Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Is Metabolic Score for Visceral Fat (METS-VF) a Better Index Than Other Adiposity Indices for the Prediction of Visceral Adiposity
Authors Torun C ![]() , Ankaralı H
, Ankaralı H ![]() , Caştur L
, Caştur L ![]() , Uzunlulu M, Erbakan AN
, Uzunlulu M, Erbakan AN ![]() , Akbaş MM
, Akbaş MM ![]() , Gündüz N, Doğan MB, Oğuz A
, Gündüz N, Doğan MB, Oğuz A
Received 16 May 2023
Accepted for publication 1 August 2023
Published 29 August 2023 Volume 2023:16 Pages 2605—2615
DOI https://doi.org/10.2147/DMSO.S421623
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Konstantinos Tziomalos
Cundullah Torun,1 Handan Ankaralı,2 Lütfullah Caştur,1 Mehmet Uzunlulu,1 Ayşe Naciye Erbakan,1 Muhammet Mikdat Akbaş,1 Nesrin Gündüz,3 Mahmut Bilal Doğan,3 Aytekin Oğuz1
1Department of Internal Medicine, Goztepe Training and Research Hospital, Istanbul Medeniyet University, Kadikoy, Istanbul, Türkiye; 2Department of Biostatistics and Medical Informatics, Goztepe Training and Research Hospital, Istanbul Medeniyet University, Kadikoy, Istanbul, Türkiye; 3Department of Radiology, Goztepe Training and Research Hospital, Istanbul Medeniyet University, Kadikoy, Istanbul, Türkiye
Correspondence: Cundullah Torun, Goztepe Training and Research Hospital, District of Kadıköy, Neighbourhood of Eğitim, Kadikoy, Province of Istanbul, 34722, Türkiye, Tel +905497949993, Fax +90 216 606 52 10, Email [email protected]
Background: Visceral adiposity is an important risk factor for cardiometabolic diseases.
Objective: To determine whether the Metabolic Score for Visceral Fat (METS-VF) is more effective than other adiposity indices in predicting visceral fat area (VFA).
Methods: In this single-center and cross-sectional study, we included patients aged 20– 50 years, without diabetes and coronary artery disease, who underwent computed tomography (CT) including the third lumbar vertebra. Age, blood pressure, waist circumference (WC), hip circumference, fasting lipids, and glucose were assessed. VFA was measured by cross-sectional examination of CT. The correlation of WC, body mass index (BMI), waist-hip ratio (WHR), lipid accumulation product (LAP), visceral adiposity index (VAI), a body shape index (ABSI), body roundness index (BRI), and METS-VF with VFA was analyzed by correlation analysis. The cut-off values and area under the curve (AUC) for identifying increased VFA (> 130 cm2) were determined.
Results: We included 185 individuals with mean age 38.2 ± 8 and female predominance (58.4%). There was a significant positive correlation between all indices and VFA (p< 0.001). ROC analysis revealed that METS-VF and WC demonstrated the highest predictive value for identifying increased VFA. In both men (p=0.001) and women (p< 0.001), METS-VF (AUC 0.922 and 0.939, respectively) showed a significant superiority over ABSI (AUC 0.702 and 0.658, respectively), and VAI (AUC 0.731 and 0.725, respectively). Additionally, in women, its superiority over WHR (AUC 0.807) was also statistically significant (p=0.003). We identified a METS-VF cut-off point > 6.4 in males > 6.5 in females and WC cut-off point > 88 cm in males (AUC 0.922), > 90.5 cm in females (AUC 0.938).
Conclusion: METS-VF is strongly associated with visceral adiposity and better to predict increased VFA. However, its superiority over WC, BMI, BRI, and LAP was not significant. The results emphasize that WC is more appealing as screening indicator for visceral adiposity considering its easy use.
Clinical Trial Registry Name: Clinicaltrials.gov (http://www.clinicaltrials.gov).
Clinical Trial Registry Url: https://clinicaltrials.gov/ct2/show/NCT05648409.
Clinical Trial Registry Number: NCT05648409.
Keywords: obesity, cardiometabolic risk, hypertriglyceridemic waist, body shape, anthropometric measurements
Introduction
Obesity is an important risk factor for cardiometabolic diseases such as type 2 diabetes, hypertension, and coronary artery disease.1 Body mass index (BMI) has long been used in the evaluation of obesity and the World Health Organization defines a BMI above 30 kg/m2 as obesity.2 However, although BMI is a simple and useful method for assessing general obesity, it does not provide sufficient insight into the separation of lean body mass and adipose tissue and the distribution of adipose tissue.
The importance of the distribution of adipose tissue in the body was first demonstrated by Vague.3 Subcutaneous adipose tissue (SAT) is widely distributed throughout the body, whereas visceral adipose tissue (VAT) is mostly found in the abdominal area. Compared to SAT, VAT exhibits higher cellular and vascular density, increased innervation, and a larger presence of inflammatory and immune cells and a higher percentage of large adipocytes.4 An increase in VAT is more closely associated with adipocyte dysfunction and associated cardiometabolic risk.5,6 Therefore, the term visceral adiposity has been frequently used and has been the focus of research interest.
