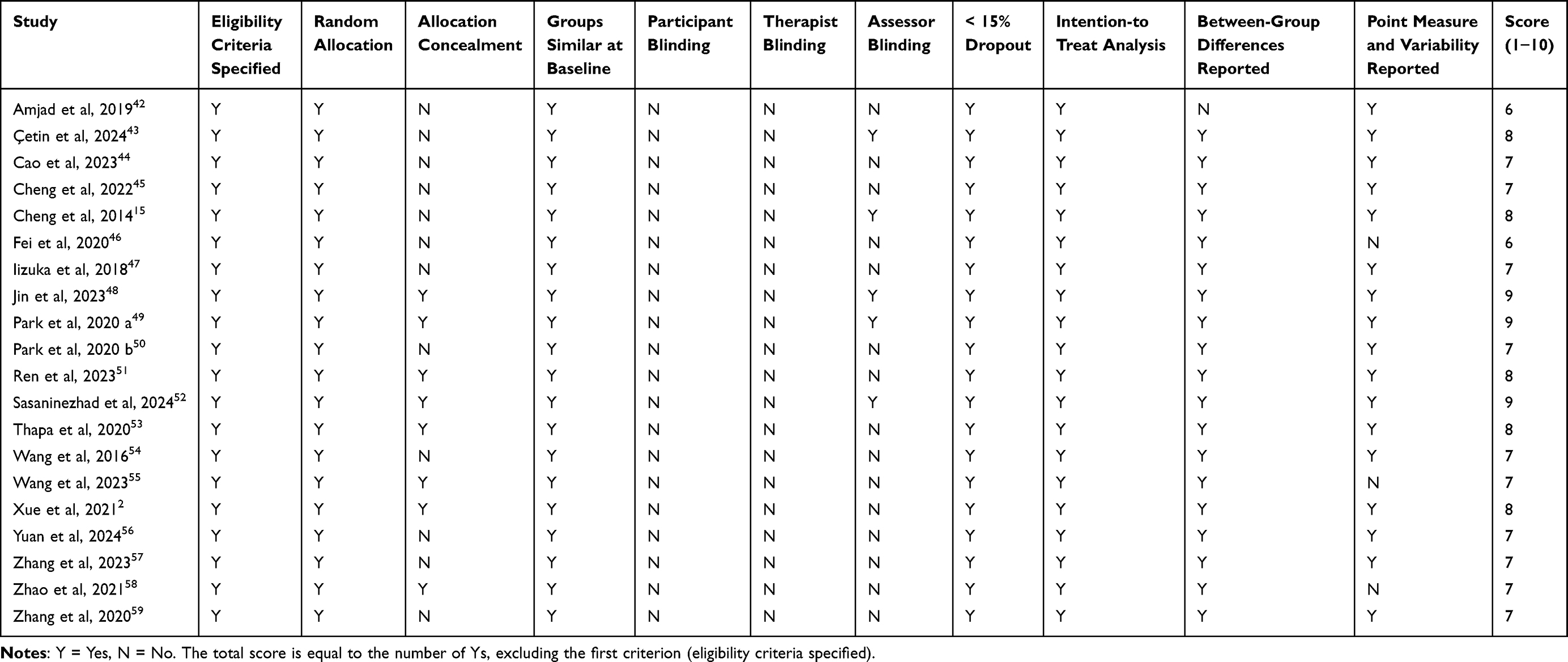 |
Table 2 Risks of Bias of the Included Studies |
Cognitive Function
Compared with the control group, the experimental group exhibited significantly higher MOCA scores (k = 16; SMD [95% CI] = 1.15 [0.24–2.07], P = 0.012) (Figure 2) and MMSE scores (k = 12; SMD [95% CI] = 1.10 [0.28–1.92], P = 0.013) (Figure 3). There was significant heterogeneity (MOCA: P < 0.0001, I2 = 86.2%; MMSE: P < 0.0001, I2 = 90.9%).
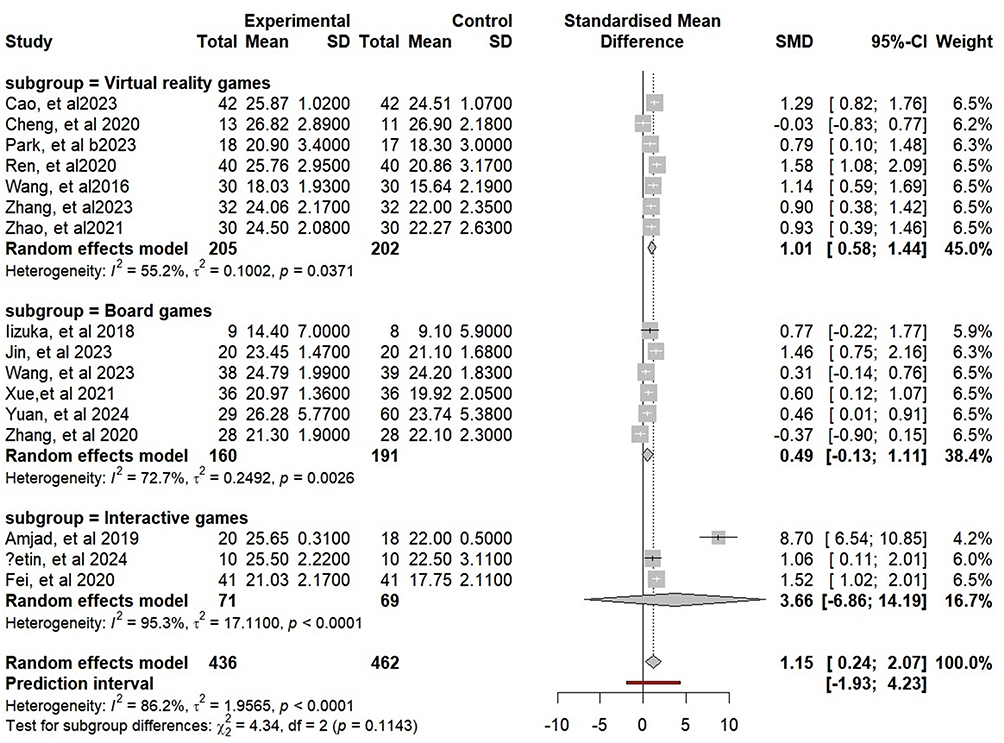 |
Figure 2 Forest plot of the impact of leisure activity intervention on MOCA. Abbreviation: MOCA, Montreal Cognitive Assessment. |
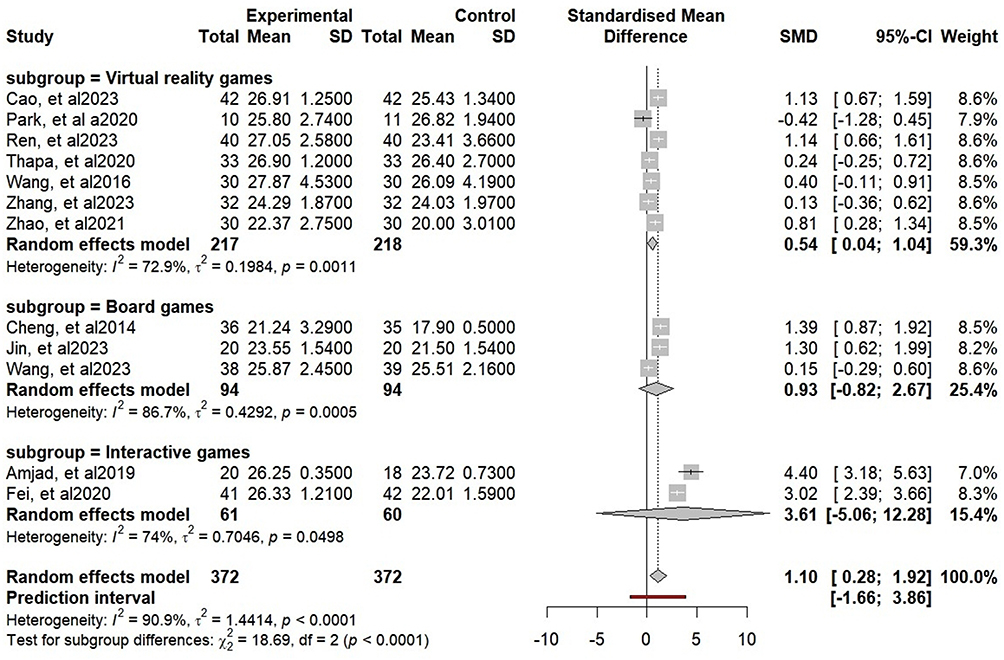 |
Figure 3 Forest plot of the impact of leisure activity intervention on MMSE scores. Abbreviation: MMSE, Minimum Mental State Examination. |
In the subgroup analysis, there was no significant difference in MOCA results among the subgroups, but the MMSE results were different (MOCA: P = 0.114; MMSE: P < 0.0001). Subgroup analysis revealed that the VR game subgroup (MMSE: SMD [95% CI] = 0.54 [0.04–1.04], I2 = 72.9%), board game subgroup (MMSE: SMD [95% CI] = 0.93 [−0.82–2.67], I2 = 86.7%), and interactive game subgroup (MMSE: SMD [95% CI] = 3.61 [−5.06–12.28], I2 = 74%) differed significantly from the control group. When studies using MOCA (k = 16) and MMSE (k = 12) were removed one by one, the effect sizes and heterogeneity remained largely unchanged (Supplementary Figures 3 and 4).
Memory Function
