Back to Journals » Journal of Blood Medicine » Volume 13
Iron Deficiency and Blood Donation: Links, Risks and Management
Authors Mantadakis E ![]() , Panagopoulou P, Kontekaki E
, Panagopoulou P, Kontekaki E ![]() , Bezirgiannidou Z, Martinis G
, Bezirgiannidou Z, Martinis G
Received 24 September 2022
Accepted for publication 5 December 2022
Published 10 December 2022 Volume 2022:13 Pages 775—786
DOI https://doi.org/10.2147/JBM.S375945
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Elpis Mantadakis,1 Paraskevi Panagopoulou,2 Eftychia Kontekaki,3 Zoe Bezirgiannidou,4 Georges Martinis3
1Department of Pediatrics, Hematology/ Oncology Unit, University General Hospital of Alexandroupolis, Thrace, Greece; 2Department of Pediatrics, Aristotle University of Thessaloniki, Medical School, Papageorgiou General Hospital, Thessaloniki, Greece; 3Blood Transfusion Centre, University General Hospital of Alexandroupolis, Thrace, Greece; 4Department of Hematology, University General Hospital of Alexandroupolis, Thrace, Greece
Correspondence: Elpis Mantadakis, Department of Pediatrics, University General Hospital of Alexandroupolis, Democritus University of Thrace Faculty of Medicine, 6th Kilometer Alexandroupolis-Makris, 68 100 Alexandroupolis, Thrace, Greece, Tel +30-25513-51424, Email [email protected]
Abstract: The purpose of this review is to raise awareness about the frequently underappreciated association of blood donation with iron deficiency, and to describe methods for its prevention and management. Blood donors cannot expect any health benefits from the donation but have justified expectations of no harm. Iron deficiency without anemia (IDWA) and iron deficiency anemia (IDA) are common consequences of regular blood donation, and this activity is the most important factor affecting iron status in regular blood donors. Awareness of blood donation as a primary cause of sideropenia is surprisingly low among physicians. Blood donation screening identifies potential donors with IDA but is frequently inadequate to detect IDWA. For the assessment of body iron stores, plasma or serum ferritin, transferrin saturation (TSAT) and soluble transferrin receptors (sTfR) concentrations are the most widely used biochemical markers, although the percentage of hypochromic mature erythrocytes and the hemoglobin content of reticulocytes are also useful. IDWA can be prevented by limiting the total volume of blood collected, by iron deficiency screening and deferral of sideropenic donors, by prolonging the interdonation intervals, and by iron supplementation between donations. IDWA tends to be more prevalent in younger people, females, and high-intensity donors. A potentially effective strategy to address sideropenia in blood donors is serum ferritin testing, but this may lead to a higher rate of deferral. Most regular blood donors cannot replenish their iron deficit by an iron-rich diet alone and will benefit from low-dose oral iron administration with various commercially available products post-donation, a well-tolerated strategy. However, valid concerns exist regarding the possibility of worsening the iron overload in donors with undiagnosed hemochromatosis or masking the symptoms of a clinically important gastrointestinal hemorrhage or other underlying medical condition. Finally, educational efforts should be intensified to improve the awareness of blood donation as a primary cause of iron deficiency among physicians of all specialties.
Keywords: blood donation, iron deficiency, iron deficiency without anemia, iron deficiency anemia, iron supplementation, transferrin saturation
Introduction
Voluntary blood donation is a selfless and irreplaceable act necessary to preserve the blood supply. Volunteer blood donors cannot expect any health benefits related to donation but have the reasonable expectation of no physical harm. Hence, maintaining donor health is no less important than ensuring a safe and continuous blood supply, and blood centers should explore screening programs for donors to improve their health, recruitment, and retention.1 In this regard, reducing and preventing possible side effects of phlebotomy without deterring current or future donors is crucial.
Considering the above, iron deficiency without anemia (IDWA) and iron deficiency anemia (IDA) are potential harms to regular blood donors, and it is the ethical duty of blood bank and other physicians (hematologists, general practitioners, etc.) to be aware of the risk of iron depletion in blood donors and evidence-based prevention measures and management of low iron stores.2,3 Donors’ behavior and genetic factors contribute to first-time donor iron status and hemoglobin, but iron supplementation is far more critical than subjects’ genetics in those donating frequently.4 The purpose of this review is to raise awareness about the frequently underappreciated association of blood donation with iron deficiency and to describe methods for its avoidance and management.
Non-Anemic Iron Deficiency
Non-anemic iron deficiency or IDWA is a disease by itself that deserves prompt diagnosis and therapy.5 IDWA is especially frequent in women of childbearing age, who also may benefit from iron supplements. It can be suspected and diagnosed with a variety of indexes derived either from the full blood count or biochemical tests (ferritin, transferrin saturation, soluble transferrin receptors (sTfR), etc). IDWA has been associated with exercise intolerance, fatigue, reduced cognitive function, pica, and restless legs syndrome (RLS). It also impairs aerobic adaptation among previously untrained women and this is correctable with oral iron supplementation.6,7 In a study of 716 adolescent girls with IDWA, participants were randomly assigned to oral ferrous sulfate or placebo for 8 weeks. Post-intervention hematological measures of iron status were significantly improved in the treatment group, while girls receiving iron performed significantly better on a test of verbal learning and memory.7 Non-anemic women with unexplained fatigue may benefit from iron supplementation, but this effect is restricted to women with low or borderline serum ferritin.8 The beneficial effect of oral iron was also shown in a randomized, placebo-controlled, trial in France in 198 women aged 18–53 years, who complained of fatigue, had ferritin <50 μg/L and hemoglobin >12 g/dl, and received either oral ferrous sulfate or placebo for 12 weeks.9
It is surprising how low among physicians is the awareness of blood donation as a primary cause of sideropenia. Only 4 out of 50 (8%) internal medicine and family practice physicians in Austria considered blood donation as a potential cause of iron deficiency, and only 28% reported knowing if one of their patients was a regular blood donor.10 In dedicated blood donors, donation activity is the single most important factor affecting iron status, far ahead of red-meat consumption or iron supplementation.11
Hemoglobin values do not necessarily reflect iron stores, and measurement of hemoglobin or hematocrit alone is insufficient for detecting blood donors with IDWA.12 Donors who have adequate iron stores are deferred from donating blood, while others who are donating blood may have inadequate iron stores.13
As mentioned earlier, IDWA can be associated with pica and could aggravate or even trigger RLS. Therefore, otherwise healthy donors with symptoms of RLS should be very cautious about donating blood, and an assessment of iron stores before the donation is a rational precaution.14 Regarding pica, its presence has been associated with a high probability of iron depletion in blood donors.15 Factors associated with pica were analyzed in four US blood collection agencies. Lower ferritin, non-Asian race, higher red cell distribution width, younger age, and RLS were significantly associated with pica.16 Iron replacement in these patients is effective and reduces symptoms.
