Back to Journals » Advances in Medical Education and Practice » Volume 12
Interprofessional Oral Health Collaboration: A Survey of Knowledge and Practice Behaviors of Hospital-Based Primary Care Medical Providers in New York City
Authors Laniado N ![]() , Cloidt M, Altonen B
, Cloidt M, Altonen B ![]() , Badner V
, Badner V
Received 9 August 2021
Accepted for publication 17 September 2021
Published 14 October 2021 Volume 2021:12 Pages 1211—1218
DOI https://doi.org/10.2147/AMEP.S332797
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Nadia Laniado,1 Megan Cloidt,1 Brian Altonen,2 Victor Badner1
1Department of Dentistry, Health+Hospitals/Jacobi Medical Center Bronx, New York, NY, 10461, USA; 2Department of Research Administration, Health+Hospitals/Central Office, New York, NY, 10013, USA
Correspondence: Nadia Laniado
Department of Dentistry, Health+Hospitals/Jacobi Medical Center, 1400 Pelham Parkway South Bronx, New York, NY, 10461, USA
Tel +1-718-918-3667
Fax +1-718-918-6147
Email [email protected]
Background: The siloed delivery of oral and medical health care in the United States has contributed to a lack of awareness of the consequences of poor oral health and has hampered effective interprofessional education and collaboration. The aim of this study was to assess the knowledge and practice behaviors of primary care medical providers in an urban safety-net hospital regarding collaboration with dentists and integration of oral health into overall health-care delivery.
Methods: A 36-item survey was designed in a web-based platform (Survey Monkey®) and electronically distributed in September 2020 to 181 primary care medical providers (physicians, nurses, physician assistants) within a municipal hospital in the Bronx, New York. The questionnaire included sections on demographics, current practices, oral health knowledge, and opinions regarding interprofessional collaboration. Descriptive statistics and bivariate analyses using the chi-square and Fisher’s exact test were performed with a significance level of 0.05.
Results: The response rate was 66% (119 respondents). The vast majority (80%) reported little or no training in oral health and 85% reported no team experience with oral health professionals. Medical providers’ confidence in examining the oral cavity was positively associated with previous additional training (p = 0.001) and with team experience (p = 0.005). The two most commonly reported barriers to willingness to collaborate were lack of formal relationships with dental providers (74%) and competing priorities (69%).
Conclusion: Overall, there is very limited awareness and integration of oral health into the clinical practice of medical providers at this safety-net hospital. However, those providers with previous training and team experience had greater oral health confidence. Given the critical importance of oral health to overall health, increased efforts should be directed to further educate and train medical providers and address barriers to interprofessional care.
Keywords: health promotion, interprofessional relations, oral health, oral health care, primary health care
Background
The historic separation of medical and dental professional education in the United States (US), apparent in the siloed delivery of oral and medical health care and services, has contributed to a lack of awareness of the consequences of poor oral health and has hampered effective interprofessional education (IPE) and collaboration.1–4 This compartmentalization of care processes has also resulted in poorer overall health outcomes and higher costs for patients.5 Those who bear the greatest burden of disease are vulnerable populations (ie, low-income individuals, ethnic minorities, immigrants, and individuals with disabilities) who may have low oral health literacy and limited access to care.6,7
There is a robust and growing body of evidence that oral health is a critical component of overall health and that poor oral health may lead to negative health outcomes including the exacerbation of chronic inflammatory diseases and conditions such as diabetes, cardiovascular disease, and pulmonary disease.8–12 The US Surgeon General’s landmark report, Oral Health in America, reminded educators and practitioners of the fundamental fact that oral diseases and disorders present a systemic burden and that health-care providers should be “ready, willing, and able to work in collaboration to provide optimal health care for their patients.”13 Yet more than 20 years since that seminal report, and despite growing awareness of oral-systemic relationships, there is still little oral health content on non-dental professional websites and slow adoption of interprofessional practices by medical providers.14,15
In recent years, many initiatives have been advanced in order to break down this fragmented structure and broaden interprofessional competencies in order to achieve the “triple aim” of improved patient experience of care, improved health of populations, and reduced costs.16–19 It has been demonstrated that IPE advances collaborative practice, reduces medical errors, and enhances health outcomes of patients and populations.20–24 The Association of American Medical Colleges (AAMC) advocated for oral health education for medical students and now expects medical students to demonstrate competence in multiple domains within oral health, such as understanding the caries and periodontal disease process and its implications for systemic health, performing oral health screenings, promoting preventive strategies, and collaborating with dental professionals.25
