Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Knowledge, Attitudes, and Practice of General Practitioners Toward Screening of Age-Related Hearing Loss in Community: A Cross-Sectional Study in Shanghai, China
Authors Ge J, Li H ![]() , Ren G, Sun X, Jiang H
, Ren G, Sun X, Jiang H
Received 26 November 2023
Accepted for publication 23 January 2024
Published 7 February 2024 Volume 2024:17 Pages 557—571
DOI https://doi.org/10.2147/JMDH.S447040
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jianli Ge,1 Huazhang Li,2 Guangwei Ren,3 Xiaoming Sun,1,4 Hua Jiang1
1Department of General Practice, Shanghai East Hospital, Tongji University School of Medicine, Shanghai, 200120, People’s Republic of China; 2Department of Science and Education, Shanghai Guangming Traditional Chinese Medicine Hospital, Shanghai, 201399, People’s Republic of China; 3Department of Science and Education, Sanlin Community Health Service Center, Shanghai, 200124, People’s Republic of China; 4School of Public Health, Fudan University, Shanghai, 200032, People’s Republic of China
Correspondence: Hua Jiang; Xiaoming Sun, Department of General Practice, Shanghai East Hospital, Tongji University School of Medicine, Shanghai, 200120, People’s Republic of China, Email [email protected]; [email protected]
Background: Age-related hearing loss (ARHL) is experiencing a continuously rising in prevalence among the elderly worldwide. General practitioners (GPs) may have a unique position in its community detection and management.
Objective: This study aims to assess the KAP of GPs regarding ARHL through questionnaire, to investigate the role of them in the management and to propose strategies for the hearing screening within the community.
Methods: An online survey was administered to 1173 GPs, selected from 56 community health centers (CHCs) in Shanghai during April to June 2022. A scale endorsed by a panel of multidisciplinary experts was used to assess knowledge (7 items), attitudes (12 items), and practice (10 items). A mean score was computed and converted into a scale ranging from 0 to 100. Odds ratios (ORs) were calculated for potential predictors of higher levels of KAP scores (with mean value as a cutoff point) through logistic modelling.
Results: A total of 1022 GPs completed the questionnaire with response rate 87.13%. The average scores are 69.90 ± 32.27, 66.09 ± 7.15, and 59.89 ± 21.99 for Knowledge, attitude, and practice, respectively. 24.3% of participants achieve a complete score of knowledge, whereas 5.48% receive zero. 11.6% consider ARHL as not a disease. Above 30.0% are not familiar with the screening tool. 10.8% refuse to undergo hearing screening. Higher levels of compliance in practice are found in the participants with higher levels of knowledge (OR=1.409, p=0.000) and more favorable attitude (OR=1.028, p=0.000). Male (OR=0.708, p=0.036) is associated with lower levels of attitudes.
Conclusion: GPs have a low level of ARHL knowledge, a lack of positive attitude towards the detection and management of it, and lower awareness in practice. Further research is required to gain a more comprehensive understanding of the attitudes held by GPs and explore more accessibility strategies.
Keywords: age-related hearing loss, KAP, general practitioners
Background
The phenomenon of population aging has emerged as a significant demographic shift since the latter part of the twentieth century, presenting a formidable challenge for numerous nations. ARHL is a term used to describe the deterioration of auditory capabilities that occurs as a result of aging. It is considered the third most prevalent chronic condition among older adults, following hypertension and arthritis1–3, The 2nd WHO Cooperative Center for Deafness Prevention StrategicPlanConference unveiled findings indicating that mild instances of deafness among the elderly can impede their communication skills and hinder their ability to carry out basic daily activities. Furthermore, in more severe cases, it was observed that deafness may contribute to the development of psychological disorders such as depression.4–7 The incidence of Alzheimer’s disease in older adults with varying degrees of hearing loss, specifically mild, moderate, and severe, is found to be twice, three times, and five times greater, respectively, contrasted to older adults with normal hearing capacity. There is a possibility that it could potentially elevate the likelihood of mortality from any cause among the elderly population.2,3,8 ARHL is distinguished by bilateral symmetrical hearing impairment predominantly affecting high-frequency sounds, some of which may be accompanied by tinnitus. The capacity for early subjective sensory speech recognition can effectively facilitate daily communication, albeit with symptoms that are often subtle and easily overlooked. It is anticipated that implementing active early screening and intervention measures will decelerate this progression, diminish the prevalence of disability, and enhance the overall life quality.9–13
Hearing screening of newborns in primary health care centers has been carried out for more than 20 years and achieved satisfactory clinical outcomes, while the hearing screening of older adults is still in the primary stage.14–16 With the promotion and implementation of the graded diagnosis and treatment system, GPs have become the first people for various health problems of community residents. However, hearing screening and timely and appropriate referral for older adults have not been popularized or valued in primary care.17,18 Up to 85% of elderly patients reported that they did not receive further advice on hearing loss from GPs.19–21 In a cohort study in Australia, less than half of patients consulted by GPs received referral and further treatment for hearing loss.18 This situation may be caused by time constraints, a lack of adequate training in hearing screening and treatment, and the GPs’ need to pay attention to more urgent medical problems, etc.19–21
Despite the fact that blood pressure or total cholesterol levels are widely understood, respondents demonstrate a lesser comprehension of what constitutes “normal” hearing levels. The prevailing viewpoint among respondents is that there is a limited range of treatment options available for the management of hearing loss. There is a notable absence of recognition regarding the enduring health consequences that can arise from the failure to address untreated hearing impairment.22 Like chronic diseases such as hypertension and diabetes, the incidence rate of ARHL is high, the onset of it is related to various personal behavioral and disease factors, which is relatively irreversible and cannot self-heal. Although it cannot be implementing primary prevention accurately, it can be screened, intervened, and delayed. The management of ARHL can refer to the current management guidelines for NCDs. Relying on the primary health care, screening and management in community led by GPs is feasible and has significant advantages.
