Back to Journals » Journal of Pain Research » Volume 18
Intradiscal Biacuplasty Treating Lumbar Degenerative Disc Disease: Long-Term Results of More Than 100 Patients
Authors Yen TH, Huang CH, Chiu YP, Ji HR, Wang YJ, Wu CY, Guo JH, Chuang TY, Chiu CD ![]()
Received 21 July 2025
Accepted for publication 14 December 2025
Published 24 December 2025 Volume 2025:18 Pages 7065—7076
DOI https://doi.org/10.2147/JPR.S554819
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Andrea Tinnirello
Tzu-Hao Yen,1,2 Ching-Hua Huang,1,2 You-Pen Chiu,3 Hui-Ru Ji,3 Yi-Jyun Wang,1 Chih-Ying Wu,4,5 Jeng-Hung Guo,1– 3 Tien-Yow Chuang,6,7,* Cheng-Di Chiu1– 3,8,*
1Spine Center, China Medical University Hospital, Taichung, Taiwan; 2Department of Neurosurgery, China Medical University Hospital, Taichung, Taiwan; 3Graduate Institute of Biomedical Science, China Medical University, Taichung, Taiwan; 4Department of Neurosurgery, China Medical University Hsinchu Hospital, Hsinchu, Taiwan; 5Graduate Institute of Integrated Medicine, China Medical University, Taichung, Taiwan; 6Department of Physical Medicine and Rehabilitation, China Medical University Hospital, Taichung, Taiwan; 7Department of Physical Medicine and Rehabilitation, Taichung Municipal Geriatric Rehabilitation General Hospital, Taichung, Taiwan; 8School of Medicine, China Medical University, Taichung, Taiwan
*These authors contributed equally to this work
Correspondence: Cheng-Di Chiu, Department of Neurosurgery, China Medical University Hospital, No. 2, Yu-Der Road, North Area, Taichung, R.o.c, 40447, Taiwan, Tel +886-4-22052121# 5034; +886-928829256, Fax +886-4-22053764, Email [email protected]; [email protected]
Purpose: Intradiscal biacuplasty (IDB) has emerged as an effective treatment for lumbar degenerative disc disease (DDD), yet long-term outcomes and decisive prognostic factors remain underexplored. This study enrolled over 100 patients with symptoms for as long as two years to examine clinical efficacy and radiological predictors of surgical success.
Methods: A neurosurgeon conducted a prospective study on 117 patients who underwent IDB at a single medical center. Clinical outcomes were assessed using the Visual Analog Scale (VAS), Oswestry Disability Index (ODI), and modified MacNab criteria at multiple time points up to two years postoperatively. Preoperative MRI scans were evaluated for disc morphology, degeneration severity, and facet joint pathology. Statistical analyses were performed to identify factors associated with clinical outcomes, satisfaction, and the need for secondary interventions.
Results: Significant reductions in VAS and ODI scores were observed from one week postoperatively and sustained over two years (ΔVAS: 95% Cl = 3.81– 6.07, Cohen’s d = 2.27, p < 0.001; ΔODI: 95% Cl = 21.13– 35.53, Cohen’s d = 1.83,). Mean VAS and ODI improvements reached 62% and 63% at six months. Over 76% of patients reported satisfactory outcomes. Disc extrusion was associated with better pain relief; in contrast, advanced facet joint degeneration led to significantly poorer VAS and ODI improvement (VAS: β= − 17.48, 95% Cl = − 31.70–-3.26, p < 0.05; ODI: β= − 21.92, 95% Cl = − 37.25–-6.59, p < 0.01). Moreover, a higher global degeneration score increased the risk of secondary surgery and was associated with patient dissatisfaction.
Conclusion: IDB is an effective and durable treatment for selected patients with lumbar DDD, especially those with disc extrusion and limited facet joint degeneration. These findings underscore the importance of careful patient selection and radiological assessment in optimizing IDB outcomes.
Keywords: disc degenerative disease, facet joint, herniated intervertebral disc, intradiscal biacuplasty
Introduction
Degenerative disc disease (DDD) is a common and clinically significant cause of chronic low back pain (LBP).1 Clinical and imaging studies indicate that DDD accounts for roughly 30–40% of chronic LBP cases.2 As a major subtype of lumbar degenerative spine disease, DDD contributes substantially to the global disease burden, with degenerative lumbar conditions affecting an estimated 266 million individuals annually.3 The prevalence of symptomatic DDD varies across regions and is generally higher in high-income countries, likely reflecting aging populations. Moreover, epidemiological projections suggest that the number of diagnosed DDD cases in the US, EU5, and Japan will continue to rise through 2032.4
Moreover, discogenic pain is also a complex condition that affects patients and presents a diagnostic challenge for physicians. It is typically marked by pain radiating to the buttock and leg, which can occur either on one side or both. Patients may also experience difficulty sitting, and pain is exacerbated when bending back forward, significantly impacting their quality of life.1 The development of discogenic pain is attributed to various factors, including degenerative changes in the intervertebral disc caused by aging or trauma.5 However, it is believed that a wide range of factors, from the initial production of cytokines to the activation of nociceptive signals within the disc, may contribute to the condition.6
Surgical interventions to promote functional regeneration of discogenic LBP are not uncommon. No generally accepted practical internal disc disruption repair strategies have yet been established. The belief that spinal fusion surgery or artificial disc replacement offers only limited improvement arises from the recognition that pain relief depends on more than just anatomical corrections and prolonged operative time.7,8 The complex, imperfect geometry of the surgical site often makes it impossible to eliminate pain signal transmission entirely.9 In principle, however, the destruction of collagens in the annulus leading to the ingrowth of nociceptive neurites into the delaminated regions seems capable of regenerating if given a favorable environment.10 Intradiscal electrothermal therapy (IDET, Smith and Nephews, London, UK) is a minimally invasive procedure designed as a substitute for spinal surgery for treating chronic discogenic pain.11 This technique uses a flexible intradiscal catheter to apply heat to the disc’s annulus, which alters the collagen structure and eradicates nociceptive nerve endings that transmit pain. While this method has shown benefits for a narrow group of carefully chosen patients, its use remains restricted because various technical difficulties hinder its application.12 Besides, IDET was also reported to be without significant benefit over placebo.13
Ongoing medical efforts to enhance or discover new treatments for lumbar DDD have resulted in several routes that clinicians can implement. In recent decades, promising developments have emerged in intradiscal biacuplasty (IDB), developed by Baylis Medical Co. in Montreal, Canada, is one of the thermal annular procedures approved by the United States Food and Drug Administration in 2005, which has proven effective in treating DDD.12 Literature suggests IDB as first tine to provide positive results targeted annular denervation and pain relief for selected patients who fail prolonged conservative care, while exercise, medications, and education remain first‑line and epidural steroid injections mainly offer transient relief for radicular inflammation.14 Systematic review presenting the effectiveness of several thermal annulus procedures, IDB are a higher level of evidence (level I, strong) than IDET (level III, fair) for the treatment of chronic, refractory discogenic pain.15
Our previous research in 2023 found significant reductions in estimated Visual Analog Scale (VAS) and Oswestry Disability Index (ODI) at 1, 3, 6, and 12 months postoperatively. We also noted that pain-killer dosage was significantly decreased at 3 months and 1 year post-operatively. Moreover, the prognosis of IDB was not related to disc height, Pfirrmann grading, or Modic endplate changes.16 Building on these findings, the present study addresses a key knowledge gap: while short-term outcomes of IDB were previously documented, the long-term durability of its effects and the factors influencing suboptimal outcomes remain unclear. To investigate this, our study focused on two main questions: (1) how long the effects of IDB could be sustained, and (2) what radiological morphological differences exist between successful and unsuccessful cases.
