Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Knowledge and Readiness for Interprofessional Learning Among Pharmacy and Clinical Nutrition Students at King Saud University
Authors Almazrou SH ![]() , Alaujan SS
, Alaujan SS ![]()
Received 31 January 2022
Accepted for publication 30 June 2022
Published 5 September 2022 Volume 2022:15 Pages 1965—1970
DOI https://doi.org/10.2147/JMDH.S360608
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Saja H Almazrou, Shiekha S Alaujan
Clinical Pharmacy Department, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia
Correspondence: Saja H Almazrou, Clinical Pharmacy Department, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia, Email [email protected]
Background: Interprofessional education (IPE) in healthcare specialties is important to optimize patient outcomes and shape professional image toward teamwork and collaboration among healthcare professionals. The aim of this study is to assess the impact of IPE on pharmacy and clinical nutrition students’ knowledge in food–drug interactions and readiness for interprofessional learning.
Methods: This pre-post study was conducted at King Saud University between February and March 2020. We held an interprofessional workshop for pharmacy and clinical nutrition students. After we introduced the faculty members who would deliver the food–drug interactions session, the students took a seven-question quiz (total score = 7) to assess their knowledge about the basic concept of food–drug interactions before the session. After that, a 45-minute lecture was provided by a clinical pharmacy faculty member. Students from both disciplines worked on three clinical scenarios. After completing the assigned scenarios, the students retook the quiz to assess their knowledge after the workshop. In addition, student readiness was assessed using the 19-item Readiness for Interprofessional Learning Scale (RIPLS).
Results: A total of 48 students were included in this study. Overall, students’ mean scores in both colleges significantly increased after the workshop (p < 0.01). The mean RIPLS total scores (SD) for pharmacy students and clinical nutrition students were 80.6 (7.48) and 81.26 (6.96), respectively, out of a maximum possible score of 95. These scores indicated positive attitudes toward interprofessional learning in both groups.
Conclusion: Pharmacy and clinical nutrition students’ knowledge regarding food–drug interaction improved after implementing the IPE session. Students also reported higher scores for interprofessional learning. This indicates their willingness to participate in future interprofessional learning activities. Roles and responsibilities domain scores were slightly lower among both groups. Simulation-based activities including profession role exchange can be added to traditional IPE sessions to improve this domain.
Keywords: interprofessional education, pharmacy, interprofessional learning, clinical nutrition
Introduction
Interprofessional education (IPE) defined as “occasions when two or more professionals learn with, from and about each other to improve collaboration and the quality of care.”1 By implementing IPE, students can share skills and knowledge between professions. This allows for better understanding, shared values, and respect for the roles of other healthcare professionals.2–4 Introducing IPE into curricula before students begin to practice sets the foundation for and values of working within interprofessional teams.5,6
Food–drug interactions are a major hidden issue that concern both pharmacists and clinical nutrition specialists.7 A study investigated the prevalence of food drug interactions in elderly patients prescriptions found that around 58% contains such interactions.8
Food drug interactions might lead to ineffective treatment or toxicity to patients.7 Moreover, those interaction significantly interferes with absorption, metabolism and excretion process.9 The collaboration between pharmacy and nutrition extends beyond hospitals settings. In a recently published survey among pharmacists and nutrition specialist found that `pharmacists acknowledged the need of nutritional and dietary care in community pharmacies and hoped that certified dietitians would be significantly involved.10
Therefore, early introduction of this topic through IPE sessions is crucial to limit the problem in clinical practice and to enhance collaboration among healthcare professionals.
IPE has been implemented in pharmacy programs with students from different professions/disciplines including medicine, dentistry, nursing, and allied health.11 In a systematic review of 29 studies published in 2018, only one study investigated IPE with clinical nutrition students and other specialties.12
Given the value of IPE in healthcare specialties to optimize healthcare outcomes, as well as the importance of previous experience in shaping professional image toward teamwork, the purpose of this study was to assess the impact of IPE on pharmacy and clinical nutrition students’ knowledge in food–drug interactions and readiness for interprofessional learning.
Methodology
Study Setting and Design
This was a pre-post study conducted at the female campus of King Saud University. Based on the curriculum of both disciplines, the food-drug interaction subject is introduced to fourth year students. Therefore, fourth-year students from the College of Pharmacy (n=65) and College of Applied Medical Sciences’ Clinical Nutrition Department (n= 34) were invited using emails between February and March 2020. The email contained information about the study procedure, venue, date, and time. Students who did not attend the food–drug interaction session, her readiness and knowledge will not be assessed and considered excluded from the study.