The National Call to Action to Promote Oral Health called for revamping health professions education to include oral health content as a key step towards eliminating oral health disparities.26 National organizations including the Liaison Committee on Medical Education, the Interprofessional Education Collaborative, the World Health Organization, and the American Association of Medical Colleges have established requirements and standards for IPE which are assessed on all United States Medical Licensing Examinations.25,27–29
In response to two Institute of Medicine reports (Advancing Oral Health in America and Improving Access to Oral Health Care for Vulnerable and Underserved Populations) the Health Resources and Services Administration (HRSA) developed the Integration of Oral Health and Primary Care Practice (IOHPCP) initiative to expand the oral health clinical competency of primary care clinicians and to integrate oral health and primary care practice.1,30,31 The HRSA’s grants for pre- and post-doctoral dental and primary care medical training programs include a focus on enhancing training to support integration of oral health within the broader health-care delivery system and new models of training for integrated oral health and medicine or primary care. Nevertheless, in settings where both medical and dental providers work together, such as many large hospital systems in the US, there is a gap in our understanding of the significant barriers that continue to exist which hamper cooperation and integration efforts.32
The aim of this study was to assess the knowledge and practice behaviors of primary care medical providers regarding oral health and interprofessional collaboration at New York City Health+Hospitals/Jacobi Medical Center, a large safety-net hospital in the Bronx, New York with an embedded dental department. This hospital, one of eleven in the largest municipal hospital system in the US, serves a largely immigrant and underserved population. This study aimed to better understand the barriers that exist in this setting in order to increase awareness of the importance of oral health and to develop programs to enhance referrals and collaboration among the medical and dental services.
Methods
Study Design
This project involved the development and administration of an anonymous cross-sectional survey instrument to primary care physicians, nurses, and physician assistants at Jacobi Medical Center to examine their knowledge and practice behaviors regarding oral health and interprofessional collaboration and referral. The use of an electronic survey allowed us to have a quantitative method for collecting information from a pool of respondents with minimal time and cost. Jacobi Medical Center is part of the New York City Health + Hospitals network which is the largest public municipal health-care system in the United States and treats the largest proportions of Medicaid and uninsured populations. The mission of Jacobi Medical Center is to serve the Bronx community by providing high-quality, cost-effective health care in a respectful way to all, regardless of income, gender identity, immigration status or ability to pay. The Jacobi Department of Dentistry is affiliated and co-located with the neighboring Albert Einstein College of Medicine in the Bronx, New York.
Participants and Recruitment
Attending physicians, internal medicine residents, nurses, and physician assistants from the primary care medical departments at Jacobi Medical Center were recruited by email for participation in the survey tool. The survey participants represented the providers potentially most amenable to IPE and collaboration with the Department of Dentistry as well as those where there were no established interprofessional referral programs.
An email link to the survey using the Survey Monkey® online software was sent to the Chair of the Department of Internal Medicine and Women’s Health for distribution to their attending physicians, residents, nurses, and physician assistants. The email described the purpose of the study, the amount of time needed to complete the survey, and assurances of participant anonymity. Participation in the survey was voluntary. Time for completion of the survey was estimated as 10 minutes. The survey was distributed to 181 individuals in September 2020. Each respondent was only able to complete the survey once. There was no incentive for participants and completion of the survey implied consent.
Survey Instrument
The 36-item survey instrument was developed by trained research team members in the Department of Dentistry and included four sections on demographics, current practices, oral health knowledge, and opinions regarding interprofessional collaboration. The survey tool was piloted by four senior internal medicine physicians and four senior dental attendings. Face and content validity analyses were performed before dissemination. The demographics section included five questions which assessed respondents’ individual sociodemographic information including age, sex, current role (attending, resident, nurse), medical specialty, and years of professional experience. The second section included 13 questions regarding current practices, oral health confidence, and opinions regarding interprofessional collaboration. The oral health knowledge section included 10 questions based on the Society of Teachers of Family Medicine’s (STFM) Smiles for Life program.33,34 The final section included eight questions which assessed participants’ opinions and attitudes towards IPE and collaboration. Survey questions were formulated to prompt either multiple choice or 5-point Likert-scale responses (“1 = always” to “5 = never”).
Data was collected in the secure Survey Monkey® platform and stored on a password-protected computer. No subject identifiers were stored. A four-week timeframe was allotted for return of the completed survey. Reminders were sent to the recipients at the end of weeks one, two, and three to encourage completion of the survey.
