Back to Journals » Infection and Drug Resistance » Volume 15
Knowledge, Practice and Associated Factors of Health Care Workers on Prevention of Catheter-Associated Urinary Tract Infections in South Wollo Zone Public Hospitals, Northeast Ethiopia
Authors Mohammed O, Gedamu S ![]() , Birrie E
, Birrie E ![]() , Seid A, Dires A
, Seid A, Dires A ![]() , Goshiye D
, Goshiye D ![]()
Received 7 July 2022
Accepted for publication 16 September 2022
Published 29 September 2022 Volume 2022:15 Pages 5729—5739
DOI https://doi.org/10.2147/IDR.S380980
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Osman Mohammed,1 Sisay Gedamu,2 Endalk Birrie,3 Ali Seid,4 Abebe Dires,2 Debrnesh Goshiye3
1Firdews Medium Clinic, Haik Town, Ethiopia; 2Department of Comprehensive Nursing, School of Nursing and Midwifery, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia; 3Department of Pediatric and Child Health Nursing, School of Nursing and Midwifery, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia; 4Dessie Health Science College, Dessie, Ethiopia
Correspondence: Sisay Gedamu, Tel +251935574801, Email [email protected]
Introduction: Health care providers are responsible for inserting and maintaining urinary catheters. Hence, it is very important that health care professionals need to be skillful and knowledgeable to prevent urinary tract infection for those patients undergoing indwelling catheter. Thus, this study aimed to assess knowledge, practice and associated factors of health care workers on prevention of catheter-associated urinary tract infections in South Wollo zone public hospitals, Northeast Ethiopia.
Methods: An institution-based cross-sectional study design was employed by using a simple random sampling technique among 413 health care workers. Data were entered into Epi-Data version 4.6 and were exported to SPSS version 26 for analysis. Bivariable logistic regression analyses were performed, and variables with P-value less than 0.25 were fitted to multivariable logistic regression. In multivariable regression analysis, variables having p-value < 0.05 were declared as significant factors for outcome variable.
Results: Out of the total 413 health care workers, 298 (72.2%) had adequate knowledge and 233 (56.4%) had adequate level of practice towards catheter-associated urinary tract infection prevention. Received training [AOR = 2.33, 95% CI: 1.404– 3.889] and being bachelor degree holder [AOR = 1.90, 95% CI: 1.084– 3.359] were significantly associated with adequate knowledge. On the other hand, being master and doctor [AOR = 4.71, 95% CI: 1.768– 12.56], adequate level of knowledge [AOR = 2.90, 95% CI: 1.785– 4.723], received training [AOR = 2.09, 95% CI: 1.315– 3.338] and work experience ≥ 20 years [AOR = 5.82, 95% CI: 1.497– 22.69] were significantly associated with adequate level of practice.
Conclusion: A substantial proportion of health care workers had inadequate knowledge and practice towards catheter-associated urinary tract infection prevention. Therefore, health care workers should strictly follow infection prevention guidelines and should update their knowledge and practice by taking short and long term training.
Keywords: knowledge, practice, associated factors, catheter-associated urinary tract infection
Introduction
A catheter is a closed drainage aseptic system consisting of a path from the tip of the catheter inserted into the bladder to the urine collection bag. Catheterization is the procedure of introducing a urinary catheter into a patient’s urinary bladder through the urethra.1 Indwelling urinary catheter is used for indications of acute or chronic urinary retention, bladder obstruction, voiding difficulties, measurement of urinary output, perioperative management, end of life care, to allow perineal healing of wounds and management of intractable incontinence.1–3
A study revealed that, there were 13 different microbial agents involved in urinary tract infections (UTIs). Among these Escherichia coli was the most frequent microbial agent of UTIs and most of the isolated microorganisms were from women.4 However, another study showed that only 2% of uropathogenic Escherichia coli pathotypes isolated from patients with non-catheter-associated UTIs were armed with the mrkD gene. No significant correlations were detected between gender and carrying uropathogenic Escherichia coli with mrkD gene.5
Although urinary catheterization has many benefits, it is not without negatives. UTIs are the common health care infection and 57% are catheter-associated urinary tract infection (CAUTI). Long-term indwelling urinary catheter users often experience catheter-related problems which differ in type and frequency among individuals.6 In some participants having a catheter provides greater freedom while for others it restricted lives as a consequence of catheterization.7 While some persons had choices in catheters, many did not because of constraints.8