Procedure and Data Collection
One-day interprofessional workshop for pharmacy and clinical nutrition students was held in one classroom. After introducing the faculty members who would deliver the food–drug interactions session, the students undertook a seven-question quiz (total score = 7) to assess their knowledge about the basic concept of food–drug interactions before the session (Appendix 1). The quiz was designed by four teaching faculties from both colleges and underwent face and content validity. After that, a clinical pharmacy faculty member provided a 45-minute lecture. The lecture started with opening remarks, then the main content was provided to the students about the definition of food-drug interactions, types and consequences of such interaction with examples, and recommendation to minimize or resolve the consequences. Finally, a list of useful electronic resources was provided to the students to aid them in solving food-drug interaction clinical scenarios.
Then, groups of pharmacy and clinical nutrition students were formed, ensuring equal distribution from both disciplines. The groups worked on four different clinical scenarios (developed by faculty members from both disciplines) pertaining to food–drug interaction (Appendix 2). Questions were given to the students after each scenario. Problem based learning was implemented in which the students solve the questions for the scenarios using the provided electronic resources and eventually provide clinical notes, as they would in clinical practice. The session concluded with a short discussion between students and faculty members for further clarification.
After completing the four scenarios, the students retook the quiz to assess their knowledge after the workshop. In addition, we collected data such as disciplines, GPA and responses to the Readiness for Interprofessional Learning Scale (RIPLS)13 in English language through an electronic Google form. RIPLS is used to assess students’ attitudes toward IPE and concerning the roles and responsibilities of other healthcare professionals.
The RIPLS consists of 19 items assessing three domains: teamwork and collaboration (9 statements, score range 9–45), negative (3 statements, score range 3–15) and positive professional identity (5 statements, score range 5–25), and roles and responsibilities (2 statements, score range 2–10).13 A 5-point Likert scale was used to assess agreement with each item (1 = strongly disagree to 5 = strongly agree)13 in the teamwork and collaboration, positive professional identity, and roles and responsibilities domains. For negative professional identity, reverse scoring was adopted from McFadyen et al14 (1 = strongly agree to 5 = strongly disagree). Higher scores indicated a more positive attitude about interprofessional collaboration and learning, indicating students’ readiness for IPE.13
Ethical Considerations
All students were reassured that participation in the study was voluntary and students who do not participate were not affected. Electronic consents was obtained from the students prior to the participation of the study. Ethical approval was obtained from King Saud University and the Medical City Institutional Review Board (E-20-4650).
Statistical Analysis
The normality test was performed for all main statistical outcomes, and all the normally distributed outcomes were expressed as mean ± standard deviation (SD). We used an independent sample t-test to compare pharmacy and clinical nutrition students’ scores. An alpha value of 0.05 was used for testing statistical significance. All data analysis was performed using SPSS Version 27.15
Results
A total of 48 female students were included in this study, of which 25 (52.1%) were from pharmacy and 23 (47.9%) were from clinical nutrition college. The mean age (SD) was 22 (0.2) and 22 (0.21) years old for pharmacy and clinical nutrition students, respectively. The mean GPA (SD) of the participants was 4.71 (0.28) and 4.41 (0.36) out of 5 for pharmacy and clinical nutrition students, respectively. Previous experience with IPE was reported by 17 (68%) pharmacy students and by 8 (34.78%) clinical nutrition students.
We analyzed students’ knowledge of food–drug interactions based on the data from all 48 students who took the quiz before and after the workshop (see Table 1). On the pre-workshop quiz, mean knowledge was statistically higher (< 0.001) in pharmacy students compared to clinical nutrition students (Mdiff = 1.46). On the post-workshop quiz, the scores of students from both colleges increased, with no significant difference between groups (Mdiff = 0.25). Overall, students’ mean scores in both colleges increased significantly after the workshop (p < 0.01; see Table 2).
