Back to Journals » Journal of Asthma and Allergy » Volume 19
Knowledge, Attitudes, and Practices on Allergic Rhinitis Environmental Control and Treatment in China
Authors Yu L, Zhang P, Shang X, Tan Y, Guan R, Lin L, Lin W ![]() , Wang K, Chen L
, Wang K, Chen L
Received 31 October 2025
Accepted for publication 18 May 2026
Published 30 June 2026 Volume 2026:19 571410
DOI https://doi.org/10.2147/JAA.S571410
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Li Yu1, Peng Zhang1, Xiaojuan Shang1, Yi Tan1, Rui Guan1, Lulu Lin1, Wei Lin1, Kuiji Wang2, Luquan Chen1
1Department of Traditional Chinese Medicine, Beijing TongRen Hospital, Capital Medical University, Beijing, 100730, People’s Republic of China; 2Department of Otolaryngology, Head and Neck Surgery, Beijing TongRen Hospital, Capital Medical University, Beijing, 100730, People’s Republic of China
Correspondence: Luquan Chen, Email [email protected]
Purpose: To examine the knowledge, attitudes, and practices (KAP) of patients with allergic rhinitis (AR) regarding environmental control and treatment.
Patients and Methods: A cross-sectional survey was conducted from June to October 2024 at Beijing Tongren Hospital involving patients with AR. Data collection and KAP score assessments were performed using a valid, self-designed questionnaire. Pearson correlation analysis and structural equation modeling (SEM) were used to assess relationships among KAP dimensions and demographic factors.
Results: A total of 393 valid questionnaires were included, with 206 participants (52.42%) identified as female and 168 (42.75%) diagnosed with AR for over five years. The mean ± SD scores for knowledge, attitude, and practice were 12.06 ± 4.19 (range: 0– 20), 28.62 ± 4.30 (range: 9– 45), and 33.14 ± 6.15 (range: 10– 50), indicating insufficient knowledge and moderate attitude and practice. Knowledge was positively correlated with attitude (r = 0.277, P < 0.001) and practice (r = 0.527, P < 0.001), and attitude was positively correlated with practice (r = 0.283, P < 0.001). SEM indicated that employment status and marital status were significantly associated with KAP scores. Smoking habits and family history showed direct negative associations with knowledge, attitude, and practice.
Conclusion: Patients with AR show insufficient knowledge, along with moderate attitudes and practices toward environmental control and treatment. To improve AR management, healthcare providers should implement educational interventions that address knowledge deficits and foster positive attitudes and practices.
Keywords: knowledge, attitude, practice, allergic rhinitis, environmental control, cross-sectional study
Introduction
Allergic rhinitis (AR) is the most common allergic condition worldwide, affecting over 500 million people globally.1–3 In China alone, approximately 250 million people (17.6%) suffer from AR, which significantly impacts their quality of life and imposes a substantial economic burden on society.4 AR is a global health issue that affects people’s quality of life and work efficiency. Clinically, AR is defined as a series of symptoms caused by an IgE-mediated inflammatory response in the nasal mucosa following exposure to allergens.2 It is considered a systemic disease as nasal dysfunction can lead to both physical and psychological discomfort.
The cardinal symptoms of AR include nasal congestion, a runny, itchy nose, and sneezing, with sleep disturbances and impaired daily functions being common among patients.5–7 Ocular symptoms such as redness, lacrimation, and conjunctival infection are also frequently observed.8 Additionally, patients with AR are at an increased risk of sleep apnea, otitis media, and snoring.9 AR significantly reduces quality of life, affecting physical performance as well as work and study efficiency.
Sensitivity to environmental allergens is a hallmark of AR. House dust mites are the most common sensitizers in indoor environments, followed by grass pollens and animal epithelia outdoors.10–12 In China, house dust mites (HDMs) are the most prevalent allergens among patients with asthma and/or AR.13 In Beijing, inhaled allergens relevant to AR are mainly pollen, dust mites, and mold. In northern China, weed and seasonal pollen exposure is also a common sensitization pattern reported in AR.
Current treatment strategies for AR primarily involve environmental control, drug therapy, immunotherapy, and surgical treatment.4 According to the Knowledge, Attitude, and Practices (KAP) theory, knowledge forms the foundation for behavior change, while attitudes and beliefs serve as the driving force behind this change.14 The KAP theory outlines that behavior change occurs in three steps: acquiring knowledge, generating attitudes/beliefs, and forming practices/behaviors.15 While other assessment or decision-making frameworks (eg, AHP or Bayesian approaches) are often used for weighting indicators or probabilistic decision support, KAP provides a concise behavior-oriented structure that directly informs patient education and intervention design. However, cognitive changes resulting from knowledge acquisition do not necessarily translate into behavior change; this requires a shift in perception, which then leads to behavioral adjustments.16 In other applied research fields, comparative and statistical assessment frameworks have been used to summarize multidimensional conditions for decision-making.17 In recent KAP research, mediation analysis and structural equation modeling have also been increasingly used to examine pathways linking knowledge, attitude, and practice, providing methodological support for the present study.18,19
Environmental factors such as home dampness, fungal allergens, and mold stains are significantly associated with AR.20 A recent review summarized the evidence for indoor allergen exposure reduction strategies and noted mixed effects of specific environmental control measures on allergen levels and clinical outcomes.21 Despite its prevalence, many patients lack adequate knowledge and appropriate attitudes towards managing AR, which can exacerbate symptoms and reduce treatment efficacy.22,23 Enhancing patients’ knowledge, attitudes, and practices is crucial for effective disease management, particularly in regions like China, where environmental allergens like house dust mites are prevalent.
Recent studies in China have evaluated patients’ KAP toward AR in general and toward allergen-specific immunotherapy, but KAP specifically targeting environmental control behaviors remains limited. Therefore, this study aims to examine the KAP of patients with AR concerning environmental control and treatment, identifying gaps in patient education and behaviors to inform targeted interventions that enhance treatment outcomes and improve quality of life for this large and affected population. The questionnaire items were developed based on guideline-recommended environmental control and treatment components, which may help identify actionable targets for patient counseling in routine clinical practice.