Currently, there exists a series of studies on the various screening techniques for ARHL23–26 as well as the health beliefs held by individuals with hearing loss.27,28 However, there is a dearth of evaluations pertaining to the knowledge, beliefs, and practices (KAP) of GPs in relation to ARHL. The study aims to assess the proficiency of GPs in Shanghai in terms of their knowledge, attitudes, and practices linked to the detection and management of ARHL. Additionally, the study also will explore the potential associations between these factors, with the ultimate goal of offering fundamental guidance for the implementation and enhancement the hearing loss screening of the elderly population within the community.
Materials and Methods
Study Participants
Shanghai comprised a total of 16 districts and 251 community health centers (CHCs), among which Pudong emerged as the largest district, boasting a CHC count that was twice the average of the remaining districts. The research employed a stratified cluster sampling technique in order to recruit participants, ensuring proportional representation based on the distribution of areas. Specifically, six CHCs were randomly chosen from the Pudong district, while three CHCs were chosen from the remaining districts. There was a total of 51 CHCs, with approximately 1173 GPs being recruited.
Study Instruments
The questionnaire was developed through the literature review about ARHL detection and management in GPs,2–10,15–26,29,30 and the related books (Hearing Rehabilitation of the Elderly31 and Basic and Clinical Audiology32). The adaptation of the intervention to the Chinese context was achieved by conducting focus group interviews with a total of 15 individuals diagnosed with ARHL and 20 caregivers, as well as 20 GPs and 15 CHC managers in Shanghai. Subsequently, a series of two Delphi consultations were conducted, involving a panel of 22 experts who possessed expertise in general practice, ENT or health system and services management. The efficacy of KAP measurement was ensured by adhering to the four criteria proposed by Collier and Bienstock:33 content specification, indicator specification, indicator collinearity, and external effectiveness. The study employed a comprehensive literature review and conducted focus group interviews in order to maintain the integrity of pertinent content. The Delphi consultation facilitated the establishment of clear indicators.
Ten questionnaires were pretested in two CHCs, respectively, and the problems found were revised and adjusted in time.
The questionnaire was comprised of four sections and contained 39 items:1) General information of participants; 2) Knowledge of GPs toward ARHL detection and management; 3) Attitudes of GPs toward ARHL detection and management; 4) Practice of GPs toward ARHL detection and management (Additional File 1).
General information of participants contained as follows: gender, age, marital status, educational level, professional title, years of GPs experience, a unit of work, daily patient visits, the proportion of patients with self-reported hearing loss, ARHL detection and management experience or training.
The assessment of knowledge pertaining to ARHL was conducted using a set of seven question items. These items encompassed various aspects of ARHL, including its prevalence, risk factors, diagnostic criteria, classification, associated hazards, screening tools, and intervention measures. One possible option is to include the term “uncertain” in order to discourage individuals from making guesses. Each correct answer was assigned a score of 1, while incorrect answers were assigned a score of 0. The aggregate score was computed and converted into a scoring framework that spans from 0 (indicating the lowest level of knowledge) to 100 (representing the highest level of knowledge). In addition, the participants were requested to assess their level of knowledge in ARHL using a visual analog scale, which spanned from 0 to 100.
The attitudes of individuals with ARHL were assessed using a set of 12 items. These items encompassed various aspects, such as the perceptions of GPs regarding the nature of the condition (including susceptibility, severity, and benefits of interventions), the potential societal responses and burdens associated with ARHL, as well as the necessary actions to be taken by healthcare providers. The participants were asked to rate each item using a five-point Likert scale, with options ranging from 1, indicating “strongly disagree”, to 5, indicating “strongly agree”. The total score was computed and converted into a scoring system that spans from 0 (indicating the least favorable attitude towards ARHL management) to 100 (indicating the most favorable attitude towards ARHL management).
The assessment of ARHL was conducted across three distinct domains, namely alerting, confirming, and managing. The domain dedicated to alerting included two questions that inquired about respondents’ inclination to receive notifications for initiating ARHL screening by tinnitus and difficulty in listening under noise, respectively, for suspected cases. These symptoms were common early complaints in ARHL patients.2–10,15–29 The participants were instructed to evaluate each item utilizing a five-point Likert scale, where the response options spanned from 1 (“never / not applicable”) to 5 (“always”). The total score for the alerting domain was computed and subsequently converted into a scoring system that spans from 0 (indicating low alertness) to 100 (indicating high alertness). The domain of confirmation encompassed three components that addressed the evaluation of risk factors, the process of screening, and the referral of patients to specialists for diagnostic purposes. The participants were asked to rate each item using a five-point Likert scale, with response options ranging from 1 (“never/not applicable”) to 5 (“always”). The cumulative score was computed for the confirming domain and converted into a scoring framework that spans from 0 (indicating low compliance) to 100 (indicating high compliance). The managerial domain encompassed four components pertaining to patient and family communication, service coordination, and non-pharmacological interventions. The participants were asked to rate each item using a five-point Likert scale, with response options ranging from 1 (“never/not applicable”) to 5 (“always”). The managing domain was evaluated by computing a summed score, which was subsequently converted into a scoring system that spans from 0 (indicating low compliance) to 100 (indicating high compliance). The researchers computed the mean score of the three practice domains, where a higher score denoted greater adherence to the pertinent clinical guidelines.