A positive effect on memory function was observed in the experimental group compared with the control group for DSB (k = 5) (SMD [95% CI] = 0.78 [0.48 to 1.09], P < 0.0001) (Figure 4) and DSF (k = 5) (SMD [95% CI] = 0.83 [0.27 to 1.39], P = 0.015) (Figure 5). There was no significant heterogeneity in either DSB or DSF (DSB: I² = 27%, P = 0.241; DSF: I² = 44%, P = 0.126).
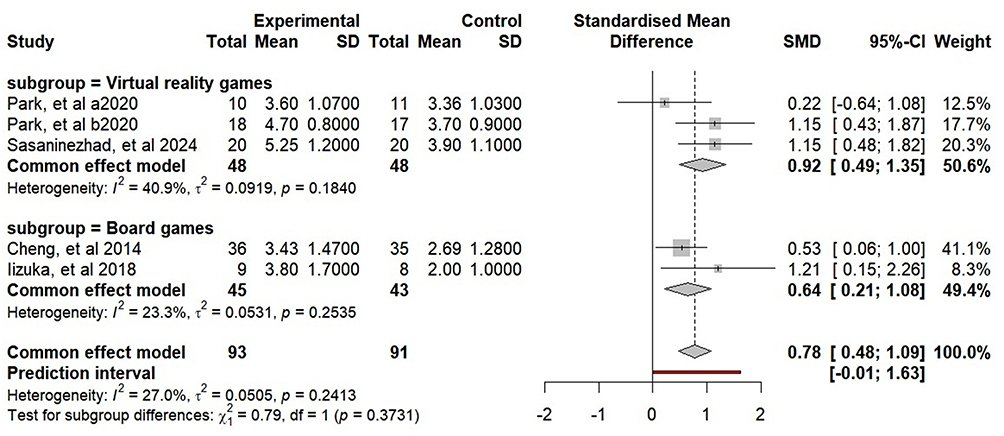 |
Figure 4 Forest plot of the impact of leisure activity intervention on DSB. Abbreviation: DSB, Digit Span. |
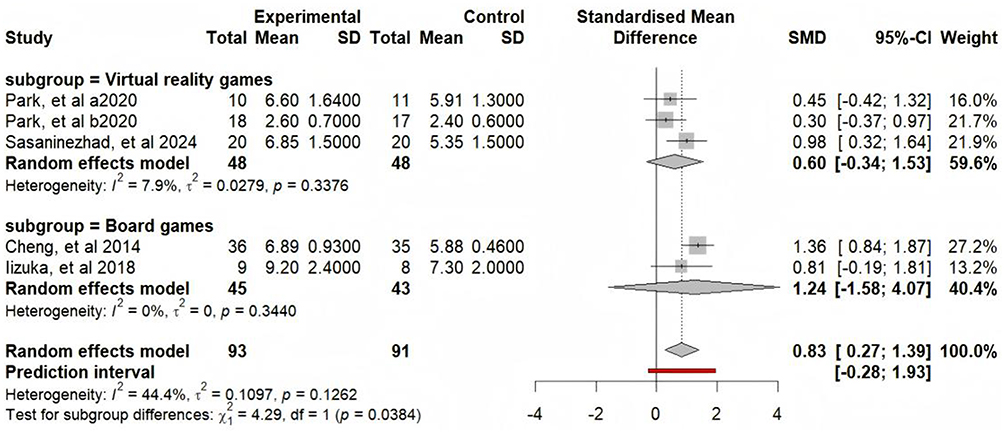 |
Figure 5 Forest plot of the impact of leisure activity interventions on the DSF. Abbreviation: DSF, Digit span forward. |
Subgroup analyses were conducted according to the memory function evaluation tool (DSB or DSF). There was no significant difference between the DSB subgroups, whereas the opposite results were observed for the DSF subgroup (DSB: P = 0.373; DSF: P = 0.038). Subgroup analysis revealed that the VR game subgroup (MMSE: SMD [95% CI] = 0.54 [0.04 to 1.04], I2 = 72.9%), board game subgroup (MMSE: SMD [95% CI] = 0.93 [−0.82 to 2.67], I2 = 86.7%), and interactive game subgroup (MMSE: SMD [95% CI] = 3.61 [−5.06 to 12.28], I2 = 74%) were significantly different from the control group.
In the subgroup analysis, compared with the control group, the VR game subgroup (DSF: SMD [95% CI] = 0.60 [−0.34 to 1.53], I2 = 7.9%) and Board game subgroup (DSF: SMD [95% CI] = 1.24 [−1.58 to 4.07], I2 = 0%) presented significant differences in the DSF. The studies that were included were removed one by one. Excluding,52 combined effect size (DSF: SMD, [95% CI] = 0.77, [−0.44 to 1.58], P = 0.056) was used. The results are presented in Supplementary Figures 5 and 6.
