Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Is Frailty a Mortality Predictor in Subjects with Chronic Obstructive Pulmonary Disease?
Authors Nishimura K ![]() , Kusunose M
, Kusunose M ![]() , Shibayama A, Nakayasu K
, Shibayama A, Nakayasu K
Received 3 October 2023
Accepted for publication 3 December 2023
Published 11 December 2023 Volume 2023:18 Pages 2955—2960
DOI https://doi.org/10.2147/COPD.S439966
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Koichi Nishimura,1,2 Masaaki Kusunose,3 Ayumi Shibayama,4 Kazuhito Nakayasu5
1National Center for Geriatrics and Gerontology, Obu, Aichi, Japan; 2Clinic Nishimura, Ayabe, Kyoto, Japan; 3Department of Respiratory Medicine, National Center for Geriatrics and Gerontology, Obu, Aichi, Japan; 4Department of Nursing, National Center for Geriatrics and Gerontology, Obu, Aichi, Japan; 5Data Research Section, Kondo P.P. Inc, Osaka, Japan
Correspondence: Koichi Nishimura, Clinic Nishimura, 4-3. Kohigashi, Kuri-cho, Ayabe, 623-0222, Japan, Tel +81-773-47-0321, Fax +81-773-47-0201, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) has been frequently associated with frailty. The association between frailty and mortality in patients with COPD has not yet been fully elucidated and it remains controversial whether frailty or airflow limitation is more important in predicting mortality.
Methods: A total of 141 subjects with stable COPD completed pulmonary function tests and the Kihon Checklist at baseline between 2015 and 2022 and were followed for a maximum of 95 months. Using the Kihon Checklist Total score, we classified patients’ frailty status as robust (0– 3), pre-frail (4– 7), and frail (8– 25).
Results: At baseline, there were 67 (47.5%) in the robust group, 36 (25.5%) pre-frail, and 38 (27.0%) frail. Death was confirmed in 29 (20.5%). Univariate Cox proportional hazards analyses revealed that all predictive relationships of frailty and airflow limitation with mortality were statistically significant, and the C-index was similar, ranging from 0.63 to 0.66. According to the Log rank test and the Cox regression model, there was a significant difference between the frail and robust groups, (p=0.004 and p=0.005, respectively). No significant differences were found in either comparison with the pre-frail group. When stratification of frailty and FEV1 as well as sex were included as explanatory variables, multivariate Cox regression analysis showed a significant difference between the robust and frail groups with respect to mortality when the robust group was used as the reference (p=0.024). The robust and pre-frail groups did not differ significantly (p=0.163).
Conclusion: The mortality of frail COPD patients is higher than those classed as robust. Despite frailty being a substantial mortality predictor, it is uncertain whether or not it is a better predictor than FEV1.
Keywords: chronic obstructive pulmonary disease, COPD, frailty, mortality
Introduction
Chronic obstructive pulmonary disease (COPD) has been linked with frailty, which is widely considered to be a major manifestation of ageing. Consequently, COPD may be thought of as a state of ageing at an accelerated rate. Patients with COPD and frailty have been found to have an increased risk of experiencing acute exacerbations, requiring hospitalization and readmissions after hospital discharge, and having impaired, health-related quality of life and exercise capacity. Nevertheless, the association between frailty and mortality in COPD patients has yet to be fully elucidated. It is uncertain whether frailty is a significant prognostic factor in this population, which is known to have a poor prognosis.
An Italian group reported the first long-term mortality study between COPD patients with and without frailty in 2011.1 In their study, frailty was assessed as clinical frailty according to the Frailty Staging System. Survival at 12 years was compared in COPD patients with and without frailty and it was concluded that there was a significant difference. This was followed in 2019 by the results of a post hoc analysis of data from the National Emphysema Treatment Trial, a large multicenter clinical trial conducted by the National Heart, Lung and Blood Institute in the United States.2 Participants in this trial with frailty had an adjusted hazard ratio (HR) of 1.4 (p=0.07) compared to participants with pre-frailty or no frailty, indicating a non-significant difference between the groups. A group from Beijing published two similar research papers indicating that the risk of all-cause mortality was higher in frail patients with COPD than in non-frail patients,3,4 and that severity of the Global Initiative for Chronic Obstructive Lung Disease (GOLD) was corrected for, but the forced expiratory volume in one second (FEV1) itself was not included in their studies. Scarlata et al also reported that the frailty index was significantly associated with lung function and severity of COPD, but not with mortality.5 Using data from the UK Biobank, Hanlon et al reported that the frailty phenotype (frail vs robust) was significantly associated with mortality and these relationships were similar before and after adjustment for FEV1.6 A recent multivariate Cox regression analysis by Brighton et al revealed that frailty measured using the Fried Frailty Phenotype (FFP) measure remained a significant independent predictor of survival, while frailty measured using the Short Physical Performance Battery did not.7
This study investigated whether COPD patients with frailty are more likely to die than COPD patients without frailty. It was also intended to determine if airflow limitation or frailty was a better indicator of mortality, as FEV1 has traditionally been regarded as the most powerful predictor of mortality in COPD patients.
