Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Is Intermittent Fasting Better Than Continuous Energy Restriction for Adults with Overweight and Obesity?
Authors Ye YF ![]() , Zhang MX
, Zhang MX ![]() , Lin Z, Tang L
, Lin Z, Tang L ![]()
Received 2 June 2022
Accepted for publication 31 August 2022
Published 15 September 2022 Volume 2022:15 Pages 2813—2826
DOI https://doi.org/10.2147/DMSO.S376409
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Gian Paolo Fadini
Ya-Fei Ye,1,2 Mei-Xian Zhang,3 Zhi Lin,4 Leiwen Tang5
1Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, 310016, People’s Republic of China; 2Health Management Centre, Taizhou Hospital, Zhejiang University, Linhai, 317000, People’s Republic of China; 3Evidence-Based Medicine Center, Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University, Linhai, 317000, People’s Republic of China; 4Operating Rooms, Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University, Linhai, 317000, People’s Republic of China; 5Nursing Department, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, 310016, People’s Republic of China
Correspondence: Leiwen Tang, Nursing Department, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, No. 3 East Qingchun Road, Hangzhou, 310016, People’s Republic of China, Tel/Fax +86-571-86006438, Email [email protected]
Abstract: As a popular weight management intervention, intermittent fasting (IF) has been widely applied to the treatment of overweight and obesity in adults. This review describes the different forms and implementation protocols of IF and their effects on body weight, body composition, cardiometabolic risk factors and other diseases. The existing evidence suggests that IF is as effective as continuous energy restriction and may be a feasible and effective approach to weight loss.
Keywords: overweight, obesity, intermittent fasting, continuous energy restriction, weight management
Introduction
Overweight and obesity have become global health issues. In 2016, China had the highest number of adults with overweight and obesity at 600 million, with rates of 34.3% and 16.4%, respectively.1,2 Overweight and obesity are major risk factors for and increase the risk of all-cause mortality from chronic diseases such as cardiovascular disease, diabetes, and cancer, reducing life expectancy by five to twenty years.3 Weight loss can significantly diminish the risk of developing overweight and obesity. Two popular weight management strategies are Continuous Energy Restriction (CER)4 and Intermittent Fasting (IF).5 The former achieves weight loss through continuous restriction of daily energy intake, but the resultant hunger reduces adherence to the regimen, which can lead to greater weight regain once the restriction on intake is removed.6 As a new method to prevent and treat obesity, IF restricts calorie intake through alternate fasting and free eating, which can also achieve weight loss, improve metabolic status, and enhance the immune system and cognitive function in a relatively short period of time in a manner similar to CER.7 However, the beneficial effects of IF on weight loss, body composition, and cardiovascular health in adults with overweight and obesity with diverse characteristics are controversial, and may be influenced by factors such as comorbidities and the duration of fasting. This review examines the different strategies and protocols used for IF, through the comparison between the effects of IF and CER on weight loss, with the aim of providing a reference for its broader clinical application for weight loss in adults with overweight and obesity.
Common Forms of IF
Alternate-Day Fasting (ADF)
ADF alternates between fasting and free-eating days to achieve weight loss. On fasting days, individuals consume only 25% of their basal calories (approximately 500 kcal), whereas on eating days, there is no restriction on calorie intake.8 Individuals with overweight and obesity can lose 3%–7% of their body weight after two to three months of ADF, which is accompanied by improvements in blood lipids, blood pressure, and insulin sensitivity.9 However, a Randomized Controlled Trial (RCT) showed that ADF had no advantages over CER in terms of compliance, weight loss or maintenance, and cardioprotection in adults with obesity and normal metabolism.10 A systematic review found that ADF was effective for short-term (two to three months) weight loss in individuals with normal weight, overweight, and obesity, although there are no long-term follow-up data. Additionally, ADF is not suitable for individuals who require regular feeding or medication such as pregnant and lactating women, elderly people, or patients with type 1 diabetes or eating disorders.11 Despite its widespread adoption, compared with CER, ADF may be less sustainable in the long term for most individuals with overweight and obesity because of the intense feeling of hunger elicited by low-calorie intake on fasting days.10
5:2 Fasting
The best-selling book “The Fast Diet” published by Mosley et al in 2013 touted the benefits of severely restricting energy intake for two days a week but eating normally during the rest of the week.12 Since then, the 5:2 fasting has become more and more popular, which involved restricting energy intake to 25%–30% of the usual level on two nonconsecutive days within a week with no restriction on the remaining five days.13 Some researchers have concluded that the 5:2 fasting method is as effective as CER in reducing weight and improving glucose and lipid metabolism, waist-to-hip ratio, and insulin sensitivity.14 Compared with ADF, 5:2 fasting can lessen the feeling of hunger and is associated with fewer undesirable reactions such as dizziness, constipation, nausea, and vomiting during the weight loss process,15,16 which encourages adherence for people with overweight and obesity. Additionally, 5:2 fasting has been shown to reduce basal metabolic rate and skeletal muscle mass.17 The effect of 5:2 fasting on weight maintenance warrants further investigation.
Time-Restricted Eating (TRE)
TRE is an IF method that requires subjects to eat within a fixed period of 8–10 h or less per day and fast at other times18 to maintain a stable circadian rhythm in their calorie intake. Compared with ADF and 5:2 fasting, TRE only limits daily meal times and not the types or quantity of food, making it more acceptable to patients and facilitating adherence. The effect of TRE on weight loss was significantly correlated with the time of carbohydrate and protein intake;19 people who ate earlier in the day lost more weight than those who ate later.20 Meanwhile, eating more staple foods in the evening was not beneficial for weight loss. In a 12-week RCT, women with overweight or obesity who consumed a high-calorie breakfast had better fasting glucose, insulin sensitivity, and blood lipids than those who consumed a high-calorie dinner.21 This result is consistent with the latest findings from healthy non-obese volunteers showing that 16:8 IF was more beneficial when food was consumed between 06:00 and 15:00 (ie, early eating) vs 11:00 and 20:00 (midday eating).22 Another study found that 12 weeks of TRE with a mealtime between 12:00 and 08:00 did not lead to weight loss in adults with overweight and obesity without controlling food intake but resulted in loss of muscle mass.23 However, in an RCT of TRE (08:00–16:00) for 12 months, there was no significant loss of muscle mass, and regardless of the time of calorie intake, TRE had a significant impact on weight loss when total calories were restricted and was found to be a safe and effective strategy for weight management.24 As there is no restriction on calorie intake and uniform regulation of allowed eating times in TRE, different studies have reported variable results. Nonetheless, the data suggest that reducing total calorie intake by limiting eating time, especially to earlier times of the day, is a beneficial weight management strategy. Given these findings, people with overweight and obesity should consider changing their traditional concept of dinner as a social meal in order to maximize weight loss.