The best methods to evaluate visceral adiposity are magnetic resonance imaging (MRI), computed tomography (CT) and dual energy x-ray (DXA). Single slice examination of MRI and CT has been shown to successfully reflect the total amount of VAT.7,8 However, the fact that both methods are expensive, difficult to access, and cannot be used routinely for primary prevention has led to the search for simpler, cheaper and reproducible methods. While waist-hip ratio (WHR) was initially used for evaluating obesity, its superiority over waist circumference (WC) could not be demonstrated in later studies.9 Therefore, WC is included among the criteria for metabolic syndrome.10
In 2000, Lemieux et al developed the concept of “hypertriglyceridemic waist circumference” which revealed the relationship between triglycerides and waist circumference with visceral adiposity.11 Based on this, novel indices, including lipid accumulation product (LAP) and visceral adiposity index (VAI), have been created to estimate visceral adiposity.12,13 Although both techniques have been found effective in predicting the incidence of metabolic syndrome among diverse patient populations, some studies have not demonstrated their superiority over traditional anthropometric measurements.14–16 In 2012, Krakauer et al developed a body shape index (ABSI) that normalizes WC for weight and height (and thus to BMI) and showed that ABSI has a stronger association with mortality than WC and BMI alone.17 In the following year, Thomas et al developed the body roundness index (BRI), which was found to have a strong correlation with visceral fat area (VFA) and be superior to BMI in identifying individuals with metabolic syndrome.18,19
The Metabolic Score for Insulin Resistance (METS-IR), developed by Bello-Chavolla et al in 2018, has been demonstrated to have a strong correlation with VFA.20 However, due to the relatively small sample size of the group for which the formula was developed, as well as the fact that nearly half of the participants in this group were diagnosed with type 2 diabetes, the use of this formula for predicting VFA in healthy individuals is limited. To address this limitation, the Metabolic Score for Visceral Fat (METS-VF) was developed, which incorporates gender, age, and waist-height ratio in addition to METS-IR and has been shown to be effective in predicting elevated VFA, as well as the incidence of type 2 diabetes and hypertension.21
However, the association between anthropometric measurements and cardiometabolic diseases may vary based on patient group characteristics and ethnicity.22,23 Therefore, the purpose of our study was to evaluate the effectiveness of METS-VF compared to other commonly used anthropometric indices (BMI, WC, LAP, VAI, ABSI, and BRI) in predicting increased VFA and to determine its optimal cut-off value in young and middle-aged Turkish patients without diabetes and coronary artery disease.
Materials and Methods
Study Population
This single center and cross-sectional study was conducted between January 2022 and November 2022 with approval from the Ethics Committee of Istanbul Medeniyet University Göztepe Training and Research Hospital (Number: 2021/0464). The principles of the Declaration of Helsinki were followed throughout the study.
Patients who had undergone abdominal CT scans including the third lumbar vertebra (L3) level in the past two weeks for any reason and were between 20–50 years old were identified from the hospital’s electronic database. Those with known malignancies, diabetes, coronary artery disease, chronic inflammatory disease, those taking steroids or antihyperlipidemic drugs, and those with acute inflammation signs on CT were excluded from the study.
The remaining patients were contacted and invited to participate in the study and those who gave written consent were questioned about gender, age, medical history, medications and smoking status. Patients who used drugs that affect body fat distribution, such as glucocorticoids, or had weight changes in the last month were excluded.
As depicted in Figure 1, a total of 185 eligible patients were ultimately included in the study. The sample size was considered in accordance with the minimum ratio of participants to variables required in multivariate methods, which should be at least 5.24 In this study, a total of 11 predictor variables were used in the prediction of VFA. The ratio was found to be 185/11 = 17 and it was seen that the minimum sample size requirement was met according to the criteria.
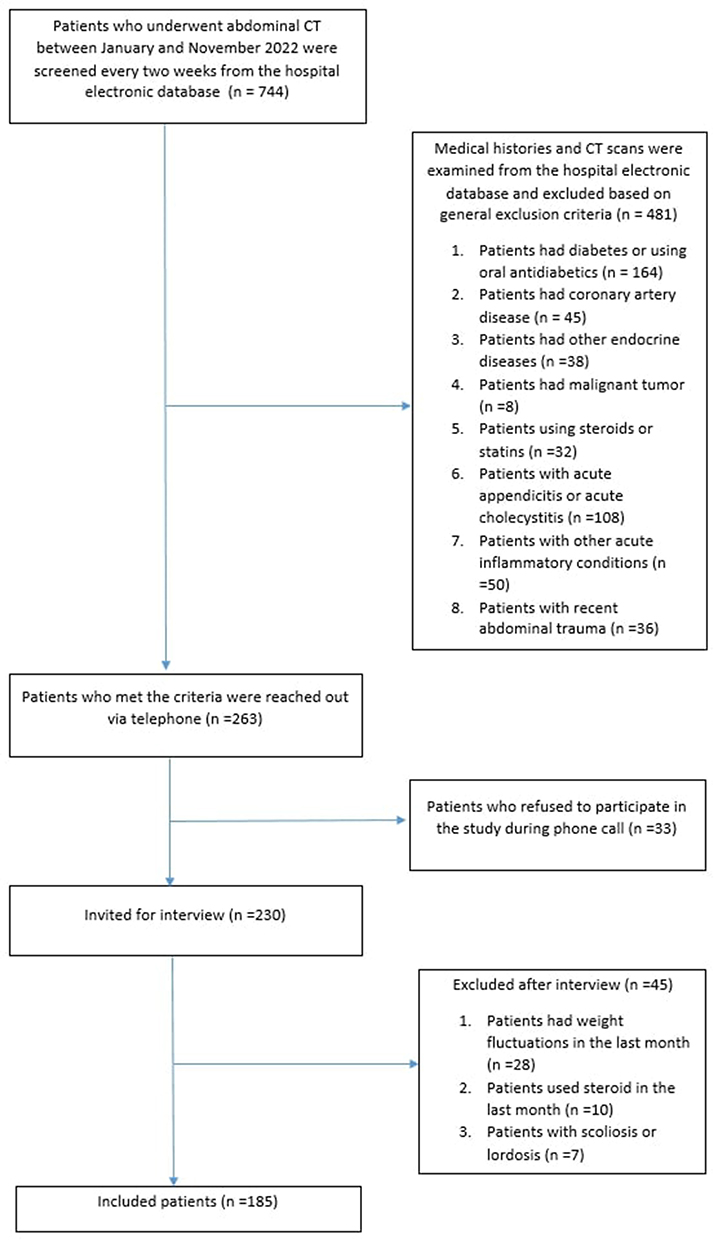 |
Figure 1 Flow diagram for inclusion and exclusion. |
Clinical Assessment
Each participant answered questions about their sociodemographic details, personal and family medical history (hypertension, diabetes, coronary artery disease, and hyperlipidemia), and smoking, using a standardized questionnaire.