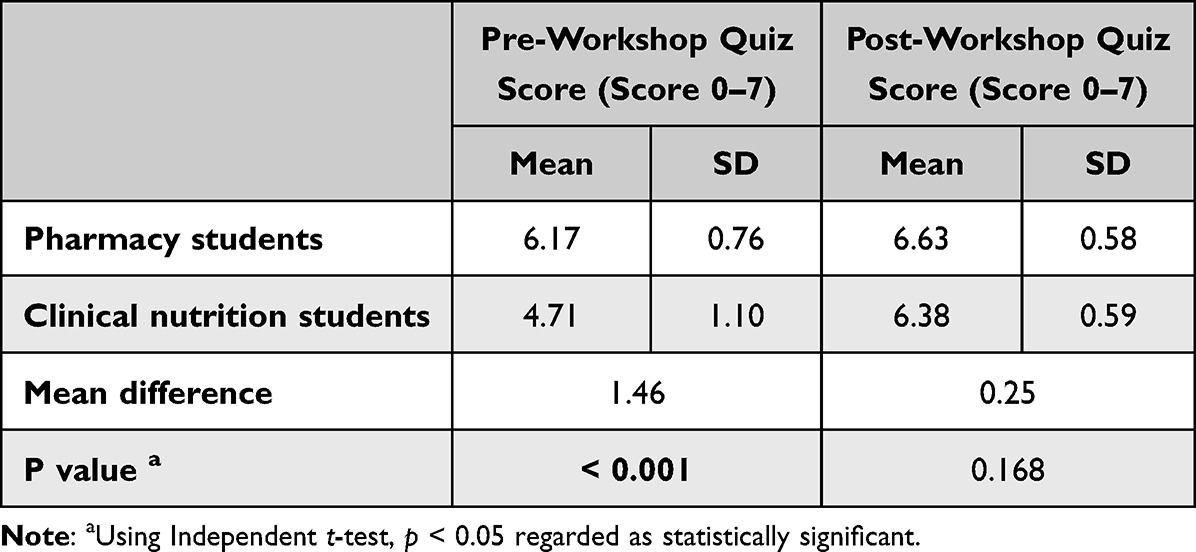 |
Table 1 Impact of the Workshop on Students’ Knowledge Scores |
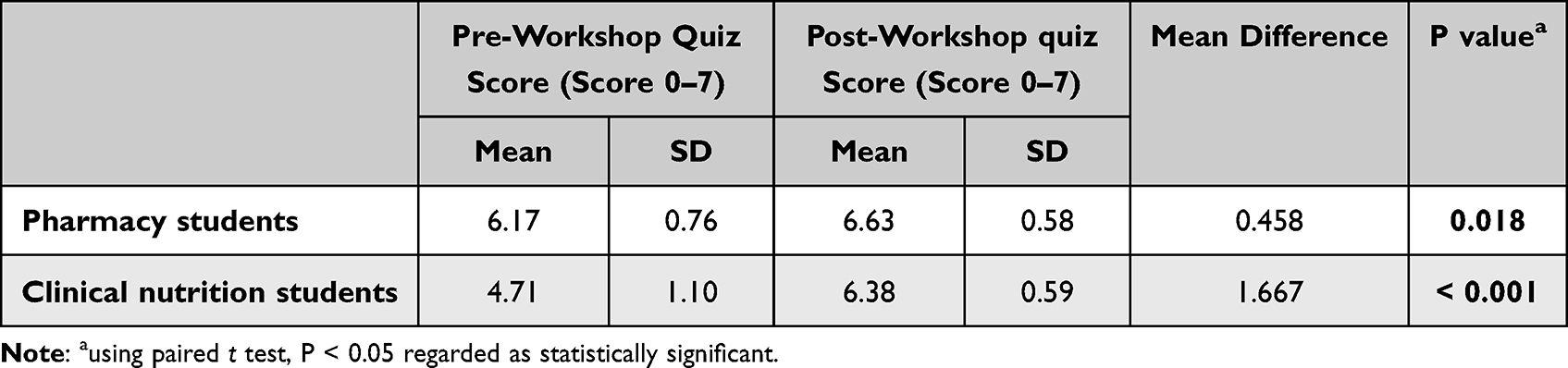 |
Table 2 Students’ Knowledge Scores by College |
RIPLS analysis of total scores and individual domains are presented in Table 3. The mean RIPLS total scores (SD) for pharmacy students and clinical nutrition students were 80.6 (7.48) and 81.26 (6.96), respectively, out of a maximum possible score of 95. This indicated positive attitudes in both groups toward interprofessional learning, with no significant difference between the two groups.
 |
Table 3 Readiness for Interprofessional Learning Scale Scores by Professional Discipline |
In domain analysis, scores were particularly high for the domains of teamwork and collaboration and positive and negative professional identity. In the roles and responsibilities domain, the average scores (SD) were 5.88 (2.20) for pharmacy students and 5.30 (1.69) for clinical nutrition students, out of a total score range between 2 and 10. We observed no significant difference between the two groups at the domain level.
