Back to Journals » Journal of Pain Research » Volume 16
Job Satisfaction Among Pain Medicine Physicians in the US
Authors Maloney JA ![]() , D’Souza RS
, D’Souza RS ![]() , Buckner Petty SA, Turkiewicz MJ, Sinha D
, Buckner Petty SA, Turkiewicz MJ, Sinha D ![]() , Patel A, Strand NH
, Patel A, Strand NH ![]()
Received 1 February 2023
Accepted for publication 30 May 2023
Published 31 May 2023 Volume 2023:16 Pages 1867—1876
DOI https://doi.org/10.2147/JPR.S406701
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Robert Twillman
Jillian A Maloney,1 Ryan S D’Souza,2 Skye A Buckner Petty,3 Michal J Turkiewicz,4 Debarshi Sinha,4 Ajay Patel,5 Natalie H Strand1
1Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, Phoenix, AZ, USA; 2Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, Rochester, MN, USA; 3Department of Quantitative Health Sciences, Mayo Clinic, Scottsdale, AZ, USA; 4Mayo Clinic Alix School of Medicine, Scottsdale, AZ, USA; 5Department of Rehabilitation & Regenerative Medicine (Patel), New York-Presbyterian Hospital-University Hospital of Columbia and Cornell, New York, NY, USA
Correspondence: Jillian A Maloney, Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, 5777 East Mayo Boulevard, Phoenix, AZ, 85054, USA, Email [email protected]
Purpose: Data are lacking on the factors that contribute to job satisfaction among pain medicine physicians. We sought to determine how sociodemographic and professional characteristics relate to job satisfaction among pain medicine physicians.
Methods: In this nationwide, multicenter, cross-sectional observational study, an electronic questionnaire related to job satisfaction was emailed in 2021 to pain medicine physicians who were members of the American Society of Anesthesiologists or the American Society of Pain and Neuroscience. The 28-item questionnaire asked physicians about sociodemographic and professional factors. Eight questions related to job satisfaction were based on a 10-point Likert scale, and 1 question was a binary (yes/no) variable. Differences in responses based on sociodemographic and professional factors were assessed with the Kruskal–Wallis rank sum test for Likert scale questions and with the Pearson χ2 test for yes/no questions.
Results: We determined that several variables, including gender, parental status, geographic location, specialty, years of practice, and volume of patients, are associated with pain medicine physicians’ outlook on job satisfaction. Overall, 74.9% of respondents surveyed would choose pain medicine as a specialty again.
Conclusion: High rates of poor job satisfaction persist among pain medicine physicians. This survey study identified several sociodemographic and professional factors that are associated with job satisfaction among pain medicine physicians. By identifying physicians at high risk for poor job satisfaction, healthcare leadership and occupational health agencies can aim to protect physicians’ well-being, enhance working conditions, and raise awareness about burnout.
Keywords: economics, outcomes, pain management
Plain Language Summary
Job satisfaction among physicians across all specialities has been evaluated; however, studies evaluating factors that affect job satisfaction for pain medicine physicians are lacking. Our study identified differences in job satisfaction when results were stratified by factors such as gender, income, practice location, and clinic volume. These results in combination with results from future studies should provide knowledge for improving physician well-being.
Introduction
Job satisfaction is a multidimensional evaluation of an employee’s emotional response to their experience at work.1 It accounts for the extent to which an employee feels positively or negatively about different aspects of a job, such as working conditions, coworkers, hours, tasks, responsibilities, and rewards.2 Job satisfaction is a key component of a physician’s quality of life and has a role in the quality of care a physician delivers to patients.3,4 Physicians with higher job satisfaction are more committed and productive and have a positive effect on the organization and the patients they serve.1,3
Several sociodemographic and professional factors that may contribute to physician job satisfaction are age, sex, practice specialty, salary, and workload.1 These factors may be important predictors of dissatisfaction and burnout, which are important issues among anesthesiologists and pain medicine physicians.5 Previous studies have found that pain medicine physicians have symptoms of burnout at significantly higher rates than most other physicians.6,7 Further, pain medicine physicians have higher rates of burnout than physicians in other anesthesia subspecialties.5 This is thought to result from their responsibilities in balancing busy outpatient and inpatient clinical practices and performing invasive procedures.5 Furthermore, pain medicine physicians work with a patient population that often has persistent pain, drug dependence, and a spectrum of behavioral or mental health issues that are challenging to treat.5 Moreover, younger physicians are the most susceptible to burnout, so the future of the subspecialty is at risk.5,8 It is imperative to better understand the reasons for job dissatisfaction and burnout among pain medicine physicians and to identify possible interventions.