The covariates assessed in this study encompassed sociodemographic attributes and the professional background of the participants. The sociodemographic characteristics measured were gender (female, male), age (< 30, 30–39,40–49, ≥ 50), marital status (married, unmarried, other), educational level (below bachelor, bachelor, postgraduate), professional title (primary, middle, associate senior, senior), years of general practice experience (< 5, 5–9, 10–14, ≥15), unit of working (urban of Pudong district, suburb of Pudong district, urban of Puxi district, suburb of Pudong district). Work experience measured included the volume of daily visiting patients (< 50, 50–69, 70–89, 90–109, ≥ 110), the proportion of patients with self-reported hearing loss over the past month (0, < 10%, 10–29%, ≥ 30%, unsure) and past experience or training in ARHL detection and management (yes, no).
Data Collection
The survey was conducted through the Sojump platform, and an email was sent before the survey, accompanied by a consent form explaining the research purpose and procedures, for respondents to read the survey before deciding to continue. The average survey time was about 10 minutes.
Statistical Analysis
The data input process was conducted using EpiData 3.0, while statistical analysis was performed using SPSS 25.0 software. In the context of measurement data, the normal distribution was represented as x ± s, whereas the abnormal distribution was represented as M (P25, P75). The classified information was represented using measures of frequency and rate. The application of an independent-sample t-test is appropriate when comparing only two groups, while comparisons among multiple groups are analyzed using a two-way ANOVA. T-test was used for independent samples of normal distribution data, and analysis of variance was used for diversity samples of normal distribution data. Correlation analysis and logistic regression analysis were employed to examine the factors that are linked to each other. P < 0.05 indicates that the observed difference is statistically significant.
Results
Sociodemographic Characteristics of Participants
The survey includes a cohort of 1173 participants, with 48 individuals declining to participate and 103 individuals withdrawing from the study prior to its completion. The data analyses were conducted using a final sample size of 1022, which accounts for approximately 11.6% of the total number of GPs in Shanghai.34 Among participants, the majority are female (69.4%); average age (37.5 ± 8.1 years old), of whom 70.6% are 30–49 years old; 86.7% have bachelor’s degrees and 12.6% have graduate degrees; 11.1% of individuals possess a working experience of 15 or more years, in contrast to 31.1% who have accumulated 10–14 years of experience, 29.4% with 5–9 years of experience, and 28.5% with less than five years of experience. Over two-thirds (77.6%) have a midcareer and above professional title. Less than 50% of participants saw more than 90 patients per day on average; the majority of them (91.9%) are uncertain about the status of self-reported hearing loss patients in the past month, and only 1.6% have ARHL detection and management experience (Table 1).
 |
Table 1 Characteristics of GPs Enrolled in the Study (n = 1022) |
Test-Retest Reliability
In this study, 42 respondents are reinvestigated repeatedly, with an interval of 7 days. The two measurement scores are evaluated by Pearson correlation analysis. The correlation coefficient of the retest reliability of the total questionnaire is 0.863. The correlation coefficient of retest reliability of three dimensions is between 0.815–0.845, indicating that the questionnaire results have good stability and consistency.
Knowledge of GPs Toward ARHL Screening and Management
The participants obtained a score of knowledge toward ARHL screening and management of 69.90 (SD = 32.27). A total of 24.3% of the participants were able to attain a complete knowledge score, while only 5.48% of the participants obtained a score of zero. A relatively greater level of knowledge is reflected in the question (hazards and treatment of ARHL); however, the other questions are all of lower levels. The understanding of participants on the characteristics, risk factors, and screening tool of ARHL is relatively poor, with 70.3%-76.5% of participants providing the correct answer. Less than 65% of participants understand the classification criteria for hearing loss (Table 2). The self-rated scale ARHL knowledge is also a tip on the same low level: the mean value of 61.63 (SD = 31.26) out of a maximum of 100.
 |
Table 2 KAP of GPs Toward ARHL Screening and Management (n = 1022) |
The Attitude of GPs Toward ARHL Screening and Management
The participants have an average score of attitudes is 66.09 (SD = 7.15). A significant proportion of respondents (65.9%) expressed agreement or strong agreement with the statement that ”All older adults suspected of ARHL should undergo a diagnostic evaluation” There are more advantages than disadvantages to screening if someone has ARHL” (65.4%), ”Early recognition and management can reduce the harm caused by ARHL” (57.5%), ”The management of patients with ARHL presents a greater number of advantages compared to disadvantages” (58.5%).
There are 67.2% of participants consider ARHL as a disease; however, 11.6% of participants still consider ARHL as a degenerative aging process. About 47.8% and 65.3% of participants held a neutral attitude towards The presence of ARHL among older individuals may impose a burden on both medical and social resources; the revelation of ARHL has the potential to induce feelings of stress and frustration among individuals and their families, respectively. About 68.4–75.3% of participants agree or strongly agree that it is GPs’ duty to recognize and manage ARHL in the CHCs. However, less than 35.8% believe that detection and management would provide economic benefits. Only 33.9% agree or strongly agree with Treating patients with ARHL through the use of hearing aids and cochlear implants offers a greater number of benefits compared to drawbacks, meanwhile, 58.6% hold a neutral attitude (Table 2).
The Practice of GPs Toward ARHL Screening and Management
On average, the participants have a practice score of 69.36 (SD = 13.25). Less than half of the participants are likely to be alerted by the existence of tinnitus (40.7%) or difficulty in listening in a noisy environment (49.7%) for suspected ARHL cases.
Meanwhile, less than half of the participants would always or usually gather the family history of hearing loss disease (32.1%) and detect the risk factors of ARHL (36.4%). Less than one-fifth of participants would always or usually perform ARHL screening (16.9%) but prefer to refer suspected ARHL patients to specialists (46.7%). About 10.8% of respondents would never or seldom conduct ARHL screening. Approximately 53% of the participants indicated a tendency to consistently or frequently engage in conversations regarding ARHL diagnosis with their family members, in contrast to 45.1% who reported similar discussions with the patients themselves. More than half of the participants would usually or always take coordinate support services (57.8%) and non-pharmacological measures (49.9%) (Table 3).