The participant’s height (in centimeters) and weight (in kilograms) were assessed with a height scale and weight machine (SECA 799+220, seca GmbH & co, Germany). The body mass index (BMI) was computed using the formula weight in kg divided by height in m².
Waist circumference was measured using a non-flexible measuring tape at the narrowest point of the abdomen between the lower part of the last rib and the top of the hip at the end of expiration, while hip circumference was measured at the widest part of the hips.
Laboratory examinations were conducted after 8–12 h overnight fasting, including total cholesterol, triglycerides, high density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C) and fasting plasma glucose using the American AU480 automatic biochemical analyzer.
Blood pressure was measured three times in both arms of the participants using using an electronic sphygmomanometer (HEM-7155, Omron, Japan), after they had rested for 5–10 minutes. Periods of relaxation were incorporated between each of the different measurements, and the average value of three blood pressure measurements was taken into consideration.
Radiological Assessment
The patients were examined by 128-channel MDCT (GE Healthcare Optima CT660, USA). The slice thickness was set to be 1–2 mm and the reconstruction interval was 1.5–2 mm. Reformatted images were obtained in the sagittal and coronal planes. Visceral and subcutaneous fat tissue measurements were performed by two radiologists with 15 and 5 years of experience using Horos v3.3.6 medical image software (https://horosproject.org/). After determining the level of the L3 vertebrae from sagittal sections, measurements were made on the axial section passing through this level. First, a manual contour was placed on the skeletal muscles of the abdominal wall using a closed polygon tool in the axial CT image, and the visceral and subcutaneous fat tissues were separated (Figure 2). Then, the threshold image tool was used to obtain the fat density by grouping the image by density, based on a Hounsfield value between −190 and −30.25 Subsequently, measurements were obtained by marking the visceral and subcutaneous areas with manual annotation using the 2D growing Region of Interest (ROI) technique.
 |
Figure 2 Fat-measurement technique in CT. After manual contour (yellow line) was placed on the abdominal wall skeletal muscles, automatic measurements of visceral adipose tissue (A, red area) and subcutaneous adipose tissue (B, red area) areas were performed with threshold values. |
Definitions
The cut-off value for increased VFA was determined as 130 cm2, as commonly used in the literature and recommended for Turkish people in the Turkey Adult Risk Factor Survey (TEKHARF) study.26,27 The exposure of interests included BMI, WC, and five novel adiposity indices: LAP, VAI, ABSI, BRI, and METS-VF. Using the following equations they were determined:

 .12
.12

 .13
.13
 .17
.17
 .18
.18
 .20
.20
 .21
.21
WHtr: Waist (cm)/Height (cm)
Tg: Triglyceride,
*Binary response variable (male = 1, female = 0).
Using the criteria of the World Health Organization (WHO), participants were categorized into four groups based on their weight, including underweight (<18.5 kg/m²), normal weight (18.5–24.9 kg/m²), overweight (25–29.9 kg/m²), and obesity (≥30 kg/m²).2 Patients with and without metabolic syndrome were identified according to the National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATP III) criteria which is the most widely accepted method.10
Statistical Analysis
Descriptive statistics of the characteristics measured in the study participants were tabulated as mean, standard deviation (SD), quartiles (25th, median, 75th), number and % frequencies. The compatibility of the numerical characteristics with the normal distribution was examined with the Kolmogorov–Smirnov test and it was determined that they fit the normal distribution. The correlation of WC, WHR, BMI, and novel adiposity indices with VFA were analyzed by Pearson correlation analysis. The sensitivity, specificity and area under the curve (AUC) of the indices in identifying increased VFA was analyzed by receiver operating characteristic (ROC) curve and the optimal cut-off values were determined. P<0.05 was accepted as the level of statistical significance. SPSS (IBM Corp. Version 23.0. Armonk, NY) and R-4.2.2 for Windows program were used for calculations.
Results
In this study, 744 patients with CT imaging including the L3 vertebra level were retrospectively screened. Among them, 481 patients were excluded based on general exclusion criteria. A total of 263 patients were reached to be invited to participate in the study, 230 patients applied for the interview. During the interview, individuals with weight fluctuations (n = 28), current steroid consumption (n = 10), and scoliosis/lordosis (n = 7) were excluded based on the detailed anamnesis (Figure 1).
