Back to Journals » Journal of Pain Research » Volume 16
Investigating the Therapeutic Effect of Intradermal Acupuncture for Acute Herpes Zoster and Assessing the Feasibility of Infrared Thermography for Early Prediction of Postherpetic Neuralgia: Study Protocol for a Randomized, Sham-Controlled, Clinical Trial
Authors Hu H ![]() , Cheng Y, Wu L
, Cheng Y, Wu L ![]() , Han D, Ma R
, Han D, Ma R ![]()
Received 15 February 2023
Accepted for publication 20 April 2023
Published 26 April 2023 Volume 2023:16 Pages 1401—1413
DOI https://doi.org/10.2147/JPR.S406841
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Hantong Hu,1,2,* Yingying Cheng,1,* Lei Wu,1 Dexiong Han,1,2 Ruijie Ma1,2
1Department of Acupuncture and Moxibustion, The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou City, People’s Republic of China; 2Department of Neurobiology and Acupuncture Research, The Third Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou City, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ruijie Ma; Dexiong Han, Department of Acupuncture and Moxibustion, The Third Affiliated Hospital of Zhejiang Chinese Medical University, No. 548 Binwen Road, Hangzhou City, People’s Republic of China, Email [email protected]; [email protected]
Introduction: Herpes zoster (HZ) can adversely influence patients’ quality of life and sometimes it can develop postherpetic neuralgia (PHN). To date, it remains challenging to be managed by currently available therapies. Intradermal acupuncture (IDA) has the potential to be an adjunctive therapy for acute HZ and infrared thermography (IRT) may be useful for predicting PHN; however, current evidence remains inconclusive. Therefore, the purposes of this trial are to 1) evaluate the efficacy and safety of IDA as an adjunctive therapy for acute HZ; 2) to explore the feasibility of IRT for early prediction of PHN and as an objective tool to aid in subjective pain assessment in acute HZ.
Methods: This study is designed as a randomized, parallel-group, sham-controlled, and patient-assessor-blinded trial, including 1-month treatment and 3-month follow-ups. Seventy-two qualified participants will be randomly split into the IDA or sham IDA group in a ratio of 1:1. Apart from standard pharmacological treatments in both groups, the two groups will receive 10 sessions of IDA or sham IDA, respectively. Primary outcome measures are the visual analog scale (VAS), indicators of herpes lesions’ recovery, the temperature of the pain area, and the incidence rate of PHN. The secondary outcome is the 36-item Short Form Health Survey (SF-36). Indicators of herpes lesions’ recovery will be assessed at each visit and follow-ups. The remaining outcomes will be assessed at baseline, 1 month after intervention, and 3-month follow-up. Safety evaluation will be determined by adverse events during the trial.
Conclusion: Expected results will determine whether IDA can enhance therapeutic effectiveness of pharmacotherapy for acute HZ with acceptable safety profile. In addition, it will verify the accuracy of IRT for early prediction of PHN and as an objective tool of subjective pain for acute HZ.
Trial Registration: Clinicaltrials.gov (identification number: NCT05348382; Registered 27 April 2022, https://clinicaltrials.gov/ct2/show/NCT05348382).
Keywords: acupuncture, herpes zoster, postherpetic neuralgia, infrared thermography, clinical trial
Introduction
Herpes zoster (HZ) is featured by a band-like rash in the dermatome that corresponds to the affected nerve. Epidemiological data has revealed that it occurs annually in at least 1 million individuals in the US,1 and the incidence rate has been increasing across the world in the past two decades.2 It is reported that at least 20–30% of the population and up to 50% of those living until age 85 years suffer from HZ.3,4 Patients with HZ frequently experience pain, which can be triggered by gentle touch. Other possible symptoms include a general feeling of being unwell, photophobia, headache, and malaise. Postherpetic neuralgia (PHN) is the most common sequelae of HZ, which is generally defined as persistent pain for more than 3 months after the onset of HZ rash5 and it is generally intractable to treat. It is reported that the frequency of PHN among patients more than 60 years old was approximately 13% at 3 months and 7% at 1 year.3
Currently, analgesic, antiviral, anti-inflammatory, and neuroleptic drugs are often used to treat HZ.2 And vaccination strategies for HZ remain inconsistent.6 Notably, the application of these therapies can be limited. For instance, some tricyclic antidepressants (eg, amitriptyline) can bring serious adverse events in older adults.7 Additionally, some HZ patients fail to respond to the aforementioned drugs. Moreover, despite timely use of the aforementioned therapies, quite a few HZ patients can still develop PHN. It is worth noting that a Cochrane review concludes that acyclovir does not significantly reduce the incidence of PHN and evidence on other antiviral treatments remains insufficient.8 Faced with such a dilemma, clinicians differ in their approaches to the management of HZ and waver in their recommendations of these therapies to HZ patients.2 In this situation, it is critical to look for other optional non-pharmacological therapies to treat HZ.
As an important component of traditional Chinese medicine (TCM), acupuncture has been used for treating HZ for a long history. Several systematic reviews and meta-analyses9,10 have supported the efficacy of acupuncture on HZ. Intradermal acupuncture (IDA) is a special modality of acupuncture, which is very easy to operate by practitioners. In contrast to other popular modalities of acupuncture, IDA may prolong the sustained impact of acupuncture by retaining the needles in the patient’s body for considerably longer durations (varying from several hours to days), so it can reduce the number of patient visits and reduce medical costs.11 Additionally, IDA is particularly ideal for patients who are afraid of traditional acupuncture since it involves no or mild pain when inserting the intradermal needle. Therefore, concerning the treatment of multiple pain conditions,12–14 especially persistent pain, IDA may have some benefits over traditional acupuncture that typically employs long filiform needles. Although some trials are previously conducted to assess the effect of IDA in acute HZ, the vast majority of previous clinical trials are limited by notable methodological concerns, such as small sample sizes, inappropriate outcome measures, non-RCT designs, and absence of placebo-controlled groups.15 To the best of our knowledge, there has been a paucity of rigorously designed randomized clinical trials (RCTs) that aim to evaluate the therapeutic effect of IDA as adjunctive therapy for acute HZ.
