Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Knowledge and Perception of Physicians of Different Specialties in Saudi Arabia Toward Helicobacter pylori
Authors Hakami OA ![]() , Alsubaie RA
, Alsubaie RA ![]() , Albaqami BA, Almutlaq HM, Alqahtani NM, Alkhonezan M, Almuqrin FF, Alghamdi AH, Alaryni AA, Qutob RA
, Albaqami BA, Almutlaq HM, Alqahtani NM, Alkhonezan M, Almuqrin FF, Alghamdi AH, Alaryni AA, Qutob RA ![]()
Received 20 January 2023
Accepted for publication 14 March 2023
Published 19 March 2023 Volume 2023:16 Pages 763—771
DOI https://doi.org/10.2147/JMDH.S403999
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Osamah Ahmad Hakami,* Refah Asheer Alsubaie,* Bayan Abdulhadi Albaqami, Haifa Matar Almutlaq, Nourah Mushabab Alqahtani, Manal Alkhonezan, Farah Fahad Almuqrin, Abdullah Hussien Alghamdi, Abdullah Abdulaziz Alaryni, Rayan Abubakker Qutob
Faculty of Medicine, Imam Mohammad Ibn Saud Islamic University, Riyadh, Saudi Arabia
*These authors contributed equally to this work
Correspondence: Refah Asheer Alsubaie, Faculty of medicine, Imam Mohammad Ibn Saud Islamic University, 7544 Othman Bin Affan Road Al-Nada, Riyadh, 13317, Saudi Arabia, Tel +966 50 255 2509, Email [email protected]
Background: Helicobacter pylori (H. pylori) is a key pathogen causing several gastrointestinal diseases. Fortunately, H. pylori infection is treatable, which can lower its comorbidities. However, data assessing physicians’ awareness of H. pylori is lacking in Saudi Arabia.
Objective: To assess the knowledge and awareness of physicians of different specialties who practice in Saudi Arabia about H. pylori infection.
Methods: This is a cross-sectional study conducted between May and September 2022 on physicians across all regions in Saudi Arabia using a validated online questionnaire covering their knowledge and awareness of H. pylori infection. An independent t-test, one-way ANOVA, and Games-Howell as a post hoc test were used to analyze the data. A General Linear Model was also employed to determine significant predictors among the variables reliant on H. pylori awareness.
Results: The results showed that the mean awareness score of 474 physicians was 76.99± 6.9, indicating that participants had sufficient knowledge about H. pylori infection. In general, the internal medicine specialists (28.3%) had better awareness of H. pylori infection than the other specialties. Moreover, the university hospital sector performed the best, scoring 80.68± 13.3, and the southern region had the highest-ranked physicians with a score of 81.56 ± 13.7 in terms of H. pylori awareness. Furthermore, the general linear model revealed a statistical significance (p< 0.05) for the following demographic aspects concerning H. pylori awareness: the physicians’ age group of 30– 39 years, duration of experience of 11– 15 years, the hospital sectors of Nation Guards (NGH) and Security Forces (SFH), and the southern and central regions of practice in Saudi Arabia.
Conclusion: Physicians in Saudi Arabia have relatively sufficient awareness of H. pylori; however, they are highly influenced by age, years of experience, the hospital sector involved, and the region where the physicians practice.