Material and Methods
Study Design and Participants
This cross-sectional study was conducted between June and October, 2024 at Beijing Tongren Hospital. The study subjects were patients with AR. This study was conducted in accordance with the Declaration of Helsinki, and received ethical approval from the Ethics Committee of Beijing Tongren Hospital affiliated to Capital Medical University; informed consent was obtained from all participants. Inclusion criteria: (1) Meets the diagnostic criteria for allergic rhinitis in the Chinese Guidelines for Diagnosis and Treatment of Allergic Rhinitis (2022); (2) Age above 18 years old; (3) History of allergic rhinitis for more than 1 year; (4) Voluntarily participate in research and be able to understand and fill out questionnaires. Exclusion Criteria: (1) Incomplete questionnaire filling; (2) Selecting answers with logical errors in the questionnaire; (3) Participants who request to withdraw from this study.
Questionnaire Design
Prior to participating in the online survey, all potential respondents were presented with a detailed informed consent statement on the initial page of the questionnaire platform (Questionnaire Star). This statement clearly outlined the study’s purpose, procedures, assurance of confidentiality, and the voluntary nature of participation. Only participants who actively clicked the “Yes” option were allowed to proceed to the main body of the survey, ensuring that participation was entirely voluntary and based on informed consent.
The questionnaire design was based on the guidelines.4 After drafting the initial version of the questionnaire, it was revised following feedback from 2 experts who were chief physician and subsequently pilot tested on a small sample of 37 participants. The reliability of the final version, as indicated by a Cronbach’s α of 0.783, demonstrated good internal consistency. We also conducted a confirmatory factor analysis (CFA) with model-fit indices and standardized factor loadings in the Tables S1 and S2, Figure S1 in supplementary materials.
The final questionnaire, written in Chinese (with an English translation included in the Figure A1), consisted of five dimensions comprising a total of 44 items. The demographic characteristics section contained 15 items, the knowledge dimension included 10 items, the attitude dimension comprised 9 items, and the practice dimension consisted of 10 items. During the statistical analysis, scores were assigned based on the responses and the number of items. For the knowledge dimension, responses were scored as follows: “very familiar” was awarded 2 points, “heard of” received 1 point, and “not clear” was given 0 points, with a total possible score ranging from 0 to 20 points. Both the attitude and practice dimensions employed a five-point Likert scale, with scoring options ranging from very positive (5 points) to very negative (1 point).
In the attitude dimension, items 3, 4, 5, 7, and 9 were scored as a=5, b=4, c=3, d=2, e=1, while items 1, 2, 6, and 8 were reverse scored as a=1, b=2, c=3, d=4, e=5, yielding a possible score range of 9 to 45 points. For the practice dimension, items 2–10 were scored as a=5, b=4, c=3, d=2, e=1, and item 1 was reverse scored as a=1, b=2, c=3, d=4, e=5, resulting in a possible score range of 10 to 50 points. Based on their responses, participants’ knowledge was categorized into three levels: insufficient (0–10 points), moderate (10–14 points), or sufficient (15–20 points). The attitude dimension was similarly categorized as negative (9–22 points), neutral (23–31 points), or positive (32–45 points), while the practice dimension was classified as negative (10–25 points), moderate (26–35 points), or positive (36–50 points).
Data Collection and Quality Control
Questionnaires were distributed to the participants through convenient sampling. The electronic questionnaire was hosted on SoJump (http://www.sojump.com), an online survey platform. The questionnaire link was distributed to participants via Quick Response Code or through a WeChat group. Before answering the questions, participants were required to click the option “I agree to participate in this study” at the beginning of the e-questionnaire. All data were collected anonymously, and to prevent duplication, IP restriction was applied, allowing only one completion of the survey from a single IP address.
Sample Size
The calculation of sample size was based on the following formula employed in the cross-sectional study:24

where n denoted the sample size. Besides, p value was assumed to be 0.5 to achieve the maximum sample size. a refers to the type I error, which was set to 0.05 in this case. Subsequently,  was yielded 1.96.
was yielded 1.96.  represents the effect sizes between groups, which was determined as 0.06, and at least 267 participants should be required. As regards the 15% of non-response rate, a total of 315 participants are required to be involved.
represents the effect sizes between groups, which was determined as 0.06, and at least 267 participants should be required. As regards the 15% of non-response rate, a total of 315 participants are required to be involved.
Statistical Analysis
Data analysis was conducted using SPSS 26 and AMOS 26 (IBM, Armonk, NY, USA). Normally distributed variables were presented as mean ± SD, while categorical data were expressed as n (%). For comparing scores across different demographic characteristics, continuous variables underwent a normality test. Normally distributed data were expressed as mean ± SD, with t-tests for comparisons between two groups. Non-normally distributed data were expressed as median (range), with Mann–Whitney U-tests for comparisons. For three or more groups, one-way ANOVA was used if the data were normally distributed and variances were equal. Pearson correlation analysis was used to assess correlations between the three dimensions, and path-analysis model was conducted to explore relationships and mediation effects between KAP scores and demographic information. Because this was a cross-sectional study, SEM/path coefficients were interpreted as associative relationships rather than causal effects. The study hypothesizes that employment status, marital status, smoking habits, duration of AR, hyperlipidemia, and family history are associated with KAP among patients. Additionally, it is hypothesized that knowledge directly impacts both attitude and practice, and that attitude further influences practice. Demographic variables with statistically significant KAP scores among different subgroups were included in the path analysis. Then, after removing the demographic variables that were not statistically significant in the first round of model (unadjusted model), the adjusted path-analysis model was obtained. A two-sided P-value less than 0.05 was considered statistically significant.
