Back to Journals » Cancer Management and Research » Volume 18

Jianpi Rougan Method in Support of Lenvatinib Therapy: A Real-World Study on Maintaining Relative Dose Intensity and Mitigating Toxicity–Driven Discontinuation in Intermediate-to-Advanced HCC
Received 12 February 2026
Accepted for publication 12 June 2026
Published 25 June 2026 Volume 2026:18 603191
DOI https://doi.org/10.2147/CMAR.S603191
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Seema Singh
Tianbin Zhang,1 Peng Kuang2
1Department of Oncology, The Second Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, Zhejiang, 310005, People’s Republic of China; 2Department of Traditional Chinese Medicine, Ji’an Central People’s Hospital, Ji’an, Jiangxi, 343000, People’s Republic of China
Correspondence: Peng Kuang, Department of Traditional Chinese Medicine, Ji’an Central People’s Hospital, No. 106 Jinggangshan Avenue, Ji’an, Jiangxi, 343000, People’s Republic of China, Email [email protected]
Purpose: To investigate the effects of Jianpi Rougan method on lenvatinib (LEN) relative dose intensity (RDI), toxicity-related treatment discontinuation, and treatment tolerability in intermediate-to-advanced hepatocellular carcinoma (HCC).
Methods: A real-world, retrospective study was conducted on 152 intermediate-to-advanced HCC patients receiving LEN. Patients were grouped based on concurrent use of Jianpi Rougan decoction (combined, n = 73) or not (monotherapy, n = 79). Primary endpoints were RDI at weeks 8, 12, and overall, and the proportion of RDI ≥ 80%. Secondary endpoints included toxicity-related discontinuation, adverse events, and short-term efficacy (objective response rate, ORR; disease control rate, DCR). Propensity score matching (PSM, 1:1) was employed to balance baseline confounders.
Results: After PSM (65 pairs, n = 130), baseline characteristics were balanced. The combined group showed significantly higher RDI at week 12 (P = 0.001) and overall (P = 0.003), increased proportion of RDI ≥ 80% (P = 0.029), fewer dose reductions (P = 0.022) and interruptions (P = 0.045), reduced toxicity-related permanent discontinuation (P = 0.021), decreased overall discontinuation (P = 0.034), and longer treatment duration (P = 0.042). Decreased appetite was less frequent in the combined group (P = 0.036), with trends towards less diarrhea and transaminase elevation. ORR and DCR were higher in the combined group, but the differences were not statistically significant (P > 0.05).
Conclusion: Jianpi Rougan method combined with LEN was associated with improved RDI, lower rates of toxicity-related treatment discontinuation, and enhanced treatment persistence in real-world practice, supporting its role as a feasible integrative strategy to maintain targeted therapy intensity.
Keywords: intermediate-to-advanced hepatocellular carcinoma, lenvatinib, relative dose intensity, Jianpi Rougan method, integrative Chinese and western medicine, real-world study, treatment tolerability, toxicity-related discontinuation
Introduction