Executive Function
The TMT-A and TMT-B serve as the primary instruments for assessing executive ability. After the leisure activity intervention, there was no significant difference in the TMT-A (k = 4) (SMD [95% CI] = −1.31 [−3.20 to 0.58], P = 0.115) (Figure 6) or TMT-B (k = 4) scores (SMD [95% CI] = −2.09 [−6.95 to 2.77], P = 0.265) (Figure 7) relative to the control group, and significant heterogeneity was observed (TMT-A: P < 0.0001, I2 = 87%; TMT-B: P < 0.0001, I2 = 93%).
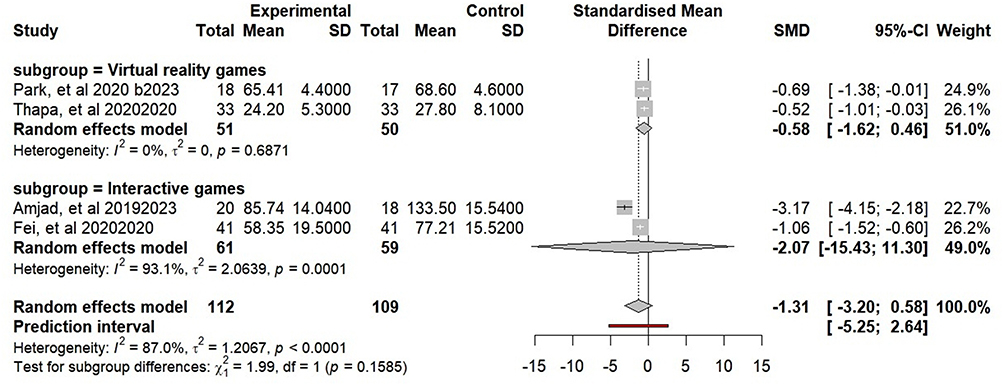 |
Figure 6 Forest plot of the impact of leisure activity intervention on TMT-A. Abbreviation: TMT-A, Trail making test-A. |
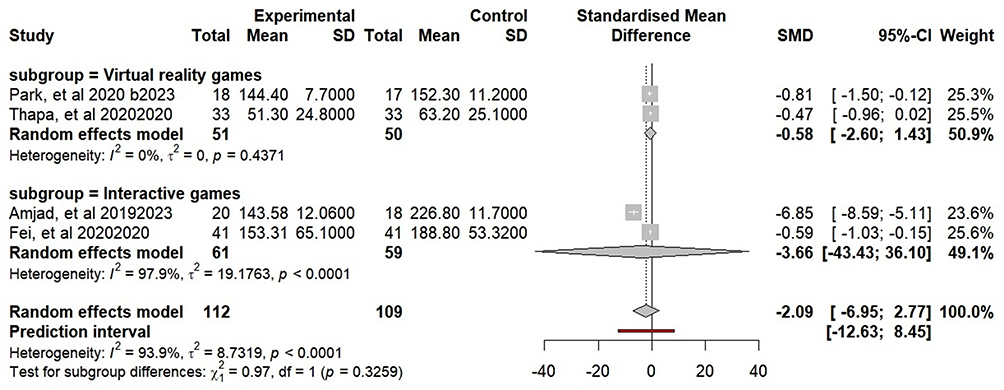 |
Figure 7 Forest plot of the impact of leisure activity intervention on TMT-B. Abbreviation: TMT-B, Trail making test-B. |
There were no notable differences between the subgroups (TMT-A: P = 0.159; TMT-B: P = 0.326). Subgroup analysis revealed that the VR subgroup (TMT-A: SMD [95% CI] = −0.58 [−1.62 to 0.46], I2 = 0%; TMT-B: SMD [95% CI] = −0.58 [−2.60 to 1.43], I2 = 0%) and the interactive games subgroup (TMT-A: SMD [95% CI] = −2.07 [−15.43 to 11.30], I2 = 93%; TMT-B: SMD [95% CI] = −3.66, [−43.43 to 36.10], I2 = 97%) exhibited decreased TMT scores. Excluding,42 the combined effect size was as follows: TMT-A: SMD, [95% CI] = −0.78, [−1.51 to −0.04], P = 0.0452; TMT-B: SMD, [95% CI] = −0.59, [−0.94 to −0.23], P = 0.0195. This finding indicates that the combined results may not be robust. For more information, please refer to Supplementary Figures 7 and 8.