Keywords: H. pylori, awareness, doctors, internal medicine, gastroenterology
Introduction
Helicobacter pylori (H. pylori) is a human bacterium with a potential risk of gastric and intestinal cancer. It is a gram-negative bacterium that produces cytokines and contributes to systemic inflammation.1 It can resist and tolerate the gastric acidic pH through several functional and structural mechanisms, thus maintaining chronic infection.2 Infected people comprise over 50% of the world’s population, with a significant regional variation.3 H. pylori infection is substantially associated with several stomach-related cancers like gastric cancer and gastric lymphoma (MALT- mucosa-associated lymphoid tissue) are all substantially linked to H. pylori infection.4 The symptoms include chronic or persistent bloating and nausea, weight loss or loss of appetite, malnutrition, heartburn, and indigestion. Furthermore, this bacterial infection has been associated with the development of atrophic inflammation of the stomach lining, which has several repercussions for gastric function.5 Extra gastric manifestations are also linked to H. pylori infection.6 For example, it has been attributed to the severity of psoriasis,7 and it has been demonstrated that eliminating this infection could dramatically improve rosacea skin problems.8 Diagnosis and therapy are usually based on the Maastricht V/Florence Consensus Report.9 Stool antigen and urea breath testings are the common H. pylori diagnostic procedures.9,10 Treatment includes a known standard combination of antibiotics and proton pump inhibitors. A 10–14 day treatment is preferable to eradicate the infection than a 7-day treatment.9,11 However, the recurrence rate of infection and associated gastrointestinal disorders are well-documented challenges,12 and antimicrobial resistance is becoming a concern for H. pylori, as shown in a survey conducted in Spain with a resistance level reaching up to 30%.13 Saudi Arabian data on H. Pylori prevalence were not consistent, and it ranged from 70% in 1989 to 10.2% in 2018. Moreover, geographic location, diagnostic methods used, time period and specialty of the treating physician varied significantly.14–19 Moreover, according to a systematic review compiling published epidemiological data on the incidence of cancers in Saudi Arabia between 2010–2019, the incidence of gastric cancer was found to be around 1.9%. However, no accurate data on its subtypes or link with H. pylori infection.20
Studies assessing the physicians’ knowledge and awareness about H. pylori are limited. In 2003, the North American Society for Paediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) conducted an internet-based survey evaluating pediatric gastroenterologists’ knowledge and practices regarding H. pylori that 514 NASPGHAN members completed. It was concluded that physicians were well informed about H. pylori infection in children despite the lack of published guidelines at the time of the survey. However, knowledge about antibiotic resistance rates was lacking.21 A survey study from Turkey evaluating the knowledge, attitude, and practice (KAP) regarding H. pylori among general practitioners showed a significant lack of updated knowledge and deviated from the guidelines.22 Furthermore, a retrospective study analyzing physicians’ practices in treating H. pylori infection in Maryland, USA, found notable non adherence to the guidelines illustrated by the fact that one-third of the patients were not tested before treatment, and post-treatment testing was not appropriate.23 Another cross-sectional study was done in Pakistan to assess KAP toward H. pylori and showed a lack of adequate knowledge in managing H. pylori infection among primary care physicians.24 Moreover, a nationwide survey conducted in China between 2014 and 2017 investigated whether the clinical practice deviates from the guidelines. Awareness of H pylori infection and related diseases varied among physicians, ranging from 45% to 95%. Around 40% did not adhere to the diagnostic approach, therapeutic options were accurate in less than 70%, and 20% did not confirm eradication of the infection.25
In Saudi Arabia, Hafiz et al conducted a cross-sectional study using an online survey evaluating the degree of knowledge of H. pylori infection among undergraduate university students. Less than 10% of the study population had a good level of knowledge on the subject, and the level was significantly and proportionately associated with the following factors: university level, family monthly income, having heard about H. pylori infection, and having a previous history of H. pylori infection. Other demographic parameters (age, gender, number of siblings) and the field of university study (health science versus non-health science) were not associated with the degree of knowledge of H. pylori.26 Up to the date of conducting this survey, we could not find any study in Saudi Arabia evaluating knowledge and awareness about H. pylori among physicians of different specialties since day-to-day clinical practice shows that many healthcare disciplines surprisingly deal with H. pylori infection in the absence of local guidelines on this matter. Hence, the purpose of this study is to lay the ground for further research assessing clinical practice against the guidelines and health policy formulation in line with the anticipated publication of practice guidelines for managing H. pylori infection by “The Saudi H. pylori Working Group recommendations” which was yet to be published by the time we conducted this study.