In addition, there has been a consensus that timely treatment of HZ and active pain management is warranted in the acute stage of HZ.7,16,17 Early efforts to alleviate acute pain for acute HZ may be vital for reducing the risk of developing PHN.7 Therefore, it is of significance to find an aided assessment tool that can accurately predict the occurrence of PHN, thereby guiding treatment strategies in the acute stage of HZ to reduce the incidence of PHN.
Infrared thermography (IRT) has been regarded as a diagnostic tool for abnormal functioning of the sensory and sympathetic nervous systems.18 Previous studies19–21 have utilized IRT to detect the thermal asymmetry in acute HZ patients and to identify whether IRT can be used for the early prediction of PHN. However, the respective results are conflicting. Some studies found that higher temperature differences between the affected area and the contralateral control area are present in the acute stage of HZ and they are positively associated with the occurrence of PHN, thereby supporting IRT as a tool for predicting PHN.20,21 On the contrary, other studies concluded that irrespective of thermal findings, IRT could not be used as a predictive tool for the development of PHN.19 Given that it remains controversial whether IRT is accurate as a predictive tool for PHN, further investigations are warranted. Moreover, owing to a lack of objective assessment tools for subjective pain in HZ patients, the vast majority of previous trials used subjective assessment tools, such as the visual analog scale (VAS) and some pain-related questionnaires, as the primary outcome to measure the pain intensity in HZ patients. However, these subjective tools can be influenced by multiple factors, especially psychological states. Thus, we will also explore whether IRT can be an objective assessment tool for subjective pain for acute HZ patients in this study. If so, the evaluation of the efficacy of acupuncture for acute HZ will be more objective and quantitative.
Taken together, the objectives of this trial are to 1) Investigate whether IDA is effective and safe as adjunctive therapy for acute HZ; 2) Investigate the feasibility of IRT for early prediction of PHN and as an objective tool to aid in subjective pain assessment in acute HZ patients.
Methods and Design
Study Design
This study is designed as a randomized, parallel-group, sham-controlled, and patient-assessor-blinded trial. The intended the trial period is from July 2022 to December 2024. Participants whose eligibility has been verified will be randomly assigned in a 1:1 ratio to the IDA group and the sham IDA group. We refer to The Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT)22 (as shown in Supplementary File) and the Revised Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA)23 to report the presented RCT.
Study Procedure
The duration of this study will include 1-month treatment and 3-month follow-ups. The flowchart of this RCT is shown in Figure 1. The enrollment, intervention, and outcome assessment schedules are listed in detail in Table 1.
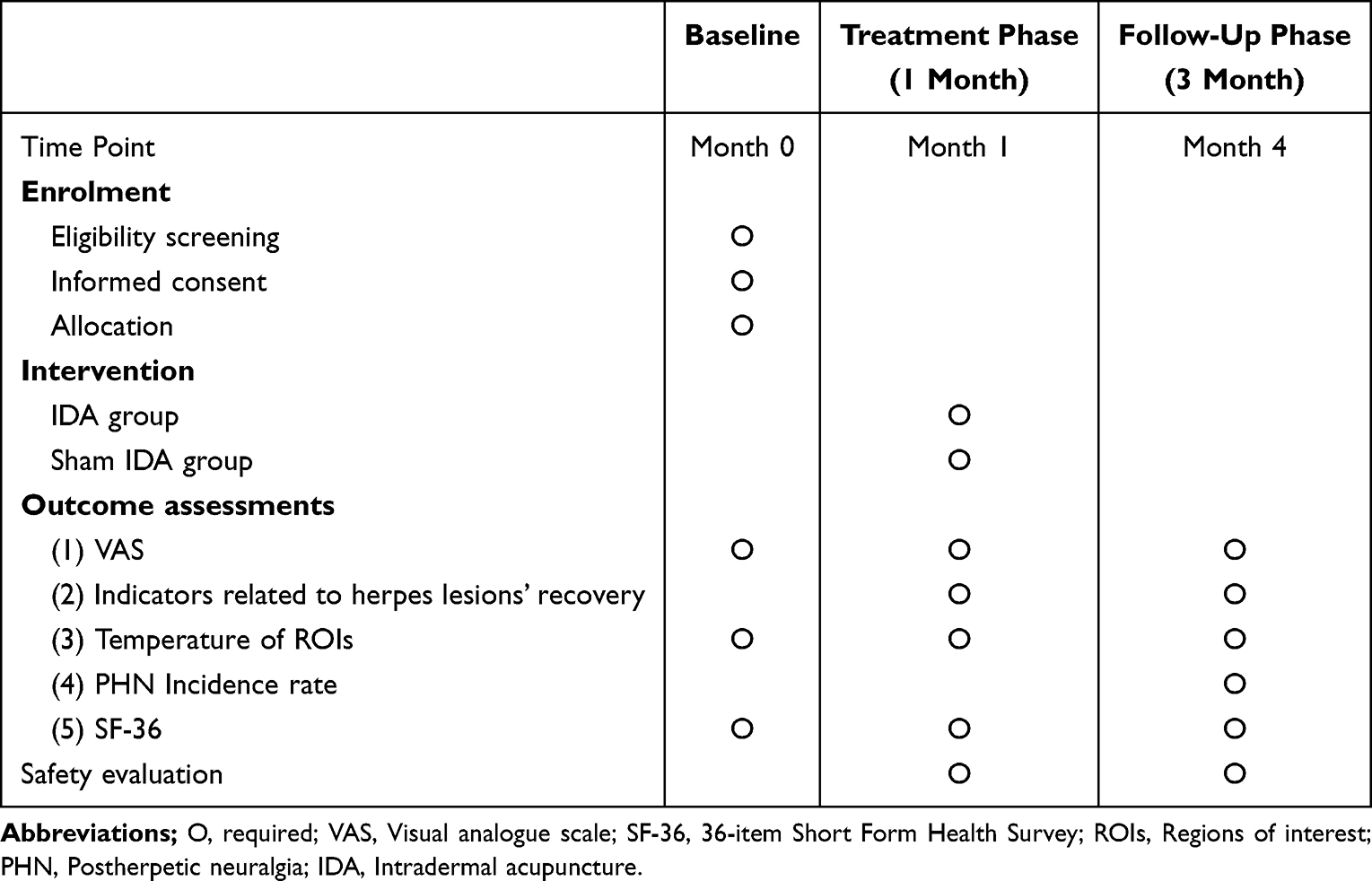 |
Table 1 Schedule of Enrolment, Interventions and Outcome Assessments |
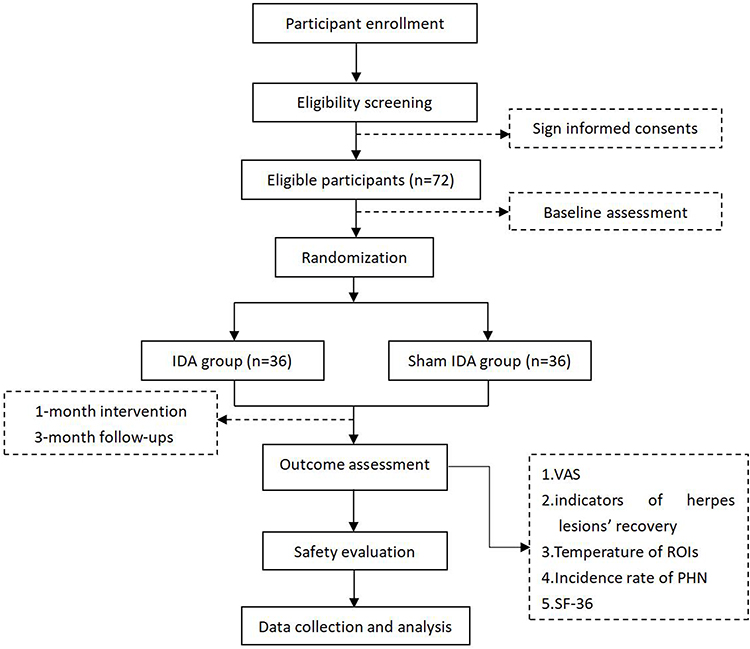 |
Figure 1 Flow chart of the study process. Abbreviations: IDA, intradermal acupuncture; PHN, postherpetic neuralgia; SF-36, Short Form 36 Health Survey; ROIs, regions of interest; VAS, visual analog scale. |
Participant Recruitment and Screening
Participants will be mainly recruited from the Third Affiliated Hospital of Zhejiang Chinese Medical University. Outpatients or inpatients from the department of neurology, department of dermatology, and department of acupuncture will be enrolled. In addition, advertisements in local newspapers and social network platforms, as well as posters in communities, will be utilized to broadcast study information to supplement participant enrollment.
Potentially eligible participants who have an interest in joining the trial will be invited to complete a screening test and eligibility assessment. Specialists from the department of dermatology and the department of neurology will confirm participant eligibility strictly in accordance with the inclusion and exclusion criteria outlined as follows. In addition, researchers who are in charge of participant recruitment will fully explain the study and obtain signed informed consent forms from each participant before including them in this trial.