Irrespective of the duration of the intervention (short term [4–12 weeks] or long term [24–102 weeks]), weight loss with ADF and 5:2 fasting was comparable to that achieved by calorie restriction (CR).10,14,15,25–34 Meanwhile, weight loss with TRE alone (1%–5% decrease from baseline over 8–12 weeks)23,35,36 was not superior to that achieved with CR and was less than that observed with ADF or 5:2 fasting unless total calorie intake was restricted along with TRE. Thus, long-term TRE combined with an appropriate energy-restricted diet can enhance weight loss, but this is mainly attributed to CR.24,37
Summarizing the effects of three forms of IF on clinical outcomes reported in the literature (Table 1), it shows that there have been no trials directly comparing the effects of the three different fasting methods; further research is needed to determine which methods are more effective for achieving weight loss.
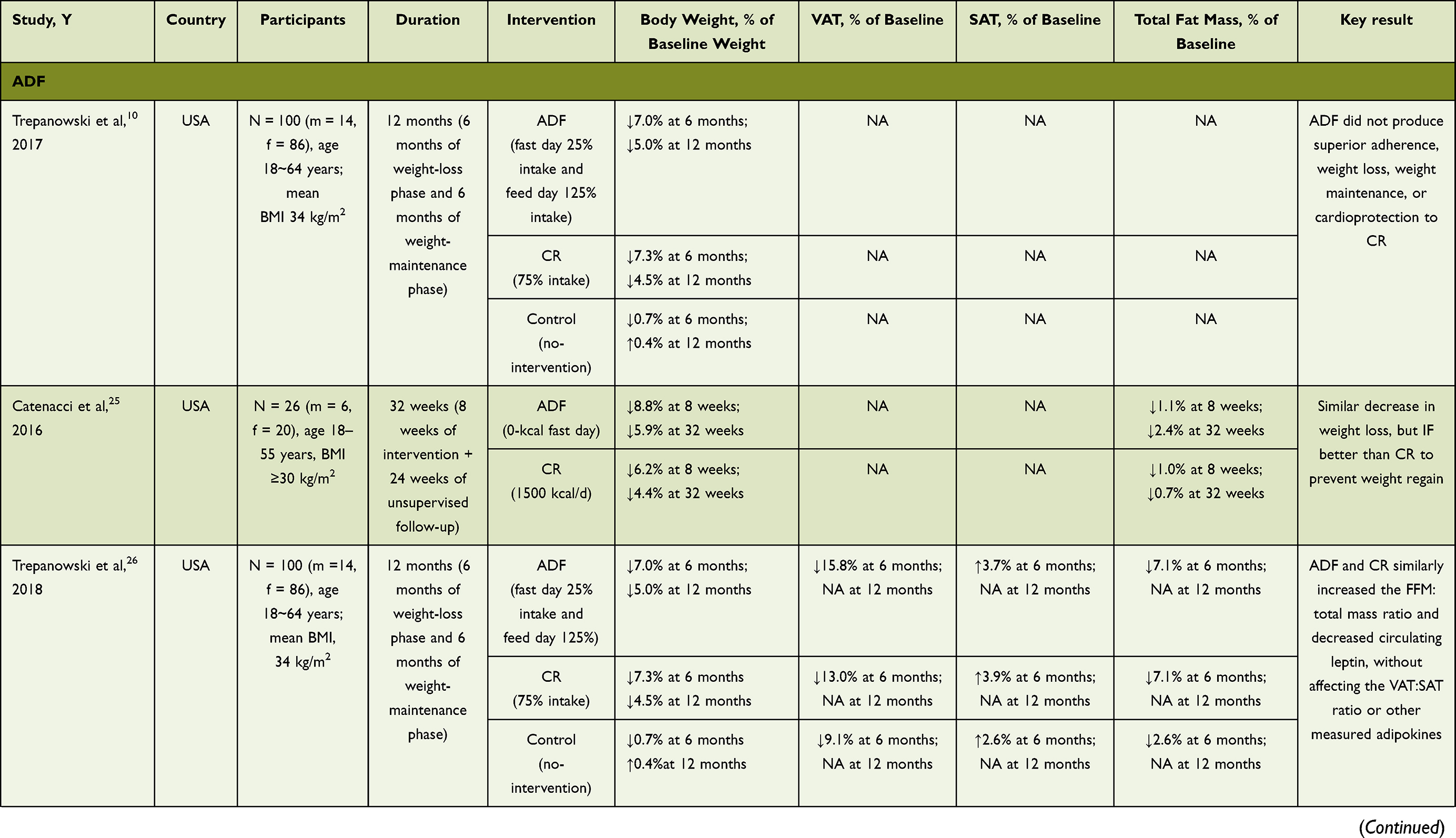 | 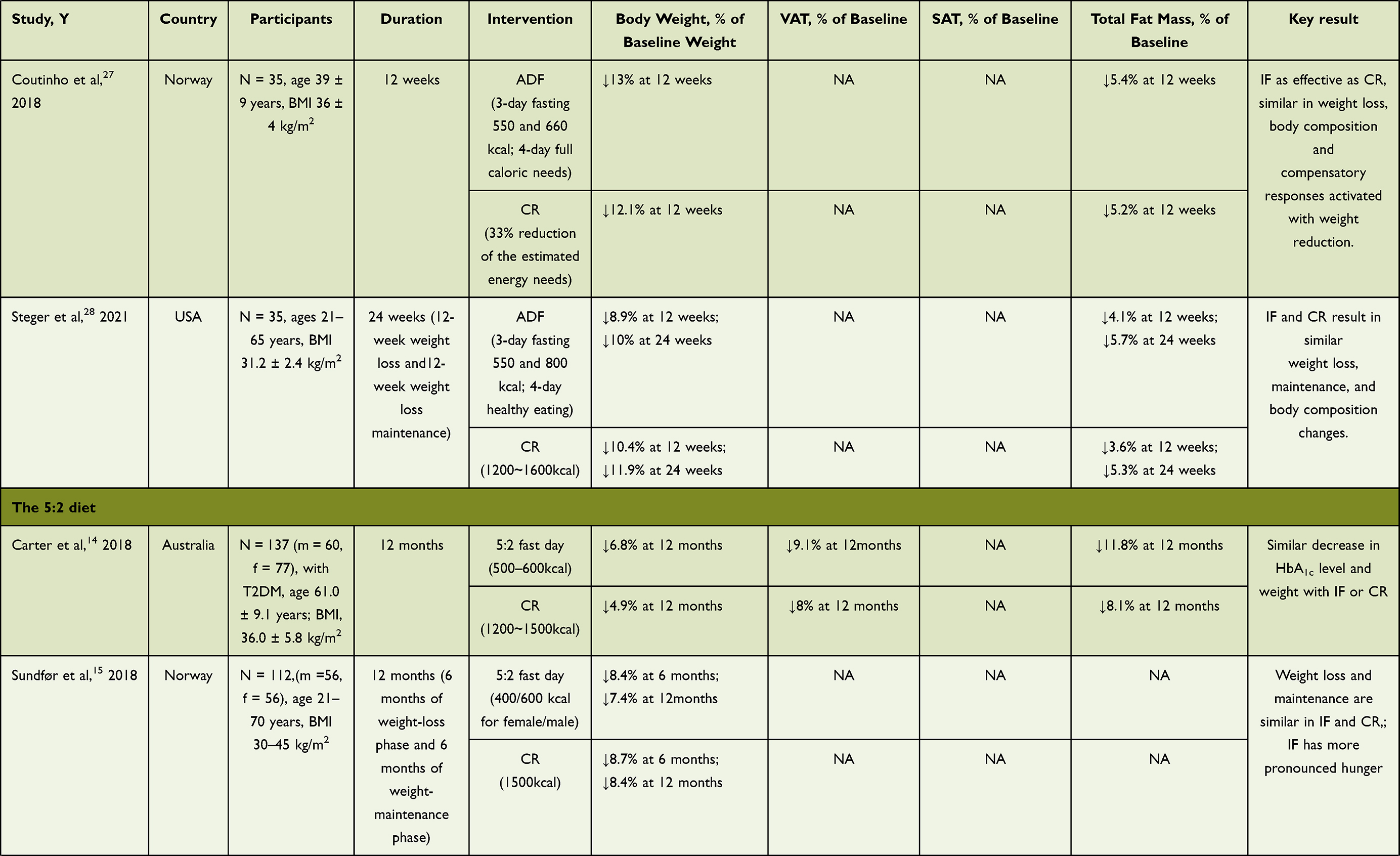 | 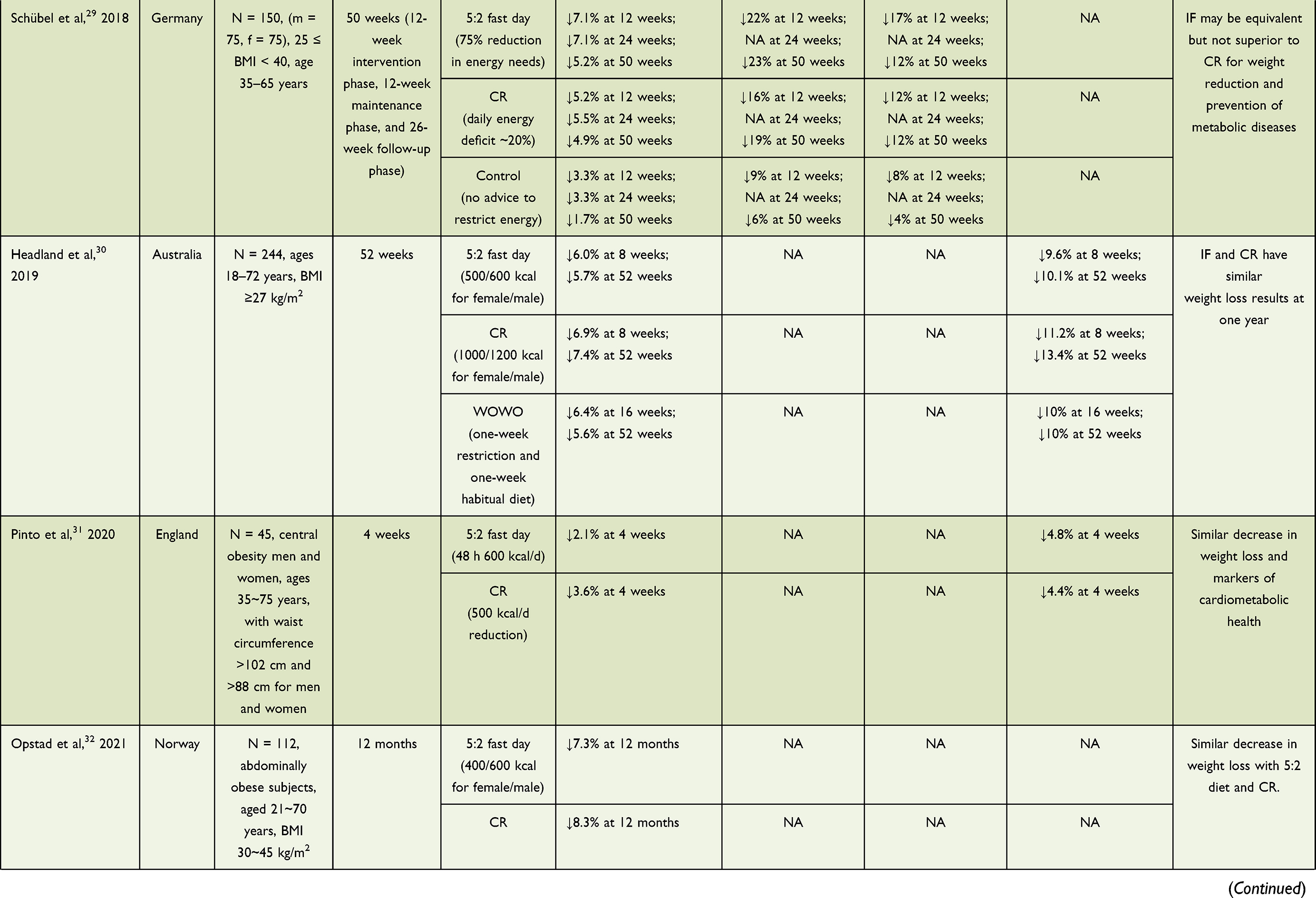 |
Table 1 Randomized Controlled Trials of IF and CR in Adults with Overweight and Obesity |  |
IF Combined with Other Interventions
IF Combined with Exercise
Many studies on IF have controlled only dietary factors and neglected the long-term effects of exercise on weight. In a study of 64 patients with obesity, IF combined with endurance exercise of moderate intensity three times a week resulted in greater reductions in body weight, body fat mass (FM), and lipid-related indicators after 12 weeks than IF or exercise alone, although there were no significant differences in lean body mass (LBM) between groups.38 Another study showed that the combination of resistance and aerobic exercise three times a week combined with IF led to larger reductions in body weight and FM than exercise alone although these parameters did not differ with respect to the IF group; on the other hand, exercise had a greater effect on cholesterol metabolism than IF or CR.39 Adults with overweight or obesity are more prone to knee joint damage in activities like running, climbing, and basketball,40 which negatively impacts their persistence with an exercise-based intervention. Effective muscle mass can be maintained by increasing protein intake and engaging in a reasonable exercise regimen. One study found that young people who fasted for 16 h a day over a 2-month period with resistance training had a reduction in body fat percentage while maintaining muscle mass;41 and a systematic review of 332 subjects showed that postprandial exercise was more effective in preventing hyperglycemia and enhancing insulin sensitivity than preprandial exercise.42 Thus, IF combined with exercise can improve the aerobic capacity of skeletal muscle, resulting in greater weight loss and providing more health benefits than IF24 or exercise alone.38
IF Combined with Meal Replacement
IF combined with meal replacement is a common weight loss intervention that has the advantage of not only allowing quantification of calorie intake on fasting days but also reducing malnutrition. In a single-blind randomized cross-over trial of eight healthy young women, processed meal replacements with a precisely calculated scientific nutrition ratio increased postprandial caloric expenditure and promoted carbohydrate oxidation to a greater extent than whole-food meals with the same total calories. Moreover, there were no differences among subjects in postprandial blood glucose response, satiety, feeling of hunger, and desire to eat, demonstrating that the processed meal replacements were an effective strategy for preventing and treating obesity.43