Statistical Analysis
Completed survey data was collected by the end of week four and exported to an Excel spreadsheet (Microsoft Corporation, Seattle, WA) and converted into a SPSS-formatted dataset (SPSS Windows version 26, Cary, NC). Descriptive statistics showing distributions of individual characteristics were performed for the survey participants overall and according to provider confidence in oral health assessment. To assess the relationship between categorical variables, the Chi-square and Fisher’s exact tests were used at a 5% level of significance. The study was reviewed by the Albert Einstein College of Medicine Institutional Review Board (IRB) and was deemed exempt (#2020-12521).
Results
One hundred nineteen (119) medical providers completed the survey (66% response rate). Characteristics of study participants overall and by oral health confidence are shown in Table 1. The majority of respondents were physicians (71%), ages 25–34 (56%), and female (69%). The vast majority (80%) reported a little or no training in oral health and 85% reported no team experience with oral health professionals. Approximately one-third (35%) had not been to the dentist themselves in over a year. Medical providers’ confidence in examining the oral cavity (assessed by responding to the question “How confident are you in examining the oral cavity?”) was significantly associated with previous additional training (p = 0.001) and having had team experience (p = 0.005).
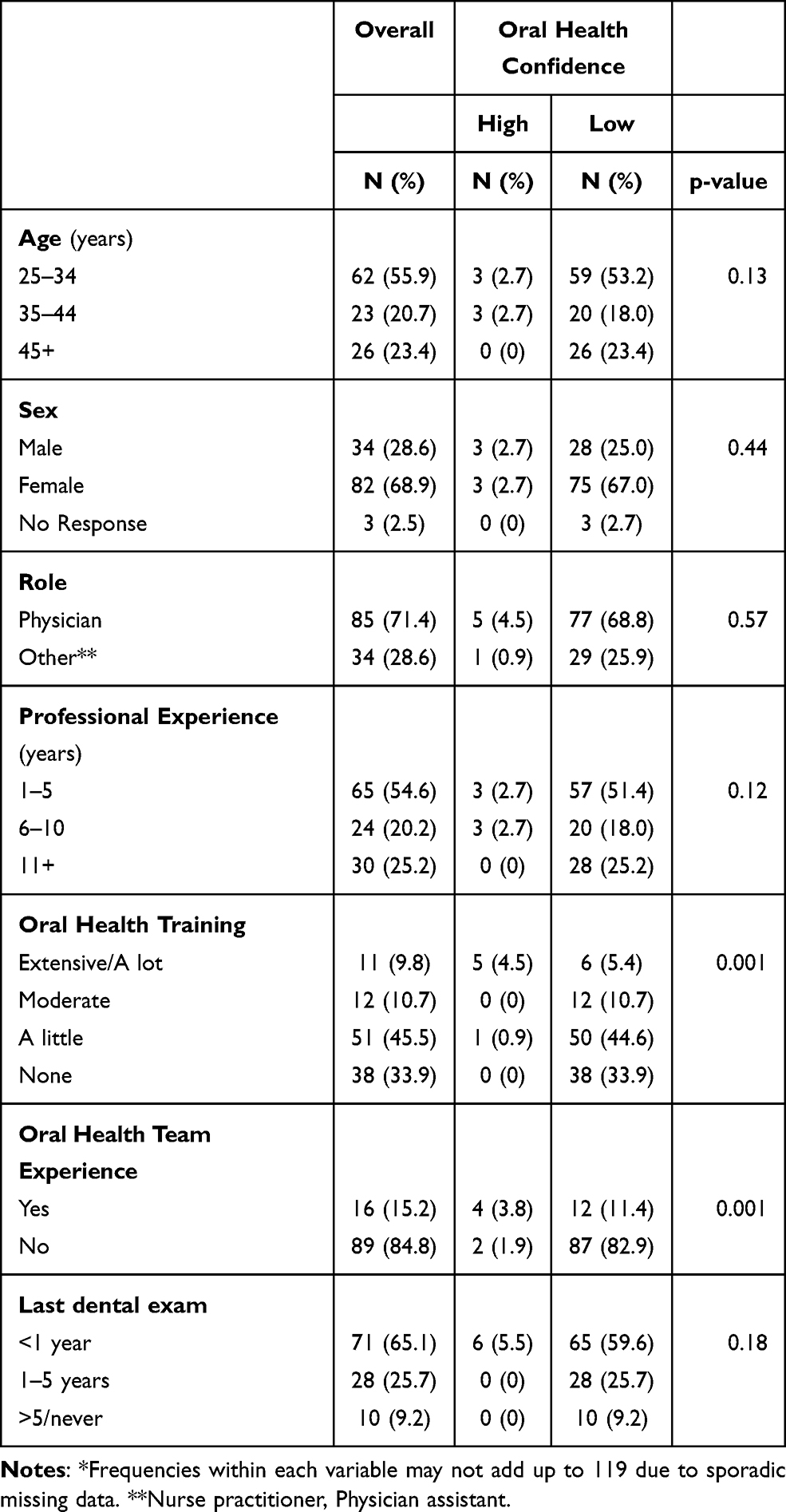 |
Table 1 Characteristics of Medical Providers Overall and by Oral Health Confidence, N = 119* |
Current practices of medical providers, shown in Figure 1, indicate that 69% rarely or never examine a patient’s oral cavity, 93% rarely or never assess a patient’s fluoride intake, 83% rarely or never perform an oral cancer screening, and 64% rarely or never inquire about a patient’s dental health. The mean score on the seven oral health knowledge questions, as shown in Table 2, was 64% with range from a high of 94% correct responses regarding knowledge of the systemic complications of oral infection to a low of 40% correct responses regarding knowledge of common sites for oral cancer. The three most prevalent major barriers to interprofessional collaboration, as shown in Table 3, were the lack of formal relationship between medical and dental professionals (74%), competing priorities (69%), and lack of electronic health record interoperability (48%).