Methods
This cross-sectional survey-based study used a validated online questionnaire to collect data from voluntary participants after obtaining informed consent. A minimum of 385 participants sample size was decided based on a confidence level of 95% and a margin of error of 5%. A convenience sampling technique was used to collect the data between May 2022 and September 2022. The inclusion criterion was all Saudi and non-Saudi physicians of different specialties who were working in the Kingdom of Saudi Arabia during the study period. Non-physicians or physicians who were not working in Saudi Arabia or did not agree to complete the survey were excluded. The questionnaire was based on a previous similar study with permission granted by the first author, Taghreed A Hafiz.26 However, the sociodemographic part was modified to suit our study population. It was constructed on Google Forms to allow ease of dissemination and automatic capturing of the completed surveys. It was then distributed electronically via text messages to the enrolled physicians on their phones through the researchers of this study, who had access to the participants’ contact information. However, it was an open survey. The Informed consent was embedded at the beginning of the survey. Nevertheless, the collected data were secure, protected, and without unique identifiers of the participants.
Simple descriptive statistics were used to analyze this research. For the categorical and nominal variables, we used them to specify the characteristics of the demographics in the form of numbers and percentages. Means and standard deviations were used to represent continuous variables. A score of H. pylori awareness was determined by translating the answers to the questions into the numbers 0 and 1, which stand for “unaware” and “aware”, respectively.
After converting each response, a simple additive method was used to obtain the total score, and the total score was converted to a hundred-point scale. Moreover, to assess the internal consistency of a questionnaire (or survey), we used reliability analysis with a model by Alpha (Cronbach). An independent t-test was used to compare two group means to establish a relationship between outcome and demographics. A one-way ANOVA test with Games-Howell as a post hoc test was utilized for more than two groups. A general linear model (GLM) was also employed to discover significant variables or demographic data predictors. Finally, the null hypothesis was rejected using a conventional p-value of 0.05.
Results
Socio-Demographic Characteristics