In a study of 164 adults with overweight or obesity that were divided into two groups using IF combined with a high protein meal replacement or the protein meal replacement alone, both groups showed significant reductions in weight, body fat, visceral fat, and LBM at week 16 with no significant differences between them. However, the combined intervention reduced participants’ cravings for food, thus improving their compliance and more effectively preventing weight regain within six months.44 In a multicenter clinical study of 300 individuals with overweight or obesity in China, a dietary program consisting of 500–600 kcal solid drinks as meal replacement on IF days not only led to body weight reduction and maintenance of weight loss but also decreased the incidence of clinical symptoms such as mouth ulcers, constipation, hair loss, and insomnia experienced by the subjects during the weight loss process.45 Another study conducted in China on patients with type 2 diabetes with comorbid obesity found that combined use of food substitutes during fasting periods safely and effectively improved metabolic indices such as blood glucose, blood pressure, and lipids; reduced body weight; improved patient compliance; and achieved stable and lasting glycemic control.46 However, whether this method is effective in improving metabolic indices in type 2 diabetes patients with normal weight remains to be determined. In a study of healthy adults with overweight and obesity using meal replacements on fasting days, short-term fasting (4 weeks) resulted in greater weight loss and improved body composition and cardiometabolic health without exacerbating the feeling of hunger or adversely affecting appetite.47 The investigators also found that two days of fasting per week was more beneficial than one day. Higher protein intake and more frequent eating were shown to reduce the amount of total and abdominal fat and improved LBM and postprandial thermogenesis; both were effective for long-term weight maintenance and are feasible for patients with overweight or obesity.48,49
IF Combined with Psychological Intervention
Obesity may be associated with psychological problems such as depression, body image disorders, stress, and low self-esteem.50 Furthermore, self-stigma in individuals with overweight and obesity can not only lead to psychological problems such as depression, anxiety, and low self-esteem but may also increase the risk of cardiovascular disease, metabolic abnormalities, and even death.51 These psychological problems can lead to a vicious cycle of unhealthy eating or overeating and reduced exercise or activity. Therefore, guidelines for weight reduction in Europe, Canada, and other countries have incorporated psychotherapy into routine weight loss approaches. Psychotherapy can increase patients’ confidence in weight reduction interventions and help them to better implement IF programs and behavioral training by addressing the psychological factors that contribute to unhealthy eating habits of individuals with overweight and obesity through psychological assessment, respect, listening, guidance, and cognitive-behavioral therapy; this can have multiplicative effects on weight reduction and maintenance.52 A 5-year prospective study showed that fasting increased the risk of binge eating and bulimic pathology.53 Disordered eating—ie, overeating—requiring psychological treatment has been suggested as a root cause of obesity. Psychologists in the United States and other countries believe that cognitive and behavioral therapies combined with dietary strategies and physical activity can improve both short- and long-term outcomes in the treatment of obesity.54,55 A scoping review shows that psychological interventions can increase patients’ awareness and compliance with their eating behaviors and enhance self-behavior management to ensure weight loss maintenance in non-surgical interventions for hospitalized adults with class II or class III obesity.56 IF in combination with supportive psychodynamic psychotherapy and physical activity is an effective strategy for long-term weight loss and body mass index (BMI), waist-to-hip ratio, and body fat reduction.57
