Back to Journals » Advances in Medical Education and Practice » Volume 14
Interprofessional Education in Health Informatics (IPEHI) for Health Sciences Programs
Authors Alanazi AT
Received 16 June 2023
Accepted for publication 15 October 2023
Published 19 October 2023 Volume 2023:14 Pages 1177—1182
DOI https://doi.org/10.2147/AMEP.S422725
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Abdullah T Alanazi1,2
1Department of Health Informatics, King Saud bin Abdul-Aziz University for Health Science (KSAU-HS), Riyadh, Saudi Arabia; 2Bioinformatics, King Abdullah International Medical Research Centre (KAIMRC), Riyadh, Saudi Arabia
Correspondence: Abdullah T Alanazi, Email [email protected]
Background: Given the significant changes the healthcare system has undergone recently; information technology has become an indispensable tool. To properly train future healthcare providers, it is vital to introduce information technology courses in Health Sciences programs. The provision of healthcare services now requires teamwork, which has led to the need for interprofessional education in health sciences schools. Therefore, this study explores the necessity of introducing Interprofessional Education in Health Informatics (IPEHI) in health sciences programs. Additionally, the structure and content of the course were assessed.
Methods: A mixed-method approach was employed in this study to explore the need for health informatics interprofessional education among individuals with a health-related science background and who possessed health informatics expertise through work experience or formal post-graduation education. Following a cross-sectional survey-based study, expert subjects from academia and the workplace were convened for Delphi meetings to create an IPEHI course founded on the CAHIIM competency framework.
Results: 128 questionnaires were collected from three cities in Saudi Arabia. Of all the respondents, 80% agreed that the present health sciences education should be expanded. Additionally, 74% of them agreed that the proposed IPE-HI (Interprofessional Education in Health Informatics) would enhance their knowledge and positively impact the healthcare system. During the second phase, eight experts were invited to identify seven domains, which include health information science and technology, social, behavioral and information science and technology applied to health, information science and technology, leadership, social and behavioral aspects of health, professionalism, and interprofessional collaborative practice. The results emphasize the need for introducing an IPE-HI, as previous studies have also shown that educating health professionals in health information technology is crucial.
Conclusion: IPEHI plays a crucial role in producing competent health science graduates. Consequently, experts have developed and validated a proposed IPE-HI course.
Keywords: interprofessional education, health informatics, health education
A Letter to the Editor has been published for this article.
Background and Aims
Today, health care is delivered through a multi-professional integrated care approach. Physicians, nurses, pharmacists, and other healthcare professionals contribute to patient care. However, the fragmentation of patient care is due to poor communication and coordination, leading to serious adverse events and poor treatment outcomes. Promoting collaborative practice for patient-centered care would require interprofessional education (IPE). According to WHO, IPE occurs when “students from two or more professions learn about, from, and with each other to enable effective collaboration and improve health outcomes”.1 More importantly, WHO emphasizes that IPE is intended to prepare students as future healthcare professionals for more collaborative healthcare practice.
Given the need for change in healthcare, information technology can promote an effective, efficient, safe, and patient-centered healthcare system.2,3 A non-inclusive list of health information systems includes HIS (Hospital Information System), Electronic prescribing, telemedicine, m-health (mobile health), PACS (Picture archiving and communication system), IoMT (internet of medical things in health care, Artificial Intelligence, Robotics and Automation, wearables, and virtual reality. Information technology can enhance accessibility to healthcare services, as the example of using telemedicine in providing some healthcare services across distance.4 Further, information technology can minimize medical errors by providing alerts and supporting the clinical decision-making process.5 In addition to enhancing the accessibility and effectiveness of healthcare services, IT has the potential to enhance the efficiency of resources and improve patient satisfaction.6
Nevertheless, some challenges can hinder the full utilization of information technology. One study concluded that lack of training and knowledge in information technology is among the top barriers to the wide adoption of health information technology.7 Hence, the successful adoption of health information systems requires clinicians to be trained and equipped with the knowledge and skills to understand the power of these information systems and how to adapt them to their context and tasks according to healthcare processes and user preferences.8
Health informatics is the application of information technology to bring up excellence in delivering healthcare services and hence reflect on improving health outcomes of individuals and communities.9 According to the US National Library of Medicine, health informatics is
the interdisciplinary study of the design, development, adoption, and application of IT-based innovations in the delivery, management, and planning of health care services.10
Healthcare has undergone a massive reform focusing on care coordination through multiple healthcare professionals supported by information technology and greater patient engagement.11 The impact of Health Informatics during COVID-19 and applications like tawakalna, Seha, and virtual clinics have shed light on the potential and promises of IT.12 They have introduced a transformative change in the delivery of healthcare services.13 Collaboration among healthcare professionals from different fields is critical to providing high-quality patient care. Interprofessional Education (IPE) is an approach aimed at promoting this collaboration. However, there is a lack of research on the effectiveness of IPE programs in healthcare. It is important to have empirical evidence demonstrating IPE’s effectiveness in improving outcomes for patients and care providers, as highlighted by a recent study.14 A recent meta-analysis has suggested that IPE programs positively impact and effectively in various healthcare disciplines.15 However, further studies are necessary to determine the effects of IPE programs on students’ competence, especially those related to using information technology. This study aims to investigate the necessity for interprofessional education in health informatics (IPEHI) and its role in equipping health sciences students with the required knowledge and skills pertaining to health informatics. Additionally, the study aims to determine the optimal content and structure of IPEHI.
