Back to Journals » Patient Preference and Adherence » Volume 17
The Perceived Impact of Iron Deficiency and Iron Therapy Preference in Exercising Females of Reproductive Age: A Cross-Sectional Survey Study
Authors Dugan C, Simpson A, Peeling P, Lim J, Davies A, Buissink P, MacLean B, Jayasuriya P, Richards T ![]()
Received 30 May 2023
Accepted for publication 12 August 2023
Published 24 August 2023 Volume 2023:17 Pages 2097—2108
DOI https://doi.org/10.2147/PPA.S397122
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Cory Dugan,1 Aaron Simpson,1 Peter Peeling,1 Jayne Lim,2 Amelia Davies,2 Paige Buissink,2 Beth MacLean,2 Pradeep Jayasuriya,2 Toby Richards2
1School of Human Sciences, University of Western Australia, Perth, WA, Australia; 2UWA Medical School and Division of Surgery, University of Western Australia, Perth, WA, Australia
Correspondence: Cory Dugan, School of Human Sciences, the University of Western Australia, 35 Stirling Highway, Crawley, WA, 6009, Australia, Tel +61 0401910790, Email [email protected]
Background: Patient perceptions of iron deficiency and efficacy of iron therapy may differ from the interpretations of doctors. Qualitative investigation at an individual level related may help define patient expectations and therapeutic targets. Therefore, we aimed to explore this concept in exercising females of reproductive age.
Methods: Exercising females (n = 403) who either (a) were currently experiencing iron deficiency, or (b) have experienced iron deficiency in the past were included. A survey comprising open-ended text response questions explored three ‘domains’: (1) the impact of iron deficiency, (2) the impact of iron tablet supplementation (where applicable), and (3) the impact of iron infusion treatment (where applicable). Questions were asked about training, performance, and recovery from exercise. Survey responses were coded according to their content, and sentiment analysis was conducted to assess responses as positive, negative, or neutral.
Results: Exercising females showed negative sentiment toward iron deficiency symptoms (mean range = − 0.94 to − 0.81), with perception that fatigue significantly impacts performance and recovery. Iron therapies were perceived to improve energy, performance, and recovery time. Participants displayed a strong positive sentiment (mean range = 0.74 to 0.79) toward iron infusion compared to a moderately positive sentiment toward oral iron supplementation (mean range = 0.44 to 0.47), with many participants perceiving that oral iron supplementation had no effect.
Conclusion: In Australia, women prefer an iron infusion in treatment of iron deficiency compared to oral iron.
Keywords: Iron deficiency, Women’s health, iron supplementation, iron supplementation preference, adherence, sentiment
Introduction
Iron deficiency (ID) is the most common nutrient deficiency globally, affecting approximately one-third of the population (2 billion people).1,2 The adverse health complications and symptoms of ID are well documented and include: fatigue, brain fog (reduced concentration), dizziness, headaches, restless legs, hair loss, and muscle weakness or soreness.3–6 Such symptoms are proposed to reduce both mental and physical health as well as overall patient quality of life.7,8
Iron deficiency is substantially prevalent in women of reproductive age, due to increased iron loss during menstruation and/or pregnancy.8–10 The prevalence rates of iron deficiency in exercising females in this age range from various cohort studies have been estimated to be as high as 50%.11–15 This is due to the combined effect of menstrual blood loss in conjunction with several avenues for iron loss during exercise; which include: food-related energy deficits (purposeful or not), exercise-induced haematuria (blood in urine), gastrointestinal bleeding, sweating, haemolysis, increased inflammation, and transient elevations in hepcidin.16–19 Research is currently ongoing as to the best strategies to overcome ID in exercising females encountering these issues. Given the inflammatory effects of exercise resulting in increased hepcidin concentrations, iron absorption is compromised in exercising populations, making it difficult to maintain optimal iron stores through diet alone.20,21 In combination with menstrual blood loss, exercising females often require iron replacement therapy to maintain optimal iron stores.
Oral iron supplementation is the most common treatment method for treating ID. Consumed as tablet or liquid preparations, oral iron supplements are widely used due to the low cost, low risk, and modest efficacy.20,22 When consumed over an 8 to 12-week period, at a dose of approximately 100 mg of elemental iron per day, exercising populations appear to increase their serum ferritin from 40 to 80%.18,23 However, due to poor absorption in the gut, the restoration of iron levels can take extended periods of time.24 In addition to the modest magnitude of the response, several potential side effects have been documented with the consumption of oral iron supplements; namely, constipation, heartburn, nausea, vomiting, diarrhoea and abdominal discomfort (gastrointestinal upset).25 Indeed, ferrous sulphate (the most common oral iron supplement) has been associated with 2.6 times the odds of gastrointestinal side effects compared to placebo.20,25 Further research has demonstrated insufficient adherence to oral iron supplements predominately due to gastrointestinal upset;26 resulting in suboptimal treatment efficacy.