Evaluation of the Effect of IF
Effects on Body Weight, Body Fat, and LBM
Most of the weight loss associated with IF is due to a reduction in body FM;58 one study calculated that 79% of the weight loss was attributable to a reduction in fat (level I evidence).59 However, some studies have found that IF can result in the loss of LBM concurrent with weight loss, typically accounting for 20%–30% of total weight loss.60 Short-term (4 weeks) IF decreased body weight and improved body composition and cardiometabolic health while having no adverse effects on the feeling of hunger or appetite, whereas long-term (52 weeks) IF reduced the amount of total and abdominal fat and increased LBM, thereby promoting weight maintenance.47,49 A lower LBM is associated with a lower metabolic rate and neuromuscular function, fatigue, and increased risk of injury, with the degree of LBM reduction positively correlated with weight regain.61 Thus, a reasonable weight loss goal is to reduce body fat while avoiding loss of muscle mass. Although both IF and CER led to varying degrees of weight regain after six months, CER increased FM and LBM, whereas IF decreased FM while increasing LBM.25 Exercise has been shown to preserve or prevent a decline in basal metabolism and prevent the loss of muscle mass in people under the age of 60, and IF combined with resistance training programs are commonly used to promote fat loss and improve glucose and insulin levels in this population.62,63 However, whether this is related to adequate protein intake and energy balance is unclear and requires examination in a larger sample size of patients who are elderly or have chronic diseases. It was also reported that IF combined with a high-protein diet reduced BMI and lipids in people with obesity and limited weight regain while increasing arterial compliance.64
Effects on Blood Glucose, Insulin, and Lipids
IF can reduce body weight and improve lipid and glucose abnormalities.65 Short-term (12-week) IF with a low-calorie, high-protein diet reduced total adiposity, abdominal and visceral FM, and plasma biomarkers (insulin, glucose, triglycerides, low-density lipoprotein [LDL], and total cholesterol) while improving metabolism (resting metabolic rate and respiratory quotient) in obese men and women.49,64 However, although IF was superior to CER in reducing insulin resistance (possibly by decreasing total energy expenditure), it also increased insulin levels and promoted fat storage, without significantly lowering blood glucose and lipids.66 On the other hand, in another RCT of centrally obese adults, IF and CER had comparable effects on cardiometabolic health and were not superior to CER in terms of increasing insulin sensitivity.31 In a study of 19 subjects with metabolic syndromes, IF significantly reduced atherogenic lipids: total cholesterol decreased by 7%, LDL cholesterol by 11%, and non–high-density lipoprotein cholesterol by 9%. Additionally, a decreasing trend was observed in the number of total cholesterol and LDL cholesterol particles.67 In an RCT of eight prediabetic men with obesity, five weeks of IF increased insulin sensitivity and islet β-cell reactivity and decreased insulin level, blood pressure, and oxidative stress, although there were no significant changes in body weight or fasting and postprandial blood glucose.68 Collectively, these findings indicate that although IF has benefits for patients with prediabetes and prehypertension, there is insufficient supporting evidence from large samples of different patient populations.