Eligibility Criteria
Physicians with expertise will diagnose HZ according to the patient’s medical history, symptoms, the appearance of distinctive lesions, and a unilateral dermatomal distribution. The eligibility criteria are listed as follows.
Inclusion Criteria
- The subjects have been diagnosed with herpes zoster;
- It is in the acute stage of herpes zoster, with a duration ≤2 weeks;
- 18≤Age≤80 years, regardless of gender;
- Significant pain assessed by the VAS score ≥4;
- Subjects have no other diseases that can cause obvious change in skin temperature;
- Subjects understand the study procedure and are willing to sign informed consent forms.
Exclusion Criteria
- Subjects have a specific type of herpes zoster, such as disseminated herpes zoster, or HZ occurs in regions that are not suitable for IDA, such as the face.
- Subjects who have received standard pharmacological treatments (eg, analgesics, antivirals, and neurotrophic drugs) or acupuncture in the past 2 weeks;
- Subjects who are pregnant or lactating;
- Subjects are unsuitable for IDA because they have a scar constitution or have serious disorders of the heart, liver, kidney, and hematological system that cause bleeding propensity;
- Subjects who are participating in other trials;
- Subjects who have severe cognitive impairment and do not have the ability to follow the trial protocol.
Participant Withdrawal Criteria
- At the discretion of the researchers due to the following situations: 1) Researchers will withdraw participants for their benefits and safety if they experience serious adverse events throughout the trial; 2) Researchers will withdraw participants who experience complications or deteriorating circumstances if they require the immediate implementation of emergency measures; 3) Researchers will withdraw participants who have poor compliance and fail to strictly follow the trial protocol;
- At the request of the participants themselves: participants are free to quit the trial at any time and for any reasons.
Randomization and Allocation Concealment
Based on a table of random numbers produced by the Statistical Product and Service Solutions program (SPSS version 25.0), eligible participants will be randomly divided to the IDA and sham IDA groups in a ratio of 1:1. In order to guarantee allocation concealment, a specially appointed coordinator who is not engaged in any other trial processes will create and maintain a randomly generated sequence. Only this specifically authorized coordinator will be accessible to the randomization list, thereby ensuring that the randomization sequence is concealed from all other researchers (eg, researchers who confirm participant eligibility, acupuncture manipulators, and outcome assessors). Sequentially numbered, opaque, sealed envelopes will be used to conceal group allocation information. Researchers who confirm the eligibility and consent of participants must phone the specifically assigned coordinator to get the corresponding random number and group allocation information of every included participant.
Blinding Method
Due to the unique nature of IDA operations, it is impractical to blind acupuncturists. Patients will be blinded to the group allocation. After enrolment, all patients will be informed by researchers that they will receive one of two effective IDA interventions for zoster-associated pain. To ensure patient blinding, the following measures will be implemented. First, the appearance of the pseudo-intradermal needles used in the sham IDA group will be identical to those in the IDA group. Second, sham IDA will be applied to the same acupoints as in the IDA group. Third, participants in the sham IDA group will be treated in a separate room to prevent communication with subjects in the IDA group. Furthermore, a survey utilizing a questionnaire will be conducted to verify the success of patient blinding. Specifically, participants will be instructed to promptly select one of three options on the questionnaire at the end of the treatment course: 1) Real treatment; 2) Sham treatment; 3) I do not know. And then the blinding index will be developed to verify the success of the patient blinding.