Four hundred seventy-four (474) physicians completed the online survey. Most participants were men (67.3%), and the majority were 25–29 years (53.6%). Most participants were resident physicians (56.1%) with <5 years of experience (58.9%). Half of them (46.4%) worked in the Ministry of Health (MOH). Among the doctors surveyed, most practice in the central region of Saudi Arabia (24.1%), predominantly in Riyadh city. In addition, most doctors were in internal medicine (28.3%), with the rest being in other disciplines. Table 1 summarizes the demographics of the participants.
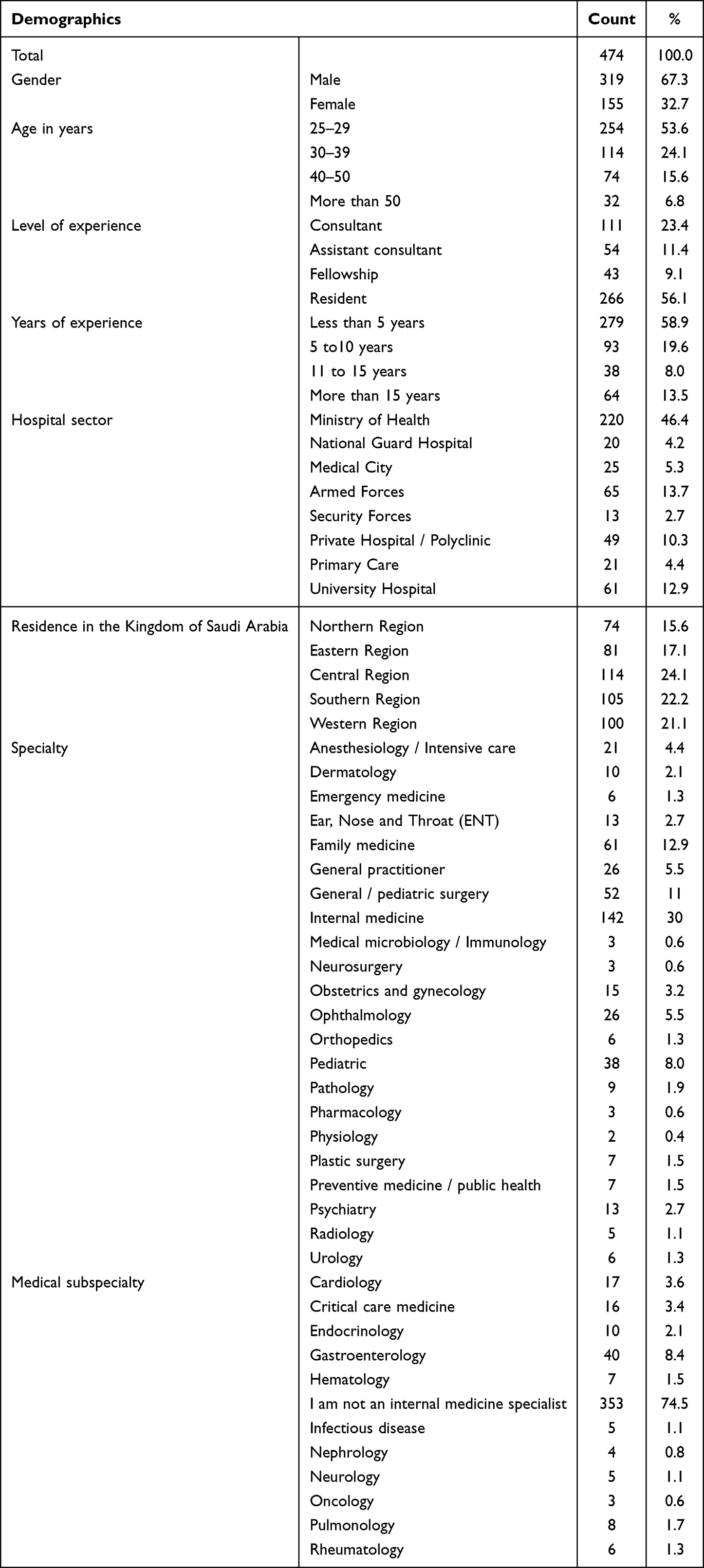 |
Table 1 Characteristics of Physicians Who Responded to the Questionnaire |
Knowledge About H. pylori Among Physicians
The average H. pylori awareness of the physicians who participated scored 76.99± 6.9. This indicates that most surveyed participants had sufficient knowledge of H. pylori infection. The results revealed that 91.6% of the participants were aware of H. pylori being a bacterium that causes stomach ulcers. A total of 58.6% responded that socioeconomic status is one of the contributing factors for this infection, and 88.6% of participants knew that hand washing is a preventive measure for H. pylori infection. As for testing choice to diagnose the infection, 87.8% chose the urea breath test, while the stool antigen test was the option to know the presence of H. pylori. Additionally, the majority of participants (88.4%) indicated that H. pylori infection is the primary cause of stomach cancer which happens when infectious bacteria start to break down the stomach lining and release a toxic substance that damages cells. A summary of the physician’s responses is shown in Figure 1.
 |
Figure 1 Summary of physicians’ awareness of H. pylori infection in Saudi Arabia. |
Statistically Significant Factors in H. pylori Awareness Among Physicians
Using a one-way ANOVA test and Games-Howell, the hospital sector and the region of practice were found to be substantially associated with H. pylori awareness, with p-values of 0.007 and 0.001, respectively. Overall, the university hospital sector performed the best, scoring 80.68±13.3 in terms of H. pylori awareness. At the same time, the southern region had the highest-ranked physicians with an awareness score of 81.56 ±13.7 for H. pylori infection. The eastern, western, and northern regions received close statistical measurements. Table 2 shows the detailed results of this analysis. Employing the general linear model to examine the relationships between the demographics and H. pylori awareness, a statistical significance of <0.05 was found for the following: physicians’ age group of 30–39-year (p = 0.025), duration of experience of 11–15 years (p = 0.018), hospital sector of NGH (p = 0.006) and security forces (p = 0.011), and region of practice in the southern (p=0.004) and central (p = 0.010) regions of Saudi Arabia. Table 3 illustrates the results of the general linear model.
