Back to Journals » Advances in Medical Education and Practice » Volume 17
Integrating Artificial Intelligence into Medical Education in LMICs: A Narrative Review
Authors Adefolalu AO ![]()
Received 1 April 2026
Accepted for publication 16 May 2026
Published 13 July 2026 Volume 2026:17 613617
DOI https://doi.org/10.2147/AMEP.S613617
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Adegoke O Adefolalu
Practice of Medicine & Clinical Integrated Programmes, Sefako Makgatho Health Sciences University, Pretoria, South Africa
Correspondence: Professor Adegoke O Adefolalu, Practice of Medicine & Clinical Integrated Programmes, Sefako Makgatho Health Sciences University, Pretoria, 0208, South Africa, Email [email protected]
Abstract: Artificial intelligence (AI) is reshaping clinical practice, yet formal AI education in medical curricula has lagged significantly behind—a gap particularly acute in low- and middle-income countries (LMICs). This narrative review examines AI integration in medical education across LMICs, with primary contextual focus on sub-Saharan Africa and African health systems within this broader framing. Available evidence suggests that a substantial proportion of medical students globally may lack formal AI education despite growing clinical AI adoption among physicians, with LMICs and African contexts disproportionately underrepresented in AI-in-medical-education literature. African contexts face compounding implementation challenges—infrastructure deficits, data scarcity, algorithmic bias in externally designed tools, and regulatory gaps—yet possess distinctive contextual opportunities. Applying a structured critical counterargument analysis, the review interrogates both the rationale for integration and the strongest arguments for delay. The review’s contribution lies in its LMICs-and-Africa-centred framing, its integration of three complementary theoretical frameworks, and its policy-oriented, phased implementation synthesis—dimensions not addressed in aggregate by existing reviews. AI integration in medical education in LMICs is a context-sensitive priority. The risks of unplanned inaction—widening competency gaps and forfeiture of iterative evaluation data—should be weighed against the risks of implementation, with careful, locally adapted, phased approaches offering the most defensible pathway forward.
Keywords: artificial intelligence, medical education, low- and middle-income countries, sub-Saharan Africa, fourth industrial revolution, curriculum integration, health equity, diffusion of innovations, technology acceptance, Kirkpatrick’s model
Background
The Widening Gap Between Clinical Reality and Educational Preparation
Artificial intelligence (AI) has fundamentally altered the trajectory of modern healthcare. Across specialties ranging from diagnostic radiology and pathology to primary care documentation and emergency triage, AI tools now assist with clinical decision-making, differential diagnosis generation, patient monitoring, and administrative automation.1,2 The Food and Drug Administration (FDA) had cleared or approved more than 1200 AI-enabled medical algorithms in the United States alone as of August 2025,3 while approximately two in three physicians globally report using AI in their clinical practice—a 78% increase from 2023.4 Available evidence suggests that many healthcare settings are rapidly approaching a tipping point of routine AI-augmented practice, though the pace and depth of adoption varies considerably across institutions and country contexts.
Yet medical education has struggled to keep pace. A 2025 international survey encompassing over 4500 students across 192 medical, dental, and veterinary faculties found that more than 75% reported receiving no formal AI education in their curricula.5 The majority of medical students acquire AI knowledge through social media and informal channels rather than structured educational programmes,6 an approach that creates heterogeneous and unverifiable competency levels while failing to address critical dimensions of ethical reasoning, bias recognition, and appropriate clinical application. Despite AI in medicine training frameworks published by the National Academy of Medicine and the World Health Organization, most medical schools have yet to implement them systematically.3
This disconnect is particularly pronounced in low- and middle-income countries (LMICs), where medical students face compounding inequities associated with the Fourth Industrial Revolution while simultaneously contending with resource limitations and infrastructural challenges.7 A critical geographical analysis of the AI-in-medical-education literature revealed a striking disparity: fewer than 10% of publications originate from Latin America, Africa, or Eastern Europe.8 In sub-Saharan Africa (SSA), the integration of medical AI has faced substantial delays, slowing its acceptance and implementation in medical interventions and healthcare services.9
Many African nations still lack the capacity or resources to develop comprehensive digital health strategies, creating a widening divide between Global North and Global South medical education systems.10 The World Health Organization forecasts a global health workforce shortfall of approximately 10 million workers by 2030, a shortage most acutely felt in LMICs,11 making competency in AI-assisted clinical tools increasingly relevant to effective practice in many settings. A Nigerian university study revealed that while students demonstrated awareness of AI, substantial gaps existed in their understanding of AI fundamentals and appropriate applications12—a pattern consistent across multiple LMIC contexts.13
Purpose and Scope of This Review
This narrative review advances a pragmatic, evidence-based position: controlled, theoretically informed integration of AI into medical education curricula is not only necessary but urgent, and the costs of delay exceed the risks of measured implementation. At the same time, applying a structured critical counterargument analysis, we explicitly examine the strongest arguments against integration—concerns about premature adoption, ethical unpreparedness, and resource constraints—and consider what weight they carry relative to the case for structured, phased action.
To support this argument, we draw upon three established theoretical frameworks—Rogers’ Diffusion of Innovations Theory,14 the Technology Acceptance Model (TAM),15 and Kirkpatrick’s Four-Level Evaluation Model16—to provide a structured, evidence-based approach for understanding and implementing AI integration in medical education. This review specifically synthesises evidence on AI in medical education with attention to African and LMIC contexts, examines theoretical frameworks applicable to technology adoption in resource-constrained settings, applies a structured critical counterargument analysis to interrogate both the rationale for integration and the strongest arguments for delay, analyses practical challenges and opportunities, and proposes evidence-based strategies for contextually appropriate, phased implementation.