Methods
This study was divided into two phases. The first phase involved a cross-sectional survey conducted across health sciences colleges in Riyadh, Jeddah, and AlAhsa. The primary aim of this phase was to evaluate the requirement for interprofessional health informatics IPEHI education. The second phase was a qualitative study that entailed Delphi meetings with experts to gather their opinions on the structure and content of IPE-HI education. To participate in the first phase, the individuals were selected purposefully from the three locations. They had to possess a background in health-related sciences and be acquainted with health informatics via work experience or formal post-graduation education. The survey utilized a validated questionnaire to obtain data on the necessity for interprofessional education in health informatics (IPEHI).16 The survey included questions about the participants’ age, gender, specialties, information technology training, and experience with health information systems. It also included five-point Likert scale questions arranged in three groups to measure the need for IPEHI. The first group concentrated on knowledge aspects, with four questions about the current level of knowledge, the necessity of health informatics education for health sciences students, the potential benefits of IPEHI, and the need for IPEHI for health sciences curricula. The second group measured the impact of IPEHI on practice aspects such as healthcare delivery, the use of HIS, the quality of healthcare, healthcare efficiency, and the effect on barriers to adopting HIS. Finally, the survey inquired about the overall perceptions towards IPHIE. The survey underwent thorough assessments for face validity and reliability, yielding a Cronbach’s alpha coefficient of 0.837, indicating a satisfactory level. Based on these results, the survey can be deemed a dependable tool for collecting data. The descriptive and inferential statistical approaches were utilized to present the findings of this phase’s data analysis.
The IPE-HI was developed in response to a recognized need. To create it, an investigator held Delphi meetings with experts, utilizing a collaborative decision-making approach involving multiple rounds of systematic feedback. The methodology employed was content analysis, with the IPEHI being designed to meet the health informatics requirements of the Commission on Accreditation for Health Informatics and Information Management Education (CAHIIM).17 Participants were chosen based on their experience and interest in health informatics, with two representatives from academic and workplace settings in three cities (Riyadh, Jeddah, and AlAhsa). During the meetings, the CAHIIM competency framework was discussed alongside the course’s intended objectives and learning outcomes. Stakeholder needs were considered, and the participants suggested important topics. Two 90-minute meetings were held, with discussions recorded and transcribed. Only topics with 50% agreement or higher were retained for the second round, with the final consensus reached through the agreement of the subjects. The final structure of the course was presented to the participants, who were asked for their feedback.
Results
Out of 151 distributed questionnaires, 128 were received, indicating an 85% response rate. After conducting an initial analysis of the surveys, it was discovered that some responses were missing. Further investigation revealed that the missing answers were random, prompting median-based imputation to fill in the gaps. The survey participants had varying backgrounds, with 47% being male. The majority of participants (78%) had ten years or less of work experience, with the age groups being divided between 20–29 years (45%) and 30–39 years (52%). The participants were from three different universities and had backgrounds in Medicine (12%), Pharmacy (16%), Nursing (23%), Information Sciences (18%), and allied health sciences (31%). As for Information Technology (IT) training, 34% of the participants had formal training, 8% received training through workshops, and 23% were self-trained. When using Health Information Systems (HIS) in their practice, most participants (68%) frequently used HIS, while 22% rarely or never used it. The survey also explored the need for Interprofessional Health Informatics Education (IPEHI), revealing that 80% of participants believed that IPE-HI could improve their current knowledge in health informatics. Additionally, 74% agreed that health informatics education should be mandatory for all health science students, and the same percentage believed that IPEHI could provide essential knowledge and skills about health information technology for health science graduates. Regarding the perceived impact of IPEHI on practice, the results showed that it had a positive impact on healthcare delivery (78.9%), quality of healthcare (78.9%), efficiency of healthcare delivery (86%), better utilization of HIS (81.6%), and minimizing barriers to the adoption of HIS (75.5%). Additionally, 80.5% agreed on the positive impact of IPE-HI on practice aspects. Overall, the survey indicated a high level of agreement (73.7%) towards IPE-HI. Table 1 describes the answers of the respondents.