 |
Table 2 Relationship Between the Demographics and Helicobacter pylori Awareness |
 |
Table 3 Demographic Predictions for Helicobacter pylori Knowledge |
Discussion
One of the most prevalent infectious diseases around the world is H. pylori.27–29 It is responsible for almost 15 thousand mortalities yearly, most of which are caused by chronic gastritis and peptic ulcer disease.30 To the best of our knowledge, this was the first study to analyze Saudi physicians’ knowledge and awareness about H. pylori. It has been demonstrated that health practitioners in Saudi Arabia have good knowledge and practices that are crucial to the successful screening and eradication rate of this infection, which would help reduce the risk of gastric cancer. H. pylori prevalence varies by country and demography. Although other variables may contribute to these differences, genetic predisposition, geography, differences in food consumption and hygiene practices, and socioeconomic class are thought to be the primary causes. The age group between 25 and 29 years had the highest rate of H. pylori infection.31
Our study revealed that internal medicine specialists scored the highest among others. This result follows a study that showed that internists in Rasht, Iran, scored higher on knowledge tests than general practitioners. The author explained that residents have done more studies in this field and are experienced in practice since they visited more patients.31
Overall, the results of this study indicate that physicians in Saudi Arabia have a good command of H. pylori knowledge. For treating gastrointestinal problems to be more effective, knowledge about it among doctors and the public needs to be increased. Survey research was undertaken in China to investigate the level of knowledge of 546 physicians from various disciplines about H. pylori infection compared to the general population. Based on the results, physicians’ knowledge was expected to be higher than that of the general population. Still, the authors found a surprising lack of support for H. pylori testing among gastroenterologists.32
Regarding the practice of H. pylori, the present study showed that most participants know how to manage the infection. This is in contrast to the previous survey studies conducted in Turkey, Maryland (USA), Pakistan, and China, where the evaluation of the knowledge, attitude, and practice regarding H. pylori among general practitioners showed a lack of updated knowledge and variable practices deviating from the guidelines in term of diagnostic testing, accurate therapeutic approaches and confirmation of eradication.22–25 Moreover, by the time of writing this manuscript, we found a very recent publication of a questionnaire-based cross-sectional study done in Al-Madinah city, Saudi Arabia evaluating the adequacy of H. pylori eradication practices among 100 primary care physicians where the authors found an unsatisfactory level of practice regarding H. pylori eradication.33
The participating physicians in our study were highly diverse; nevertheless, our study did not assess patients’ data in terms of diagnosis, management, and treatment outcomes to objectively evaluate the current practices, which is the main limitation. Furthermore, the Saudi Gastroenterology Association published the practice guidelines of the Saudi H. pylori Working Group Recommendations in October 2022.34 Therefore the door is open for future research prospects involving these local guidelines.
Conclusion
Our study concluded that adequate knowledge and perception of H. pylori infection was identified among physicians of various specialties working in Saudi Arabia. Age, years of experience, the hospital sector, and the region where the physicians’ practice were the main influencing factors. Further studies are recommended to assess adherence to guidelines in diagnosing and managing H. pylori infection.
Data Sharing Statement
All data associated with this study are present in the paper.
Ethical Approval
The study was approved by the Institutional Review Board at Imam Mohammad Ibn Saud Islamic University with IRB No. 249/2022. Informed consent was embedded at the beginning of electronic survey. This study was conducted in accordance with the World Medical Association (WMA) Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that there are no conflicts of interests in this work.