Methods
Review Design and Rationale
We conducted a narrative review following the Scale for the Assessment of Narrative Review Articles (SANRA) criteria.17 Narrative reviews provide a flexible yet rigorous approach for knowledge synthesis particularly appropriate for topics requiring meaningful integration of complex, broad evidence with detailed, nuanced interpretation. For the purposes of this review, “AI integration in medical education” is defined as the intentional incorporation of AI-related content and competencies into undergraduate medical curricula, encompassing AI literacy (conceptual understanding and critical appraisal), clinical AI use (safe and appropriate application of AI-assisted tools), AI ethics (bias recognition, data governance, and equity considerations), and to a lesser extent, technical development skills. This review addresses LMICs broadly, with sub-Saharan Africa and African health systems serving as the primary contextual case focus, reflecting both the literature’s geographic gaps and the author’s contextual expertise. Given the interdisciplinary nature of AI integration in medical education—spanning technology, pedagogy, ethics, health policy, and global health equity—and the need to synthesise diverse evidence types including empirical studies, theoretical frameworks, policy analyses, and contextual reports from resource-limited settings, a narrative review methodology was deemed most appropriate. Systematic and scoping reviews of this topic have been published;18,19 our contribution lies in: (1) the contextualised application of three complementary theoretical frameworks specifically to LMIC and African medical education settings; (2) a structured critical counterargument analysis that explicitly presents, evaluates, and responds to the strongest arguments against integration; and (3) a policy-oriented, phased implementation synthesis tailored to resource-constrained contexts—dimensions not addressed in combination by existing reviews.
Literature Search Strategy
Initial searches were conducted between January 15–22, 2026; updated searches to capture the most recent literature were performed on May 10–11, 2026. We searched the following databases: PubMed/MEDLINE, Google Scholar (first 200 results per search string), ERIC (Education Resources Information Center, via EBSCOhost), Web of Science Core Collection (Clarivate Analytics), African Journals OnLine (AJOL), and Africa-Wide Information (via EBSCOhost). Search terms included combinations of: “artificial intelligence” OR “AI” OR “machine learning” OR “large language models”; “medical education” OR “undergraduate medical education” OR “curriculum”; “low- and middle-income countries” OR “LMICs” OR “Africa” OR “sub-Saharan Africa” OR “developing countries”; and “Fourth Industrial Revolution” OR “digital divide” OR “educational equity”. Seminal theoretical works (Rogers 1962; Davis 1989; Kirkpatrick 1994) were included regardless of date. For African-specific content, we supplemented searches with targeted country names (Nigeria, Kenya, South Africa, Ethiopia, Ghana, Tanzania, Uganda, Rwanda) and regional grey literature sources including African Union policy documents and WHO African Regional Office reports.
Inclusion and Exclusion Criteria
Publications were included if they: were published between 2020 and 2025 (seminal works excepted); focused on AI in undergraduate medical or health professions education; were relevant to LMICs, Africa, or resource-limited settings; discussed implementation strategies, challenges, or outcomes; or contributed theoretically or empirically to understanding technology adoption. We excluded publications focused primarily on postgraduate or continuing medical education, non-AI technologies (unless directly relevant to context), opinion pieces without substantive analysis, and non-English publications.
Selection Process and Source Characterisation
The literature search was conducted between January 15-22, 2026 and May 10-11, 2026. Database searches identified 2725 records: PubMed/MEDLINE (n=1247), Google Scholar (n=856), ERIC (n=89), Web of Science (n=432), African Journals OnLine (n=34), and Africa-Wide Information (n=67). An additional 78 records were identified through grey literature and hand-searching, yielding a total of 2803 records. After importing all records into Zotero reference management software, 856 duplicate records were removed, yielding 1947 unique records for screening. Title and abstract screening was conducted by the author against the inclusion/exclusion criteria. Approximately 1744 records were excluded at this stage on the basis of the stated criteria, retaining 203 records for full-text review. Full texts of 203 articles were retrieved; 17 could not be obtained despite contacting authors. Of the 186 full-text articles assessed for eligibility, 149 were excluded (insufficient LMIC/Africa focus, insufficient methodological detail, primarily theoretical content without practical application, or duplicate data from the same study), yielding 37 records for final narrative synthesis.
Source Characterisation
The 37 included sources comprised peer-reviewed journal articles (including empirical studies, systematic and scoping reviews, theoretical and conceptual papers, and implementation reports) and grey literature (policy documents and professional body reports). By geographic origin of study settings: approximately 38% originated from high-income countries with direct LMIC applicability, approximately 26% from African countries, approximately 19% from other LMIC contexts (Asia and Latin America), and the remainder from multi-national studies including African institutions. A standardised data extraction form was used to capture bibliographic details, study design, geographic context, AI focus, educational context, key findings, theoretical frameworks applied, and LMIC/African relevance. Peer-reviewed journal articles formed the primary evidence base. Grey literature—comprising policy documents from the African Union, WHO, and national health ministries, as well as reports from professional bodies—was treated as supplementary and contextual evidence and is explicitly distinguished from peer-reviewed findings in the synthesis narrative. Evidence was synthesised thematically, organised around the three theoretical frameworks, with strength of claims calibrated to the quality and consistency of supporting sources.
Analytical Framework
Three complementary theoretical frameworks served as analytical lenses throughout our synthesis:
- Rogers’ Diffusion of Innovations Theory:14 to understand adoption dynamics, timing implications, and the factors influencing innovation spread within healthcare and educational systems.
- Technology Acceptance Model (TAM):15 to identify factors determining whether individuals accept and effectively use AI technologies in educational and clinical contexts.
- Kirkpatrick’s Four-Level Evaluation Model:16 to structure assessment approaches across the levels of reaction, learning, behaviour, and results.
These frameworks guided evidence synthesis and informed our recommendations for implementation strategies, as summarised in Table 1.