CAUTI can cause a lot of complications. It increases morbidity and the length of hospital stay. Besides, these patients would require extended courses of antibiotic use, subsequently providing a breeding ground for antibiotic-resistant strains.3,9,10 The high prevalence of antibiotic resistance and virulence genes in conjunction with a significant relationship between the strains reveals a high pathogenic capacity of the isolated microorganism. This leads to the choice of more effective antibiotic regimens for treatment of infections.11 CAUTI leads to catheter blockage, development of renal stones or stones along the urinary tract.12,13 It also creates urine leakage, urethral strictures, gross hematuria and developed bladder cancer.14 Another study revealed that the most significant catheter complications were severe mechanical trauma, symptomatic bacterial infection, and anaphylaxis, hypersensitivity and catheter toxicity.15,16 The worst part is that the cost of care is significantly raised in such patients, especially if it is complicated by bacteremia, meningitis and septic shock which significantly increase the risk of mortality in these patients.17
While CAUTI is common, it is preventable by using evidence-based guidelines for appropriate indwelling urinary catheter use, insertion, maintenance and care. CAUTI prevention practices are commonly followed by wearing gloves, hand washing, maintaining a sterile barrier, using a no-touch insertion technique and limiting duration of the placement of urinary catheters.18,19
Reducing the risk of CAUTI involves a collaborative effort between different stakeholders. But engagement of health care workers to prevent CAUTI is vital.20 Their knowledge regarding the indication of catheterization was suboptimal.21 Health care workers also had an obligation to acquire appropriate knowledge and practices to prevent UTIs. However, different studies have documented that health care professionals had inadequate knowledge and practice towards CAUTI preventions. A study done in Mangaluru showed that the majority of nurses (80.85%) had average knowledge, 11.2% nurses had low knowledge and only a few (7.23%) nurses had high knowledge regarding prevention of CAUTI.22 Nearly half of participants (48.13%) in Pakistan had poor knowledge towards CAUTI prevention.23 In Nigeria and Rwanda, 23.3% and 64.52% of participants had poor knowledge of CAUTI prevention, respectively.24,25 In Egypt King Abdul-Aziz university hospital around two thirds of nurses (62.77%) had a low level of knowledge.26
With regard to CAUTI prevention practice, in a Nigeria tertiary care center 29.0% of respondents had poor practice.24 In King Abdul-Aziz university hospital 83.94% of nurses had a poor level of practices towards CAUTI prevention.26
With the presence of various findings in different settings in the world, studying knowledge and practice of health care workers towards prevention of CAUTI is unquestionable. In addition in the current study areas to the authors’ knowledge, there were no published data about CAUTI prevention knowledge and practice among health care workers until the data collection period of this study. So this study aimed to assess knowledge, practice and associated factors towards prevention of CAUTI among health care workers in public hospitals found in South Wollo zone, Northeast Ethiopia, 2021.
Methods and Materials
Study Area and Period
The study was conducted in South Wollo zone public hospitals from March 2021 to April 2021. South Wollo zone is bordered on the south by North Shewa, on the west by East Gojjam, on the northwest by South Gondar, on the north by North Wollo, on the northeast by Afar Region and on the east by Oromo Special Zone. There are 14 government hospitals in South Wollo zone. From the total of 14 government hospitals one third (5 hospitals) were selected randomly for our study.
Study Design
An institution based cross-sectional study design was conducted.
Population
The source population were all health care workers whose work was associated with catheter insertion in South Wollo zone public hospitals and the study population were all health care workers whose work was associated with catheter insertion in selected South Wollo zone public hospitals during the study period.
Inclusion and Exclusion Criteria
Inclusion criteria were all health care workers who served six months or more and whose work was associated with catheter insertion. But health care workers on annual leave, sick leave and study leave during the data collection period were excluded from the study.
Sample Size Determination
A single population proportion formula [n = (Z a/2)2 P(1 – P)/d2] was used to determine the required sample size. The assumptions used to calculate the sample size were: 95% level of confidence interval (Z a/2 = 1.96), 5% margin of error. Until the data collection period of this study to the researchers’ knowledge, there were no published data about health care workers knowledge and practice towards prevention of CAUTI in Ethiopia so that we used 50% proportion to get the maximum sample size assumptions. Then by adding a 10% non-response rate the final sample size was 422 health care workers.