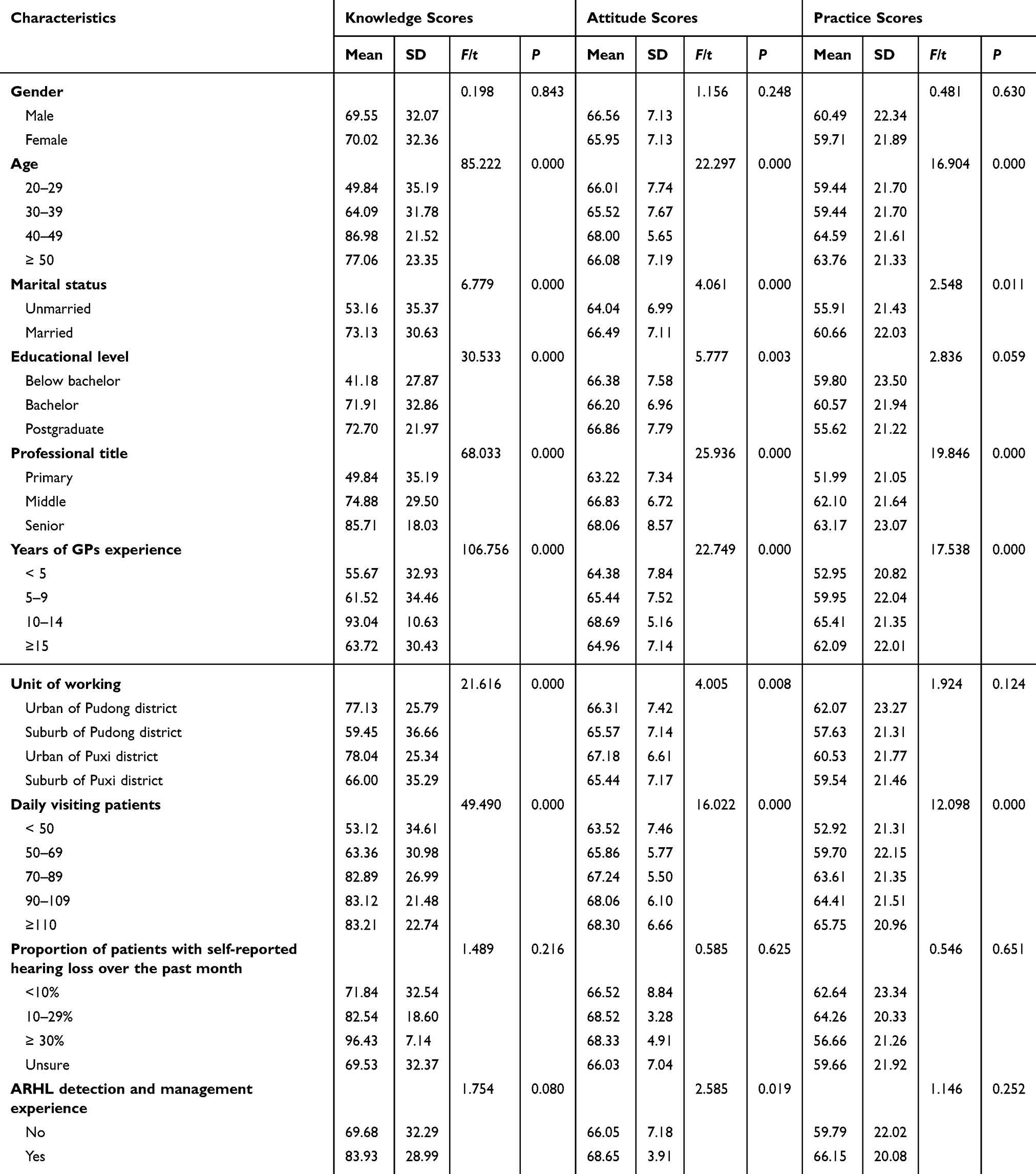 |
Table 3 ARHL KAP Scores by Sociodemographic Characteristics of Participants |
Sociodemographic Characteristics Connected to KAP (Knowledge, Attitude, and Practice)
Age is linked to knowledge (P=0.001), attitudes (P =0.001), and practice (P =0.013) scores, and all of them are in a linear manner. Greater knowledge scores, lower attitudes, and practice scores are observed in the female participants, but the difference is not statistically significant. Higher KAP scores are also found in those who are married (P =0.000, 0.000, 0.011). Postgraduates among the participants are associated with higher knowledge (P =0.000), attitudes (P =0.003), and practice (P =0.059) scores compared to bachelor or below bachelor. Similarly, higher professional titles are associated with greater knowledge scores (P =0.000), attitude scores (P =0.000), and practice scores (P =0.000). The participants who have 10–14 years of GP experience have greater KAP scores (P <0.001). Those who worked in the urban districts had greater knowledge scores (P =0.000) and greater attitude scores (P =0.008). The more daily visiting patients the participants have, the higher KAP scores they get (all P =0.000). The participants who experienced ARHL detection and management would get higher KAP scores but differences with no statistical significance.
The multivariate logistic regression model confirms that male (OR=0.708, P =0.036) is linked to reduced levels of attitudes. Being married is linked to levels of practice (OR=1.549, P =0.057). Educational level (Bachelor) is linked to greater levels of knowledge (OR=1.106, P =0.000); the same trend can be seen among postgraduates with higher levels of KAP, but there is no difference in statistics. (Table 4).
 |
Table 4 Logistic Regression Results of Predictors of ARHL KAP Scores |
Working in an urban unit is a significant predictor of higher levels of knowledge (OR=−1.277, P =0.000), more positive attitudes (OR=1.703, P =0.014), and higher compliance in practice (OR=1.053, P =0.037).