Materials and Methods
A total of 141 patients (130 males) with stable COPD from the outpatient clinic of the Department of Respiratory Medicine of the National Center for Geriatrics and Gerontology participated in the present study as part of a previously reported hospital-based cohort study.8 The research was approved by the National Center for Geriatrics and Gerontology Institute’s Ethics Committee (No. 1138–3). The present study complies with the Declaration of Helsinki and prior written informed consent was obtained from all participants. Inclusion criteria were age >50 years, smoking history >10 pack-years, post-bronchodilator FEV1/FVC ratio of less than 0.7, no abnormal shadows on chest radiographs, no active lung disease, no uncontrolled comorbidities, and no changes in treatment regimen in the preceding four weeks. Exclusion criteria were history of asthma and exacerbation of COPD in the previous three months. They completed pulmonary function tests and the Kihon Checklist at baseline on the same day between February 2015 and February 2022 and were followed until January 2023 for a maximum of 95 months. All subjects underwent spirometry more than 60 minutes after inhalation of long-acting bronchodilators. Survival of all enrolled subjects was assessed through mid-January 2023. For subjects who did not attend an outpatient clinic, telephone or postal contact with families or primary health professionals were used to obtain information on mortality. The period from enrolment to the last participation or event was recorded for analysis. The Kihon Checklist is a self-administered questionnaire consisting of 25 items that are yes/no questions. The Kihon Checklist Total score ranges from 0 (no frailty) to 25 (severe frailty), and we classified patients’ frailty status as robust (0–3), pre-frail (4–7), and frail (8–25), as previously reported.8,9
Univariate and multivariate Cox proportional hazards analyses were performed to investigate the relationships between measurements at baseline and subsequent events. Results of the regression analyses are presented as an HR with the corresponding 95% confidence intervals (CI). The C-index of an event prediction model is the property of correctly discriminating between event and non-event-onset individuals, and is often used when comparing different measures, ie, when comparing different models. The closer the value of the C index is to 1.0, the better the risk prediction. Kaplan-Meier curves and Log rank tests were also used for these time-to-event endpoints. A p-value of less than 0.05 was considered statistically significant. All results are expressed as mean ± standard deviation (SD).
Results
In the present analysis, 141 subjects (130 males) were included (Table 1). The stages of COPD as defined by airflow limitation were GOLD I in 43 (30.5%), GOLD II in 74 (52.5%), GOLD III in 19 (13.5%) and GOLD IV in 5 (3.5%). The number of patients with relatively severe illnesses was low. Baseline screening for frailty using the Kihon Checklist Total score showed that 67 (47.5%) were in the robust group, 36 (25.5%) were pre-frail and 38 (27.0%) were frail. They were observed for up to 95 months, with a mean observation of 54.5 (±27.4) months, and a median of 54 months. Death was confirmed in 29 (20.5%) of the 141 study participants.
 |
Table 1 Patient Characteristics at Baseline in 141 Subjects with COPD |
Compared to robust patients, the HR of mortality in patients classed as frail was statistically significant according to the univariate Cox proportional hazards model. Furthermore, all predictive relationships with mortality were found to be statistically significant, and the C-index was similar, ranging from 0.63 to 0.66 (Table 2). Survival in the frail, pre-frail and robust groups was then analyzed using the Kaplan-Meier method, the results of which are shown in Figure 1. According to the Log rank test and the Cox regression model, there was a significant difference between the frail and robust groups, (p=0.004 and p=0.005, respectively). No significant differences were found in either comparison with the pre-frail group (Log rank test, robust vs pre-frail, p=0.061 and pre-frail vs frail, p=0.304). Multivariate regression analysis was then performed to examine the associations of frailty and airflow limitation with mortality (Table 2). When stratification of frailty, sex and FEV1 were included as explanatory variables, there was a significant difference between the robust and frail groups with respect to mortality when the robust group was used as the reference (p=0.024). There was no significant difference between the robust and pre-frail groups (p=0.163). Multivariate Cox regression analysis showed that frail subjects had a significantly higher risk of death compared to robust patients, and that higher values of FEV1 showed a decreased risk of death.
