Back to Journals » Nature and Science of Sleep » Volume 14
Is There a Place for Medicinal Cannabis in Treating Patients with Sleep Disorders? What We Know so Far
Authors Maddison KJ, Kosky C, Walsh JH ![]()
Received 1 March 2022
Accepted for publication 6 May 2022
Published 18 May 2022 Volume 2022:14 Pages 957—968
DOI https://doi.org/10.2147/NSS.S340949
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Kathleen J Maddison,1,2 Christopher Kosky,1 Jennifer H Walsh1,2
1West Australian Sleep Disorders Research Institute, Department of Pulmonary Physiology & Sleep Medicine, Sir Charles Gairdner Hospital, Perth, Western Australia, Australia; 2Centre for Sleep Science, University of Western Australia, Perth, Western Australia, Australia
Correspondence: Jennifer H Walsh, West Australian Sleep Disorders Research Institute, Department of Pulmonary Physiology & Sleep Medicine, Sir Charles Gairdner Hospital, Internal Mailbox 201, QEII Medical Centre, Hospital Avenue, Nedlands, Perth, Western Australia, 6009, Australia, Tel +61 6488 8694, Email [email protected]
Abstract: The legalization of cannabis for medicinal, and in some countries, recreational, purposes in addition to growth in the cannabis industry has meant that cannabis use and interest in the area has increased rapidly over the past 20 years. Treatment of poor sleep and sleep disorders are two of the most common reasons for the current use of medicinal cannabis. However, evidence for the role of medical cannabis in the treatment of sleep disorders has not been clearly established, thus making it challenging for clinicians to make evidence-based decisions regarding efficacy and safety. This narrative review summarizes the highest quality clinical evidence currently available in relation to the use of medicinal cannabis for the treatment of sleep disorders including insomnia, obstructive sleep apnea, restless legs syndrome, rapid eye movement sleep behavior disorder, nightmare disorder and narcolepsy. A summary of the effect of cannabis on sleep quality and architecture is also presented. Currently, there is insufficient evidence to support the routine use of medicinal cannabis as an effective and safe treatment option for any sleep disorder. Nevertheless, emerging evidence is promising and warrants further investigation using standardized cannabinoid products and validated quantitative measurement techniques.
Keywords: cannabinoid, insomnia, obstructive sleep apnea, restless legs syndrome, REM behavior disorder, nightmare disorder
Introduction
Healthy sleep is essential for physical, mental and emotional health. However, only 50% of the population report achieving regular adequate sleep.1 Causes of inadequate sleep include work, family disruptors, lifestyle choices and untreated sleep disorders. Many of the treatment options for sleep disorders are imperfect due to poor adherence, tolerance or side effects. Treatment alternatives are therefore required.
Cannabis has been utilized for its various intoxicating and medicinal effects for thousands of years.2 However, our scientific understanding of its constituents and mechanisms of action has only begun to develop in the past 60 years. Fueled by the legalization of cannabis for medicinal use in the US, and other countries, from the 1990s there has been an explosion of research in the area. We now understand that the cannabis plant is comprised of over 500 phytochemicals including more than 100 phytocannabinoids (colloquially referred to as cannabinoids), the most well recognized and extensively studied being ∆9-tetrahydrocannabinol (THC), cannabidiol (CBD) and cannabinol (CBN). With the upsurge in research into naturally occurring phytocannabinoids, synthetic phytocannabinoids have been manufactured for medicinal use as analogues to THC (dronabinol, nabilone), CBD or a combination of THC and CBD (nabiximols). We also understand that phytocannabinoids as well as endogenous cannabinoids (endocannabinoids) work within the endocannabinoid system and activate cannabinoid receptors type 1 (CB1) and type 2 (CB2), predominantly located in the central nervous system. Also important are the enzymes responsible for synthesis and degradation of endocannabinoids. Pre-clinical work has established a number of potential molecular mechanisms for the role of cannabinoids in moderating sleep and wake and has been reviewed elsewhere.3–5
Historically, the intoxicating effect of THC has driven the recreational use of cannabis, whereas the non-intoxicating CBD has been promoted as a health aid. There is also evidence that CBD and CBN can moderate the intoxicating and psychological effects of THC.6 In this rapidly advancing field, we now also understand that each cannabinoid can induce different therapeutic effects, which include anxiolytic, antiemetic, anticonvulsant, appetite stimulating, appetite suppressing, antispasmodic, anti-inflammatory, antioxidant, analgesic and sedating. The most common self-reported medical reasons for using cannabinoids are to treat pain, mental health, and sleep problems.7 In Australia, where prescriptions are required to legally access cannabis products for medicinal purposes, the number of applications for access to medicinal cannabis products has increased exponentially since legalization in 2016: 15 applications were submitted in 2016; 2560 in 2018; and 122,4900 in 2021. In 2022, “insomnia” and “sleep disorders” were the third and fourth most common reasons for prescription.8 Despite this increasing use of cannabis products for the treatment of sleep disorders, evidence for its benefit has been limited. This narrative review summarizes the current clinical evidence base for the effect of cannabinoids on sleep quantity and quality and the therapeutic use of cannabinoids in the treatment of sleep disorders. A discussion on the challenges to the field and recommendations for advancing our understanding will also be provided.
Search Methodology
Online databases PubMed, Web of Science, Google Scholar and Scopus were searched between Jan and Feb 2022 using terms including cannabis, THC, tetrahydrocannabinol, cannabinol, CBD, sleep, sleep disorder, insomnia, sleep apnea, restless legs syndrome, REM behavior disorder, nightmare, and narcolepsy. As the review was focused on the utility of cannabis for clinical use, the search was limited to clinical research, except in the cases of obstructive sleep apnea, narcolepsy and idiopathic hypersomnia where some preclinical data is discussed.