Quality of Life
In the experimental group, the ADL scores (k = 3) (SMD [95% CI] = 0.81 [0.53 to 1.08], P < 0.0001) (Figure 8) were significantly higher than those in the control group. This finding indicates substantial heterogeneity in the results (ADL: P = 0.307, I2 = 15%).
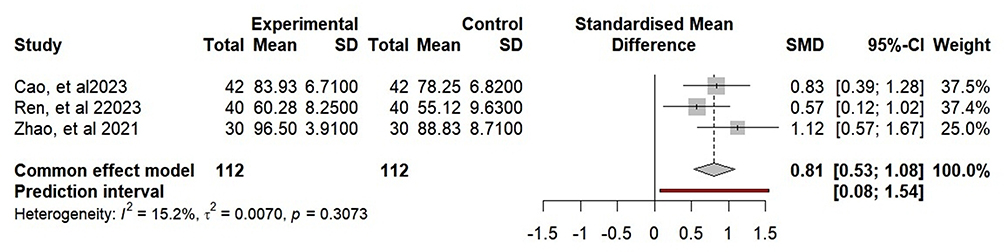 |
Figure 8 Forest plot of the impact of leisure activity intervention on ADLs. Abbreviation: ADL, Activities of Daily Living. |
Discussion
The benefits of leisure activities on cognitive function have been confirmed, but whether leisure activities can improve cognition and memory in patients with cognitive impairment remains unknown. Our study is the first to analyze the effectiveness of leisure activities on cognition and memory in patients with cognitive impairment. Overall, after leisure activity interventions, patients’ overall cognition, memory, executive ability, and quality of life improved.
Virtual Reality Games
VR games are a new rehab technique. VR games use computers to create virtual environments that mimic real objects and space.61 With sensing devices, patients can immerse themselves in these virtual cognitive settings and interact naturally.62 In 10 VR game studies, the VR game subgroup exhibited excellent consistency across cognitive tests such as the MOCA and MMSE. This approach minimized the degree of clinical heterogeneity. Subgroup analysis revealed that VR game interventions positively affected patients’ cognitive and memory function. The immersive, multisensory nature of VR games engages players, boosting immersion and memory in virtual worlds.
VR technology affects neural plasticity in multiple ways. VR technology can balance the cholinergic and dopamine systems (Kim et al, 2011) and release neurotrophic factors for nerve health.63 Research has shown that VR cognitive training can change neuronal plasticity through forced learning.64 During VR training, players may activate neural systems related to cognitive pathways by observing their movements, enhancing consciousness and cognitive function.65,66 This review revealed that VR game interventions are effective for cognitively impaired patients. VR games improve cognitive, memory, and quality of life. However, no statistical differences were observed in the execution of functions (TMT-A/B). This may be due to the complexity of the task, such as TMT-B requiring simultaneous visual tracking and cognitive transformation, which places high demands on executive function and may exceed the scope of current interventions. Therefore, VR games are recommended as alternatives to traditional cognitive rehabilitation for better cognitive and memory enhancement.
Board Games
This meta-analysis explores how board games can boost cognitive function in elderly, cognitively impaired patients. Among the seven studies included in the analysis, four focused on mahjong, whereas the rest focused on Go, poker, chess, and card games.
Subgroup analysis revealed that board game interventions significantly improved patients’ MOCA and MMSE scores. This aligns with recent research on mahjong’s ability to enhance cognitive skills and attention in the elderly. Iizuka et al reported that playing Go increases fluorodeoxyglucose uptake in the left temporal gyrus, improving memory task performance.47,67 Another study revealed that long-term Go players have more white matter connections in key brain areas, suggesting enhanced cognitive function and neural communication.68
However, in the included studies, the board game subgroup did not have a significant effect on memory function (DSF). This might be because Go’s simple black and white pieces limit certain cognitive improvements. Additionally, the intervention intensity and duration might not be enough to sustain relevant biological effects in executive function-related brain regions.
Overall, this meta-analysis indicates that board game interventions could be a potential treatment for improving cognitive function in cognitively impaired patients. However, more high-quality research is needed to confirm the overall results.
Interactive Games
Interactive games allow players to directly interact with their surroundings via body movements, and no complex controllers are needed. They are widely used in the rehabilitation of individuals with cognitive impairment. Common platforms are “Nintendo Wii” and “Microsoft Xbox 360 Kinect”.69 This study included only 3 relevant interactive game studies. During screening, we found little research on DSB and DSF applications, possibly due to different memory function evaluation criteria.
Interactive games follow task-oriented exercise principles, with repetition and high intensity as keys.70,71 Shepherd et al suggested that when neurons are damaged, repeated, strong activation of neural networks can reactivate brain pathways and improve function.72 In addition, a previous study suggested that interactive games can improve cognitive function in MCI patients. One possible reason for the improvement in cognition is that these games require participants to integrate attention resources,73,74 visual motor skills,75,76 processing speed,77,78 visual spatial ability,79,80 and executive function.81 However, in our study, there was no significant improvement in patients’ cognitive function, which may be due to some interactive games may prioritize attention or memory training over executive function. In conclusion, interactive games seem to enhance cognitive function. However, more in-depth research is needed to assess their reliability and long-term effects more completely.