In addition, separated researchers will undertake the treatment, outcome measurement, and statistical analysis independently. Assessors who are not aware of the allocation information will undertake the outcome assessment. Besides, statistical analyses will be carried out by external statisticians, thereby blinding them to the information of group allocation.
Interventions
Participants in both groups will receive standard pharmacological treatments for acute HZ, which comprise the following analgesic, antiviral, and neurotrophic drugs: 1) Gabapentine with individualized dosage: based on the recommended scheme by the manufacturer, the initial dose of 300 mg/d (taken in one time) is gradually increased to 900 mg/d (taken in 3 times) dependent on patients’ individual need, but the maximal dose should not exceed 1800 mg/d (taken in 3 times). Once symptoms have been relieved for at least one week, the daily amount of gabapentine dosage can be gradually reduced. 2) Vaxilovir: the dose is 0.3 g/time, 2 times a day; 3) Mecobalamin: 0.5 mg/time, 3 times a day.
In addition to standard pharmacotherapy, the two groups will receive IDA or sham IDA as adjunctive interventions, respectively. The schematic diagram of IDA and sham IDA is shown in Figure 2a and b, respectively. After needle insertion, intradermal needles will be retained in acupoints for 48 hours, with a 1-day interval between each session. Ten consecutive sessions will be delivered during a full treatment course that lasts for one month.
 |
Figure 2 The schematic diagram of intradermal acupuncture and sham intradermal acupuncture. (a) Intradermal acupuncture; (b) Sham intradermal acupuncture. |
IDA Group
Participants will receive IDA in this group. All IDA operations will be performed by acupuncturists who have a qualification certificate and independently undertake acupuncture clinical treatment for more than 5 years. The treatment strategies of IDA are developed dependent on a consensus process with experienced acupuncture experts. In addition, all IDA operations are strictly in accordance with “Standardized Manipulations of Acupuncture and Moxibustion-Part 8: Intradermal Needle” (GB/T 21709.8-2008)24 that belongs to the National Standard of the People’s Republic of China.
Before the operation, the patient will be instructed to take a comfortable position according to the location of HZ, ensuring all HZ sites are fully exposed. After routine sterilization of the operator’s hands and the patient’s skin surrounding the selected acupoints, the intradermal needle (0.2 mm in diameter and 1.5 mm in length, Seirin Pyonex®; manufactured by Seirin Corporation, Shizuoka, Japan) will be inserted in every selected acupoint and retained in sites for 48 hours. Points around the HZ sites (about 1 cm peripherally) are selected for IDA encircled needling. The distance between each acupoint is about 1–2 cm. Meanwhile, IDA is also performed in Ashi acupoints (ie, the worst pain points) in the distribution area of HZ. The operator will rip the adhesive tape off the intradermal needles and put them on the chosen acupoints. Then, depending on the patient’s tolerance, they will apply pressure perpendicularly over the chosen acupoints with the intradermal needles. The total number of intradermal needles for each IDA treatment session is directly proportional to the size of HZ lesion areas. In order to boost stimulation for treatment enhancement, patients will also be asked to press the intradermal needles 4 times (with an interval of at least 3 hours) every 24 hours throughout the needle retention period, with each time lasting around 30 seconds. It is worth noting that the retention of intradermal needles will not impact patients’ daily lives because the intradermal needles are extremely short and cause virtually no subjective sensation during needle retention.
Sham IDA Group
Sham IDA will be applied in the same acupoints as the IDA group using pseudo-intradermal needling (ie, with no intradermal needles under the adhesive tape) in reference to similar studies.25,26 Without any intradermal needles under the micropore medical tape (as shown in Figure 2b), the tape will merely be adhered to the surface of the same acupoints. In order to improve patient blinding, the size of the micropore medical tape, as well as the appearance, is the same as that in the IDA group. In addition, in order to prevent interaction with participants in the real IDA group, the sham IDA group’s participants will receive their intervention in a separate room.
Infrared Thermography Assessment
An experiment room is set up for IRT assessment, with the room temperature controlled at 26°C and the humidity controlled at 40–50%. The experiment room is free from direct sunlight and obvious air convection. Meanwhile, tea, alcohol, coffee, and smoking are prohibited within one day before participants receive an infrared thermography assessment. Participants are also required to avoid exercise and food one hour before infrared thermography.
IRT Procedures
After entering the experiment room, the patient is instructed to take off clothes to fully expose HZ lesion sites, ensuring rest for 30 min to adapt to the room environment. An infrared thermal imager (NEC R450, manufactured by NEC AVIO, Japan) will be used for assessment. The height and angle of the camera of the infrared thermal imager will be modified to ensure all regions of interest (ROIs) can be seen on the camera screen. The ROIs include the HZ pain area of the affected site and the contralateral control area of the unaffected side. Once the size of ROIs is moderate on the camera screen, infrared thermograms will be taken and stored by the infrared thermal imager. Subsequently, all infrared thermograms will be imported to the computer and the temperature of ROIs will be extracted and analyzed using the software InfRec Analyzer NS9500 (manufactured by NEC AVIO, Japan).
Outcome Measures
Primary Outcomes
Pain Intensity
Pain intensity is evaluated by the VAS, which is the most commonly used assessment tool for subjective symptoms, especially pain intensity.27,28 The intensity of pain will be rated depending on a specific point of the 0–10 scale. In detail, 0 point indicates no pain; 0–3 points can be interpreted as slight and bearable pain; 4–6 points can be interpreted as pain that affects sleep, but it is still tolerable; 7–10 points can be interpreted as intense and unbearable pain that affects sleep or other activities.
Assessment points: at baseline, at 1 month after intervention, and at 3-month follow-up.
Secondary Outcomes
Indicators Related to Herpes Lesions’ Recovery
Using the initial appearance of HZ as the starting time, the indicators related to herpes lesions’ recovery include (A) stopping time of HZ: the number of days required for HZ to stop increasing; (B) crusting time of HZ: the number of days required for HZ crusting; (C) removal time of HZ scabs: the number of days required for all HZ scabs to be completely shed.
Assessment points: At each patient visit during the 1-month treatment course, during 3-month follow-up.