As chronic low back pain is a long‑standing condition, short‑term relief may not reflect sustained functional improvement or reduced need for further interventions. Long‑term outcomes therefore inform durability, cost‑effectiveness, and patient counseling, and can reveal delayed adverse events or recurrence that only emerge with extended follow‑up. Most IDB studies report effects only up to six months,17,18 so establishing durability is crucial to determine whether IDB is a definitive treatment or a bridge to other procedures. In addition, comparing radiological differences between responders and non‑responders can identify anatomical predictors of outcome and clarify which pain generators IDB targets. Imaging markers that predict poor response would help avoid ineffective procedures, guide alternative treatments, and improve patient selection and follow‑up strategies.
In this expanded cohort of over 100 patients treated by a single surgeon at a single center, we conducted serial assessments over a two-year follow-up using VAS, ODI, and MacNab scores, as well as recording postoperative rehabilitation use and any subsequent interventions. Notably, we also examined patient-reported satisfaction and sought to identify reasons why a subset of patients experienced suboptimal improvement, providing a more comprehensive understanding of IDB effectiveness, clinical outcomes, and prognostic indicators.
Methods
Study Subject
This clinical study was conducted in accordance with the Declaration of Helsinki and was supervised by the Institutional Review Board of China Medical University Hospital (Approval No. CMUH110-REC2-113). All patients provided written informed consent after understanding the purpose and methods of the study. Patient data were collected from individuals who underwent L-spine IDB surgery at a single medical center in recent years, based on the surgical indications for IDB who suffered from chronic lower back pain for more than 6 months though after receiving conservative treatments such as medication or rehabilitation. All included patients were over 20 years old, maintained more than 50% of disc height preoperatively, and had a positive response to intraoperative challenge discography. Patient recruitment was conducted using a prospective consecutive enrollment approach. To focus on evaluating the efficacy of IDB surgery, we excluded: (1) Patients who had previously undergone spine surgery before IDB, and (2) Patients who underwent other types of spine surgery simultaneously with the IDB procedure. In principle, patients were followed up for a maximum of two years unless they underwent additional spine surgery during the follow-up period or declined further participation, leading to early termination of follow-up (Figure 1). Collected patient data included preoperative MRI imaging, medical records, satisfaction surveys, and questionnaires.
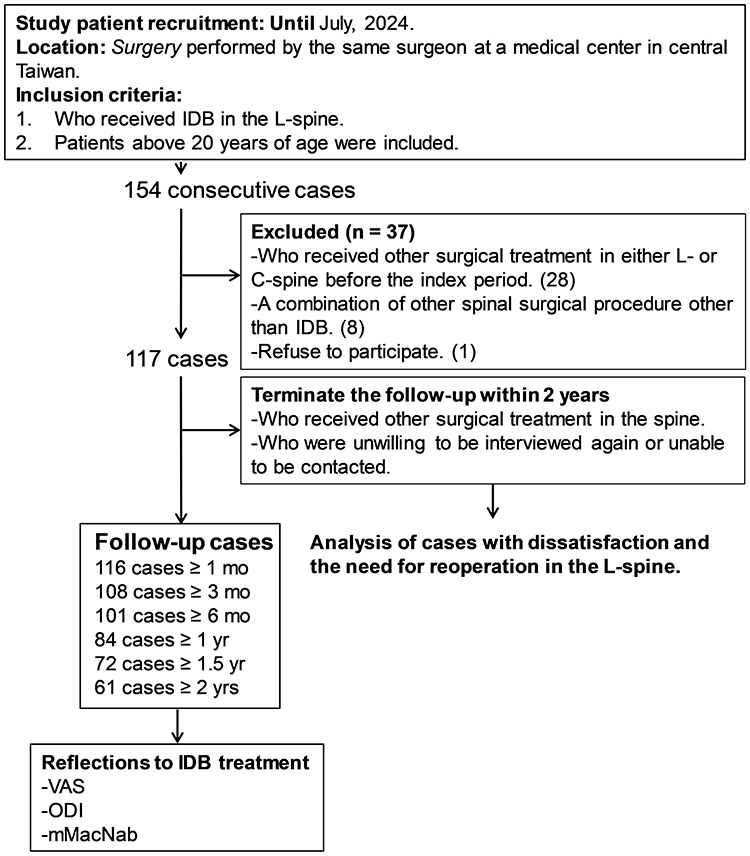 |
Figure 1 Overall flow of the study and patient selection. |
IDB Surgery
The IDB procedure has been previously described in detail.16 Briefly, prophylactic antibiotics were administered 30 minutes before the procedure. Patients were positioned prone with pillow support and ankle pads for comfort. Local anesthesia or intravenous sedation (eg, fentanyl, propofol, or midazolam) was used as needed. Using a posterolateral oblique approach under fluoroscopic guidance, two transdiscal introducers were advanced into the intervertebral discs. Provocative discography identified the pain-generating disc level. Radiofrequency probes were then placed at the annulus-nucleus junction in the posterior third of the disc, confirmed via lateral C-arm fluoroscopy. The disc was gradually heated to 50°C over 15 minutes for therapeutic ablation. All IDB procedures were performed by a single neurosurgeon to ensure consistency and reproducibility.