Effects on Cardiometabolic Health
IF not only alleviates blood pressure and improves lipid and glucose levels and other cardiovascular disease-related risk factors, it also reduces the risk of coronary heart disease and improves the prognosis of cardiac events.65 Short-term intervention with a low-calorie, high-protein diet lowered cholesterol and improved BMI as well as cardiovascular variables such as resting heart rate and blood pressure. Compared with a heart-healthy diet, IF with a low-calorie, high-protein diet for one year had certain advantages for cardiometabolic health such as weight reduction, prevention of low-density-lipoprotein rebound, and enhanced arterial compliance.47,64 Meal timing also influences cardiometabolic health; according to the American Heart Association, nighttime fasting can reduce the risk of cardiovascular disease.8 A study of lean and healthy adults showed that although IF yielded comparable overall weight loss to energy restriction and balanced diets, subjects in the IF group showed less weight loss due to fat reduction and there were no specific benefits in terms of metabolic regulation or cardiovascular health.69 This is supported by the finding from a study of 139 obese adults that IF was not more effective than daily CR in reducing body weight, body fat, and cardiovascular metabolic risk factors.24 More clinical studies are needed to determine whether IF has benefits for the prevention and treatment of cardiovascular diseases.
Effects of IF on Other Diseases
Apart from body weight, IF can be applied to the management of metabolic disorders such as diabetes and Non-alcoholic Fatty Liver Disease (NAFLD).70 In a randomized trial of 137 adults with type 2 diabetes, IF had similar effects to CER in reducing hemoglobin A1c level and improving blood glucose. On the other hand, IF showed superior performance for lowering body weight and in increasing insulin sensitivity.14 In patients with NAFLD, IF for eight weeks decreased BMI, alanine aminotransferase level, and steatosis and fibrosis rates compared with a normal diet, with good compliance among patients in the IF group.71 ADF also resulted in greater weight loss and improvement in blood lipid levels in a shorter period (4–12 weeks) than TRE.72
In patients with Multiple Sclerosis (MS), IF was as safe and effective as CER in reducing body weight and improving mood.73 Meanwhile, IF was shown to improve the immune recovery of patients with MS by altering intestinal flora composition and reducing the inflammatory response.74 By reducing fat, IF not only improves body shape but also diminishes the risk of obesity-related diseases such as dyslipidemia, type 2 diabetes, hypertension, and NAFLD. In preclinical studies, fasting and CR have been shown to prolong life- and healthspan, induce autophagy, and ameliorate symptoms of various diseases, such as CVDs, type 2 diabetes, neurodegenerative diseases, cancer, or ischemic injuries.75 It should be noted that although IF can lead to better clinical outcomes compared with other dietary modifications, the benefits are mainly derived from energy restriction rather than fasting; as such, it should not be considered as the ideal dietary intervention.76 Future studies should also prioritize testing the health benefits of these diets in patients with type 1 diabetes, polycystic ovary syndrome and thyroid disorders.77 Based on human studies, we outline the overall effects of IF versus CR (Figure 1).
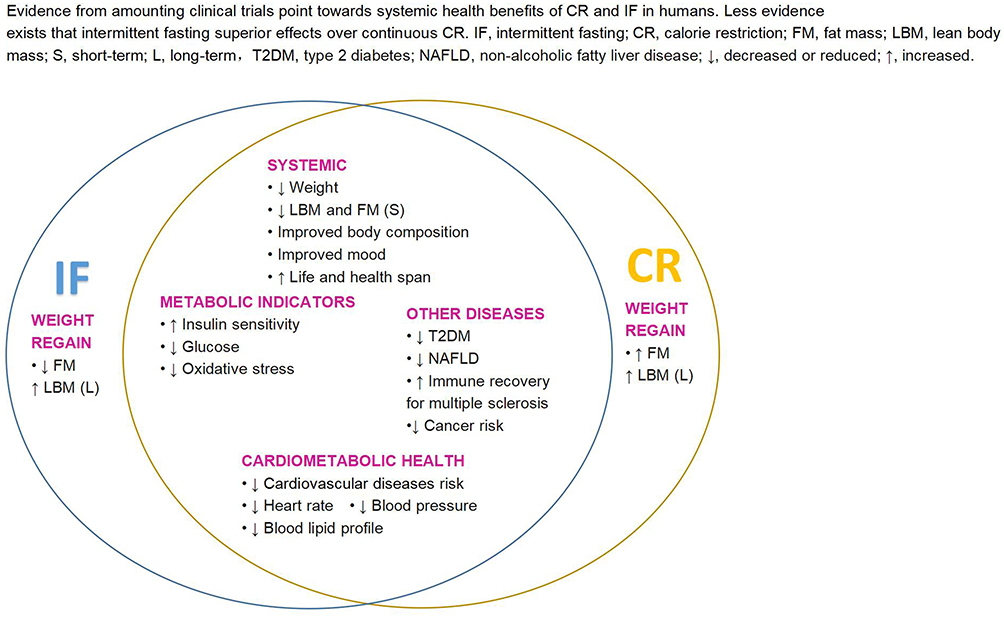 |
Figure 1 Overall effects of IF versus CR. |
Summary
Preclinical and clinical evidence suggests that IF is an effective nonpharmacologic therapy for weight loss that can decrease body weight and improve body composition (total body fat, abdominal fat, and LBM) as well as physiologic indices such as blood glucose, lipids, insulin sensitivity, and cardiovascular metabolism in adults with overweight and obesity. Most IF-related intervention studies have been conducted over a short period, with some long-term clinical trials lasting more than one year. Moreover, the study subjects have mainly been adults with overweight and obesity with or without diabetes mellitus, hyperlipidemia, or other comorbidities. Longitudinal population studies with large samples are needed to evaluate the safety and effectiveness of IF. Given the diverse forms of IF and its combination with other interventions such as exercise, meal replacement, and psychotherapy, the effects of IF on weight loss vary considerably across studies. IF is only one dietary strategy, and dietary components also play a key role in the development of obesity. Changing our lifestyle towards healthy eating and more physical activity may help reduce or prevent the development of obesity.78 Future studies should address the synergistic effects of IF combined with other interventions in weight management as a means to improve adherence79 to weight loss regimens for long-term weight control.
All studies that adopt IF to manage weight are required to undergo ethics review.
Funding
This work was funded by Zhejiang Basic Public Welfare Research Project (LGF20H260013) and the Initial Scientific Research Fund for PhD from Taizhou Hospital of Zhejiang Province (2018BSKYQDJJ15).
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Pan XF, Wang L, Pan A. Epidemiology and determinants of obesity in China. Lancet Diabetes Endocrinol. 2021;9(6):373–392. doi:10.1016/S2213-8587(21)00045-0
2. China Medical Information Guide. Report on nutrition and chronic diseases in China (2020): more than half of adult residents in China are overweight or obese. Chin Med Inform Guide. 2020;35(24):15.