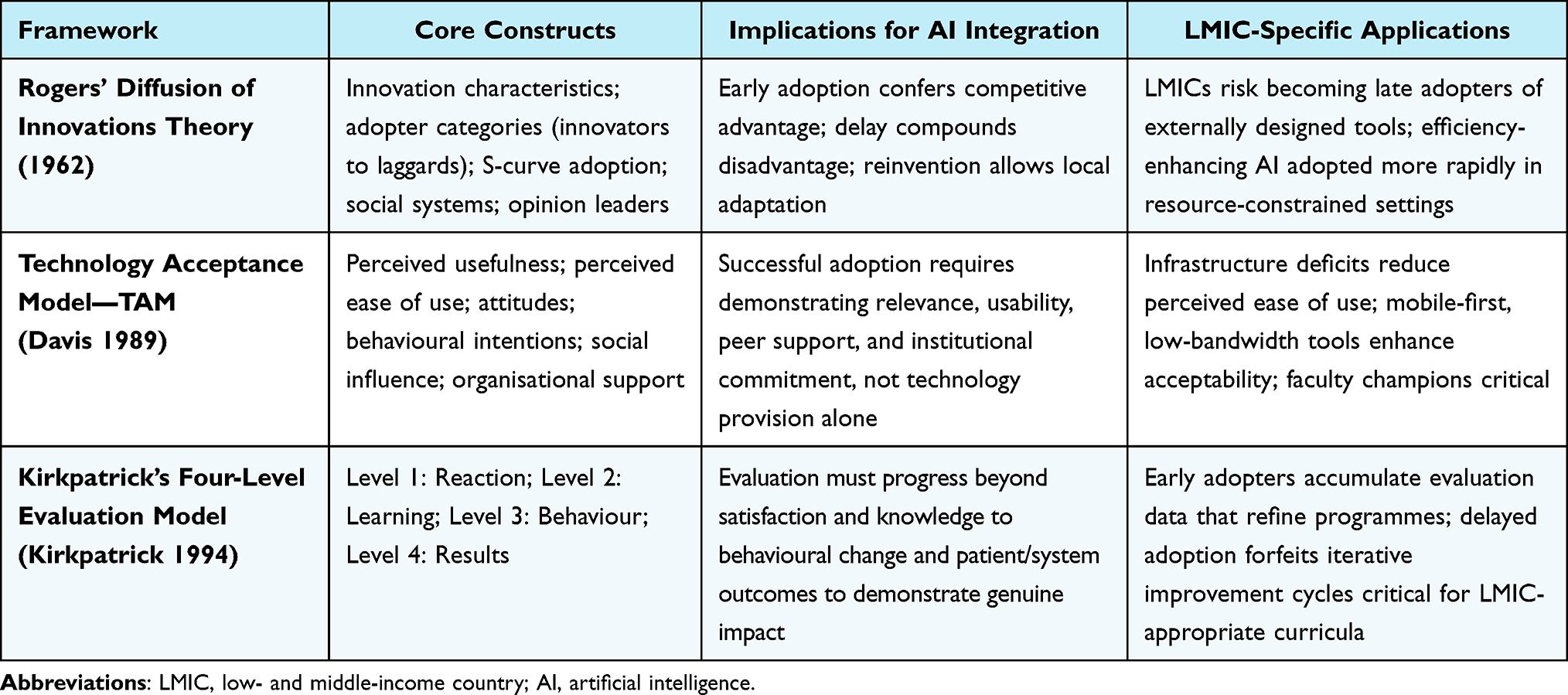 |
Table 1 Theoretical Frameworks Applied in This Review: Key Concepts and Implications for AI Integration in Medical Education |
Reflexivity Statement
The author brings perspectives from medical education, global health, clinical practice in resource-limited settings, and African healthcare contexts. We acknowledge that our interpretive positions shape our synthesis and have sought to represent diverse viewpoints, particularly centring voices from African and LMIC scholars. We recognise the limitations inherent in narrative review methodology, including potential selection bias and the influence of author perspectives on interpretation. We have applied a structured critical counterargument analysis—explicitly presenting, evaluating, and engaging with the strongest arguments against integration—to mitigate confirmation bias and strengthen analytical rigour.
Results and Discussion
The Current Landscape: AI Adoption in Healthcare and Medical Education
Rapid Clinical Adoption and the Education-Practice Chasm
The clinical landscape has already been transformed. The Lancet Digital Health recently characterised generative AI as poised to fundamentally reshape both medical practice and physician training, with large language models such as GPT-5, LLaMA, and DeepSeek enabling new modes of clinical reasoning support, documentation automation, and educational simulation.11 Applying Diffusion of Innovations Theory to this trajectory reveals that healthcare is traversing the steep portion of the S-curve, where adoption accelerates from early adopters to the early majority. AI applications now span multiple specialties, from diagnostic radiology and pathology to primary care documentation, emergency triage, and clinical decision support.1,2
For African contexts specifically, AI technologies offer compelling responses to longstanding healthcare challenges. Medical AI was first piloted in Africa in the mid-1980s, when deployment in Kenya improved health worker-patient interaction quality with evidence of increased symptom elicitation.10 More recently, AI algorithms have been deployed to analyse retinal images for diabetic retinopathy screening in Ghana and Kenya,20 and AI-enabled diagnostic tools are supporting healthcare workers across Nigeria, Morocco, Ethiopia, and South Africa.21 Given the shortages of skilled health workers in SSA—where medical education capacities are limited and the physician-to-population ratio remains critically low—AI-powered clinical tools represent one of the most scalable pathways to increasing both the quantity and quality of medical care.10
Yet this transformation also presents significant risks that medical education must address. The Technology Acceptance Model provides insight into a critical vulnerability: without demonstrable perceived usefulness coupled with manageable perceived ease of use, healthcare workers may resist or misuse AI technologies—potentially amplifying existing health inequities rather than ameliorating them.22 Without proper education and preparation, medical graduates may lack the competencies required to critically evaluate AI outputs, understand system limitations, or identify and address algorithmic biases that disproportionately affect marginalised populations.