An alternative therapy is intravenous iron therapy with direct injection of iron into the circulation allowing for absorption restrictions at the gut to be bypassed.27 Intravenous iron allows for rapid increases in iron status, studies reporting 200–400% increases in ferritin levels from a dose of 300 to 550 mg of iron.18,23,27,28 Despite the increased efficacy of treatment, due to the higher cost and more invasive nature of therapy, it is reserved for more severe cases of ID or when oral iron supplements are not tolerated. Adverse reactions to intravenous iron therapies are rare (such as hypersensitivity and anaphylaxis). However, despite being infrequent, they can be life threatening.29 Notwithstanding, newer intravenous iron supplementation formulations have been developed with ongoing advances in pharmaceutical technologies,30 and there has been a rapid increase in parenteral therapies for women of reproductive age in Australia (where intravenous iron is available on Medicare through GP practices).31 These preparations have allowed physicians to safely administer a full treatment dose in a clinical setting in 15–30 minutes.32 However, this research is purely from a clinical perspective, in non-healthy individuals (ie individuals with other adverse health complications aside from ID).
Regardless of the supplementation method, where serum ferritin is <40 μg/L, research suggests that there will be significant increases in serum ferritin if some form of intervention is undertaken.33,34 However, this does not necessarily correlate to improved fatigue and work capacity. Several randomised control trials have been conducted on the topic, with conflicting results. As with the ambivalence found in the clinical trials, differing conclusions exist across systematic reviews and meta-analyses.34–37 These reviews were highlighted in a recent Cochrane meta-analysis,37 where it was explained that substantial heterogeneity significantly impacted the outcomes, primarily due to the differences in research protocols (ie different definitions of iron deficiency, different participant characteristics, varying supplementation type and dose, inconsistent administration routes). This review was recently updated and suggested that iron therapy may improve fatigue scores; however, this is still supported by very low-quality evidence.38
When examining the literature concerning preference and adherence to these iron therapies, minimal research was found at the individual level. One systematic review, using the Cochrane methodology, has been conducted, comprising 12 studies across 17 countries, majority of which were third world countries. This review used thematic analysis to develop a conceptual framework of social determinants of iron supplementation among women of reproductive age. Several domains emerged; however, they were mainly drivers at the cultural or societal level (such as political circumstances, societal norms and values, education and communication, socio-economic circumstances, community and social support).39
To the best of our knowledge, no study has investigated individual perceptions regarding the efficacy of iron supplementation in healthy, exercising women of reproductive age. Despite the plethora of research investigating iron therapy from a quantitative perspective, there has been a relative inattention to integrating qualitative findings at the individual level, specifically in the case of iron therapies.39,40 In Australia, where IV iron is readily available and common practice, we wished to assess the perceived impact of ID on training, exercise capacity and recovery and the perceived efficacy of oral iron and IV iron on exercise capacity and recovery.
Methods
Research Design & Participants
A qualitative cross-section survey design was adopted (details below). The inclusion criteria were pre-menopausal females aged between 18 and 65 who were undertaking 3 or more hours of exercise per week. No exclusion criteria was applied to this population. However, individuals were asked if they have/had ID or anaemia, or if they were taking any medications or supplements. This data was recorded, and only those who reported a history of ID or anaemia were asked follow-up open-ended survey questions. Ethics approval to conduct this research was provided by the University of Western Australia (UWA HERC RA/4/20/6465). This research was conducted in compliance with recognised international standards and adheres to the declaration of Helsinki. As such, all individuals were required to provide informed consent prior to participating in the research.
Survey Design
The survey has previously been used and validated6,41–44 (Appendix 1). Yes/no polar questions were asked to collect information on participant demographics, history of iron supplementation, and average number of hours they exercised each week. Eight open-ended free-text questions were asked. These questions were designed to invite participants to describe – in their own words – the impact of iron deficiency, as well as the perceived efficacy of iron therapies (both oral and intravenous) on exercise training, performance, and recovery (Appendix 1).
Data Analysis
Data were screened, and descriptive characteristics were calculated. Open-ended survey items required two authors (AS, CD) to independently familiarise themselves with the data, initially coding 10% of responses for cross-examination of inter-rater agreement. Once agreement was confirmed, AS coded the remaining responses for each survey item, repeatedly cross-checking with CD to ensure accuracy.
Manifest content (ie literal/semantic meaning of words, as opposed to latent/underlying meaning) in responses to open-ended questions were determined and assigned to categories.45 After initial coding, frequency counts were also performed to highlight key terms or phrases used by participants. Finally, we performed a basic manual sentiment analysis to determine whether each response was framed positively (given a score of 1), negatively (given a score of −1), or neutral/ambiguous (given a score of 0), which was then summated to determine an overall participant sentiment (or tone) for each survey item.46,47 For example, a general sentiment of 0.5 for a question on the impact of oral iron supplementation on performance would indicate that participants (on average) had a moderate positive sentiment about the impact of oral iron supplementation (ie it is generally perceived as having a positive impact). Two authors (JF, HN) independently coded the sentiment of each response, with disagreements settled by a third author (AS). Cohen’s kappa (κ)48 coefficients are presented for each survey item as a measure of interrater reliability, with confidence intervals being calculated from standard error values.