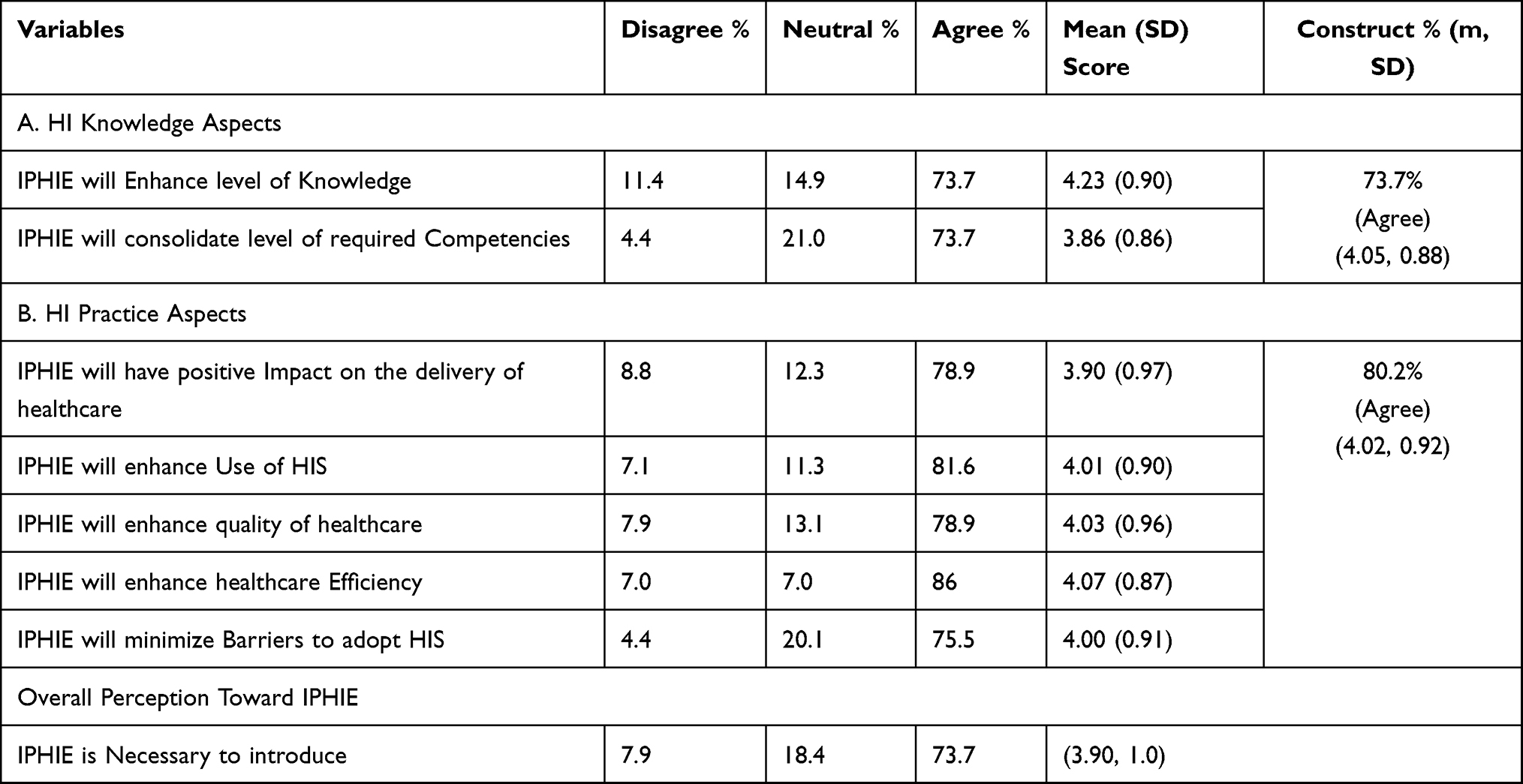 |
Table 1 Impact of the IPEHI |
The study used independent-sample t-tests to examine whether there were differences in how males and females perceived the impact of IPEHI on HI Knowledge Aspects, Practice Aspects, and overall perception of IPHIE. The results showed that gender did not significantly affect these outcomes (alpha levels > 0.05). Furthermore, a one-way ANOVA analysis was performed to assess the impact of respondents’ experience and background on the three primary outcomes of the study: impact on Knowledge Aspects, Practice Aspects, and overall perception of IPEHI. The analysis revealed that experience and background did not significantly impact the outcomes statistically (alpha levels > 0.05).