To our knowledge, the current evidence does not identify sociodemographic or professional risk factors that may be negative predictors of job satisfaction among pain medicine physicians. We sought to conduct a nationwide survey study that collected data on job satisfaction, sociodemographic variables, and professional variables. The primary aim was to produce a descriptive report of job satisfaction and secondarily to identify differences stratified by demographics. We predicted that there are several factors, including professional and personal factors, significantly associated with job satisfaction. This can help bridge the gap in our understanding of job satisfaction among pain medicine physicians and help identify those who are at high risk for job dissatisfaction and burnout.
Methods
Study Design
Our study was approved by the Mayo Clinic Institutional Review Board. The study was granted a waiver for informed consent because it did not evaluate new or existing patient records, did not pose a risk that was greater than minimal, and was deemed to be compliant with the Health Insurance Portability and Accountability Act because safeguards were in place to protect the personal health information of the participants. This was a nationwide, multicenter, cross-sectional, observational study, in which participants who were pain medicine physicians were invited to complete an electronic questionnaire related to job satisfaction.
Study Population and Data Extraction
After reviewing articles that evaluated job satisfaction, 2 of the coauthors created an electronic 28-item questionnaire to evaluate the job satisfaction of practicing pain medicine physicians (Appendix). The questionnaire was voluntary and was emailed in 2021 to pain medicine physicians who were members of the American Society of Anesthesiologists (ASA) or the American Society of Pain and Neuroscience (ASPN). In addition to the data from questionnaire items related to job satisfaction, data were collected on sociodemographic variables, including gender (male, female, other); marital status (married or in domestic partnership, single); partner’s employment status (full-time, part-time, not employed); and parental status (yes, no). Further, professional variables were also collected from respondents and included medical specialty (anesthesiology, physical medicine and rehabilitation [PM&R], neurology, interventional radiology, medicine, other); geographic region of practice in the US (Northeast, Southeast, Midwest, Northwest, Southwest); years in practice since fellowship graduation (1–5, 6–10, 11–15, 16–20, >20); practice setting (partner in private practice, employee in private practice, solo provider in private practice, academic medical center, other); most common insurance payer (commercial, Medicare, Medicaid, split Medicare and commercial); opioid management offered in practice (yes, no); and number of patients seen per day (0–10, 11–20, 21–30, 31–40, >40). Responses to 8 questionnaire items related to job satisfaction were recorded on a 10-point Likert scale, whereas 1 questionnaire item (“Would you choose pain medicine as a specialty again?”) was recorded as a binary (yes/no) variable. The 9 questionnaire items related to job satisfaction are listed in the Appendix.
Statistical Analysis
Sociodemographic variables and professional variables were summarized as frequencies and percentages for nominal variables and as means, medians, and 25th to 75th interquartile ranges for the variables measured with the 10-point Likert scale. Differences in responses based on sociodemographic variables and professional variables were assessed with the Kruskal–Wallis rank sum test for Likert scale questions and with the Pearson χ2 test for yes/no questions. P values less than 0.05 were considered statistically significant. All analyses were conducted with R version 3.6 (R Foundation).
Results
Baseline Characteristics
In total, 275 participants submitted responses to the questionnaire (Table 1). Some questions may not have been answered because they were not relevant to the respondent; thus, the total number of respondents per question varied and is reflected in Tables 1–3. Respondents were members of the ASA and ASPN.