Sampling Technique and Procedure
There are 14 public hospitals that deliver service for community in South Wollo zone. From the total 14 hospitals found in South Wollo, five hospitals (Akesta Hospital, Mekidela Hospital, Boru Meda Hospital, Dessie Comprehensive Specialized Hospital and Haik Hospital) were selected by using a lottery method. Then, proportional allocation was done to allocate samples to each hospital based on the number of health care workers. A simple random sampling technique was used to select the final study participants from the prepared sampling frame (Figure 1).
 |
Figure 1 Sampling procedure and technique to assess HCW knowledge and practice towards CAUTI prevention in South Wollo zone public hospitals, Northeast Ethiopia. |
Data Collection Tools
Data were collected by using a pretested and structured self-administered questionnaire developed after review of documents related to the topic of interest (Supplementary Figure 1). The tool consists of:
- Socio-demographic characteristics: consists of 9 questions aimed to gather information about the study participants’ background, which included age, gender, religion, marital status, educational status, profession, years of work experience, current working unit and attended training program on urinary catheter procedures.
- Knowledge questionnaires: examine the level of health care workers' knowledge on infection control in the use of urethral catheter. Knowledge towards prevention of CAUTI measured by 15 questionnaires. Each item had been coded in which one indicates correct answer and zero indicates incorrect answer.
- Practice questionnaires: examine health care workers' extent of practices on infection control in the use of urethral catheter. Practice towards prevention of CAUTI measured by 9 questionnaires. Every correct answer was given one point and wrong answer was given zero points.
- Attitude questionnaires: attitude of health care workers was assessed by 8 questions and the answers had to be given as whether they agree or disagree with the statements. The score of negative items were reversed to calculate the attitude.
Data Collection Procedures and Quality Assurance
Before Data Collection
The questionnaire was translated from English to Amharic language which is the local language of the study area. Three data collectors and two supervisors were provided a one day intensive training on the techniques of data collection, objectives of the study, ethical issues, procedures, tools and ways of collecting the data. Prior to data collection, a pretest was conducted among 21 individuals (5% of the sample size) who worked in Jamma Hospital. Based on the findings of the pre-test, ambiguous Amharic questionnaires were amended. To test the reliability of the tool, Cronbach alpha values were calculated for questions assessing knowledge and practice of health care workers towards prevention of CAUTI and were found to be 0.71 and 0.76, respectively.
During Data Collection
If the participant was not available during the first visit, an attempt was made to reach them twice again. By far, those with no opportunity to reach them at the third trial were considered as non-respondents. An ongoing checkup for completeness and consistency of responses was made by the supervisors on a daily basis.
After Data Collection
Data were entered into Epi-Data software version 4.6 then exported to SPSS. Data verification was conducted visually, by running frequency and cross-tabulation, and possible correction was made by cross-checking from the original questionnaires.
Operational Definitions
- Adequate knowledge: respondents who scored 8–15 correct answers from 15 knowledge questionnaires.
- Inadequate knowledge: respondents who scored 0–7 correct answers from 15 knowledge questionnaires.
- Adequate practice: respondents who got 5–9 correct answers from 9 practice questionnaires.
- Inadequate practice: respondents who got 0–4 correct answers from 9 practice questionnaires.
- Favourable attitude: if the score was above or equal to 4 from 8 attitude questionnaires.
- Unfavourable attitude: if the score was below 4 from 8 attitude questionnaires.
Data Process and Analysis
The data were initially coded, checked and entered into Epi-Data software version 4.1 then they were exported to SPSS software version 26.0 for cleaning and statistical analysis. Descriptive statistics such as frequencies‚ mean and standard deviation were carried out to see the distribution of the participants within the variables included in the study. After cross-tabulation of each explanatory variable with the outcome variable, binary logistic regression analysis was done. Variables with P-value less than 0.25 in bivariable analysis were selected as candidates for multivariable logistic regression analysis model. Statistical significant association was declared at a P-value less than 0.05 in multivariable logistic regression analysis. Adjusted odds ratio with its 95% CI was used to show the strength of association between explanatory and the outcome variables.
Results
Socio-Demographic, Knowledge and Practice Characteristics
From a total of 422 participants required, 413 health care workers were involved in the study, yielding a response rate of 97.9%. Among them, 241 (58.4%) participants were males. From those who had adequate knowledge towards CAUTI prevention, 179 (60.1%) of them were males. The mean age of respondents was 31.70 (SD ±5.91) years old, and 190 (46.0%) were ≤30 years. The majority 247 (59.8%) of the respondents were married followed by single, 144 (34.9%). Around two thirds of the respondents, 258 (62.5%) were bachelor degree holders. Among those who had adequate knowledge, 188 (63.1%) of participants were bachelor degree holders. From those who had adequate practice towards prevention of CAUTI, 151 (64.8%) of them were males. Of those health care providers who had adequate practice on CAUTI prevention, 162 (69.5%) of them were nurses. From the total who had adequate practice, 173 (74.2%) of the participants had work experience of ≤9 years (Table 1).