Hepatocellular carcinoma (HCC) is the most common primary liver malignancy and remains one of the leading causes of cancer-related mortality worldwide. Recent epidemiological data indicate that liver cancer continues to impose a substantial global health burden, particularly in East Asia, where chronic hepatitis B virus infection remains a major etiological factor. Despite advances in surveillance and diagnostic techniques, a substantial proportion of patients are still diagnosed at an intermediate or advanced stage, thereby losing the opportunity for potentially curative treatments such as surgical resection, liver transplantation, or local ablation.1,2 Consequently, systemic therapy has become the cornerstone of treatment for these patients. Recent advances in molecular oncology and translational research have substantially improved the understanding of HCC pathogenesis, therapeutic targets, and the tumor immune microenvironment, providing new opportunities for precision medicine and individualized treatment strategies.3–5 In parallel, molecular targeted therapy, immunotherapy, and combination treatment strategies have significantly improved clinical outcomes in patients with unresectable HCC, although treatment-related toxicities and treatment sustainability remain important challenges in real-world practice.6–8 Among these agents, lenvatinib (LEN), a multikinase inhibitor, has demonstrated favorable antitumor activity and has been established as an important first-line treatment option for unresectable HCC.9
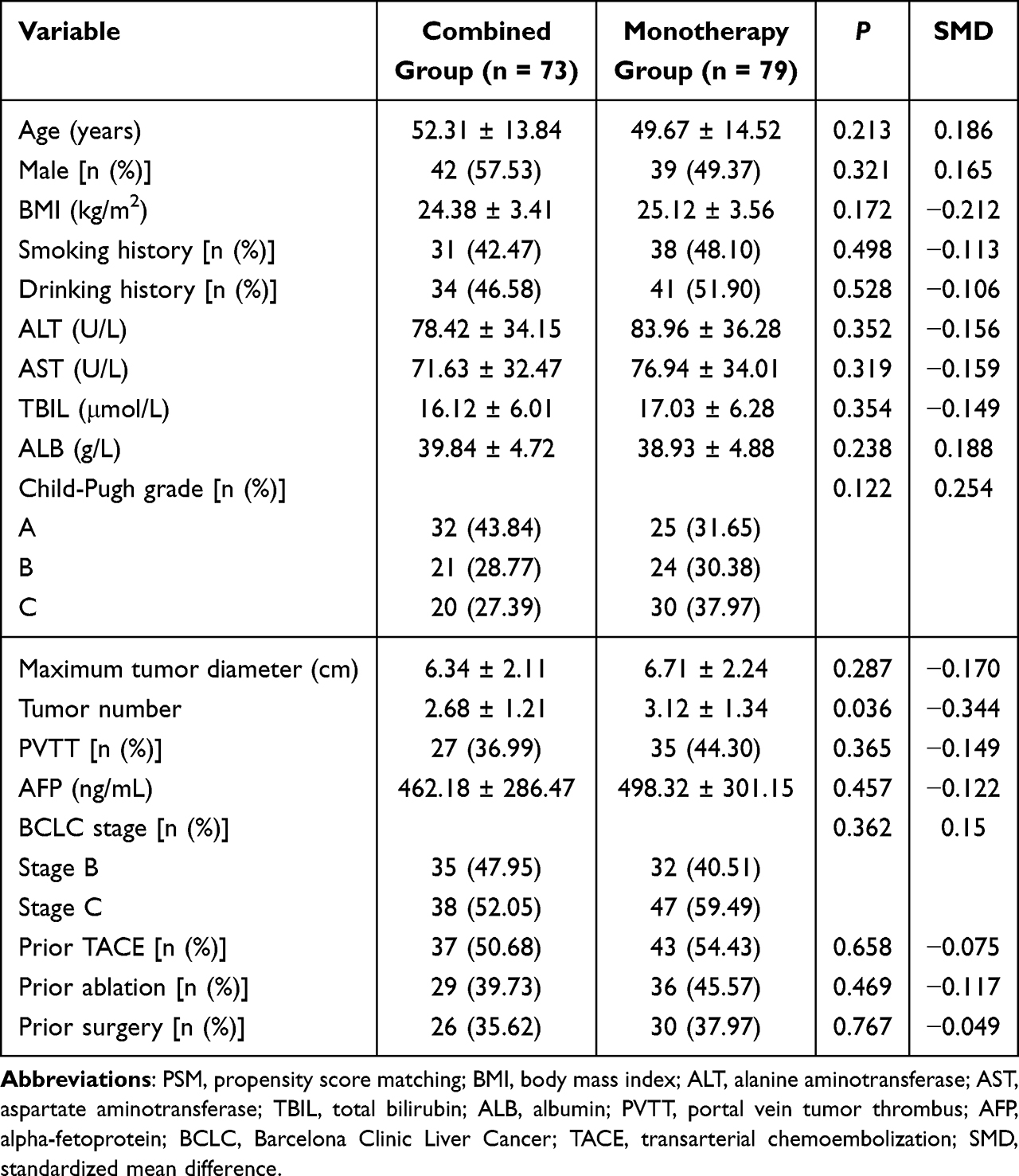 |
Table 1 Baseline Characteristics Before PSM |
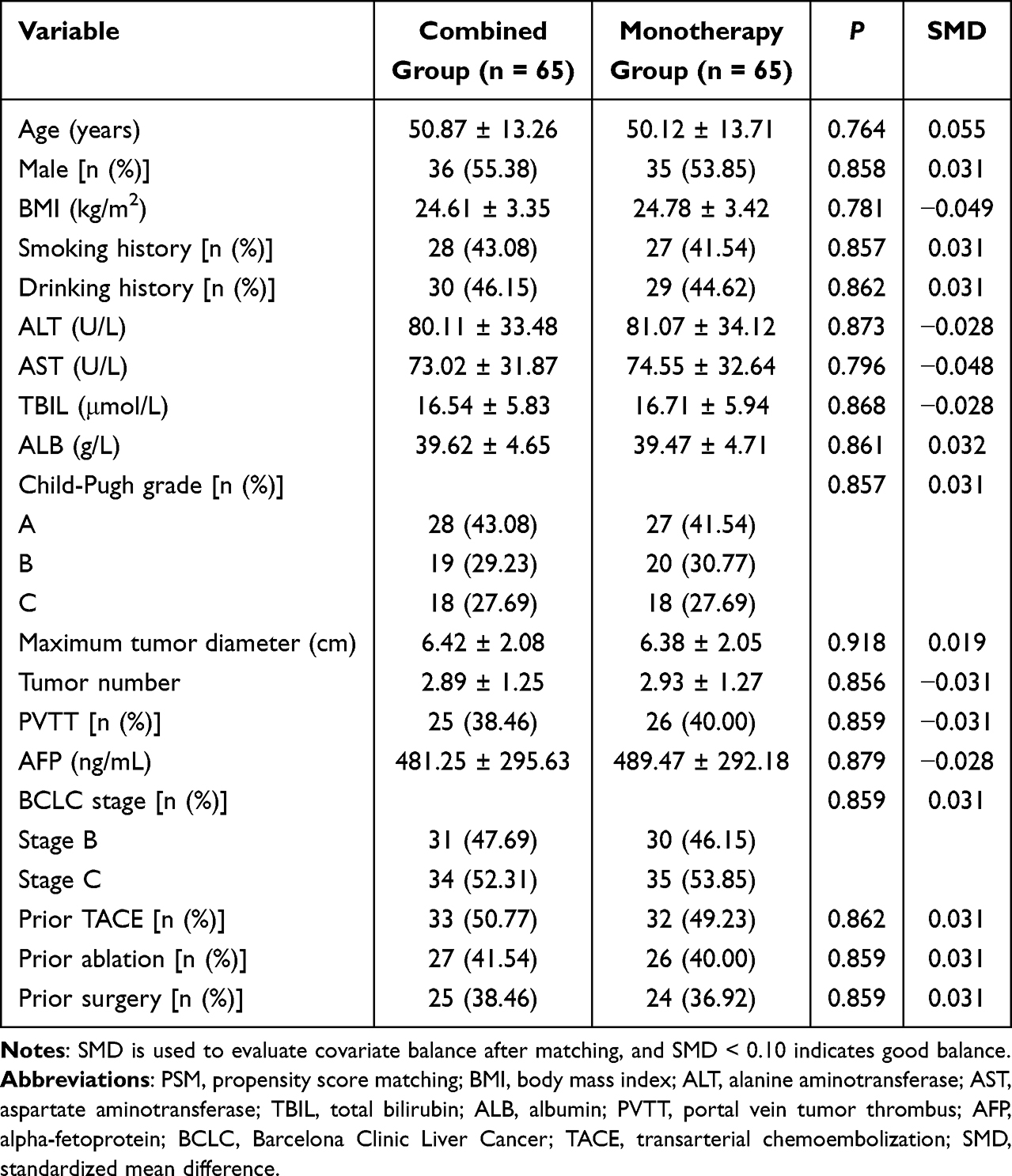 |
Table 2 Baseline Characteristics After PSM |
However, LEN treatment is often accompanied by adverse events (AEs) such as hypertension, diarrhea, fatigue, and hand-foot syndrome, whose frequency and severity are more pronounced in real-world populations.10 Previous studies indicate that the efficacy of LEN is somewhat dose-intensity dependent. In clinical practice, AEs frequently lead to dose reductions or premature treatment discontinuation, creating a vicious cycle of toxicity–dose reduction–discontinuation–compromised efficacy, which becomes a key issue affecting long-term patient benefit.11,12
Relative dose intensity (RDI) reflects the ratio of the actual cumulative drug dose received by the patient over a planned period to the standard planned dose, providing a comprehensive evaluation of treatment persistence and accessibility.13 Studies have suggested that in various anti-cancer treatments, a higher RDI is associated with better progression-free survival (PFS) and overall survival (OS).14 Compared to pure efficacy endpoints, RDI more closely reflects real-world clinical practice by indicating a patient’s overall tolerance to the treatment regimen and treatment continuity. Therefore, RDI is considered an important surrogate marker for assessing the real-world benefit of targeted therapy, particularly suitable for retrospective and real-world studies.
In traditional Chinese medicine (TCM) theory, HCC is often categorized as a deficiency in origin and excess in manifestation syndrome, with liver stagnation and spleen deficiency as the root cause, and blood stasis and toxin accumulation as the manifestations.15 Patients with intermediate-to-advanced disease often present with symptoms such as poor appetite, fatigue, abdominal distension, loose stools, and emotional depression, which highly overlap with the clinical manifestations of targeted therapy-related AEs. The Jianpi Rougan method, centered on harmonizing the liver and spleen and supporting healthy Qi, is commonly used in clinical practice to improve digestive function, alleviate fatigue, and address mood disorders.