Results
Descriptive Characteristics
One thousand and forty-two females completed the questionnaire. Of this sample, a sub-sample of 403 individuals completed the survey, answering all polar questions and at least one open-ended text question (based on their responses to current/history of ID, anaemia, and iron therapy). The average age was 29.84 ± 10.59 years old. The mean height was 166.48 ± 8.8cm and the average weight was 64.80 ± 11.15 kg. The number of hours exercised per week was 7.63 ± 4.29 hours.
In the entire sample, previous history of ID was reported by 338 (83.9%) of participants. Previous history of anaemia was reported by 131 (32.5%) of participants. Of these participants, 354 (87.8%) reported the use of some form of iron supplementation; with 331 (82.1%) reported the previous use of oral iron supplements, and 153 (38%) iron infusions.
Open Ended Survey Items
Across all items, response word counts were low (two to five words on average). A full description of key terms and phrases, sentiment, and reliability analyses is presented in Table 1. Manifest content analyses are presented in three broad topic areas: (1) Participants’ perceptions of the impact of ID symptoms on performance and recovery; (2) participants’ perceptions of the impact of oral iron supplementation on training, performance, and recovery; and (3) participants’ perceptions of the impact of iron infusion treatment on training, performance, and recovery. All codes identified within participants’ text responses (with examples) are presented in Table 2 (topic area 1), Table 3 (topic area 2), and Table 4 (topic area 3), and a schematic presentation of code categories is provided in Figure 1.
 |
Table 1 Key Terms, Overall Sentiment and Interrater Reliability for Sentiment Analyses |
 |
Table 2 Content and Examples of Responses on the Impact of Iron Deficiency Symptoms |
 |
Table 3 Content and Examples of Responses on the Impact of Iron Tablet Supplementation |
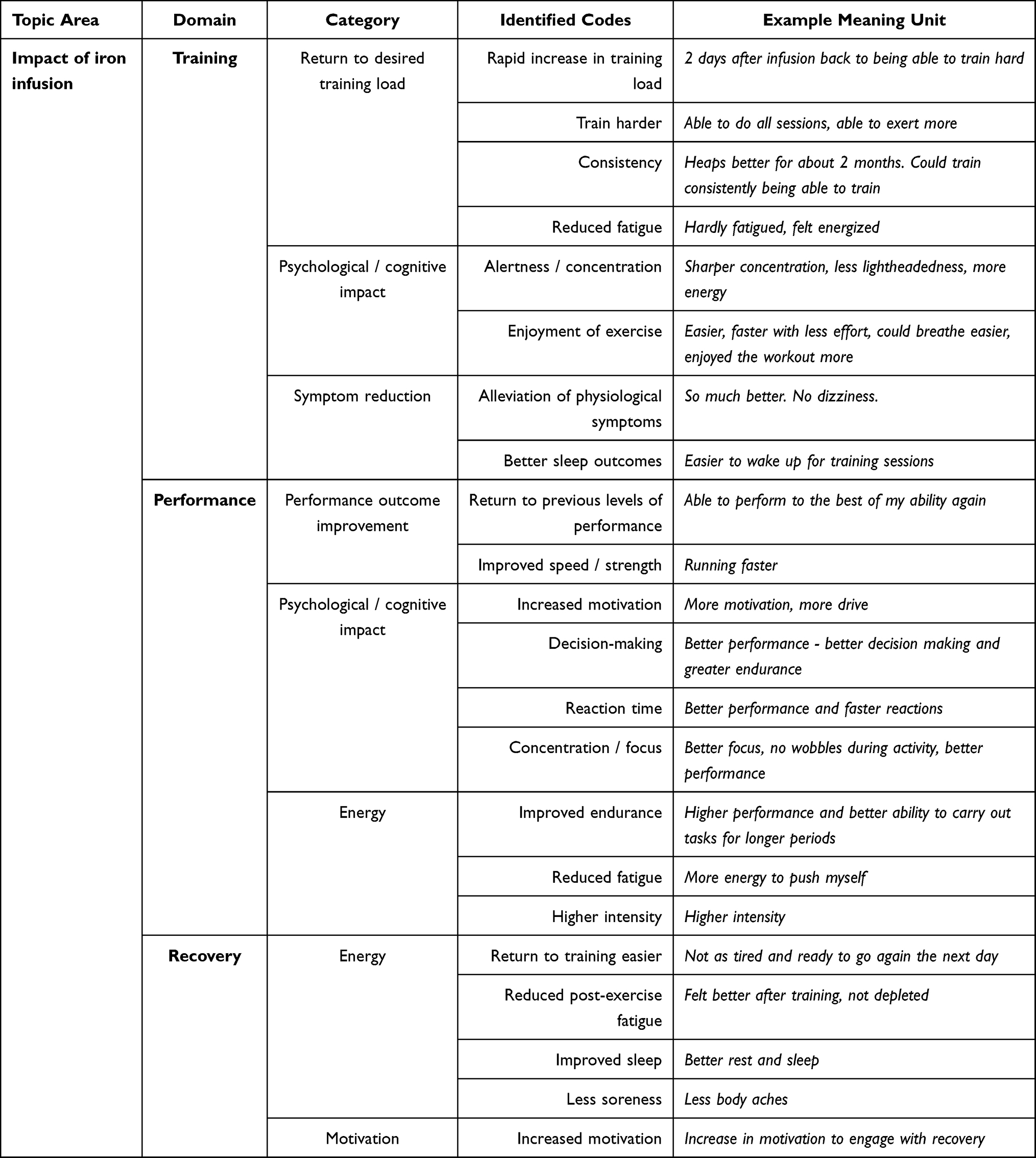 |
Table 4 Content and Examples of Responses on the Impact of Iron Infusion |
 |
Figure 1 A graphical presentation of code categories within each domain. Notes: The figure includes all categories of codes for each domain, but does not provide the individual codes within each category. For a full description of codes identified within participants’ responses, see Tables 2–4. The colours included in the figure are for differentiation between domains only (ie, for ease of reading) and are not to be interpreted as providing any information or inferences about the dataset. |
Perceived Impact of Iron Deficiency