The model also shows that higher levels of attitude scores are observed in the participants with greater knowledge (OR=2.305, P =0.000). Greater compliance levels in practice are observed in the participants with greater knowledge levels (OR=1.409, P =0.000) and more favorable attitudes (OR=1.028, P =0.000) (Table 4).
Discussion
The study included 1022 GPs, who cover different ages, years of work, educational backgrounds, and position titles, making the study participants representative. The finding shows that scores (Mean ± SD) of knowledge, attitudes, and practice were all less than 70. GPs possess a reduced ARHL knowledge level, a lack of a positive attitude towards the detection and management, and lower awareness in practice. Thus, the KAP towards ARHL of GPs in Shanghai is worrying.
With the rising in the incidence rate, ARHL has been a worldwide concern. But, poor knowledge of ARHL among GPs is a problem. From the study data, it could be seen that only 24.3% of participants achieved a full knowledge score, while 5.48% obtained a zero score. Only 70% know the classification criteria for ARHL, and 71.8% know the characteristics of ARHL. Above 30.0% are not familiar with the screening tools for ARHL. The cross-sectional survey of Australian GPs from Schneider JM et al also shows that GPs have opportunities to identify hearing loss, but they have low knowledge of ARHL management18. An international study of staff of long-term-care (including GPs) in six countries, England, South Korea, India, Greece, Indonesia, and Australia, reveal that most healthcare professionals are aware that their dementia patients have hearing impairments and need screening tests. Nevertheless, their understanding of conducting screening tests and interpreting the outcomes is limited.35,36 Meanwhile, a majority of participants express a lack of confidence in their ability to assist residents with the utilization of assistive hearing aids. This lack of confidence primarily stems from a perceived deficiency in training.35,36 In our study, there are similar conclusions as well, only 1.6% have ARHL detection and management experience or training. Therefore, health authorities need to develop relevant continuing medical education and link training effectiveness to performance.
Depending on the outcomes of the study, it is observed that GPs in Shanghai do not exhibit explicitly positive attitudes toward the detection and management of ARHL. The average attitudes score is only 66.09 ± 7.15. 11.6% of the study participants do not consider ARHL as a disease, but over one-fifth (20.7%) of the study participants hold a neutral position. The investigation into the attitudes of Australian GPs regarding the discussion of hearing-related matters revealed a lack of comprehensive understanding regarding the implications of hearing loss and the advantages of hearing technology. Additionally, it was observed that these practitioners occasionally made assumptions that older individuals would not prioritize addressing their hearing concerns.21,37 Similar findings in the USA indicated that most GPs were unaware of how to or when to detect hearing loss.37,38 Our study also shows that whether suspect ARHL should undergo detection, 26.6% still hold a neutral attitude. There is a positive sign, though, that more than 68% of participants endorse their function in ARHL recognition and management, contrasted with < 6% clearly objecting to the study.
However, there is still some confusion and barriers for GPs to fulfill the role. Data from our study shows that 33.5% −58.6% hold a neutral attitude towards the opinion of“ more benefits than drawbacks to manage and treat ARHL.”A partial proportion of GPs worry about disclosure of ARHL diagnosis to patients and families (17.7%) or thought disclosure of ARHL diagnosis to patients and families would cause stress and frustration (25.3%). The National Academies of Science consensus paper confirmed the importance of identifying and treating hearing loss,39 though 60.2% of the participants are skeptical about the economic benefits of ARHL detection.
From the study, we find that there exists a correlation between lower levels of ARHL knowledge and the presence of unfavorable attitudes, which aligns with previous research conducted by Dawes et al36 In KAP theory, if the prevalence and severity of ARHL are underestimated, it might weaken the GPs’ understanding and recognition of the importance of detection and management of ARH. A lack of knowledge and confidence in ARHL detection and management might lead to a pessimistic attitude among GPs. Doubting the effectiveness of ARHL detection and management, as well as the uncertainty of benefits, could exacerbate the hesitation of GPs towards ARHL detection and diagnosis.
Dawes P et al36 found that only staff experience and having received training were associated with capacity. Our investigation shows that higher education level and professional title, longer general practitioner experience, urban working, and more daily visiting patients were linked to more favorable attitudes toward ARHL detection and management, which may be related to more residents’ medical needs and more opportunities for continuing education. Participants with experience in ARHL detection and management would get higher KAP scores but differences with no statistical significance. This might be a bias caused by an imbalanced sample size.
The self-reported practice intentions of GPs regarding community detection and management of ARHL reveal a notable lack of compliance with recommended practices. Only 40.7% of participants would take tinnitus as the criteria for ARHL detection, and only 49.7% of them would take difficulty in listening in a noise environment as the criteria in our study.
This finding is similar to those studies in the USA. A patient could only become part of a community ARHL management program when they received confirmation of ARHL diagnosis following the screening. But in their consultations, GPs usually do not doubt or consider this to be important.40,41.
Unfortunately, our study finds that only 16.9% of the participants would utilize the screening methods, while 10.8% would never or seldom perform the screening. Meanwhile, less than 40% of the participants would gather a family history of hearing loss (32.1%) and detect risk factors (36.4%) of ARHL.
Previous studies also suggested that 75% of cases of hearing loss are not adequately diagnosed or treated. The implementation of widely used screening methods has demonstrated efficacy in accurately identifying individuals with hearing loss, but they were rarely used.40–42 Although some studies called on GPs to pay more attention to improving the detection rate and intervention rate of hearing loss,43,44 there seemed to be no practical management plan. In the medical consultation of GPs, an average of 1.5 health problems needed to be handled 43.44. They lacked time and needed to prioritize more urgent health conditions. Because hearing loss is invisible, patients usually do not ask the GPs about hearing problems spontaneously, so it is not surprising that the GPs will detect patients’ hearing loss irregularly.