Finally, 185 subjects, including 77 males (41.6%) and 108 females (58.4%) with a mean age of 38.2 ± 8 years, were included. Of the participants, 2.2% were underweight, 43.2% were of normal weight, 28.6% were overweight, and 26% were obese based on their BMI. According to the NCEP ATP-III criteria, metabolic syndrome was diagnosed in 12 (15.6%) men and 20 (18.5%) women.
The descriptive statistics in Table 1 demonstrate that men had higher values for WC, WHR, height, weight, systolic blood pressure, LDL-C, triglycerides, METS-VF, and ABSI than women, while HDL-C and subcutaneous fat area were higher in women (p < 0.05 for all).
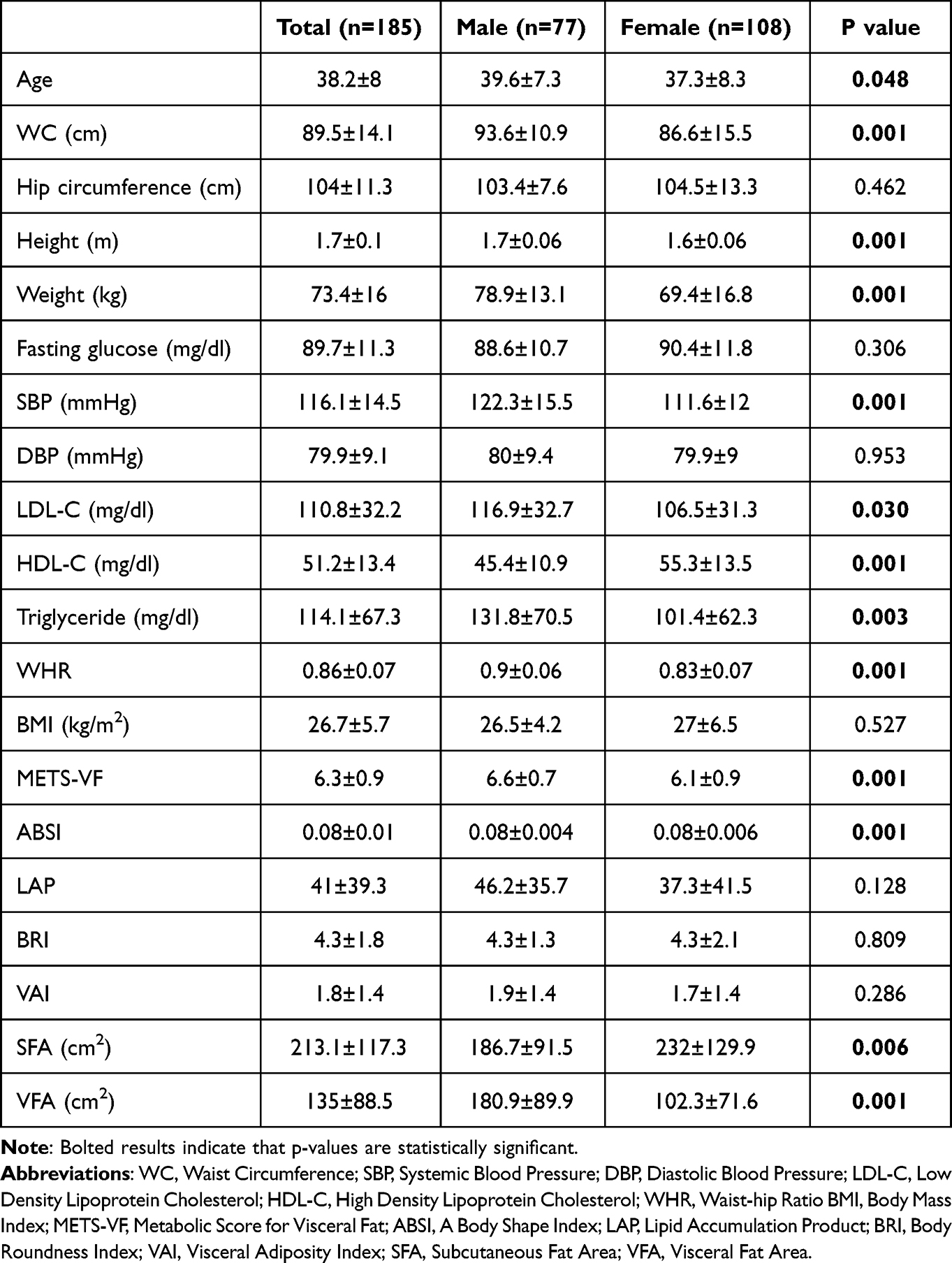 |
Table 1 Demographic and Clinical Characteristics of Participants |
There was a significant positive correlation between all indices and VFA (p <0.001 for all). Waist circumference (r=0.78 p < 0.001) and METS-VF (r=0.77 p < 0.001) had the strongest correlation with VFA. When the 95% CI of the correlation coefficients in Table 2 were analyzed, it was observed that the associations of WC and METS-VF with VFA were significantly stronger than the associations of ABSI, VAI and LAP with VFA.