Results
Demographic Characteristics
A total of 507 questionnaires were initially collected in this study. The following data were excluded: 1) 14 cases where the response time was less than 60 seconds; 2) 10 cases where the respondents were under 18 years of age; 3) 81 cases where respondents selected both “none of the above” and other underlying diseases; 4) 1 cases with invalid responses in the knowledge section; 5) 8 cases with missing values in the attitude section. This resulted in 393 valid questionnaires remaining (Figure 1). Among the participants, 206 (52.42%) were female, with a mean age of 38.19 ± 11.41 years. Additionally, 161 (40.97%) had an associate or bachelor’s degree, 168 (42.75%) had been diagnosed with AR for more than 5 years, 173 (44.02%) had a relative suffering from AR, and 195 (49.62%) were being treated with nasal spray or oral antiallergic medication. The mean ± SD scores for knowledge, attitude, and practice were 12.06 ± 4.19 (possible range: 0–20), 28.62 ± 4.30 (possible range: 9–45), and 33.14 ± 6.15 (possible range: 10–50), respectively, indicating insufficient knowledge, moderate attitude and practice. Analyses of demographic characteristics indicated that participants’ knowledge, attitude, and practice scores varied significantly across education level (P < 0.001, P = 0.030, P < 0.001), employment status (P < 0.001, P = 0.037, P < 0.001), marital status (P < 0.001, P < 0.001, P < 0.001), smoking habits (P < 0.001, P < 0.001, P < 0.001), drinking habits (P = 0.014, P = 0.021, P < 0.001), and digestive system diseases (P = 0.029, P = 0.019, P = 0.016). Furthermore, differences in knowledge scores were more likely among participants with varying average monthly income per capita (P = 0.018), duration of AR (P < 0.001), hyperlipidemia status (P < 0.001), atherosclerosis status (P = 0.001), depression or other psychological diseases (P = 0.020), and family history of AR (P < 0.001). Differences in attitude scores were more likely among those with different health insurance statuses (P = 0.043). Additionally, practice scores were more likely to vary based on gender (P < 0.001), duration of AR (P < 0.001), hyperlipidemia status (P = 0.001), atherosclerosis status (P = 0.019), and family history of AR (P = 0.003) (Table 1).