As expected, there was a strong negative sentiment of ID in regard to exercise performance (sentiment mean −0.94) and recovery (sentiment mean −0.81). Several categories emerged from the manifest content. Both physiological (energy decline, reduced ability to exercise) and psychological (decreases in motivation, increase in cognitive challenges) impacts were reported on exercise performance (Table 2). Longer recovery times were also described, which resultantly inhibited regular exercise routines (Table 2).
Perceived Efficacy of Oral Iron Supplementation
Moderate positive sentiment was observed regarding the perceived efficacy of oral iron supplementation on training (sentiment mean +0.45), performance (sentiment mean +0.47), and recovery (sentiment mean +0.44). Similar categories emerged from the manifest content for the 3 domains (Table 3). Participants commonly reported symptom reduction as well as improved; performance outcomes, energy levels, cognitive abilities, and training load. However, there was also a high number of neutral/ambiguous responses. Participants often described their experience with words such as “no”, “not”, “none”, or “nil”, indicating a perceived lack of benefit. Also, some side effects were frequently noted by participants in all three of the above domains. Most often, these were issues such as stomach aches, constipation, and vomiting.
Perceived Efficacy of Intravenous Iron Supplementation
Strong positive sentiment was observed concerning the perceived efficacy of intravenous iron supplementation on training (sentiment mean +0.79), performance (sentiment mean +0.76), and recovery (sentiment mean +0.74). Several categories emerged from the manifest content regarding the 3 domains, as shown in Table 4. All categories were derived from highly positive identified codes, suggesting a greater preference for intravenous iron supplementation.
Discussion
The present study demonstrates a clear perceived impact of ID in active or habitually exercising women of reproductive age. In accordance with previous research,6,41 the greatest perceived impact relating to ID was fatigue and energy decline. Specifically, participants reported that they were unable to; perform at optimal levels, that fatigue was a significant barrier to exercise, and consequently, that there was a reduction in their ability to exercise. In terms of recovery, participants reported that they required additional rest between exercise bouts, which inhibited their desired routine (ie keeping up with a structured exercise routine or training schedule). Such outcomes can be detrimental to exercise performance due to a decreased training volume within a specific time frame. Psychological impacts were also commonly reported. For example, participants described decreases in motivation to exercise in conjunction with difficulties in cognition (ability to focus/concentrate), which ultimately affected decision-making. Overall, there was a very strong negative sentiment towards ID both from a physiological and a psychological perspective.