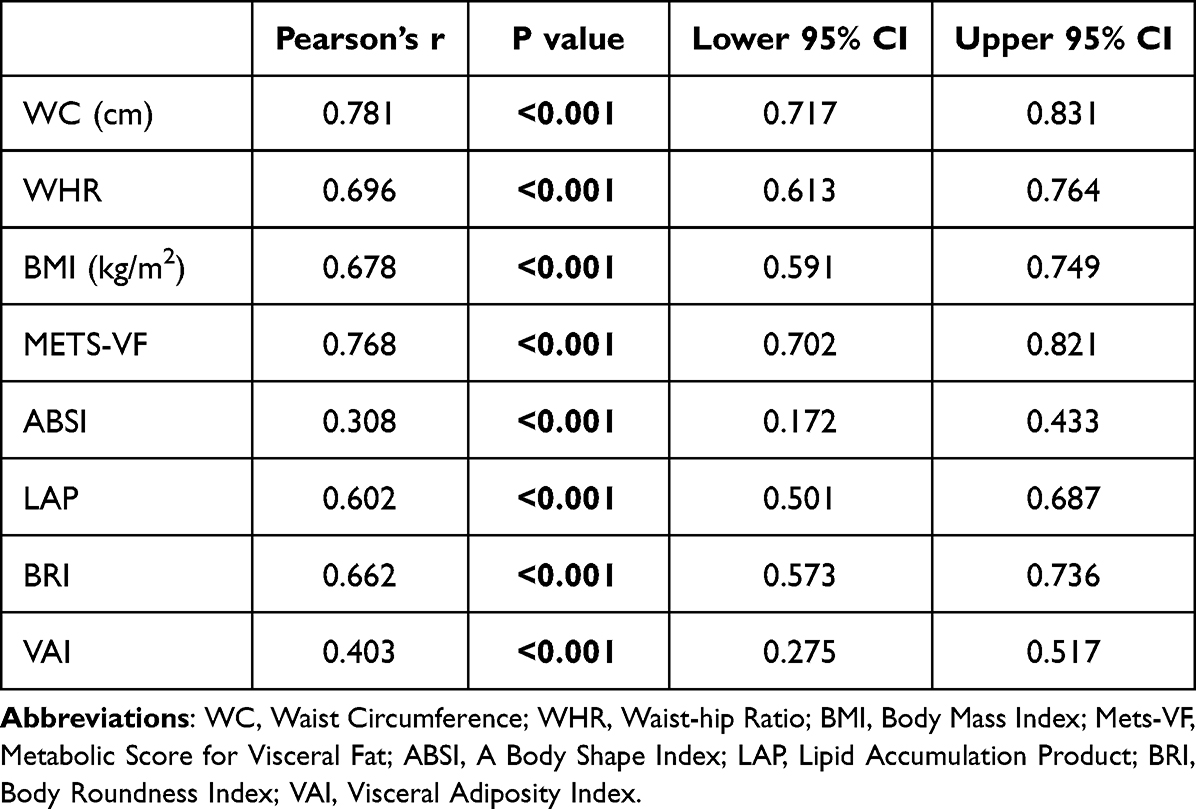 |
Table 2 Association of Adiposity Indices with Visceral Fat Area |
The cut-off values, classification success rates and AUCs of each method were calculated separately for males and females (Table 3). The Metabolic Score for Visceral Fat and WC demonstrated the highest predictive value in identifying increased VFA (>130 cm2) with AUCs of 0.94 for females and 0.92 for males. The AUC value of METS-VF was significantly higher than those of ABSI and VAI in both genders and higher than the AUC value of the WHR in women. However, the differences between METS-VF and the other indices were not significant (Table 4).
 |
Table 3 Cut-Off Values and Classification Accuracy of Adiposity Indices in Identifying Increased Visceral Fat Area |
 |
Table 4 P-values Obtained as a Result of Comparing the AUC Values of the Adiposity Indices |
Discussion
This study showed that all investigated adiposity indices were significantly correlated with VFA. Metabolic Score for Visceral Fat and WC were the two best methods for identifying increased VFA (>130 cm2). In men, a METS-VF cut-off point of >6.4 and a WC cut-off point of >88 cm were identified, while in women, the corresponding cut-off points were >6.5 and >90.5 cm, respectively.
Metabolic syndrome is often linked to obesity as a significant risk factor, but it’s worth noting that even lean individuals can exhibit insulin resistance, which is a key component of the metabolic syndrome.28 The amount and distribution of body fat, rather than overall weight, is the crucial factor in the increased risk associated with obesity. Specifically, visceral adiposity is strongly associated with adipocyte dysfunction and related cardiometabolic risks.29 This study represents the first investigation into the link between METS-VF and visceral adiposity in apparently healthy Turkish people.
In this study, a strong correlation (r=0.77) was found between METS-VF and visceral adiposity, and the formula had a high AUC value (>0.9) in identifying increased VFA at optimal cut-off values. The first validation study of the formula included 350 patients, 34.8% of whom had diabetes and a mean BMI of 40.1 kg/m2, from bariatric surgery clinics in India.30 It demonstrated that a METS-VF score above 7.3 predicted increased VFA with an AUC of 0.78. A recent study by Antonio-Villa et al excluded patients with diabetes, similar to our study, and found that METS-VF strongly correlated with VFA (r=0.75) and effectively identified subjects with increased VFA (AUC 0.84), consistent with our findings.31 These results suggest that the higher AUC values found compared to the Indian study may be attributed to differences in patient selection, and that METS-VF may be more suitable for identifying individuals at high cardiometabolic risk before the onset of metabolic complications. Notably, the group in which the METS-VF was developed excluded individuals with cardiovascular disease, those taking oral antidiabetic drugs other than metformin, and those with diabetic complications.