Previous research suggests that TCM as supportive therapy can improve the quality of life and treatment tolerance in cancer patients to some extent.16 However, systematic evaluation at the real-world level regarding its potential to help patients maintain the dose intensity of targeted agents and reduce toxicity-related dose reductions or discontinuations is still lacking. Given these considerations, we conducted a real-world retrospective cohort study to evaluate whether Jianpi Rougan therapy was associated with improved maintenance of lenvatinib dose intensity, reduced toxicity-related discontinuation, and better treatment tolerability in patients with intermediate-to-advanced HCC.
Materials and Methods
Study Population
This single-center, retrospective cohort study enrolled patients with intermediate-to-advanced HCC treated at our hospital between January 2024 and June 2025. The Ethics Committee reviewed the study protocol and specifically approved the waiver of informed consent prior to study initiation because only anonymized retrospective clinical data were analyzed and no additional patient intervention was involved.
Inclusion criteria were: 1) Pathologically or clinically diagnosed HCC according to the American Association for the Study of Liver Diseases/European Association for the Study of the Liver guidelines;17 2) Initially diagnosed as Barcelona Clinic Liver Cancer (BCLC) stage B or C; 3) Receiving first-line systemic therapy with LEN; 4) Having received at least one cycle of LEN with at least one post-baseline safety or efficacy assessment record; 5) Aged 18–80 years with complete clinical data. Exclusion criteria were: 1) Previous receipt of other systemic anti-cancer therapies (eg, chemotherapy, immunotherapy); 2) Concurrent other malignancies or severe psychiatric disorders; 3) Poor treatment adherence preventing accurate assessment of actual drug intake; 4) No follow-up data despite receiving treatment.
Based on treatment regimen, patients were divided into two groups: combined group (received standard LEN treatment combined with TCM decoction based on the Jianpi Rougan method) and monotherapy group (received standard LEN treatment alone without TCM). Basic clinical information, including demographics, liver function, tumor burden, and prior treatment history, was collected via the hospital information system (HIS), picture archiving and communication system (PACS), and laboratory information system (LIS). The study protocol was approved by The Second Affiliated Hospital of Zhejiang Chinese Medical University (Approval No. 2025–021-01) Ethics Committee, complying with the ethical principles of the Declaration of Helsinki. Due to the retrospective nature and absence of privacy disclosure risks, informed consent was waived. All data were anonymized before analysis.
The sample size calculation was based on the primary endpoint, LEN RDI. Referring to previous real-world data, the average RDI for patients with intermediate-to-advanced HCC on LEN monotherapy was approximately 65–70%, with a standard deviation (SD) of 20–25%.18 We hypothesized that the Jianpi Rougan decoction could improve tolerability, thereby increasing RDI. It was assumed that the mean RDI would be 70% in the monotherapy group and 80% in the combined group, with an overall SD of 20% for both groups. With a two-sided α = 0.05 and power (1-β) = 0.80, using PASS 15.0 software (NCSS, LLC. Kaysville, Utah, USA) for a two-sample t-test, the minimum required sample size was 64 per group. Considering the retrospective design and the planned use of propensity score matching (PSM, 1:1 matching, caliper = 0.02) to control for confounding baseline characteristics (eg, age, Child-Pugh grade, tumor burden), an estimated 10–15% sample loss was anticipated. To ensure sufficient statistical power post-matching and account for potential data loss, the target sample size was set at 152 patients. This sample size provides adequate power for the primary RDI analysis and allows exploratory analysis for secondary endpoints including toxicity-related discontinuation (assuming 25% in monotherapy group vs. < 10% in combined group).
Grouping and Treatment Regimens
Combined group (Jianpi Rougan method + LEN): Patients received standard LEN alongside a standardized TCM decoction based on the Jianpi Rougan method. The core formula was fixed: Atractylodes macrocephala (Baizhu) 15 g, Poria cocos (Fuling) 15 g, Paeonia lactiflora (Baishao) 12 g, Bupleurum chinense (Chaihu) 10 g, Angelica sinensis (Danggui) 10 g, and Curcuma aromatica (Yujin) 10 g. Limited, predefined modifications were allowed: For significant fatigue/poor appetite, Astragalus membranaceus (Huangqi) 15 g and Codonopsis pilosula (Dangshen) 15 g were added. For marked emotional depression/liver stagnation, Cyperus rotundus (Xiangfu) 10 g and Albizia julibrissin (Hehuanpi) 15 g were added. For damp-heat or elevated transaminases, Artemisia capillaris (Yinchen) 15 g and Gardenia jasminoides (Zhizi) 10 g were added. For pain or blood stasis signs, Salvia miltiorrhiza (Danshen) 15 g and Ligusticum chuanxiong (Chuanxiong) 10 g were added. A maximum of 1–2 modification categories were allowed per prescription. All decoctions were prepared uniformly by the hospital pharmacy: one dose daily, decocted to 200 mL, and taken twice daily. The TCM treatment duration required a minimum of 3 months or coverage of ≥ 50% of the LEN treatment period if < 3 months. Unplanned interruption exceeding 14 days led to exclusion from the combined group analysis.
Monotherapy group (LEN): Patients received standard-dose LEN only. The standard dose was 12 mg/day for body weight ≥ 60 kg and 8 mg/day for weight < 60 kg. Dose adjustments were permitted based on clinical response and AEs per physician’s judgment.
Data Collection and Variable Definitions
Data were collected retrospectively using a standardized case report form from HIS, LIS, and PACS. The variables included: 1) Demographics: age, gender, weight, body mass index (BMI), smoking/drinking history, and Eastern Cooperative Oncology Group (ECOG) performance status (PS; 0 = fully active to 5 = fully bedridden); 2) Liver function: alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin (TBIL), albumin (ALB), and Child-Pugh grade; 3) Tumor characteristics: maximum tumor diameter, tumor number, presence of portal vein tumor thrombus (PVTT), alpha-fetoprotein (AFP) level, and BCLC stage; 4) Prior treatment history: transarterial chemoembolization (TACE), ablation, or resection; 5) Treatment details: starting dose of LEN, treatment dates, dose adjustments, TCM usage (for combined group); 6) Safety: treatment-emergent AEs graded per the National Cancer Institute Common Terminology Criteria for AEs (NCI-CTCAE) version 5.0; 7) Short-term efficacy: objective response rate (ORR) and disease control rate (DCR) assessed radiologically per the modified Response Evaluation Criteria in Solid Tumors (mRECIST).