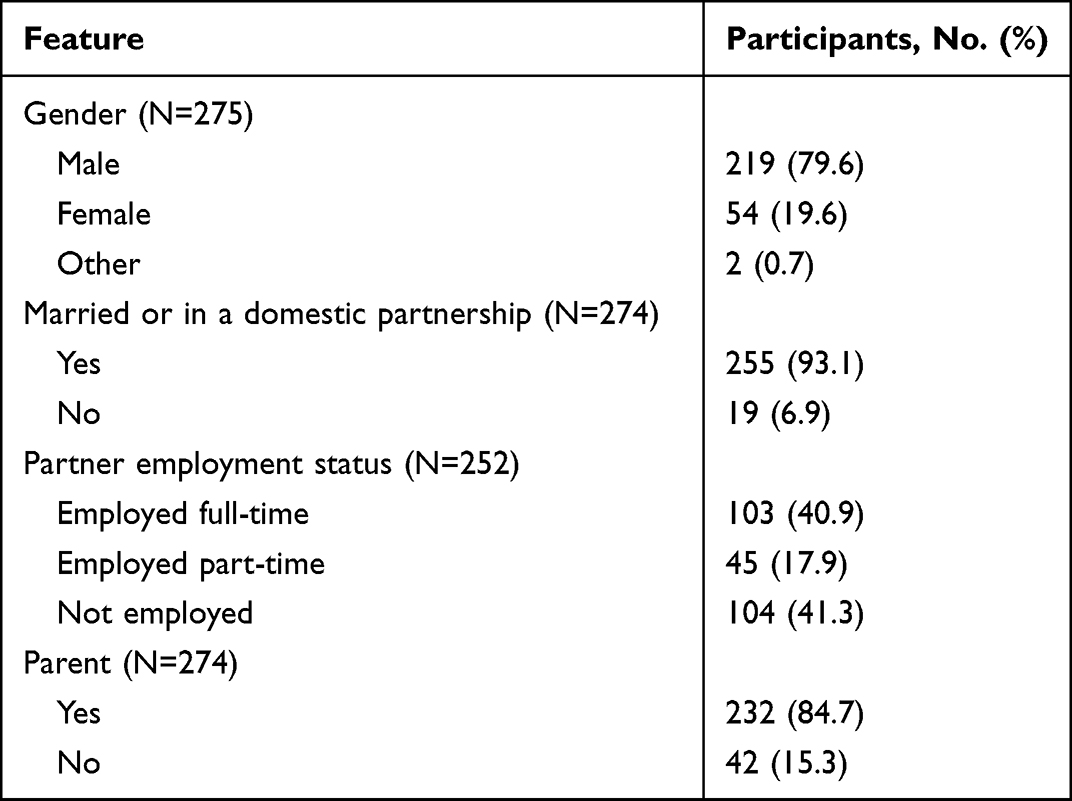 |
Table 1 Personal Demographics of Participants |
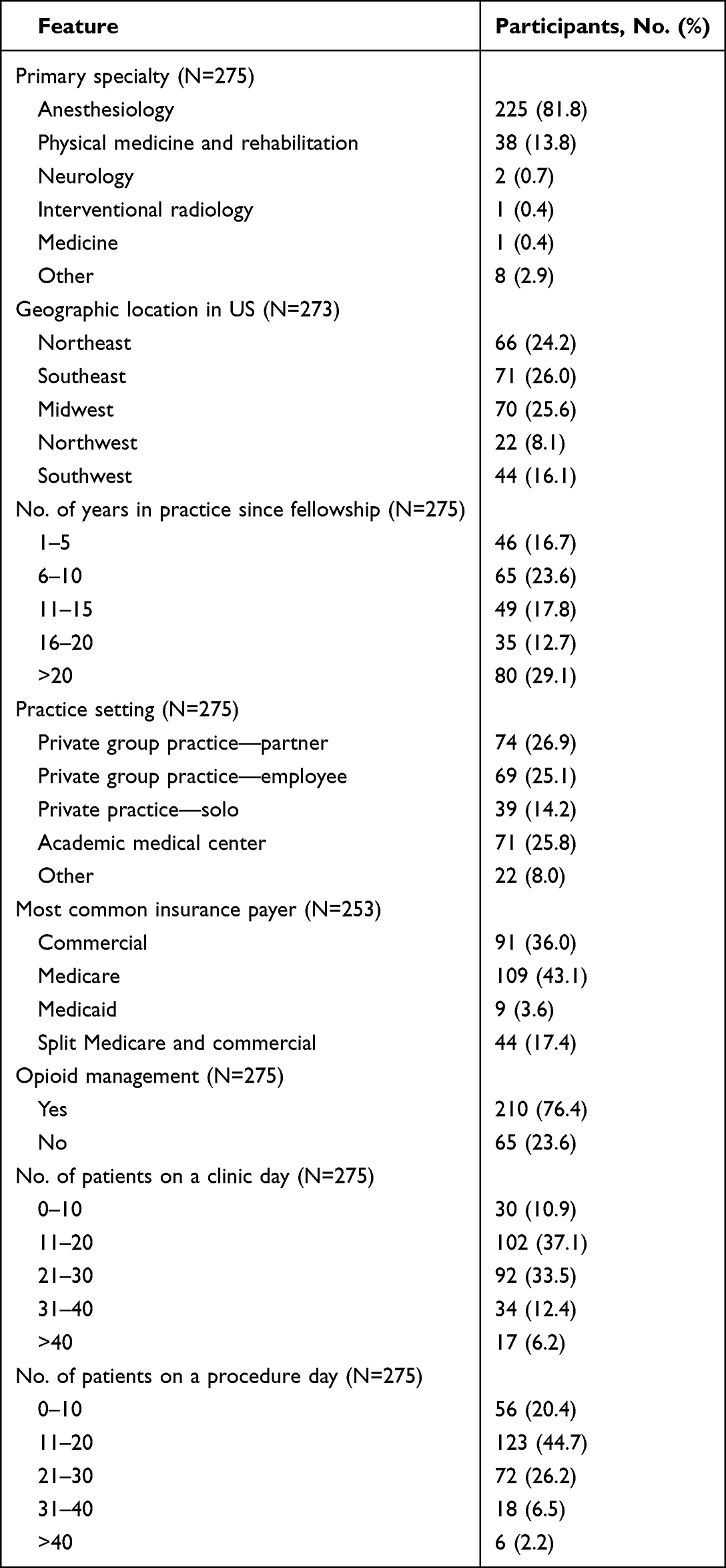 |
Table 2 Professional Demographics of Participants |
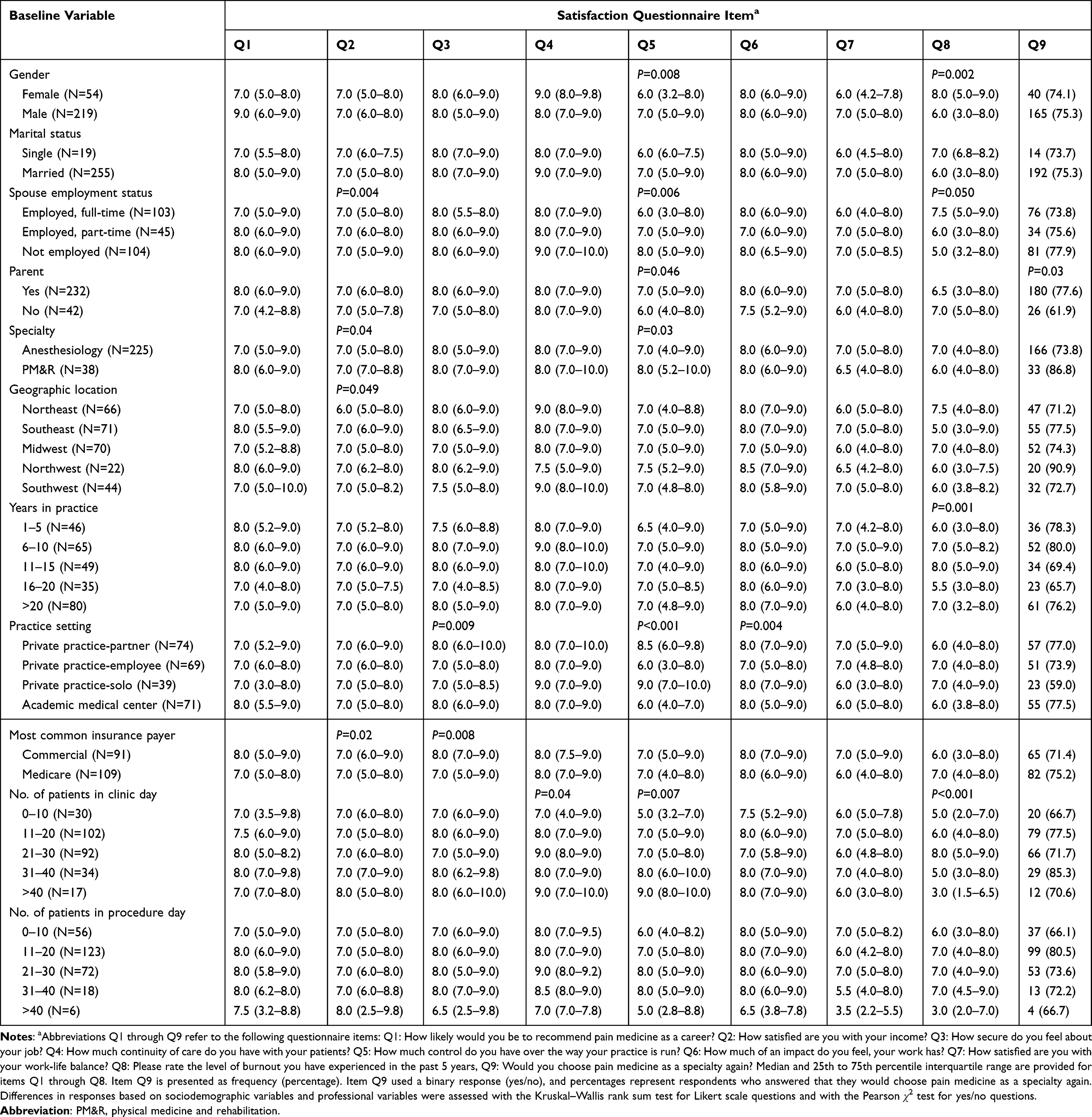 |
Table 3 Satisfaction Questionnaire Items by Sociodemographic and Professional Variables |
More respondents were men (219; 79.6%) than women (54; 19.6%); 2 respondents (0.7%) identified their gender as Other (Table 1). Most respondents were married or in a domestic partnership (255; 93.1%). Of these, the majority reported that the partner was employed full-time (103; 40.9%) or part-time (45; 17.9%) outside the home, with 41.3% (104) of partners not working. Most respondents had children (232; 84.7%); the median number of children was 2. The majority of respondents (74.9%) would choose pain medicine as a specialty again.