Each donation causes a loss of approximately 210 to 240 mg of iron, as 1 mL of red cells contains 1.12 mg of iron. In a study from Germany, 26% of regular donors had ferritin levels <15 μg/L and 12% suffered from IDA.17 IDWA tends to be more prevalent in younger people, females, and those with a more intensive blood donation history. A prospective national study in France of 11,258 WB donors showed that iron deficiency was more frequent in women than in men (39.5% vs 18%). Among 7200 repeated donors, women <50 years old, new female donors, and repeated donors of both sexes had the highest prevalence of iron deficiency. In these identified subgroups, the prevalence of iron deficiency was up to 72.1%.18
Current practices by blood banks identify potential donors with IDA but are inadequate to detect IDWA.19 This is particularly true for premenopausal women and teenagers. A nationally representative study in the US showed that the problem is indeed more intense among adolescents and adult females.20 A stratified approach to prevention and treatment considering risk factors and serum ferritin testing is likely to be the most effective management strategy.21
In the US, a minimum acceptable hemoglobin concentration of 12.5 g/dL and a minimum interval between donations of 56 days is required for blood donation irrespective of the donor’s sex. This is counterintuitive since iron requirements are substantially higher in women of childbearing age. Thus, it is not surprising that in the REDS-II Donor Iron Status Evaluation (RISE) study, only 1.6% of attempted donations by men were deferred due to anemia versus 17.7% of attempts by women.13 A recent study in 30,806 teenage donors in the US showed that 11.4% of females and 9.7% of males had inadequate iron stores at index donation. Follow-up donation iron stores were highly dependent on index ferritin and achieving a ≥90% prevalence of adequate ferritin at 12 months required index ferritin values >50 ng/mL. Teenagers with borderline or low iron stores should consider receiving iron supplements to permit regular donations. In addition, increasing the minimum recommended inter-donation interval to allow time for a refill of iron losses should strongly be considered.22 A large, randomized trial of 45,000 donors in the United Kingdom showed that more frequent donations than is standard practice resulted in more deferrals and IDWA.23 In an Australian study of >3000 blood donors, the prevalence of serum ferritin <15 ng/mL in new donors was 12% in females and 1.3% in males. The prevalence of iron deficiency in female WB-only donors was 26.4%, increasing with donation frequency and young age, while in males it was 6.3% with no evident change with age or donation frequency.24
Female blood donors of childbearing age who donate blood on a regular but moderate basis do not appear to be at higher risk of adverse pregnancy outcomes, such as low birth weight, preterm birth, and stillbirth.26 This is reassuring knowing that IDA is associated with preterm delivery and low birth weight and that iron supplementation during pregnancy decreases these risks.
Volunteer WB donor eligibility criteria vary substantially by country due to cultural and historical reasons, body habitus changes, and other causes, and these differences likely affect the prevalence of IDWA and IDA among donors.25 In the US and elsewhere, despite guidelines described in the AABB Bulletin #12-03, nearly no blood center routinely monitors donor iron status because of the increased cost and the workload related to reviewing the results and counseling the donor. A recent, revised version of these recommendations (AABB Bulletin #17-02) that strongly encourages monitoring iron status in at-risk subgroups has recently been circulated (July 2022).26 In Switzerland, premenopausal women are allowed to donate only three times a year, serum ferritin is measured in all WB donors, albeit not in every visit, and iron-depleted donors are offered three possibilities, ie, to extend the donation interval, to follow a more iron-fortified diet or to receive oral iron supplements.27 In Denmark, ferritin screening is performed on the first donation and every 10 subsequent donations, or more frequently depending upon prior results. Iron-depleted donors are given iron supplements. Not surprisingly, deferrals for iron deficiency have decreased in these two countries.28 Moreover, many centers around the globe try to develop hemoglobin-based algorithms in order to identify the donors who will benefit from ferritin measurement.
Finally, although IDWA is mainly a problem for WB donors, it can also affect plateletpheresis donors, who have smaller iron losses per donation but are able to donate much more frequently than WB donors. An Irish study showed that male plateletpheresis donors had a statistically significant drop in serum ferritin after donation, while they had significantly lower serum ferritin levels than first-time male blood donors.29 Similarly, a study from India showed that regular plateletpheresis donation may lead to depletion of iron stores and subclinical iron deficiency.30
Prevention of Non-Anemic Iron Deficiency in Blood Donors
IDWA in blood donors can be prevented by limiting the volume of blood collected to 400–500 mL per donation, by iron deficiency screening and deferral of sideropenic donors, by blood donation only after hemoglobin/ hematocrit and iron stores recovery, by oral or parenteral iron therapy between donations, by lengthening the inter-donation interval, and by switching WB donors to low-frequency plasma or plateletpheresis donors.31 To date, many blood services do not follow all these recommendations.
Methods for Assessment of Body Iron Stores in Blood Donors
For the assessment of body iron stores, plasma or serum ferritin, transferrin saturation, and sTfR concentrations are the most widely used biochemical markers. The percentage of hypochromic mature erythrocytes and the hemoglobin content of reticulocytes (Ret-He) have also been shown to be much better screening measures for the identification of iron depletion in blood donors than hemoglobin.32 Unfortunately, measurement of capillary hemoglobin only is what is usually available in most blood centers. Regarding hepcidin, it may serve as a marker of the iron repletion needed for erythropoiesis, although it cannot serve as a predictor of response to iron treatment,34 its use is almost exclusively limited to research purposes, and there is a lack of a gold standard measurement assay, pending resolution of the international efforts for harmonization.