RDI
RDI was calculated as: RDI (%) = (actual cumulative dose received/planned cumulative dose) × 100%.19 The planned dose was 12 mg/day (≥ 60 kg) or 8 mg/day (< 60 kg). RDI was calculated for the first 8 weeks (early RDI), first 12 weeks, and the entire treatment period. Patients were categorized into high-intensity (RDI ≥80%) and low-intensity (RDI <80%) groups. The threshold of RDI ≥80% was selected because maintenance of this level of dose intensity has been associated with improved clinical outcomes in patients receiving lenvatinib therapy. The 8-week and 12-week time points were chosen because early dose intensity during the first 2–3 months of treatment has been reported to be predictive of subsequent treatment response and treatment continuation.20
Toxicity-Related Treatment Discontinuation Rate
Toxicity-related treatment discontinuation rate was defined as the proportion of patients permanently discontinuing LEN due to treatment-related AEs.21 The focus was on discontinuations due to severe AEs (eg, hypertension, diarrhea).
Safety and Tolerability
All AEs were recorded and graded per the NCI-CTCAE v5.0.22 The incidence of grade ≥ 3 AEs (eg, severe hypertension, diarrhea, hand-foot syndrome) was analyzed to assess tolerability differences.
Short-Term Efficacy Evaluation
Efficacy was assessed by imaging at 3–6 months post-treatment using the mRECIST.23 Responses were categorized as complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD). ORR (CR + PR) and DCR (CR + PR + SD) were calculated.
Statistical Analysis
All statistical analyses were performed using R software (version 4.3.2; R Foundation for Statistical Computing, Vienna, Austria). Propensity score matching was conducted using the MatchIt package (version 4.7.0), and covariate balance was assessed using the cobalt package (version 4.6.0). Continuous variables were presented as mean ± standard deviation or median (interquartile range) based on distribution. Categorical variables were presented as number (percentage). Group comparisons used appropriate parametric or non-parametric tests. To reduce confounding bias from baseline differences inherent to real-world studies, PSM was employed. A multivariate logistic regression model calculated PS, followed by 1:1 nearest neighbor matching. The standardized mean difference (SMD) was used to evaluate covariate balance, and SMD < 0.10 indicated good balance post-matching, visualized via Love plots. In the matched cohort, continuous outcomes were compared using paired tests, binary outcomes were compared with paired contingency analyses, and time-to-event outcomes were estimated via the Kaplan-Meier method. All tests were two-sided, with P < 0.05 considered statistically significant.
Results
Patient Disposition and Baseline Characteristics
A total of 172 patients were screened, and 20 were excluded (10 failed the inclusion/exclusion criteria, 6 had missing key data, 4 other reasons). The original cohort comprised 152 patients (combined group: n = 73; monotherapy group: n = 79). After PSM [1:1 nearest neighbor matching on logit(PS) with caliper restriction] balancing age, gender, BMI, smoking/drinking history, ALT, AST, TBIL, ALB, Child-Pugh grade, maximum tumor diameter, tumor number, PVTT, AFP, BCLC stage, and prior treatments (TACE, ablation, surgery), 65 matched pairs (n = 130) were obtained. Post-matching, covariate balance improved markedly, with most SMDs below 0.10 (Love plot, Figure 1), indicating good comparability. Baseline characteristics before and after PSM are shown in Tables 1 and 2.
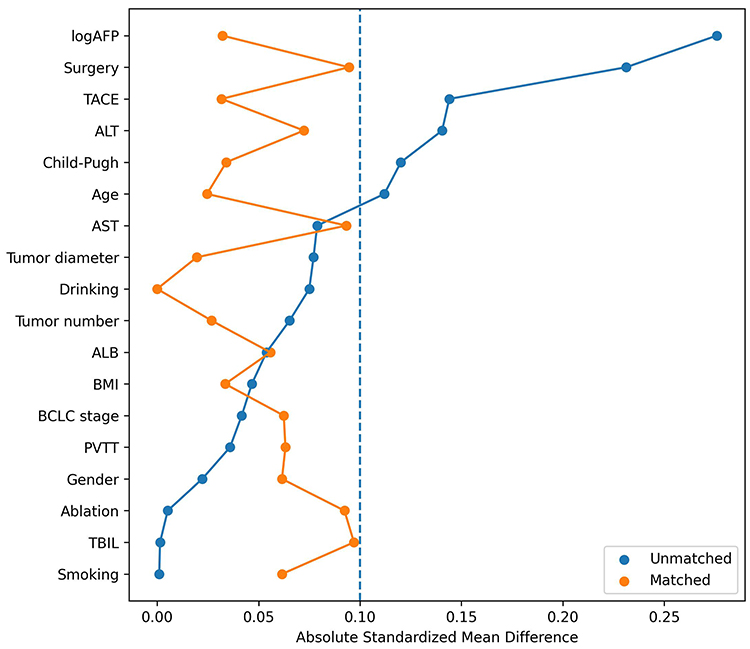 |
Figure 1 Love plot showing covariate balance before and after PSM. Abbreviation: PSM, propensity score matching. |
Comparison of LEN RDI
In the matched cohort, the combined group demonstrated significantly better dose maintenance capability (Figure 2 and Table 3). Both early (8-week) and 12-week RDI were significantly higher in the combined group, as was the overall RDI. The rate of achieving RDI ≥ 80% within 12 weeks was significantly higher in the combined group (P = 0.029). Regarding dose adjustments, the combined group had lower rates of both dose reductions and dose interruptions (P = 0.022 and P = 0.045, respectively), suggesting a potential association between Jianpi Rougan therapy and improved treatment sustainability.