Questionnaire Survey
The survey included the VAS (0–10), the ODI, and the modified MacNab criteria (mMacNab), assessing pain intensity, quality of life, and surgical satisfaction, respectively. The detailed questionnaire content has been described in previous studies.19–21 Surveys were conducted at multiple time points: preoperatively (pre-op) and postoperatively at 1 week (post-op), 1 month, 3 months, 6 months, 1 year, 1.5 years, and 2 years. Follow-up was discontinued if the patient met the criteria for study termination. The mMacNab criteria were evaluated based on the patient’s latest completed survey. To determine whether patients sought additional treatments following IDB, the questionnaire also included inquiries about their post-IDB status, categorized as requiring no further treatment, undergoing rehabilitation, or having pursued additional surgical intervention. Assessments were conducted via outpatient clinic visits for patients who returned for follow-up and telephone interviews for those who did not attend their scheduled visits. Missing data occurred when patients could not be reached by phone for follow-up visits. In such cases, the data for that time point were left blank and not included in the reported number of cases for follow-up. The primary outcome was 6-month VAS improvement, and associations with imaging parameters were assessed using Cohen’s d over 0.5 to evaluate effective sample sizes.
Radiological Evaluation of Degenerative Disc
The radiological evaluation was conducted by three neurosurgeons. The assessment included preoperative MRI images of all patients who underwent single-level IDB surgery. The evaluated indicators were as follows: Disc height, scored 0–4; High Intensity Zone (HIZ, scored 0–1); Disc character, scored 0–4; Disc degeneration, scored 0–5; End plate Modic changes, scored 0–3; Facet joint grade, scored 0–3; Stenosis, scored 0–3. A higher score for each indicator represents more severe degeneration of the respective phenotype. The analysis involved grouping patients based on surgical satisfaction and whether they sought subsequent surgery, to explore the impact of preoperative degeneration indicators on the success rate of IDB. Additionally, in order to decrease the confusion resulted from the mutual interference of multiple segments results, we analyze the prognostic factors only based on single segment patients. Univariate analysis was used to examine the differences in postoperative VAS improvement between patients with mild and severe degeneration for each indicator. A detailed imaging evaluation table is provided in the Figure S1.
Statistical Analysis
Changes in patient outcomes over time were analyzed using one-way ANOVA, with the Brown-Forsythe test applied for F-testing. Tukey’s multiple comparisons test was used for post-hoc analysis. Two-way ANOVA was conducted to compare differences between two groups over time. For univariate analysis of two-group comparisons based on a single cutoff, multiple unpaired t-tests were performed with Bonferroni-Dunn correction. Chi-square analysis was used to assess the association between different radiological indicators and patient outcomes. A p-value < 0.05 was considered statistically significant. Statistical analyses were performed using GraphPad Prism 10.1.2 (GraphPad Software, Inc., CA, US).
Results
To investigate and analyze the actual effectiveness of IDB surgery, we reviewed the eligibility criteria of 154 patients who underwent IDB surgery for indicated conditions over the past several years. All patients were enrolled consecutively. After screening, 37 patients were excluded, leaving a total of 117 patients included in the study, with more than 170 levels of discs treated with IDB (Figure 1 and Table 1). The patients were followed up for a maximum of two years, with an average follow-up duration of 503.9 ± 272.6 days. The follow-up assessments included pain scores, quality of life, and satisfaction with surgery. Over 100 cases were followed for at least six months.
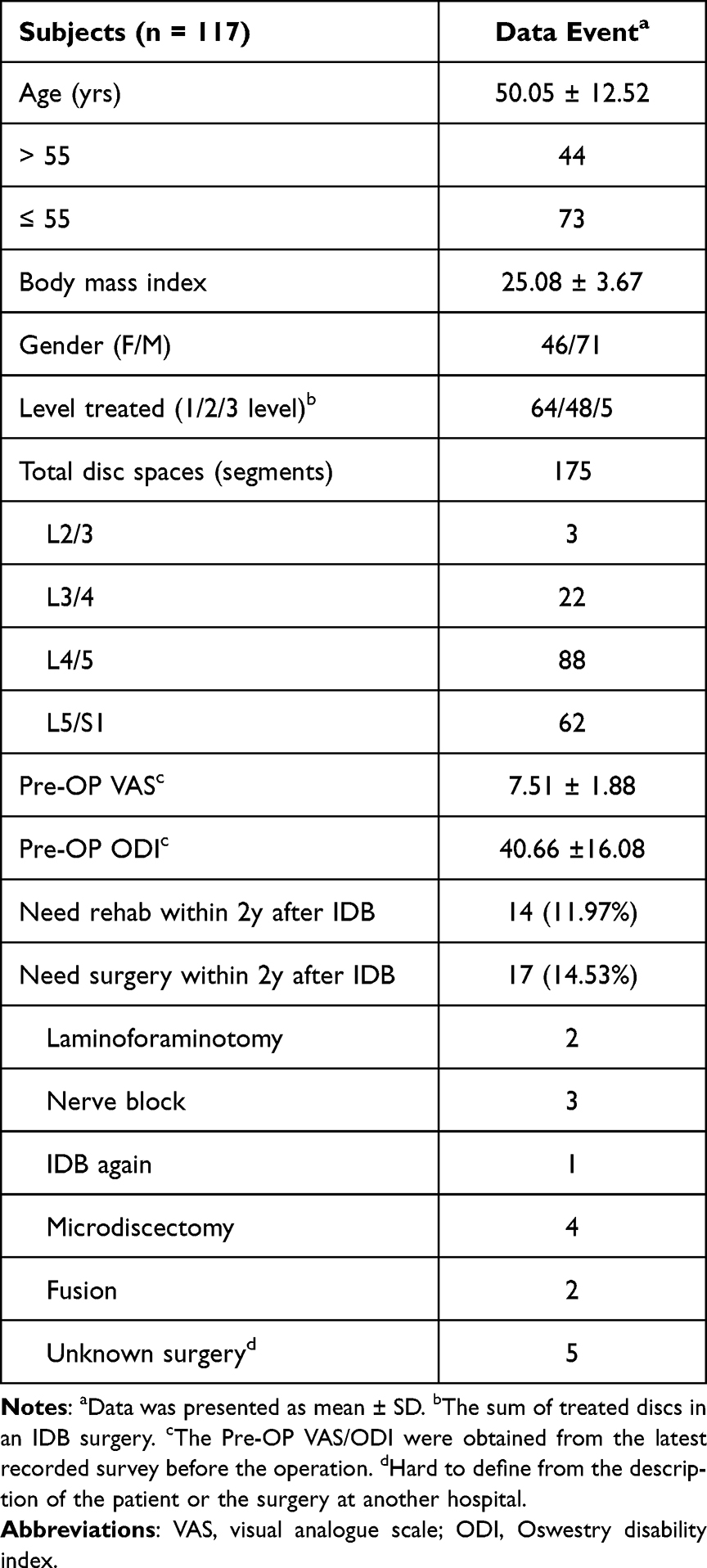 |
Table 1 Demographic Data of the Study Patients |
The results showed a significant improvement in VAS scores one week after surgery (p < 0.001), with further stabilization observed after three months (post vs 3m, 1y, 1.5y, 2y, p < 0.05). Additionally, no significant recurrence of symptoms was observed throughout the two-year follow-up period (Figure 2). A similar trend was observed in ODI scores, with a significant improvement at one week postoperatively (p < 0.001), followed by further improvements from one month onward (post vs 1m–2y, p < 0.001). According to the survey results, the VAS score improved from a preoperative value of 7.51 ± 1.88 to 2.82 ± 2.39 at six months postoperatively, representing an improvement of approximately 62%. Similarly, the ODI score improved from 40.66 ± 16.08% preoperatively to 15.13 ± 13.21% at six months postoperatively, with an improvement rate of approximately 63%. Furthermore, the mMacNab criteria revealed that over 76% of patients subjectively considered the surgery to be effective (Table 2). These findings suggest that IDB surgery is effective in treating DDD and can maintain stable outcomes for at least two years.