Educational Lag and Geographic Disparities
Despite the pervasive clinical adoption of AI, formal AI education remains strikingly absent from most medical school curricula. A 2025 international survey of over 4500 students across 192 faculties found that more than 75% reported no formal AI education, with the majority acquiring their knowledge through social media and informal channels.5 This informal approach creates heterogeneous competency levels and fails to address critical skills including ethical reasoning, bias recognition, and appropriate clinical application. A scoping review published in BMC Medical Education confirmed that institutional barriers to AI adoption in undergraduate medical education (UME)—including faculty unpreparedness, absence of standardised learning outcomes, and lack of assessment frameworks—remain pervasive and disproportionately affect LMIC institutions.19
Research from Iranian medical students demonstrated that while 77.9% believed AI would benefit their careers, substantial gaps existed in their understanding of AI fundamentals.13 In Nigeria, medical students showed varied knowledge levels about AI, with enthusiasm but limited formal exposure.12 In Saudi Arabia, a 2025 multi-centre faculty survey found that knowledge rates averaged 58.9% across all groups, with only one-third of faculty agreeing on the reliability of AI-generated outputs.23 These findings, taken together, reflect a global educational deficit that is consistently most pronounced in non-Anglo-North-American settings.8
The consequences of this deficit are multi-dimensional. First, it perpetuates technological illiteracy among future physicians, limiting their ability to utilise AI tools or critically evaluate outputs. Second, it fails to build the ethical frameworks necessary for responsible AI deployment, including considerations of bias, privacy, transparency, and accountability.24 Third, it leaves students unprepared for AI-augmented clinical practice, potentially compromising patient safety and care quality.
The African Context: Unique Challenges and Opportunities
Infrastructure and Resource Constraints
The Fourth Industrial Revolution has amplified existing global inequities in medical education.25 While institutions in high-income countries invest in AI-enhanced simulation laboratories, personalised learning platforms, and comprehensive digital health infrastructures, many African medical schools contend with intermittent power supply, inadequate internet connectivity, outdated hardware, and insufficient data storage infrastructure. A systematic scoping review of AI in LMIC healthcare identified challenges including data availability, security concerns, resource limitations, regulatory gaps, poor internet connectivity, and digital literacy deficits as the primary barriers to AI integration in healthcare systems in SSA.9 With the low level of digitisation and limited electronic medical record adoption across Africa, locally generated health data—essential for training contextually appropriate AI systems—remains scarce.10
The consequences of this divide extend beyond individual institutions. Medical graduates trained without adequate AI literacy may find themselves professionally disadvantaged in an increasingly competitive global healthcare market. More critically, healthcare systems in LMICs may struggle to implement beneficial AI technologies if their workforce lacks the competencies to deploy, maintain, and critically evaluate these systems—creating a circular dependency in which educational lag perpetuates healthcare system lag.
Algorithmic Bias and Data Colonialism
The concept of algorithmic bias is particularly consequential in African contexts. Because most AI applications are developed outside Africa, most training datasets reflect physiological, epidemiological, and social characteristics of Western populations.10 Existing large language models providing medical advice are trained on data sources that reflect and embed the biases of WEIRD (Western, Educated, Industrialised, Rich, and Democratic) societies.26 For LLMs to be clinically useful for community health workers in African countries, they require training based on an understanding of local medical practices, languages, and vernacular—a condition rarely satisfied by existing commercial models.26
The manifestations of this bias extend to fundamental representational failures: AI image-generation systems trained on biased datasets have struggled to produce accurate depictions of African healthcare contexts, reflecting racial biases with historical roots in colonialism that remain embedded in global health datasets.27 More clinically consequentially, diagnostic algorithms trained predominantly on data from individuals of European descent may exhibit systematically reduced accuracy when applied to African populations, with potentially life-threatening implications for conditions including dermatological diagnoses, pulse oximetry readings, and cardiovascular risk stratification.28 Medical education must prepare graduates to recognise, critique, and address these biases—understanding both their technical origins and their historical and social contexts.
Opportunities for Innovation and Leapfrogging
African contexts also possess distinctive opportunities within this transformation. With smartphone penetration projected to increase substantially over the next decade, mobile-first AI solutions represent a more scalable and accessible entry point than PC-dependent platforms.10 Large and diverse patient populations provide substantial datasets for AI training and validation once appropriate data governance frameworks are established. Unique disease profiles and healthcare challenges create opportunities for locally relevant AI innovation, and resource constraints may drive creative, cost-effective solutions adaptable to similar settings globally.
African innovation in AI is not merely aspirational but actively occurring. A group of Nigerian high school students developed an MIT open-source-based application to identify counterfeit medicines, winning a Silicon Valley competition.10 Researchers at the Nelson Mandela African Institution of Science and Technology created BakiShule (Swahili: “stay in school”), a machine learning dropout-prediction system deployed in Tanzanian secondary schools.27 In Uganda and Kenya, an open-access web-based machine learning application was developed to supervise community health workers using deep learning to track performance against set targets.9 Growing interest in data science across the continent—evidenced by record applications to the 2024 Data Science Africa annual meeting27—signals an expanding foundation upon which medical AI education can build.
Decolonising AI in Medical Education
Calls to decolonise global health have emphasised the unequal power dynamics between those most affected by health problems and those who dictate research priorities, own data, and lead the field.27 AI integration in medical education offers an opportunity to address these power imbalances by positioning African institutions as co-creators rather than consumers of AI technologies, developing locally relevant applications addressing African health priorities, training African data scientists and AI specialists, and establishing ethical frameworks grounded in African values and contexts.27 The African Union’s Continental AI Strategy explicitly emphasises the need for African-led AI development and governance,29 and medical education can serve as a critical site for building the workforce required to fulfil this vision.