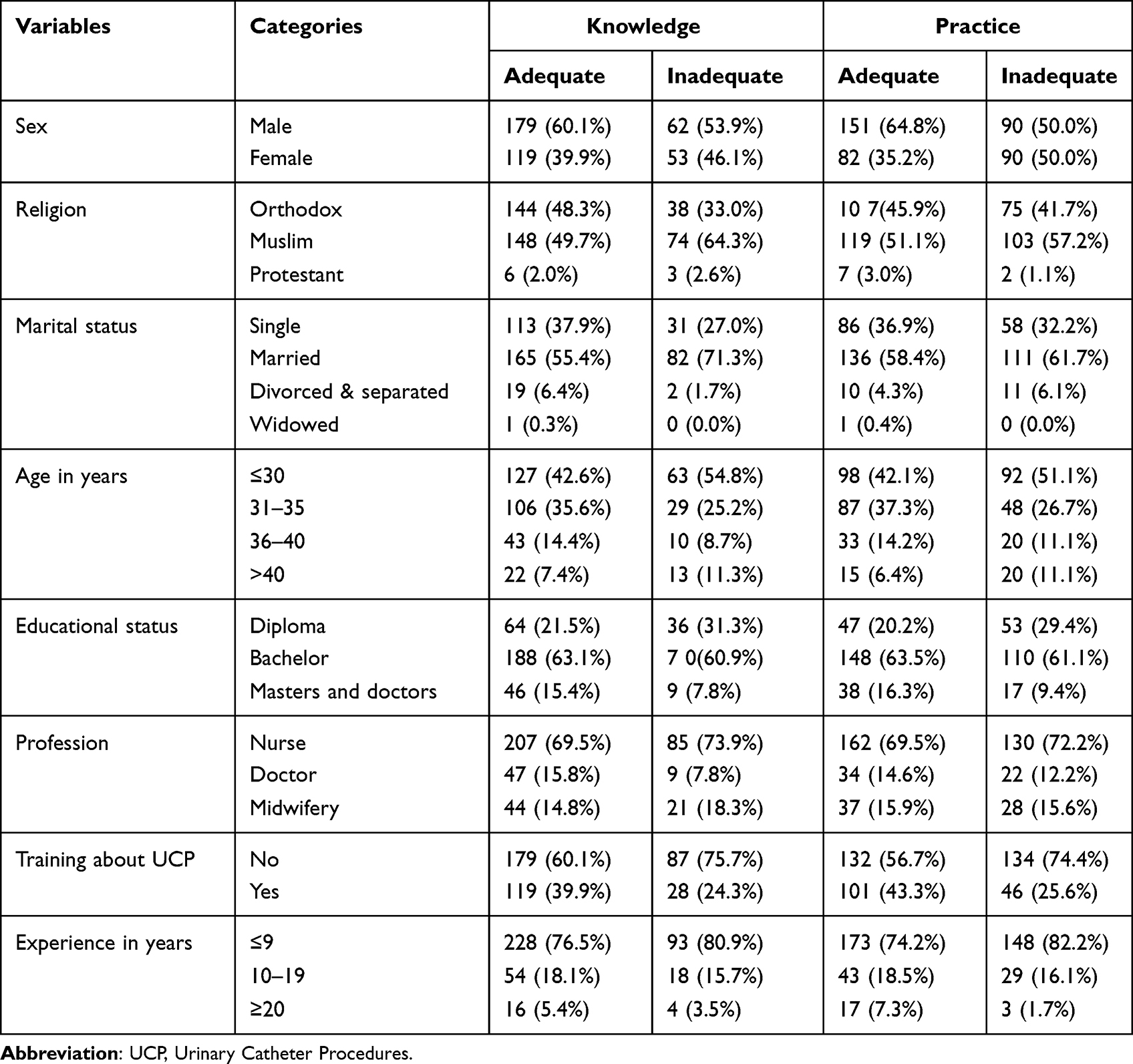 |
Table 1 Socio-Demographic Characteristics, Knowledge and Practice of Health Care Workers on Prevention of CAUTI in South Wollo Zone Public Hospitals, Northeast Ethiopia, 2021 |
Knowledge and Practice Towards Prevention of CAUTI
Considering the knowledge of the respondents, 298 (72.2%) health care workers had adequate level of knowledge. From the total of respondents, 233 (56.4%) had adequate level of practice towards CAUTI prevention (Figure 2).
 |
Figure 2 Knowledge and practice of health care workers on prevention of CAUTI in South Wollo zone public hospitals, Northeast Ethiopia, 2021. |
Factors Associated with Knowledge Towards Prevention of CAUTI
Variables with a p-value less than 0.25 in bivariable logistic regression analysis (educational status, profession, training, experience, sex and age) were entered into multivariable logistic regression and 2 of which had significantly association with knowledge at P-value <0.05.