The second phase was conducted in an academic institution and eight experts participated in the two meetings. 4 experts were not able to join the study due to their tights schedule. Three experts come from academic profession and 5 are experts from healthcare industry. Two meetings were conducted, and the content of the IPEHI was established through using the CAHIIM competency-driven education. Using this competency framework has help the investigator to ensure that the saturation level is reached. CAHIIM framework aims to ensure that students demonstrate competence in a wide range of domains, including health, information science and technology, social and behavioral science, health information science and technology, human factors and socio-technical systems, social and behavioral aspects of health, social, behavioral, and information science and technology applied to health, professionalism, interprofessional collaborative practice, and leadership. The goal is to equip students with a diverse skillset encompassing various aspects of healthcare, technology, and interpersonal skills necessary to excel in their respective fields. Upon being presented with the results of the first phase and being thoroughly oriented to the CAHIIM framework, the experts expressed their agreement and appreciation for the outcome. One expert said, “With the rapid adoption of information technology in the healthcare industry, future healthcare providers must become proficient users to stay competitive”. Other experts mentioned. “In the near future, computer systems may be able to suggest diagnoses and treatment options based on findings associations between diseases and personal characteristics and behaviors”. The experts carefully examined and analyzed the results, considering every detail and aspect of the framework. They could fully comprehend the implications of the results and understand how they aligned with the CAHIIM framework.
At the Delphi meetings, experts recommended covering the following domains: Health Information Science and Technology, Social and Behavioral Aspects of Health, Leadership, Professionalism, and Interprofessional Collaborative Practice. Additionally, they suggested exploring how Social, Behavioral, and Information Science and Technology can be applied to improve health outcomes. Table 2 presents a list of topics recommended by experts for designing the IPEHI course.
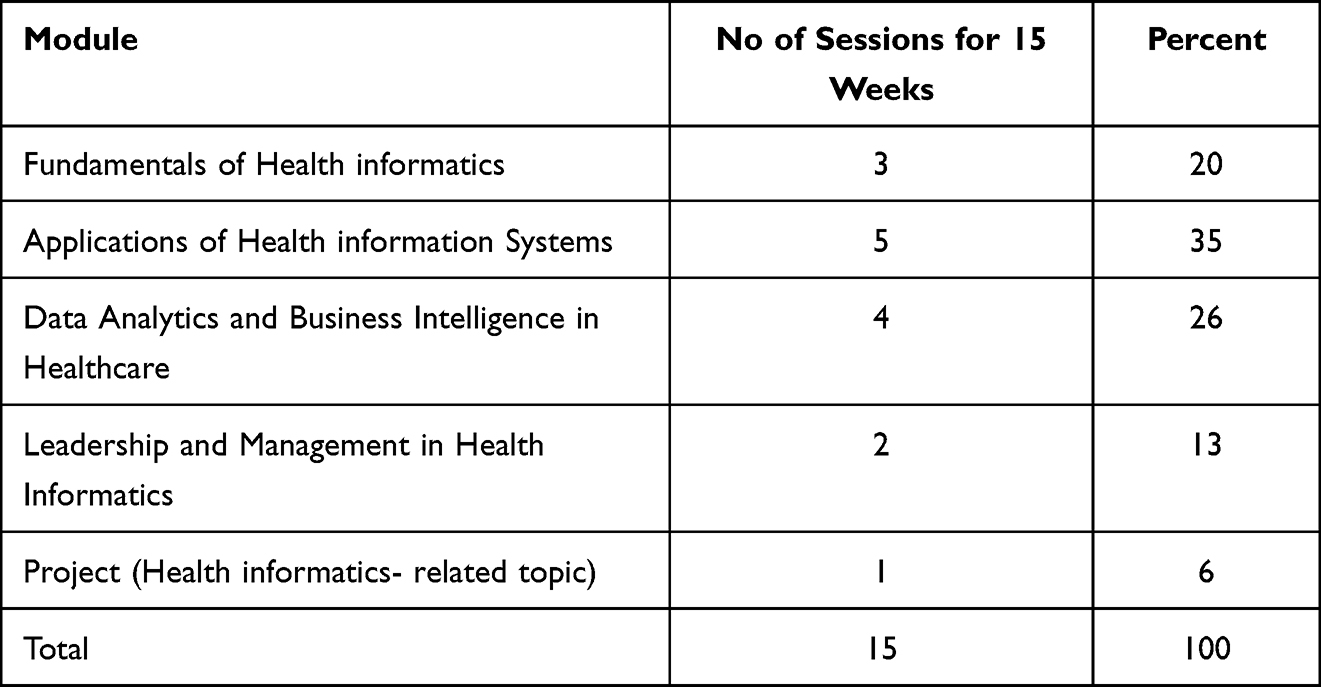 |
Table 2 Proposed IPEHI Course |
The course that is being proposed will cover the following topics: an introduction to health information and information technology, clinical applications and health information systems, health data quality and analytics, and a module on leadership and management in health informatics. Upon completing the course, students must showcase their learning by presenting a project on a health informatics-related topic.
Discussion
The study’s findings indicate the need for the implementation of IPE-HI. This outcome is consistent with prior research that underscores the importance of education and training in health informatics. The participants conveyed a favorable view regarding the influence of IPHIE on knowledge-related aspects, which can boost comprehension and strengthen crucial skills.18,19 Most of the survey participants agreed that the integration of Interprofessional Education for Health Informatics (IPE-HI) would lead to improved