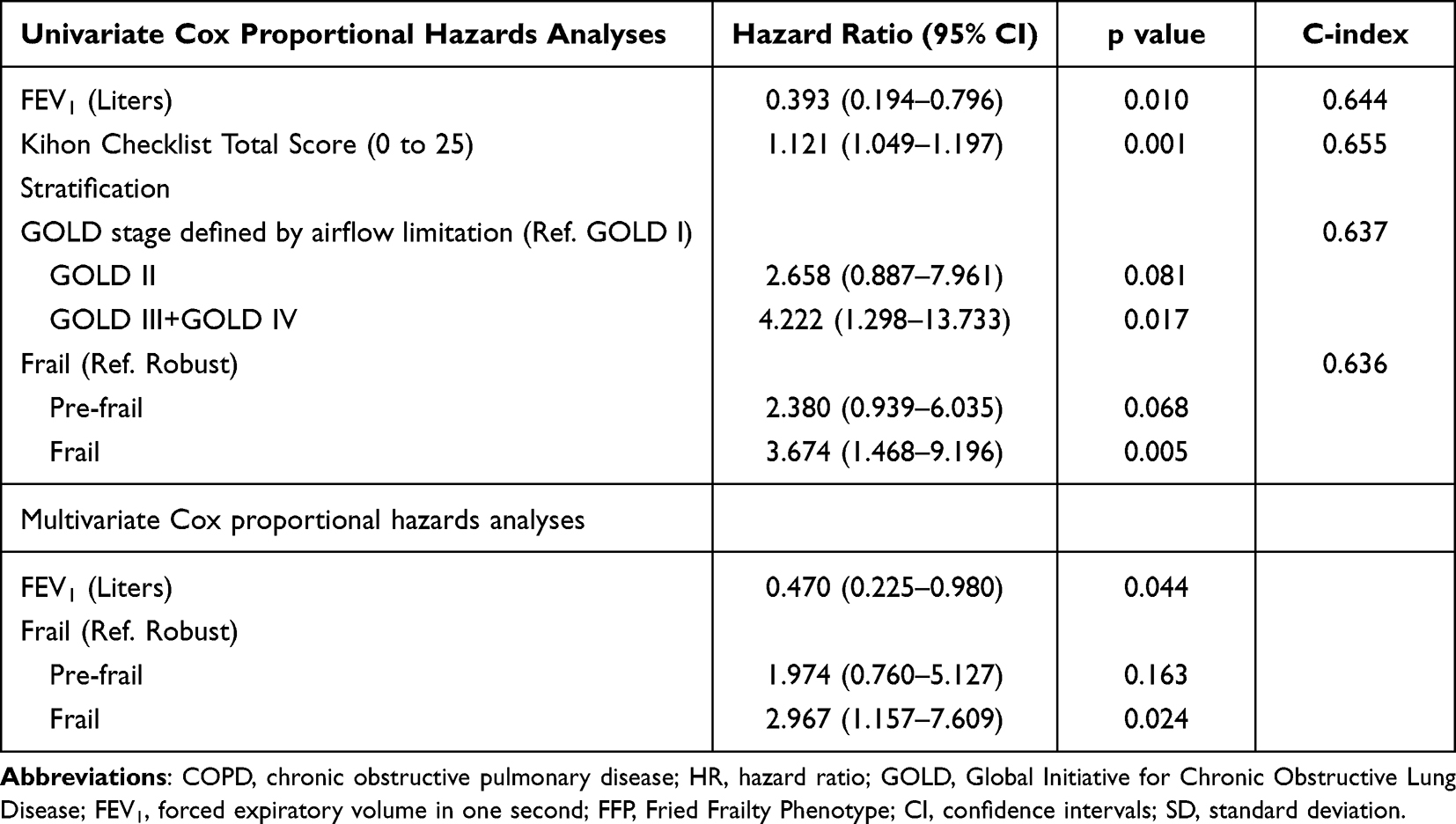 |
Table 2 Univariate and Multivariate Cox Proportional Hazards Analyses on the Relationship Between Baseline Measurements and Mortality |
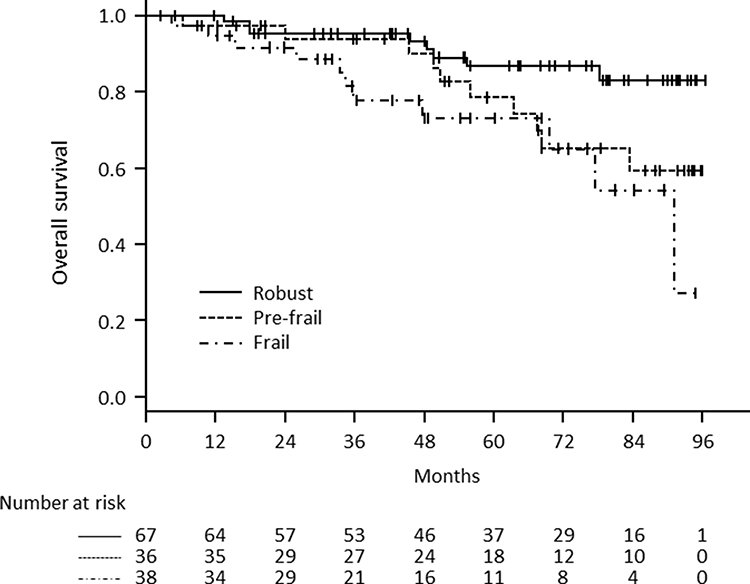 |
Figure 1 Kaplan–Meier survival curves based on three strata (frail, pre-frail and robust) defined by Kihon Checklist Total score. |
Discussion
This study compared the mortality of frail and non-frail COPD patients and also evaluated whether airflow limitation or frailty is a better predictor of mortality. Results from multivariate Cox proportional hazards analyses revealed that mortality in COPD patients with frailty was higher than those classed as robust. However, no significant differences were observed when comparing robust patients to those who were pre-frail, or pre-frail to frail. These findings may be considered a narrow result since frail COPD patients only have a worse prognosis when compared to those classed as robust. Although dyspnea, exercise capacity, and daily physical activity have been reported to be the most important prognostic indicators of COPD in the 21st century, it is widely accepted that FEV1 is the most important and convenient prognostic indicator for COPD, both historically and in daily practice.10 This is also supported by the findings of the present study. Although frailty was found to be an important mortality predictor, it is uncertain whether or not it is a better predictor than FEV1.
Generically, it is not easy to compare the prognostic ability of different indices, but the C-index may be the most reasonable one to compare in univariate Cox proportional hazards analyses. The C-index of frailty and the Kihon Checklist Total score were comparable to those of FEV1 as well as the disease stage of airflow limitation according to the GOLD document when evaluated with univariate Cox proportional hazards analyses. This suggests that frailty and the Kihon Checklist Total score have a similar predictive capacity of mortality to FEV1 as well as GOLD stage.