From the “Knowledge, attitude, practice” theory, it is the most difficult and a challenging stage to change from believing in the knowledge to acting; the failure of transformation is often an important factor leading to the poor effect of chronic disease prevention and control.45,46 Our study shows similar results, indicating that participants with greater knowledge exhibited higher levels of attitude scores. Additionally, participants with more favorable attitudes demonstrated higher levels of compliance in practice. Therefore, strengthening the homogenization training and learning of GPs in otorhinolaryngology expertise and using various ways to improve the construction of GPs’ talent team are the premise and key ways to improve the ability of GPs to actively participate in hearing loss screening.
Conclusion
ARHL was described as an imperceptible disability. Many adults have lived for years or even decades under the psychosocial influence of uncontrollable hearing loss.47 Hearing screening for the older adults can improve the detection rate of hearing loss and increase the proportion of receiving hearing loss compensation treatment (including hearing aids).17,48 In light of the demographic shift towards an aging population in Shanghai and the rising prevalence of ARHL, our study reveals that GPs in Shanghai are inadequately equipped to assume the responsibilities associated with this condition. In general, their level of knowledge in ARHL is relatively limited. There is a noticeable absence of clearly positive attitudes towards the detection and management of ARHL.
While continuous medical education can play an important role in the development of ARHL detecting and management in community, training by itself is not enough. Training alone does not foster positive attitudes that mediate the association between knowledge and practice.
Future research endeavors should take into account the utilization of more sophisticated approaches, such as the implementation of electronic health record (EHR) systems. These systems have the capability to notify healthcare professionals to conduct screenings for ARHL in individuals aged 55 years or older using a validated single-question screener.17,49 Such as the Chronic Care Model,50 ARHL can be reference to the management model of chronic diseases, requires a systems approach involving the patients, care providers, and a platform that enables effective interactions between the two. The major purpose of such a team-based partnership approach is to improve the quality (continuity and coordination) of care, but it may also bring benefits to the patients in resource-poor settings through its “offset effect” on the demand of the already scarce infrastructure and qualified medical workforce.51
Strengths and Limitations
This research endeavor represents the inaugural attempt to examine the KAP of GPs in Shanghai regarding the testing and management of ARHL within the community setting.
Although it follows strict research protocol design and tool development, there are still some limitations.
Firstly, the collection of data was conducted through the utilization of a self-report questionnaire, a method that has the potential to introduce recall bias and reporting errors.
Secondly, there is a higher proportion of females with a bachelor’s degree or above participants. This demographic composition may lead to an overestimation of the knowledge level among GPs even though the overall knowledge level regarding ARHL in this sample is already considered to be low.
Third, Shanghai is widely recognized as one of the most advanced and prosperous regions within the China. It is imperative to exercise caution when attempting to extrapolate the findings to other regions within China. There is a recommendation to augment the number of participants hailing from diverse geographical regions and varying socio-cultural backgrounds.
Finally, it is important to note that training alone does not cultivate favorable attitudes that serve as mediators of the links between knowledge and practice. Further researches are required to gain a more comprehensive understanding of the attitudes held by GPs and its influencing factors in Shanghai. Relevant management policies need to be proposed by the health authority and explore more accessibility, executable and homogeneous screening management approach.
Abbreviations
ARHL, Age-related hearing loss; GPs, general practitioners; CHCs, community health centers.
Data Sharing Statement
The entirety of the data produced or examined throughout this research endeavor has been incorporated within this published scholarly article, along with its accompanying Supplementary Information. Consensus among all authors is reached regarding the practice of sharing data.
Consent for Publication
All participants provided written informed consent for the publication of their data.
Ethical Considerations
The research obtained ethical approval and ensured that participants offered informed consent before their participation. Before the initiation of the current investigation, the requisite ethical clearance was obtained from the Academic Ethics Committee of Shanghai East hospital, specifically identified as {No. [2021] (094)}. It is important to note that the current study does not encompass any ethical concerns.
The execution of my submission adhered to the principles outlined in the Declaration of Helsinki.
Acknowledgment
The authors express thanks to Professor Jirong Duan from Hearing Clinic, Punan Hospital, Shanghai.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Supported by the National Key Research and Development Program of China (No. 2022YFC3601504); Pudong New Area Health Commission Discipline Leader Training Program Project (No. PWRd2020-12); Scientific research project of Shanghai Health and Family Planning Commission (No.201940235); and Shanghai Municipal Health Commission (No. 202140248).
Disclosure
The authors have no competing interests in this work.