In a study with 5275 individuals (3083 Inuit, 1397 Africans and 795 Europeans), it was demonstrated that anthropometric measures like BMI and WC do not reflect the same amount of VFA across ethnic groups. Therefore, it is necessary to demonstrate the performance of the anthropometric measurements for VFA estimation in different ethnic groups and determine the cut-off values for each ethnic group.32 Although METS-VF was originally created for the Mexican population, our data and data from India indicate a strong correlation between METS-VF and VFA, which suggests its potential usefulness as a reliable predictor of visceral adiposity across different populations. It’s important to note that formulas based on anthropometric measurements may produce varying results depending on patient characteristics, and study design. In our study, the reason for the difference in the METS-VF cut-off value from the original study can be explained by a variation in the threshold chosen for increased VFA.
Lipid accumulation product and VAI are methods based on the concept of hypertriglyceridemic waist circumference, which is based on the importance of body fat distribution.12,13 Although LAP and VAI have been used to estimate the risk associated with visceral adiposity, it is important to remember that neither method was designed to predict the amount of VAT. In some of previous studies, both methods had a weak association with the VFA when compared with traditional anthropometric measurements, which is consistent with the results of our study.33,34
A body shape index and BRI are methods that use anthropometric measurements and do not require blood sampling.17,18 In the study by Krakauer et al. ABSI was found to be successful in predicting the incidence of mortality.17 However, subsequent studies have shown that ABSI has less ability to predict the incidence of metabolic syndrome and diabetes compared to both traditional and novel anthropometric indices.35,36 Although clinical outcomes were not analyzed in our study, ABSI was shown to have the weakest association with VFA. In a cross-sectional study conducted by Liu et al in China with 233 patients the relationship between WC, ABSI and BRI with VFA was examined and the relationship of ABSI was shown to be weaker (p<0.05) compared to the other two methods.37 These results suggest that ABSI is not a good method to predict visceral adiposity and associated risk factors. In a study, BRI has been shown to be better than most other anthropometric indices in predicting the incidence of cardiometabolic disease.38 The strong association of BRI with VFA in our study is consistent with the results of previous studies comparing the association of anthropometric indices with visceral adiposity.37
It is an expected finding that WC and BMI are strongly associated with VFA, but it is noteworthy that their associations with VFA are stronger than other adiposity indices except METS-VF. The results of a small number of studies comparing the association of traditional and novel anthropometric indices with VFA also reveal a strong association between traditional methods and VFA, similar to our study.34
In this study, WC, which has strong correlation with VFA, appears to be a convenient and easy method to assess visceral adiposity in a healthy Turkish population. It is noteworthy that the WC value corresponding to increased VFA is found to be higher in women than men. In the TEKHARF study conducted in Türkiye, it was shown that WC values of 95 cm in males and 83 cm in females were associated with increased metabolic risk.39,40 In another study reported from Türkiye, WC of 83 cm in females and 93 cm in males were determined as cut-off values for cardiometabolic risk associated with insulin resistance.41 Lemieux et al showed that approximately 95 cm was successful in predicting increased VFA (>130 cm2) in both sexes.42 When these studies are evaluated together, it can be understood that the WC cut-off values vary according to the characteristics of the population and the endpoint of the studies. Our findings suggest that WC limits may be closer to each other in males and females in our country and show the need for more comprehensive studies.
Our main limitation is that CT examinations were not performed prospectively. Although we excluded patients with a major or critical medical condition on CT evaluation, this may have resulted in selection bias from the general population. Another limitation is the measurement of cross-sectional VFA instead of total VAT volume from CT. Although cross-sectional areas measured at the appropriate level from abdominal CT correlated well with total VAT, this method may have prevented us from fully estimating the VAT burden of the participants.8 Lastly, the study included patients between the ages of 20 and 50 years, which means the results may not be applicable to elderly patients. On the other hand, our study has many strength. First, we excluded all conditions that may affect the body fat distribution and the results of the used indices increases the reliability of our study. Second, we provide detailed interpretation of many anthropometric indices and AUC-ROC analysis for diagnostic accuracy. Our study also proposes optimal cut-off points for these indices.
To conclude, METS-VF is a recently developed formula for estimating visceral adiposity which is a significant risk factor for cardiometabolic comorbidities. Our study found a strong association between METS-VF and visceral adiposity, suggesting that it is a reliable index for predicting increased VFA in both Turkish men and women. However, due to its ease of use, WC measurement may be more practical for screening purposes. Nonetheless, more comprehensive studies with patients with different characteristics and ages are needed to further support these findings.
Data Sharing Statement
De-identified individual participant data collected during this trial will be shared from 2 years to 5 years after article publication. These data will be available to researchers who provide a methodologically sound proposal for the purposes of achieving specific aims outlined in that proposal. Proposals should be directed to Cundullah Torun via email ([email protected]) and will be reviewed by him. To gain access, data requesters will need to sign a data access agreement and to confirm that data will only be used for the agreed purpose for which access was granted.
Acknowledgments
We confirm that Ethical Committee approval was sought where necessary and guidelines on patient consent have been met and any details of informed consent obtained are indicated within the text of the submitted manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no competing interests in this work.
References
1. Satman I, Omer B, Tutuncu Y, et al. Twelve-year trends in the prevalence and risk factors of diabetes and prediabetes in Turkish adults. Eur J Epidemiol. 2013;28(2):169–180. doi:10.1007/s10654-013-9771-5
2. World Health Organization. Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser. 2000;894:i–xii, 1–253. PMID: 11234459.