utilization of Health Information Systems (HIS), eliminate obstacles to HIS adoption, and have a positive impact on the quality, delivery, and efficiency of healthcare services. These findings are consistent with the conclusions drawn by previous research studies. Altuwaijri affirmed the positive effects of the HI program on knowledge and the future implementation of HIS in the healthcare sector.20 A set of competencies were selected and added to the IPE-HI course. According to Nelson and Staggers, these targeted competencies are intended to support the primary goal of the course.10 An expert group approved and suggested the competencies for the course, while the panel identified the IPEHI Learning modules and mapped them with the agreed-upon competencies. Interprofessional education (IPE) is a collaborative learning approach that brings students from diverse healthcare disciplines to enhance their understanding of interprofessional teamwork and provide better patient care. IPE promotes effective communication, teamwork, and collaborative decision-making among healthcare providers. IPE allows learners to share their knowledge, skills, and experiences, which can improve patient outcomes and reduce medical errors.21 The HI-specific requirements and health sciences curriculum determine the scope of learning in IPE. This approach provides a unique opportunity for students to gain insight into the potential, applications, and limitations of information technology in healthcare and to develop a holistic understanding of their uses in providing patient care. According to our findings, this study utilized a mixed-method approach incorporating quantitative and qualitative methods. Although the survey-based study was conducted in three cities, all sites are affiliated with one institution. Thus, national-level research is necessary to assess the effectiveness of this innovative HI course for interprofessional education (IPE). The qualitative aspect of the study focused on exploring the essential topics of IPEHI rather than confirming its effectiveness. It is essential to remember that participants’ views and opinions may have been influenced by social desirability and hype surrounding technologies. We recommend designing learning outcomes (LOs) for the proposed IPEHI and establishing an innovative assessment plan encompassing formative, summative, and standard approaches. Additional research and evidence would be invaluable in delivering Health informatics in interprofessional education.
Conclusion
The study demonstrates that interprofessional health informatics education (IPEHI) is indispensable for health sciences students. The study revealed that most participants agreed that Interprofessional Health Informatics Education (IPEHI) could significantly improve their health informatics knowledge and should be compulsory for every health science student. Additionally, IPEHI was perceived to positively impact healthcare delivery, quality, efficiency, better utilization of Health Information Systems (HIS), and the minimization of barriers to the adoption of HIS. The experts recommended including topics related to Health Information Science and Technology, Social and Behavioral Aspects of Health, Leadership, Professionalism, and Interprofessional Collaborative Practice, as well as exploring how Social, Behavioral, and Information Science and Technology can be applied to enhance health outcomes.