References
1. Chadha S, Cieza A. World health organization, and its initiative for ear and hearing care. Otolaryngol Clin North Am. 2018;51(3):535–542. doi:10.1016/j.otc.2018.01.002
2. De Sousa KC, Smits C, Moore DR, Chada S, Myburgh H, Swanepoel W. Global use, and outcomes of the hear WHO mHealth hearing test. Digit Health. 2022;8:20552076221113204. doi:10.1177/20552076221113204
3. Kim G, Na W, Kim G, Han W, Kim J. The development and standardization ofSelf-assessment for Hearing Screening of the Elderly. Clin Interv Aging. 2016; 11:787–795. doi: 10.2147/CIA.S107102
4. Brewster KK, Hu M-C, Wall MM, et al., Age-related hearing loss, neuropsychological performance, and incident dementia in older adults. J Alzheimers Dis. 2021; 80(2):855–864doi:10.3233/JAD-200908
5. Golub JS, Luchsinger JA, Manly JJ, Stern Y, Mayeux R, Schupf N. Observed hearing loss and incident dementia in a multiethnic cohort. J Am Geriatr Soc. 2017;65(8):1691–1697. doi:10.1111/jgs.14848
6. Jayakody Dona MP, Almeida OP, Speelman CP, et al. Association between speech and high-frequency hearing loss and depression, anxiety and stress in older adults. Maturitas. 2018;110:86–91. doi:10.1016/j.maturitas.2018.02.002
7. Zazove P, Plegue MA, Mulhem E, et al. The association of hearing loss with hospitalization. J Am Board Fam Med. 2023;36(3):439–448. doi:10.3122/jabfm.2022.220407R1
8. Huang AR, Jiang K, Lin FR, Deal JA, Reed NS. Hearing loss and dementia prevalence in older adults in the US. JAMA. 2023;329(2):171–173. doi:10.1001/jama.2022.20954
9. Patel R, McKinnon BJ. Hearing loss in the elderly. Clinics in Geriatric Medicine. 2018;34(2):163–174[J]. doi:10.1016/j.cger.2018.01.001
10. Nieman CL, Oh ES. Hearing Loss. Ann Intern Med. 2020;173(11):ITC81–ITC96. doi:10.7326/AITC202012010
11. Cosh S, Helmer C, Delcourt C, Robins TG, Tully PJ. Depression in elderly patients with hearing loss: current perspectives. Clin Interv Aging. 2019;14:1471–1480. doi:10.2147/CIA.S195824
12. Lin FR, Pike JR, Albert MS, et al. Hearing intervention versus health education control to reduce cognitive decline in older adults with hearing loss in the USA (ACHIEVE): a multicentre, randomised controlled trial. Lancet. 2023;402(10404):786–797. doi:10.1016/S0140-6736(23)01406-X
13. Hackenberg B, Döge J, Lackner KJ, et al. Hearing loss and its burden of disease in a large German cohort-hearing loss in Germany. Laryngoscope. 2022;132(9):1843–1849. doi:10.1002/lary.29980
14. Deng XS, Ji F, Yang SM. Correlation between maximum phonetically balanced word recognition score and pure-tone auditory threshold in elder age-related hearing loss patients Over 80 years old [J]. Acta Otolaryngol. 2014;134(2):168–172. doi:10.3109/00016489
15. Tomioka K, Ikeda H, Hanaie K, et al. The hearing handicap inventory for elderly-screening (HHIE-S) versus a single question: reliability, validity, and relations with quality-of-life measures in the elderly community, Japan[J]. Qual Life Res. 2013;22(5):1151–1159. doi:10.1007/s11136-012-0235-2
16. Labanca L, Guimarães FS, Costa-Guarisco LP, Couto EAB, Gonçalves DU. Screening of hearing in elderly people: assessment of accuracy and reproducibility of the whispered voice test[J]. Cien Saude Colet. 2017;22(11):3589–3598. doi:10.1590/1413-812320172211.31222016
17. Zazove P, Plegue MA, McKee MM, et al. effective hearing loss screening in primary care: the early auditory referral-primary care study. Ann Fam Med. 2020;18(6):520–527. doi:10.1370/afm.2590
18. Schneider JM, Gopinath B, McMahon CM, et al. Role of general practitioners in managing age-related hearing loss. Med J Aust. 2010;192(1):20–23. doi:10.5694/j.1326-5377.2010.tb03395.x
19. Kiely KM, Anstey KJ. Putting age-related hearing loss on the public health agenda in Australia [J]. Public Health Res Pract. 2021;31(5):3152125. doi:10.17061/phrp3152125
20. Yueh B, Piccirillo JF. Screening for hearing loss in older adults: insufficient evidence does not mean insufficient benefit. JAMA. 2021;325(12):1162–1163. doi:10.1001/jama.2021.2020
21. Feltner C, Wallace IF, Kistler CE, Coker-Schwimmer M, Jonas DE. Screening for hearing loss in older adults: updated evidence report and systematic review for the us preventive services task force. JAMA. 2021;325(12):1202–1215. doi:10.1001/jama.2020.24855
22. Carlson ML, Nassiri AM, Marinelli JP, Lohse CM; Hearing HealthCollaborative. Awareness, perceptions, and literacy surrounding hearing loss and hearing rehabilitation among the adult population in the United States. OtolNeurotol. 2022;43(3):e323–e330. doi:10.1097/MAO.0000000000003473
23. Diao M, Sun J, Jiang T, et al. Comparison between self-reported hearing and measured hearing thresholds of the elderly in China. Ear Hear. 2014;35(5):e228–32. doi:10.1097/AUD.0000000000000050
24. Wallace C, If KCE, Coker-Schwimmer M, Jonas DE, Middleton JC. Screening for Hearing Loss in Older Adults: An Evidence Review for the U.S. Preventive Services Task Force. Rockville (MD): Agency for Healthcare Research and Quality (US); 2021.
25. Kovalová M, Mrázková E, Škerková M, Čada Z, Janoutová J. The importance of screening for hearing loss in the elderly[J]. Otolaryngol Pol. 2012; 76(3):32–38. doi:10.5604/01.3001.0015.6493
26. Yang TH, Chu YC, Chen YF, et al. Diagnostic validity of self-reported hearing loss in elderly Taiwanese individuals: diagnostic performance of a hearing self-assessment questionnaire on audiometry. Int J Environ Res Public Health. 2021;18(24):13215. doi:10.3390/ijerph182413215
27. Saunders GH, Frederick MT, Silverman SC, Nielsen C, Laplante-Lévesque A. Description of adults seeking hearing help for the first time according to two health behavior change approaches: transtheoretical model (stages of change) and health belief model. Ear Hear. 2016;37(3):324–333. doi:10.1097/AUD.0000000000000268
28. Wang D, Li C, Wang Y, et al. Health education intervention on hearing health risk behaviors in college students. Int J Environ Res Public Health. 2021;18(4):1560. doi:10.3390/ijerph18041560.