3. Vague J. The degree of masculine differentiation of obesities: a factor determining predisposition to diabetes, atherosclerosis, gout, and uric calculous disease. Am J Clin Nutr. 1956;4(1):20–34. doi:10.1093/ajcn/4.1.20
4. Ibrahim MM. Subcutaneous and visceral adipose tissue: structural and functional differences. Obes Rev. 2010;11(1):11–18. doi:10.1111/j.1467-789X.2009.00623.x
5. Pouliot MC, Després JP, Nadeau A, et al. Visceral obesity in men. Associations with glucose tolerance, plasma insulin, and lipoprotein levels. Diabetes. 1992;41(7):826–834. doi:10.2337/diab.41.7.826
6. Cnop M, Landchild MJ, Vidal J, et al. The concurrent accumulation of intra-abdominal and subcutaneous fat explains the association between insulin resistance and plasma leptin concentrations: distinct metabolic effects of two fat compartments. Diabetes. 2002;51(4):1005–1015. doi:10.2337/diabetes.51.4.1005
7. Shen W, Punyanitya M, Wang Z, et al. Visceral adipose tissue: relations between single-slice areas and total volume. Am J Clin Nutr. 2004;80(2):271–278. doi:10.1093/ajcn/80.2.271
8. Kvist H, Chowdhury B, Grangård U, Tylén U, Sjöström L. Total and visceral adipose-tissue volumes derived from measurements with computed tomography in adult men and women: predictive equations. Am J Clin Nutr. 1988;48(6):1351–1361. doi:10.1093/ajcn/48.6.1351
9. Pouliot MC, Després JP, Lemieux S, et al. Waist circumference and abdominal sagittal diameter: best simple anthropometric indexes of abdominal visceral adipose tissue accumulation and related cardiovascular risk in men and women. Am J Cardiol. 1994;73(7):460–468. doi:10.1016/0002-9149(94)90676-9
10. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA. 2001;285(19):2486–2497. doi:10.1001/jama.285.19.2486
11. Lemieux I, Pascot A, Couillard C, et al. Hypertriglyceridemic waist: a marker of the atherogenic metabolic triad (hyperinsulinemia; hyperapolipoprotein B; small, dense LDL) in men? Circulation. 2000;102(2):179–184. doi:10.1161/01.CIR.102.2.179
12. Kahn HS. The “lipid accumulation product” performs better than the body mass index for recognizing cardiovascular risk: a population-based comparison. BMC Cardiovasc Disord. 2005;5(1):26. doi:10.1186/1471-2261-5-26
13. Amato MC, Giordano C, Galia M, et al. Visceral Adiposity Index: a reliable indicator of visceral fat function associated with cardiometabolic risk. Diabetes Care. 2010;33(4):920–922. doi:10.2337/dc09-1825
14. Chiang J-K, Koo M. Lipid accumulation product: a simple and accurate index for predicting metabolic syndrome in Taiwanese people aged 50 and over. BMC Cardiovasc Disord. 2012;12(1):78. doi:10.1186/1471-2261-12-78
15. Oh JY, Sung YA, Lee HJ. The visceral adiposity index as a predictor of insulin resistance in young women with polycystic ovary syndrome. Obesity. 2013;21(8):1690–1694. doi:10.1002/oby.20096
16. Wang B, Zhang M, Liu Y, et al. Utility of three novel insulin resistance-related lipid indices for predicting type 2 diabetes mellitus among people with normal fasting glucose in rural China. J Diabetes. 2018;10(8):641–652. doi:10.1111/1753-0407.12642
17. Krakauer NY, Krakauer JC, Li S. A new body shape index predicts mortality hazard independently of body mass index. PLoS One. 2012;7(7):e39504. doi:10.1371/journal.pone.0039504
18. Thomas DM, Bredlau C, Bosy-Westphal A, et al. Relationships between body roundness with body fat and visceral adipose tissue emerging from a new geometrical model. Obesity. 2013;21(11):2264–2271. doi:10.1002/oby.20408
19. Rico-Martín S, Calderón-García JF, Sánchez-Rey P, Franco-Antonio C, Martínez Alvarez M, Sánchez Muñoz-Torrero JF. Effectiveness of body roundness index in predicting metabolic syndrome: a systematic review and meta-analysis. Obes Rev. 2020;21(7):e13023. doi:10.1111/obr.13023
20. Bello-Chavolla OY, Almeda-Valdes P, Gomez-Velasco D, et al. METS-IR, a novel score to evaluate insulin sensitivity, is predictive of visceral adiposity and incident type 2 diabetes. Eur J Endocrinol. 2018;178(5):533–544. doi:10.1530/EJE-17-0883
21. Bello-Chavolla OY, Antonio-Villa NE, Vargas-Vázquez A, et al. Metabolic Score for Visceral Fat (METS-VF), a novel estimator of intra-abdominal fat content and cardio-metabolic health. Clin Nutr. 2020;39(5):1613–1621. doi:10.1016/j.clnu.2019.07.012
22. McKeigue PM, Shah B, Marmot MG. Relation of central obesity and insulin resistance with high diabetes prevalence and cardiovascular risk in South Asians. Lancet. 1991;337(8738):382–386. doi:10.1016/0140-6736(91)91164-P
23. Bodicoat DH, Gray LJ, Henson J, et al. Body mass index and waist 398 circumference cut-points in multi-ethnic populations from the UK and India: the ADDITION399 Leicester, Jaipur heart watch and New Delhi cross-sectional studies. PLoS One. 2014;9(3):e90813. doi:10.1371/journal.pone.0090813