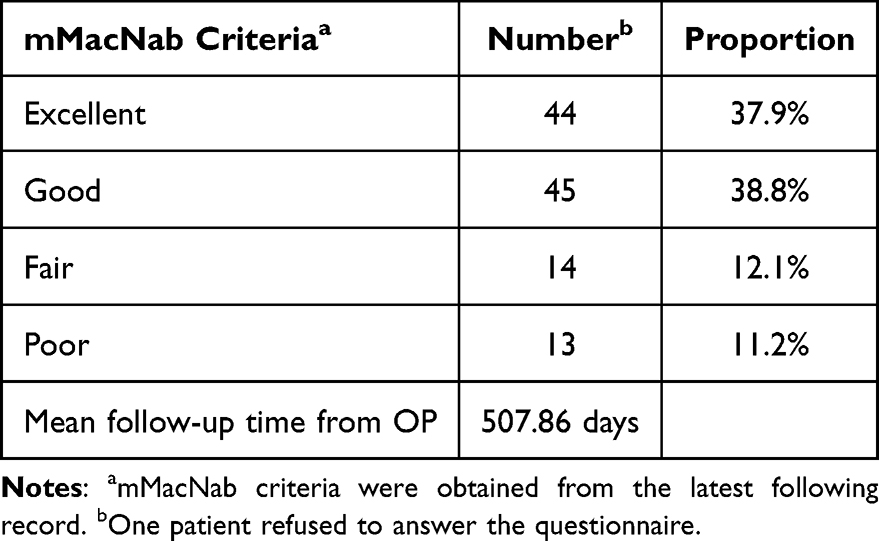 |
Table 2 Modified MacNab Criteria |
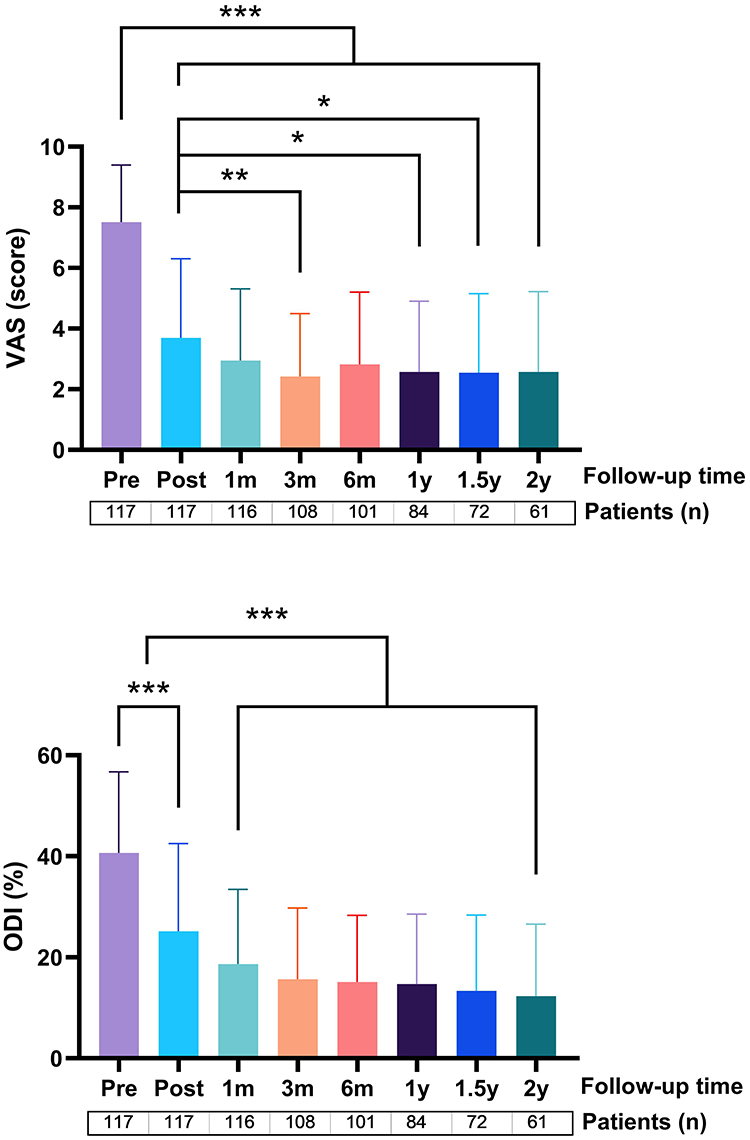 |
Figure 2 Changes in VAS and ODI before and after surgery for all collected cases. The analysis was performed using One-way ANOVA followed by Turkey’s multiple comparison test for inter-group comparisons. The number of participants in each period is listed below the chart. *, **, *** represent p values < 0.05, 0.01, and 0.001, respectively. Abbreviations: ns, not significant; Pre, preoperative; Post, postoperative; M, months; Y, years. |
We observed that approximately 23.3% of patients considered the surgical efficacy to be limited. Additionally, in another questionnaire, 11.97% of patients indicated the necessity of continuing rehabilitation therapy within two years postoperatively, while 14.53% underwent additional lumbar spine surgeries within two years to alleviate their condition (Table 1). These findings suggest that about one-fourth of patients exhibited suboptimal responsiveness to IDB surgery. Theoretically, disc interventional therapy is more suitable for relatively younger populations, as their discs contain sufficient components to undergo ablation. Although all patients who received IDB had more than 50% of disc height preservation, we analyzed whether postoperative outcomes were affected in patients older than 55 years. The results showed no significant differences in VAS and ODI improvements over time between patients older and younger than 55 years (Figure S2).