The Relationship Between Intervention Duration, Frequency, and Cognitive Effects
Compared to TCRT (where effects may fade within 6–12 months), our analysis suggests that long-term leisure activities (≥6 months) show more persistent cognitive benefits, possibly due to their integration into daily life. However, short-term interventions (<3 months) showed inconsistent results, indicating potential decay of effects over time. The overall analysis showed that the correlation coefficient between the total intervention duration and the improvement of MOCA score was r=0.38 (p=0.02), and the correlation coefficient with the improvement of MMSE score was r=0.35 (p=0.03), indicating that a longer intervention period (such as 24 weeks vs 4 weeks) is more conducive to cognitive function improvement. Frequency analysis showed that the correlation coefficient between the number of interventions per week (1–10 times) and cognitive score improvement was r=0.15 (p=0.21), indicating that there was no statistically significant difference in the effect between “high-frequency short cycles” (such as 10 times per week x 4 weeks) and “low-frequency long cycles.
Strengths and Limitations
This meta-analysis offers the first, latest, and most comprehensive summary of how leisure activities can improve cognitive function in patients with various cognitive impairment etiologies. However, this study has limitations. First, blind method implementation in areas such as mahjong, poker, Go, and VR game interventions is difficult because of their unique nature. Second, the lack of quantitative indicators of exercise intensity in these studies makes direct cross-sectional comparisons difficult. Third, most board game intervention literature is from China, which may lead to regional bias. Fourth, this study excluded non English research, which may introduce selection bias. High-quality research from non-English countries (eg, Korean, Japan) might exist but was inaccessible due to language restrictions, potentially affecting the comprehensiveness of our findings. Future reviews should prioritize multilingual inclusion or professional translation support to mitigate this bias. This will help us better understand how effective leisure activities are in enhancing cognitive function among elderly, cognitively impaired people. Finally, a potential limitation is the variability in neuropsychological tests across included studies, which may affect the comparability of results.
Conclusion
Leisure activities could be a viable cognitive intervention for patients with cognitive impairment. Such activities can enhance cognitive function, memory, executive function, and quality of life, with effects on par with or even better than those of TCRT. Given the promising results of this review and the clinical challenges of TCRT, there is a substantial evidence to promote the integration of leisure activities as a supplement or alternative to evidence-based cognitive rehabilitation in treatment plans. This change is likely to yield positive results.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Huang F, Zhang M, Wang S. Changes in cognitive function among older adults: a latent profile transition analysis. Arch Gerontol Geriatr. 2019;80:12–19. doi:10.1016/j.archger.2018.09.006
2. Xue B, Xiao A, Luo X, Li R. The effect of a game training intervention on cognitive functioning and depression symptoms in the elderly with mild cognitive impairment: a randomized controlled trial. Int J Methods Psychiatr Res. 2021;30(4):e1887. doi:10.1002/mpr.1887
3. Korczyn AD. Parkinson’s and Alzheimer’s diseases: focus on mild cognitive impairment. Parkinsonism & Related Disorder. 2016;22(Suppl 1):S159–61. Parkinsonism Relat Disord. doi:10.1016/j.parkreldis.2015.09.053
4. Domínguez-Chávez CJ, Cj M, Salazar-González BC. Mild cognitive impairment: a concept analysis. Nurs Forum. 2019;54(1):68–76. doi:10.1111/nuf.12299
5. Edmonds EC, McDonald CR, Marshall A, et al. Early versus late MCI: improved MCI staging using a neuropsychological approach. Alzheimers Dement. 2019;15(5):699–708. doi:10.1016/j.jalz.2018.12.009
6. Petersen RC, Lopez O, Armstrong MJ, et al. Practice guideline update summary: mild cognitive impairment: report of the guideline development, dissemination, and implementation subcommittee of the American Academy of neurology. Neurology. 2018;90(3):126–135. doi:10.1212/wnl.0000000000004826
7. Cogollor JM, Rojo-Lacal J, Hermsdörfer J, et al. Evolution of cognitive rehabilitation after stroke from traditional techniques to smart and personalized home-based information and communication technology systems: literature review. JMIR Rehabil Assist Technol. 2018;5(1):e4. doi:10.2196/rehab.8548
8. Tangalos EG, Petersen RC. Mild cognitive impairment in geriatrics. Clin Geriatr Med. 2018;34(4):563–589. doi:10.1016/j.cger.2018.06.005
9. Barage SH, Sonawane KD. Amyloid cascade hypothesis: pathogenesis and therapeutic strategies in Alzheimer’s disease. Neuropeptides. 2015;52:1–18. doi:10.1016/j.npep.2015.06.008