24. Baeza-Delgado C, Cerdá Alberich L, Carot-Sierra JM, et al. A practical solution to estimate the sample size required for clinical prediction models generated from observational research on data. Eur Radiol Exp. 2022;6(1):22. doi:10.1186/s41747-022-00276-y
25. Silva A, Gomes F, Pereira SS, Monteiro MP, Araújo A, Faria G. Visceral obesity is associated with lower stage colon tumors in males without survival advantage. Surg Oncol. 2021;37:101606. doi:10.1016/j.suronc.2021.101606
26. Després JP, Lamarche B. Effects of diet and physical activity on adiposity and body fat distribution: implications for the prevention of cardiovascular disease. Nutr Res Rev. 1993;6(1):137–159. doi:10.1079/NRR19930010
27. Onat A, Uğur M, Can G, Yüksel H, Hergenç G. Visceral adipose tissue and body fat mass: predictive values for and role of gender in cardiometabolic risk among Turks. Nutrition. 2010;26(4):382–389. doi:10.1016/j.nut.2009.05.019
28. Buscemi S, Chiarello P, Buscemi C, et al. Characterization of metabolically healthy obese people and metabolically unhealthy normal-weight people in a general population cohort of the ABCD study. J Diabetes Res. 2017;2017:9294038. doi:10.1155/2017/9294038
29. Neeland IJ, Ross R, Després JP, et al.; International Atherosclerosis Society; International Chair on Cardiometabolic Risk Working Group on Visceral Obesity. Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: a position statement. Lancet Diabetes Endocrinol. 2019;7(9):715–725. doi:10.1016/S2213-8587(19)30084-1
30. Kapoor N, Jiwanmall SA, Nandyal MB, et al. Metabolic score for visceral fat (METS-VF) estimation - A novel cost-effective obesity indicator for visceral adipose tissue estimation. Diabetes Metab Syndr Obes. 2020;13:3261–3267. doi:10.2147/DMSO.S266277
31. Antonio-Villa NE, Juárez-Rojas JG, Posadas-Sánchez R, Reyes-Barrera J, Medina-Urrutia A. Visceral adipose tissue is an independent predictor and mediator of the progression of coronary calcification: a prospective sub-analysis of the GEA study. Cardiovasc Diabetol. 2023;22(1):81. doi:10.1186/s12933-023-01807-6
32. Rønn PF, Andersen GS, Lauritzen T, et al. Ethnic differences in anthropometric measures and abdominal fat distribution: a cross-sectional pooled study in Inuit, Africans and Europeans. J Epidemiol Commun Health. 2017;71(6):536–543. doi:10.1136/jech-2016-207813
33. Wander PL, Hayashi T, Sato KK, et al. Design and validation of a novel estimator of visceral adipose tissue area and comparison to existing adiposity surrogates. J Diabetes Complicat. 2018;32(11):1062–1067. doi:10.1016/j.jdiacomp.2018.09.004
34. Elisha B, Messier V, Karelis A, et al. The Visceral Adiposity Index: relationship with cardiometabolic risk factors in obese and overweight postmenopausal women--A MONET group study. Appl Physiol Nutr Metab. 2013;38(8):892–899. doi:10.1139/apnm-2012-0307
35. Wu K, He S, Zheng Y, Chen X. ABSI is a poor predictor of insulin resistance in Chinese adults and elderly without diabetes. Arch Endocrinol Metab. 2018;62(5):523–529. doi:10.20945/2359-3997000000072
36. Yang J, Wang F, Wang J, et al. Using different anthropometric indices to assess prediction ability of type 2 diabetes in elderly population: a 5 year prospective study. BMC Geriatr. 2018;18(1):218. doi:10.1186/s12877-018-0912-2
37. Liu J, Fan D, Wang X, Yin F. Association of two novel adiposity indicators with visceral fat area in type 2 diabetic patients: novel adiposity indexes for type 2 diabetes. Medicine. 2020;99(19):e20046. doi:10.1097/MD.0000000000020046
38. Liu B, Liu B, Wu G, Yin F. Relationship between body-roundness index and metabolic syndrome in type 2 diabetes. Diabetes Metab Syndr Obes. 2019;12:931–935. doi:10.2147/DMSO.S209964
39. Onat A, Uyarel H, Hergenç G, Karabulut A, Albayrak S, Can G. Determinants and definition of abdominal obesity as related to risk of diabetes, metabolic syndrome and coronary disease in Turkish men: a prospective cohort study. Atherosclerosis. 2007;191(1):182–190. doi:10.1016/j.atherosclerosis.2006.03.012
40. Onat A, Sari I, Hergenç G, et al. Predictors of abdominal obesity and high susceptibility of cardiometabolic risk to its increments among Turkish women: a prospective population-based study. Metabolism. 2007;56(3):348–356. doi:10.1016/j.metabol.2006.10.016
41. Uzunlulu M, Oğuz A, Aslan G, Karadağ F. Cut-off values for waist circumference in Turkish population: is there a threshold to predict insulin resistance? Turk Kardiyol Dern Ars. 2009;37(6):17–23.
42. Lemieux S, D P, Bouchard C, Tremblay A, Després JP. A single threshold value of waist girth identifies normal-weight and overweight subjects with excess visceral adipose tissue. Am J Clin Nutr. 1996;64(5):685–693. doi:10.1093/ajcn/64.5.685
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.