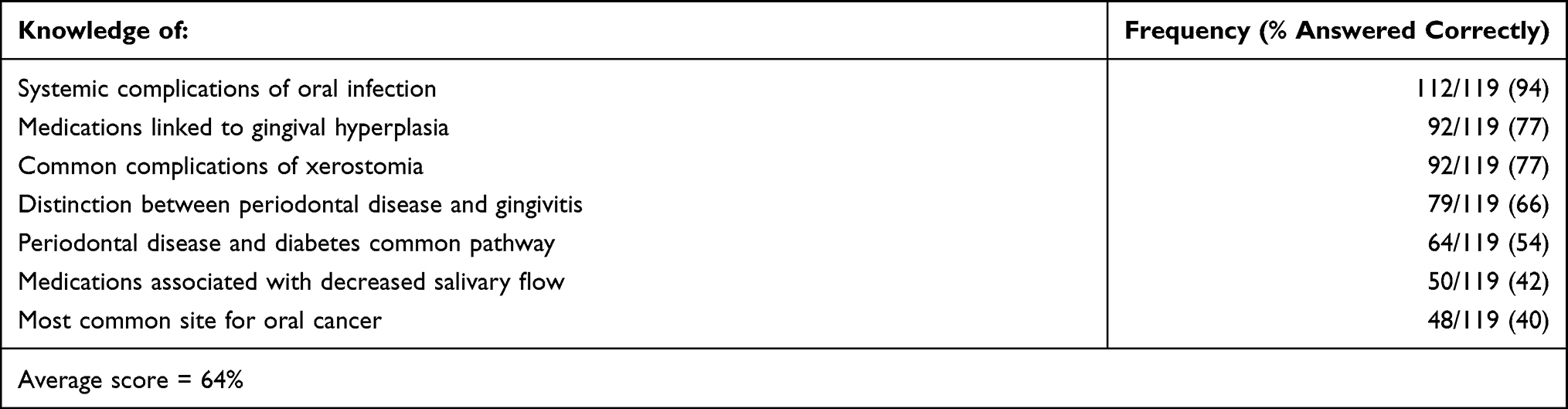 |
Table 2 Survey Responses to Oral Health Knowledge Questions, N = 119 |
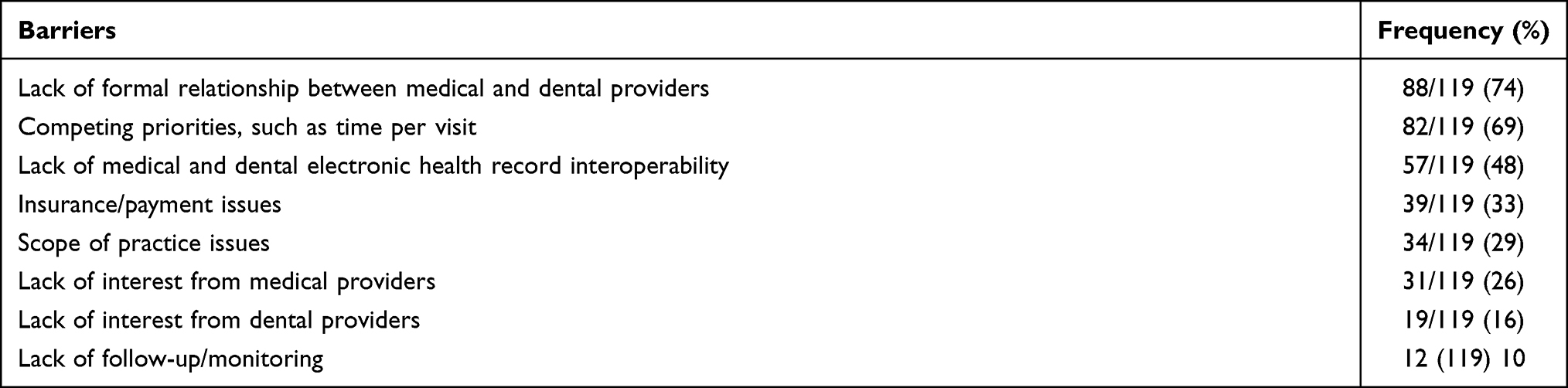 |
Table 3 Barriers to Interprofessional Collaboration, N=119 |
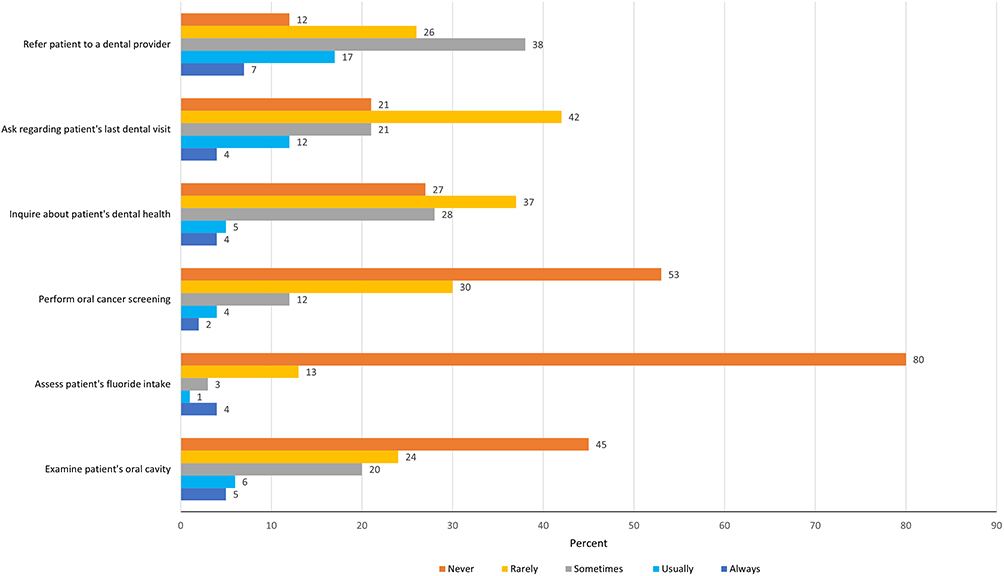 |
Figure 1 Current practices of survey participants, N = 119. |
Discussion
To our knowledge, this is the first study to assess the knowledge and practice behaviors of primary care providers at a large safety-net municipal hospital regarding oral health knowledge and clinical practice. Our results suggest that the majority of medical providers lacked oral health training, lacked oral health team experience, and had poor confidence in their own oral health skills. This is supported by studies demonstrating lack of confidence in performing oral health examinations by physicians as well as inconsistent oral health training in professional school.35,36 Notably, however, the more training and team experience that medical providers had the higher their oral health confidence. However, they were deficient in clinical oral health practice behaviors, interprofessional integration, and referral to dentists.
Our findings are supported by other studies in the US that have shown that oral health knowledge improves incorporation of oral health examination into medical care as well as referral to dental providers.34,37–40 Studies outside of the US (Malaysia, Australia, India, and Ethiopia) have also demonstrated inadequate oral health knowledge among health-care providers and a call for improvement in their training and skills.41–43 With renewed emphasis on the impact of poor oral health on general health, oral health prevention services (ie, fluoride varnish, caries risk assessment, and anticipatory guidance) and referrals from primary care physicians in obstetrics/gynecology and chronic disease services are rising.19 Furthermore, case studies in the US, such as “Into the Mouths of Babes,” in which medical providers deliver preventive oral health-care services, have demonstrated that integration of medical and dental care increased access to and coordination of patient care.44 Yet with the increased understanding that health and health care require a team-based approach in order to address patients’ needs, this study highlights the persistent barriers that exist with regard to education, training, and workflow to promote collaboration among medical and dental professionals.