The Temperature of ROIs
Infrared thermography will be used to assess the temperature of ROIs, as described previously in detail. In reference to previous similar studies,19–21 the ROIs include the HZ pain area of the affected site and the contralateral control area of the unaffected side. The temperature (including the maximum, and average temperature) of ROIs will be extracted and calculated by IRT and the software InfRec Analyzer NS9500. Moreover, the temperature difference (ΔT) between the HZ pain area of the affected side and the contralateral control area of the unaffected side will also be calculated by infrared thermography.
Assessment points: at baseline, at 1 month after intervention, and at 3-month follow-up.
Incidence of PHN
At the 3-month follow-up after the final IDA treatment, specialized researchers from the department of dermatology and the department of neurology who are in charge of participant follow-ups will contact each participant by telephone. In case of persisting pain in the respective area, it will be classified as PHN. The percentage of participants who suffer from PHN in each group will be recorded to evaluate the incidence of PHN.
Assessment points: at 3-month follow-up.
Quality of Life
Quality of life will be evaluated by the 36-item Short Form Health Survey (SF-36). The SF-36 is a highly recognized self-report tool to evaluate the quality of life, which consists of 8 health-related dimensions (ie, physical function, bodily pain, general health, vitality, mental health, social function, and role of physical and emotional health) in the conduct of daily activities. The reliability and validity of SF-36 for evaluating the quality of life have been intensively confirmed by previous studies29 and it is also frequently used as an important outcome in trials involving acute HZ.30
Assessment points: at baseline, at 1 month after intervention, and at 3-month follow-up.
Safety Evaluation
Safety evaluation will be determined by the incidence of adverse events associated with treatment in each group, which will be recorded timely during the treatment course and the follow-up period. Adverse events will be classified as unrelated, possibly related, or related to treatment.
Adverse events related to IDA mainly include intolerable needle pain (VAS ≥ 8 points), local hematoma, local infections, and other uncomfortable feelings after acupuncture (eg, nausea, vomiting, palpitation, dizziness, headache, and insomnia lasting for a long time). Adverse events related to Western medication mainly include blurred or double vision, weakness, drowsiness, vomiting, nausea, and so on. At each patient visit, each participant will be inquired whether any of the above-mentioned adverse events have occurred. If so, symptoms, average degree, and duration of related adverse events will be recorded timely.
In addition, the severity of adverse events will be quantified as mild, moderate, or severe. If any severe adverse events occur, the trial will be discontinued promptly and rescue measures will be taken promptly. Meanwhile, severe events will be submitted to the Institutional Ethical Review Board of the Third Affiliated Hospital of Zhejiang Chinese Medical University as soon as possible.
Sample Size Estimation
In a 1:1 ratio, eligible participants will be separated into two groups. The required number of participants is calculated using the PASS V.16.0 software (NCSS, Kaysville, Utah, USA). Owing to a lack of available data obtained by previous relevant RCTs, we have to refer to the results of our pilot study to calculate the sample size. In detail, using the VAS score as the primary outcome, it is estimated that the difference value of the mean VAS score between the two groups at the end of 1-month treatment course will be 1.95, with a combined standard deviation of 1.14. With a statistical power of 0.80 to reject a null effect at the 0.05 level of significance, each group requires 31 subjects. Furthermore, assuming a dropout rate of 15%, each group needs 36 participants. Thus, a total of 72 subjects are required as the final sample size.
Statistical Analysis Plan
SPSS 25.0 software (IBM Corp.) will be used for statistical analysis, and all statistical tests will be taken as two-side tests, with a significance level of P < 0.05. Continuous variables in the normal distribution will be expressed as means ± standard deviations, while continuous variables in the non-normal distribution will be reported as median with 25 to 75% quartiles (interquartile range, IQR). In addition, categorical variables will be expressed as frequency rates and percentages in each category. For continuous variables in normal distribution, repeated-measures analysis of variance (repeated measures ANOVA) will be used to perform within-group and between-group comparisons by assessing changes in continuous variables before and after intervention at different time points, while non-parametric tests will be adopted to conduct within-group and between-group comparison for continuous variables in non-normal distribution. In cases of potential baseline imbalances in specific characteristics (eg, individualized dose and timing of medication) between groups, analysis of covariance (ANCOVA) will be used to estimate treatment effects. Moreover, when available, subgroup analyses or logistic regression analysis based on specific baseline characteristics (eg, varying durations of HZ, age stratifications, gender distributions) will be conducted to explore the potential effects of these factors on subsequent clinical outcomes.
The correlation analysis between quantitative data will be carried out by Pearson correlation analysis. The accuracy of IRT for early prediction of PHN will be analyzed using the receiver operating characteristic (ROC) curve analysis. In detail, the temperature difference (ΔT) between the HZ pain area of the affected side and the corresponding control area of the unaffected side before treatment and at the end of 1-month treatment course will be used as the test variable, and the incidence of PHN at the 3-month follow-up will be selected as the state variable. The ROC curve analysis will be performed to calculate the area under the curve, thereby exploring the prediction threshold of ΔT, the false-negative rate, and the false-positive rate of IRT for predicting PHN. The validity of infrared thermography will be determined according to the area under the curve (AUC). The interpretation of AUC values will be in accordance with the following guidelines: low (0.5 ≤AUC < 0.7), moderate (0.7 ≤AUC < 0.9), or high (0.9 ≤AUC ≤1) diagnostic accuracy.
Ethical Approval and Trial Registration
The trial will be carried out strictly following the Declaration of Helsinki. Before the conduct of this trial, the Institutional Ethical Review Board of the Third Affiliated Hospital of Zhejiang Chinese Medical University has evaluated the ethical considerations and the ethical approval document is obtained (approval number: ZSLL-KY-2022-031-01). Before enrollment in this trial, participants will be fully informed of the procedures, benefits, and potential risks of this trial. Participants have the full right to determine whether they want to participate in the trial. Informed consent forms should be signed by participants before taking part in this trial.
Meanwhile, to ensure transparency and reduce performance bias of the trial, the protocol has been prospectively registered at the Clinicaltrials registry with the registration number NCT05348382. All amendments to the study protocol will be reported timely before the enrollment of the first participant.