Most respondents reported that anesthesiology was their primary specialty (225; 81.8%) (Table 2); for others, the primary specialty was PM&R (38; 13.8%), neurology (2; 0.7%), interventional radiology (1; 0.4%), medicine (1; 0.4%), and other (8; 2.9%). After completing fellowship, most respondents had been practicing for 6 to 10 years (65; 23.6%) or for more than 20 years (80; 29.1%). On a typical clinic day, most respondents saw 11 to 20 patients (102; 37.1%) or 21 to 30 patients (92; 33.5%). On a typical procedure day, most respondents saw 11 to 20 patients (123; 44.7%). Results for other baseline variables are shown in Table 1 and Table 2.
Most respondents reported that they would recommend pain medicine as a career (median [IQR], 8.0 [5.0–9.0]). Additionally, 74.9% of respondents reported that they would choose pain medicine as a specialty again. Overall, respondents reported that they were satisfied with their income (median [IQR], 7.0 [5.0–8.0]).
Association Between Sociodemographic Characteristics and Questionnaire Items Related to Job Satisfaction
Responses to job satisfaction questions (with responses ranging from 1–10) are summarized in Figure 1 and stratified by sociodemographic characteristics in Table 3. Compared to male respondents, female respondents reported decreased control over the way their practice is run (median [IQR], 6.0 [3.2–8.0] vs 7.0 [5.0–9.0]; P=0.008) and higher degree of burnout in the past 5 years (median [IQR], 8.0 [5.0–9.0] vs 6.0 [3.0–8.0]; P=0.002). Respondents who were parents reported greater control of the way they run their practice (median [IQR], 7.0 [5.0–9.0] vs 6.0 [4.0–8.0]; P=0.046) and a preference for choosing pain medicine as a specialty again (77.6% vs 61.9%; P=0.03) compared to respondents without children.
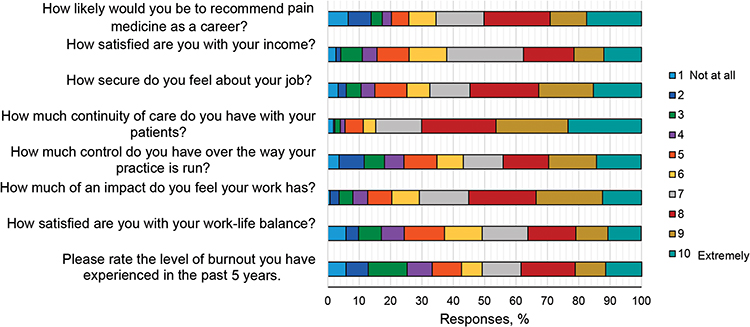 |
Figure 1 Questionnaire Results Related to Job Satisfaction Among Pain Medicine Physicians (N=275). |
Among respondents with a spouse, those married to a full-time employed spouse reported lower satisfaction with their own income compared to those with a part-time employed spouse (median [IQR], 7.0 [5.0–8.0] vs 7.0 [6.0–8.0]; P=0.005) or an unemployed spouse (median [IQR], 7.0 [5.0–8.0] vs 7.0 [5.0–9.0]; P=0.005). Respondents married to a full-time employed spouse also reported less control over the way they run their practice compared to those with a part-time employed spouse (median [IQR], 6.0 [3.0–8.0] vs 7.0 [5.0–9.0]; P=0.03) or an unemployed spouse (median [IQR], 6.0 [3.0–8.0] vs 8.0 [5.0–9.0]; P=0.002). Finally, respondents with a full-time employed spouse reported a higher degree of burnout compared to those with an unemployed spouse (median [IQR], 7.5 [5.0–9.0] vs 5.0 [3.2–8.0]; P=0.02).