To correct ID, individuals generally engage in iron therapies through oral supplementation or intravenous iron infusions. Both forms of therapy have their advantages and disadvantages, mainly due to tolerability and safety issues.30 For example, oral iron therapy can take several months to correct iron stores49 and is typically associated with gastrointestinal side effects, such as: constipation, nausea, vomiting, diarrhoea and abdominal discomfort.25 Nevertheless, the present study has demonstrated a moderate positive sentiment between oral iron supplementation and exercise performance, training, and recovery. Indeed, in response to oral iron supplementation, participants commonly noted exercise performance improvements, symptom reduction and increases in energy levels – typically allowing for a return to desired training/recovery routines. Further, participants described cognitive improvements, such as greater focus and productivity, allowing for better results at competitions. These findings support oral iron as the first line of treatment to correct ID,20,22 especially considering contemporary research demonstrating more efficient ways to achieve equilibrium between iron absorption and tolerability from oral iron supplement approaches (ie lower dose, enteric coated tablets, alternate day supplementation, etc.).49–51
In more severe cases of ID (such as iron deficiency anaemia), or when oral iron supplements are not tolerated due to gastrointestinal side effects, other forms of therapy might be considered by the practitioner, such as intravenous iron infusions. Previous research has shown high levels of non-adherence towards oral iron supplements,26,30 mainly due to gastrointestinal side effects, in addition to weight gain under treatment.26 This could explain, in part, the rapid increase in intravenous iron therapy for women of reproductive age in Australia.31 The present study demonstrates a high sentiment towards intravenous iron therapies and exercise performance, training, and recovery, with both physiological and psychological benefits reported from such approaches. Physiologically, participants reported greater energy levels and reduced fatigue, allowing for rapid increases in training loads (some reported as little as 2 days). Further, with regard to recovery, participants commonly described a reduction in post-exercise fatigue, improved sleep, and less soreness, allowing for an easier return to optimal training loads. Psychologically, participants reported higher levels of perceived concentration, improved focus, better reaction time, and improved decision-making. Overall, similar to oral iron supplementation, positive sentiment was generally characterised by participants regarding parenteral iron therapies with respect to exercise performance, training, and recovery. However, unlike oral iron therapy, adverse reactions from IV approaches (such as hypersensitivity and anaphylaxis) can be life-threatening.29 Notwithstanding, newer and safer intravenous iron formulations have been developed with ongoing advances in pharmaceutical technologies,29,30,32,52–54 providing further evidence for increased use of intravenous iron. This research, however, is purely from a clinical perspective, in non-healthy individuals (ie individuals with other adverse health complications aside from ID).
Recent research has questioned the rise in intravenous iron therapies in iron deficient individuals who are otherwise healthy, specifically those that are iron deficient without anaemia (IDNA).31 Fivefold increased incidence rates have been observed in intravenous iron therapies between 2013 and 2017 for women of reproductive age in Australia.31 Although this selection of treatment has been justified in clinical practise,32 the change in popularity of treatment has raised concerns about whether intravenous iron is used appropriately and cost effectively in exercising populations,31,55 especially given that the literature on the efficacy of intravenous iron therapies on exercise performance in individuals with IDNA is equivocal.33–36,56 Indeed, studies have shown studies both increases18 and no change27,28 to exercise capacity in response to a dose of intravenous iron. A recent review article has highlighted the need for a greater understanding of the increased use of intravenous iron in such populations. It was concluded that qualitative studies would provide important information on the motivating factors for exercising populations to seek intravenous therapies of all kinds, which would inform educational strategies to meet nutritional and performance needs.55 The present study demonstrates positive sentiment responses for the efficacy of oral and intravenous iron supplements on exercise performance, training, and recovery; with a greater positive sentiment being observed in intravenous iron therapies. These findings highlight the need for quantitative research investigating physiological evidence on the efficacy of iron supplementations in exercise performance, as the current literature remains divergent.37 Due to the heterogeneity of the current literature, even meta-analysis methodologies cannot reach consensus on this topic.33–37,56,57 As such, future research should consider individual patient data meta-analysis techniques in conjunction with highly powered randomised control trials.
The findings of this study should be considered in light of its limitations. First, the average response duration was very short; although we were able to extract meaning from the short responses, more detailed responses may have resulted in a greater understanding of the perspectives of the participants. In the future, researchers should explore methods to elicit more in-depth responses to ID queries. Second, keywords were treated in isolation—that is, direction of the term was not considered (for example, the word “better” in isolation has a different meaning to “it did not get better”). However, we are confident that the data presented in this study accurately represent the general perceptions of the participants, and we provide bigram and trigram data for additional context.
Overall, positive sentiment was demonstrated for both oral iron supplementation and intravenous iron therapy to correct ID and anaemia, with a greater sentiment toward intravenous iron therapies in exercising females of reproductive age. This could explain the rapid increase in intravenous iron use; however, qualitative responses suggest several similarities between the two therapies with respect to their efficacy in treatment, suggesting that the cheaper and safer option should be used as first-line treatment (oral iron supplementation); which corroborates previous research. However, further research is required to determine the efficacy of intravenous iron therapy on exercise performance, particularly in IDNA exercising females of reproductive age.
Acknowledgment
No funding was provided for this research.