10. Begcevic I, Brinc D, Brown M, et al. Brain-related proteins as potential CSF biomarkers of Alzheimer’s disease: a targeted mass spectrometry approach. J Proteomics. 2018;182:12–20. doi:10.1016/j.jprot.2018.04.027
11. Cioffi F, Adam RHI, Broersen K. Molecular mechanisms and genetics of oxidative stress in alzheimer’s disease. J Alzheimers Dis. 2019;72(4):981–1017. doi:10.3233/jad-190863
12. Ferreira-Vieira TH, Guimaraes IM, Silva FR, Ribeiro FM. Alzheimer’s disease: targeting the Cholinergic System. Curr Neuropharmacol. 2016;14(1):101–115. doi:10.2174/1570159x13666150716165726
13. Heppner FL, Ransohoff RM, Becher B. Immune attack: the role of inflammation in Alzheimer disease. Nat Rev Neurosci. 2015;16(6):358–372. doi:10.1038/nrn3880
14. Liu Z, Zhou T, Ziegler AC, Dimitrion P, Zuo L. Oxidative stress in neurodegenerative diseases: from molecular mechanisms to clinical applications. Oxid Med Cell Longev. 2017;2017:2525967. doi:10.1155/2017/2525967
15. Cheng ST, Chow PK, Song YQ, Yu EC, Lam JH. Can leisure activities slow dementia progression in nursing home residents? A cluster-randomized controlled trial. Int Psychogeriatr. 2014;26(4):637–643. doi:10.1017/s1041610213002524
16. Zhang T, Zhou R, Wang T, Xin Y, Liu X, Huang H. Effects of traditional mind-body movement therapy on chronic cardiopulmonary dyspnoea: a systematic review and meta-analysis. Thorax. 2023;78(1):69–75. doi:10.1136/thoraxjnl-2021-218030
17. Aziz NA, Leonardi-Bee J, Phillips M, Gladman JR, Legg L, Walker MF. Therapy-based rehabilitation services for patients living at home more than one year after stroke. Cochrane Database Syst Rev. 2008;2008(2):Cd005952. doi:10.1002/14651858.CD005952.pub2
18. Forster A, Lambley R, Hardy J, et al. Rehabilitation for older people in long-term care. Cochrane Database Syst Rev. 2009;(1):Cd004294. doi:10.1002/14651858.CD004294.pub2
19. Cheng ST, Chow PK, Yu EC, Chan AC. Leisure activities alleviate depressive symptoms in nursing home residents with very mild or mild dementia. Am J Geriatr Psychiatry. 2012;20(10):904–908. doi:10.1097/JGP.0b013e3182423988
20. Fancourt D, Aughterson H, Finn S, Walker E, Steptoe A. How leisure activities affect health: a narrative review and multi-level theoretical framework of mechanisms of action. Lancet Psychiatry. 2021;8(4):329–339. doi:10.1016/s2215-0366(20)30384-9
21. Tieri G, Morone G, Paolucci S, Iosa M. Virtual reality in cognitive and motor rehabilitation: facts, fiction and fallacies. Expert Rev Med Devices. 2018;15(2):107–117. doi:10.1080/17434440.2018.1425613
22. Gamito P, Oliveira J, Coelho C, et al. Cognitive training on stroke patients via virtual reality-based serious games. Disabil Rehabil. 2017;39(4):385–388. doi:10.3109/09638288.2014.934925
23. He D, Cao S, Le Y, Wang M, Chen Y, Qian B. Virtual reality technology in cognitive rehabilitation application: bibliometric analysis. JMIR Serious Games. 2022;10(4):e38315. doi:10.2196/38315
24. Pozzi FE, Appollonio I, Ferrarese C, Tremolizzo L. Can traditional board games prevent or slow down cognitive impairment? a systematic review and meta-analysis. J Alzheimers Dis. 2023;95(3):829–845. doi:10.3233/jad-230473
25. Zhu L, Wang Y, Wu Y, et al. Longitudinal associations between the frequency of playing Mahjong and cognitive functioning among older people in China: evidence from CLHLS, 2008-2018. Front Public Health. 2024;12:1352433. doi:10.3389/fpubh.2024.1352433
26. Cheng ST, Chan AC, Yu EC. An exploratory study of the effect of mahjong on the cognitive functioning of persons with dementia. Int J Geriatr Psychiatry. 2006;21(7):611–617. doi:10.1002/gps.1531
27. Ching-Teng Y. Effect of board game activities on cognitive function improvement among older adults in adult day care centers. Soc Work Health Care. 2019;58(9):825–838. doi:10.1080/00981389.2019.1656143
28. Liu Y, Song Y, Tamura R. Hedonic and utilitarian motivations of home motion-sensing game play behavior in china: an empirical study. Int J Environ Res Public Health. 17(23). doi:10.3390/ijerph17238794
29. Sato K, Ochi A, Watanabe K, Yamada K. Effects of dance video game training on cognitive functions of community-dwelling older adults with mild cognitive impairment. Aging Clin Exp Res. 2023;35(5):987–994. doi:10.1007/s40520-023-02374-2
30. Bellens A, Roelant E, Sabbe B, Peeters M, van Dam PA. A video-game based cognitive training for breast cancer survivors with cognitive impairment: a prospective randomized pilot trial. Breast. 2020;53:23–32. doi:10.1016/j.breast.2020.06.003
31. Särkämö T. Cognitive, emotional, and neural benefits of musical leisure activities in aging and neurological rehabilitation: a critical review. Ann Phys Rehabil Med. 2018;61(6):414–418. doi:10.1016/j.rehab.2017.03.006
32. Narme P. Benefits of game-based leisure activities in normal aging and dementia. Geriatr Psychol Neuropsychiatr Vieil. 2016;14(4):420–428. doi:10.1684/pnv.2016.0632
33. Verghese J, Lipton RB, Katz MJ, et al. Leisure activities and the risk of dementia in the elderly. N Engl J Med. 2003;348(25):2508–2516. doi:10.1056/NEJMoa022252