Association Between Professional Characteristics and Questionnaire Items Related to Job Satisfaction
Responses to job satisfaction questions stratified by professional characteristics are displayed in Table 3. Pain physicians with prior residency training in PM&R reported higher satisfaction with their income (median [IQR], 7.0 [7.0–8.8] vs 7.0 [5.0–8.0]; P=0.04) and greater perceived control over their practice (median [IQR], 8.0 [5.2–10.0] vs 7.0 [4.0–9.0]; P=0.03) compared to pain physicians with prior residency in anesthesiology.
Responses also varied by practice setting. Respondents who practiced in the Northeast US reported lower satisfaction with their income compared to respondents located in other regions (P=0.049). Respondents who had practiced 16 to 20 years reported the lowest degree of burnout compared to those who had practiced 1 to 15 years or more than 20 years (P<0.001). Physicians employed as partners in private practice reported feeling more secure about their job compared to physicians in private practice who were non-partnered employees (median [IQR], 8.0 [6.0–10.0] vs 7.0 [5.0–8.0]; P=0.006) or who were practicing solo (median [IQR], 8.0 [6.0–10.0] vs 7.0 [5.0–8.5]; P=0.003). Physicians who practiced solo reported greater control of their practice compared to physicians in private practice who were non-partnered employees (median [IQR], 9.0 [7.0–10.0] vs 6.0 [3.0–8.0]; P<0.001) and physicians working in academic medical centers (median [IQR], 9.0 [7.0–10.0] vs 6.0 [4.0–7.0]; P<0.001). Finally, physicians who practiced solo felt their work had greater impact compared to physicians in private practice who were non-partnered employees (median [IQR], 8.0 [7.0–9.0] vs 7.0 [5.0–8.0]; P<0.006).
Respondents who primarily saw patients insured with commercial insurance reported greater satisfaction with their income (median [IQR], 7.0 [6.0–9.0] vs 7.0 [5.0–8.0]; P=0.01) and greater job security (median [IQR], 8.0 [7.0–9.0] vs 7.0 [5.0–9.0]; P=0.001) compared to respondents who primarily saw patients insured with Medicare. Respondents who saw more than 30 patients during clinic days reported greater control of their practice (median [IQR], 9.0 [6.0–10.0] vs 7.0 [4.0–8.0]; P<0.001) and lower degree of burnout (median [IQR], 4.0 [3.0–7.8] vs 7.0 [4.0–8.0]; P=0.005) compared to respondents who saw no more than 30 patients during clinic days.
Discussion
The relationships between physician job satisfaction, physician burnout, and physician suicide are becoming increasingly apparent. Physicians have higher levels of burnout than the general American population, and pain medicine physicians in particular have high levels of burnout.1,2 Interestingly, burnout is higher among chronic pain physicians than among physicians in other anesthesia subspecialties.3 Although the prevalence of job dissatisfaction and burnout among physicians treating chronic pain has been explored, the underlying associations are less clear. The present study identified several negative predictors of job satisfaction, which we discuss below.
Female respondents reported having less control over their practice and higher levels of burnout, both of which are consistent with other reports on burnout in the literature.4 An unexpected finding is the lack of difference in income satisfaction between male and female respondents, especially considering reports that show that female physicians receive significantly less income than male physicians.5,6,9 We speculate that high compensation in the specialty overall compared to other medical specialties may attenuate gender disparities in pay.
The employment status of a physician’s spouse was also a predictor of job satisfaction. Respondents married to a spouse working full-time reported significantly lower satisfaction with income, lower control over their practice, and higher levels of burnout. A potential explanation may be insufficient physician incomes where the cost of living is high, so that a spouse is needed to work full-time. Another explanation is a lack of social support from a working partner. Further, it is plausible that burnout is more frequently reported by physicians with a spouse who is working full-time because of limitations in leisurely time spent together and a greater burden from family and household responsibilities.