Effect of Cannabinoids on Sleep and Sleep Architecture
For several reasons, the effect of cannabinoids on sleep is challenging to summarize. Many studies specifically recruited participants with a history of chronic or heavy recreational cannabis use,9–14 who appear to have poorer sleep compared to non-users.15,16 Therefore, baseline or placebo data in these participants may be a reflection of sleep architecture associated with withdrawal, which can be significant.17–19 Also challenging for isolating effects of specific cannabinoids is that a number of studies have examined the effects of smoking or consuming whole cannabis/flower with unknown cannabinoid concentrations.17,19–21 Another issue is that many studies have investigated the effects of cannabinoids on sleep in populations with health ailments12,22–24 or sleep disorders,25,26 which are likely to confound effects on sleep outcomes. Finally, as highlighted in recent reviews,27–29 the overwhelming majority of studies have employed self-report measures of sleep quantity and quality, with only a handful of predominantly early studies including robust measures of sleep and sleep architecture from electroencephalography or polysomnography (PSG). Therefore, this section of the review focuses on controlled, cross-over design studies that have included predominantly non-experienced cannabis users and objective measures of sleep quality and architecture (Table 1).19,30–33 The majority of studies have focused on the effects of a THC dominant cannabinoid formulation,19,30–32 although one study investigated the effects of THC alone as well as two doses of a balanced THC:CBD formulation.31 Another study investigated the effects of CBD alone.33
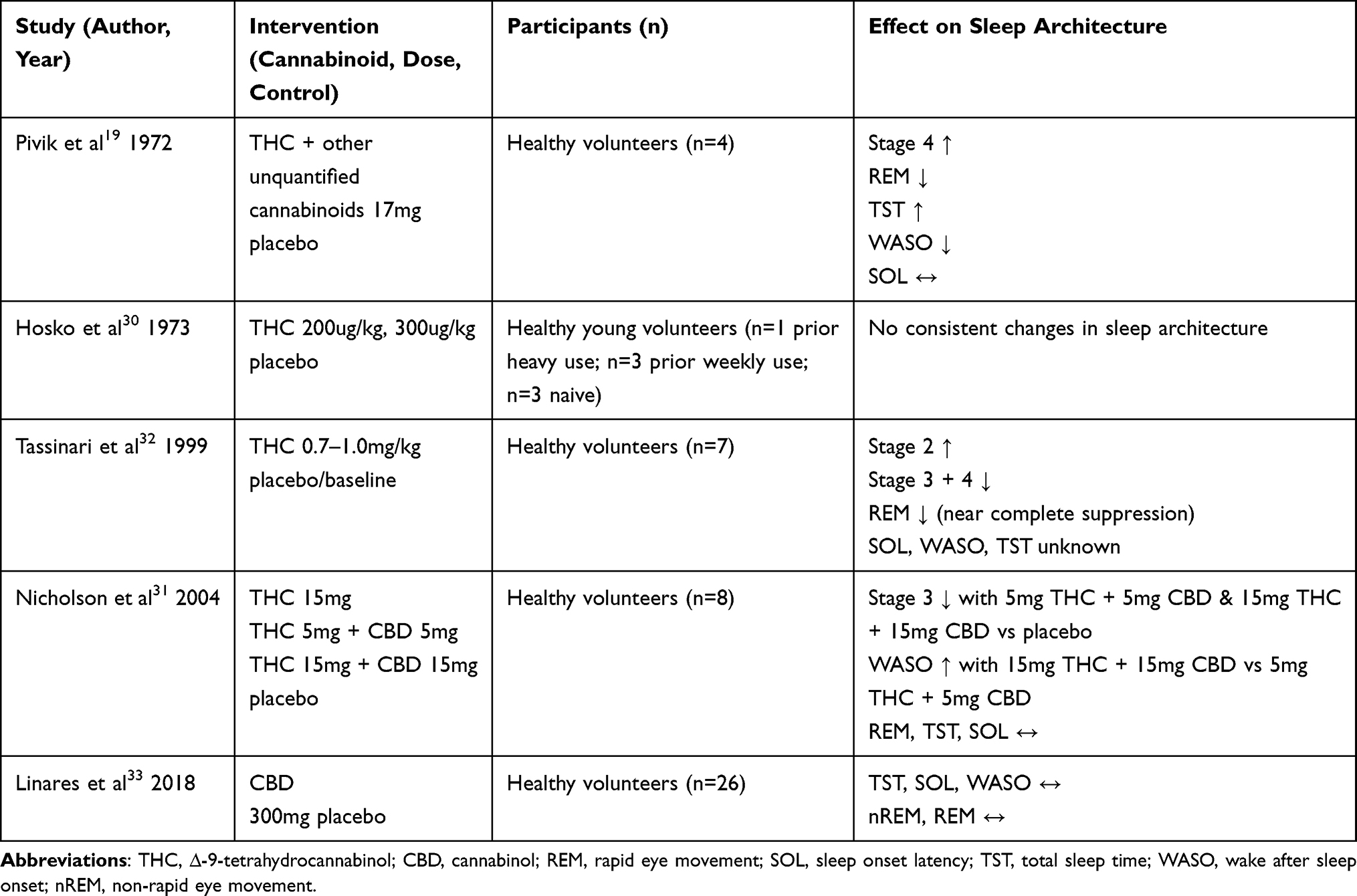 |
Table 1 Trials Evaluating the Effect of Cannabinoids on Sleep Architecture |
The largest and most recent study on effects of cannabinoids on sleep, by Linares et al, identified no change in any measure of sleep quantity or architecture when 27 healthy young volunteers took a single 300mg dose of CBD compared to placebo.33 Of studies which included THC, in regard to the putative sedating properties of cannabinoids, none identified an improvement in the time taken to fall asleep (sleep onset latency; SOL) although one study19 (n = 6) reported a reduction in wake time after sleep onset (WASO) and another (n = 8) reported a slight decrease in WASO when a 5mg balanced THC:CBD formation was taken, and an increase in WASO when a 15mg balanced THC:CBD formation was taken, resulting in a significant difference between doses.31 Only one study reported an increase in total sleep time (TST).19 Two studies reported a reduction in Stage 3 and/or Stage 4 sleep31,32 while another reported an increase.19 Perhaps more consistent is the data indicating that rapid eye movement (REM) sleep is reduced when taking THC; two studies identified a reduction19 or near complete suppression,32 albeit at a very high dose of 0.7–1.0mg/kg in the case of REM suppression. Two other studies reported no significant effect of THC on REM.31,33
On balance, it is apparent from the limited data in healthy, predominantly cannabis naïve participants, that the evidence in relation to the effect of cannabinoids on sleep quality is mixed and more well-controlled studies of individual and combined cannabinoids in broad and refined populations are required. Consideration should also be given to the impact of the method of data collection on the sleep variables being quantified. Trials of larger populations with reliable home-based, or less intrusive, monitoring over several nights are needed before we can confidently establish the true effects of cannabinoids on sleep quality and architecture. Further to this, effects of varying methods of delivery (smoked/vaporized versus oral consumption) should also be examined as the pharmacokinetics differ significantly with route of delivery.34 Finally, studies of acute versus chronic effects as well as withdrawal from use at doses that are relevant to therapeutic use are also needed.
Insomnia
Insomnia is typically defined as difficulty with sleep initiation or maintenance despite opportunity, with subsequent impairment in daytime function. In the case of chronic insomnia, present in up to 15% of the population,35,36 these symptoms occur at least three times per week and last for at least three months.37,38 Chronic insomnia is best treated with cognitive behavioral therapy for insomnia, although it is not always effective and access to treatment is limited in most countries. Pharmacological therapies are therefore often used and also have an important role when there is a short-term need. However, many conventional pharmacological therapies have common and undesirable side effects including daytime sedation and cognitive impairment, dependence, tolerance and abuse potential. Cannabis products are emerging as a potential alternative therapy for insomnia. Indeed, insomnia, or the lesser-defined “poor sleep,” is one of the most common reasons for using and prescribing medicinal cannabis.7,39 However, there is surprisingly little empirical data for the use of cannabinoids in the treatment of these conditions. Although many studies have examined the efficacy of cannabinoids on sleep parameters as a secondary outcome in patients with pain or other conditions,40 the majority have limited capacity to detect improvements in sleep as participants were not selected based on the presence of poor sleep, thereby creating a potential ceiling effect. A number of studies and case series are also limited by the lack of blinding or a control condition. This section of the review will focus on blinded, randomized, controlled studies that have assessed changes in sleep as a primary outcome in response to cannabinoid therapies in a population presenting with poor sleep or insomnia, either in the presence of another medical condition or not (Table 2). Sleep disorders secondary to cannabis withdrawal were excluded.