Theoretical Foundations for AI Integration in Medical Education
To effectively address AI integration in medical education, we must first understand the theoretical mechanisms governing how innovations are adopted within educational and healthcare systems. The three complementary frameworks summarised in Table 1 provide the analytical architecture for our synthesis.
Rogers’ Diffusion of Innovations Theory
Everett Rogers’ Diffusion of Innovations Theory,14 first published in 1962 and extensively applied in healthcare and medical education contexts, explains how, why, and at what rate new ideas and technologies spread through populations. According to Rogers, innovation diffusion depends on five key elements: the innovation itself, adopters, communication channels, time, and the social system. Adopter categories—innovators, early adopters, early majority, late majority, and laggards—occupy distinct positions on the adoption S-curve, with each position carrying different competitive implications.
For AI in medical education, Diffusion of Innovations Theory predicts that delays in adoption create cumulative disadvantages: early adopters gain influence over implementation standards, develop institutional expertise, establish best practices, and position themselves as innovation leaders. Research on diffusion in healthcare confirms that adoption is influenced by perceived relative advantage, compatibility with existing systems, complexity, trialability, and observability—all of which are modifiable through deliberate curriculum design and institutional strategy. The theory also clarifies why resource-constrained settings often preferentially adopt efficiency-enhancing innovations: relative advantage in operational efficiency provides a compelling adoption rationale that is particularly salient in LMICs where physician-to-patient ratios are chronically low.
Technology Acceptance Model
The Technology Acceptance Model,15 developed by Davis in 1989, provides complementary insights into the human factors determining whether individuals accept and use new technologies. TAM has been extensively validated in medical education contexts, with a recent systematic review identifying 39 studies applying the model to evaluate technology acceptance among medical students and educators between 2010 and 2023.22 TAM posits that adoption is primarily determined by perceived usefulness (the degree to which a person believes using the technology will enhance performance) and perceived ease of use (the degree to which a person believes using the technology will be effortless), with both factors shaping attitudes and behavioural intentions. Extended TAM models incorporate social influence and organisational support as additional determinants.
Recent applications of TAM to AI in medical education demonstrate its predictive validity. A 2024 study of Chinese medical students found high willingness to use large language models in learning, with attitudes playing crucial mediating roles between perceived usefulness, ease of use, and behavioural intentions. TAM emphasises that technology provision alone is insufficient; successful adoption requires attending to human factors, peer influence, organisational commitment, and systematic barriers—dimensions that are frequently poorly addressed in LMIC implementation contexts.
Kirkpatrick’s Four-Level Evaluation Model
Kirkpatrick’s Model16 provides a hierarchical framework for evaluating educational programme effectiveness across four levels: Level 1 (Reaction)—participants’ satisfaction and engagement; Level 2 (Learning)—knowledge and skill acquisition; Level 3 (Behaviour)—application of learning in real-world practice; and Level 4 (Results)—long-term outcomes and organisational impact. Applied to AI curriculum development, this model establishes that the ultimate measures of success are not student satisfaction or examination performance but behavioural change in clinical practice and measurable improvements in patient and system outcomes—objectives achievable only through sustained, systematically evaluated implementation.
The model’s emphasis on higher-level outcomes reinforces a central argument of this review: delays in AI integration represent not merely knowledge gaps but missed opportunities to develop competencies that translate into improved clinical performance and better patient outcomes. Medical schools focusing exclusively on Levels 1 and 2 (reaction and learning) without progressing to Level 3 (behavioural application) and Level 4 (outcome measurement) risk implementing superficial AI education that fails to achieve meaningful impact.30
The Cost of Delay: A Structured Critical Counterargument Analysis
The Case for Delay: Strongest Counterarguments
Intellectual rigour demands that we engage seriously with the strongest arguments in favour of delaying AI integration into medical education. These arguments fall into four categories:
First, the ethical unpreparedness argument: AI systems are embedded with algorithmic biases, trained on non-representative data, and deployed within inadequate regulatory frameworks. Introducing students to these tools before robust ethical frameworks are established risks normalising harmful practices and producing graduates ill-equipped to identify or challenge AI-mediated harm—particularly consequential in settings where patient populations are most vulnerable to technology-encoded discrimination.
Second, the resource allocation argument: in settings where basic medical education infrastructure remains incomplete—where simulation laboratories, digital libraries, and reliable internet are still aspirational—investing limited resources in AI integration may represent a misalignment of priorities. The opportunity cost of AI curriculum development may be borne by more immediately needed educational investments.
Third, the faculty unpreparedness argument: educating students in AI competencies requires faculty who themselves possess those competencies. Where faculty lack AI expertise, student education may be superficial, inaccurate, or counterproductive. Rushing implementation before faculty capacity is established may do more harm than good.
Fourth, the evidence base argument: robust empirical evidence from LMIC medical school contexts demonstrating the effectiveness, cost-efficiency, and safety of AI integration in medical education is limited. Proceeding without a sufficient evidence base risks implementing ineffective programmes that waste scarce resources and potentially harm student development.
Rebuttal: Why These Arguments Support Structured Integration, Not Delay
Each of these arguments, upon analysis, provides a rationale for how to integrate AI rather than whether to integrate it. The ethical unpreparedness argument demonstrates why ethical reasoning, bias recognition, and regulatory critique should be core components of AI curricula—not why students should be shielded from AI. Exposure without education is already occurring through informal channels;5,6 structured education replaces unguided exposure with critical understanding. The resource allocation argument fails to account for the long-term resource costs of workforce unpreparedness: healthcare systems unable to deploy AI tools due to a literacy-deficient workforce will bear substantially greater costs in missed efficiency gains, diagnostic errors, and competitive disadvantage than those invested in foundational AI education.