Quality Control
First, during the intervention period, all IDA operations will be carried out by two experienced acupuncturists who have a qualification certificate and have independently performed acupuncture clinical treatment for more than 5 years. They will undergo rigorous training on IDA performance procedures according to the treatment regimen and the National Standard of the People’s Republic of China entitled “Standardized Manipulations of Acupuncture and Moxibustion-Part 8: Intradermal Needle” (GB/T 21709.8-2008).24 Thus, the standardization and consistency of IDA operations are expected for this trial. Furthermore, outcome assessors will receive intensive training to ensure all outcome assessments are conducted in a consistent and relatively unbiased manner.
Second, throughout the trial, independent researchers will collect all data in the case report forms (CRFs) and double-enter it into the electronic data capture system in a timely manner. Dropouts or withdrawals from the trial will be noted by providing specific reasons. We will employ a data safety monitoring committee. The committee’s staff will be in charge of data monitoring and will have the authority to release data that has been blinded. They will also check for the consistency between the raw and recorded data. In addition, every 3 months, the principal investigator and other primary members of the research team will meet to address concerns that have occurred during the trial and to debate the best solutions.
Evaluation of Acceptability of IDA to Patients
The average number of completed IDA and sham IDA treatments in both groups will be recorded to evaluate patient acceptability.
Adherence Improvement
In order to improve participant adherence and reduce the dropout rate, we will develop two appealing approaches as follows: 1) All treatment costs (including IDA and pharmacotherapy) and IRT examination fees during the trial course are free of charge for the included participants; 2) If participants develop PHN at 3-month follow-ups, they can choose to receive 10 additional free acupuncture sessions. In addition, before patient inclusion, researchers will offer them a detailed explanation of the study, including the trial’s aims, intervention procedures, patient visit schedules, outcome measurements, patient benefits, and so on. This will build the foundations for better adherence.
Confidentiality
To protect the participants’ confidentiality and anonymity, all researchers will be required to sign a confidentiality agreement before the performance of this trial. CRFs and medical records of the participants will be retained in the hospital as needed and will be retrieved when necessary. Personal information and medical history of the patient will not be made public. Other institutions or persons will not have access to the personal information of participants. Besides, data will be anonymized before publication to prevent the identification of individuals.
Discussion
As a non-pharmaceutical therapeutic approach and a common type of the acupuncture therapy, IDA has been widely used for various kinds of pain conditions.31 In recent years, the number of trials investigating the efficacy of IDA for acute HZ has been increasing. Modern research has also found that the analgesic effect of IDA may be achieved by improving microcirculation, stimulating the receptors of subcutaneous tissues, and producing a neuro-immuno-endocrine response to release active substances that bond to the corresponding receptors on the surface of sensory afferent nerves.32 The skin-brain axis is also the core involved in the relevant mechanisms.32 Nonetheless, the vast majority of previous trials in this field are limited by methodological concerns.31 More trials with credible methodology are urgently needed. Therefore, we conduct this randomized, sham-controlled, and patient-assessor-blinded trial to ascertain whether IDA enhance the therapeutic effect of pharmacotherapy in reducing pain intensity, improving quality of life, shortening the disease duration, and reducing the incidence of PHN in patients with acute HZ. At the time of manuscript submission, the trial is still ongoing and at the stage of recruiting participants.
Several major strengths and highlights concerning the design of this trial should be addressed. First, regarding the selection from various modalities of acupuncture, IDA is adopted as an adjunctive therapy for acute HZ in this trial. Compared with other modalities of acupuncture therapy, IDA has the advantage of a much longer retention duration of needles, thereby exerting more sustained stimulation effects of acupuncture and additionally reducing personnel and time expenditures of patients.11 At the same time, because IDA is characterized by mild or even no pain during the insertion of intradermal needles, this patient-friendly acupuncture modality is more welcomed by patients with pain conditions who fear other modalities of acupuncture. Nonetheless, it remains inconclusive whether the analgesic effect of IDA is equivalent to conventional acupuncture for treating pain conditions such as acute HZ. Therefore, the primary objective of this trial is to investigate whether IDA can enhance the therapeutic effectiveness of pharmacotherapy for acute HZ with acceptable safety profile. The subsequent study results will determine whether IDA can be recommended as a supplemental non-pharmacological therapy for acute HZ.
Second, to the best of our knowledge, compared with previous trials concerning acupuncture for HZ, this is the first acupuncture-related trial to adopt IRT as an outcome measurement. IRT is a noninvasive assessment tool that aids in the diagnosis of multiple diseases.33 Some studies found that patients diagnosed with acute HZ can probably exhibit IRT-assessed temperature asymmetry due to the unilateral distribution of HZ lesions.21 Moreover, IRT might have the potential as a forecasting tool of PHN. Nevertheless, previous studies have conflicting results regarding the accuracy of IRT for early prediction of PHN. For instance, Ko et al20 utilized IRT to assess the temperature difference between the affected and contralateral dermatome in subjects with acute HZ, and their results revealed that as the temperature difference increased, the occurrence of PHN increased significantly (P<0.05). On the contrary, Han et al19 assessed the temperature asymmetry in 110 acute HZ patients using IRT. And they found that the affected side was warmer in 35 patients and cooler in 33 patients than the contralateral side. Meanwhile, the temperature differences were not correlated with the incidence of PHN (P>0.05). The aforementioned conflicting results from three previous studies19–21 are investigated, and possible reasons for these discrepancies are discussed as follows. First, two studies19,20 included patients with HZ located in both the face and other regions (cervical/thoracic/lumbar regions), while another study21 only included patients located in cervical/thoracic/lumbar regions. Second, the definitions for the duration of acute HZ and PHN are quite heterogeneous across studies. Two studies20,21 defined acute HZ as “HZ patients with skin eruptions developing 1–7 days” and PHN as “pain persisting or appearing 30 days after rash onset”, while another study19 defined acute HZ as “<6 months after healing of the skin rash” and PHN as “at least 1 year”. To overcome limitations in previous studies,19–21 our study adopts more rational definitions for the duration of acute HZ and PHN. Additionally, we will exclude patients with HZ located in the face. Moreover, compared to non-controlled previous studies,19–21 our research is designed as a randomized, sham-controlled, patient-assessor-blinded trial to further explore the accuracy of IRT for early prediction of PHN. In addition, as an extremely subjective symptom, to date, the assessment of pain has been excessively dependent on subjective tools such as VAS or pain-related questionnaires, which can be influenced by various factors,34 especially patients’ psychological states. There has been a great paucity of objective tools to quantitatively assess pain intensity. Assuming that there is a close correlation between VAS and objectively IRT-assessed temperature, IRT may aid in the objective assessment of pain. Taken together, our study will ascertain the reliability of IRT as a forecasting tool of PHN in the stage of acute HZ and, additionally, as an objective assessment tool of subjective pain in acute HZ patients. Subsequent study results will contribute to the objective and quantitative evaluation of the efficacy of acupuncture for acute HZ, which is of great significance for improving the standard and validity of acupuncture trials.