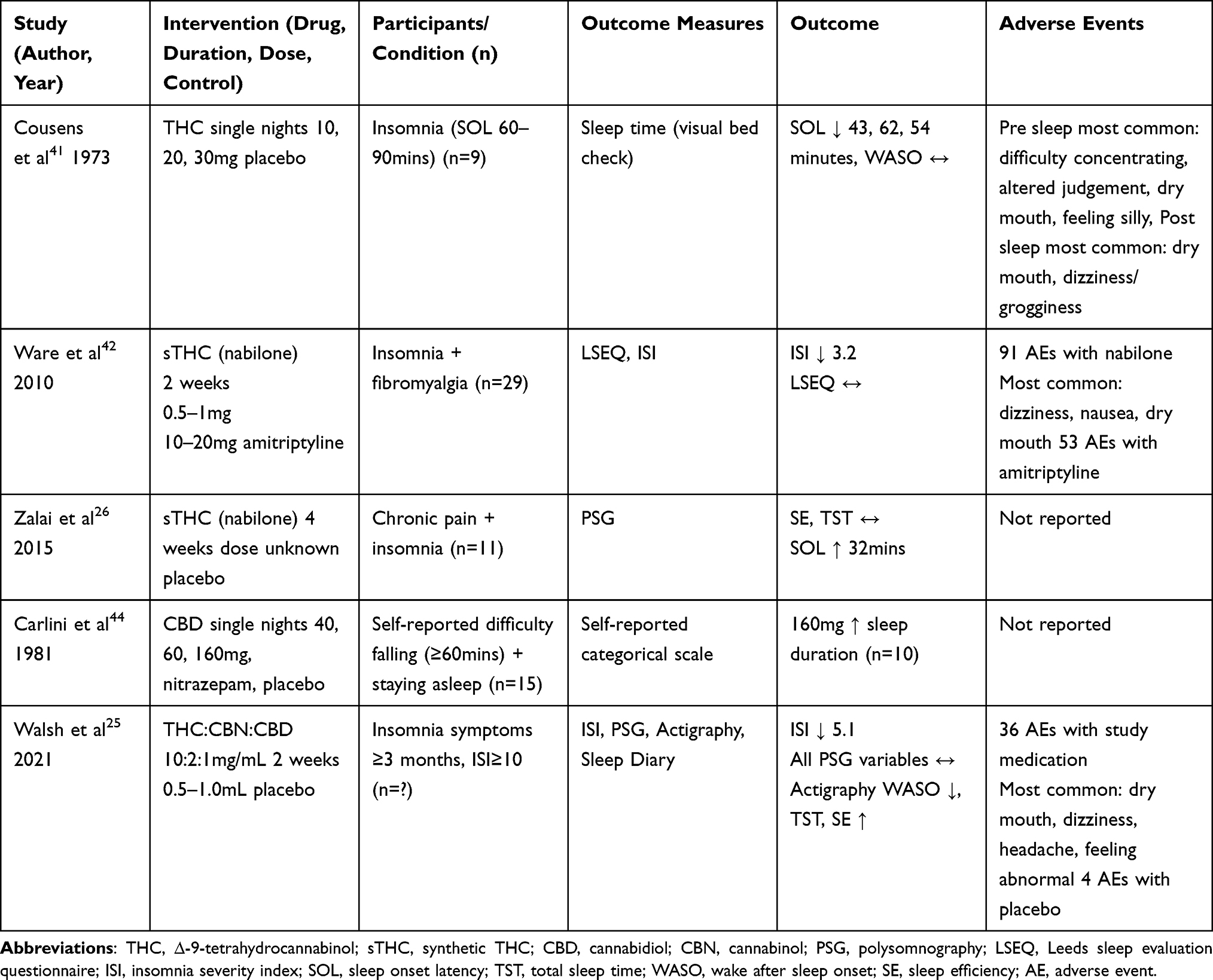 |
Table 2 Blinded, Randomized, Cross-Over Trials Evaluating the Effect of Cannabinoids on Poor Sleep or Insomnia |
Effect of THC on Insomnia
The earliest published double-blind, randomized, controlled study of the effect of THC on insomnia involved a single night of each of 10, 20, 30mg THC and a placebo in nine people with self-reported symptoms of insomnia (SOL, 60–90 mins).41 Sleep was measured by an “experienced sleep observer” who, following visual inspection of the participants at 15 min intervals across the night, classified each period as sleep or wake. Compared to placebo, SOL decreased by 43–62 minutes when taking THC, although there was no difference in the number of awakenings or time spent awake during the night. Adverse events were greater in a dose-dependent manner when taking THC than when taking placebo. Adverse events were more frequent in the evening, prior to sleep, than in the morning. Difficulty concentrating, altered judgement, dry mouth and feeling silly were the most adverse events in the evening, and dry mouth and dizziness/grogginess were the most common adverse events in the morning. Feelings of being “stoned” or “spaced” during the next day were more common at the higher doses. Two participants noted that they experienced an absence or reduction in dreaming with the 20 and 30mg THC doses.
Two subsequent randomized controlled cross-over trials have investigated the effect of synthetic THC (sTHC, nabilone) on sleep and/or insomnia symptoms in patients with chronic pain and comorbid insomnia.26,42 In 29 patients with fibromyalgia and chronic insomnia, insomnia symptoms (insomnia severity index, ISI) were significantly improved when taking 0.5–1.0mg nabilone compared to 10–20mg amitriptyline (ISI adjusted difference = 3.25 units) for 2 weeks. While both nabilone and amitriptyline were beneficial compared to baseline as assessed by the ISI, measures of sleep quality according to the Leeds sleep evaluation questionnaire were not improved. Adverse events were more frequent while taking nabilone than amitriptyline (91 versus 53) although no serious advents occurred. The most common adverse events while taking nabilone were dizziness, nausea, dry mouth and drowsiness, with one participant experiencing severe drowsiness. No differences in pain when taking the nabilone versus amitriptyline were identified, suggesting that the improvement in sleep was not secondary to improvement in pain.42 In a separate double-blind, randomized, placebo-controlled study (published only in abstract form) of 11 patients with chronic pain of unspecified etiology, and insomnia, in comparison to placebo, nabilone (dose unknown) taken over 4 weeks significantly increased PSG-measured SOL from 29.6 to 61.4 minutes (measured on a single night). Sleep efficiency and TST also non-significantly increased by 3.8% and 5.5%, respectively. Although the effects of nabilone on these objective measures of sleep were mixed, pain was significantly improved while taking nabilone compared to placebo. The number of adverse events was not reported.26
Effect of CBD on Insomnia
CBD has been promoted more widely, certainly among social media,43 as a cannabinoid with sedating properties. However, there is limited robust evidence for this notion. Carlini et al44 conducted a double-blind, randomized, placebo controlled trial with 3 doses of CBD (40, 80, 160mg) and an active comparator (5mg nitrazepam) over 5 separate nights, 1 week apart. The 15 cannabis naïve participants were known to the investigators and had a history of taking at least 1 hour to fall asleep and poor sleep through the night. Participants took the medication 30 minutes before bedtime and sleep quality was evaluated from self-reported difficulty falling and staying asleep and the number awakenings over the night. More participants reported longer sleep duration when taking 160mg CBD compared to when taking placebo, but no differences in the time taken to fall asleep or sleep maintenance were reported. There were no significant differences in self-reported sleep quantity or quality when taking the 40 and 80mg doses of CBD compared to placebo. It is also interesting to note that dream recall was significantly reduced when taking CBD, regardless of dose, compared to placebo and nitrazepam. The authors speculated that CBD may decrease the capacity to dream or dream recall. It is also possible that the amount of REM sleep was reduced. Adverse events were not reported although the number of people reporting feelings of sleepiness or difficulty concentrating in the morning was not significantly different after taking 160mg CBD than when taking placebo.