3. Abdelaal M, le Roux CW, Docherty NG. Morbidity and mortality associated with obesity. Ann Transl Med. 2017;5(7):161. doi:10.21037/atm.2017.03.107
4. Rodriguez AJ, Scott D, Ebeling P. Effect of weight loss induced by energy restriction on measures of arterial compliance: a systematic review and meta-analysis. Atherosclerosis. 2016;252:201–202. doi:10.1016/j.atherosclerosis.2016.06.043
5. Zhang MG, Chu TS, Zhu GF, et al. Clinical effects of light fasting in the treatment of abnormal glucose tolerance. Heart J. 2016;28(2):192–193. doi:10.13191/j.chj.2016.0052
6. MacLean PS, Wing RR, Davidson T, et al. NIH working group report: innovative research to improve maintenance of weight loss. Obesity. 2015;23(1):7–15. doi:10.1002/oby.20967
7. de Cabo R, Mattson MP. Effects of intermittent fasting on health, aging, and disease. N Engl J Med. 2019;381(26):2541–2551. doi:10.1056/NEJMra1905136
8. St-Onge M-P, Ard J, Baskin ML, et al. Meal timing and frequency: implications for cardiovascular disease prevention: a scientific statement from the American Heart Association. Circulation. 2017;135(9):e96–e121. doi:10.1161/CIR.0000000000000476
9. Alhamdan BA, Garcia-Alvarez A, Alzahrnai AH, et al. Alternate-day versus daily energy restriction diets: which is more effective for weight loss? A systematic review and meta-analysis. Obes Sci Pract. 2016;2(3):293–302. doi:10.1002/osp4.52
10. Trepanowski JF, Kroeger CM, Barnosky A, et al. Effect of alternate-day fasting on weight loss, weight maintenance, and cardioprotection among metabolically healthy obese adults: a randomized clinical trial. JAMA Intern Med. 2017;177(7):930–938. doi:10.1001/jamainternmed.2017.0936
11. Ganesan K, Habboush Y, Sultan S. Intermittent fasting: the choice for a healthier lifestyle. Cureus. 2018;10(7):e2947. doi:10.7759/cureus.2947
12. Mosley M, Spencer M. The FastDiet: Lose Weight, Stay Healthy, and Live Longer with the Simple Secret of Intermittent Fasting. New York: Atria; 2013.
13. Patterson RE, Sears DD. Metabolic effects of intermittent fasting. Annu Rev Nutr. 2017;37(1):371–393. doi:10.1146/annurev-nutr-071816-064634
14. Carter S, Clifton PM, Keogh JB. Effect of intermittent compared with continuous energy restricted diet on glycemic control in patients with type 2 diabetes: a randomized noninferiority trial. JAMA Netw Open. 2018;1(3):e180756. doi:10.1001/jamanetworkopen.2018.0756
15. Sundfor TM, Svendsen M, Tonstad S. Effect of intermittent versus continuous energy restriction on weight loss, maintenance and cardiometabolic risk: a randomized 1-year trial. Nutr Metab Cardiovasc Dis. 2018;28(7):698–706. doi:10.1016/j.numecd.2018.03.009
16. Hajek P, Przulj D, Pesola F, et al. A randomised controlled trial of the 5:2 diet. PLoS One. 2021;16(11):e258853. doi:10.1371/journal.pone.0258853
17. Sun GL, Deng CJ, Huang LC, et al. Effect of “5+2” intermittent fasting combined with medium-chain triacylglycerol on body fat and glycolipid metabolism in overweight/obese patients. Guangxi Med. 2020;42(21):2800–2805. doi:10.11675/j.issn.0253-4304.2020.21.11
18. Harris L, Hamilton S, Azevedo LB, et al. Intermittent fasting interventions for treatment of overweight and obesity in adults: a systematic review and meta-analysis. JBI Database Syst Rev Implement Rep. 2018;16(2):507–547. doi:10.11124/JBISRIR-2016-003248
19. Rynders CA, Thomas EA, Zaman A, Pan Z, Catenacci VA, Melanson EL. Effectiveness of intermittent fasting and time-restricted feeding compared to continuous energy restriction for weight loss. Nutrients. 2019;11(10):2442. doi:10.3390/nu11102442
20. Garaulet M, Gomez-Abellan P, Alburquerque-Bejar JJ, Lee YC, Ordovas JM, Scheer FA. Timing of food intake predicts weight loss effectiveness. Int J Obes. 2013;37(4):604–611. doi:10.1038/ijo.2012.229
21. Jakubowicz D, Barnea M, Wainstein J, Froy O. High caloric intake at breakfast vs. dinner differentially influences weight loss of overweight and obese women. Obesity. 2013;21(12):2504–2512. doi:10.1002/oby.20460
22. Xie Z, Sun Y, Ye Y, et al. Randomized controlled trial for time-restricted eating in healthy volunteers without obesity. Nat Commun. 2022;13(1):1003. doi:10.1038/s41467-022-28662-5
23. Lowe DA, Wu N, Rohdin-Bibby L, et al. Effects of time-restricted eating on weight loss and other metabolic parameters in women and men with overweight and obesity: the TREAT randomized clinical trial. JAMA Intern Med. 2020;180(11):1491–1499. doi:10.1001/jamainternmed.2020.4153
24. Liu D, Huang Y, Huang C, et al. Calorie restriction with or without time-restricted eating in weight loss. N Engl J Med. 2022;386(16):1495–1504. doi:10.1056/NEJMoa2114833
25. Catenacci VA, Pan Z, Ostendorf D, et al. A randomized pilot study comparing zero-calorie alternate-day fasting to daily caloric restriction in adults with obesity. Obesity. 2016;24(9):1874–1883. doi:10.1002/oby.21581
26. Trepanowski JF, Kroeger CM, Barnosky A, et al. Effects of alternate-day fasting or daily calorie restriction on body composition, fat distribution, and circulating adipokines: secondary analysis of a randomized controlled trial. Clin Nutr. 2018;37(6Pt A):1871–1878. doi:10.1016/j.clnu.2017.11.018
27. Coutinho SR, Halset EH, Gåsbakk S, et al. Compensatory mechanisms activated with intermittent energy restriction: a randomized control trial. Clin Nutr. 2018;37(3):815–823. doi:10.1016/j.clnu.2017.04.002
28. Steger FL, Donnelly JE, Hull HR, Li X, Hu J, Sullivan DK. Intermittent and continuous energy restriction result in similar weight loss, weight loss maintenance, and body composition changes in a 6 month randomized pilot study. Clin Obes. 2021;11(2):e12430. doi:10.1111/cob.12430
29. Schübel R, Nattenmüller J, Sookthai D, et al. Effects of intermittent and continuous calorie restriction on body weight and metabolism over 50 wk: a randomized controlled trial. Am J Clin Nutr. 2018;108(5):933–945. doi:10.1093/ajcn/nqy196
30. Headland ML, Clifton PM, Keogh JB. Effect of intermittent compared to continuous energy restriction on weight loss and weight maintenance after 12 months in healthy overweight or obese adults. Int J Obes. 2019;43(10):2028–2036. doi:10.1038/s41366-018-0247-2
31. Pinto AM, Bordoli C, Buckner LP, et al. Intermittent energy restriction is comparable to continuous energy restriction for cardiometabolic health in adults with central obesity: a randomized controlled trial; the Met-IER study. Clin Nutr. 2020;39(6):1753–1763. doi:10.1016/j.clnu.2019.07.014