Based on previous research on IDB, preoperative imaging assessments can help identify factors influencing IDB effectiveness.16 Therefore, we conducted a univariate analysis on MR images of single-level IDB surgery to investigate the impact of disc degeneration on VAS improvement at six months postoperatively (Table 3 and Figures S3–S4). Although statistical significance was not reached, the results showed that patients with preoperative disc herniation classified as extrusion had better outcomes compared to those with protrusion (VAS improvement 65.17% vs 48.42%, p = 0.063). Furthermore, the presence of facet joint issues negatively impacted IDB effectiveness, with VAS improvement being only 49.39% compared to 70.44% in patients without facet joint involvement (p < 0.05). Regarding the likelihood of achieving significant VAS improvement (80%), extrusion was found to be four times more favorable than protrusion (p < 0.05, Chi-square), while the absence of facet joint issues was associated with a fivefold higher probability of improvement compared to cases with facet joint involvement (p < 0.05, Chi-square). Additionally, as the severity of facet joint degeneration increased, VAS improvement rates declined accordingly (p < 0.05, regression).
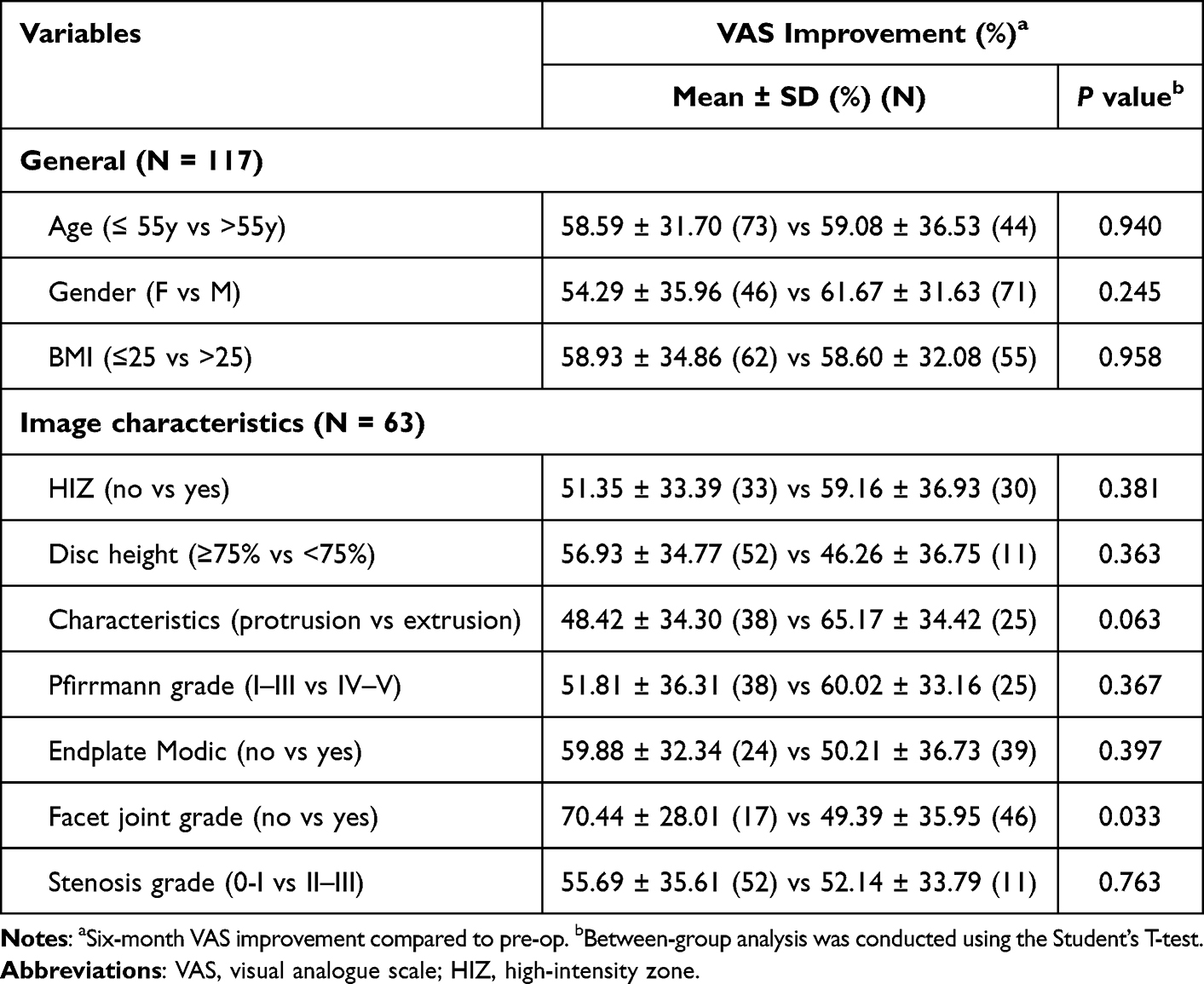 |
Table 3 Univariate Analysis of Pre-op General and MR Assessment |
Subsequently, a multivariate analysis was performed to examine how facet joint grade, compared with other disc MR characteristics, age, and BMI, influenced postoperative outcomes (Table 4). Among these factors, facet joint grade showed a significant negative association with postoperative improvement. Each incremental increase in facet joint grade resulted in a 17.5% decrease in VAS improvement at six months (95% CI: –31.70 to –3.261, p < 0.05) and a 21.9% decrease in ODI improvement (95% CI: –37.25 to –6.592, p < 0.01). Consistent with the previous findings, higher grades of disc herniation progression were positively associated with better postoperative ODI improvement (β = 19.78, 95% CI: 2.450–37.11, p < 0.05). In summary, the analysis of the overall surgical population indicates that IDB is beneficial for treating patients with disc extrusion but is less effective in addressing pain and loss of quality of life caused by facet joint pathology.