Considering ferritin, its measurement at regular intervals is a useful indicator of iron depletion in blood donors.17 Even though the correlation between ferritin and hemoglobin is poor, donors with low ferritin have much higher odds of deferral at subsequent donation visits.33 Gorlin et al, have shown that it is feasible to use serum ferritin for the determination of iron stores to reduce potential deferrals for low hemoglobin in regular blood donors that are offered appropriate iron replacement therapy.34
One potentially effective strategy to address IDWA and IDA in blood donors is serum ferritin testing in females donating ≥ twice per year and men donating ≥ three times per year. This strategy can identify donors with low iron stores who will benefit from appropriate iron supplementation, and patients with undiagnosed hemochromatosis who must avoid taking iron supplements. It may also lead to referrals for further evaluation and treatment of anemia in first-time or infrequent blood donors with underlying diseases, such as gastrointestinal malignancies.35 The population-based Danish Blood Donor Study showed that ferritin was the strongest predictor of the risk of low hemoglobin.36 A recent study from Iceland included WB donors and new donors between 1997–2019. Before October 2017, ferritin was measured only for new donors and intermittently for WB donors, but thereafter for all donors at every donation visit. In January 2018, the ferritin threshold for donation increased from 14 to 16 μg/L for new donors and from 8 to 10 μg/L for WB donors. After the policy change, the proportion of WB donations associated with iron deficiency decreased from 6.4% to 4% for males and from 18.9% to 14.1% for females.37 In a Canadian blood center that practices routine ferritin testing, the minimum hemoglobin for donation was increased to 13 g/dL for males and the minimum inter-donation interval was changed to 84 days for females based on their iron status. This led to a significant reduction in deferrals for low hemoglobin.38 Donors informed of their low ferritin donated less often and had a lower return rate compared to donors with normal ferritin, but they had an increase in follow-up ferritin when tested one year after initial testing.39 In conclusion, regular ferritin testing may improve donor management. However, simply providing donors with ferritin results and written information on iron deficiency is likely insufficient to improve their understanding of iron needs and may lead to an inadequate increase in iron intake over time.39 France et al, have shown that providing information to blood donors regarding their risk of iron depletion enhances the overall awareness of donation-related sideropenia with no negative impact on donor retention. Combining education with an action plan may normalize the iron balance.40
In contrast, regular ferritin measurement in all blood donors may be associated with a decrease in blood donation and additional operational costs and these issues should be considered by blood banks before its implementation. Canadian investigators developed a simulation model representing a population of blood donors tested for ferritin who may exit the blood donation system. Data were derived from operational data, donor research studies from the Canadian Blood Services, and previously published sources. They estimated that red cell collections will decline by 3.1–19.2% after ferritin testing is put in place. Therefore, blood agencies need to ensure that donors with low ferritin will modify their lifestyle and eventually return to the donor pool.41
Besides ferritin, zinc protoporphyrin (ZPP) is another marker of sideropenia used mostly in the Netherlands. Increased levels of ZPP indicate iron deficiency and elevated ZPP was predictive of deferral due to low hemoglobin in a Dutch study of 4598 WB donors.42
Other markers of iron deficiency are sTfR and Ret-He. The accuracy of Ret-He in detecting latent iron deficiency was studied in 501 blood donors in India. The study used sTfR as the gold standard and showed that sTfR and Ret-He detected IDWA in 148 and 135 donors, respectively. In comparison to sTfR, Ret-He had a sensitivity of 92.7%, which was significantly higher than that of ferritin, iron, and TIBC in detecting latent iron deficiency.43 Use of the sTfR-F index (ratio of sTfR to log10 ferritin) and a combined cell index, as described by Boulton et al, show that the iron status of men giving three donations in two years resembled that of menstruating women and that men not taking iron supplements can become markedly iron-deficient on donating six times over a two year period.44
Increased frequency of blood donations is associated with microcytosis and hypochromia, as indicated by lower MCV and MCH, respectively. These immediately available red blood cell indices, or newer parameters measured by automated blood cell analyzers such as the percentage of hypochromic erythrocytes, should be used to monitor early onset iron depletion in regular blood donors.45 In a Malaysian study, the percentage of hypochromic red cells with a cut‐off value of 0.6% was excellent in evaluating iron status among blood donors with very high sensitivity and specificity. It also has the additional advantage of a faster turnaround time than conventional biochemical markers of sideropenia.46 In a pilot study of 150 Swedish blood donors versus 104 controls, donors had significantly more microcytic erythrocytes (median 0.9% vs 0.6%), lower serum ferritin concentration (median 43 vs 91 μg/L), and higher sTfR-F index (median 1.60 vs 1.27). Microcytic erythrocytes and mean cell hemoglobin of reticulocytes (MCHr) predicted iron depletion with moderate sensitivity that was improved when these two parameters were combined.47
In a study from New Zealand, blood donation, being of Asian ethnicity, and history of iron deficiency were all stronger predictors of suboptimal iron status than differences in dietary patterns in premenopausal women.48 In the RISE study, in a cohort of 2425 first-time/reactivated and frequent blood donors, among frequent donors, 66.1% of women and 48.7% of men had iron-deficient erythropoiesis, while absent iron stores (ferritin <12 μg/L) were seen in 16.4% and 27.1% of men and women, respectively. Increased donation intensity, female sex, premenopausal status, black race, low body weight, and younger age were important independent predictors of absent iron stores or iron-deficient erythropoiesis.13,49 The association of decreased iron stores with the female sex was expected since premenopausal women have higher daily iron requirements (1.5 mg vs 1 mg) due to menstrual blood loss.10 The RISE study concluded that iron supplementation may allow frequent donation without iron depletion. However, given that no intervention was performed, the basis of this conclusion and whether it should apply to all donors has been legitimately questioned.50 Consequently, blood banks should try to better identify their own donor population at real risk of iron deficiency and tailor targeted interventions to minimize harm.
Dependence only on food intake to replenish iron stores in regular blood donors is inadequate, especially in settings where IDA is common, to begin with. For example, in Ghana, where IDA is endemic and post-blood donation iron supplementation is not widely practiced, more than three-quarters of the blood donors could not achieve pre-donation iron stores five months post-last donation.51
Studies of Iron Supplementation in Regular Blood Donors
Given the numerous oral and several parenteral available iron products, iron supplementation in regular blood donors should be individualized. For example, ferrous sulfate often causes significant gastrointestinal side effects. In this case, alternative oral iron products should be considered.52 Many studies have been performed to test the efficacy and tolerability of the various iron formulations in the replenishment of iron stores of blood donors. The chosen iron replacement strategy should be convenient, easily available, cheap, and with minimal complications. The most important of these studies are shown in Table 1 and briefly reviewed below.