32. Opstad TB, Sundfør T, Tonstad S, Seljeflot I. Effect of intermittent and continuous caloric restriction on Sirtuin1 concentration depends on sex and body mass index. Nutr Metab Cardiovasc Dis. 2021;31(6):1871–1878. doi:10.1016/j.numecd.2021.03.005
33. Conley M, Le Fevre L, Haywood C, Proietto J. Is two days of intermittent energy restriction per week a feasible weight loss approach in obese males? A randomised pilot study. Nutr Diet. 2018;75(1):65–72. doi:10.1111/1747-0080.12372
34. Pannen ST, Maldonado SG, Nonnenmacher T, et al. Adherence and dietary composition during intermittent vs. continuous calorie restriction: follow-up data from a randomized controlled trial in adults with overweight or obesity. Nutrients. 2021;13(4):1195. doi:10.3390/nu13041195
35. Isenmann E, Dissemond J, Geisler S. The effects of a macronutrient-based diet and time-restricted feeding (16:8) on body composition in physically active individuals-A 14-week randomised controlled trial. Nutrients. 2021;13(9):3122. doi:10.3390/nu13093122
36. Chow LS, Manoogian E, Alvear A, et al. Time-restricted eating effects on body composition and metabolic measures in humans who are overweight: a feasibility study. Obesity. 2020;28(5):860–869. doi:10.1002/oby.22756
37. Thomas EA, Zaman A, Sloggett KJ, et al. Early time-restricted eating compared with daily caloric restriction: a randomized trial in adults with obesity. Obesity. 2022;30(5):1027–1038. doi:10.1002/oby.23420
38. Bhutani S, Klempel MC, Kroeger CM, Trepanowski JF, Varady KA. Alternate day fasting and endurance exercise combine to reduce body weight and favorably alter plasma lipids in obese humans. Obesity. 2013;21(7):1370–1379. doi:10.1002/oby.20353
39. Cho AR, Moon JY, Kim S, et al. Effects of alternate day fasting and exercise on cholesterol metabolism in overweight or obese adults: a pilot randomized controlled trial. Metabolism. 2019;93:52–60. doi:10.1016/j.metabol.2019.01.002
40. Conrozier T, Eymard F, Chouk M, Chevalier X. Impact of obesity, structural severity and their combination on the efficacy of viscosupplementation in patients with knee osteoarthritis. BMC Musculoskelet Disord. 2019;20(1):376. doi:10.1186/s12891-019-2748-0
41. Moro T, Tinsley G, Bianco A, et al. Effects of eight weeks of time-restricted feeding (16/8) on basal metabolism, maximal strength, body composition, inflammation, and cardiovascular risk factors in resistance-trained males. J Transl Med. 2016;14(1):290. doi:10.1186/s12967-016-1044-0
42. Aqeel M, Forster A, Richards EA, et al. Correction: Marah Aqeel et al. “The effect of timing of exercise and eating on postprandial response in adults: a systematic review”. Nutrients. 2020;12(5):221. doi:10.3390/nu12051263
43. Mohr AE, Ramos C, Tavarez K, Arciero PJ. Lower postprandial thermogenic response to an unprocessed whole food meal compared to an iso-energetic/macronutrient meal replacement in young women: a single-blind randomized cross-over trial. Nutrients. 2020;12(8):2469. doi:10.3390/nu12082469
44. Bowen J, Brindal E, James-Martin G, Noakes M. Randomized trial of a high protein, partial meal replacement program with or without alternate day fasting: similar effects on weight loss, retention status, nutritional, metabolic, and behavioral outcomes. Nutrients. 2018;10(9):1145. doi:10.3390/nu10091145
45. Liu F, Li QF, Li HL, et al. A multicenter, open clinical study on the effect of meal replacement-assisted “5+2 light fasting” on weight loss in overweight/obese adults in China. China Med J. 2021;56(04):422–425. doi:10.3969/j.issn.1008-1070.2021.04.019
46. Tang F, Lin X. Effects of fasting-mimicking diet and specific meal replacement foods on blood glucose control in patients with type 2 diabetes: a randomized controlled trial. Oxid Med Cell Longev. 2020;2020:6615295. doi:10.1155/2020/6615295
47. Arciero PJ, Arciero KM, Poe M, et al. Intermittent fasting two days versus one day per week, matched for total energy intake and expenditure, increases weight loss in overweight/obese men and women. Nutr J. 2022;21(1):36. doi:10.1186/s12937-022-00790-0
48. Arciero PJ, Ormsbee MJ, Gentile CL, Nindl BC, Brestoff JR, Ruby M. Increased protein intake and meal frequency reduces abdominal fat during energy balance and energy deficit. Obesity. 2013;21(7):1357–1366. doi:10.1002/oby.20296
49. Arciero PJ, Edmonds R, He F, et al. Protein-pacing caloric-restriction enhances body composition similarly in obese men and women during weight loss and sustains efficacy during long-term weight maintenance. Nutrients. 2016;8(8):476. doi:10.3390/nu8080476
50. Russell-Mayhew S, McVey G, Bardick A, Ireland A. Mental health, wellness, and childhood overweight/obesity. J Obes. 2012;2012:281801. doi:10.1155/2012/281801
51. Pearl RL, Wadden TA, Hopkins CM, et al. Association between weight bias internalization and metabolic syndrome among treatment-seeking individuals with obesity. Obesity. 2017;25(2):317–322. doi:10.1002/oby.21716
52. Hjelmesaeth J, Rosenvinge JH, Gade H, Friborg O. Effects of cognitive behavioral therapy on eating behaviors, affective symptoms, and weight loss after bariatric surgery: a randomized clinical trial. Obes Surg. 2019;29(1):61–69. doi:10.1007/s11695-018-3471-x
53. Stice E, Davis K, Miller NP, Marti CN. Fasting increases risk for onset of binge eating and bulimic pathology: a 5-year prospective study. J Abnorm Psychol. 2008;117(4):941–946. doi:10.1037/a0013644
54. Van Dorsten B, Lindley EM. Cognitive and behavioral approaches in the treatment of obesity. Med Clin North Am. 2011;95(5):971–988. doi:10.1016/j.mcna.2011.06.008
55. Chu DT, Minh NN, Nga VT, et al. An update on obesity: mental consequences and psychological interventions. Diabetes Metab Syndr. 2019;13(1):155–160. doi:10.1016/j.dsx.2018.07.015
56. Rees M, Collins CE, De Vlieger N, McDonald VM. Non-surgical interventions for hospitalized adults with class II or class III obesity: a scoping review. Diabetes Metab Syndr Obes. 2021;14:417–429. doi:10.2147/DMSO.S280735
57. Juchacz K, Klos P, Dziedziejko V, Wojciak RW. The effectiveness of supportive psychotherapy in weight loss in a group of young overweight and obese women. Nutrients. 2021;13(2):532. doi:10.3390/nu13020532
58. Welton S, Minty R, O’Driscoll T, et al. Intermittent fasting and weight loss: systematic review. Can Fam Physician. 2020;66(2):117–125.