Income satisfaction was rated higher by pain medicine physicians whose primary specialty was PM&R than by physicians in anesthesiology, despite the lower average income for PM&R physicians.4 Respondents may have been influenced by other factors, such as the cost of living in their area or their household size. Another possibility is the substantial increase in compensation for pain medicine fellowship–trained PM&R physicians compared with other PM&R subspecialties.4 In contrast, compensation remains similar for pain medicine fellowship–trained anesthesiologists compared with other anesthesia subspecialties.
Further, income satisfaction was noted to be lower among pain medicine physicians who practiced in the Northeast; this finding could be related to the higher cost of living in relation to compensation in that region. We did not ask participants for the state where they practiced or whether the practice was in an urban or a rural area, which may help explain this disparity in income satisfaction based on geography.
Physician employees at academic centers and in private practice reported that they had less control over their practice and a lower sense of impact, and private practice partners were more likely to report a greater sense of job security than private practice employees or private solo practitioners. These are consistent with studies of other specialties,10–12 which have found that private practitioners felt less security because of competition with other physicians, but otherwise they had greater autonomy in their work.
Interestingly, physicians with more than 20 years of experience in practice reported significantly less burnout than all other groups surveyed. Previous studies have posited that older physicians may have lower levels of burnout because they have more experience and confidence in their roles and in managing burnout, which may help explain this finding.13
Physicians who primarily saw patients insured by Medicare reported significantly less satisfaction with income and felt less secure about their jobs compared to those who primarily saw patients who had commercial insurance. A potential explanation may be related to the high commercial payment rates relative to Medicare.14 For instance, a study demonstrated that for physician services, commercial insurance paid 143% of Medicare rates and ranged from 118% to 179% of Medicare rates.15
Limitations
This study has several limitations. The questionnaire runs the risk of responder bias and selection bias because it was distributed only to members of major anesthesiology subspecialty societies and resulted in a larger proportion of responses from anesthesiologists. The response rate is unavailable for our study as the questionnaire was distributed by the professional societies and the total number of physicians it was sent to was unavailable. According to the American Association of Medical Colleges, in 2021 there were 6240 active pain medicine and pain management physicians in the US.16 Therefore, another limitation is the small sample size for our questionnaire. Although the group of participants is representative of gender in anesthesiology,16 we cannot be certain that it is representative of pain medicine physicians. In addition, our cross-sectional observation would be strengthened by a longitudinal approach because many of the factors we assessed (eg, job insecurity and control over practice) have been linked to the development of burnout.17 While acknowledging these limitations in our study design, we were nevertheless successful in obtaining a participant group with a profile from various backgrounds. The findings may help serve as the foundation for future studies to further our understanding of the underlying causes of physician burnout in pain medicine and factors that contribute to job satisfaction.
Conclusion
In this nationwide, cross-sectional, observational survey study, we sought to determine which sociodemographic and professional factors were associated with job satisfaction among pain medicine physicians. We found differences in characteristics of job satisfaction when results were stratified by factors such as gender, parental status, geographic location, specialty, years of practice, and clinic volume. Although responder and selection bias are a concern given the population surveyed, we were able to elicit valuable information to help us better understand physician job satisfaction in pain medicine. Future studies with a larger and more diverse population could further elucidate granular differences in the role of social and professional factors in relation to job satisfaction. Using the information from this study on negative predictors of job satisfaction, healthcare leadership and occupational health agencies can target and identify physicians who are at high risk for job dissatisfaction and burnout and protect physicians’ well-being.
Abbreviations
ASA, American Society of Anesthesiologists; ASPN, American Society of Pain and Neuroscience; PM&R, physical medicine and rehabilitation.
Data Sharing Statement
The authors confirm that the data supporting the findings of this study are available within the article and its Supplementary Materials.
Ethics Approval and Informed Consent
Our study was approved by the Mayo Clinic Institutional Review Board. The study was granted a waiver for informed consent because it did not evaluate new or existing patient records, did not pose a risk that was greater than minimal, and was deemed to be compliant with the Health Insurance Portability and Accountability Act because safeguards were in place to protect the personal health information of the participants.
Consent for Publication
Informed consent was waived for this study because patient records were not involved. All the participants were physicians who voluntarily completed the questionnaire, and no personally identifiable information was involved in the analysis.
Acknowledgment
Randall J. Fritz, DVM, Mayo Clinic, substantively edited the manuscript. The Scientific Publications staff at Mayo Clinic provided proofreading, administrative, and clerical support.
Author Contributions
All authors made a significant contribution to the reported work in 1 or more areas, including conception, study design, execution, acquisition of data, and analysis and interpretation; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was required for this project.