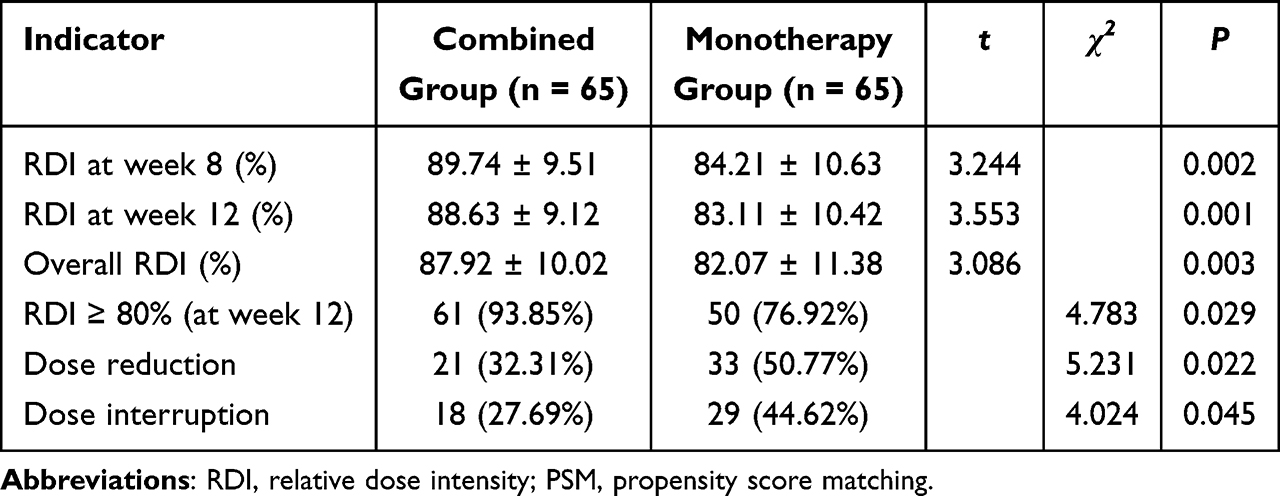 |
Table 3 Comparison of RDI and Dose Adjustments (Post-PSM) |
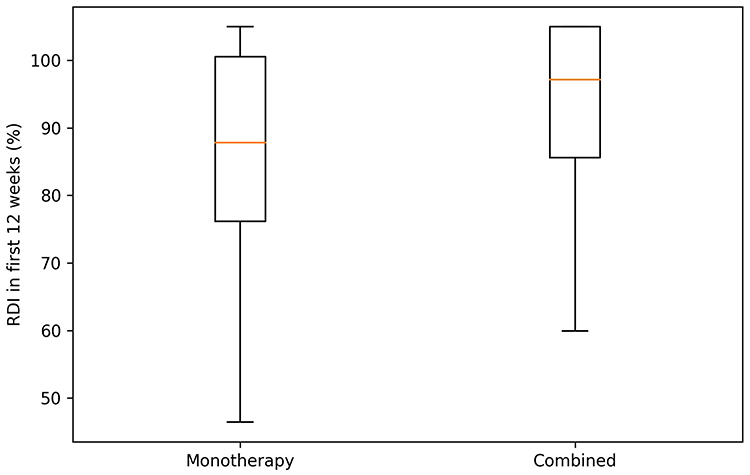 |
Figure 2 Comparison of LEN RDI distribution in first 12 weeks between groups after PSM. Abbreviations: LEN, lenvatinib; RDI, relative dose intensity; PSM, propensity score matching. |
Treatment Discontinuation and Time to Treatment Failure (TTF)
Permanent discontinuation rate due to AEs was significantly lower in the combined group (P = 0.021). Discontinuation rate due to disease progression was also lower (P = 0.044). The overall discontinuation rate was significantly reduced in the combined group (P = 0.034) (Table 4). TTF was longer in the combined group (5.33 ± 2.14 months vs. 4.58 ± 2.08 months, P = 0.042). Kaplan-Meier curves showed a higher probability of remaining on treatment in the combined group (Figure 3).
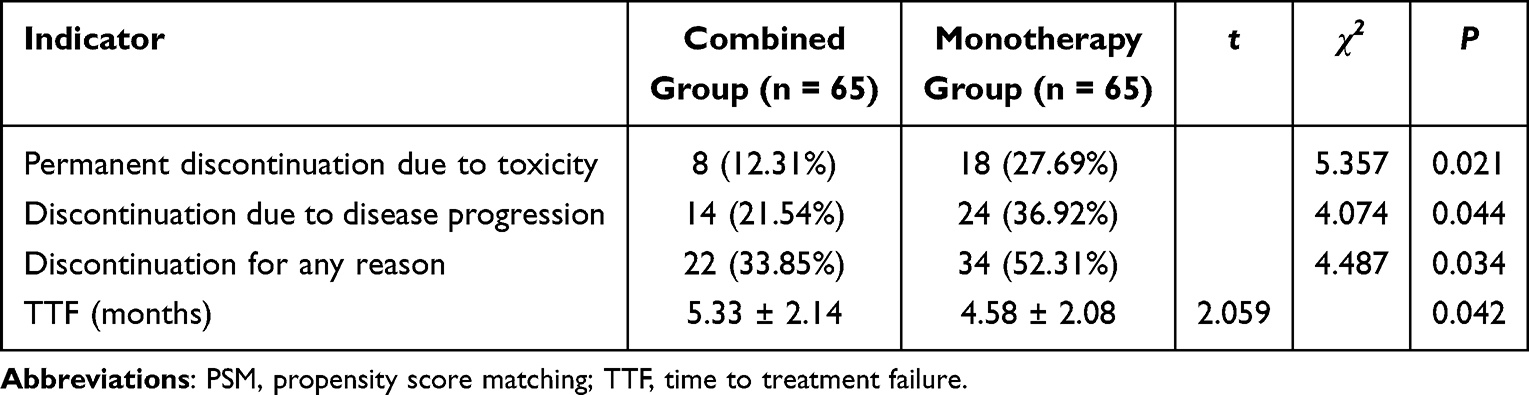 |
Table 4 Treatment Discontinuation and Duration (Post-PSM) |
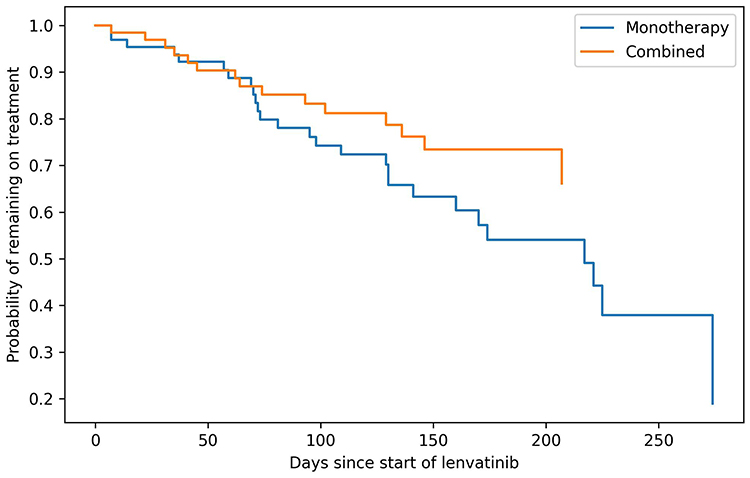 |
Figure 3 Kaplan-Meier curves for treatment continuation in the matched cohorts. |
Safety and AEs
The overall incidence of AEs of any grade did not differ significantly between the groups. Regarding symptoms more relevant to the Jianpi Rougan theory, the incidence of decreased appetite was significantly lower in the combined group (P = 0.036), with trends towards lower rates of diarrhea and elevated transaminases. No significant difference was observed in grade ≥ 3 AEs (Table 5). Typical AEs for targeted therapy (eg, hypertension, hand-foot syndrome) showed no significant inter-group differences.