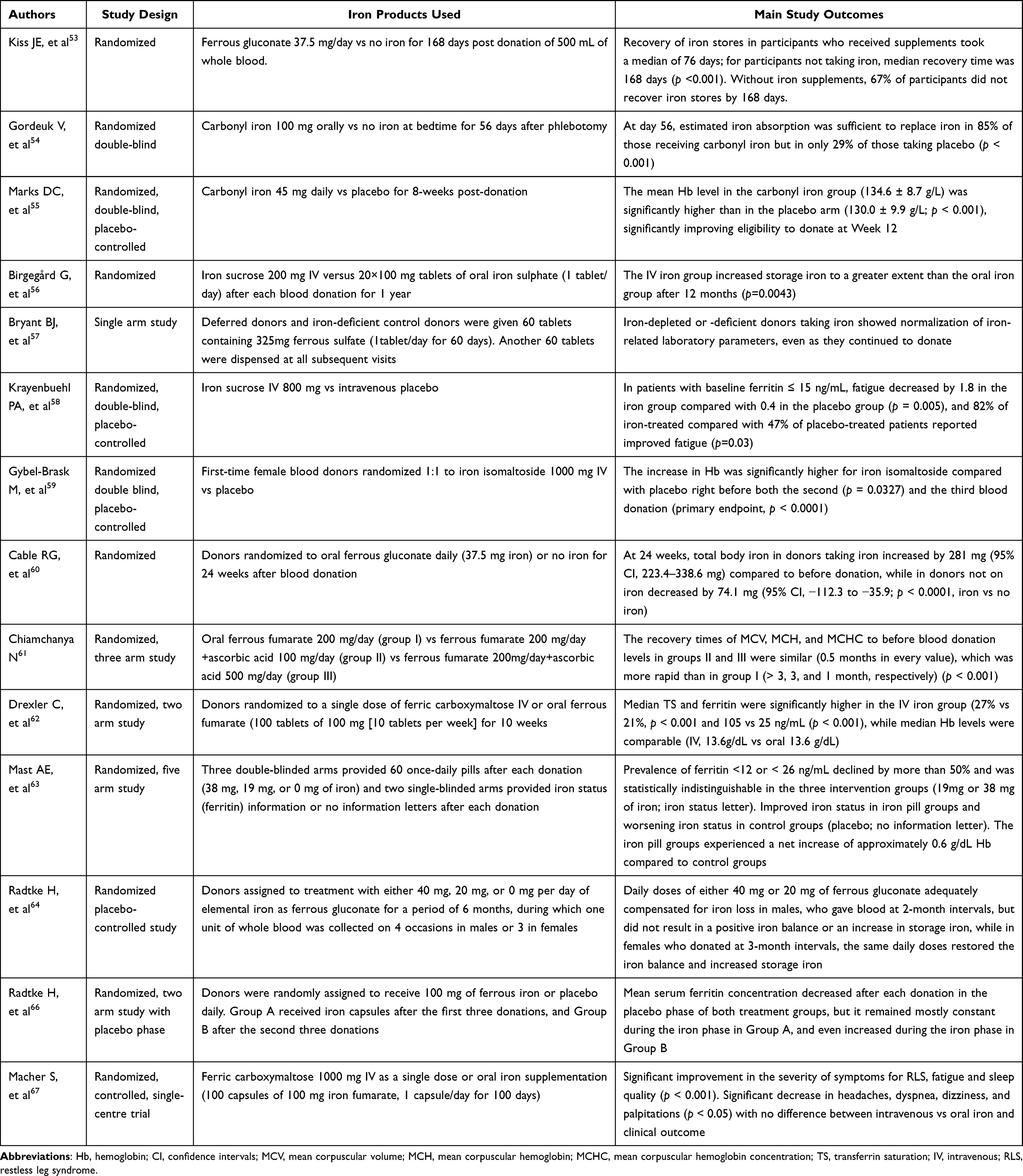 |
Table 1 Studies of Oral or Parenteral Iron Supplementation in Blood Donors |
The Hemoglobin and Iron Recovery Study that was part of the Recipient Epidemiology and Donor Evaluation Study-III (REDS-III), conducted by the National Heart, Lung, and Blood Institute in the US compared donors who did not receive iron supplementation with those who did. Using a ferritin cut-off of 26 ng/mL, recipients of iron supplementation had shortened time to 80% hemoglobin recovery in both the low-and higher-ferritin groups.53 Even in iron-replete donors, the mean hemoglobin recovery was only 70% at eight weeks since absorption of dietary iron is a limiting factor for the refill of iron stores.53 A study comparing placebo vs carbonyl iron in women 18 to 40 years old for 56 days after phlebotomy showed that therapy, diet, or both, was sufficient to replenish the iron stores in 85% of those receiving carbonyl iron vs only 29% of those taking placebo. Moreover, deferral rates from repeat donations were 8% and 36% respectively.54 An Australian Red Cross Blood Service study investigated the effect of carbonyl iron daily or placebo for 8 weeks, as post-donation iron replacement therapy. Donors receiving carbonyl iron had significantly higher ferritin and mean hemoglobin at week 12. In addition, the proportion of iron-deficient donors was significantly lower in the carbonyl iron group, thus improving eligibility to re-donate at week 12. Approximately 87% of the donors receiving carbonyl iron indicated that they would continue to take it, even though significantly more donors receiving iron supplements had at least one gastrointestinal side effect.55 Hence, short-term carbonyl iron supplementation in female blood donors seems to be effective in replacing safely the iron loss of phlebotomy.
A Swedish randomized study on 120 donors with at least five previous WB donations compared IV iron sucrose vs oral iron sulfate for 20 days, after each blood donation for 1 year. Both treatments were safe, but the IV iron sucrose group increased iron stores to a significantly greater extent than the oral iron group. Moreover, female donors, particularly <50 years of age, were more responsive to intravenous iron sucrose compared to the oral formulation.56 In another study, routine administration of ferrous sulfate tablets for 60 days was safe and effective and prevented the development of iron deficiency in blood donors.57 Of the donors receiving ferrous sulfate, intolerance requiring a switch to ferrous gluconate developed in 21%, but only 5% of donors were intolerant to both products and discontinued iron replacement therapy.57 In a randomized, double-blind, placebo-controlled study, premenopausal women presenting with fatigue, serum ferritin ≤ 50 ng/mL, and hemoglobin ≥ 12 g/dL were randomized to receive either 800 mg of intravenous iron sucrose or placebo. Fatigue and serum iron status were assessed at baseline and after 6 and 12 weeks. Overall, 82% of iron-treated compared with 47% of placebo-treated patients reported improved fatigue, a significant difference. Drug-associated adverse events were observed in 21% of iron-treated patients and in 7% of placebo-treated ones, but none of these events was serious.58 A Danish study showed that IV iron isomaltoside before the second and third blood donation was well tolerated and increased the hemoglobin, improved plasma ferritin and transferrin saturation, and also improved fatigue symptoms.59 A randomized study comparing ferrous gluconate vs placebo for 24 weeks after blood donation showed that only donors on iron supplementation replaced their iron stores.60 A study of female regular blood donors in Thailand showed that a combination of ferrous fumarate 200 mg and ascorbic acid 500 mg daily was well tolerated, and effective to accelerate hemoglobin recovery to the pre-donation values.61 In a clinical trial of blood donors with ferritin <30 ng/mL, donors were randomized to either a single dose of intravenous ferric carboxymaltose or oral iron fumarate. A single dose of ferric carboxymaltose was highly effective to prevent IDWA/IDA, although oral iron was an acceptable alternative.62 A US study examined the efficacy of two different doses of elemental iron (38 mg vs 19 mg. vs placebo vs nothing) in 692 frequent blood donors. Withdrawal from the study was more common in those taking iron pills (39% vs 7%), but no difference in adverse events was seen between those receiving iron or placebo, and moreover, those taking iron had improved iron status regardless of the dose.63 A German study also showed that only 20 mg of elemental iron per day as ferrous gluconate for 6 months could adequately compensate for iron loss in donors who donated WB up to four (females) or six (males) times per year.64 The same group in a subsequent study showed that 20 mg of elemental iron as ferrous gluconate and 400 mg of ascorbic acid daily for only 30 days post-donation adequately compensated for iron loss in most WB donors.65 The same authors also examined the effect of supplementation with 100 mg of oral ferrous iron-glycine-sulfate-complex vs placebo after each of three, two-unit red cell apheresis, and demonstrated its efficacy in preventing iron deficiency.66 Finally, Macher et al, compared the frequency and severity of symptoms associated with iron deficiency before and after intravenous or oral iron supplementation in iron-deficient blood donors. Clinical symptoms were evaluated by a survey before and after 8 to 12 weeks of iron therapy. A significant improvement in well-being was reported with both oral and parenteral iron therapy, while there was no difference between the type of iron supplementation and clinical outcome.67
The Recommended Dose of Oral Iron Supplementation for Regular Blood Donors
The Panel on Micronutrients of the Institute of Medicine has established the tolerable upper limit of daily elemental iron intake at 45 mg. By subtracting the approximately 11 mg/day average dietary iron intake of a western diet, this allows for approximately 34 mg of supplemental iron before gastrointestinal side effects are seen.68 The STRIDE study of blood donors’ iron supplementation supports this figure since adverse events did not differ among subjects receiving elemental iron 19 or 38 mg/day or placebo, and supplements were effective at both doses for alleviating iron deficiency in regular blood donors.63