Effect of Mixed Cannabinoid Formulations on Insomnia
The most robust investigation of the effect of a cannabinoid formulation on insomnia involved a novel (ZTL-101) formulation of THC:CBN:CBD (20:2:1mg/mL).25 A double-blind, randomized, placebo-controlled trial investigated the effect of 2 weeks of the ZTL-101 formulation, and 2 weeks of placebo, on insomnia symptoms (classified according to the ISI) in 24 participants with chronic insomnia. Improvements in insomnia were quantified by changes in the ISI (primary outcome measure) as well as subjective measures of SOL, WASO, TST, sleep quality and feelings of being refreshed upon waking. In addition, objective measures of sleep were determined from actigraphy and PSG. Insomnia symptoms were significantly reduced while taking the ZTL-101 formation compared to placebo (ISI adjusted difference = −5.1). Subjective measures of SOL, WASO, TST, sleep quality and feeling of being refreshed upon waking were improved with the ZTL-101 formulation compared to placebo. Actigraphy derived measures of TST and WASO were also improved with ZTL-101 (mean differences = 33.4 and −10.2 minutes). There was no improvement in PSG derived measures of the same variables, possibly due to the single night, laboratory-based, PSG assessment versus 2 week, at-home, actigraphy assessment. Sleep architecture was also not different when taking ZTL-101 and placebo although the proportion of time in REM was reduced by 3.5% when taking ZTL-101 which just failed to meet significance (p=0.056). Adverse events were significantly more frequent when taking ZTL-101 than placebo (36 versus 4) although all were mild and resolved overnight or soon after waking. The most frequent adverse events were dry mouth, dizziness, headache and feeling abnormal.
Obstructive Sleep Apnea
Obstructive sleep apnea (OSA) is an increasingly common sleep-related breathing disorder characterized by recurrent episodes of complete and/or partial collapse of the upper airway. OSA is a heterogenous disorder with at least four key pathophysiological endotypes including 1) anatomical compromise, 2) low arousal threshold, 3) unstable ventilatory control and 4) impaired upper airway dilator function. Untreated OSA is associated with consequences including increased risk of cardiovascular and metabolic disease, depression and sleepiness-related accidents. Mainstream treatments such as continuous positive airway pressure therapy, oral appliance therapy and upper airway surgical options, primarily target the anatomical deficiency that contributes to OSA, in part because this is the most likely cause,45 but also because few treatment alternatives that target the other OSA endotypes are currently available. Pharmaceutical therapies may provide an additional option or adjunct therapy for individuals with OSA.46
Early animal work examined the potential role of sTHC (dronabinol) on respiratory stability in a Sprague-Dawley rat model of central sleep apnea and found that systemically administered dronabinol decreased the apnea index by 42% and 58% in non-rapid eye movement (NREM) and REM sleep respectively, although this was only at 1.0mg/kg and 10.0mg/kg doses.47 A subsequent study has identified that the mechanism of action of systemically administered dronabinol in apnea suppression is dependent on activation of the CB1 and CB2 receptors, possibly via modulation of the serotonin receptors on the vagal nerve.48 Furthermore, dronabinol was shown to increase both tonic and phasic genioglossus muscle activity.48 Therefore, despite arising from an animal model of central sleep apnea, these results offer a possible mechanism via which THC may provide therapeutic benefit for the management of OSA.
Subsequently, two clinical studies have examined dronabinol for the treatment of OSA. The first being a 3-week single arm open label, with potential dose escalation, proof of concept study completed by 15 of 17 enrolled OSA participants (apnea hypopnea index [AHI] ≥15 events.hr−1).49 Prasad et al demonstrated a mean decrease in AHI of 14±17.5 events.hr−1 from baseline (AHI = 48.4±17.6 events.hr−1) following once daily oral administration of 2.5mg, 5.0mg and 10mg of dronabinol (maximum tolerated) 30 minutes before bedtime. While it is noted that the variance of this decrease is large and that some individuals had little to no response, approximately half of the participants did demonstrate a decrease in AHI and only one participant demonstrated an increase in AHI while taking dronabinol at week 3 compared to baseline. Despite the demonstrated improvements in the AHI, no improvements in oxygenation were observed, the arousal index remained unchanged and sleep architecture was not degraded.
The same research team conducted a second, comprehensive, 6-week randomized, parallel group, placebo-controlled trial.50 Of 76 OSA participants (AHI ≥ 15 events.hr−1) enrolled, 56 completed the protocol in one of the three groups; placebo (n = 25), 2.5mg dronabinol (n = 21), or 10mg dronabinol (n = 27) taken daily, 60 minutes before bedtime. Compared to those taking placebo, AHI was reduced by 10.7±4.4 events.hr−1 and 12.9±4.3 events.hr−1 for those taking 2.5mg and 10mg of dronabinol, respectively. However, the reduction in AHI in those taking 10mg was largely driven by an 8.5 events.hr−1 increase in AHI in the placebo group; relative to AHI at baseline, neither dronabinol group showed a statistically significant reduction in AHI. There were no differences in oxygenation or arousal indices between the groups, although daytime sleepiness (Epworth sleepiness scale) was significantly reduced compared to baseline in those taking the high dose of dronabinol and not changed in the group taking the low dose or placebo. Sleep architecture was relatively unaffected by treatment although the proportion of REM sleep was increased slightly in those taking dronabinol and there was a slight decrease in NREM sleep.
Adverse events were common in both trials, with 75%49 and 96%51 of the participants experiencing at least one adverse event with 10mg dronabinol. Adverse events while taking the 2.5mg dose were experienced in 76%49 and 59%51 of participants. The most frequent adverse events reported were sleepiness, headache, nausea/vomiting and dizziness, and the majority of the events were rated as mild (73%), with only 2% rated as severe.50 No serious adverse events were reported in the proof of concept trial,49 and one possibly treatment related (diarrhea and vomiting requiring hospitalization) was reported in the randomized control trial.50
The American Academy of Sleep Medicine currently advises against the routine use of medicinal cannabis and/or its synthetic analogues for OSA treatment based on the limited evidence relating to efficacy and safety.52 However, the trials to date are promising and warrant further investigation into the therapeutic potential of cannabinoids for OSA. Placebo-controlled trials of dronabinol or other synthetic or phytocannabinoids, which include larger samples size and longer follow-up periods to examine both safety and efficacy, are needed. With increasing recognition for the need for precision medical management and targeted treatment plans, it is also important that we consider treatment responses for specific OSA endotypes. It is possible that short-term cannabinoid therapy could be beneficial for reducing anxiety and improving acceptance and adherence to continuous positive airway pressure therapy for treatment of OSA, and it may also have the potential to suppress treatment emergent central sleep apnea.
Restless Legs Syndrome
Restless legs syndrome (RLS) is a common sensorimotor disorder characterized by an unpleasant urge to move the legs. In the absence of another medical explanation for the symptoms, it is clinically defined by the presence of 1) an irresistible urge to move the legs; 2) a worsening of symptoms with inactivity; 3) partial or total relief of symptoms with movement; and 4) a worsening of symptoms in the evening (ie diurnal in nature). RLS negatively affects sleep quality and quality of life, especially when it is moderate to severe. Secondary RLS is diagnosed when symptoms are associated with iron deficiency, pregnancy, and end-stage renal disease. The pathophysiology of RLS is uncertain, but dysfunction of the dopaminergic system in the central nervous system and brain iron deficiency are implicated. Standard pharmacological treatment includes dopamine agonists, opiates and anticonvulsant medications along with and avoidance of caffeine, antidepressants, dopamine-blocking anti-emetics and centrally acting antihistamines. However, the use of dopamine agonists can be associated with severe side effects such as augmentation and impulse control disorder and in some cases, patients remain refractory to treatment. Arising from patient reports of symptom resolution from occasional recreational cannabis use cannabis has been proposed as a potential treatment alternative for patients with RLS.53
The observations from two case series of patients with treatment resistant RLS who smoked cannabis are promising. The first case series reported complete resolution of RLS symptoms in five patients with severe treatment resistant RLS who illegally smoked cannabis and one who took a sublingual dose of CBD.53 The second case series of 12 patients with moderate to severe RLS54 reported total remission of symptoms in 66% of patients with another three patients reporting 60%, 80% and 90% symptom relief from smoked cannabis without ceasing their currently prescribed medication for RLS. Only one in 12 patients reported no symptom improvement. It is also interesting that of those who experienced complete symptom relief with smoked cannabis two also reported good symptom improvement with CBD alone, while one patient reported CBD to have no benefit.54 It should be noted that there is strong risk of bias in these unblinded, uncontrolled case series with no baseline comparator. Furthermore, objective measures of RLS are lacking. However, the data is very promising and worthy of further investigation with carefully conducted randomized control trial to establish the true potential and efficacy of cannabinoids in the treatment of RLS.