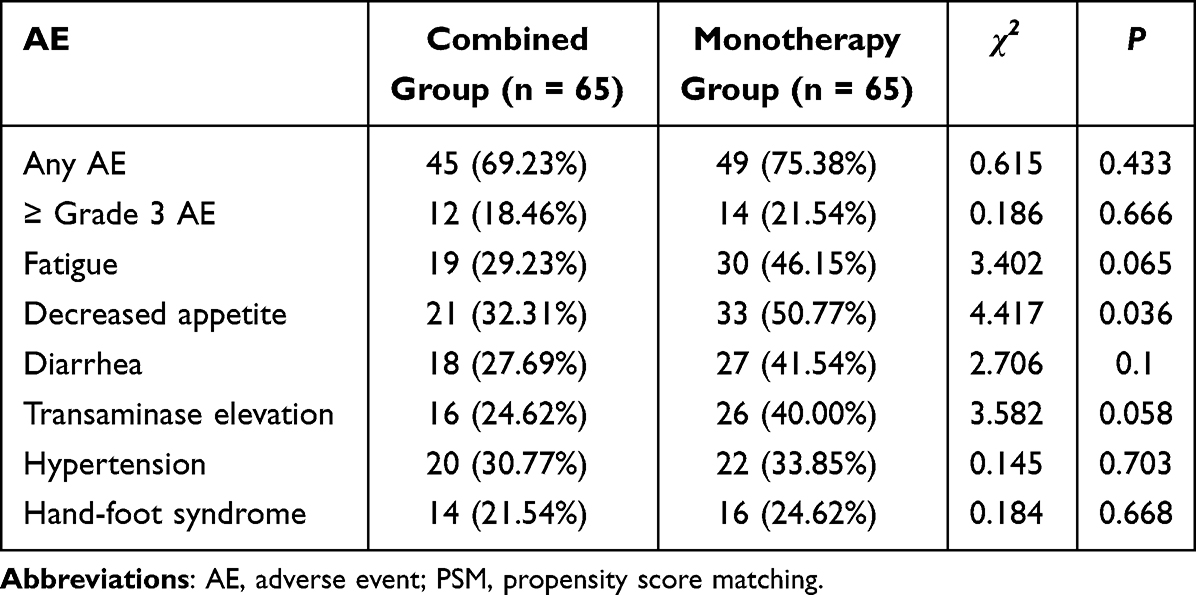 |
Table 5 Comparison of AEs (Post-PSM) |
Tumor Response and Radiological Changes
In the matched cohort, both ORR and DCR were numerically higher in the combined group, but the differences were not statistically significant (P > 0.05). The distribution of best response (CR/PR/SD/PD) is shown in Table 6, with no significant overall distribution difference (P > 0.05). A waterfall plot suggested a greater overall magnitude of tumor shrinkage in the combined group (Figure 4).
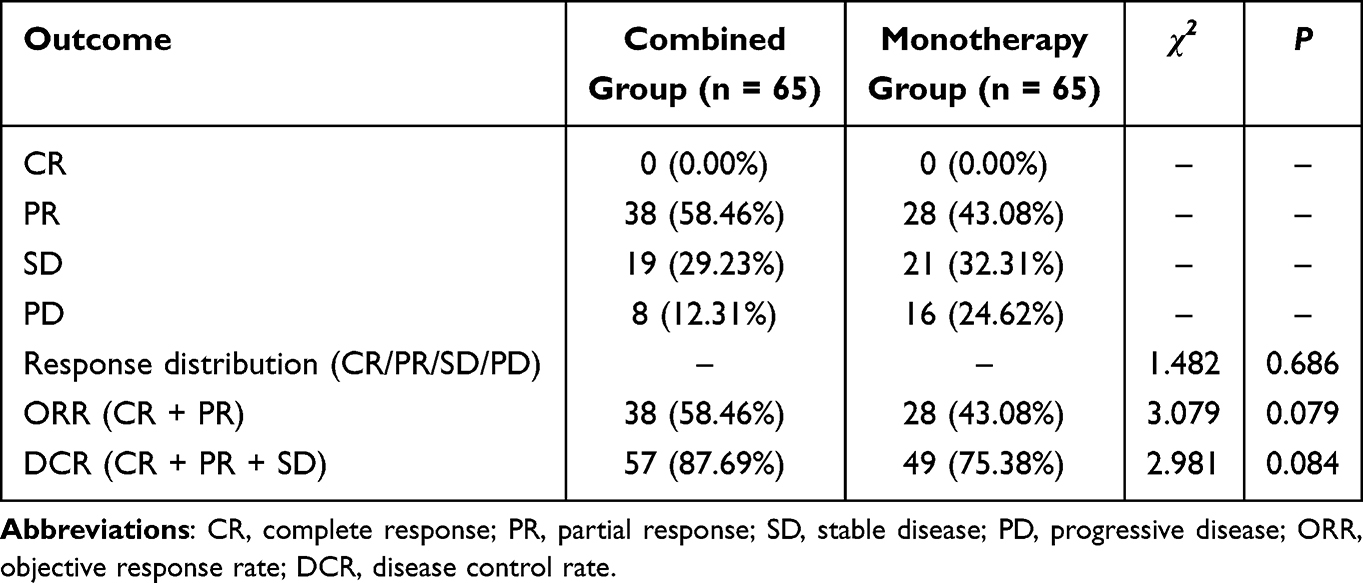 |
Table 6 Tumor Response and Short-Term Efficacy in the Matched Cohort |
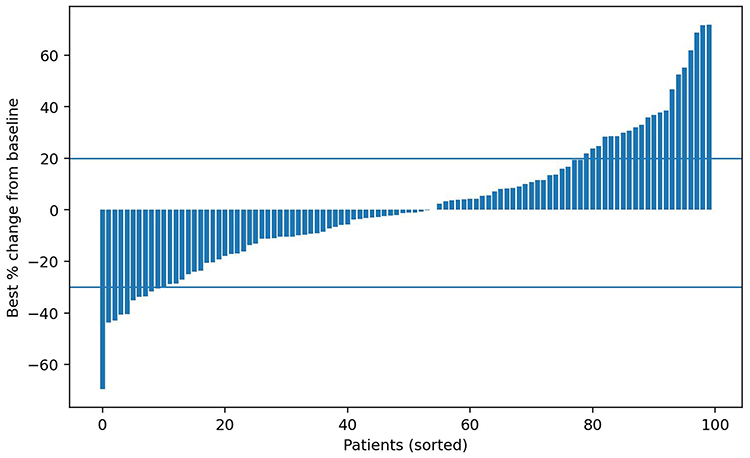 |
Figure 4 Waterfall plot showing changes in maximum tumor diameter for patients in the matched cohort after PSM. Abbreviation: PSM, propensity score matching. |
Discussion
With targeted therapy becoming a cornerstone of systemic treatment for intermediate-to-advanced HCC, maintaining treatment continuity and adequate dose intensity in real-world practice has emerged as a critical determinant of therapeutic benefit. This real-world retrospective cohort study systematically evaluated the impact of the Jianpi Rougan method combined with LEN on treatment sustainability. After PSM balancing key baseline characteristics, the results showed the combined group had significantly higher RDI at weeks 8, 12, and overall, along with a higher proportion achieving RDI ≥ 80%. Concurrently, the combined group had a significantly lower rate of permanent discontinuation due to toxicity and exhibited longer treatment duration. These findings provide direct evidence of the real-world value of the Jianpi Rougan method in supporting targeted therapy from two dimensions: receiving adequate dose and remaining on treatment longer.