Nurses who had a bachelor degree were about 2 times more likely to have adequate knowledge compared with a diploma [AOR = 1.90, 95% CI: 1.084–3.359]. Health care workers who got training about urinary catheter procedures were about 2 times more likely to have adequate knowledge when we compared with health care workers who did not get training [AOR = 2.33, 95% CI: 1.404–3.889] (Table 2).
 |
Table 2 Factors Associated with Knowledge of Health Care Workers on Prevention of CAUTI in South Wollo Zone Public Hospitals, Northeast Ethiopia, 2021 |
Factors Associated with Practice Towards Prevention of CAUTI
Considering bivariable logistic regression analysis, 7 independent variables (P-value <0.25) were entered into multivariable regression analysis and 4 of which had significantly association with practice.
Masters and doctors were about 5 times more likely to have adequate level of practice when compared with a diploma [AOR = 4.71, 95% CI: 1.768–12.56]. Individuals who had work experience equal to or greater than 20 years were about 6 times more likely to have adequate level of practice compared with workers who had work experience less than or equal to 9 years [AOR = 5.82, 95% CI: 1.497–22.69]. Health care workers who got training were about 2 times more likely to have adequate level of practice when we compared with health care workers who did not get training [AOR = 2.09, 95% CI: 1.315–3.338]. Furthermore, health care workers who had adequate level of knowledge were about 3 times more likely to have adequate level of practice compared with health care workers who had inadequate knowledge [AOR = 2.90, 95% CI: 1.785–4.723] (Table 3).
 |
Table 3 Factors Associated with Practice of Health Care Workers on Prevention of CAUTI in South Wollo Zone Public Hospitals, Northeast Ethiopia, 2021 |
Discussion
Knowledge and practice of health care workers towards CAUTI prevention are a critical concern. This study attempted to assess the level of knowledge, practice and associated factors among health care workers on prevention of CAUTI in South Wollo zone public hospitals. The study revealed that 72.2% [95% CI: 67.9–76.5%] of health care workers had adequate level of knowledge. This was higher than studies done in Pakistan (51.88%) and Egypt (37.23%) of respondents who were scored adequate level knowledge.23,26 But, this finding was lower than a study conducted in a selected hospital of Mangaluru, India (80.85%) of the respondents scored average level of knowledge.22 It was also lower than a study done in Nigeria (76.7%) of those scored fair level of knowledge.24 The variations between findings could be related to differences in sample size of the studies and socio-demographic characteristics of the participants.
In this study, educational status was an important factor of the level of knowledge. Health workers having a bachelor degree were about 2 times more likely to have adequate knowledge when compared with diplomas. This finding was consistent with the studies conducted in India and selected hospitals at Nellore.22,27 This could be due to the fact that health care workers who have more educational status can get more knowledge through the learning process. However, in this study, masters and doctors had increased level knowledge, but they did not show significant association.
On the other hand, the current study findings showed that health care workers who got training were about 2 times more likely to have adequate knowledge when compared with health care workers who did not get training. This finding was consistent with studies done at Nellore. This could be due to the fact that updating the knowledge of health workers through training about infection prevention principles could improve the older understanding and could have resulted in adequate score on knowledge questions.27
The study also showed that 56.4% [95% CI: 51.7–61.1%] of health care workers had adequate level of practice towards CAUTI prevention. This finding indicated the presence of a huge gap in CAUTI prevention practice among health care workers in the hospitals. This needs multidisciplinary involvement to reduce unnecessary indwelling urinary catheter use.28 Furthermore, a reminder to stop order of catheter use is also helpful to reduce CAUTI.29 In addition, using a protocol resulted in a reduction of catheter reinsertion rates and number of catheter days.30 This finding was higher than a study done in Egypt (16.1%) of respondents who were scored good level of practice.26 But, it was lower than study conducted in Nigeria where 71% of respondents had good level of practice.24 The possible reason for lower finding in the current study might be due to limited training about infection prevention, only 35.6% of health care workers received infection prevention training.
In this study, it was found that educational status was an important factor for adequate level of practice. Masters and doctors were about 5 times more likely to have adequate practice when we compared with diploma holders. The possible justification for this might be due to the reason that health care providers who had more educational status could get more skills through their advanced process of learning.
In the present study, experience of health care workers was an important factor for adequate level of practice. Professionals who had work experience greater than or equal to 20 years were about 6 times more likely to have adequate level of practice compared with workers who had work experience less than or equal to 9 years. This finding was supported by another study where longer duration of work experience was significantly associated with good practice of infection prevention.31 The strong positive association of this finding could be due to the fact that as the work service years increases, health care professionals were repeatedly exposed to infection prevention principles and became more experienced and increased practical implementation capability.