Recovery of Blood Collected from Donors with IDWA Compared to Iron-Replete Donors
An important issue is whether the recovery of transfused blood is diminished in donors with IDWA compared to iron-replete ones. Α multicenter study of 13,403 donors that evaluated stored blood for osmotic and oxidative hemolysis and iron status by plasma ferritin measurement and self-reported intake of iron supplements, showed that prior donation intensity was negatively associated with in vitro oxidative hemolysis in multivariate analyses correcting for race-ethnicity, age, and sex.69 Moreover, in healthy human volunteers, a high proportion of storage-induced micro-erythrocytes in long-stored red blood cell concentrates correlates with poor transfusion recovery.70 The clinical significance of this information is unknown and remains to be determined by future studies with carefully selected endpoints.
Potential Adverse Effects of Oral Iron Supplementation in Regular Blood Donors
Regular blood donors are healthy, and they may object to taking oral pills daily, a maneuver that is viewed as turning them into patients. The STRIDE study, which, as previously explained, randomized 692 donors into one of two educational groups, or one of three interventional groups showed that de-enrolment within 60 days was more common in the interventional group, although not more common in those receiving iron than placebo.71 In a study of 1974 blood donors, 89% of whom were between the ages of 18 and 50 years, 49% declared that they would rather visit their general practitioner and 46% would rather receive iron supplementation. A higher number of donations was significantly associated with a preference for iron supplementation, and regular female donors were even more willing to take iron supplements.72
An important issue with oral iron supplementation in regular blood donors is safety, given the potential association of intravenous iron administration with infections.73 In this regard, a study of 82,062 Danish blood donors, who completed a questionnaire on health-related items showed that iron supplementation was safe, as it was not associated with an increased risk of infections requiring hospitalization or oral administration of antimicrobials.74
Another concern with providing iron to all blood donors is the possibility of worsening iron overload in donors with undiagnosed hemochromatosis, masking the symptoms of a clinically important gastrointestinal hemorrhage or other underlying medical conditions -most importantly gastrointestinal cancer, and causing side effects, mainly from the gastrointestinal tract. Finally, the potential risk of accidental iron poisoning in children of donors should be considered, since iron salts remain the leading cause of death from pediatric accidental poisoning.75,76
Conclusions
As shown by numerous studies, IDWA and IDA are very common among regular blood donors. There is an ethical obligation of blood bank physicians to preserve the health of volunteer blood donors by limiting iron deficiency, but without compromising the precious blood supply. The latter may be at risk due to the shrinking blood donor base and the potentially increasing blood requirements imposed by the aging population and other reasons, eg, climate change and its associated medical disasters. The optimal strategies to achieve that are not totally clear and ongoing clinical research will clarify unresolved issues. Pending further research in this area, most regular blood donors will benefit from the systematic administration of iron supplements post-donation. The AABB bulletin #17-02 correctly advocates low-dose iron supplements (≥18 mg/day for 60 days after WB donation or after every fourth or fifth apheresis donation), longer inter-donation intervals to allow dietary recovery of iron stores, or ferritin testing to help donors decide on ways of improving their iron status.22,26 While providing donors with iron supplements is effective in preventing declines in ferritin concentration and lowers the possibility of future donation deferrals for low hemoglobin, many factors should be taken into consideration when prescribing iron supplements in blood donors, such as the cost, potential side effects, availability of blood bank physicians for providing education in preventing iron deficiency, establishing responsibility for donors prescribed iron, etc.77 A double-blind, randomized controlled trial is underway to optimize the efficacy of oral iron supplementation while minimizing gastrointestinal complaints in WB donors (FORTE trial). Twelve hundred of them with ferritin ≤30 μg/L will be randomly assigned to one of six arms, ie, to receive capsules containing 0 mg, 30 mg, or 60 mg of iron, either on alternate days or daily for 56 days. At baseline and on days 56, 122, and 182 of follow-up, ferritin and hemoglobin will be measured, along with an assessment by questionnaire of the general health, compliance, dietary iron intake, gastrointestinal side effects, and iron deficiency-related symptoms.78 Finally, educational efforts should be intensified to improve the awareness of blood donation as a primary cause of iron deficiency among physicians of all specialties.
Abbreviations
AABB, American Association of Blood Banks; IDA, iron deficiency anemia; IDWA, iron deficiency without anemia; MCH, mean corpuscular (cell) hemoglobin; MCHr, mean cell hemoglobin of reticulocytes; MCV, mean corpuscular (cell) volume; Ret-He, reticulocyte hemoglobin content; RLS, restless leg syndrome; sTfR, soluble transferrin receptors; TIBC, total iron binding capacity; TSAT, transferrin saturation; US, United States of America; WB, whole blood; ZPP, zinc protoporphyrin.
Consent for Publication
All authors approved the submitted text and are accountable for all aspects of this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was available for this manuscript.