Strengths of this study include the high response rate among primary care medical providers within this hospital system. An additional strength of this study is the focus on adults, not children, as a majority of research on IPE and collaboration has focused on the pediatric population since in the US they, and not adults, have essential dental benefits. This is also the first study, to our knowledge, to examine the barriers to interprofessional collaboration that exist at a large municipal safety-net hospital located in the county with the poorest overall health ranking in the entire state of New York.45 Other strengths are the unique co-location of both medical and dental services in this study (less than one percent of dentists currently work in a hospital setting).46 Limitations of this study include lack of generalizability of the findings as this was a single-site study as well as lack of construct validity of the survey instrument. In addition, the low sample sizes for nurses and physician assistants prevented us from more detailed analyses by role.
The results of this study suggest that increased oral health education of medical providers and improved bidirectional communication between medical providers and oral health-care team members is urgently needed. The present study found that only 54% of survey responders were aware of the common pathway between periodontal disease and diabetes, and only 42% were aware of medications that were associated with xerostomia. It is concerning that compared to an earlier analysis of oral health curricula in US residency programs, a recent program update found that less oral health is being taught.35,47 For a hospital that serves a vulnerable patient population with multiple chronic conditions (ie, diabetes mellitus, obesity, cardiovascular disease, and HIV), such as in this study, this collaboration has even greater significance as well as greater potential to address the impact of oral health on overall health.
Based on the results of this study, we have begun on-site educational seminars for medical providers regarding oral health, instruction in caries risk assessment and fluoride varnish, and have embedded dental residents in medical clinics to teach and train medical colleagues. In addition, in the dental clinic, we are providing evidence-based practices, such as chairside HbA1c screening in the dental clinic to screen for prediabetes with referral back to primary care for follow-up.48 Other pilot studies include elective rotations for our medical students at the hospital’s dental clinic as well as online didactic courses in oral health.
In addition to education and training of medical providers, we are investing in systems to integrate electronic health records and communication. Although our electronic health records are currently not integrated, we are currently under contract with a software vendor to establish an interoperable electronic health record by the end of 2022. Integration of oral health into primary care promises not only to improve patient experiences and outcomes but also to decrease costs through improved prevention and early treatment. Future studies will examine the impact and effectiveness of these improved models of integration of oral health into primary care practices, as well as patient acceptance of oral health screening as part of a medical examination.
Conclusions
The understanding that oral health is critical to overall health has led to a call for increased IPE and training of medical providers in oral disease and prevention. This study, at a municipal hospital in New York City, suggests that medical providers lack oral health training and team experience and additionally have poor confidence in their own oral health skills. Given the critical importance of oral health to overall health, and the increasing focus and requirements for oral health education and integration by national and international medical organizations, these findings support increased efforts to educate and train medical providers in order to guide and advance interprofessional collaboration and patient-centered care.
Abbreviations
US, United States; IPE, Interprofessional Education; AAMC, Association of American Medical Colleges; HRSA, Health Resources and Services Administration; IOHPCP, Oral Health and Primary Care Practice; STFM, Society of Teachers of Family Medicine; IRB, Institutional Review Board.
Data Sharing Statement
The dataset used and analyzed during this study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
All responders read a statement in the introduction to the survey instrument that declared “By completing the survey, you are consenting to participate in this study.” This study was approved by the Institutional Review Board (IRB) of the Albert Einstein College of Medicine, Bronx, New York, US. The IRB number is 2020-12521.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
This study was supported by the US Health Resources and Services Administration (HRSA) grant number D88HP37548. They have no role in the study design, execution, or publication of the study.
Disclosure
The authors declare that they have no competing interests.
References
1. Institute of Medicine. Advancing Oral Health in America. Washington DC: National Academies Press; 2011.
2. Mertz EA. The dental-medical divide. Health Aff (Millwood). 2016;35(12):2168–2175. doi:10.1377/hlthaff.2016.0886
3. Donoff RB, Daley GQ. Oral health care in the 21st century: it is time for the integration of dental and medical education. J Dent Educ. 2020;84(9):999–1002. doi:10.1002/jdd.12191
4. Enthoven AC. Integrated delivery systems: the cure for fragmentation. Am J Manag Care. 2009;15:S284–S290.
5. Simon L. Overcoming historical separation between oral and general health care: interprofessional collaboration for promoting health equity. AMA J Ethics. 2016;18(9):941–949.