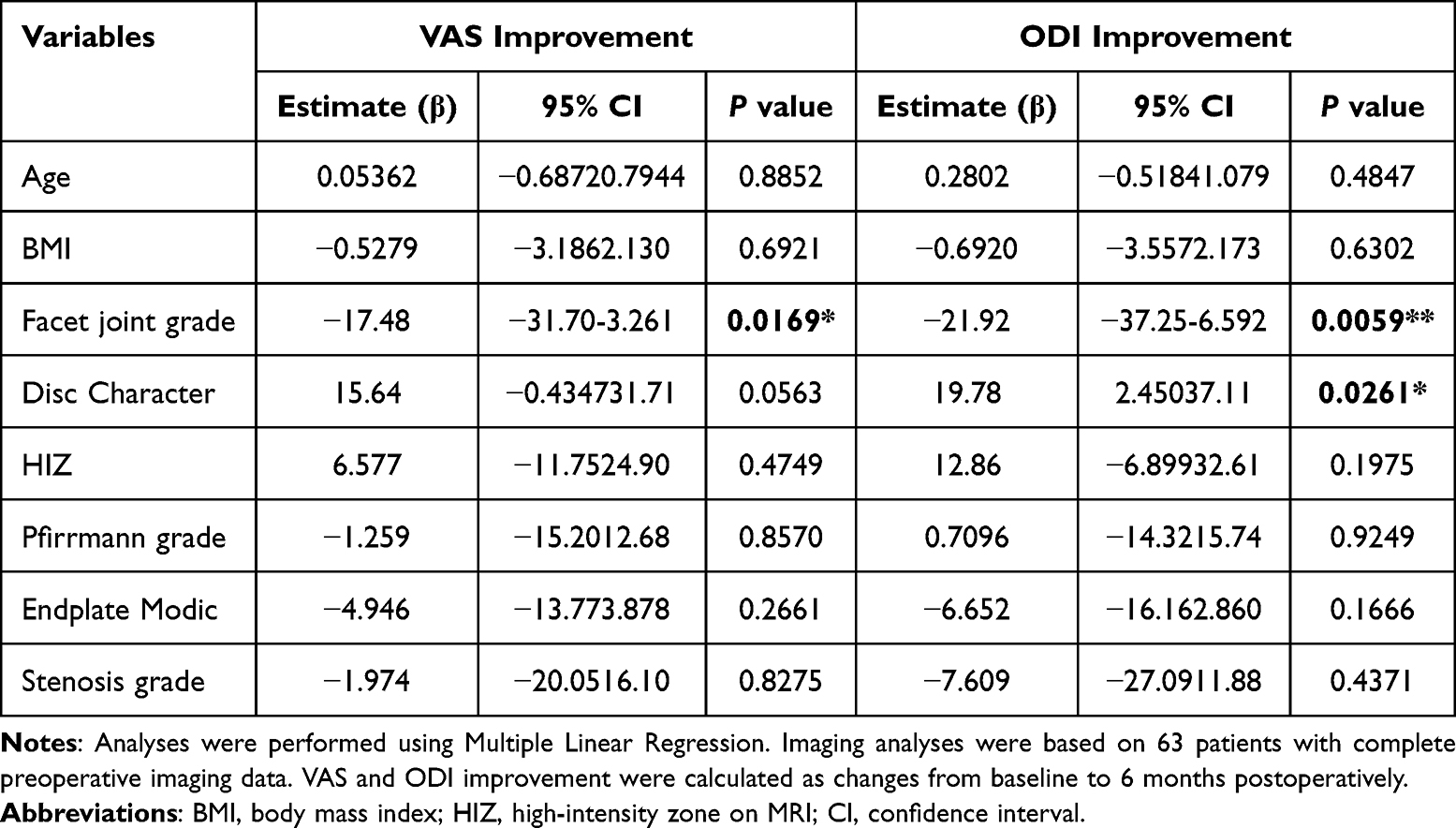 |
Table 4 Multivariate Analysis of Associations Between Preoperative Demographic and Disc Imaging Parameters and Postoperative Outcome Improvement |
Next, we identified cases of single-level surgical failure, including patients with poor postoperative satisfaction (mMacNab C&D, N = 14) and those requiring revision surgery (N = 11). We then analyzed preoperative factors that may have contributed to these outcomes (Figure 3). The results showed that both groups exhibited a higher overall severity of degenerative indicators compared to other patients, with a significant trend (p < 0.05 for mMacNab C&D cases; p < 0.01 for revision surgery cases). These findings suggest that severe overall disc degeneration may be a key factor in poor IDB outcomes, particularly in cases where the procedure was clearly ineffective.
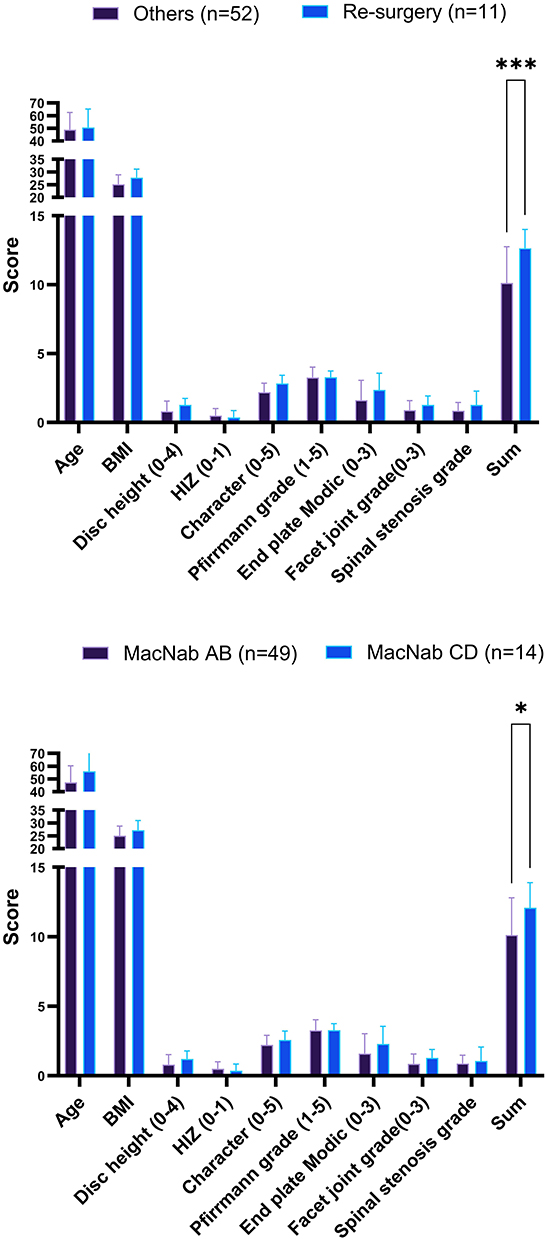 |
Figure 3 Preoperative MRI analysis of cases with surgical failure. Patients with poor surgical outcomes are classified based on those who underwent more surgeries (upper panel) and those with poor postoperative satisfaction (lower panel). The sum is the total score derived from 7 imaging indicators. *, *** represent p values < 0.05 and 0.001, respectively. |
Discussion
The present study represents a significant advancement in IDB research, incorporating the longest follow-up period and the largest population ever documented for this procedure.22,23 Our series of IDB cases has demonstrated remarkable efficacy in improving DDD, achieving up to a 62% and 63% improvement in VAS and ODI scores, respectively. These findings closely align with those reported in other studies.24,25 Furthermore, IDB has achieved a subjective satisfaction rate of 76.7%, with a mean follow-up duration of 508 days. These results underscore IDB’s crucial therapeutic role in managing degenerative intervertebral disc conditions, effectively bridging the gap between conservative treatment and open surgery. Its long-term efficacy in alleviating pain and improving functional outcomes has persisted for up to two years, further reinforcing the durability and reliability of IDB as a viable treatment option for lumbar DDD.