29. Bennett RJ, Meyer CJ, Ryan B, Barr C, Laird E, Knowledge ERH. Beliefs, and practices of Australian audiologists in addressing the mental health needs of adults with hearing loss. Am J Audiol. 2020;29(2):129–142. doi:10.1044/2019_AJA-19-00087
30. Rj B, Cm B, Conway N, Sf F. Promoting hearing loss support in general practice: a qualitative concept-mapping study. Public Health Res Pract. 2021;31(5):3152131. doi:10.17061/phrp3152131
31. Chen Z, Duan Ji R, Zhang M, Limei Y. Auditory Rehabilitation of the Elderly[M]. Beijing: Beijing Publishing House; 2010:1–255.
32. Demin H, Shiang X, Shufeng W, Liu B, Hua Z. Basic and Clinical Audiology. Beijing: Science and technology literature and Technology Press; April 2004. 1–621.
33. Collier JE, Bienstock CC. Model misspecification: contrasting formative and reflective indicators for a model of e-service quality. J Market Theory Prac. 2014;17(3):283–293. doi:10.2753/MTP1069-6679170306
34. Shanghai Statistics Bureau. Shanghai statistical yearbook 2022. Available from: https://www.yearbookchina.com/naviBooklist-n3020013183-1.html;.
35. Kwak C, Seo YJ, Park KH, Han W. Analysis of the knowledge, attitudes, and practice model of healthcare professionals on hearing loss at elderly dementia residences in Korea. Healthcare. 2012;10(5):792. doi:10.3390/healthcare10050792
36. Leroi P, Chauhan I, Han N, et al. Hearing and vision health for people with dementia in residential long term care: knowledge, attitudes and practice in England, South Korea, India, Greece, Indonesia and Australia. Int J Geriatr Psychiatry. 2021;36(10):1531–1540. doi:10.1002/gps.5563
37. Gilliver M, Hickson L. Medical practitioners’ attitudes to hearing rehabilitation for older adults. International Journal of Audiology. 2011;50(12):850–856. doi:10.3109/14992027.2011.601468
38. Robinson BE, Barry PP, Renick N, Bergen MR, Stratos GA. Physician confidence and interest in learning more about common geriatric topics: a needs assessment. J Am Geriatr Soc. 2001;49(7):963–967. doi:10.1046/j.1532-5415.2001.49188.x
39. Committee on Accessible and Affordable Hearing Health Care for Adults; Board on Health Sciences Policy; Health and Medicine Division. National Academies of Sciences, Engineering, and Medicine. Hearing Health Care for Adults: Priorities for Improving Access and Affordability. Washington (DC): National Academies Press (US);
40. Wallhagen MI, Pettengill E. Hearing impairment: significant but underassessed in primary care settings. Journal of Gerontological Nursing. 2008;34(2):36–42. doi:10.3928/00989134-20080201-12
41. Bogardus, Jr ST Jr, Yueh B, Shekelle PG. Screening and management of adult hearing loss in primary care: clinical applications. JAMA. 2003;289(15):1986–1990. doi:10.1001/jama.289.15.1986
42. Chou R, Dana T, Bougatsos C, Fleming C, Beil T. Screening adults aged 50 years or older for hearing loss: a review of the evidence for the U.S. preventive services task force. Ann Intern Med. 2011;154(5):347–355. doi:10.7326/0003-4819-154-5-201103010-00009
43. Bennett RJ, Fletcher S, Conway N, Barr C. The role of the general practitioner in managing age-related hearing loss: perspectives of general practitioners, patients and practice staff. BMC Fam Pract. 2020;21(1):87. doi:10.1186/s12875-020-01157-2
44. Cardoso CL, Bós ÂJ, Gonçalves AK, et al. Sensitivity and specificity of portable hearing screening in middle-aged and older adults. Int Arch Otorhinol. 2013;18(1):6. doi:10.1055/s-0033-1358660
45. Wang J, Chen L, Yu M, He J. Impact of knowledge, attitude, and practice (KAP)-based rehabilitation education on the KAP of patients with intervertebral disc herniation. Ann Palliat Med. 2020;9(2):388–393. doi:10.21037/apm.2020.03.01
46. Yang Z, Liu S, Dai M, Zhang H. Knowledge, attitude and practice of advance care planning among nursing interns: a mixed-methods approach. Nurse Educ Pract. 2021;56:103183. doi:10.1016/j.nepr.2021.103183
47. Simpson AN, Matthews LJ, Cassarly C, Dubno JR. Time from hearing aid candidacy to hearing aid adoption: a longitudinal cohort study. Ear & Hearing. 2019;40(3):468–476. doi:10.1097/AUD.0000000000000641
48. Desjardins JL, Sotelo LR. Self-reported reasons for the non-use of hearing aids among Hispanic adults with hearing loss[. American Journal of Audiology. 2021;30(3):709–716. doi:10.1044/2021_AJA-21-00043
49. DeJonckheere M, McKee MM, Guetterman TC, et al. Implementation of a hearing loss screening intervention in primary care. Ann Fam Med. 2021;19(5):388–395. doi:10.1370/afm.2695
50. Wagner EH, Austin BT, Davis C, Hindmarsh M, Schaefer J, Bonomi A. Improving chronic illness care: translating evidence into action. Health Aff (Millwood). 2001;20(6):64–78. doi:10.1377/hlthaff.20.6.64
51. Lai SH, Tsoi T, Tang CT, et al. An integrated, collaborative healthcare model for the early diagnosis and management of dementia: preliminary audit results from the first transdisciplinary service integrating family medicine and geriatric psychiatry services to the heart of patients homes. BMC Psychiatry. 2019;19(1):61. doi:10.1186/s12888-019-2033-7
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.