The findings of some prior studies on the mortality in COPD patients with frailty versus those without frailty reveal poorer outcomes in the former.1,3,4,6,7 However, it is essential to use a statistically sound approach to determine which factors have the highest predictive power since many measurements at baseline are highly correlated. Unfortunately, they were statistically analyzed in some studies without the correction of the baseline FEV1 although the GOLD stage based on airflow limitation is often adjusted for, and it could be argued that this lacks scientific validity. Many studies have reported on the prognostic value of frailty in the general population, but our aim was to identify important prognostic factors in clinical practice for patients with COPD.
Attention has been paid to the distinction between definitions of frailty in the literature. This is because researchers in this field have hypothesized that the way frailty is defined could have an impact on whether or not it is a predictor of mortality.4,6,7 In four studies that used the classic approach to defining frailty, called the FFP, all concluded that frailty was a significant predictor of mortality.3,4,6,7 Conversely, some studies that used alternative methods of diagnosing frailty did not find it to be a predictor of mortality, although the number of series does not match the number of articles because some of the studies examined the same subject with several different methods of diagnosing frailty and compared the results.1,2,4–7 This study also uses the Kihon Checklist, an alternative method of diagnosing frailty that is only used in Japan.8,9 This should be a major limitation of this study since there is little evidence of the Kihon Checklist being validated in the general population. However, the results were positive.
It should be stated that one of the other limitations is that this single-center study was limited by the number of patients with COPD. Secondly, co-morbidities and frequency of COPD exacerbations prior to the study were not recorded at baseline. Thirdly, because our study included predominantly men, generalizing these results to women with COPD may be unwarranted. However, as the number of women with COPD in Japan is quite low, the study reflects the reality of clinical COPD in our population.