References
1. Bardazzi F, Magnano M, Fiorini G, et al. Helicobacter pylori infection in psoriatic patients during biological therapy.. Italian Journal of Dermatology and Venereology. 2021;156(5):570–574. doi:10.23736/S2784-8671.19.06410-1
2. Ansari S, Yamaoka Y. Survival of Helicobacter pylori in gastric acidic territory. Helicobacter. 2017;22(4). doi:10.1111/hel.12386
3. Hooi JKY, Lai WY, Ng WK, et al. Global Prevalence of Helicobacter pylori Infection: systematic Review and Meta-Analysis. Gastroenterology. 2017;153(2):420–429. doi:10.1053/j.gastro.2017.04.022
4. Yang JC. Treatment of Helicobacter pylori infection: current status and future concepts. World J Gastroenterol. 2014;20(18):5283–5293. doi:10.3748/wjg.v20.i18.5283
5. Scida S, Russo M, Miraglia C, et al. Relationship between Helicobacter pylori infection and GERD.. Acta Biomed. 2018;89(8–S):40–43. doi:10.23750/abm.v89i8-S.7918
6. Gravina AG, Zagari RM, De Musis C, Romano L, Loguercio C, Romano M. Helicobacter pylori and extragastric diseases: a review. World J Gastroenterol. 2018;24(29):3204–3221. doi:10.3748/wjg.v24.i29.3204
7. Mesquita PMD, Filho DA, Jorge MT, Berbert ALCV, Mantese SADO, Rodrigues JJ. Relationship of Helicobacter pylori seroprevalence with the occurrence and severity of psoriasis. An Bras Dermatol. 2017;92(1):52–57. doi:10.1590/abd1806-4841.20174880
8. Gravina A, Federico A, Ruocco E, et al. Helicobacter pylori infection but not small intestinal bacterial overgrowth may play a pathogenic role in rosacea. United European Gastroenterol J. 2015;3(1):17–24. doi:10.1177/2050640614559262
9. Malfertheiner P, Megraud F, O’Morain CA, et al. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut. 2017;66(1):6–30. doi:10.1136/gutjnl-2016-312288
10. Lopes AI, Vale FF, Oleastro M. Helicobacter pylori infection - recent developments in diagnosis.. World J Gastroenterol. 2014;20(28):9299–9313. doi:10.3748/wjg.v20.i28.9299
11. Fischbach W, Malfertheiner P. Helicobacter Pylori Infection.. Dtsch Arztebl Int. 2018;115(25):429–436. doi:10.3238/arztebl.2018.0429
12. Cui R, Zhou L. Helicobacter pylori infection: an overview in 2013, focus on therapy.. Chin Med J. 2014;127(3):568–573.
13. Miqueleiz-Zapatero A, Alba-Rubio C, Domingo-García D, et al. Primera encuesta nacional sobre el diagnóstico de la infección por Helicobacter pylori en los laboratorios de microbiología clínica en España. Enferm Infecc Microbiol Clin. 2020;38(9):410–416. doi:10.1016/j.eimc.2019.11.008
14. Al-Moagel MA, Evans DG, Abdulghani ME, et al. Prevalence of Helicobacter (formerly Campylobacter) pylori infection in Saudi Arabia, and comparison of those with and without upper gastrointestinal symptoms.. Am J Gastroenterol. 1990;85(8):944–948.
15. Almadi MA, Aljebreen AM, Tounesi FA, Abdo AA. Helicobacter pylori prevalence among medical students in a high endemic area.. Saudi Med J. 2007;28(6):896–898.
16. Telmesani AM. Helicobacter Pylori: prevalence and relationship with abdominal pain in school children in Makkah city, western Saudi Arabia. Saudi J Gastroenterol. 2009;15(2):100–103. doi:10.4103/1319-3767.45359
17. Hanafi MI, Mohamed AM. Helicobacter pylori infection: seroprevalence and predictors among healthy individuals in Al Madinah, Saudi Arabia. J Egypt Public Health Assoc. 2013;88(1):40–45. doi:10.1097/01.EPX.0000427043.99834.a4
18. Akeel M, Elmakki E, Shehata A, et al. Prevalence and factors associated with H. pylori infection in Saudi patients with dyspepsia. Electron Physician. 2018;10(9):7279–7286. doi:10.19082/7279
19. Alharbi RH, Ghoraba M. Prevalence and patient characteristics of Helicobacter pylori among adult in primary health care of security forces hospital Riyadh, Saudi Arabia, 2018. J Family Med Prim Care. 2019;8(7):2202–2206. doi:10.4103/jfmpc.jfmpc_398_19
20. Alqahtani WS, Almufareh NA, Domiaty DM, et al. Epidemiology of cancer in Saudi Arabia thru 2010-2019: a systematic review with constrained meta-analysis.. AIMS Public Health. 2020;7(3):679–696. doi:10.3934/publichealth.2020053
21. Chang HY, Sharma VK, Howden CW, Gold BD. Knowledge, Attitudes, and Practice Styles of North American Pediatric Gastroenterologists:Helicobacter pylori Infection. J Pediatr Gastroenterol Nutr. 2003;36(2):235–240. doi:10.1097/00005176-200302000-00015
22. Canbaz S, Sunter AT, Peksen Y, Leblebicioglu H. Survey of general practitioners knowledge about Helicobacter pylori infection. BMC Gastroenterol. 2005;5(1):4. doi:10.1186/1471-230X-5-4
23. Howden CW, Blume SW, de Lissovoy G. Practice patterns for managing Helicobacter pylori infection and upper gastrointestinal symptoms.. Am J Manag Care. 2007;13(1):37–44.