This study also revealed that health care professionals who had adequate level of knowledge were about 3 times more likely to have adequate level of practice compared with those health care providers who had inadequate knowledge towards CAUTI prevention. This finding is in line with a study conducted in Nigeria where practice was significantly associated with knowledge.24 However, it was contradicted with another study.26
Moreover, health care workers who got training were about 2 times more likely to have adequate level of practice when we compared with health care workers who did not get training. This result is supported by another study in which health care professionals who had taken infection prevention training were more likely to practice infection prevention than those who have not taken the training.31,32 The possible justification for this finding might be due to the fact that training could upgrade the knowledge and skill of health care providers in that they would easily comprehend basic principles, standards of practice and implement it accordingly.
In general in this study, a substantial number of health care workers had inadequate knowledge and practice regarding prevention of CAUTI. The possible justifications for this might be due to lower educational status (presence of diploma holders) of health care professionals, did not get training about CAUTI preventions and short duration of work experience. In addition, it might also due to poor health infrastructure of the health institutions in the study areas.
This study had possible limitations that the readers need to know. First, it could be related to the method of data collection used so that there could be social desirability and recall bias. Second, since we used a cross-sectional study design, the direction of relationship between variables cannot always be determined. Third, this study was carried out on 5 selected South Wollo zone government hospitals; our findings may not be representative at national level.
Conclusion
A significant number of health care professionals had inadequate knowledge and practice towards CAUTI prevention. The likelihood of knowledge significantly increased if health care workers had received training about urinary catheter procedures and bachelor degree holders. Furthermore, health care workers were more likely to have adequate practice if they were masters and doctors, adequate level of knowledge, took urinary catheter procedures training and work experience ≥20 years. Therefore, health care workers should strictly follow hospital acquired infection prevention guidelines and should update their CAUTI prevention knowledge and practice through reading and by taking short term training. Health care professionals should also upgrade their educational status. Hospital administrators should provide appropriative on job continuous training on CAUTIs prevention. Researchers should do further research by using observational study designs to determine actual practices.
Abbreviations
AOR, Adjusted Odds Ratio; CAUTI, Catheter-Associated Urinary Tract Infections; CI, Confidence interval; COR, Crude Odds Ratio; CSA, Central Statistical Agency; DCSH, Dessie Comprehensive Specialized Hospital; HCW, Health Care Workers; SPSS, Statistical Package for Social Science; UCP, Urinary Catheter Procedures, UTI, Urinary Tract Infection.
Data Sharing Statement
The data sets used and analyzed during this study are available from the corresponding author on reasonable request.
Ethical Consideration
Ethical clearance was obtained from Wollo University College of medicine and health science research ethical review committee. Communications with administrators of selected hospitals were held through formal letter. Before data collection written consent was obtained from all study participants after information is provided about the purpose of the study, non-invasiveness of the data collection procedure and confidentiality of the information. This study was conducted in accordance with the Declaration of Helsinki.
Consent for Publication
Not applicable. No individual personal details, images, or videos are being used in this study.
Acknowledgments
Authors would like to acknowledge data collectors, supervisors and the study participants for their valuable contribution to the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No organization funded this study.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Geng V, Cobussen-Boekhorst H, Farrell J, et al. Catheterisation. Indwelling Catheters in Adults. Urethral and suprapubic. Evidence-Based Guidelines for Best Practice in Urological Health Care. European Association of Urology Nurses (EAUN); 2012.
2. Kim B, Pai H, Choi WS, et al. Current status of indwelling urinary catheter utilization and catheter-associated urinary tract infection throughout hospital wards in Korea: a multicenter prospective observational study. PLoS One. 2017;12(10):e0185369. doi:10.1371/journal.pone.0185369
3. Chenoweth C, Saint S. Preventing catheter-associated urinary tract infections in the intensive care unit. Crit Care Clin. 2013;29(1):19–32. doi:10.1016/j.ccc.2012.10.005
4. Behzadi P, Behzadi E. The microbial agents of urinary tract infections at central laboratory of Dr. Shariati Hospital, Tehran, Iran. Turk Klin Tip Bilim. 2008;28(4):445.