6. Northridge ME, Kumar A, Kaur R. Disparities in access to oral health care. Annu Rev Public Health. 2020;41:513–535. doi:10.1146/annurev-publhealth-040119-094318
7. Zhang W, Wu YY, Wu B. Racial/ethnic disparities in dental service utilization for foreign-born and US -born middle-aged and older adults. Res Aging. 2019;41:845–867.
8. Willink A, Reed NS, Swenor B, Leinbach L, DuGoff EH, Davis K. Dental, vision, and hearing services: access, spending, and coverage for medicare beneficiaries. Health Aff (Millwood). 2020;39(2):297–304. doi:10.1377/hlthaff.2019.00451
9. Wu CZ, Yuan YH, Liu HH, et al. Epidemiologic relationship between periodontitis and type 2 diabetes mellitus. BMC Oral Health. 2020;20(1):204. doi:10.1186/s12903-020-01180-w
10. Beck JD, Moss KL, Morelli T, Offenbacher S. Periodontal profile class is associated with prevalent diabetes, coronary heart disease, stroke, and systemic markers of c-reactive protein and interleukin-6. J Periodontol. 2018;89(2):157–165. doi:10.1002/JPER.17-0426
11. Manger D, Walshaw M, Fitzgerald R, et al. Evidence summary: the relationship between oral health and pulmonary disease. Br Dent J. 2017;222(7):527–533. doi:10.1038/sj.bdj.2017.315
12. Siddiqi A, Zafar S, Sharma A, Quaranta A. Diabetes mellitus and periodontal disease: the call for interprofessional education and interprofessional collaborative care - a systematic review of the literature. J Interprof Care. 2020;1–9. doi:10.1080/13561820.2020.1825354
13. U.S. Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General. Rockville, MD: US Department of Health and Human Services, National Institute of Dental and Craniofacial Research. National Institutes of Health; 2000.
14. Shimpi N, Glurich I, Panny A, Acharya A. Knowledgeability, attitude, and practice behaviors of primary care providers toward managing patients’ oral health care in medical practice: Wisconsin statewide survey. J Am Dent Assoc. 2019;150(10):863–872. doi:10.1016/j.adaj.2019.05.020
15. Weintraub JA, Jamison AR, Rozier RG, Atchison KA. Assessing oral health content in nondental professional association websites. J Public Health Dent. 2021;81(3):240–244. doi:10.1111/jphd.12441
16. Greiner AC, Knebel E. Health Professions Education: A Bridge to Quality. Health Professions Education: A Bridge to Quality. Washington, DC: The National Academies Press; 2003.
17. Dolce MC, Barrow J, Jivraj A, Pham D, Da Silva JD. Interprofessional value-based health care: nurse practitioner-dentist model. J Public Health Dent. 2020;80(Suppl 2):S44–S49. doi:10.1111/jphd.12419
18. Dolce MC, Parker JL, Werrlein DT. Innovations in oral health: a toolkit for interprofessional education. J Interprof Care. 2017;31(3):413–416. doi:10.1080/13561820.2016.1258394
19. Atchison KA, Rozier G, Weintraub JA. Integration of oral health and primary care, National Academy of Medicine. NAM Perspectives. 2018;8(10). doi:10.31478/201810e
20. Ahern J, Nunn J. The integration of oral health-related best practice recommendations in the management of patients with diabetes: a cross-sectional survey of primary care physicians. J Public Health Dent. 2020. doi:10.1111/jphd.12397
21. Bridges DR, Davidson RA, Odegard PS, Maki IV, Tomkowiak J. Interprofessional collaboration: three best practice models of interprofessional education. Med Educ Online. 2011;16:6035.
22. Chazin S, Crawford M. Oral Health Integration in Statewide Delivery System and Payment Reform. Center for Health Care Strategies, Inc; 2016.
23. Cole JR
24. Perrier RS, Goldman J, Freeth D, Zwarenstein M. Interprofessional education: effects on professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2013;3. doi:10.1002/14651858.CD002213.pub3
25. American Association of Medical Colleges. Report Ix: Contemporary Issues in Medicine: Oral Health Education for Medical and Dental Students. Washington DC: American Association of Medical Colleges; 2008.
26. U.S. Department of Health and Human Services. A National Call to Action to Promote Oral Health. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institutes of Health, National Institute of Dental and Craniofacial Research. NIH publication no.03-5303; 2003.
27. Interprofessional education collaborative expert panel. Core Competencies for Interprofessional Collaborative Practice. Washington, DC: Interprofessional education collaborative; 2011.