IDB’s effectiveness is believed to be supported by Level I evidence, signifying its strong impact on chronic, refractory discogenic pain.15 Two randomized controlled trials suggest that IDB may be considered a first-line treatment for this condition.17,18 However, in our study, although the mMacNab satisfactory rate (including excellent and good responses) reached 76.7%, 17 patients (14.53%) ultimately underwent open surgery. Among these, 13 patients (including five with unspecified operative methods) proceeded with open surgery, while four underwent repeat interventional therapy. An analysis of our cohort, based on general patient data and preoperative lumbar MRI findings, indicated that the need for a second procedure was associated with higher BMI scores, more severe disc degeneration, and higher total degenerative scores (Figure 3 and Figure S1). Bulut et al and several other publications have documented that higher BMI is a risk factor for early disc degeneration and increases the likelihood of recurrent herniated intervertebral discs.26–29 These results emphasize the importance of careful patient selection. In cases where disease severity approaches the upper limits of IDB’s efficacy, physicians must thoroughly discuss these limitations with patients. Our multivariate analysis, controlling for age, BMI, and disc characteristics, demonstrated that facet joint degeneration independently predicts suboptimal outcomes. Specifically, higher facet joint grades were significantly associated with less improvement in both VAS (β = −17.48, P = 0.017) and ODI (β = −21.92, P = 0.006), while age, BMI, and disc characteristics were not significant predictors for VAS or ODI improvement. Additionally, unsatisfactory outcomes were predominantly observed in older patients and those with significantly higher grades of facet joint degeneration. This underscores the importance of assessing facet joints alongside disc degeneration to avoid overlooking high-grade facet joint degeneration, which may contribute not only to motion-related pain in addition to discogenic pain, but also to limitations in daily function and overall quality of life.30
According to our previous publication, the disc characteristic of protrusion or extrusion was identified as the only significant factor influencing the one-year outcome of IDB.16 However, we expanded the patient cohort in the present study and extended the follow-up period to two years. Our findings show that, while disc characteristics remain influential, their significance regarding VAS improvement after IDB has diminished to near statistical insignificance. Notably, with the longer follow-up, facet joint issues emerged as a more significant factor affecting IDB outcomes. Bashkuev et al in their finite element model study revealed that early mechanical changes associated with disc degeneration have the greatest impact on facet joint loading.31 As degeneration progresses, facet joint deterioration increasingly influences disc loading. This suggests that, alongside the progression of disc degeneration, facet joint degeneration may co-exist and serve as an early indicator of more advanced spinal degeneration. Over time, this degeneration appears to reduce the efficacy of IDB, likely because IDB primarily targets cartilage but has limited impact on bony structures or bone spurs.32
Although this prospective study represents the largest and longest-followed cohort investigating IDB treatment for lumbar DDD, it remains limited. The non-randomized, single-center design and potential selection bias may limit the generalizability of our findings. We did not report the duration of pain symptoms prior to surgery, so we were unable to analyze its correlation with postoperative outcomes. In addition, this study did not assess possible central or peripheral sensitization, which is also an important limitation. Future studies should include evaluation tools such as the Central Sensitization Inventory (CSI) and PainDETECT/DN4 to assess neuropathic features.
Nevertheless, clinicians should carefully select patients by thoroughly evaluating disc and facet joint pathology, overall health status, and baseline functional limitations. Our findings suggest that patients with high-grade facet joint degeneration may experience less improvement in pain, function, and quality of life and should be counseled about the potential need for secondary interventions. Future multicenter, randomized studies are warranted to validate and extend these observations.
Conclusions
IDB can achieve long-term effectiveness in treating contained lumbar DDD. However, patients with high‑grade facet joint degeneration—especially when accompanied by advanced disc degeneration—tend to have poorer pain relief, smaller functional and quality‑of‑life improvements, and a greater risk of needing subsequent surgery. Thus, IDB may be best viewed as a stepwise or bridging intervention between conservative therapy and definitive fusion/fixation for selected patients. Thorough preoperative imaging evaluation and explicit patient counseling are therefore recommended to optimize prognosis.
Data Sharing Statement
The datasets generated or analyzed during this study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors acknowledge the administrative, technical, and financial support provided by China Medical University Hospital, Taichung, Taiwan [DMR-114-028].
Disclosure
The authors declare that they have no competing interests.
References
1. Kirnaz S, Capadona C, Wong T, et al. Fundamentals of intervertebral disc degeneration. World Neurosurg. 2022;157:264–273. doi:10.1016/j.wneu.2021.09.066
2. Manchikanti L, Singh V, Falco FJ, Benyamin RM, Hirsch JA. Epidemiology of low back pain in adults. Neuromodulation. 2014;17(Suppl 2):3–10. doi:10.1111/ner.12018
3. Ravindra VM, Senglaub SS, Rattani A, et al. Degenerative lumbar spine disease: estimating global incidence and worldwide volume. Global Spine J. 2018;8(8):784–794. doi:10.1177/2192568218770769
4. Yang N, Di J, Wang W, Feng H. Global burden of low back pain from 1990 to 2021: a comprehensive analysis of risk factors and trends using the global burden of disease study 2021. BMC Public Health. 2025;25(1):1886. doi:10.1186/s12889-025-23178-1
5. Fujii K, Yamazaki M, Kang JD, et al. Discogenic back pain: literature review of definition, diagnosis, and treatment. JBMR Plus. 2019;3(5):e10180. doi:10.1002/jbm4.10180
6. Risbud MV, Shapiro IM. Role of cytokines in intervertebral disc degeneration: pain and disc content. Nat Rev Rheumatol. 2014;10(1):44–56. doi:10.1038/nrrheum.2013.160
7. Bai DY, Liang L, Zhang -B-B, et al. Total disc replacement versus fusion for lumbar degenerative diseases - a meta-analysis of randomized controlled trials. Medicine. 2019;98:e16460. doi:10.1097/MD.0000000000016460
8. Bouterse A, Cabrera A, Jameel A, Chung D, Danisa O. Application of machine learning to identify risk factors for outpatient opioid prescriptions following spine surgery. Biomedicine. 2024;14(4):51–60. doi:10.37796/2211-8039.1471
9. Park SY, Moon S-H, Park MS, et al. Intradiscal electrothermal treatment for chronic lower back pain patients with internal disc disruption. Yonsei Med J. 2005;46(4):539–545. doi:10.3349/ymj.2005.46.4.539
10. Bron JL, Helder MN, Meisel HJ, Van Royen BJ, Smit TH. Repair, regenerative and supportive therapies of the annulus fibrosus: achievements and challenges. Eur Spine J. 2009;18(3):301–313. doi:10.1007/s00586-008-0856-x