5. Khonsari MS, Behzadi P, Foroohi F. The prevalence of type 3 fimbriae in Uropathogenic Escherichia coli isolated from clinical urine samples. Meta Gene. 2021;28:100881. doi:10.1016/j.mgene.2021.100881
6. Wilde MH, McMahon JM, Crean HF, Brasch J. Exploring relationships of catheter‐associated urinary tract infection and blockage in people with long‐term indwelling urinary catheters. J Clin Nurs. 2017;26(17–18):2558–2571. doi:10.1111/jocn.13626
7. Fowler S, Godfrey H, Fader M, Timoney AG, Long A. Living with a long-term, indwelling urinary catheter: catheter users’ experience. J Wound Ostomy Continence Nurs. 2014;41(6):597–603. doi:10.1097/WON.0000000000000069
8. Wilde MH, Brasch J, Zhang Y. A qualitative descriptive study of self‐management issues in people with long‐term intermittent urinary catheters. J Adv Nurs. 2011;67(6):1254–1263. doi:10.1111/j.1365-2648.2010.05583.x
9. Tenke P, Mezei T, Bőde I, Köves B. Catheter-associated urinary tract infections. Eur Urol Suppl. 2017;16(4):138–143. doi:10.1016/j.eursup.2016.10.001
10. Mohamed AH, Sheikh Omar NM, Osman MM, Mohamud HA, Eraslan A, Gur M. Antimicrobial resistance and predisposing factors associated with catheter-associated UTI caused by uropathogens exhibiting multidrug-resistant patterns: a 3-year retrospective study at a tertiary Hospital in Mogadishu, Somalia. Trop Med Int. 2022;7(3):42. doi:10.3390/tropicalmed7030042
11. Ahmadi M, Ranjbar R, Behzadi P, Mohammadian T. Virulence factors, antibiotic resistance patterns, and molecular types of clinical isolates of Klebsiella Pneumoniae. Expert Rev Anti Infect Ther. 2022;20(3):463–472. doi:10.1080/14787210.2022.1990040
12. Yuan F, Huang Z, Yang T, et al. Pathogenesis of Proteus mirabilis in Catheter-Associated Urinary Tract Infections. Urol Int. 2021;105(5–6):354–361. doi:10.1159/000514097
13. Norsworthy AN, Pearson MM. From catheter to kidney stone: the uropathogenic lifestyle of Proteus mirabilis. Trends Microbiol. 2017;25(4):304–315. doi:10.1016/j.tim.2016.11.015
14. Hollingsworth JM, Rogers MA, Krein SL, et al. Determining the noninfectious complications of indwelling urethral catheters: a systematic review and meta-analysis. Ann Intern Med. 2013;159(6):401–410. doi:10.7326/0003-4819-159-6-201309170-00006
15. Dellimore K, Helyer A, Franklin S. A scoping review of important urinary catheter induced complications. J Mater Sci Mater Med. 2013;24(8):1825–1835. doi:10.1007/s10856-013-4953-y
16. Young A, Mitacek R. Penile erosion in a paraplegic man with indwelling urinary catheter and scrotal edema. Urol Case Rep. 2017;12:62–63. doi:10.1016/j.eucr.2017.03.001
17. Nicolle LE. Catheter associated urinary tract infections. Antimicrob Resist Infect Control. 2014;3(1):1–8. doi:10.1186/2047-2994-3-23
18. Fink R, Gilmartin H, Richard A, Capezuti E, Boltz M, Wald H. Indwelling urinary catheter management and catheter-associated urinary tract infection prevention practices in nurses improving care for healthsystem elders hospitals. Am J Infect Control. 2012;40(8):715–720. doi:10.1016/j.ajic.2011.09.017
19. Clayton JL. Indwelling urinary catheters: a pathway to health care–associated infections. AORN J. 2017;105(5):446–452. doi:10.1016/j.aorn.2017.02.013
20. Fakih MG, Krein SL, Edson B, Watson SR, Battles JB, Saint S. Engaging health care workers to prevent catheter-associated urinary tract infection and avert patient harm. Am J Infect Control. 2014;42(10):S223–S229. doi:10.1016/j.ajic.2014.03.355
21. Jain M, Dogra V, Mishra B, Thakur A, Loomba PS. Knowledge and attitude of doctors and nurses regarding indication for catheterization and prevention of catheter-associated urinary tract infection in a tertiary care hospital. Indian J Crit Care Med. 2015;19(2):76. doi:10.4103/0972-5229.151014
22. Benny AM, Idiculla AS, Kunjumon A, George A, Sequera SK, Sequera SKL. Nurses’ knowledge on prevention of catheter-associated urinary tract infection in a selected hospital of mangaluru. J Health Allied Sci NU. 2020;10(03):128–131. doi:10.1055/s-0040-1716664
23. Shehzadi A, Ali A, Bhatti MR. Knowledge and attitude of nurses towards the prevention of catheter associated urinary tract infection in ICU, S of A Public Hospital Lahore. Saudi J Nurs Health Care. 2018;1(3):119–124.