Our overall analysis revealed no significant differences in students’ responses to the RIPLS. However, clinical nutrition students’ scores were significantly higher in items related to the value of IPE in understanding clinical problems and maximizing patient benefit.
Discussion
We conducted this pre-post study to assess the impact of IPE on pharmacy and clinical nutrition students’ knowledge and readiness for interprofessional learning. Our results showed that students scored higher on food drug interaction assessment after the IPE session, and further revealed that the improvement in food drug interaction knowledge was significantly greater among pharmacy students compared to clinical nutrition students. We believe that the overall improvement in knowledge was due to the provided lecture and then the interactive discussion between the students from both disciplines and finally the overall discussion with the instructor.
When readiness was compared between pharmacy and clinical nutrition students, all three sub-scale’s scores (teamwork and collaboration, professional identity, and roles and responsibilities) were high. This indicated that all students had a positive attitude regarding the importance of interprofessional learning.
Scores in the roles and responsibility domain were slightly lower in both groups. Interprofessional education can take the form of debates on a particular health issue, a grand roundtable discussion on a case in which interprofessional patient competencies are required, reflective sessions, case studies, research, community service, service learning, simulation-based activities or even a simple class or online discussion in which interprofessional expertise is required to facilitate comprehensive discussion of a particular concept.16
Wang et al17 implemented profession-role exchange experiences among medicine, pharmacy and nursing students. Profession-role exchange is an innovative simulation-based experiential learning method in which healthcare students from many professions participate as characters in a role-playing game. Students play each other’s roles in a setting comparable to a medical setting. This new positional experience could be beneficial, as students become more conscious and value the possible contributions of future members of a collaborative patient treatment team and objectively perceive tasks from their colleagues’ perspectives. Wang et al found that students who were engaged in profession-role exchange experiences had significantly higher scores in the roles and responsibilities subscale compared to control group students.
Despite the fact that students in our study and in similar studies18–21 had high readiness for IPE, faculty members reported several barriers to implementing IPE. According to Bashatah et al,22 IPE implementation is often hampered by a lack of technical assistance; time restrictions; a lack of administrative support and training; a lack of appreciation; and difficulties in forming collaborative partnerships, such as siloed curricula and calendars. In addition, faculty members have limited insight into each other’s professions. Mladenovic et al discussed the importance of faculty members training for interprofessional education.23 This training should brought faculty together in a nonhierarchical setting to learn about one other’s professions and programs, as well as to establish new terminology for the shared content on patient safety that students are now expected to study. Professors evaluations of the training and co-facilitation are extremely good, with some faculty experiencing a “IPE revelation” when they meet new people and form new partnerships.23 This suggests that putting IPE into practice necessitates close collaboration between faculty members from different schools and support from universities’ higher authorities.
This feasibility study is important to identify barriers to implementing IPE before embarking on larger studies. Numerous issues related to IPE including coordination between the two groups, topic selection and writing clinical scenarios were revealed during this study.
Limitations
There are several limitations to this study. For example, we had a small sample size; therefore, our statistical results need to be interpreted with caution. In addition, we could not assess male students’ perceptions of these strategies due to practical issues associated with campus segregation.
Conclusion
Pharmacy and clinical nutrition students’ knowledge regarding food–drug interaction improved after implementing the IPE session. Students also reported higher scores for interprofessional learning. This indicates their willingness to participate in future interprofessional learning activities. Roles and responsibilities domain scores were slightly lower among both groups.
For future studies, faculty members training and simulation-based activities including profession role exchange can be added to traditional IPE sessions to improve interprofessional education.
Acknowledgment
The authors would like to acknowledge Dr. Ingrid Echeverry and Dr. May Ahmad Alshahwan from Department of Community Health Sciences, College of Applied Medical Sciences, King Saud University for their assistance during the workshop. Also we acknowledge the Researcher Supporting Project (RSP-2022R452), King Saud University for funding the publication of this work.
Funding
The author [SSA] received a fund from the Researcher Supporting Project (RSP-2022R452), King Saud University, Riyadh, Saudi Arabia, to support the publication of this article. The funding agency had no role in designing the study, conducting the analysis, interpreting the data or writing the manuscript.
Disclosure
The authors declare no conflicts of interest.