Third, regarding the placebo control, pseudo-intradermal needling (ie, with no intradermal needles under the adhesive tape to penetrate the skin) is designed to implement sham IDA with references to similar studies.25,26 Without needle penetration, the tape will merely be adhered to the surface of the same acupoints as the IDA group. The size of the adhesive tape, as well as the appearance, is also the same as that in the IDA group. In addition, in order to prevent interaction with participants in the real IDA group, the sham IDA group’s participants will receive their intervention in a separate room. The feasibility of patient blinding is anticipated by such measures.
Limitations
Nevertheless, it is worth noting that our study has several limitations. First, although we refer to similar studies25,26 to design the modality of sham IDA, it remains unclear whether it is completely inert without any specific treatment effect.35 Additionally, the feasibility of patient blinding dependent on this modality of sham IDA needs further confirmation at the end of the trial. Second, owing to the special nature of IDA operation, the blinding of acupuncturists is absent in our trial, to some extent, it may induce performance bias. Third, given that Gabapentine is adopted using the individualized dosage, the between-group difference in the Gabapentine dosage may affect the results of this study. It cannot be totally eliminated that differences in Gabapentin dosage may have a greater impact on therapeutic effect than the difference between IDA and sham IDA. Therefore, at the end of the trial, we will consider an additional statistical analysis of Gabapentin dosage between the two groups to analyze the relationship between Gabapentin dosage and treatment effect in both groups.
Conclusions
The present study protocol presents a randomized, sham-controlled, and patient-assessor-blinded trial that mainly aims to ascertain the efficacy and safety of IDA as adjunctive therapy for acute HZ. In addition, it will explore the feasibility of IRT for early prediction of PHN and as an objective assessment tool of subjective pain for acute HZ patients. Subsequent findings are expected to promote the clinical application of IDA and enrich more effective therapeutic approaches of acute HZ.
Abbreviations
HZ, Herpes zoster; PHN, postherpetic neuralgia; IDA, Intradermal acupuncture; IRT, infrared thermography; RCT, randomized clinical trial; VAS, visual analog scale; SPIRIT, the Standard Protocol Items: Recommendations for Interventional Trials; STRICTA, the Revised Standards for Reporting Interventions in Clinical Trials of Acupuncture; CRFs, case report forms; TCM, traditional Chinese medicine; ROIs, Regions of interest.
Data Sharing Statement
The data presented in this study are available on request from the corresponding author.
Ethics Approval and Consent to Participate
The study will be conducted according to the guidelines of the Declaration of Helsinki and ethics approval (ZSLL-KY-2022-031-01) has been obtained from the Institutional Ethical Review Board of the Third Affiliated Hospital of Zhejiang Chinese Medical University. Before registration, all participants read and sign the written consent form. A copy of the signed consent form is given to the participant.
Funding
The trial is financially funded by the Zhejiang Provincial Administration of Traditional Chinese Medicine (grant No. 2022ZB184), the Zhejiang Province High-Level Health Talent Project (Zhejiang Health Office [2021] No. 40), and the Fifth National Batch of Outstanding Traditional Chinese Medicine Clinical Talent Training Program (National Traditional Chinese Medicine Education Correspondence [2022] No. 1).
Disclosure
The authors declare that they have no competing interests.
References
1. Cohen JI, Solomon CG. Herpes zoster. N Engl J Med. 2013;369(18):255–263. doi:10.1056/NEJMcp1302674
2. Rosamilia LL. Herpes zoster presentation, management, and prevention: a modern case-based review. Am J Clin Dermatol. 2020;21(1):97–107. doi:10.1007/s40257-019-00483-1
3. Yawn BP, Saddier P, Wollan PC, St Sauver JL, Kurland MJ, Sy LS. A population-based study of the incidence and complication rates of herpes zoster before zoster vaccine introduction. Mayo Clin Proc. 2007;82(11):1341–1349. doi:10.4065/82.11.1341
4. Kawai K, Yawn BP, Wollan P, Harpaz R. Increasing incidence of herpes zoster over a 60-year period from a population-based study. Clin Infect Dis. 2016;63(2):221–226. doi:10.1093/cid/ciw296
5. Johnson RW, Rice ASC, Solomon CG. Clinical practice. Postherpetic neuralgia. N Engl J Med. 2014;371(16):1526–1533. doi:10.1056/NEJMcp1403062
6. Silver B, Zhu H. Varicella zoster virus vaccines: potential complications and possible improvements. Virol Sin. 2014;29(5):265–273. doi:10.1007/s12250-014-3516-9
7. Schmader K. Herpes zoster. Ann Intern Med. 2018;169(3):Itc19–Itc31. doi:10.7326/L18-0558
8. Chen N, Li Q, Yang J, Zhou M, Zhou D, He L. Antiviral treatment for preventing postherpetic neuralgia. Cochrane Database Syst Rev. 2014;2:Cd006866.