24. Ahmed S, Salih M, Jafri W, Ali Shah H, Hamid S. Helicobacter pylori infection: approach of primary care physicians in a developing country. BMC Gastroenterol. 2009;9(1):23. doi:10.1186/1471-230X-9-23
25. Song C, Xie C, Zhu Y, et al. Management of Helicobacter pylori infection by clinicians: a nationwide survey in a developing country. Helicobacter. 2019;24(6):e12656. doi:10.1111/hel.12656
26. Hafiz TA, D’Sa JL, Zamzam S, Dionaldo MLV, Mubaraki MA, Tumala RB. Helicobacter pylori Infection: comparison of Knowledge between Health Science and Non-Health Science University Students. Int J Environ Res Public Health. 2021;18(15):8173. doi:10.3390/ijerph18158173
27. Camilo V, Sugiyama T, Touati E. Pathogenesis of Helicobacter pylori infection. Helicobacter. 2017;22:e12405. doi:10.1111/hel.12405
28. Thorell K, Lehours P, Vale FF. Genomics of Helicobacter pylori. Helicobacter. 2017;22:e12409. doi:10.1111/hel.12409
29. Wroblewski LE, Peek RM, Wilson KT. Helicobacter pylori and Gastric Cancer: factors That Modulate Disease Risk. Clin Microbiol Rev. 2010;23(4):713–739. doi:10.1128/CMR.00011-10
30. Institute of Medicine (US) Committee to Study Priorities for Vaccine Development. Vaccines for the 21st Century: A Tool for Decision making. In: Stratton KR, Durch JS, Lawrence RS, eds. Washington (DC): National Academies Press (US); 2000.
31. Hasosah M, Satti M, Shehzad A, et al. Prevalence and Risk Factors of Helicobacter pylori Infection in Saudi Children: a Three-Year Prospective Controlled Study. Helicobacter. 2015;20(1):56–63. doi:10.1111/hel.12172
32. Wu Y, Su T, Zhou X, Lu N, Li Z, Du Y. Awareness and attitudes regarding Helicobacter pylori infection in Chinese physicians and public population: a national cross-sectional survey. Helicobacter. 2020;25(4):e12705. doi:10.1111/hel.12705
33. Al-Dubai SAR, Alharbi OA, Tolah HW, et al. Adequacy of practice regarding Helicobacter pylori eradication in Al-Madinah, Kingdom of Saudi Arabia: a cross-sectional study. Med Sci. 2022;26:ms546e2623.
34. Alsohaibani F, Peedikayil M, Alshahrani A, et al. Practice guidelines for the management of Helicobacter pylori infection: the Saudi H. pylori Working Group recommendations. Saudi J Gastroenterol. 2022. doi:10.4103/sjg.sjg_288_22
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Psychological Impact of COVID-19 on Doctors and Medical Students of Punjab, Pakistan: A Logistic Regression Analysis
Junaid Tahir M, Tariq W, Anas Tahseen Asar M, Irfan Malik M, Kamal Akhtar F, Malik M, Akhtar Q, Abbasher Hussien Mohamed Ahmed K, Talha Awan M, Ullah K, Asghar MS
Journal of Multidisciplinary Healthcare 2022, 15:1297-1308
Published Date: 8 June 2022