The faculty unpreparedness argument misidentifies the bottleneck: it argues not for delay but for immediate investment in faculty development, which itself requires implementation to begin. Faculty develop AI expertise through teaching AI; the tacit knowledge required to effectively educate students about AI limitations, ethical deployment, and contextual appropriateness emerges from practice, not from prior preparation.5 And regarding the evidence base: the limited evidence from LMIC contexts is precisely the condition that integration is needed to remedy. As Kirkpatrick’s Model makes clear, evidence is generated through systematic implementation and evaluation—it cannot precede implementation. Early-adopting institutions are generating this evidence now; delayed adopters will eventually implement programmes without the benefit of contextualised evidence, facing a steeper disadvantage than those who began iterating early.
Diffusion of Innovations Theory offers the definitive framing: delay does not protect against the risks of innovation; it compounds the disadvantages of late adoption while doing nothing to resolve the underlying problems. The healthcare AI transformation is already underway. Graduates entering practice will encounter AI systems regardless of their educational preparation. The question is whether they will encounter these systems equipped with the knowledge, critical thinking, and ethical frameworks to use them responsibly, or whether they will encounter them unprepared—a condition that carries substantially greater patient safety risks than structured, phased educational integration.
The Compounding Costs of Inaction
McKinsey data indicate that 85% of healthcare leaders from payers, health systems, and healthcare services and technology groups were exploring or had already adopted generative AI capabilities as of Q4 2024.31 Each cohort of medical graduates without formal AI education enters practice increasingly misaligned with this clinical reality, and the gap widens with each graduating class. For African medical schools specifically, delays compound existing disadvantages: diffusion research demonstrates that resource-constrained settings often become late adopters, missing opportunities to shape innovation trajectories and forced eventually to adopt models designed for entirely different contexts.
At the individual level, TAM research demonstrates that students without educational exposure to AI develop negative attitudes based on fear, uncertainty, or misinformation—attitudes that create persistent barriers to effective technology use even when formal training is eventually provided. Early integration, by contrast, builds positive attitudes during formative professional development when students are most receptive to new learning paradigms. The social influence mechanisms described in both TAM and Diffusion of Innovations Theory amplify this effect: as AI literacy becomes normalised within healthcare, students without training become isolated from the professional networks where such literacy is expected.
At the system level, Kirkpatrick’s Level 4 outcomes highlight that delays in educational integration translate directly into delays in healthcare system capacity development. Healthcare systems require AI-literate professionals to implement beneficial technologies, provide feedback for system improvement, identify appropriate clinical applications, and develop contextually relevant innovations. Without this workforce capacity, healthcare systems cannot realise the potential benefits from technological investments—creating economic inefficiencies, missed care improvement opportunities, and widening global health disparities.
A Framework for Contextually Appropriate Integration
Acknowledging both the urgency of AI integration and the legitimate concerns surrounding it, we propose a theoretically grounded, contextually adapted framework for medical schools in African and LMIC settings, synthesised in Table 2.
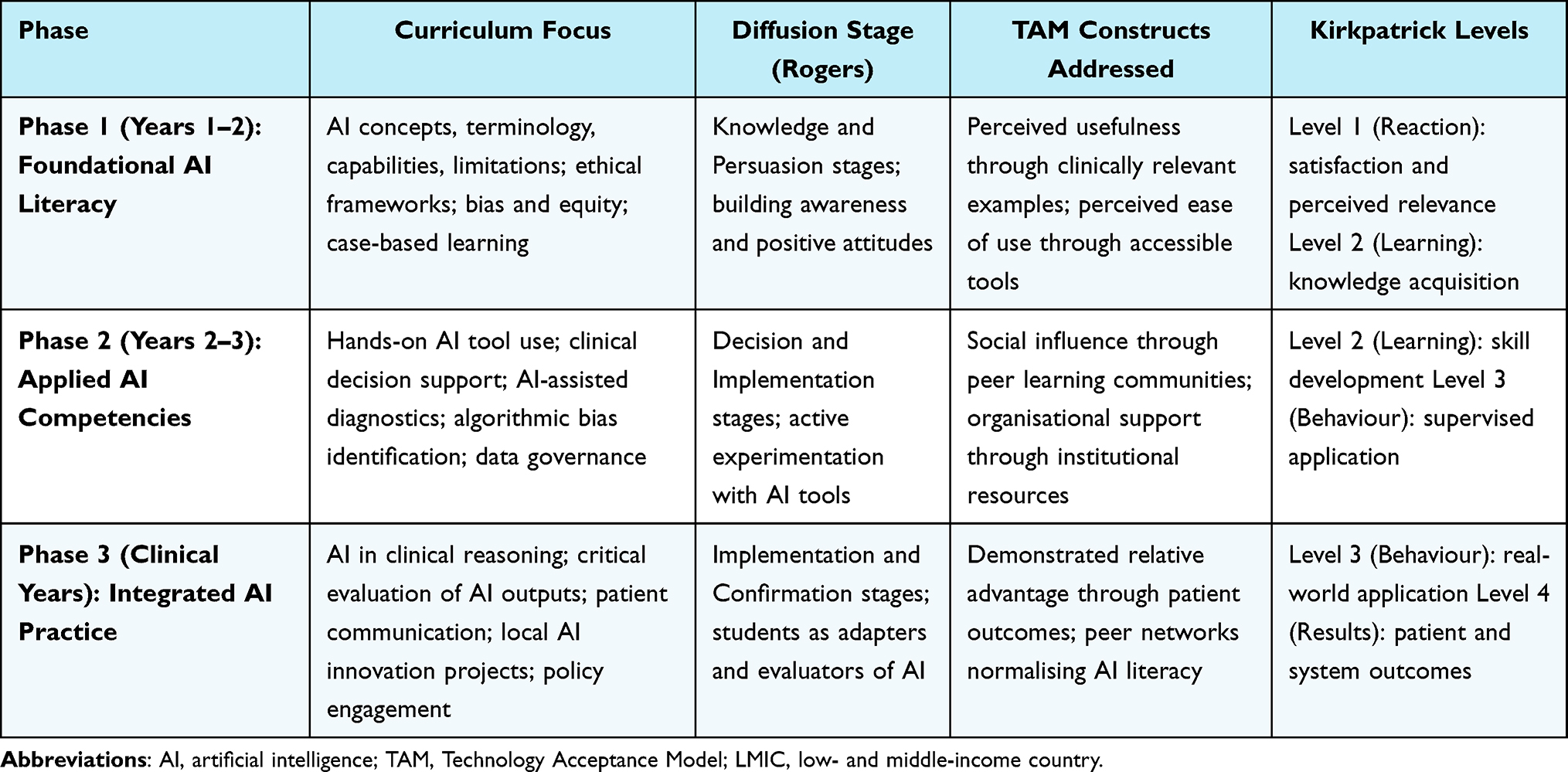 |
Table 2 Proposed Phased Framework for AI Integration in Medical Education in LMIC Settings |
Phased Implementation Strategy Based on Diffusion Stages
Rather than attempting comprehensive curriculum overhaul—an approach likely to fail under resource constraints—medical schools should adopt phased integration approaches aligned with Rogers’ innovation-decision stages (Table 2). Initial phases address the knowledge and persuasion stages by introducing foundational AI literacy: basic concepts, terminology, capabilities, limitations, and ethical frameworks. This phase corresponds to Kirkpatrick Levels 1 and 2, focusing on building awareness, positive attitudes, and foundational knowledge.