Ethics
This study was approved by the King Abdullah International Medical Research Center Review Board (NRC23R/479/08). Informed consent was obtained from the study participants. The guidelines outlined in the Declaration of Helsinki were followed.
Disclosure
The author reports no conflicts of interest in this work.
References
1. World Health Organization. Framework for Action on Interprofessional Education and Collaborative Practice. World Health Organization; 2010.
2. Sheikh A, Sood HS, Bates DW. Leveraging health information technology to achieve the “triple AIM” of healthcare reform. J Am Med Inform Assoc. 2015;22(4):849–856. doi:10.1093/jamia/ocv022
3. Reider J. The health information technology special issue: has IT become a mandatory part of health and healthcare? Am J Manag Care. 2018;24(1):17.
4. Alanazi AT, Al Hader B. Telemedicine patient satisfaction and cost: a comparative study in the COVID-19 Era. Cureus. 2022;14(10):1–6.
5. Alanazi A, Aldosari B, Alalawi W. An evaluation of drug-drug interaction alerts produced by clinical decision support systems in a Tertiary Hospital. Cureus. 2023;15(8). doi:10.7759/cureus.43141
6. AlGhamdi MA. Applying innovative ehealth to improve patient experience within healthcare organizations in the Kingdom of Saudi Arabia.
7. Aldosari B. Causes of EHR projects stalling or failing: a study of EHR projects in Saudi Arabia. Comput Biol Med. 2017;91:372–381. doi:10.1016/j.compbiomed.2017.10.032
8. Shark AR. The information technology gap in public administration: what we can learn from the certified public manager and senior executive service programs. J Public Aff Educ. 2016;22(2):213–230. doi:10.1080/15236803.2016.12002242
9. Sheikh A, Anderson M, Albala S, et al. Health information technology and digital innovation for national learning health and care systems. Lancet Digit Health. 2021;3(6):e383–e96. doi:10.1016/S2589-7500(21)00005-4
10. Nelson R, Staggers N. Health Informatics-E-Book: An Interprofessional Approach. Elsevier Health Sciences; 2016.
11. Groves P, Kayyali B, Knott D, Kuiken SV. The’big data’revolution in healthcare: accelerating value and innovation; 2016.
12. Alassaf N, Bah S, Almulhim F, AlDossary N, Alqahtani M. Evaluation of official healthcare informatics applications in Saudi Arabia and their role in addressing COVID-19 pandemic. Healthc Inform Res. 2021;27(3):255–263. doi:10.4258/hir.2021.27.3.255
13. Alkhalifah JM, Seddiq W, Alshehri BF, Alhaluli AH, Alessa MM, Alsulais NM. The role of the COVID-19 pandemic in expediting digital health-care transformation: Saudi Arabia’s experience. Inform Med Unlocked. 2022;33:101097. doi:10.1016/j.imu.2022.101097
14. Illingworth P, Chelvanayagam S. The benefits of interprofessional education 10 years on. Br J Nurs. 2017;26(14):813–818. doi:10.12968/bjon.2017.26.14.813
15. Guraya SY, Barr H. The effectiveness of interprofessional education in healthcare: a systematic review and meta-analysis. Kaohsiung J Med Sci. 2018;34(3):160–165. doi:10.1016/j.kjms.2017.12.009
16. Al Agili DE. A needs assessment for a master’s program in dental public health in Jeddah Saudi Arabia. Adv Med Educ Pract. 2013;4:55. doi:10.2147/AMEP.S41173
17. Commission on accreditation for health informatics and information management. www.cahiim.org; 2022. Available from: https://www.cahiim.org/.
18. Yu X, Xie Y, Pan X, Mayfield-Johnson S, Whipple J, Azadbakht E. Developing an evidence-based public health informatics course. J Med Lib Assoc. 2015;103(4):194. doi:10.3163/1536-5050.103.4.007
19. Hunt SL, Bakker CJ. A qualitative analysis of the information science needs of public health researchers in an academic setting. J Med Lib Assoc. 2018;106(2):184. doi:10.5195/jmla.2018.316
20. Altuwaijri MM. Supporting the Saudi e-health initiative: the Master of Health Informatics programme at KSAU-HS. EMHJ. 2010;16(1):119–124. doi:10.26719/2010.16.1.119
21. Mahajan R, Mohammed CA, Sharma M, Gupta P, Singh T. Interprofessional education: an approach to improve healthcare outcomes. Indian Pediatr. 2018;55(3):241–249. doi:10.1007/s13312-018-1326-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.