34. Dartigues JF, Foubert-Samier A, Le Goff M, et al. Playing board games, cognitive decline and dementia: a French population-based cohort study. BMJ Open. 2013;3(8):e002998. doi:10.1136/bmjopen-2013-002998
35. Kurita S, Doi T, Tsutsumimoto K, et al. Association of physical activity and cognitive activity with disability: a 2-year prospective cohort study. Phys Ther. 2020;100(8):1289–1295. doi:10.1093/ptj/pzaa052
36. Chiu YC, Huang CY, Kolanowski AM, et al. The effects of participation in leisure activities on neuropsychiatric symptoms of persons with cognitive impairment: a cross-sectional study. Int J Nurs Stud. 2013;50(10):1314–1325. doi:10.1016/j.ijnurstu.2013.01.002
37. Yates LA, Ziser S, Spector A, Orrell M. Cognitive leisure activities and future risk of cognitive impairment and dementia: systematic review and meta-analysis. Int Psychogeriatr. 2016;28(11):1791–1806. doi:10.1017/s1041610216001137
38. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097
39. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83(8):713–721. doi:10.1093/ptj/83.8.713
40. de Morton NA. The PEDro scale is a valid measure of the methodological quality of clinical trials: a demographic study. Aust J Physiother. 2009;55(2):129–133. doi:10.1016/s0004-9514(09)70043-1
41. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634. doi:10.1136/bmj.315.7109.629
42. Amjad I, Toor H, Niazi IK, et al. Xbox 360 kinect cognitive games improve slowness, complexity of EEG, and cognitive functions in subjects with mild cognitive impairment: a randomized control trial. Games Health J. 2019;8(2):144–152. doi:10.1089/g4h.2018.0029
43. Çetin B, Kılınç M, Çakmaklı GY. The effects of exergames on upper extremity performance, trunk mobility, gait, balance, and cognition in Parkinson’s disease: a randomized controlled study. Acta Neurol Belg. 2024;124(3):853–863. Epub 2024 Jan 5. PMID: 38182919. doi:10.1007/s13760-023-02451-3
44. Lianping Cao GY. Effect of VR technology combined with repetitive transcranial magnetic stimulation in the treatment of alzheimer’s disease mild cognitive impairment. J Hubei Univ Sci Technol. 2023;37(3):212–215. doi:10.16751/j.cnki.2095-4646.2023.03.0212
45. Cheng TC, Huang SF, Wu SY, Lin FG, Lin W-S, Tsai P-Y. Integration of virtual reality into transcranial magnetic stimulation improves cognitive function in patients with Parkinson’s disease with cognitive impairment: a proof-of-concept study. J Parkinsons Dis. 2022;12(2):723–736. PMID: 34897103. doi:10.3233/JPD-212978
46. Xiaoyan Fei JC. Intervention study of multi-modal dance exercise on cognitive function and footstep accuracy of elderly with mild cognitive impairment. J Heze Univ. 2020;42(5):79–82. doi:10.16393/j.cnki.37-1436/z.2020.05.017
47. Iizuka A, Suzuki H, Ogawa S, et al. pilot randomized controlled trial of the go game intervention on cognitive function. Am J Alzheimers Dis Other Demen. 2018;33(3):192–198. doi:10.1177/1533317517753362
48. Xuan Jin HZ, Qingjie S. Effect of mahjong training combined with donepezil on patients with cognitive impairment after ischemic stroke. Progress Clin Medi. 2023;13(3):4935–4941. doi:10.12677/ACM.2023.133704
49. Park JH, Liao Y, Kim DR. Feasibility and Tolerability of a Culture-Based Virtual Reality (VR) training program in patients with mild cognitive impairment: a randomized controlled pilot study. Int J Environ Res Public Health. 2020;17(9):3030. PMID: 32349413; PMCID: PMC7246563. doi:10.3390/ijerph17093030
50. Park JS, Jung YJ, Lee G. Virtual reality-based cognitive-motor rehabilitation in older adults with mild cognitive impairment: a randomized controlled study on motivation and cognitive function. Healthcare. 2020;8(3):335. PMID: 32932997; PMCID: PMC7551774. doi:10.3390/healthcare8030335
51. Hongyu Ren JM, Sen H, Mingxuan L, Cheng H, Haotian S. Analysis of the therapeutic effect of repetitive transcranial magnetic stimulation combined with virtual reality technology in patients with Parkinson’s disease and cognitive impairment. Chin J Exp Surg. 2023;40(11):2343. doi:10.3760/cma
52. Sasaninezhad M, Moradi A, Farahimanesh S, Choobin MH, Almasi-Dooghaee M. Enhancing cognitive flexibility and working memory in individuals with mild cognitive impairment: exploring the impact of virtual reality on daily life activities. Geriatr Nurs. 2024;56:32–39. doi:10.1016/j.gerinurse.2023.12.008
53. Thapa N, Park HJ, Yang JG, et al. The effect of a virtual reality-based intervention program on cognition in older adults with mild cognitive impairment: a randomized control trial. J Clin Med. 2020;9(5):1283. PMID: 32365533; PMCID: PMC7288029. doi:10.3390/jcm9051283
54. Dawei Wang LL, Vr A. Virtual reality rehabilitation training system combined with the original complex pass after the clinical observation of acupuncture treatment of mild cognitive dysfunction. 2016;16(13):17–18. doi:10.3969/j.issn.1671-3141.2016.13.010
55. Wei Wang RL, Zhou L, Chen X. Clinical observation of the treatment of mild vascular cognitive impairment with butadiene phthalide combined with mahjong exercise therapy. Chinese Health Care. 2023;41(15):35–38.