Previous studies have confirmed the correlation between LEN efficacy and dose intensity. The REFLECT trial and subsequent real-world analyses indicate that early RDI decline is associated with shorter PFS and OS.24 Some cohort studies further found that patients maintaining RDI ≥ 80% during the first 8–12 weeks achieved more durable disease control and better survival outcomes.25 Notably, our study showed that the combined group maintained higher RDI without increasing severe AE rates; instead, it significantly reduced symptoms including fatigue, appetite loss, and transaminase elevation. These findings suggest a potential association between Jianpi Rougan therapy and improved dose maintenance capacity without an apparent increase in severe adverse events, aligning with existing evidence that RDI is a key determinant of real-world benefit from targeted therapy.26
From a TCM theoretical perspective, HCC patients often present with a pattern of deficiency in origin and excess in manifestation, with liver stagnation and spleen deficiency. Tumor burden, impaired liver function, and long-term targeted therapy further weaken spleen transportation and liver dispersion. The Jianpi Rougan formula, with core herbs such as Atractylodes macrocephala, Poria cocos, Paeonia lactiflora, and Bupleurum chinense, addresses both strengthening healthy Qi and relieving stagnation. It may improve spleen deficiency symptoms including poor appetite and fatigue, while alleviating emotional depression and liver Qi stagnation. Previous integrative medicine studies suggest spleen-fortifying formulas may mitigate gastrointestinal toxicity from chemotherapy or targeted therapy by improving gastrointestinal motility, enhancing nutrient absorption, modulating gut microbiota, and reducing inflammation.27 Liver-soothing and dispersion-regulating herbs might alleviate hepatocyte injury and transaminase elevation by modulating the hypothalamic-pituitary-adrenal axis, improving stress response, and enhancing hepatic microcirculation.28 Compared to monotherapy, the combination with TCM intervention showed more significant benefits for AEs closely related to spleen deficiency and liver stagnation (fatigue, appetite loss, liver enzyme abnormalities), while its impact on specific targeted therapy toxicities like hypertension and hand-foot syndrome was relatively limited. This pattern of selective improvement aligns with the core feature of TCM syndrome differentiation and treatment. Rather than directly counteracting drug toxicity, TCM focuses on supporting healthy Qi, restoring balance, and improving the internal milieu,29 which lends theoretical plausibility to its potential mechanism.
Regarding short-term efficacy, although ORR and DCR showed upward trends in the combined group, they did not reach statistical significance. This finding is consistent with some integrative medicine studies reporting limited differences in short-term radiological response, with potential benefits for long-term outcomes.30 Considering the limited sample size, short follow-up, and primary focus on treatment sustainability rather than survival endpoints in this study, these trends may indicate that the dose maintenance advantage has not yet fully translated into measurable radiological benefit. Notably, the waterfall plot suggested a greater overall magnitude of tumor shrinkage in the combined group, implying that with longer follow-up or larger samples, higher RDI might translate into clearer efficacy and survival advantages, consistent with the established chain of RDI-efficacy-survival relationships.20
This study still has several limitations. First, the retrospective design inherently carries selection bias and unmeasured confounding factors. Although PSM was used, it cannot fully replace prospective randomized controlled trials. Second, sample size and follow-up duration limited the assessment of hard endpoints such as OS and PFS. Third, the allowance for herbal prescription modifications based on syndrome differentiation, while reflecting real-world practice, introduced intervention heterogeneity, making it difficult to quantify the independent effect of individual components precisely. Furthermore, mechanistic investigations, including pharmacological experiments and biomarker-based studies, were beyond the scope of the present study and warrant further exploration in future research. Therefore, future multicenter prospective randomized controlled trials involving larger and more diverse populations are warranted to further validate these findings and improve their generalizability. Although predefined modification rules were applied, the individualized adjustment of herbal prescriptions may still have introduced a degree of intervention heterogeneity.
Conclusion
The combination of the Jianpi Rougan method with LEN was associated with higher dose maintenance capacity and lower rates of toxicity-related treatment discontinuation in this real-world cohort. Its effects align closely with previous research evidence indicating that RDI determines the real-world benefit of targeted therapy. The observed association between Jianpi Rougan therapy and improved treatment sustainability may be partly attributable to its potential effects on spleen/stomach function, hepatic stress adaptation, and systemic tolerability. It offers a biologically plausible and clinically feasible integrative Chinese and Western medicine approach for systemic treatment of intermediate-to-advanced HCC. Future prospective, multicenter randomized studies are warranted to further validate its impact on survival outcomes and define the optimal intervention model.
Data Sharing Statement
The data used and/or analyzed during the current study are available from the corresponding author.
Ethics Approval
This study was approved by the Ethics Committee of The Second Affiliated Hospital of Zhejiang Chinese Medical University (Approval No. 2025-021-01) and was conducted in accordance with the ethical principles of the Declaration of Helsinki. The Ethics Committee reviewed and approved the waiver of informed consent. Owing to the retrospective nature of the study, minimal risk to participants, and the use of anonymized clinical data, written informed consent was waived.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflict of interest.