24. Tobin E, Nnadi C, Ogedegbe S, et al. Prevention of catheter associated urinary tract infections: assessment of knowledge and practices among nurses in a tertiary care centre in Nigeria. Int J Infect Dis. 2020;101:274. doi:10.1016/j.ijid.2020.09.719
25. Mukakamanzi J. Knowledge, Attitude and Practices of Nurses Towards the Prevention of Catheter-Associated Urinary Tract Infection in Selected Referral Hospitals in Rwanda. University of Rwanda; 2017.
26. Algarni SS, Sofar SSS, Wazqar DY. Nurses’knowledge and Practices Toward Prevention of Catheter-Associated Urinary Tract Infection at King Abdulaziz University Hospital. J Health Med Nurs. 2019;4(1):50–73.
27. Prasanna K, Radhika M. Knowledge regarding catheter care among staff nurses. Int J Appl Sci. 2015;1(8):182–186.
28. Fakih MG, Dueweke C, Meisner S, et al. Effect of nurse-led multidisciplinary rounds on reducing the unnecessary use of urinary catheterization in hospitalized patients. Infect Control Hosp Epidemiol. 2008;29(9):815–819. doi:10.1086/589584
29. Meddings J, Rogers MA, Macy M, Saint S. Systematic review and meta-analysis: reminder systems to reduce catheter-associated urinary tract infections and urinary catheter use in hospitalized patients. Clin Infect Dis. 2010;51(5):550–560. doi:10.1086/655133
30. Jamil ML, Wurst H, Robinson P, et al. Urinary catheter alleviation navigator protocol (UCANP): overview of protocol and review of initial experience. Am J Infect Control. 2021;50:81–85. doi:10.1016/j.ajic.2021.06.019
31. Desta M, Ayenew T, Sitotaw N, Tegegne N, Dires M, Getie M. Knowledge, practice and associated factors of infection prevention among healthcare workers in Debre Markos referral hospital, Northwest Ethiopia. BMC Health Serv Res. 2018;18(1):1–10. doi:10.1186/s12913-018-3277-5
32. Al-Ahmari AM, AlKhaldi YM, Al-Asmari BA. Knowledge, attitude and practice about infection control among primary care professionals in Abha City, Kingdom of Saudi Arabia. Fam Med Prim Care Rev. 2021;10(2):662. doi:10.4103/jfmpc.jfmpc_1278_20
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge and Practice of Wound Care and Associated Factors among Nurses Working in South Wollo Zone Government Hospitals, Ethiopia
Tegegne B, Yimam F, Mengesha Yalew Z, Wuhib M, Mekonnen L, Asmamaw Yitayew Y, Ademe S, Tsegaye D, Eshetie Y, Chanie M
Chronic Wound Care Management and Research 2022, 9:1-11
Published Date: 20 July 2022
Knowledge, Attitudes, and Practices Regarding Ergonomic Hazards Among Healthcare Workers in a Saudi Government Hospital

ALHazim SS, Al-Otaibi ST, Herzallah NH
Journal of Multidisciplinary Healthcare 2022, 15:1771-1778
Published Date: 24 August 2022
Knowledge, Attitude, Perceived Responsibilities, and Associated Factors Regarding Colostomy Care Among Nurses Working in Surgical Units at Amhara Region General and Referral Hospitals, Ethiopia: A Mixed Method Study
Tiruneh TE, Alem G, Taddele M, Tizazu ZM, Minale FK, Alemu KD
Nursing: Research and Reviews 2022, 12:191-206
Published Date: 13 October 2022
Self-Medication Prevalence and Factors Associated with Knowledge and Attitude Towards Self-Medication Among Undergraduate Health Science Students at GAMBY Medical and Business College, Bahir Dar, Ethiopia
Siraj EA, Yayehrad AT, Kassaw AT, Kassahun D, Solomon E, Abdela H, Gizachew G, Awoke E
Patient Preference and Adherence 2022, 16:3157-3172
Published Date: 5 December 2022
Current Perspectives, Practices, and Barriers Faced by Community Pharmacists Regarding Pharmaceutical Care Services for Diabetes Mellitus in the United Arab Emirates
Jairoun AA, Al-Hemyari SS, Shahwan M, Jairoun SA, Alorfi NM, Zyoud SH, Suliman AA, Shahwan MK, Alnuaimi G, Shahwan M, Al-Qirim T, El-Dahiyat F
Journal of Multidisciplinary Healthcare 2024, 17:2563-2576
Published Date: 23 May 2024