REM Behavior Disorder
Rapid eye movement sleep behaviour disorder (RBD) is a parasomnia characterised by dream enactment behaviour due to the loss of protective skeletal muscle atonia in REM sleep.55 Typically, dreams involve fighting, defending against attackers or playing sport. Enactment of these dreams can result in punching, kicking, vocalisation and falling out of bed.56 RBD frequently causes injury to the individual or their bed partner.57 Although based on small randomised trials, recommended treatments for RBD include clonazepam and melatonin.58 However, the success of these medications is limited, with benefits often waning over time. Furthermore, medications such as clonazepam have significant adverse effects including nocturnal confusion, falls, morning drowsiness and worsening of OSA. Other therapeutic options for RBD are needed.
Cannabis has been used in the treatment of RBD with conflicting results. Chagas et al reported a case series of 4 patients with Parkinson’s disease and RBD symptoms successfully treated with CBD.59 The patients had RBD symptoms based on clinical assessment by a neurologist specialising in sleep. Two of the patients had REM without atonia confirmed by overnight PSG and all had a bed partner who could corroborate RBD activity. No patient had previously received treatment for RBD. Prior to starting treatment, RBD symptoms were occurring 2–4 times a week in three patients and nightly for one of the patients. Three of the patients were treated 75mg CBD and one patient with 300mg CBD for 6 weeks. Whilst taking CBD, three of the patients reported experiencing no RBD symptoms and one patient reported having symptoms once per week. RBD symptoms returned at the same frequency and intensity when CBD was stopped.
A subsequent 12-week randomised placebo-controlled trial of CBD for RBD in Parkinson’s disease found it no better than placebo for treating RBD symptoms.60 De Almeida et al carefully characterised patients with RBD, confirmed the diagnosis by loss of REM atonia and ensured the 33 participants included had a bed partner to monitor RBD activity, which was the primary outcome measure. Participants were randomised to placebo (n = 16) or 75mg to 300mg CBD (n = 17) daily oral capsules, taken in the evening. Despite significant differences in the number of RBD events during the baseline period (3.26 events in the CBD group versus 5.15 events in the placebo group; p = 0.0235) both groups had a reduction in events during the trial so there was no difference between the groups after 12 weeks (2.07 in the CBD group versus 2.95 in the placebo group). It is interesting to note that there was a significant improvement in self-reported sleep satisfaction between the 4th and 8th week in the participants taking CBD compared to those taking placebo but this difference was not sustained at 12 weeks. There were also no differences in PSG-derived measures of sleep quality or architecture between the groups, despite taking CBD/placebo for 12 weeks. Adverse events were not common and less frequent in those taking CBD than placebo and included epigastric pain, headache, drowsiness, sadness and dizziness.
The findings from this study do not demonstrate a convincing beneficial effect of CBD on RBD; rather, they highlight the waxing and waning natural history of RBD. However, like most studies investigating RBD, this study relied on reports of RBD activity frequency from the participant or bedpartner. Further studies utilising an objective and reliable method of measuring symptom severity are needed as CBD appears safe but its efficacy in the treatment of RBD remains unclear.
PTSD-Related Nightmare Disorder
Recurring nightmares of a past traumatic event are a key feature of post-traumatic stress disorder (PTSD).37 Nightmares are one of the most distressing symptoms of PTSD and are difficult to treat. Recommended treatments, such as image rehearsal therapy and prazosin, have moderate efficacy.61–63
Nabilone, a sTHC, has been reported to have a beneficial effect on PTSD-related nightmare disorder in two retrospective case series.64,65 The earliest published case series included 47 patients of a psychiatric clinic with PTSD-related nightmares at least once weekly, despite treatment.65 Patients recorded sleep and nightmare frequency for at least one week prior to starting treatment. Nabilone was taken nightly (mean dose 0.5mg, range 0.2–4.0mg). Side effects such as dizziness, memory difficulty and headache lead to early treatment discontinuation in 28% of patients, while 72% experienced cessation or reduction in nightmare frequency/severity. Some patients (9%) were able to cease treatment without return of symptoms after 4–12 months. The second case series included 104 inmates who received nabilone at some point during their stay at a correctional institution.64 The most common indications for use were insomnia (n = 101), nightmares (n = 90), and chronic pain (n = 68). Over a mean treatment period of 11.2 weeks, the mean final dose was 4.0mg. According to self-report, participants reported a reduction in the number of nights they had nightmares per week (5.2±2.2 versus 0.9±1.8 nights/week) over the treatment period. Interestingly, the number of self-reported hours slept also improved (5.0±1.4 vs 7.2±1.2 hours/night).
Using a more robust double-blind randomised placebo control design, Jetly et al examined the effect of Nabilone in 19 military veterans with PTSD-related nightmares.66 The starting dose of Nabilone was 0.5mg titrated up to a maximum of 3mg daily. Based on validated questionnaires, participants taking nabilone demonstrated improvement in PTSD-related recurring dream frequency and intensity, clinician view of functioning and general well-being compared to placebo. The study was small and not powered so may have suffered from a type 1 error.66 However, this study along with the two case series64,65 provides initial evidence that THC maybe helpful in PTSD-related nightmare disorder.
Narcolepsy and Idiopathic Hypersomnia
There have been no published clinical studies of medical cannabis for the treatment of central disorders of hypersomnolence such as narcolepsy and idiopathic hypersomnia. However, animal studies suggest they may offer a potential treatment option. Excessive sleepiness has been shown to be reduced following CBD administration in rats with narcoleptic symptoms (hypocretin deficient)67,68 and REM has been shown to be reduced following sTHC administration in a rat model.69 Theoretically, the combined REM-suppressing effect of THC and wake-promoting effect of CBD could be harnessed to treat patients with narcolepsy. The THC-induced attenuation in REM sleep might also benefit other REM sleep state conditions that often co-occur with narcolepsy such as nightmares, sleep paralysis, REM sleep behaviour disorder, sleep wake hallucinations and cataplexy. Further supporting a potential role for cannabinoids in the treatment of narcolepsy is the existing clinical evidence suggesting that the acute use of THC may increase the proportion of slow wave sleep and promote REM suppression (see - Effect of cannabinoids on sleep and sleep architecture), which is similar to the effect of sodium oxybate, an effective treatment for type 1 (hypocretin deficient) narcolepsy.