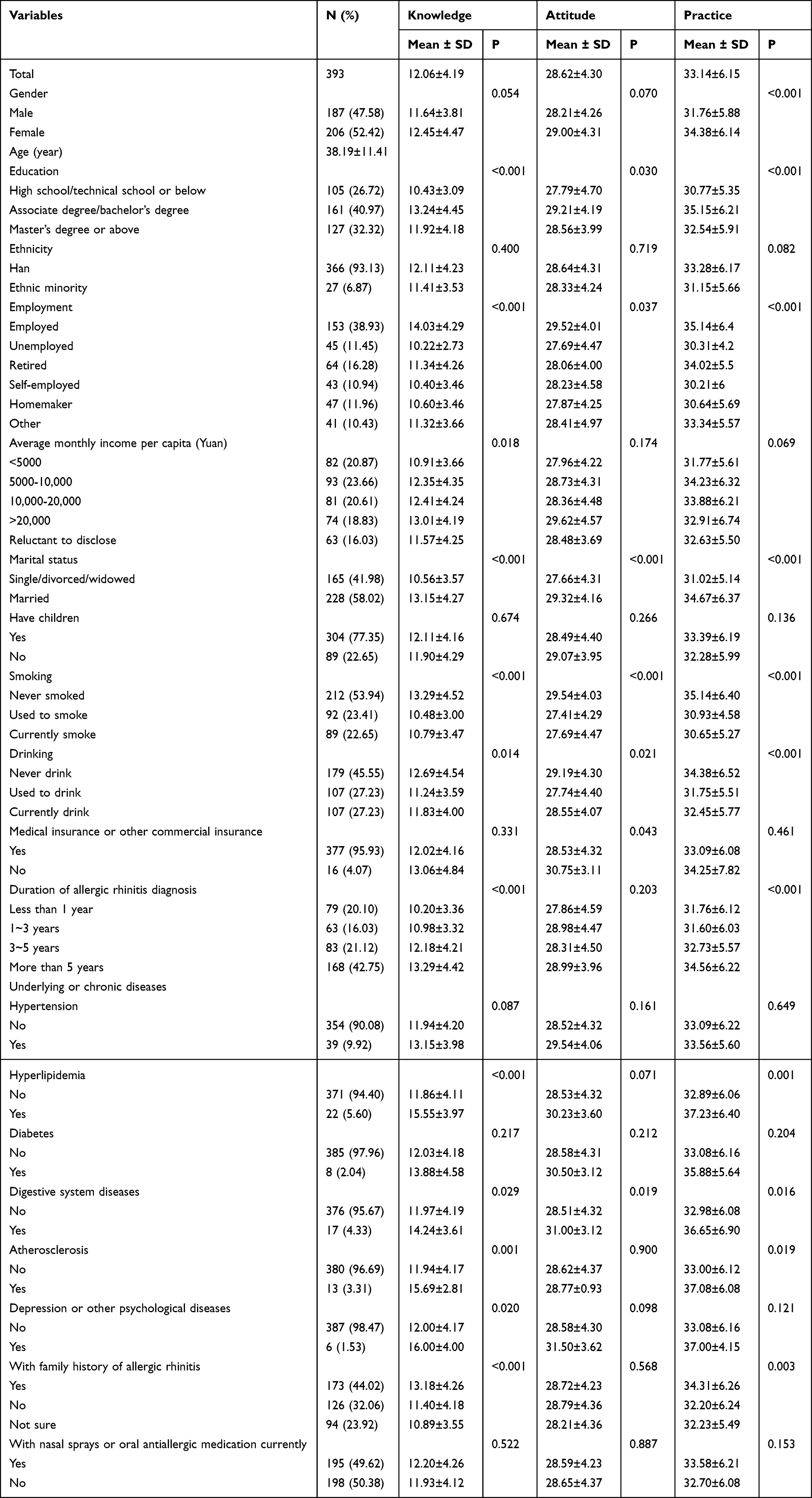 |
Table 1 Demographic Characteristics and KAP Scores |
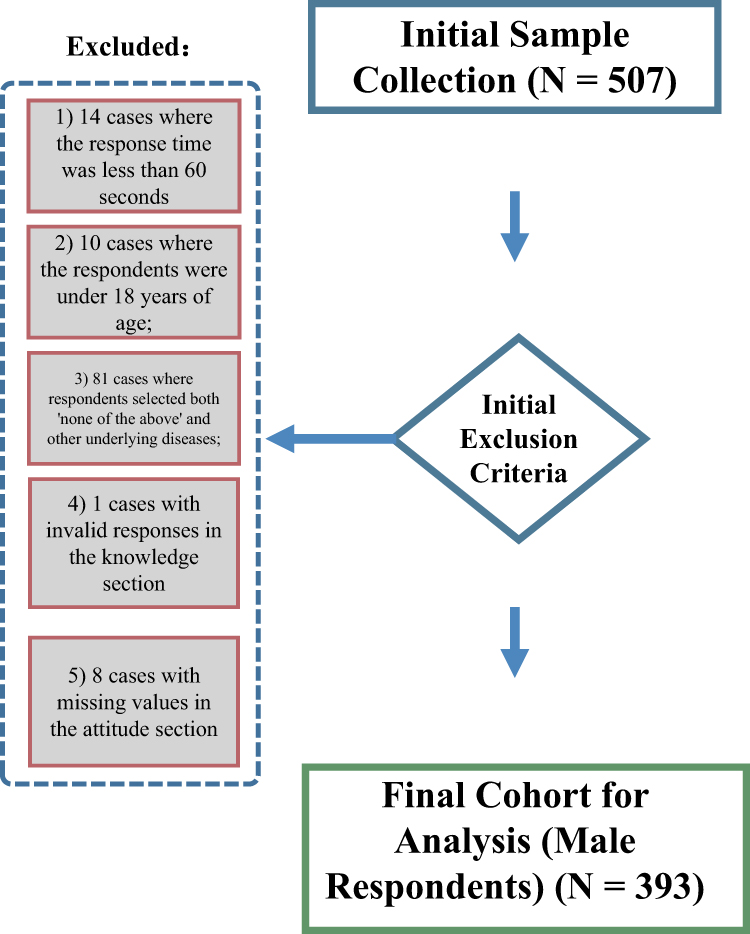 |
Figure 1 Study flowchart. |
Knowledge, Attitude, and Practice
The distribution of knowledge dimensions shown that the three questions with the highest number of participants choosing the “Unclear” option were “Common medications for AR include: antihistamines, glucocorticoids, decongestants, anticholinergics, mast cell stabilizers, etc”. (K7) with 26.97%, “AR cannot be completely cured and requires long-term treatment and chronic disease management”. (K10) with 26.72%, and “Drug treatment for AR is simple and effective; therefore, medication is the first choice for treating AR”. (K6) with 25.70% (Table S3 and Figure 2A). Responses to the attitude dimension showed that 50.89% strongly agreed or agreed that they felt anxious and helpless about the symptoms of AR (A2), and similarly 50.89% strongly agreed or agreed that recurrent episodes of AR made them feel anxious and irritable (A8). On the other hand, 33.84% disagreed or strongly disagreed that marriage with a person with AR would be passed on to their children (A9) (Table S4 and Figure 2B). Regarding related practices, 12.21% always avoid social occasions and public places due to AR (P1). However, 15.27% never go to the hospital for examination to find out the allergens (P2), 13.49% never pay attention to avoiding allergens (P3), and 13.99% were unable to maintain a positive and optimistic mindset (P8) (Table S5 and Figure 2C).
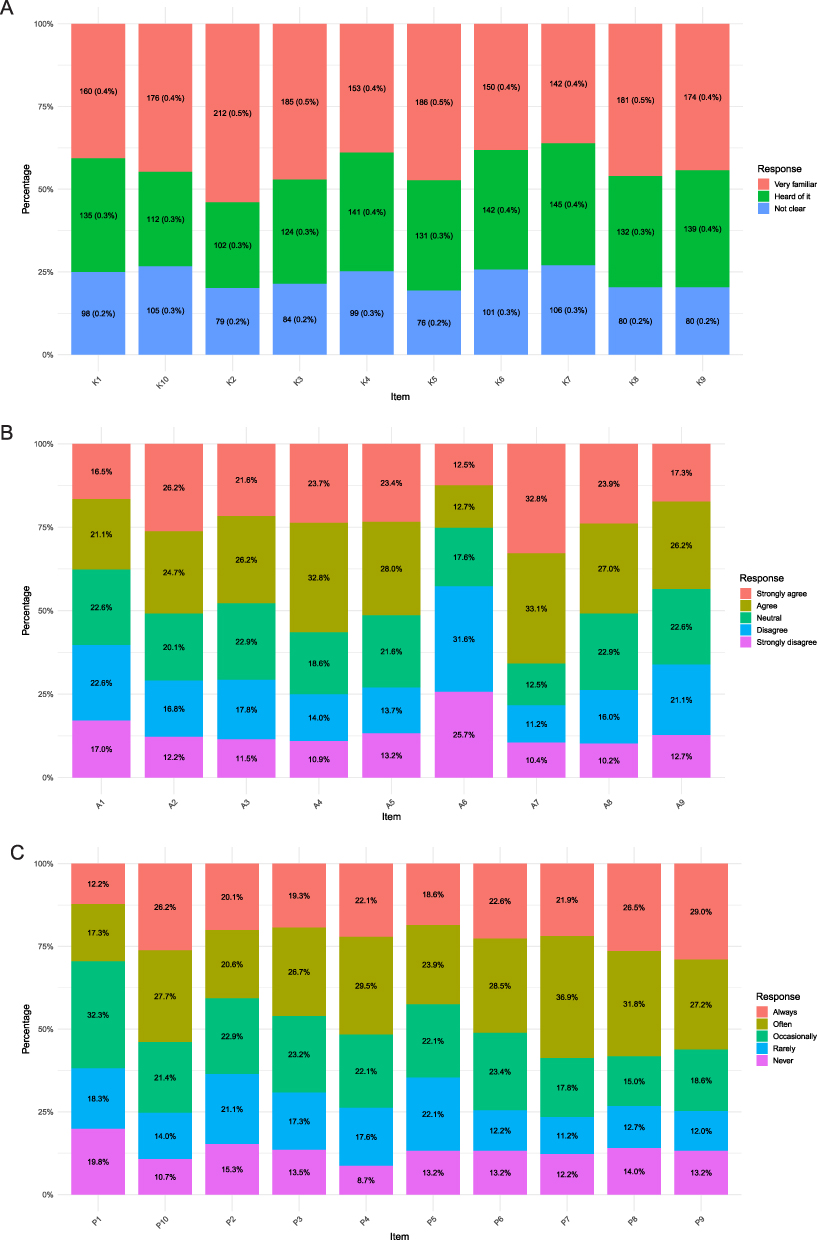 |
Figure 2 Knowledge (A), attitude (B), and practice (C) scores distribution. |
Correlations Between KAP
In the correlation analysis, significant positive correlations were found between knowledge and attitude (r = 0.277, P < 0.001), knowledge and practice (r = 0.527, P < 0.001), as well as attitude and practice (r = 0.283, P < 0.001), respectively (Table 2).