Disclosure
The authors have nothing to disclose about the current review article.
References
1. Reiss RF. Blood donor well-being: a primary responsibility of blood collection agencies. Ann Clin Lab Sci. 2011;41(1):3–7.
2. Goldman M, Uzicanin S, Scalia V, O’Brien SF. Iron deficiency in Canadian blood donors. Transfusion. 2014;54(3pt2):775–779. doi:10.1111/trf.12380
3. Boulton F. Managing donors and iron deficiency. Vox Sang. 2004;87(s2):22–24. doi:10.1111/j.1741-6892.2004.00448.x
4. Mast AE, Langer JC, Guo Y, et al. Genetic and behavioral modification of hemoglobin and iron status among first‐time and high‐intensity blood donors. Transfusion. 2020;60(4):747–758. doi:10.1111/trf.15743
5. Pratt JJ, Khan KS. Non-anaemic iron deficiency - a disease looking for recognition of diagnosis: a systematic review. Eur J Haematol. 2016;96(6):618–628. doi:10.1111/ejh.12645
6. Brownlie T, Utermohlen V, Hinton PS, Giordano C, Haas JD. Marginal iron deficiency without anemia impairs aerobic adaptation among previously untrained women. Am J Clin Nutr. 2002;75(4):734–742. doi:10.1093/ajcn/75.4.734
7. Bruner AB, Joffe A, Duggan AK, Casella JF, Brandt J. Randomised study of cognitive effects of iron supplementation in non-anaemic iron-deficient adolescent girls. Lancet. 1996;348(9033):992–996. doi:10.1016/S0140-6736(96)02341-0
8. Verdon F. Iron supplementation for unexplained fatigue in non-anaemic women: double blind randomised placebo controlled trial. BMJ. 2003;326(7399):1124. doi:10.1136/bmj.326.7399.1124
9. Vaucher P, Druais PL, Waldvogel S, Favrat B. Effect of iron supplementation on fatigue in nonanemic menstruating women with low ferritin: a randomized controlled trial. CMAJ. 2012;184(11):1247–1254. doi:10.1503/cmaj.110950
10. Amrein K, Macher S, Schröck M, Schlenke P, Drexler C. Iron deficiency in blood donors: perceptions and management among general practitioners and internists. Transfusion. 2017;57(10):2548–2549. doi:10.1111/trf.14297
11. Lobier M, Castrén J, Niittymäki P, Palokangas E, Partanen J, Arvas M. The effect of donation activity dwarfs the effect of lifestyle, diet and targeted iron supplementation on blood donor iron stores. PLoS One. 2019;14(8):e0220862. doi:10.1371/journal.pone.0220862
12. Cançado RD, Chiattone CS, Alonso FF, Langhi Júnior DM, Alves R. Iron deficiency in blood donors. Sao Paulo Med J. 2001;119(4):132–134. doi:10.1590/S1516-31802001000400003
13. Cable RG, Glynn SA, Kiss JE, et al. Iron deficiency in blood donors: the REDS-II Donor Iron Status Evaluation (RISE) study. Transfusion. 2012;52(4):702–711. doi:10.1111/j.1537-2995.2011.03401.x
14. Allen RP. Iron, RLS and blood donations. Sleep Med. 2004;5(2):113–114. doi:10.1016/j.sleep.2003.12.005
15. Bryant BJ, Yau YY, Arceo SM, Hopkins JA, Leitman SF. Ascertainment of iron deficiency and depletion in blood donors through screening questions for pica and restless legs syndrome. Transfusion. 2013;53(8):1637–1644. doi:10.1111/trf.12061
16. Liu H, Burns RT, Spencer BR, Page GP, Mast AE. For the NHLBI Recipient Epidemiology Donor Evaluation Study (REDS)‐III. Demographic, clinical, and biochemical predictors of pica in a large cohort of blood donors. Transfusion. 2021;61(7):2090–2098. doi:10.1111/trf.16409
17. Alvarez-Ossorio K, Kluter S. Low ferritin levels indicate the need for iron supplementation: strategy to minimize iron-depletion in regular blood donors. Transfus Med. 2000;10(2):107–112. doi:10.1046/j.1365-3148.2000.00239.x
18. Fillet A, Martinaud C, Malard L, et al. Iron deficiency among French whole‐blood donors: first assessment and identification of predictive factors. Vox Sang. 2021;116(1):42–52. doi:10.1111/vox.12991
19. Coad J, Pedley K. Iron deficiency and iron deficiency anemia in women. Scand J Clin Lab Invest. 2014;74(sup244):82–89. doi:10.3109/00365513.2014.936694
20. Patel EU, White JL, Bloch EM, et al. Association of blood donation with iron deficiency among adolescent and adult females in the United States: a nationally representative study. Transfusion. 2019;59(5):1723–1733. doi:10.1111/trf.15179
21. Badami KG, Taylor K. Iron status and risk-profiling for deficiency in New Zealand blood donors. N Z Med J. 2008;121(1274):50–60.
22. Vassallo RR, Hilton JF, Bravo MD, Vittinghoff E, Custer B, Kamel H. Recovery of Iron Stores After Adolescents Donate Blood. Pediatrics. 2020;146(1):e20193316. doi:10.1542/peds.2019-3316
23. Di Angelantonio E, Thompson SG, Kaptoge S, et al. Efficiency and safety of varying the frequency of whole blood donation (INTERVAL): a randomised trial of 45 000 donors. Lancet. 2017;390(10110):2360–2371. doi:10.1016/S0140-6736(17)31928-1
24. Salvin HE, Pasricha SR, Marks DC, Speedy J. Iron deficiency in blood donors: a national cross-sectional study. Transfusion. 2014;54(10):2434–2444. doi:10.1111/trf.12647
25. Karp JK, King KE. International variation in volunteer whole blood donor eligibility criteria. Transfusion. 2010;50(2):507–513. doi:10.1111/j.1537-2995.2009.02392.x
26. AABB. Updated Strategies to Limit or Prevent Iron Deficiency in Blood Donors. Bethesda, MD: AABB Association Bulletin AABB; 2017.