11. Estefan M, Estefan V. StatPearls. 2025.
12. Helm S, Hayek SM, Benyamin RM, Manchikanti L. Systematic review of the effectiveness of thermal annular procedures in treating discogenic low back pain. Pain Physician. 2009;12(1;1):207–232. doi:10.36076/ppj.2009/12/207
13. Freeman BJ, Fraser RD, Cain CM, Hall DJ, Chapple DC. A randomized, double-blind, controlled trial: intradiscal electrothermal therapy versus placebo for the treatment of chronic discogenic low back pain. Spine. 2005;30(21):2369–2377. doi:10.1097/01.brs.0000186587.43373.f2
14. Fukui S, Nitta K, Iwashita N, et al. Intradiscal pulsed radiofrequency for chronic lumbar discogenic low back pain: a one year prospective outcome study using discoblock for diagnosis. Pain Physician. 2013;16(4;7):E435–442. doi:10.36076/ppj.2013/16/E435
15. HelmIi S, Simopoulos TT, Stojanovic M, Abdi S, El Terany MA. Effectiveness of thermal annular procedures in treating discogenic low back pain. Pain Physician. 2017;20(20;6):447–470. doi:10.36076/ppj/447
16. Md MY, Goh C-H, Wu C-Y, et al. An analysis of the clinical and radiological prognostic factors affecting the outcomes of lumbar intradiscal biacuplasty. Int J Med Sci. 2023;20(8):1115–1122. doi:10.7150/ijms.85777
17. Desai MJ, Kapural L, Petersohn JD, et al. A prospective, randomized, multicenter, open-label clinical trial comparing intradiscal biacuplasty to conventional medical management for discogenic lumbar back pain. Spine. 2016;41(13):1065–1074. doi:10.1097/BRS.0000000000001412
18. Kapural L, Vrooman B, Sarwar S, et al. A randomized, placebo-controlled trial of transdiscal radiofrequency, biacuplasty for treatment of discogenic lower back pain. Pain Med. 2013;14(3):362–373. doi:10.1111/pme.12023
19. McCarthy M, Chang C-H, Pickard SA, et al. Visual analog scales for assessing surgical pain. J Am Coll Surg. 2005;201(2):245–252. doi:10.1016/j.jamcollsurg.2005.03.034
20. Fairbank JC, Pynsent PB. The oswestry disability index. Spine. 2000;25(22):2940–2952. doi:10.1097/00007632-200011150-00017
21. Cheng J, Zheng W, Wang H, et al. Posterolateral transforaminal selective endoscopic diskectomy with thermal annuloplasty for discogenic low back pain: a prospective observational study. Spine. 2014;39:B60–65. doi:10.1097/BRS.0000000000000495
22. Kapural L, Vrooman B, Sarwar S, et al. Radiofrequency intradiscal biacuplasty for treatment of discogenic lower back pain: a 12-month follow-up. Pain Med. 2015;16(3):425–431. doi:10.1111/pme.12595
23. Desai MJ, Kapural L, Petersohn JD, et al. Twelve-month follow-up of a randomized clinical trial comparing intradiscal biacuplasty to conventional medical management for discogenic lumbar back pain. Pain Med. 2017;18(4):751–763. doi:10.1093/pm/pnw184
24. Kapural L, Ng A, Dalton J, et al. Intervertebral disc biacuplasty for the treatment of lumbar discogenic pain: results of a six-month follow-up. Pain Med. 2008;9(1):60–67. doi:10.1111/j.1526-4637.2007.00407.x
25. Karaman H, Tüfek A, Kavak GÖ, et al. 6-month results of transdiscal biacuplasty on patients with discogenic low back pain: preliminary findings. Int J Med Sci. 2010;8(1):1–8. doi:10.7150/ijms.8.1
26. Zhou J, Mi J, Peng Y, Han H, Liu Z. Causal associations of obesity with the intervertebral degeneration, low back pain, and sciatica: a two-sample mendelian randomization study. Front Endocrinol. 2021;12:740200. doi:10.3389/fendo.2021.740200
27. Hoffeld K, Lenz M, Egenolf P, et al. Patient-related risk factors and lifestyle factors for lumbar degenerative disc disease: a systematic review. Neurochirurgie. 2023;69(5):101482. doi:10.1016/j.neuchi.2023.101482
28. Quah C, Syme G, Swamy GN, et al. Obesity and recurrent intervertebral disc prolapse after lumbar microdiscectomy. Ann R Coll Surg Engl. 2014;96(2):140–143. doi:10.1308/003588414X13814021676873
29. Bulut G, Isik S, Etli MU, Yaltirik CK. The impact of demographic characteristics, obesity, surgical level, and intervertebral disc properties on recurrence of lumbar disc herniation. World Neurosurg. 2024;190:e748–e753. doi:10.1016/j.wneu.2024.07.214
30. Lee JY, Lee HI, Lee SH, Kim NH. Mechanical influence of facet tropism in patients with chronic discogenic pain disorder. Bone Joint Res. 2024;13(9):452–461. doi:10.1302/2046-3758.139.BJR-2023-0363.R1
31. Bashkuev M, Reitmaier S, Schmidt H. Relationship between intervertebral disc and facet joint degeneration: a probabilistic finite element model study. J Biomech. 2020;102:109518. doi:10.1016/j.jbiomech.2019.109518
32. Puneet Sayal MD, Tyler Crone MS, Alan Dine BS, et al. Intervertebral disc temperature mapping during disc biacuplasty in the human cadaver. Pain Physician. 2015;18(2;3):E217–223. doi:10.36076/ppj/2015.18.E217
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.