Disclosure
PJ reports personal fees from Vifor Pharma and Pfizer Australia, outside the submitted work. TR reports grants from UK, NIHR HTA, grants from Australian, NHMRC, grants, personal fees and non-financial support from Pharmacosmos; grants, personal fees and non-financial support from Vifor Pharma and BioAge Labs; grants from NIHR EME, Pfizer Australia; personal fees from Medtronic; grants from Australian MRFF, outside the submitted work; and TR is a regular speaker at national and international conferences on anaemia, blood transfusion, wound healing and vascular diseases for which he has received expenses for travel, accommodation and sundries. TR has worked with several agencies promoting meetings or healthcare. TR is director of The Iron Clinic Ltd and director of Veincare London Ltd also TR is the Vascular lead for 18-week wait Ltd. No funding was provided by these institutions for this research. The other authors report no conflicts of interest in this work.
References
1. Longo DL, Longo DL, Longo DL. Iron-deficiency anemia. N Engl J Med. 2015;372(19):1832–1843. doi:10.1056/NEJMra1401038
2. Kassebaum NJ. The global burden of anemia. Hematol Oncol Clin. 2016;30(2):247–308. doi:10.1016/j.hoc.2015.11.002
3. Pasricha S-R, Tye-Din J, Muckenthaler MU, Swinkels DW. Iron deficiency. Lancet. 2020. doi:10.1016/s0140-6736(20)32594-0
4. Zia A, Stanek J, Christian‐Rancy M, Savelli S, O’Brien SH. Iron deficiency and fatigue among adolescents with bleeding disorders. Am J Hematol. 2021;97:60–67. doi:10.1002/ajh.26389
5. Beatrix J, Piales C, Berland P, Marchiset E, Gerbaud L, Ruivard M. Non-anemic iron deficiency: correlations between symptoms and iron status parameters. Eur J Clin Nutr. 2022;76(6):835–840. doi:10.1038/s41430-021-01047-5
6. Dugan C, Scott C, Abeysiri S, Baikady RR, Richards T. The need to screen for anemia in exercising women. Medicine. 2021;100(39):e27271. doi:10.1097/md.0000000000027271
7. Munro MG, Mast AE, Powers JM, et al. The relationship between heavy menstrual bleeding, iron deficiency, and iron deficiency anemia. Am J Obstet Gynecol. 2023;229:1–9. doi:10.1016/j.ajog.2023.01.017
8. Peuranpää P, Heliövaara‐Peippo S, Fraser I, Paavonen J, Hurskainen R. Effects of anemia and iron deficiency on quality of life in women with heavy menstrual bleeding. Acta Obstet Gynecol Scand. 2014;93(7):654–660. doi:10.1111/aogs.12394
9. Nelson AL, Ritchie JJ. Severe anemia from heavy menstrual bleeding requires heightened attention. Am J Obstet Gynecol. 2015;213(1):97. e1–97. e6. doi:10.1016/j.ajog.2015.04.023
10. Fraser IS, Mansour D, Breymann C, Hoffman C, Mezzacasa A, Petraglia F. Prevalence of heavy menstrual bleeding and experiences of affected women in a European patient survey. Int J Gynaecol Obstet. 2015;128(3):196–200. doi:10.1016/j.ijgo.2014.09.027
11. Haymes EM, Puhl JL, Temples TE. Training for cross-country skiing and iron status. Med Sci Sports Exerc. 1986;18(2):162–167. doi:10.1249/00005768-198604000-00003
12. Selby GB, Eichner ER. Endurance swimming, intravascular hemolysis, anemia, and iron depletion: new perspective on athlete’s anemia. Am J Med. 1986;81(5):791–794. doi:10.1016/0002-9343(86)90347-5
13. Sinclair LM, Hinton P. Prevalence of iron deficiency with and without anemia in recreationally active men and women. J Am Diet Assoc. 2005;105(6):975–978. doi:10.1016/j.jada.2005.03.005
14. DellaValle DM, Haas JD. Impact of iron depletion without anemia on performance in trained endurance athletes at the beginning of a training season: a study of female collegiate rowers. Int J Sport Nutr Exerc Metab. 2011;21(6):501–506. doi:10.1123/ijsnem.21.6.501
15. Koehler K, Braun H, Achtzehn S, et al. Iron status in elite young athletes: gender-dependent influences of diet and exercise. Eur J Appl Physiol. 2012;112(2):513–523. doi:10.1007/s00421-011-2002-4
16. Nielsen P, Nachtigall D. Iron supplementation in athletes. Sports Med. 1998;26(4):207–216. doi:10.2165/00007256-199826040-00001
17. Garvican LA, Lobigs L, Telford R, Fallon K, Gore CJ. Haemoglobin mass in an anaemic female endurance runner before and after iron supplementation. Int J Sports Physiol Perform. 2011;6(1):137–140. doi:10.1123/ijspp.6.1.137
18. Garvican LA, Saunders PU, Cardoso T, et al. Intravenous iron supplementation in distance runners with low or suboptimal ferritin. Med Sci Sports Exerc. 2014;46(2):376–385. doi:10.1249/MSS.0b013e3182a53594
19. Peeling P, Sim M, Badenhorst CE, et al. Iron status and the acute post-exercise hepcidin response in athletes. PLoS One. 2014;9(3):e93002. doi:10.1371/journal.pone.0093002