References
1. Zwarenstein M, Atkins J, Barr H, Hammick M, Koppel I, Reeves S. A systematic review of interprofessional education. J Interprof Care. 1999;13(4):417–424. doi:10.3109/13561829909010386
2. Karim R, Ross C. Interprofessional education (IPE) and chiropractic. J Can Chiropr Assoc. 2008;52(2):76–78.
3. Craddock D, O’Halloran C, Borthwick A, McPherson K. Interprofessional education in health and social care: fashion or informed practice? Learn Heal Soc Care. 2006;5(4):220–242. doi:10.1111/j.1473-6861.2006.00135.x
4. Jones RV. Working together–learning together. J R Coll Gen Pract Occas Pap. 1986;33:1–26.
5. Engquist B, Johnsson L, Hammil M, Short F. Proceedings PDC Seventh Annual Conference: Simulation and Visualization on the Grid; 2000.
6. Casto RM. Preservice courses for interprofessional practice. Theory Pract. 1987;26(2):103–109. doi:10.1080/00405848709543258
7. Bushra R, Aslam N, Khan AY. Food-drug interactions. Oman Med J. 2011;26(2):77–83. doi:10.5001/omj.2011.21
8. Neves S, Marques A, Diniz A, et al. Prevalence and predictors of potential drug-food interactions among the elderly using prescription drugs. J Chem Pharm Res. 2016;8:965.
9. Genser D. Food and drug interaction: consequences for the nutrition/health status. Ann Nutr Metab. 2008;52(Suppl 1):29–32. doi:10.1159/000115345
10. Kizaki H, Ota T, Mashima S, et al. Questionnaire survey investigation of the present status of dietetic consultation at community pharmacies from the perspectives of registered dietitians and pharmacists. BMC Health Serv Res. 2021;21. doi:10.1186/s12913-021-06959-3
11. El-Awaisi A, Joseph S, El Hajj MS, Diack L. A comprehensive systematic review of pharmacy perspectives on interprofessional education and collaborative practice. Res Soc Adm Pharm. 2018;14(10):863–882. doi:10.1016/j.sapharm.2017.11.001
12. Judge MP, Polifroni EC, Maruca AT, Hobson ME, Leschak A, Zakewicz H. Evaluation of students’ receptiveness and response to an interprofessional learning activity across health care disciplines: an approach toward team development in healthcare. Int J Nurs Sci. 2015;2(1):93–98.
13. Parsell G, Bligh J. The development of a questionnaire to assess the readiness of health care students for interprofessional learning (RIPLS). Med Educ. 1999;33(2):95–100. doi:10.1046/j.1365-2923.1999.00298.x
14. McFadyen AK, Webster V, Strachan K, Figgins E, Brown H, McKechnie J. The readiness for interprofessional learning scale: a possible more stable sub-scale model for the original version of RIPLS. J Interprof Care. 2005;19(6):595–603. doi:10.1080/13561820500430157
15. IBM Corp. IBM SPSS statistics for windows, version 27.0; 2020.
16. Herrmann G, Woermann U, Schlegel C. Interprofessional education in anatomy: learning together in medical and nursing training. Anat Sci Educ. 2015;8(4):324–330. doi:10.1002/ase.1506
17. Wang J, Guo J, Wang Y, et al. Use of profession-role exchange in an interprofessional student team-based community health service-learning experience. BMC Med Educ. 2020;20. doi:10.1186/s12909-020-02127-z
18. Algahtani H, Shirah B, Bukhari H, et al. Perceptions and attitudes of different healthcare professionals and students toward interprofessional education in Saudi Arabia: a cross-sectional survey. J Interprof Care. 2020;35:1–6. doi:10.1080/13561820.2020.1758642
19. Zamil H, Meo SA. Medical students’ readiness and perceptions about interprofessional education: a cross sectional study. Pakistan J Med Sci. 2020;36. doi:10.12669/pjms.36.4.2214.
20. Al-Eisa E, Alderaa A, AlSayyad A, et al. The perceptions and readiness toward interprofessional education among female undergraduate health-care students at King Saud University. J Phys Ther Sci. 2016;28:1142–1146. doi:10.1589/jpts.28.1142
21. Al-Qahtani M. Measuring healthcare students’ attitudes toward interprofessional education. J Taibah Univ Med Sci. 2016;11. doi:10.1016/j.jtumed.2016.09.003.
22. Bashatah A, Alahmary K, Arifi M, et al. Interprofessional cooperation: an interventional study among Saudi healthcare teaching staff at King Saud University. J Multidiscip Healthc. 2020;2020:1537–1544. doi:10.2147/JMDH.S279092
23. Mladenovic J, Tilden V. Strategies for overcoming barriers to IPE at a health sciences university. J Interprofessional Educ Pract. 2017;8:10–13. doi:10.1016/j.xjep.2017.05.002
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.