27. O’Meara A, Infanti L, Stebler C, et al. The value of routine ferritin measurement in blood donors. Transfusion. 2011;51(10):2183–2188. doi:10.1111/j.1537-2995.2011.03148.x
28. Goldman M, Magnussen K, Gorlin J, et al. International Forum regarding practices related to donor haemoglobin and iron. Vox Sang. 2016;111(4):449–455. doi:10.1111/vox.12431
29. Duggan F, O’Sullivan K, Power JP, Healy M, Murphy WG. Serum ferritin in plateletpheresis and whole blood donors. Transfus Apher Sci. 2016;55(1):159–163. doi:10.1016/j.transci.2016.06.004
30. Chinigi Sab P, Kaur G, Kaur P, et al. Assessment of serum iron stores in regular plateletpheresis donors. Transfus Apher Sci. 2022;61(1):103291. doi:10.1016/j.transci.2021.103291
31. O’Meara A, Infanti L, Sigle J, Stern M, Buser A. Switching iron-deficient whole blood donors to plateletpheresis. Transfusion. 2012;52(10):2183–2188. doi:10.1111/j.1537-2995.2012.03584.x
32. Radtke H, Meyer T, Kalus U, et al. Rapid identification of iron deficiency in blood donors with red cell indexes provided by Advia 120. Transfusion. 2005;45(1):5–10. doi:10.1111/j.1537-2995.2005.04205.x
33. Prinsze FJ, Groot R, Timmer TC, Zalpuri S, Hurk K. Donation‐induced iron depletion is significantly associated with low hemoglobin at subsequent donations. Transfusion. 2021;61(12):3344–3352. doi:10.1111/trf.16688
34. Gorlin J, Katz L, Elsmore D, et al. Prevalence of blood donor iron deficiency and feasibility ferritin-based iron replacement: a blood collection agency-based study. Vox Sang. 2016;111(2):206–208. doi:10.1111/vox.12408
35. Mast AE. Low hemoglobin deferral in blood donors. Transfus Med Rev. 2014;28(1):18–22. doi:10.1016/j.tmrv.2013.11.001
36. Kotzé SR, Pedersen OB, Petersen MS, et al. Predictors of hemoglobin in Danish blood donors: results from the Danish Blood Donor Study. Transfusion. 2015;55(6):1303–1311. doi:10.1111/trf.13011
37. Gestsdottir E, Magnusson MK, Lund SH, et al. Monitoring iron stores in Icelandic blood donors from 1997 through 2019. Transfus Med. 2022;32(2):128–134. doi:10.1111/tme.12856
38. Goldman M, Yi Q, Steed T, O’Brien SF. Changes in minimum hemoglobin and interdonation interval: impact on donor hemoglobin and donation frequency. Transfusion. 2019;59(5):1734–1741. doi:10.1111/trf.15155
39. Goldman M, Uzicanin S, Scalia J, Scalia V, O’Brien SF. Impact of informing donors of low ferritin results. Transfusion. 2016;56(9):2193–2198. doi:10.1111/trf.13691
40. France JL, France CR, Rebosa M, Shaz BH, Kessler DA. Promoting awareness of donation‐related iron depletion among high risk blood donors. Transfusion. 2021;61(12):3353–3360. doi:10.1111/trf.16694
41. Blake JT, O’Brien SF, Goldman M. The impact of donor ferritin testing on blood availability in Canada. Vox Sang. 2022;117(1):17–26. doi:10.1111/vox.13126
42. Baart AM, de Kort WLAM, Moons KGM, Atsma F, Vergouwe Y. Zinc protoporphyrin levels have added value in the prediction of low hemoglobin deferral in whole blood donors. Transfusion. 2013;53(8):1661–1669. doi:10.1111/j.1537-2995.2012.03957.x
43. Tiwari AK, Bhardwaj G, Arora D, et al. Applying newer parameter Ret‐He (reticulocyte haemoglobin equivalent) to assess latent iron deficiency (LID) in blood donors–study at a tertiary care hospital in India. Vox Sang. 2018;113(7):639–646. doi:10.1111/vox.12700
44. Boulton C, Inskip P. A study of the iron and HFE status of blood donors, including a group who failed the initial screen for anaemia. Br J Haematol. 2000;108(2):434–439. doi:10.1046/j.1365-2141.2000.01878.x
45. Alexander HD, Sherlock JP, Bharucha C. Red cell indices as predictors of iron depletion in blood donors. Clin Lab Haematol. 2000;22(5):253–258. doi:10.1046/j.1365-2257.2000.00323.x
46. Amir N, Md Noor S, Subbiah I, Osman M, Seman Z. Percentage of hypochromic red cells as a potential screening test to evaluate iron status in blood donors. Int J Lab Hem. 2019;41(3):418–423. doi:10.1111/ijlh.13009
47. Aardal Eriksson E, Mobäck C, Jakobsson S, Hoffmann JJML. Iron depletion in blood donors – have extended erythrocyte and reticulocyte parameters diagnostic utility? Transfus Apher Sci. 2015;53(1):76–81. doi:10.1016/j.transci.2015.03.011
48. Beck KL, Conlon CA, Kruger R, et al. Blood Donation, Being Asian, and a History of Iron Deficiency Are Stronger Predictors of Iron deficiency than dietary patterns in premenopausal women. Biomed Res Int. 2014;2014:1–7. doi:10.1155/2014/652860
49. Cable RG, Glynn SA, Kiss JE, et al. Iron deficiency in blood donors: analysis of enrollment data from the REDS-II Donor Iron Status Evaluation (RISE) study. Transfusion. 2011;51(3):511–522. doi:10.1111/j.1537-2995.2010.02865.x
50. Sayers MH. Iron supplementation? Ferritin screening? Why questions persist. Transfusion. 2019;59(5):1616–1619. doi:10.1111/trf.15303
51. Adu P, Banom S, Amediku MK, Amoaning RE, Quarshie AAA, Simpong DL. Poor iron store recovery in voluntary blood donors in the northern zone of Ghana; a five-month three-centre cohort study. Transfus Apher Sci. 2021;60(2):103040. doi:10.1016/j.transci.2020.103040
52. Wood EM, Miller JP. Low ferritin levels indicate the need for iron supplementation: strategy to minimize iron depletion in regular blood donors. Transfus Med. 2001;11(1):59–60. doi:10.1046/j.1365-3148.2001.00276.x
53. Kiss JE, Brambilla D, Glynn SA, et al. Oral Iron supplementation after blood donation: a randomized clinical trial. JAMA. 2015;313(6):575. doi:10.1001/jama.2015.119
54. Gordeuk V, Brittenham G, Bravo J, Hughes M, Keating L. Prevention of iron deficiency with carbonyl iron in female blood donors. Transfusion. 1990;30(3):239–245. doi:10.1046/j.1537-2995.1990.30390194345.x
55. Marks DC, Speedy J, Robinson KL, et al. An 8-week course of 45 mg of carbonyl iron daily reduces iron deficiency in female whole blood donors aged 18 to 45 years: results of a prospective randomized controlled trial. Transfusion. 2014;54(3pt2):780–788. doi:10.1111/trf.12464
56. Birgegård G, Schneider K, Ulfberg J. High incidence of iron depletion and restless leg syndrome (RLS) in regular blood donors: intravenous iron sucrose substitution more effective than oral iron. Vox Sang. 2010;99(4):354–361. doi:10.1111/j.1423-0410.2010.01368.x
57. Bryant BJ, Yau YY, Arceo SM, Daniel-Johnson J, Hopkins JA, Leitman SF. Iron replacement therapy in the routine management of blood donors. Transfusion. 2012;52(7):1566–1575. doi:10.1111/j.1537-2995.2011.03488.x
58. Krayenbuehl PA, Battegay E, Breymann C, Furrer J, Schulthess G. Intravenous iron for the treatment of fatigue in nonanemic, premenopausal women with low serum ferritin concentration. Blood. 2011;118(12):3222–3227. doi:10.1182/blood-2011-04-346304
59. Gybel-Brask M, Seeberg J, Thomsen LL, Johansson PI. Intravenous iron isomaltoside improves hemoglobin concentration and iron stores in female iron-deficient blood donors: a randomized double-blind placebo-controlled clinical trial. Transfusion. 2018;58(4):974–981. doi:10.1111/trf.14521
60. Cable RG, Brambilla D, Glynn SA, et al. Effect of iron supplementation on iron stores and total body iron after whole blood donation. Transfusion. 2016;56(8):2005–2012. doi:10.1111/trf.13659
61. Chiamchanya N. Rapid recovery time of hemoglobin level in female regular blood donors with ferrous fumarate and high dose of ascorbic acid supplement. J Med Assoc Thai. 2013;96(2):165–171.