Disclosure
Dr Strand is a consultant for Nimbus Therapeutics, Nevro Corp, and Abbott Laboratories. Dr. D’Souza receives grant funding from Nevro Corp and Saol Therapeutics. The authors report no other conflicts of interest in this work.
References
1. Zhang Z, Shi G, Li L, Bian Y. Job satisfaction among primary care physicians in western China. BMC Fam Pract. 2020;21(1):219. doi:10.1186/s12875-020-01292-w
2. Ommen O, Driller E, Kohler T, et al. The relationship between social capital in hospitals and physician job satisfaction. BMC Health Serv Res. 2009;9:81. doi:10.1186/1472-6963-9-81
3. Oh YI, Kim H, Kim K. Factors affecting Korean physician job satisfaction. Int J Environ Res Public Health. 2019;16(15):2714. doi:10.3390/ijerph16152714
4. Schmit Jongbloed LJ, Cohen-Schotanus J, Borleffs JCC, Stewart RE, Schonrock-Adema J. Physician job satisfaction related to actual and preferred job size. BMC Med Educ. 2017;17(1):86. doi:10.1186/s12909-017-0911-6
5. Hyman SA, Card EB, De Leon-Casasola O, Shotwell MS, Shi Y, Weinger MB. Prevalence of burnout and its relationship to health status and social support in more than 1000 subspecialty anesthesiologists. Reg Anesth Pain Med. 2021;46(5):381–387. doi:10.1136/rapm-2020-101520
6. Shanafelt TD, West CP, Sinsky C, et al. Changes in burnout and satisfaction with work-life integration in physicians and the general US working population between 2011 and 2017. Mayo Clin Proc. 2019;94(9):1681–1694. doi:10.1016/j.mayocp.2018.10.023
7. Shanafelt TD, Boone S, Tan L, et al. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch Intern Med. 2012;172(18):1377–1385. doi:10.1001/archinternmed.2012.3199
8. Ashton-James CE, McNeilage AG, Avery NS, Robson LHE, Costa D. Prevalence and predictors of burnout symptoms in multidisciplinary pain clinics: a mixed-methods study. Pain. 2021;162(2):503–513. doi:10.1097/j.pain.0000000000002042
9. MedScape. Physician compensation report 2022: incomes gain, pay gaps remain. WebMD; 2022. Available from: https://www.medscape.com/viewarticle/972296.
10. Mahoney ST, Irish W, Strassle PD, et al. Practice characteristics and job satisfaction of private practice and academic surgeons. JAMA Surg. 2021;156(3):247–254. doi:10.1001/jamasurg.2020.5670
11. Balch CM, Shanafelt TD, Sloan JA, Satele DV, Freischlag JA. Distress and career satisfaction among 14 surgical specialties, comparing academic and private practice settings. Ann Surg. 2011;254(4):558–568. doi:10.1097/SLA.0b013e318230097e
12. Bell DJ, Bringman J, Bush A, Phillips OP. Job satisfaction among obstetrician-gynecologists: a comparison between private practice physicians and academic physicians. Am J Obstet Gynecol. 2006;195(5):1474–1478. doi:10.1016/j.ajog.2006.05.039
13. Peisah C, Latif E, Wilhelm K, Williams B. Secrets to psychological success: why older doctors might have lower psychological distress and burnout than younger doctors. Aging Ment Health. 2009;13(2):300–307. doi:10.1080/13607860802459831
14. Seibold MF. Impact of commercial over-reimbursement on hospitals: the curious case of central Indiana. Int J Health Econ Manag. 2019;19(1):99–114. doi:10.1007/s10754-018-9249-9
15. Lopez E, Neuman T, Jacobson G, Levitt L. How much more than Medicare do private insurers pay? A review of the literature. Kaiser Family Foundation; 2022. Available from: https://www.kff.org/medicare/issue-brief/how-much-more-than-medicare-do-private-insurers-pay-a-review-of-The-literature/.
16. Association of American Medical Colleges. Active physicians by sex and specialty, 2019. Association of American Medical Colleges; 2022. Available from: https://www.aamc.org/data-reports/workforce/interactive-data/active-physicians-sex-and-specialty-2019.
17. Geuskens GA, Koppes LL, van den Bossche SN, Joling CI. Enterprise restructuring and the health of employees: a cohort study. J Occup Environ Med. 2012;54(1):4–9. doi:10.1097/JOM.0b013e31823c766e
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.