There is a clear need for clinical studies evaluating the efficacy of cannabinoids in the treatment of disorders of hypersomnolence. Given the low adverse event rate when CBD has been used in clinical trials and the encouraging preclinical data, it seems logical to start with randomised control studies of CBD as an adjunct treatment for excessive daytime sleepiness in narcolepsy.27
Discussion/Future Directions/Challenges to the Field
This review has summarized the most rigorous clinical evidence, of that available, relating to cannabinoid use in the treatment of sleep disorders to date. As very few randomized controlled trials have been conducted, much of the available evidence arises from uncontrolled, unblinded trials of short duration, and case series. Therefore, sufficient evidence is currently not available to support the routine use of a cannabinoid as an effective and safe treatment option for sleep disorders. However, the data from the existing studies is promising and warrants further investigation of cannabinoids for the treatment of all sleep disorders discussed in this review.
Future research trials of rigorous design should include quantitative measures of sleep or validated measures of symptoms of sleep disorders and the focus should be on cannabinoid products of standardized formulation that allow for titration and have an innocuous route of delivery; the effect of smoked cannabis on lung health in particular remains unclear.70,71 Route of delivery will also alter the therapeutic effects, as will prior consumption of food, previous cannabis exposure, sex, body composition, age and whether it is a cannabinoid taken in combination or isolation.34,72–74 Also required is investigation into the safety and efficacy longer-term use and effects on dependence and tolerance as well as withdrawal. It is also imperative to quantify effects on daytime function and performance, specifically driving performance and to compare these results to the consequences of untreated sleep disorders. Finally, when using phytocannabinoid-based products, it might be important to quantify the terpenes, another phytochemical present in the cannabis plant, which may independently impact health and sleep.75
It is worth noting that the focus of the current review was limited to clinical studies where sleep or a sleep disorder symptom was the focus. However, as revealed in a recent meta-analysis, it is likely that sleep is also improved when cannabinoids are used to treat other conditions such as pain.76 It is important that sleep outcomes, assessed using valid and quantitative tools, continue to be measured in these populations as sleep disorders or poor sleep often co-occur with many physical and mental health conditions and may exacerbate the condition or negatively impact recovery.77,78
Conclusion
There is currently insufficient evidence to support the clinical use of any cannabinoid as a safe and effective routine treatment for any sleep disorder. However, encouraging outcomes from recent studies in relation to some disorders indicates that pursuit of elucidating the potential role of cannabinoids for the treatment of sleep disorders is warranted.
Disclosure
JW and KM have received research group funding from Zelira Therapeutics and Incannex Healthcare Limited. They have received no personal income from these companies. CK has no conflicts to declare.
References
1. Adams RJ, Appleton SL, Taylor AW, et al. Sleep health of Australian adults in 2016: results of the 2016 Sleep Health Foundation national survey. Sleep Health. 2017;3(1):35–42. doi:10.1016/j.sleh.2016.11.005
2. Zuardi AW. History of cannabis as a medicine: a review. Braz J Psychiatry. 2006;28(2):153–157. doi:10.1590/s1516-44462006000200015
3. Kesner AJ, Lovinger DM. Cannabinoids, Endocannabinoids and Sleep. Front Mol Neurosci. 2020;13:125. doi:10.3389/fnmol.2020.00125
4. Prospero-Garcia O, Amancio-Belmont O, Becerril Melendez AL, Ruiz-Contreras AE, Mendez-Diaz M. Endocannabinoids and sleep. Neurosci Biobehav Rev. 2016;71:671–679. doi:10.1016/j.neubiorev.2016.10.005
5. Petrunich-Rutherford ML, Calik MW. Effects of Cannabinoid Agonists and Antagonists on Sleep in Laboratory Animals. Adv Exp Med Biol. 2021;1297:97–109. doi:10.1007/978-3-030-61663-2_7
6. Niesink RJ, van Laar MW. Does Cannabidiol Protect Against Adverse Psychological Effects of THC? Front Psychiatry. 2013;4:130. doi:10.3389/fpsyt.2013.00130
7. Lintzeris N, Mills L, Suraev A, et al. Medical cannabis use in the Australian community following introduction of legal access: the 2018-2019 Online Cross-Sectional Cannabis as Medicine Survey (CAMS-18). Harm Reduct J. 2020;17(1):37. doi:10.1186/s12954-020-00377-0
8. Association ATG. Special Access Scheme-B. Available from: https://www.tga.gov.au/medicinal-cannabis-special-access-scheme-category-b-data.
9. Feinberg I, Jones R, Walker J, Cavness C, Floyd T. Effects of marijuana extract and tetrahydrocannabinol on electroencephalographic sleep patterns. Clin Pharmacol Ther. 1976;19(6):782–794. doi:10.1002/cpt1976196782
10. Feinberg I, Jones R, Walker JM, Cavness C, March J. Effects of high dosage delta-9-tetrahydrocannabinol on sleep patterns in man. Clin Pharmacol Ther. 1975;17(4):458–466. doi:10.1002/cpt1975174458
11. Karacan I, Fernandez-Salas A, Coggins WJ, et al. Sleep electroencephalographic-electrooculographic characteristics of chronic marijuana users: part I. Ann N Y Acad Sci. 1976;282:348–374. doi:10.1111/j.1749-6632.1976.tb49909.x
12. Bedi G, Foltin RW, Gunderson EW, et al. Efficacy and tolerability of high-dose dronabinol maintenance in HIV-positive marijuana smokers: a controlled laboratory study. Psychopharmacology. 2010;212(4):675–686. doi:10.1007/s00213-010-1995-4
13. Gorelick DA, Goodwin RS, Schwilke E, et al. Around-the-clock oral THC effects on sleep in male chronic daily cannabis smokers. Am J Addict. 2013;22(5):510–514. doi:10.1111/j.1521-0391.2013.12003.x
14. Haney M, Gunderson EW, Rabkin J, et al. Dronabinol and marijuana in HIV-positive marijuana smokers. Caloric intake, mood, and sleep. J Acquir Immune Defic Syndr. 2007;45(5):545–554. doi:10.1097/QAI.0b013e31811ed205
15. Carr M, Borcsok R, Taylor M, Segust S, Pigeon W, Bradshaw C. Reduced Rem Sleep Percent in Frequent Cannabis Versus Non-Cannabis Users. Sleep. 2020;43:A62–A63.
16. Freemon FR. The effect of chronically administered delta-9-tetrahydrocannabinol upon the polygraphically monitored sleep of normal volunteers. Drug Alcohol Depend. 1982;10(4):345–353. doi:10.1016/0376-8716(82
17. Barratt ES, Beaver W, White R. The effects of marijuana on human sleep patterns. Biol Psychiatry. 1974;8(1):47–54.
18. Freemon FR. Effects of marihuana on sleeping states. JAMA. 1972;220(10):1364–1365.
19. Pivik RT, Zarcone V, Dement WC, Hollister LE. Delta-9-tetrahydrocannabinol and synhexl: effects on human sleep patterns. Clin Pharmacol Ther. 1972;13(3):426–435. doi:10.1002/cpt1972133426
20. Ogeil RP, Phillips JG, Rajaratnam SMW, Broadbear JH. Risky drug use and effects on sleep quality and daytime sleepiness. Hum Psychopharm Clin. 2015;30(5):356–363. doi:10.1002/hup.2483
21. Pranikoff K, Karacan I, Larson EA, Williams RL, Thornby JI, Hursch CJ. Effects of marijuana smoking on the sleep EEG. Preliminary studies. JFMA. 1973;60(3):28–31.