28. World Health Organization. Framework for Action on Interprofessional Education and Collaborative Practice. Geneva: World Health Organization; 2010.
29. Liaison committee on medical education. Functions and Structure of a Medical School: Standards for Accreditation of Medical Education Programs Leading to the MD Degree; 2013.
30. Institute of Medicine. Improving Access to Oral Health Care for Vulnerable and Underserved Populations. Washington DC: National academies press; 2011.
31. U.S. Department of Health and Human Services HRSA. Integration of Oral Health and Primary Care Practice; 2014.
32. Harnagea H, Couturier Y, Shrivastava R, et al. Barriers and facilitators in the integration of oral health into primary care: a scoping review. BMJ Open. 2017;7(9):e016078. doi:10.1136/bmjopen-2017-016078
33. Clark MBDA, Maier R, Deutchman M, et al. Smiles for Life: A National Oral Health Curriculum.
34. Forbes J, Sierra T, Papa J. Advancing oral health knowledge and attitudes of physician assistant students using the smiles for life oral health curriculum. Fam Med. 2018;50(10):775–778. doi:10.22454/FamMed.2018.435186
35. Silk H, King R, Bennett IM, Chessman AW, Savageau JA. Assessing oral health curriculum in US family medicine residency programs: a CERA study. Fam Med. 2012;44(10):19–22.
36. Dwiel K, Hesketh MA, Alpert JL, et al. The impact of oral health training for primary care clinicians: a systematic review. Fam Med. 2019;51(3):251–261. doi:10.22454/FamMed.2019.232634
37. Al-Habashneh R, Barghout N, Humbert L, Khader Y, Alwaeli H. Diabetes and oral health: doctors’ knowledge, perception and practices. J Eval Clin Pract. 2010;16(5):976–980. doi:10.1111/j.1365-2753.2009.01245.x
38. Shimpi N, Schroeder D, Kilsdonk J, et al. Medical providers’ oral health knowledgeability, attitudes, and practice behaviors: an opportunity for interprofessional collaboration. J Evid Based Dent Pract. 2016;16(1):19–29. doi:10.1016/j.jebdp.2016.01.002
39. Khanbodaghi A, Natto ZS, Forero M, Loo CY. Effectiveness of interprofessional oral health program for pediatric nurse practitioner students at Northeastern University, United States. BMC Oral Health. 2019;19(1):170. doi:10.1186/s12903-019-0861-y
40. Cooper D, Kim J, Duderstadt K, Stewart R, Lin B, Alkon A. Interprofessional oral health education improves knowledge, confidence, and practice for pediatric healthcare providers. Front Public Health. 2017;5:209. doi:10.3389/fpubh.2017.00209
41. Yimenu DK, Adelo ES, Siraj EA, et al. Health professionals oral health knowledge and practice: unleashing the hidden challenges. J Multidiscip Healthc. 2020;13:459–469. doi:10.2147/JMDH.S254964
42. Philip P, Villarosa A, Gopinath A, Elizabeth C, Norman G, George A. Oral health knowledge, attitude and practices among nurses in a tertiary care hospital in Bangalore, India: a cross-sectional survey. Contemp Nurse. 2019;55(2–3):261–274. doi:10.1080/10376178.2019.1647790
43. Ahmad MS, Abuzar MA, Razak IA, Rahman SA, Borromeo GL. Perceptions of oral health education and practice among nursing students in Malaysia and Australia. Int J Dent Hyg. 2021;19(2):215–222. doi:10.1111/idh.12488
44. Atchison KA, Weintraub JA, Rozier RG. Bridging the dental-medical divide: case studies integrating oral health care and primary health care. J Am Dent Assoc. 2018;149(10):850–858. doi:10.1016/j.adaj.2018.05.030
45. Blomme C, Roubal A, Givens M, Johnson S, Brown L. County Health Rankings State Report. University of Wisconsin population health institute; 2020.
46. Nalliah RP, Allareddy V, Allareddy V. Dentists in the US should be integrated into the hospital team. Br Dent J. 2014;216(7):391–392. doi:10.1038/sj.bdj.2014.245
47. Silk H, Savageau JA, Sullivan K, Sawosik G, Wang M. An update of oral health curricula in US family medicine residency programs. Fam Med. 2018;50(6):437–443. doi:10.22454/FamMed.2018.372427
48. Greenberg BL, Glick M, Frantsve-Hawley J, Kantor ML. Dentists’ attitudes toward chairside screening for medical conditions. J Am Dent Assoc. 2010;141(1):52–62. doi:10.14219/jada.archive.2010.0021
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.