20. McCormick R, Sim M, Dawson B, Peeling P. Refining treatment strategies for iron deficient athletes. Sports Med. 2020;50(12):2111–2123. doi:10.1007/s40279-020-01360-2
21. McKay AKA, Peeling P, Pyne DB, et al. Chronic adherence to a ketogenic diet modifies iron metabolism in elite athletes. Med Sci Sports Exerc. 2019;51:548–555. doi:10.1249/MSS.0000000000001816
22. Mansour D, Hofmann A, Gemzell-Danielsson K. A review of clinical guidelines on the management of iron deficiency and iron-deficiency anemia in women with heavy menstrual bleeding. Adv Ther. 2020;38:201–225. doi:10.1007/s12325-020-01564-y
23. Dawson B, Goodman C, Blee T, et al. Iron supplementation: oral tablets versus intramuscular injection. Int J Sport Nutr Exerc Metab. 2006;16(2):180–186. doi:10.1123/ijsnem.16.2.180
24. Richards MT. Anaemia in hospital practice. Br J Hosp Med. 2012;73(10):571–575. doi:10.12968/hmed.2012.73.10.571
25. Tolkien Z, Stecher L, Mander AP, Pereira DIA, Powell JJ. Ferrous sulfate supplementation causes significant gastrointestinal side-effects in adults: a systematic review and meta-analysis. PLoS One. 2015;10(2):e0117383. doi:10.1371/journal.pone.0117383
26. Gereklioglu C, Asma S, Korur A, Erdogan F, Kut A. Medication adherence to oral iron therapy in patients with iron deficiency anemia. Pak J Med Sci. 2016;32(3):604–607. doi:10.12669/pjms.323.9799
27. Burden RJ, Pollock N, Whyte GP, et al. Effect of intravenous iron on aerobic capacity and iron metabolism in elite athletes. Med Sci Sports Exerc. 2015;47(7):1399–1407. doi:10.1249/MSS.0000000000000568
28. Woods A, Garvican-Lewis LA, Saunders PU, et al. Four weeks of IV iron supplementation reduces perceived fatigue and mood disturbance in distance runners. PLoS One. 2014;9(9):e108042. doi:10.1371/journal.pone.0108042
29. Rampton D, Folkersen J, Fishbane S, et al. Hypersensitivity reactions to intravenous iron: guidance for risk minimization and management. Haematologica. 2014;99(11):1671–1676. doi:10.3324/haematol.2014.111492
30. Girelli D, Ugolini S, Busti F, Marchi G, Castagna A. Modern iron replacement therapy: clinical and pathophysiological insights. Int J Hematol. 2018;107(1):16–30. doi:10.1007/s12185-017-2373-3
31. Shand AW, Bell J, Henry A, et al. Rapid increase in intravenous iron therapy for women of reproductive age in Australia. Med J Aust. 2020;213(2):85–86. doi:10.5694/mja2.50618
32. Richards T, Breymann C, Brookes MJ, et al. Questions and answers on iron deficiency treatment selection and the use of intravenous iron in routine clinical practice. Ann Med. 2021;53(1):274–285. doi:10.1080/07853890.2020.1867323
33. Pasricha S-R, Low M, Thompson J, Farrell A, De-Regil L-M. Iron supplementation benefits physical performance in women of reproductive age: a systematic review and meta-analysis. J Nutr. 2014;144(6):906–914. doi:10.3945/jn.113.189589
34. Burden RJ, Morton K, Richards T, Whyte GP, Pedlar CR. Is iron treatment beneficial in, iron-deficient but non-anaemic (IDNA) endurance athletes? A systematic review and meta-analysis. Br J Sports Med. 2015;49(21):1389–1397. doi:10.1136/bjsports-2014-093624
35. Houston BL, Hurrie D, Graham J, et al. Efficacy of iron supplementation on fatigue and physical capacity in non-anaemic iron-deficient adults: a systematic review of randomised controlled trials. BMJ open. 2018;8(4):e019240. doi:10.1136/bmjopen-2017-019240
36. Rubeor A, Goojha C, Manning J, White J. Does iron supplementation improve performance in iron-deficient nonanemic athletes? Sports Health. 2018;10(5):400–405. doi:10.1177/1941738118777488
37. Miles LF, Litton E, Imberger G, Story D. Intravenous iron therapy for non‐anaemic, iron‐deficient adults. Cochrane Database Syst Rev. 2019. doi:10.1002/14651858.CD013084.pub2
38. Dugan C, Cabolis K, Miles LF, Richards T. Systematic review and meta‐analysis of intravenous iron therapy for adults with non‐anaemic iron deficiency: an abridged Cochrane review. J Cachexia Sarcopenia Muscle. 2022;13:2637–2649. doi:10.1002/jcsm.13114
39. Nagata JM, Gatti LR, Barg FK. Social determinants of iron supplementation among women of reproductive age: a systematic review of qualitative data. Matern Child Nutr. 2012;8(1):1–18. doi:10.1111/j.1740-8709.2011.00338.x
40. Atkins S, Lewin S, Smith H, Engel M, Fretheim A, Volmink J. Conducting a meta-ethnography of qualitative literature: lessons learnt. BMC Med Res Methodol. 2008;8(1):21. doi:10.1186/1471-2288-8-21
41. Abeysiri S, Dugan C, Raobaikady R, Richards T, Scott C. The need to screen for anaemia in female populations. J Sci Med Sport. 2021;24:S30–S31. doi:10.1016/j.jsams.2021.09.081
42. Bruinvels G, Pedlar C, Burden R, Yong T, Cushway T, Richards T. Heavy Menstrual Bleeding and iron status in exercising women in Singapore.