 |
Table 2 Correlation Analysis |
Interactions Between KAP
After adjustment, variables without statistical significance were removed based on the unadjusted model, the estimates for the model were shown in Table S6. In this cross-sectional path-analysis model, the reported direct and indirect effects represent statistical associations (potential pathways) rather than causal effects. The fitting index of the adjusted model (CMIN/DF = 1.961, RMSEA = 0.050; IFI = 0.946; TLI = 0.893; CFI = 0.943) outperformed the respective threshold value, signifying that the data satisfactorily fit the path-analysis model (Table S6), the specific effects of the factors on KAP were shown in Table S7. Specifically, in the adjusted path-analysis model, employment status was directly associated with knowledge (β = −0.389, P = 0.010) and was indirectly associated with attitude (β = −0.085, P = 0.008) and practice (β = −0.247, P = 0.009). Marital status was directly associated with knowledge (β = 1.401, P = 0.010), attitude (β = 0.844, P = 0.038), and practice (β = 1.382, P = 0.027), and was indirectly associated with attitude (β = 0.308, P = 0.006) and practice (β = 1.020, P = 0.015). Smoking habit was directly associated with knowledge (β = −0.858, P = 0.011), attitude (β = −0.627, P = 0.014), and practice (β = −1.071, P = 0.012), and was indirectly associated with attitude (β = −0.189, P = 0.007) and practice (β = −0.642, P = 0.008). Duration of AR was directly associated with knowledge (β = 0.701, P = 0.011) and was indirectly associated with attitude (β = 0.154, P = 0.006) and practice (β = 0.446, P = 0.006). Family history was directly associated with knowledge (β = −0.685, P = 0.008) and was indirectly associated with attitude (β = −0.151, P = 0.014) and practice (β = −0.436, P = 0.007). Furthermore, knowledge was directly associated with practice (β = 0.603, P = 0.034) (Table 3 and Figure 3).
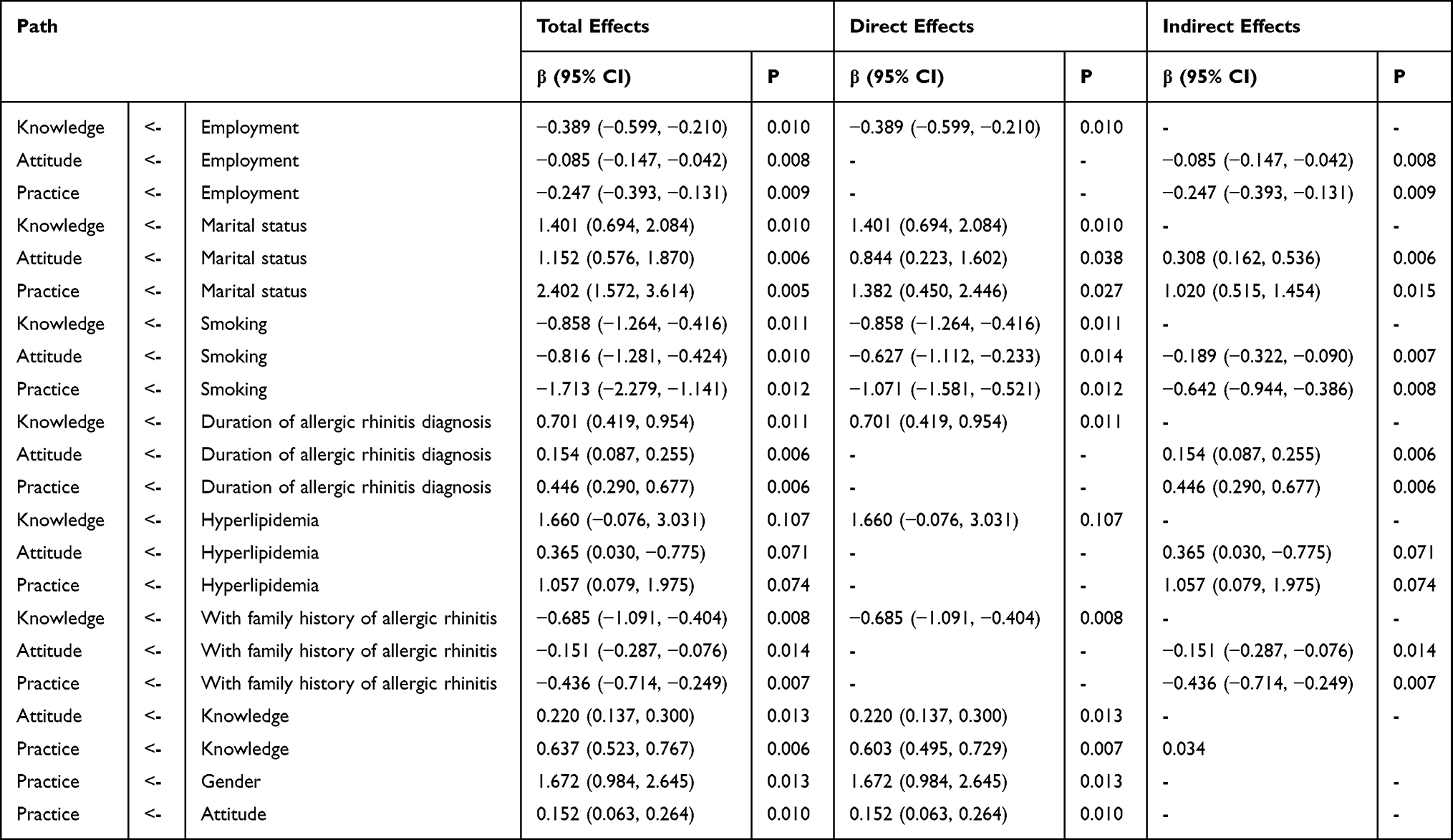 |
Table 3 Mediation Analysis Based on the Adjusted Path-Analysis Model |
 |
Figure 3 Path-analysis model diagram after adjustment. |
Discussion
Patients with AR exhibited insufficient knowledge and moderate attitudes and practices toward environmental control and treatment, indicating gaps in patient education. The findings of this study align with previous research that has reported similar deficiencies in KAP among patients with chronic conditions. For instance, one study indicated that patients with AR lack sufficient knowledge and have poor attitudes, though their behaviors were relatively better, underscoring the need for continuous, high-quality educational interventions.23 Additionally, another study focusing on allergen-specific immunotherapy (AIT) found that patients with AR had limited understanding, negative attitudes, and low motivation towards AIT.22 Such deficiencies in knowledge, particularly regarding environmental triggers and treatment options, may contribute to poor adherence to recommended practices, ultimately exacerbating symptoms and diminishing quality of life.