References
1. Vogel A, Meyer T, Sapisochin G, Salem R, Saborowski A. Hepatocellular carcinoma. Lancet. 2022;400(10360):1345–12. doi:10.1016/s0140-6736(22)01200-4
2. Ganesan P, Kulik LM. Hepatocellular carcinoma: new developments. Clin Liver Dis. 2023;27(1):85–102. doi:10.1016/j.cld.2022.08.004
3. Sensi B, Angelico R, Toti L, et al. Mechanism, potential, and concerns of immunotherapy for hepatocellular carcinoma and liver transplantation. Curr Mol Pharmacol. 2024;17:e18761429310703. doi:10.2174/0118761429310703240823045808
4. Xu W, Liao S, Hu Y, Huang Y, Zhou J. Upregulation of miR-3130-5p enhances hepatocellular carcinoma growth by suppressing ferredoxin 1: miR-3130-5p enhances HCC growth via inhibiting FDX1. Curr Mol Pharmacol. 2024;17:e18761429358008. doi:10.2174/0118761429358008250305070518
5. Gudivada IP, Amajala KC. Integrative bioinformatics analysis for targeting hub genes in hepatocellular carcinoma treatment. Curr Genom. 2025;26(1):48–80. doi:10.2174/0113892029308243240709073945
6. Wu Y, Sun R, Ren S, Zengin G, Li M. Neuronal reshaping of the tumor microenvironment in tumorigenesis and metastasis: bench to clinic. Med Adv. 2025;3(4):364–371. doi:10.1002/med4.70044
7. Li Y, Kang Z, Du Y. Beyond PD-1/PD-L1: new immune checkpoints and therapeutic combinations in cancer immunotherapy. Med Bull. 2026;2(1):61–93. doi:10.1002/mdb2.70018
8. Franzè MS, Saffioti F, Mavroeidis VK. Interactions between tumor microenvironment and resistance to transarterial and systemic treatments for HCC. Cancer Drug Resistance. 2025;8:33. doi:10.20517/cdr.2024.212
9. Qin Y, Han S, Yu Y, et al. Lenvatinib in hepatocellular carcinoma: resistance mechanisms and strategies for improved efficacy. Liver Int. 2024;44(8):1808–1831. doi:10.1111/liv.15953
10. Motzer RJ, Taylor MH, Evans TRJ, et al. Lenvatinib dose, efficacy, and safety in the treatment of multiple malignancies. Expert Rev Anticancer Ther. 2022;22(4):383–400. doi:10.1080/14737140.2022.2039123
11. Chen Y, Dai S, Cheng CS, Chen L. Lenvatinib and immune-checkpoint inhibitors in hepatocellular carcinoma: mechanistic insights, clinical efficacy, and future perspectives. J Hematol Oncol. 2024;17(1):130. doi:10.1186/s13045-024-01647-1
12. Huang M, Long J, Yao Z, et al. METTL1-mediated m7G tRNA modification promotes lenvatinib resistance in hepatocellular carcinoma. Cancer Res. 2023;83(1):89–102. doi:10.1158/0008-5472.Can-22-0963
13. Shayne M, Harvey RD, Lyman GH. Prophylaxis and treatment strategies for optimizing chemotherapy relative dose intensity. Expert Rev Anticancer Ther. 2021;21(10):1145–1159. doi:10.1080/14737140.2021.1941891
14. Nielson CM, Bylsma LC, Fryzek JP, Saad HA, Crawford J. Relative dose intensity of chemotherapy and survival in patients with advanced stage solid tumor cancer: a systematic review and meta-analysis. Oncologist. 2021;26(9):e1609–e1618. doi:10.1002/onco.13822
15. Liu Z, Zhang T, Xue CM, Zhang WT, Zhu BC, Hua GD. Research hotspots of traditional chinese medicine for liver cancer in the future directions: a bibliometric analysis. J Hepatocell Carcinoma. 2025;12:3105–3161. doi:10.2147/jhc.S555310
16. Lu CL, Li X, Zhou HM, et al. Traditional Chinese medicine in cancer care: an overview of 5834 randomized controlled trials published in Chinese. Integr Cancer Ther. 2021;20:15347354211031650. doi:10.1177/15347354211031650
17. Lee YT, Wang JJ, Zhu Y, Agopian VG, Tseng HR, Yang JD. Diagnostic criteria and LI-RADS for hepatocellular carcinoma. Clin Liver Dis. 2021;17(6):409–413. doi:10.1002/cld.1075
18. Kirino S, Tsuchiya K, Kurosaki M, et al. Relative dose intensity over the first four weeks of lenvatinib therapy is a factor of favorable response and overall survival in patients with unresectable hepatocellular carcinoma. PLoS One. 2020;15(4):e0231828. doi:10.1371/journal.pone.0231828
19. Levin L, Hryniuk WM. Dose intensity analysis of chemotherapy regimens in ovarian carcinoma. J Clin Oncol. 1987;5(5):756–767. doi:10.1200/jco.1987.5.5.756
20. Tokunaga T, Tateyama M, Tanaka K, et al. Optimal management of lenvatinib therapy for patients with unresectable hepatocellular carcinoma by balancing the therapeutic effect with the relative dose intensity. Hepatol Res. 2022;52(1):105–119. doi:10.1111/hepr.13720
21. Okusaka T, Ikeda K, Kudo M, et al. Safety and efficacy of lenvatinib by starting dose based on body weight in patients with unresectable hepatocellular carcinoma in REFLECT. J Gastroenterol. 2021;56(6):570–580. doi:10.1007/s00535-021-01785-0
22. Freites-Martinez A, Santana N, Arias-Santiago S, Viera A. Using the common terminology criteria for adverse events (CTCAE - Version 5.0) to evaluate the severity of adverse events of anticancer therapies. Actas Dermo-Sifiliograficas. 2021;112(1):90–92. doi:10.1016/j.ad.2019.05.009
23. Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30(1):52–60. doi:10.1055/s-0030-1247132
24. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised Phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173. doi:10.1016/s0140-6736(18)30207-1
25. Takahashi A, Moriguchi M, Seko Y, et al. Impact of relative dose intensity of early-phase lenvatinib treatment on therapeutic response in hepatocellular carcinoma. Anticancer Res. 2019;39(9):5149–5156. doi:10.21873/anticanres.13710
26. Kimura M, Yamada S, Go M, Yasuda S, Toyoda H, Usami E. Identifying risk factors of dose reduction or treatment discontinuation due to fatigue or gastrointestinal symptoms in patients receiving lenvatinib treatment for hepatocellular carcinoma. J Oncol Pharm Pract. 2026;32(1):24–31. doi:10.1177/10781552241281900
27. Liao X, Bu Y, Jia Q. Traditional Chinese medicine as supportive care for the management of liver cancer: Past, present, and future. Genes Dis. 2020;7(3):370–379. doi:10.1016/j.gendis.2019.10.016
28. Lv S, Zhao Y, Wang L, et al. Antidepressant active components of Bupleurum chinense DC-Paeonia lactiflora Pall herb pair: pharmacological mechanisms. Biomed Res Int. 2022;2022:1–15. doi:10.1155/2022/1024693
29. Latte-Naor S, Mao JJ. Putting integrative oncology into practice: concepts and approaches. J Oncol Pract. 2019;15(1):7–14. doi:10.1200/jop.18.00554
30. Yan H, Li Y, Guo B, Yang B, Tang D. The effect of Traditional Chinese Medicine on patients undergoing targeted therapy for primary liver cancer: a systematic review and meta-analysis. Front Oncol. 2025;15. doi:10.3389/fonc.2025.1674965
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Population Sensitive to Lenvatinib Plus Anti-PD-1 for Unresectable Hepatocellular Carcinoma Infected with Hepatitis B Virus

Chang X, Yu S, Pang J, Zhang W, Kong H, Huang J, Zhang G, Zhang H, Gu Y, Chen Y, Yang B, Liu J, Zeng Z
Journal of Hepatocellular Carcinoma 2023, 10:847-861
Published Date: 6 June 2023