56. Fengying Yuan XF, Junmin Q. Effect of agomelatine combined with poker-based entertainment therapy on cognitive function in patients with first-episode major depressive disorder. Clin Focus. 2024;39(2):130–133. doi:10.3969/j.issn.1004-583X.2024.02.006
57. Liming Zhang LG, Xue C, Zhao Y, Zhao R, Liu A. Clinical effectiveness of virtual reality technology combined with repetitive transcranial magnetic stimulation for mild cognitive impairment in Parkinson’s disease. Chin J Rehabilitation. 2023;38(3):148–152. doi:10.3870/zgkf.2023.03.005
58. Rongrong Zhao GL, Guo C, Cai N, Zhao C. Application of virtual reality technology in cognitive rehabilitation training in patients with mild cognitive impairment. Neural Injury and Functional Reconstruction. 2021;16(10):590–592. doi:10.16780/j.cnki.sjssgncj.202210476
59. Zhang H, Peng Y, Li C, et al. Playing mahjong for 12 weeks improved executive function in elderly people with mild cognitive impairment: a study of implications for tbi-induced cognitive deficits. Front Neurol. 2020;11:178. PMID: 32292385; PMCID: PMC7120035. doi:10.3389/fneur.2020.00178
60. Lesinski M, Hortobágyi T, Muehlbauer T, Gollhofer A, Granacher U. Effects of balance training on balance performance in healthy older adults: a systematic review and meta-analysis. Sports Med. 2015;45(12):1721–1738. doi:10.1007/s40279-015-0375-y
61. Ren Y, Lin C, Zhou Q, Yingyuan Z, Wang G, Lu A. Effectiveness of virtual reality games in improving physical function, balance and reducing falls in balance-impaired older adults: a systematic review and meta-analysis. Arch Gerontol Geriatr. 2023;108:104924. doi:10.1016/j.archger.2023.104924
62. Lin X, Li R, Chen Z, Xiong J. Design strategies for VR science and education games from an embodied cognition perspective: a literature-based meta-analysis. Front Psychol. 2023;14:1292110. doi:10.3389/fpsyg.2023.1292110
63. Riva G, Mancuso V, Cavedoni S, Stramba-Badiale C. Virtual reality in neurorehabilitation: a review of its effects on multiple cognitive domains. Expert Rev Med Devices. 2020;17(10):1035–1061. doi:10.1080/17434440.2020.1825939
64. Maggio MG, De Cola MC, Latella D, et al. What about the role of virtual reality in Parkinson disease’s cognitive rehabilitation? preliminary findings from a randomized clinical trial. J Geriatr Psychiatry Neurol. 2018;31(6):312–318. doi:10.1177/0891988718807973
65. Mao H, Li Y, Tang L, et al. Effects of mirror neuron system-based training on rehabilitation of stroke patients. Brain Behav. 2020;10(8):e01729. doi:10.1002/brb3.1729
66. Buccino G, Solodkin A, Small SL. Functions of the mirror neuron system: implications for neurorehabilitation. Cogn Behav Neurol. 2006;19(1):55–63. doi:10.1097/00146965-200603000-00007
67. Iizuka A, Ishii K, Wagatsuma K, et al. Neural substrate of a cognitive intervention program using Go game: a positron emission tomography study. Aging Clin Exp Res. 2020;32(11):2349–2355. doi:10.1007/s40520-019-01462-6
68. Lee B, Park JY, Jung WH, et al. White matter neuroplastic changes in long-term trained players of the game of “Baduk” (GO): a voxel-based diffusion-tensor imaging study. Neuroimage. 2010;52(1):9–19. doi:10.1016/j.neuroimage.2010.04.014
69. Bower KJ, Louie J, Landesrocha Y, Seedy P, Gorelik A, Bernhardt J. Clinical feasibility of interactive motion-controlled games for stroke rehabilitation. J Neuroeng Rehabil. 2015;12:63. doi:10.1186/s12984-015-0057-x
70. Laver KE, Lange B, George S, Deutsch JE, Saposnik G, Crotty M. Virtual reality for stroke rehabilitation. Cochrane Database Syst Rev. 2017;11(11):Cd008349. doi:10.1002/14651858.CD008349.pub4
71. Swanson LR, Whittinghill DM. Intrinsic or extrinsic? using videogames to motivate stroke survivors: a systematic review. Games Health J. 2015;4(3):253–258. doi:10.1089/g4h.2014.0074
72. Shepherd RB. Exercise and training to optimize functional motor performance in stroke: driving neural reorganization? Neural Plast. 2001;8(1–2):121–129. doi:10.1155/np.2001.121
73. Kronenberg G, Bick-Sander A, Bunk E, Wolf C, Ehninger D, Kempermann G. Physical exercise prevents age-related decline in precursor cell activity in the mouse dentate gyrus. Neurobiol Aging. 2006;27(10):1505–1513. doi:10.1016/j.neurobiolaging.2005.09.016
74. Audiffren M, Tomporowski PD, Zagrodnik J. Acute aerobic exercise and information processing: energizing motor processes during a choice reaction time task. Acta Psychol. 2008;129(3):410–419. doi:10.1016/j.actpsy.2008.09.006
75. Swain RA, Harris AB, Wiener EC, et al. Prolonged exercise induces angiogenesis and increases cerebral blood volume in primary motor cortex of the rat. Neuroscience. 2003;117(4):1037–1046. doi:10.1016/s0306-4522(02)00664-4
76. Chen Hi HI, Chiang IP, Jen CJ. Exercise training increases acetylcholine-stimulated endothelium-derived nitric oxide release in spontaneously hypertensive rats. J Biomed Sci. 1996;3(6):454–460. doi:10.1007/bf02258049
77. Kempermann G, Fabel K, Ehninger D, et al. Why and how physical activity promotes experience-induced brain plasticity. Front Neurosci. 2010;4:189. doi:10.3389/fnins.2010.00189
78. Shatil E. Does combined cognitive training and physical activity training enhance cognitive abilities more than either alone? A four-condition randomized controlled trial among healthy older adults. Front Aging Neurosci. 2013;5:8. doi:10.3389/fnagi.2013.00008
79. Tang D, Chen J, Xu P. The effect of digital era on human visual working memory. Brain Behav. 2025;15(1):e70220. doi:10.1002/brb3.70220
80. Zhang YX, Tang DL, Moore DR, Amitay S. Supramodal enhancement of auditory perceptual and cognitive learning by video game playing. Front Psychol. 2017;8:1086. doi:10.3389/fpsyg.2017.01086
81. Green CS, Bavelier D. Exercising your brain: a review of human brain plasticity and training-induced learning. Psychol Aging. 2008;23(4):692–701. doi:10.1037/a0014345
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Protective Effects of Pioglitazone on Cognitive Impairment and the Underlying Mechanisms: A Review of Literature
Alhowail A, Alsikhan R, Alsaud M, Aldubayan M, Rabbani SI
Drug Design, Development and Therapy 2022, 16:2919-2931
Published Date: 31 August 2022
Impact of DL-3-n-Butylphthalide on Progression in Alzheimer’s Disease: A Retrospective Cohort Analysis
Zhang Y, Qiu J, Shang Y, Zhao X, Yang S, Chen Y, Dai S, Ai M, Huang W, Zhang J, Liu X
Neuropsychiatric Disease and Treatment 2025, 21:2495-2511
Published Date: 18 November 2025
Determinants of Post-Stroke Cognitive Impairment After Acute Ischemic Stroke: A Systematic Review and Meta-Analysis
Shen F, Guo X
Neuropsychiatric Disease and Treatment 2026, 22:608599
Published Date: 9 July 2026