Subsequent phases engage the decision and implementation stages through TAM constructs: demonstrating perceived usefulness via clinically relevant applications, ensuring perceived ease of use through hands-on experiences with accessible AI tools, building positive attitudes through success experiences and peer influence, and addressing perceived risks through transparent ethical discussions and safety frameworks. A phased integration strategy—starting with foundational literacy during preclinical education and advancing toward complex applications in clinical training—offers a practical and sustainable pathway, as demonstrated by a recently published model from a US medical school that integrated AI literacy across all four years of training using connectivism and constructivist principles.3
Advanced phases focus on implementation and confirmation stages, corresponding to Kirkpatrick Levels 3 and 4: students apply AI in supervised clinical contexts, receive feedback on appropriate and inappropriate use, contribute to local AI adaptation and innovation, and participate in evaluating patient and system outcomes.
Faculty Development Aligned with TAM Principles
Training educators in AI usage is essential for effective integration.5,32 Faculty development must address both TAM constructs and pedagogical adaptations required for AI-enhanced teaching. Practically, this means demonstrating how AI enhances teaching effectiveness (perceived usefulness), providing user-friendly tools and adequate technical support (perceived ease of use), building faculty self-efficacy through graduated training experiences, creating peer learning communities leveraging social influence mechanisms, and securing institutional commitment that signals organisational priority. Faculty development should extend beyond technical training to encompass ethical frameworks, pedagogical strategies for AI-enhanced learning, assessment approaches maintaining academic integrity, and evaluation methods aligned with Kirkpatrick’s Model.
From a diffusion perspective, faculty represent crucial opinion leaders whose adoption patterns powerfully influence institutional trajectories. Investing in faculty development creates internal champions who accelerate broader adoption through social influence, model appropriate AI use for students, and contribute to implementation refinement through experiential feedback. South-South collaboration offers particular promise in this regard: a medical school in Nigeria might partner with institutions in India, Brazil, or Rwanda that have implemented AI curricula in similar resource contexts, sharing lessons, materials, and faculty expertise.
Context-Appropriate Curricula for African Settings
Curriculum development in African medical schools must account for local contexts, resources, healthcare priorities, and epistemological traditions rather than simply adopting frameworks developed in high-income countries. Context-appropriate curricula should address AI applications for infectious disease surveillance common in African epidemiological profiles, resource allocation optimisation in constrained healthcare systems, community health worker support in rural and remote areas, and diagnostic assistance where specialist availability is critically limited. Crucially, curricula must address the specific challenges of algorithmic bias in African populations, data privacy in contexts with weak regulatory frameworks, appropriate use of AI where basic diagnostics may be unavailable,33 and the integration of AI with traditional healing practices—a dimension rarely addressed in Western AI curricula but essential for cultural acceptability and patient-centred care in many African settings.
As one set of commentators argued, debates that dominate AI discussions in high-income contexts (such as the replacement of physicians by AI) must be contextualised when much of Africa still struggles with basic healthcare delivery infrastructure.27 Medical students in these settings require frameworks that address contextual realities rather than idealised high-resource environments.
Ethical Education and the Decolonial Imperative
AI literacy must extend far beyond technical competence to encompass critical evaluation skills and robust ethical reasoning. Students must learn to question algorithmic outputs, recognise potential biases, understand system limitations, and appreciate appropriate versus inappropriate applications across different clinical and social contexts. Ethical education should specifically address multiple dimensions relevant to African settings: bias and fairness in algorithms trained on non-representative datasets; privacy and data governance in settings with weak regulatory protections; transparency and explainability when patient populations may have limited technological literacy; accountability and responsibility when errors occur; patient autonomy and informed consent within family-centred and communal decision-making norms; and equitable access to AI-enhanced healthcare.