In terms of the relationships between KAP, the correlation analysis and SEM results both support the significant associations among knowledge, attitude, and practice. Both the correlation analysis and the path-analysis model showed consistent positive associations among knowledge, attitude, and practice. These findings align with existing literature that suggests higher knowledge levels are associated with more positive attitudes and better practices in managing chronic diseases.25,26 For instance, the significant positive impact of knowledge on practice is consistent with the idea that patients who are better informed about their condition are more likely to engage in effective management behaviors.27 The influence of attitude on practice further underscores the importance of fostering positive attitudes through educational programs. From a practical perspective, our findings support translating guideline-based environmental control into simple, allergen-targeted actions that patients can implement at home. For house dust mite exposure, clinicians can emphasize measures such as reducing indoor humidity, washing bedding regularly, and using allergen-impermeable covers for pillows and mattresses. For pollen-related symptoms, avoidance strategies can be framed around peak-season planning (eg, limiting outdoor exposure during high-count periods, changing clothes after outdoor activities, and keeping windows closed when pollen levels are high). For dampness and mold, counseling can focus on identifying and addressing moisture sources, improving ventilation, and promptly cleaning visible mold. For pet-related allergen exposure, patients can be advised to minimize close contact and reduce allergen reservoirs in living spaces. These practical messages can be delivered as brief, step-by-step checklists during routine visits and tailored to the patient’s likely triggers and resources. Taken together, our findings suggest a coherent behavioral pattern: knowledge is the most upstream and consistently linked component, with more favorable attitudes accompanying higher knowledge and better self-management practices. This supports an education-first strategy for AR environmental control and treatment, while also highlighting the need to tailor delivery for subgroups with lower KAP performance. In particular, the observed associations with employment status, marital status, smoking habits, and family history indicate that contextual and lifestyle factors may coincide with reduced knowledge and, through knowledge–attitude pathways, with less optimal practices. Therefore, interventions should prioritize clear, guideline-based messages on allergen avoidance and medication use and use subgroup-appropriate formats to improve uptake.
Regarding significant differences across demographic variables, the higher practice scores in females were consistent with the path-analysis results, in which gender was significantly associated with practice. This suggests that gender-specific factors may influence the way patients manage their condition, possibly due to differences in health-seeking behaviors or access to resources. Similarly, smoking habits were significantly associated with all three KAP dimensions in the path-analysis model, with lower scores observed among current and former smokers compared with non-smokers. These findings are in line with research showing that smoking is associated with poorer health outcomes and lower engagement in preventive practices.28
Interestingly, some variables showed significant differences in two dimensions but not in the third. For instance, marital status was significantly associated with knowledge and practice but not attitude.
The distribution of responses in the knowledge dimension reveals that a significant portion of patients with AR have only a basic understanding of key aspects related to their condition, with a notable percentage lacking clarity on essential topics such as common allergens and treatment methods. For instance, a considerable number of respondents were not clear about the role of foods as potential allergens, and many were uncertain about the effectiveness of drug treatment. These gaps in knowledge are concerning, as they can lead to poor disease management and increased symptom severity. To address these gaps, it is crucial to implement targeted educational programs that focus on enhancing patient awareness of specific allergens and effective treatment options. Providing patients with easily accessible information, perhaps through mobile health apps or educational workshops, could significantly improve their knowledge and, consequently, their ability to manage the disease. Additionally, tailored interventions should be developed for groups that demonstrated the most significant knowledge gaps, such as those with lower education levels or those who are unemployed, as indicated by the statistical differences observed in the study.29,30
The analysis of the attitude dimension reveals mixed perceptions among patients, with a considerable proportion expressing negative feelings such as anxiety, helplessness, and insecurity due to their condition. Many patients also seem to underestimate the seriousness of AR, which could lead to insufficient treatment adherence and poor health outcomes. To improve patient attitudes, it is essential to provide psychological support and counseling, helping patients develop a more positive outlook toward managing their condition. For example, incorporating mental health resources into routine care for AR patients could alleviate feelings of anxiety and helplessness. Additionally, creating patient support groups where individuals can share experiences and coping strategies might help reduce feelings of isolation and insecurity. Educational campaigns that emphasize the chronic nature of AR and the importance of active management can also help shift attitudes towards more proactive and engaged disease management.31–33
The responses in the practice dimension highlight several areas where patients’ behaviors fall short, particularly in aspects related to proactive management of AR. A significant number of patients reported rarely or never engaging in practices such as saline nasal irrigation, following medical advice consistently, or avoiding allergens. This lack of adherence to recommended practices is concerning and reflects the need for more robust patient education and support systems. To enhance adherence to recommended practices, healthcare providers should consider developing personalized action plans that include clear, step-by-step instructions tailored to individual patient needs. For instance, providing patients with visual guides or instructional videos on proper nasal irrigation techniques could increase the frequency of this practice.34,35 Moreover, implementing reminder systems, such as text message alerts or mobile app notifications, could help patients adhere to their medication schedules and follow-up appointments.36,37 Given the statistical differences observed in practice behaviors based on demographic factors, targeted interventions should be designed to support specific groups, such as younger patients or those with lower incomes, who may face additional challenges in managing their condition effectively.
This study has several limitations. First, the cross-sectional design limits the ability to establish causal relationships between the variables and to capture changes in KAP over time. Future longitudinal follow-up studies are warranted to track KAP changes over time and better clarify temporal relationships among the study variables. In addition, AR symptoms and allergen exposure can vary across seasons and across living environments, which may influence patients’ environmental-control behaviors and treatment choices over time. Future work could incorporate long-term temporal assessments (eg, repeated measurements across pollen and non-pollen seasons) and spatial assessments (eg, multi-center recruitment across different districts or regions, with basic characterization of local exposure patterns such as dampness/mold, indoor humidity, or seasonal pollen peaks) to better capture exposure variability and contextual factors related to KAP. Second, the use of self-reported questionnaires may introduce response bias, as participants might overestimate or underestimate their KAP levels. Third, the study was conducted at a single institution, which may limit the generalizability of the findings to broader populations. In addition, the use of convenience sampling may have introduced selection bias, further limiting the representativeness of the sample and the generalizability to community-dwelling patients and other regions. Future studies should consider multi-center designs across different regions and settings (eg, hospitals, communities, and primary care clinics) to reduce single-institution bias and improve generalizability. Additionally, broader participant coverage, including adolescents (12–17 years), older adults (>65 years), and rural populations, would help evaluate KAP patterns across age groups and living environments.