22. Blake DR, Robson P, Ho M, Jubb RW, McCabe CS. Preliminary assessment of the efficacy, tolerability and safety of a cannabis-based medicine (Sativex) in the treatment of pain caused by rheumatoid arthritis. Rheumatology. 2006;45(1):50–52. doi:10.1093/rheumatology/kei183
23. Frank B, Serpell MG, Hughes J, Matthews JN, Kapur D. Comparison of analgesic effects and patient tolerability of nabilone and dihydrocodeine for chronic neuropathic pain: randomised, crossover, double blind study. BMJ. 2008;336(7637):199–201. doi:10.1136/bmj.39429.619653.80
24. Narang S, Gibson D, Wasan AD, et al. Efficacy of dronabinol as an adjuvant treatment for chronic pain patients on opioid therapy. J Pain. 2008;9(3):254–264. doi:10.1016/j.jpain.2007.10.018
25. Walsh JH, Maddison KJ, Rankin T, et al. Treating insomnia symptoms with medicinal cannabis: a randomized, crossover trial of the efficacy of a cannabinoid medicine compared with placebo. Sleep. 2021;44(11):65. doi:10.1093/sleep/zsab149
26. Zalai D, Chung SA, Hussain N, Shapiro CM. Does cannabinoid really improve sleep? Testing the sleep effects of nabilone in chronic pain patients: a placebo-controlled, randomized, pilot study. Psychother Psychosom. 2015;84(Supplement 1):81.
27. Suraev AS, Marshall NS, Vandrey R, et al. Cannabinoid therapies in the management of sleep disorders: a systematic review of preclinical and clinical studies. Sleep Med Rev. 2020;53:101339. doi:10.1016/j.smrv.2020.101339
28. Kuhathasan N, Dufort A, MacKillop J, Gottschalk R, Minuzzi L, Frey BN. The use of cannabinoids for sleep: a critical review on clinical trials. Exp Clin Psychopharmacol. 2019;27(4):383–401. doi:10.1037/pha0000285
29. Babson KA, Sottile J, Morabito D. Cannabis, Cannabinoids, and Sleep: a Review of the Literature. Curr Psychiatry Rep. 2017;19(4):23. doi:10.1007/s11920-017-0775-9
30. Hosko MJ, Kochar MS, Wang RI. Effects of orally administered delta-9-tetrahydrocannabinol in man. Clin Pharmacol Ther. 1973;14(3):344–352. doi:10.1002/cpt1973143344
31. Nicholson AN, Turner C, Stone BM, Robson PJ. Effect of Delta-9-tetrahydrocannabinol and cannabidiol on nocturnal sleep and early-morning behavior in young adults. J Clin Psychopharmacol. 2004;24(3):305–313. doi:10.1097/01.jcp.0000125688.05091.8f
32. Tassinari CA, Ambrosetto G, Peraita-Adrado MR, Gastaut H. The neuropsychiatric syndrome of Delta(9)-tetrahydrocannabinol and cannabis intoxication in naive subjects - A clinical and polygraphic study during wakefulness and sleep. Marihuana Med. 1999;1:649–664.
33. Linares IMP, Guimaraes FS, Eckeli A, et al. No Acute Effects of Cannabidiol on the Sleep-Wake Cycle of Healthy Subjects: a Randomized, Double-Blind, Placebo-Controlled, Crossover Study. Front Pharmacol. 2018;9:315. doi:10.3389/fphar.2018.00315
34. Grotenhermen F. Pharmacokinetics and pharmacodynamics of cannabinoids. Clin Pharmacokinet. 2003;42(4):327–360. doi:10.2165/00003088-200342040-00003
35. Morin CM, Benca R. Chronic insomnia. Lancet. 2012;379(9821):1129–1141. doi:10.1016/s0140-6736(11
36. Reynolds AC, Appleton SL, Gill TK, Adams RJ. Chronic insomnia disorder in Australia: a report to the Sleep Health Foundation. 2019.
37. Association AP. Diagnostic and Statistical Manual of Mental Disorders.
38. Medicine AAoS. International Classification of Sleep Disorders.
39. Hazekamp A, Ware MA, Muller-Vahl KR, Abrams D, Grotenhermen F. The Medicinal Use of Cannabis and Cannabinoids-An International Cross-Sectional Survey on Administration Forms. J Psychoactive Drugs. 2013;45(3):199–210. doi:10.1080/02791072.2013.805976
40. AminiLari M, Wang L, Neumark S, et al. Medical Cannabis and Cannabinoids for Impaired Sleep: a Systematic Review and Meta-Analysis of Randomized Clinical Trials. Sleep. 2021;1:42. doi:10.1093/sleep/zsab234
41. Cousens K, DiMascio A. (-) Delta 9 THC as an hypnotic. An experimental study of three dose levels. Psychopharmacologia. 1973;33(4):355–364. doi:10.1007/bf00437513
42. Ware MA, Fitzcharles MA, Joseph L, Shir Y. The effects of nabilone on sleep in fibromyalgia: results of a randomized controlled trial. Anesth Analg. 2010;110(2):604–610. doi:10.1213/ANE.0b013e3181c76f70
43. Soleymanpour M, Saderholm S, Kavuluru R. Therapeutic Claims in Cannabidiol (CBD) Marketing Messages on Twitter. Proceedings (IEEE Int Conf Bioinformatics Biomed). 2021;2021:3083–3088. doi:10.1109/bibm52615.2021.9669404
44. Carlini EA, Cunha JM. Hypnotic and antiepileptic effects of cannabidiol. J Clin Pharmacol. 1981;21(S1):417S–427S. doi:10.1002/j.1552-4604.1981.tb02622.x
45. Eckert DJ, White DP, Jordan AS, Malhotra A, Wellman A. Defining phenotypic causes of obstructive sleep apnea. Identification of novel therapeutic targets. Am J Respir Crit Care Med. 2013;188(8):996–1004. doi:10.1164/rccm.201303-0448OC
46. Taranto-Montemurro L, Messineo L, Wellman A. Targeting Endotypic Traits with Medications for the Pharmacological Treatment of Obstructive Sleep Apnea. A Review of the Current Literature. J Clin Med. 2019;8(11):54. doi:10.3390/jcm8111846
47. Carley DW, Paviovic S, Janelidze M, Radulovacki M. Functional role for cannabinoids in respiratory stability during sleep. Sleep. 2002;25(4):391–398.
48. Calik MW, Carley DW. Cannabinoid type 1 and type 2 receptor antagonists prevent attenuation of serotonin-induced reflex apneas by dronabinol in Sprague-Dawley rats. PLoS One. 2014;9(10):e111412. doi:10.1371/journal.pone.0111412
49. Prasad B, Radulovacki MG, Carley DW. Proof of concept trial of dronabinol in obstructive sleep apnea. Front Psychiatry. 2013;4:21. doi:10.3389/fpsyt.2013.00001
50. Carley DW, Prasad B, Reid KJ, et al. Pharmacotherapy of Apnea by Cannabimimetic Enhancement, the PACE Clinical Trial: effects of Dronabinol in Obstructive Sleep Apnea. Sleep. 2018;41(1):58. doi:10.1093/sleep/zsx184
51. ClinicalTrialsgov. Safety and Efficacy Study of Dronabinol to Treat Obstructive Sleep Apnea (PACE). 2021. Available from: https://clinicaltrials.gov/ct2/show/results/NCT01755091?term=PACE&view=results
52. Ramar K, Rosen IM, Kirsch DB, et al. Medical Cannabis and the Treatment of Obstructive Sleep Apnea: an American Academy of Sleep Medicine Position Statement. J Clin Sleep Med. 2018;14(4):679–681. doi:10.5664/jcsm.7070
53. Megelin T, Ghorayeb I. Cannabis for restless legs syndrome: a report of six patients. Sleep Med. 2017;36:182–183. doi:10.1016/j.sleep.2017.04.019
54. Ghorayeb I. More evidence of cannabis efficacy in restless legs syndrome. Sleep Breath. 2020;24(1):277–279. doi:10.1007/s11325-019-01978-1
55. Schenck CH, Bundlie SR, Ettinger MG, Mahowald MW. Chronic behavioral disorders of human REM sleep: a new category of parasomnia. Sleep. 1986;9(2):293–308. doi:10.1093/sleep/9.2.293
56. Fernandez-Arcos A, Iranzo A, Serradell M, Gaig C, Santamaria J. The Clinical Phenotype of Idiopathic Rapid Eye Movement Sleep Behavior Disorder at Presentation: a Study in 203 Consecutive Patients. Sleep. 2016;39(1):121–132. doi:10.5665/sleep.5332
57. Olson EJ, Boeve BF, Silber MH. Rapid eye movement sleep behaviour disorder: demographic, clinical and laboratory findings in 93 cases. Brain. 2000;123(Pt 2):331–339. doi:10.1093/brain/123.2.331
58. Aurora RN, Zak RS, Maganti RK, et al. Best practice guide for the treatment of REM sleep behavior disorder (RBD). J Clin Sleep Med. 2010;6(1):85–95.