59. Harvie MN, Pegington M, Mattson MP, et al. The effects of intermittent or continuous energy restriction on weight loss and metabolic disease risk markers: a randomized trial in young overweight women. Int J Obes. 2011;35(5):714–727. doi:10.1038/ijo.2010.171
60. Cava E, Yeat NC, Mittendorfer B. Preserving healthy muscle during weight loss. Adv Nutr. 2017;8(3):511–519. doi:10.3945/an.116.014506
61. Willoughby D, Hewlings S, Kalman D. Body composition changes in weight loss: strategies and supplementation for maintaining lean body mass, a brief review. Nutrients. 2018;10(12):12. doi:10.3390/nu10121876
62. Sandoval C, Santibanez S, Villagran F. Effectiveness of intermittent fasting to potentiate weight loss or muscle gains in humans younger than 60 years old: a systematic review. Int J Food Sci Nutr. 2021;72(6):734–745. doi:10.1080/09637486.2020.1868412
63. Keenan S, Cooke MB, Belski R. The effects of intermittent fasting combined with resistance training on lean body mass: a systematic review of human studies. Nutrients. 2020;12(8):2349. doi:10.3390/nu12082349
64. Zuo L, He F, Tinsley GM, Pannell BK, Ward E, Arciero PJ. Comparison of high-protein, intermittent fasting low-calorie diet and heart healthy diet for vascular health of the obese. Front Physiol. 2016;7:350. doi:10.3389/fphys.2016.00350
65. Dong TA, Sandesara PB, Dhindsa DS, et al. Intermittent fasting: a heart healthy dietary pattern? Am J Med. 2020;133(8):901–907. doi:10.1016/j.amjmed.2020.03.030
66. Cioffi I, Evangelista A, Ponzo V, et al. Intermittent versus continuous energy restriction on weight loss and cardiometabolic outcomes: a systematic review and meta-analysis of randomized controlled trials. J Transl Med. 2018;16(1):371. doi:10.1186/s12967-018-1748-4
67. Wilkinson MJ, Manoogian E, Zadourian A, et al. Ten-hour time-restricted eating reduces weight, blood pressure, and atherogenic lipids in patients with metabolic syndrome. Cell Metab. 2020;31(1):92–104. doi:10.1016/j.cmet.2019.11.004
68. Sutton EF, Beyl R, Early KS, Cefalu WT, Ravussin E, Peterson CM. Early time-restricted feeding improves insulin sensitivity, blood pressure, and oxidative stress even without weight loss in men with prediabetes. Cell Metab. 2018;27(6):1212–1221. doi:10.1016/j.cmet.2018.04.010
69. Templeman I, Smith HA, Chowdhury E, et al. A randomized controlled trial to isolate the effects of fasting and energy restriction on weight loss and metabolic health in lean adults. Sci Transl Med. 2021;13(598):598. doi:10.1126/scitranslmed.abd8034
70. Patikorn C, Roubal K, Veettil SK, et al. Intermittent fasting and obesity-related health outcomes: an umbrella review of meta-analyses of randomized clinical trials. JAMA Netw Open. 2021;4(12):e2139558. doi:10.1001/jamanetworkopen.2021.39558
71. Johari MI, Yusoff K, Haron J, et al. A randomised controlled trial on the effectiveness and adherence of modified alternate-day calorie restriction in improving activity of non-alcoholic fatty liver disease. Sci Rep. 2019;9(1):11232. doi:10.1038/s41598-019-47763-8
72. Cai H, Qin YL, Shi ZY, et al. Effects of alternate-day fasting on body weight and dyslipidaemia in patients with non-alcoholic fatty liver disease: a randomised controlled trial. Bmc Gastroenterol. 2019;19(1):219. doi:10.1186/s12876-019-1132-8
73. Fitzgerald KC, Vizthum D, Henry-Barron B, et al. Effect of intermittent vs. daily calorie restriction on changes in weight and patient-reported outcomes in people with multiple sclerosis. Mult Scler Relat Disord. 2018;23:33–39. doi:10.1016/j.msard.2018.05.002
74. Morales-Suarez-Varela M, Collado SE, Peraita-Costa I, Llopis-Morales A, Soriano JM. Intermittent fasting and the possible benefits in obesity, diabetes, and multiple sclerosis: a systematic review of randomized clinical trials. Nutrients. 2021;13(9):3179. doi:10.3390/nu13093179
75. Hofer SJ, Carmona-Gutierrez D, Mueller MI, Madeo F. The ups and downs of caloric restriction and fasting: from molecular effects to clinical application. Embo Mol Med. 2022;14(1):e14418. doi:10.15252/emmm.202114418
76. Santos HO. Intermittent fasting and fat mass: What is the clinical magnitude? Obesities. 2022;2(1):1–7. doi:10.3390/obesities2010001
77. Varady KA, Cienfuegos S, Ezpeleta M, Gabel K. Clinical application of intermittent fasting for weight loss: progress and future directions. Nat Rev Endocrinol. 2022;18(5):309–321. doi:10.1038/s41574-022-00638-x
78. Kopp W. Development of obesity: the driver and the passenger. Diabetes Metab Syndr Obes. 2020;13:4631–4642. doi:10.2147/DMSO.S280146
79. Kumar NK, Merrill JD, Carlson S, German J, Yancy WJ. Adherence to low-carbohydrate diets in patients with diabetes: a narrative review. Diabetes Metab Syndr Obes. 2022;15:477–498. doi:10.2147/DMSO.S292742
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Impact of Semaglutide, a Glucagon-Like Peptide-1 Receptor Agonist, on Obesity Management: A Review
Alorfi NM, Algarni AS
Clinical Pharmacology: Advances and Applications 2022, 14:61-67
Published Date: 3 August 2022
Association Between Nutritional Knowledge, Dietary Regimen, and Excess Body Weight in Primary School Teachers
Saintila J, Calizaya-Milla YE, Calizaya-Milla SE, Elejabo-Pacheco AA, Sandoval-Valentin GA, Rodriguez-Panta SG
Journal of Multidisciplinary Healthcare 2022, 15:2331-2339
Published Date: 14 October 2022
Adolescents with Type 2 Diabetes: Overcoming Barriers to Effective Weight Management
Salama M, Biggs BK, Creo A, Prissel R, Al Nofal A, Kumar S
Diabetes, Metabolic Syndrome and Obesity 2023, 16:693-711
Published Date: 9 March 2023
Patient and Healthcare Professional Preferences for Prescription Weight Loss Medications in Australia: Two Discrete Choice Experiments
Fifer S, Keen B, Porter A
Patient Preference and Adherence 2024, 18:435-454
Published Date: 19 February 2024
The Economic Impact of Obesity in Turkey: A Micro-Costing Analysis
Gogas Yavuz D, Akhtar O, Low K, Gras A, Gurser B, Yilmaz ES, Basse A
ClinicoEconomics and Outcomes Research 2024, 16:123-132
Published Date: 5 March 2024