Conclusion
In conclusion, patients with AR exhibited insufficient knowledge and moderate attitudes and practices toward environmental control and treatment, indicating clear gaps in patient education. Our path-analysis model further suggests that KAP may vary across subgroups, with factors such as employment status, marital status, smoking habits, and family history showing significant associations with KAP. Importantly, the model suggests that some factors may be indirectly associated with practice through knowledge and attitude, highlighting knowledge as a potentially modifiable target for intervention. Accordingly, strengthening patients’ knowledge of guideline-based environmental control and treatment may help improve attitudes and, in turn, promote better practices, particularly in subgroups for whom knowledge is reduced by these contextual factors. Therefore, educational interventions should be tailored to the needs of these groups, for example by providing simplified and easy-to-understand materials for patients with lower educational attainment, strengthening counseling on allergen avoidance and medication use for smokers, and offering practical, step-by-step action plans for patients with limited resources or support. Future work should validate these findings in broader populations and evaluate whether targeted, subgroup-specific education can improve KAP and clinical management of AR over time.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of Beijing Tongren Hospital affiliated to Capital Medical University (TREC2024-KY085). The study was conducted in accordance with the Declaration of Helsinki. All participants were informed about the study protocol and provided written informed consent to participate in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
1. National Key R&D Program of China (2022YFC2504100) 2. High-level Public Health Talents Training Program of Beijing Municipal Health Commission, No. 02-046 3. The scarce resources and representative achievements of the Beijing Traditional Chinese Medicine Torch Inheritance Project, 2023-XQZY-02.
Disclosure
The authors declare that they have no competing interests.
References
1. Bousquet J, Onorato GL, Bachert C, et al. CHRODIS criteria applied to the MASK (MACVIA-ARIA Sentinel NetworK) good practice in allergic rhinitis: a SUNFRAIL report. Clin Transl Allergy. 2017;7(1):37. doi:10.1186/s13601-017-0173-8
2. Bousquet J, Schunemann HJ, Fonseca J, et al. MACVIA-ARIA Sentinel NetworK for allergic rhinitis (MASK-rhinitis): the new generation guideline implementation. Allergy. 2015;70(11):1372–13. doi:10.1111/all.12686
3. Tan R, Cvetkovski B, Kritikos V, et al. Identifying the hidden burden of allergic rhinitis (AR) in community pharmacy: a global phenomenon. Asthma Res Pract. 2017;3(1):8. doi:10.1186/s40733-017-0036-z
4. Cheng L, Chen J, Fu Q, et al. Chinese society of allergy guidelines for diagnosis and treatment of allergic rhinitis. Allergy Asthma Immunol Res. 2018;10(4):300–353. doi:10.4168/aair.2018.10.4.300
5. Bousquet J, Khaltaev N, Cruz AA, et al. Allergic rhinitis and its impact on asthma (ARIA) 2008 update (in collaboration with the world health organization, GA(2)LEN and AllerGen). Allergy. 2008;63 Suppl 86:8–160. doi:10.1111/j.1398-9995.2007.01620.x
6. Small P, Keith PK, Kim H. Allergic rhinitis. Allergy Asthma Clin Immunol. 2018;14(Suppl 2):51. doi:10.1186/s13223-018-0280-7
7. Wheatley LM, Togias A. Clinical practice. Allergic rhinitis. N Engl J Med. 2015;372(5):456–463. doi:10.1056/NEJMcp1412282
8. Ismail NFF, Neoh CF, Lim SM, et al. The immediate effect of facial candling on inflammatory mediators, substance P, symptoms severity, and quality of life in allergic rhinitis patients: study protocol for a randomized controlled trial. Medicine. 2017;96(30):e7511. doi:10.1097/MD.0000000000007511
9. Meltzer EO. Allergic rhinitis: burden of illness, quality of life, comorbidities, and control. Immunol Allergy Clin North Am. 2016;36(2):235–248. doi:10.1016/j.iac.2015.12.002
10. Bush RK. Indoor allergens, environmental avoidance, and allergic respiratory disease. Allergy Asthma Proc. 2008;29(6):575–579. doi:10.2500/aap.2008.29.3172
11. Platts-Mills TA. Allergen avoidance in the treatment of asthma and rhinitis. N Engl J Med. 2003;349(3):207–208. doi:10.1056/NEJMp030082
12. Zhong Z, Wang F, Wang T, Li L, Tan G. Aeroallergen spectrum of patients with child allergic rhinitis in Changsha area of China. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2011;25(17):774–776.
13. Li J, Sun B, Huang Y, et al. A multicentre study assessing the prevalence of sensitizations in patients with asthma and/or rhinitis in China. Allergy. 2009;64(7):1083–1092. doi:10.1111/j.1398-9995.2009.01967.x
14. Gao L, Su S, Du N, et al. Medical and non-medical students’ knowledge, attitude and willingness towards the COVID-19 vaccine in China: a cross-sectional online survey. Hum Vaccin Immunother. 2022;18(5):2073757. doi:10.1080/21645515.2022.2073757
15. Twinamasiko N, Olum R, Gwokyalya AM, Nakityo I, Wasswa E, Sserunjogi E. Assessing knowledge, attitudes and practices towards COVID-19 public health preventive measures among patients at mulago national referral hospital. Risk Manag Healthc Policy. 2021;14:221–230. doi:10.2147/RMHP.S287379
16. Wang J, Chen L, Yu M, He J. Impact of knowledge, attitude, and practice (KAP)-based rehabilitation education on the KAP of patients with intervertebral disc herniation. Ann Palliat Med. 2020;9(2):388–393. doi:10.21037/apm.2020.03.01
17. Chi YL, Mak HWL. From comparative and statistical assessments of liveability and health conditions of districts in Hong Kong towards future city development. Sustainability. 2021;13(16):8781. doi:10.3390/su13168781
18. Cheng C, Zhang W, Jin B, Yang S, Lu H, Ren Y. Knowledge, attitude, and practice (KAP) towards pulmonary nodules among Chinese adults: a mediation analysis. Sci Rep. 2024;14(1):28950. doi:10.1038/s41598-024-79657-9
19. Liang B, Wang B, Liang J, Sun X. Knowledge, attitude, and practice of healthcare professionals toward sarcopenia. Sci Rep. 2025;15(1):19826. doi:10.1038/s41598-025-04358-w
20. Wang J, Li B, Yu W, et al. Rhinitis symptoms and asthma among parents of preschool children in relation to the home environment in Chongqing, China. PLoS One. 2014;9(4):e94731. doi:10.1371/journal.pone.0094731
21. Beheshti R, Grant TL, Wood RA. Minimizing indoor allergen exposure: what works? Curr Allergy Asthma Rep. 2024;25(1):3. doi:10.1007/s11882-024-01185-3
22. Fan X, Zhang J. Knowledge, attitudes, and practices of patients with allergic rhinitis towards allergen-specific immunotherapy. Patient Prefer Adherence. 2024;18:1531–1545. doi:10.2147/PPA.S468957
23. Gu W, Yan D, Yuan Z, et al. Knowledge, attitudes, and practice towards allergic rhinitis in patients with allergic rhinitis: a cross-sectional study. BMC Public Health. 2023;23(1):1633. doi:10.1186/s12889-023-16607-6
24. Pourhoseingholi MA, Vahedi M, Rahimzadeh M. Sample size calculation in medical studies. Gastroenterol Hepatol Bed Bench. 2013;6(1):14–17.