Conclusion
Our multivariate Cox proportional hazards analysis demonstrated that frail COPD patients had a higher mortality rate than those classed as robust. Nonetheless, no significant differences were noticed when comparing robust patients to those who were pre-frail, or pre-frail to frail. Despite frailty being a substantial mortality predictor, it is uncertain whether or not it is a better predictor than FEV1.
Acknowledgments
Hideki Kojima, a certified social worker, is acknowledged by the authors for his valuable aid in reaching out to the dropout participants. This study was partly supported by the Research Funding for Longevity Sciences (22-7) from the National Center for Geriatrics and Gerontology, Japan.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Galizia G, Cacciatore F, Testa G, et al. Role of clinical frailty on long-term mortality of elderly subjects with and without chronic obstructive pulmonary disease. Aging Clin Exp Res. 2011;23(2):118–125. doi:10.1007/BF03351076
2. Kennedy CC, Novotny PJ, LeBrasseur NK, Wise RA, Sciurba FC, Benzo RP. Frailty and clinical outcomes in chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2019;16(2):217–224. doi:10.1513/AnnalsATS.201803-175OC
3. Luo J, Zhang D, Tang W, Dou LY, Sun Y. Impact of frailty on the risk of exacerbations and all-cause mortality in elderly patients with stable chronic obstructive pulmonary disease. Clin Interv Aging. 2021;16:593–601. doi:10.2147/CIA.S303852
4. Zhang D, Tang W, Dou LY, Luo J, Sun Y. Four different frailty models predict health outcomes in older patients with stable chronic obstructive pulmonary disease. BMC Geriatr. 2022;22(1):57. doi:10.1186/s12877-022-02750-z
5. Scarlata S, Finamore P, Laudisio A, et al. Association between frailty index, lung function, and major clinical determinants in chronic obstructive pulmonary disease. Aging Clin Exp Res. 2021;33(8):2165–2173. doi:10.1007/s40520-021-01878-z
6. Hanlon P, Lewsey J, Quint JK, et al. Frailty in COPD: an analysis of prevalence and clinical impact using UK Biobank. BMJ Open Respir Res. 2022;9:1.
7. Brighton LJ, Nolan CM, Barker RE, et al. Frailty and mortality risk in COPD: a cohort study comparing the fried frailty phenotype and short physical performance battery. Int J Chron Obstruct Pulmon Dis. 2023;18:57–67. doi:10.2147/COPD.S375142
8. Kusunose M, Oga T, Nakamura S, Hasegawa Y, Nishimura K. Frailty and patient-reported outcomes in subjects with chronic obstructive pulmonary disease: are they independent entities? BMJ Open Respir Res. 2017;4(1):e000196. doi:10.1136/bmjresp-2017-000196
9. Satake S, Senda K, Hong YJ, et al. Validity of the Kihon Checklist for assessing frailty status. Geriatr Gerontol Int. 2016;16(6):709–715. doi:10.1111/ggi.12543
10. Anthonisen NR, Wright EC, Hodgkin JE. Prognosis in chronic obstructive pulmonary disease. Am Rev Respir Dis. 1986;133(1):14–20. doi:10.1164/arrd.1986.133.1.14
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Recognition and Management of Hospital-Acquired Sepsis Among Older General Medical Inpatients: A Multi-Site Retrospective Study
Barker N, Scott IA, Seaton R, Mehta N, Kalke VR, Redpath L
International Journal of General Medicine 2023, 16:1039-1046
Published Date: 21 March 2023
Factors Affecting Mortality in Elderly Hypertensive Hospitalized Patients with COVID-19: A Retrospective Study
Xu Q, Li F, Chen X
Clinical Interventions in Aging 2023, 18:1905-1921
Published Date: 20 November 2023
Association Between Serum Anion Gap and Mortality in Critically Ill Patients with COPD in ICU: Data from the MIMIC IV Database
Chen X, Yang Q, Gao L, Chen W, Gao X, Li Y, Ao L, Sun D
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:579-587
Published Date: 29 February 2024
Postoperative Adverse Outcomes in Patients With Frailty Undergoing Urologic Surgery Among American Patients: A Propensity-Score Matched Retrospective Cohort Study
Hsu CW, Chang CC, Lam F, Liu MC, Yeh CC, Chen TL, Lin CS, Liao CC
Clinical Epidemiology 2025, 17:241-250
Published Date: 12 March 2025
Association Between Chronic Obstructive Pulmonary Disease and Survival in Patients with Lung Cancer: A Nationwide Cohort Study
Chan KH, Liu WC, Chang YC, Konara Mudiyanselage SP, Chuang TJ, Tsai YT
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:617198
Published Date: 23 June 2026