62. Drexler C, Macher S, Lindenau I, et al. High-dose intravenous versus oral iron in blood donors with iron deficiency: the IronWoMan randomized, controlled clinical trial. Clinical Nutrition. 2020;39(3):737–745. doi:10.1016/j.clnu.2019.03.025
63. Mast AE, Bialkowski W, Bryant BJ, et al. A randomized, blinded, placebo-controlled trial of education and iron supplementation for mitigation of iron deficiency in regular blood donors. Transfusion. 2016;56(6pt2):1588–1597. doi:10.1111/trf.13469
64. Radtke H, Tegtmeier J, Röcker L, Salama A, Kiesewetter H. Daily doses of 20 mg of elemental iron compensate for iron loss in regular blood donors: a randomized, double-blind, placebo-controlled study. Transfusion. 2004;44(10):1427–1432. doi:10.1111/j.1537-2995.2004.04074.x
65. Radtke H, Tegtmeier J, Röcker L, Salama A, Kiesewetter H. Compensating for iron loss in regular blood donors using ferrous gluconate and ascorbic acid. Transfusion. 2005;45(7):1236–1237. doi:10.1111/j.1537-2995.2005.00183.x
66. Radtke H, Mayer B, Röcker L, Salama A, Kiesewetter H. Iron supplementation and 2-unit red blood cell apheresis: a randomized, double-blind, placebo-controlled study. Transfusion. 2004;44(10):1463–1467. doi:10.1111/j.1537-2995.2004.04045.x
67. Macher S, Herster C, Holter M, et al. The effect of parenteral or oral iron supplementation on fatigue, sleep, quality of life and restless legs syndrome in Iron-deficient blood donors: a secondary analysis of the IronWoMan RCT. Nutrients. 2020;12(5):1313. doi:10.3390/nu12051313
68. Vassallo RR. Donor iron depletion in context. Transfusion. 2021;61(1):318–321. doi:10.1111/trf.16219
69. Kanias T, Stone M, Page GP, et al. Frequent blood donations alter susceptibility of red blood cells to storage‐ and stress‐induced hemolysis. Transfusion. 2019;59(1):67–78. doi:10.1111/trf.14998
70. Roussel C, Morel A, Dussiot M, et al. Rapid clearance of storage-induced microerythrocytes alters transfusion recovery. Blood. 2021;137(17):2285–2298. doi:10.1182/blood.2020008563
71. Bialkowski W, Bryant BJ, Schlumpf KS, et al. The strategies to reduce iron deficiency in blood donors randomized trial: design, enrolment and early retention. Vox Sang. 2015;108(2):178–185. doi:10.1111/vox.12210
72. Chueca M, Bouvet G, Duron-Martinaud S, Doyen M, Poirrier L, Martinaud C. Iron-deficiency among blood donors: donors’ opinion on iron supplementation strategy. Transfus Clin Biol. 2020;27(4):218–221. doi:10.1016/j.tracli.2020.08.004
73. Shah AA, Donovan K, Seeley C, et al. Risk of infection associated with administration of intravenous Iron: a systematic review and meta-analysis. JAMA Netw Open. 2021;4(11):e2133935. doi:10.1001/jamanetworkopen.2021.33935
74. Kaspersen KA, Dinh KM, Mikkelsen S, et al. Oral iron supplementation is not associated with short-term risk of infections: results from the Danish blood donor study. Transfusion. 2019;59(6):2030–2038. doi:10.1111/trf.15221
75. Shannon M. Ingestion of Toxic Substances by Children. N Engl J Med. 2000;342(3):186–191. doi:10.1056/NEJM200001203420307
76. Litovitz TL, Klein-Schwartz W, Caravati EM, Youniss J, Crouch B, Lee S. 1998 annual report of the American association of poison control centers toxic exposure surveillance system. Am J Emerg Med. 1999;17(5):435–487. doi:10.1016/S0735-6757(99)90254-1
77. Pasricha SR, Marks DC, Salvin H, et al. Postdonation iron replacement for maintaining iron stores in female whole blood donors in routine donor practice: results of two feasibility studies in Australia. Transfusion. 2017;57(8):1922–1929. doi:10.1111/trf.14173
78. Karregat J, Sweegers MG, Quee FA, et al. Ferritin-guided iron supplementation in whole blood donors: optimal dosage, donor response, return and efficacy (FORTE)—a randomised controlled trial protocol. BMJ Open. 2022;12(3):e056316. doi:10.1136/bmjopen-2021-056316
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Clinical and Biological Manifestations in Women with Iron Deficiency Without Anemia Compared to Iron Deficiency Anemia in a General Internal Medicine Setting: A Retrospective Cohort Study
Hirosawa T, Hayashi A, Harada Y, Shimizu T
International Journal of General Medicine 2022, 15:6765-6773
Published Date: 23 August 2022
The Perceived Impact of Iron Deficiency and Iron Therapy Preference in Exercising Females of Reproductive Age: A Cross-Sectional Survey Study
Dugan C, Simpson A, Peeling P, Lim J, Davies A, Buissink P, MacLean B, Jayasuriya P, Richards T
Patient Preference and Adherence 2023, 17:2097-2108
Published Date: 24 August 2023