25. Gatulytė I, Verdiņa V, Vārpiņa Z, Lublóy Á. Level of health literacy in Latvia and Lithuania: a population-based study. Arch Public Health. 2022;80(1):166. doi:10.1186/s13690-022-00886-3
26. Sasanfar B, Toorang F, Rostami S, et al. The effect of nutrition education for cancer prevention based on health belief model on nutrition knowledge, attitude, and practice of Iranian women. BMC Womens Health. 2022;22(1):213. doi:10.1186/s12905-022-01802-1
27. Wang S, Yan D, Hu X, Liu J, Liu D, Wang J. Comparison of attitudes toward the medical student-led community health education service to support chronic disease self-management among students, faculty and patients. BMC Med Educ. 2023;23(1):17. doi:10.1186/s12909-023-04008-7
28. Heckman CJ, Wackowski OA, Mukherjee R, et al. Cigarette relighting: a series of pilot studies investigating a common yet understudied smoking behavior. Int J Environ Res Public Health. 2021;18(12):6494. doi:10.3390/ijerph18126494
29. Iordache A, Boruga M, Mușat O, Jipa DA, Tătaru CP, Mușat GC. Relationship between allergic rhinitis and allergic conjunctivitis (allergic rhinoconjunctivitis) - review. Rom J Ophthalmol. 2022;66(1):8–12. doi:10.22336/rjo.2022.3
30. Siddiqui ZA, Walker A, Pirwani MM, Tahiri M, Syed I. Allergic rhinitis: diagnosis and management. Br J Hosp Med. 2022;83(2):1–9. doi:10.12968/hmed.2021.0570
31. Conway AE, Verdi M, Kartha N, et al. Allergic diseases and mental health. J Allergy Clin Immunol Pract. 2024;12(9):2298–2309. doi:10.1016/j.jaip.2024.05.049
32. Lee GN, Koo HYR, Han K, Lee YB. Analysis of quality of life and mental health in patients with atopic dermatitis, asthma and allergic rhinitis using a nation-wide database, KNHANES VII. Allergy Asthma Immunol Res. 2022;14(2):273–283. doi:10.4168/aair.2022.14.2.273
33. Rodrigues J, Pinto JV, Alexandre PL, et al. Allergic rhinitis seasonality, severity, and disease control influence anxiety and depression. Laryngoscope. 2023;133(6):1321–1327. doi:10.1002/lary.30318
34. Shin YH, Hwang J, Kwon R, et al. Global, regional, and national burden of allergic disorders and their risk factors in 204 countries and territories, from 1990 to 2019: a systematic analysis for the global burden of disease study 2019. Allergy. 2023;78(8):2232–2254. doi:10.1111/all.15807
35. Yang HJ. Action-plan and as-needed therapy in allergic rhinitis. Clin Exp Pediatr. 2024;67(6):267–273. doi:10.3345/cep.2023.00654
36. Bédard A, Basagaña X, Anto JM, et al. Treatment of allergic rhinitis during and outside the pollen season using mobile technology. A MASK study. Clin Transl Allergy. 2020;10(1):62. doi:10.1186/s13601-020-00342-x
37. Kvedarienė V, Biliute G, Didziokaitė G, et al. Mobile health app for monitoring allergic rhinitis and asthma in real life in Lithuanian MASK-air users. Clin Transl Allergy. 2022;12(9):e12192. doi:10.1002/clt2.12192
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge, Attitudes and Practices Towards Psoriasis Among Patients and Their Family Members
Zhang X, Du H, Liu X, Liu L, Zhang T
Clinical, Cosmetic and Investigational Dermatology 2024, 17:769-782
Published Date: 3 April 2024
Knowledge, Attitudes and Practices Toward Physical Literacy Among the College Students During COVID-19 School Closure
Ma C, Yue M, Zhu X
Journal of Multidisciplinary Healthcare 2024, 17:1629-1640
Published Date: 15 April 2024
Knowledge, Attitude and Practice of Radiologists Regarding Artificial Intelligence in Medical Imaging
Huang W, Li Y, Bao Z, Ye J, Xia W, Lv Y, Lu J, Wang C, Zhu X
Journal of Multidisciplinary Healthcare 2024, 17:3109-3119
Published Date: 4 July 2024
Knowledge, Attitude, and Practice Toward Varicocele in Patients with Varicoceles: A Cross-Sectional Study in Chinese Patients
Gong P, Shen J, Yang Y, Xue D, Lu H, Zhuang Q, Wang X, Tian Z, Chen Y, Chen C, Cao Y
International Journal of General Medicine 2024, 17:3423-3432
Published Date: 7 August 2024
Knowledge, Attitude, and Practice Towards Rehabilitation in Patients with Breast Cancer: A Cross-Sectional Study
Zhou Y, Lu Q, Yu X
Journal of Multidisciplinary Healthcare 2025, 18:1483-1492
Published Date: 12 March 2025