43. Bruinvels G, Burden R, Brown N, Richards T, Pedlar C. The prevalence and impact of heavy menstrual bleeding among athletes and mass start runners of the 2015 London Marathon. Br J Sports Med. 2016;50(9):566. doi:10.1136/bjsports-2015-095505
44. Bruinvels G, Burden R, Brown N, Richards T, Pedlar C. The prevalence and impact of heavy menstrual bleeding (menorrhagia) in elite and non-elite athletes. PLoS One. 2016;11(2). doi:10.1371/journal.pone.0149881
45. Kleinheksel AJ, Rockich-Winston N, Tawfik H, Wyatt TR. Demystifying content analysis. Am J Pharm Educ. 2020;84(1):127–137. doi:10.5688/ajpe7113
46. Van Atteveldt W, Van Der Velden MA, Boukes M. The validity of sentiment analysis: comparing manual annotation, crowd-coding, dictionary approaches, and machine learning algorithms. Commun Methods Meas. 2021;15(2):121–140. doi:10.1080/19312458.2020.1869198
47. Boukes M, Van De Velde B, Araujo T, Vliegenthart R. What’s the Tone? Easy doesn’t do it: analyzing performance and agreement between off-the-shelf sentiment analysis tools. Commun Methods Meas. 2020;14(2):83–104. doi:10.1080/19312458.2019.1671966
48. Cohen J. A coefficient of agreement for nominal scales. Educ Psychol Meas. 1960;20(1):37–46. doi:10.1177/001316446002000104
49. Stoffel NU, von Siebenthal HK, Moretti D, Zimmermann MB. Oral iron supplementation in iron-deficient women: how much and how often? Mol Aspects Med. 2020;75:100865. doi:10.1016/j.mam.2020.100865
50. Stoffel NU, Zeder C, Brittenham GM, Moretti D, Zimmermann MB. Iron absorption from supplements is greater with alternate day than with consecutive day dosing in iron-deficient anemic women. Haematologica. 2020;105(5):1232–1239. doi:10.3324/haematol.2019.220830
51. McCormick R, Dreyer A, Dawson B, et al. The effectiveness of daily and alternate day oral iron supplementation in athletes with suboptimal iron status (part 2). Int J Sport Nutr Exerc Metab. 2020;30(3):191–196. doi:10.1123/ijsnem.2019-0310
52. Auerbach M, Deloughery T. Single-dose intravenous iron for iron deficiency: a new paradigm. Hematology. 2016;2016(1):57–66. doi:10.1182/asheducation-2016.1.57
53. Ponikowski P, Filippatos G, Colet JC, et al. The impact of intravenous ferric carboxymaltose on renal function: an analysis of the FAIR‐HF study. Eur J Heart Fail. 2015;17(3):329–339. doi:10.1002/ejhf.229
54. Avni T, Bieber A, Grossman A, Green H, Leibovici L, Gafter-Gvili A. The safety of intravenous iron preparations: systematic review and meta-analysis. Mayo Clin Proc. 2015;90(1):12–23. doi:10.1016/j.mayocp.2014.10.007
55. Lewis N, Hodgson A, Khanbhai T, et al. Rise of intravenous nutrition products among professional team sport athletes: reasons to be concerned? BMJ. 2022;379. doi:10.1136/bmj-2022-072141
56. Miles LF, Litton E, Imberger G, Story D. Intravenous iron therapy for non‐anaemic iron deficient adults. Cochrane Database Syst Rev. 2018;2018(8):CD013084. doi:10.1002/14651858.CD013084
57. Cusack H, Hewlings S. The impact of iron supplementation on athletic performance in elite-level female athletes–A systematic review. Strength Cond J. 2023;45:342–353. doi:10.1519/SSC.0000000000000742
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Iron Deficiency and Blood Donation: Links, Risks and Management
Mantadakis E, Panagopoulou P, Kontekaki E, Bezirgiannidou Z, Martinis G
Journal of Blood Medicine 2022, 13:775-786
Published Date: 10 December 2022