9. Qi T, Lan H, Zhong C, et al. Systematic review and meta-analysis: the effectiveness and safety of acupuncture in the treatment of herpes zoster. Ann Palliat Med. 2022;11(2):756–765. doi:10.21037/apm-22-109
10. Cui Y, Wang F, Li H, Zhang X, Zhao X, Wang D. Efficacy of acupuncture for herpes zoster: a systematic review and meta-analysis. Complement Med Res. 2021;28(5):463–472. doi:10.1159/000515138
11. Usichenko TI, Henkel BJ, Klausenitz C, et al. Effectiveness of acupuncture for pain control after cesarean delivery: a randomized clinical trial. JAMA Netw Open. 2022;5(2):e220517. doi:10.1001/jamanetworkopen.2022.0517
12. Kotani N, Hashimoto H, Sato Y, et al. Preoperative intradermal acupuncture reduces postoperative pain, nausea and vomiting, analgesic requirement, and sympathoadrenal responses. Anesthesiology. 2001;95(2):349–356. doi:10.1097/00000542-200108000-00015
13. Wang XQ, Xiao L, Duan PB, et al. The feasibility and efficacy of perioperative auricular acupuncture technique via intradermal needle buried for postoperative movement-evoked pain after open radical gastrectomy: a randomized controlled pilot trial. Explore. 2022;18(1):36–43. doi:10.1016/j.explore.2021.09.007
14. Chen L, Li M, Fan L, et al. Optimized acupuncture treatment (acupuncture and intradermal needling) for cervical spondylosis-related neck pain: a multicenter randomized controlled trial. Pain. 2021;162(3):728–739. doi:10.1097/j.pain.0000000000002071
15. Qian G, Zeng J, Lu L, et al. Evaluation of reporting quality in randomised controlled trials of acupuncture for acute herpes zoster by the CONSORT statement and STRICTA guidelines. Evid Based Complement Alternat Med. 2020;2020:4308380. doi:10.1155/2020/4308380
16. Yang HL. Consensus interpretation of herpes zoster in China. Chin J Dermatol. 2018;51(09):699–701. Chinese.
17. Werner RN, Nikkels AF, Marinović B, et al. European consensus-based (S2k) guideline on the management of herpes zoster - guided by the European Dermatology Forum (EDF) in cooperation with the European Academy of Dermatology and Venereology (EADV), part 2: treatment. J Eur Acad Dermatol Venereol. 2017;31(1):20–29. doi:10.1111/jdv.13957
18. Fitzgerald A, Berentson-Shaw J. Thermography as a screening and diagnostic tool: a systematic review. N Z Med J. 2012;125(1351):80–91.
19. Han SS, Jung CH, Lee SC, Jung HJ, Kim YH. Does skin temperature difference as measured by infrared thermography within 6 months of acute herpes zoster infection correlate with pain level? Skin Res Technol. 2010;16(2):198–201. doi:10.1111/j.1600-0846.2009.00417.x
20. Ko EJ, No YA, Park KY, Li K, Seo SJ, Hong CK. The clinical significance of infrared thermography for the prediction of postherpetic neuralgia in acute herpes zoster patients. Skin Res Technol. 2016;22(1):108–114. doi:10.1111/srt.12237
21. Park J, Jang WS, Park KY, et al. Thermography as a predictor of postherpetic neuralgia in acute herpes zoster patients: a preliminary study. Skin Res Technol. 2012;18(1):88–93. doi:10.1111/j.1600-0846.2011.00535.x
22. Chan AW, Tetzlaff JM, Altman DG, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med. 2013;158(3):200–207. doi:10.7326/0003-4819-158-3-201302050-00583
23. MacPherson H, Altman DG, Hammerschlag R, et al. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): extending the CONSORT statement. PLoS Med. 2010;7(6):e1000261. doi:10.1371/journal.pmed.1000261
24. Luo L, Yuan CK, Yin HY, Zeng F, Tang Y, Yu SG. Experience and discussion on the national standard standardized manipulation of acupuncture and moxibustion. Part 8: intradermal needle. Zhongguo Zhen Jiu. 2012;32(2):155–158.
25. Cho SY, Lee DH, Shin HS, et al. The efficacy and safety of acupuncture for cerebral vasospasm after subarachnoid hemorrhage: study protocol for a randomized controlled trial. Trials. 2015;16:68. doi:10.1186/s13063-015-0591-7
26. Luo H, Peng J, Ma Q, et al. Intradermal acupuncture for rheumatoid arthritis: study protocol for a randomised controlled trial. Trials. 2021;22(1):450. doi:10.1186/s13063-021-05416-0
27. Heller GZ, Manuguerra M, Chow R. How to analyze the visual analogue scale: myths, truths and clinical relevance. Scand J Pain. 2016;13:67–75. doi:10.1016/j.sjpain.2016.06.012
28. Chiarotto A, Maxwell LJ, Ostelo RW, Boers M, Tugwell P, Terwee CB. Measurement properties of visual analogue scale, numeric rating scale, and pain severity subscale of the brief pain inventory in patients with low back pain: a systematic review. J Pain. 2019;20(3):245–263. doi:10.1016/j.jpain.2018.07.009
29. Lins L, Carvalho FM. SF-36 total score as a single measure of health-related quality of life: scoping review. SAGE Open Med. 2016;4:2050312116671725. doi:10.1177/2050312116671725
30. Kramer S, Baeumler P, Geber C, et al. Somatosensory profiles in acute herpes zoster and predictors of postherpetic neuralgia. Pain. 2019;160(4):882–894. doi:10.1097/j.pain.0000000000001467
31. Li YQ, Mao YQ, Wang X, Cao X, Yin HY, Yong CK. Hotspots and trends of intradermal needle research: bibliometrics and knowledge map analysis. J Chengdu Univ Chin Med 2022. 45(2):1–5. Chinese.
32. Song SY, Wang XJ, Zhang JB, Gu YY, Hou XF. The origin, development and mechanisms of special acupuncture needle tools for cutaneous region. Zhen Ci Yan Jiu. 2019;44(7):533–537. Chinese. doi:10.13702/j.1000-0607.190015
33. Faust O, Rajendra Acharya U, Ng EYK, Hong TJ, Yu W. Application of infrared thermography in computer aided diagnosis. Infrared Phys Technol. 2014;66:160–175. doi:10.1016/j.infrared.2014.06.001
34. Thong ISK, Jensen MP, Miró J, Tan G. The validity of pain intensity measures: what do the NRS, VAS, VRS, and FPS-R measure? Scand J Pain. 2018;18(1):99–107. doi:10.1515/sjpain-2018-0012
35. Kim K, Lee S. Intradermal acupuncture along with analgesics for pain control in advanced cancer cases: a pilot, randomized, patient-assessor-blinded, controlled trial. Integr Cancer Ther. 2018;17(4):1137–1143. doi:10.1177/1534735418786797
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.