59. Chagas MH, Eckeli AL, Zuardi AW, et al. Cannabidiol can improve complex sleep-related behaviours associated with rapid eye movement sleep behaviour disorder in Parkinson’s disease patients: a case series. J Clin Pharm Ther. 2014;39(5):564–566. doi:10.1111/jcpt.12179
60. de Almeida CMO, Brito MMC, Bosaipo NB, et al. Cannabidiol for Rapid Eye Movement Sleep Behavior Disorder. Mov Disord. 2021;36(7):1711–1715. doi:10.1002/mds.28577
61. Aurora RN, Zak RS, Auerbach SH, et al. Best practice guide for the treatment of nightmare disorder in adults. J Clin Sleep Med. 2010;6(4):389–401.
62. Seda G, Sanchez-Ortuno MM, Welsh CH, Halbower AC, Edinger JD. Comparative meta-analysis of prazosin and imagery rehearsal therapy for nightmare frequency, sleep quality, and posttraumatic stress. J Clin Sleep Med. 2015;11(1):11–22. doi:10.5664/jcsm.4354
63. Morgenthaler TI, Auerbach S, Casey KR, et al. Position Paper for the Treatment of Nightmare Disorder in Adults: an American Academy of Sleep Medicine Position Paper. J Clin Sleep Med. 2018;14(6):1041–1055. doi:10.5664/jcsm.7178
64. Cameron C, Watson D, Robinson J. Use of a synthetic cannabinoid in a correctional population for posttraumatic stress disorder-related insomnia and nightmares, chronic pain, harm reduction, and other indications: a retrospective evaluation. J Clin Psychopharmacol. 2014;34(5):559–564. doi:10.1097/jcp.0000000000000180
65. Fraser GA. The use of a synthetic cannabinoid in the management of treatment-resistant nightmares in posttraumatic stress disorder (PTSD). CNS Neurosci Ther. 2009;15(1):84–88. doi:10.1111/j.1755-5949.2008.00071.x
66. Jetly R, Heber A, Fraser G, Boisvert D. The efficacy of nabilone, a synthetic cannabinoid, in the treatment of PTSD-associated nightmares: a preliminary randomized, double-blind, placebo-controlled cross-over design study. Psychoneuroendocrinology. 2015;51:585–588. doi:10.1016/j.psyneuen.2014.11.002
67. Murillo-Rodriguez E, Millan-Aldaco D, Palomero-Rivero M, Morales-Lara D, Mechoulam R, Drucker-Colin R. Cannabidiol Partially Blocks the Excessive Sleepiness in Hypocretindeficient Rats: preliminary Data. CNS Neurol Disord Drug Targets. 2019;18(9):705–712. doi:10.2174/1871527318666191021143300
68. Murillo-Rodriguez E, Sarro-Ramirez A, Sanchez D, et al. Potential Effects of Cannabidiol as a Wake-Promoting Agent. Curr Neuropharmacol. 2014;12(3):269–272. doi:10.2174/1570159x11666131204235805
69. Calik MW, Carley DW. Effects of Cannabinoid Agonists and Antagonists on Sleep and Breathing in Sprague-Dawley Rats. Sleep. 2017;40(9):55. doi:10.1093/sleep/zsx112
70. Biehl JR, Burnham EL. Cannabis Smoking in 2015: a Concern for Lung Health? Chest. 2015;148(3):596–606. doi:10.1378/chest.15-0447
71. Tan WC, Sin DD. What are the long-term effects of smoked marijuana on lung health? CMAJ. 2018;190(42):E1243–E1244. doi:10.1503/cmaj.181307
72. Oh DA, Parikh N, Khurana V, Cognata Smith C, Vetticaden S. Effect of food on the pharmacokinetics of dronabinol oral solution versus dronabinol capsules in healthy volunteers. Clin Pharmacol. 2017;9:9–17. doi:10.2147/CPAA.S119676
73. Lucas CJ, Galettis P, Schneider J. The pharmacokinetics and the pharmacodynamics of cannabinoids. Br J Clin Pharmacol. 2018;84(11):2477–2482. doi:10.1111/bcp.13710
74. Cooper ZD, Craft RM. Sex-Dependent Effects of Cannabis and Cannabinoids: a Translational Perspective. Neuropsychopharmacology. 2018;43(1):34–51. doi:10.1038/npp.2017.140
75. Andre CM, Hausman JF, Guerriero G. Cannabis sativa: the Plant of the Thousand and One Molecules. Front Plant Sci. 2016;7:19. doi:10.3389/fpls.2016.00019
76. AminiLari M, Wang L, Neumark S, et al. Medical cannabis and cannabinoids for impaired sleep: a systematic review and meta-analysis of randomized clinical trials. Sleep. 2022;45(2):87. doi:10.1093/sleep/zsab234
77. Gee B, Orchard F, Clarke E, Joy A, Clarke T, Reynolds S. The effect of non-pharmacological sleep interventions on depression symptoms: a meta-analysis of randomised controlled trials. Sleep Med Rev. 2019;43:118–128. doi:10.1016/j.smrv.2018.09.004
78. Duss SB, Seiler A, Schmidt MH, et al. The role of sleep in recovery following ischemic stroke: a review of human and animal data. Neurobiol Sleep Circadian Rhythms. 2017;2:94–105. doi:10.1016/j.nbscr.2016.11.003
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
All-Cause Mortality in People with Co-Occurring Insomnia Symptoms and Sleep Apnea: Analysis of the Wisconsin Sleep Cohort
Lechat B, Loffler KA, Wallace DM, Reynolds A, Appleton SL, Scott H, Vakulin A, Lovato N, Adams R, Eckert DJ, Catcheside PG, Sweetman A
Nature and Science of Sleep 2022, 14:1817-1828
Published Date: 13 October 2022
Subjective Sleep Disruption and Mood Disorders are Associated with the Risk of Chronic Pain in Patients with Obstructive Sleep Apnea
Liu L, Li X, Xue P, Wu M, Zeng S, Dai Y, Zhou J
Nature and Science of Sleep 2022, 14:2023-2032
Published Date: 7 November 2022
Performance of Four Screening Tools for Identifying Obstructive Sleep Apnea Among Patients with Insomnia
Shi C, Wang Y, Luo J, Huang R, Xiao Y
Nature and Science of Sleep 2025, 17:379-390
Published Date: 3 March 2025