Medical education provides an opportunity to operationalise calls for decolonising AI by positioning African institutions as co-creators rather than consumers of AI technologies, developing locally relevant applications addressing African health priorities, and establishing ethical frameworks grounded in African values—ubuntu (interconnectedness and communal responsibility), respect for elder knowledge and traditional healing, and holistic approaches to health—rather than simply importing Western bioethical principles.27,29
Collaborative Partnerships and Resource Sharing
African medical schools should pursue collaborative partnerships to overcome resource constraints and accelerate curriculum development. These partnerships should include equitable North-South arrangements that prioritise capacity building over dependency; South-South collaborations sharing experiences among institutions facing similar challenges; engagement with technology companies under frameworks supporting local capacity rather than commercial dependency; and participation in open educational resource initiatives that reduce development costs through shared infrastructure. The African Union’s Continental AI Strategy provides a governance framework emphasising African leadership in AI development and deployment;29 medical education partnerships should align with this framework, ensuring that African institutions maintain meaningful control over educational priorities and approaches rather than becoming implementation sites for externally designed programmes.
Addressing Specific LMIC Constraints Through Theoretical Lenses
Infrastructure limitations reduce perceived ease of use in TAM terms, but not all AI education requires sophisticated infrastructure.34 Many foundational concepts can be taught using case-based learning, simulations running on standard computers, or cloud-based platforms accessible through mobile devices. Given Africa’s growing smartphone penetration—with mobile internet access expanding rapidly across all regions—mobile-first AI education strategies may represent the most appropriate and sustainable entry point.10 For faculty expertise gaps, diffusion theory emphasises the importance of interpersonal communication channels: remote experts can contribute through virtual workshops, online mentorship programmes, and collaborative teaching arrangements. Junior faculty members or graduate students with technology backgrounds may serve as peer educators, creating bidirectional learning that addresses expertise limitations while building institutional capacity.
Financial constraints need not prevent implementation when strategically managed. Open educational resources, freely available AI tools (including some large language models and open-source image recognition platforms), and collaborative curriculum development models can substantially reduce costs. Diffusion research confirms that relative advantage strongly influences adoption rates: institutions should emphasise and communicate the cost-effectiveness of AI educational approaches that demonstrate clear improvements over traditional methods—such as AI-powered virtual patients that provide more consistent, scalable clinical reasoning practice than traditional standardised patient programmes at lower per-student cost.35
Comprehensive Evaluation Using Kirkpatrick’s Model
Systematic evaluation across all four Kirkpatrick levels should be embedded from the first moment of implementation, not added retrospectively.36 Level 1 (Reaction) evaluation assesses student and faculty satisfaction, engagement with materials, perceived relevance, and attitudes toward AI technologies. For African contexts, Level 1 evaluation should specifically assess perceived cultural appropriateness, relevance to local healthcare challenges, and accessibility under existing infrastructure constraints.
Level 2 (Learning) evaluation measures knowledge gains about AI concepts and capabilities, understanding of limitations and appropriate applications (particularly in resource-limited settings), competencies in using AI tools including mobile and low-bandwidth applications, abilities to interpret and critically evaluate AI outputs (recognising bias and inappropriate recommendations), and ethical reasoning regarding AI use in African healthcare contexts.
Level 3 (Behaviour) evaluation examines whether learning translates into clinical practice by observing students’ application of AI knowledge during clinical rotations, assessing the quality of their clinical reasoning when integrating AI tools, evaluating their critical analysis of AI recommendations, documenting their patient communication regarding AI-assisted care, and tracking their contributions to identifying locally appropriate AI applications. This level addresses the fundamental question of whether education produces meaningful behavioural change rather than merely satisfactory examination performance.
Level 4 (Results) evaluation investigates long-term outcomes including graduate preparedness for AI-enhanced practice in African healthcare settings, patient care quality and safety indicators, healthcare system efficiency metrics, contributions to AI innovation and contextual adaptation, impacts on health equity and access, and influence on policy and regulatory framework development.37 While Level 4 outcomes require extended timeframes to manifest, establishing measurement frameworks from inception enables longitudinal tracking that will generate the contextualised evidence base currently lacking for LMIC settings.
Policy Implications and Recommendations
For Medical Schools
Medical schools should: (1) establish AI education as an institutional priority with dedicated resources and accountability structures; (2) begin with foundational curricula immediately, even if advanced programmes require additional development time; (3) invest in faculty development as the critical enabler of effective student education; (4) develop context-appropriate curricula addressing local healthcare priorities and challenges; (5) engage students as partners in curriculum development and local AI innovation; (6) implement comprehensive evaluation frameworks from inception across all Kirkpatrick levels; and (7) form strategic partnerships that support capacity building while maintaining institutional autonomy.
For Ministries of Health and Education
Government stakeholders should: (1) develop national AI-in-health strategies that include workforce development and medical education components; (2) establish regulatory and ethical frameworks for AI in healthcare, engaging medical educators in their development; (3) invest in digital health infrastructure supporting both clinical implementation and educational needs; (4) create incentives for medical schools to implement AI curricula and evaluate outcomes; (5) support South-South collaboration and knowledge sharing; and (6) ensure that AI integration advances rather than undermines health equity goals.
For International Organisations and Funders
International stakeholders should: (1) provide financial and technical support for AI curriculum development in African medical schools; (2) facilitate partnerships that build local capacity rather than creating dependency; (3) support development of open educational resources appropriate for African contexts; (4) fund rigorous research on effective AI integration strategies in resource-limited settings; (5) recognise and amplify African innovation in AI and medical education; and (6) support ethical framework development grounded in African values and contexts.
For Regional Bodies (African Union, ECOWAS, EAC, SADC)
Regional bodies should: (1) harmonise approaches to AI regulation and medical education standards across member states; (2) facilitate regional collaborations and resource sharing; (3) advocate for African leadership in global AI governance discussions; (4) support development of Africa-specific AI applications addressing regional health priorities; and (5) monitor and actively address intra- and inter-country digital divides.
Limitations
This narrative review has several limitations warranting acknowledgement. As a narrative rather than systematic review, literature selection involved subjective judgement that may introduce selection bias, despite our deliberate application of SANRA criteria and a structured critical counterargument approach to mitigate this risk. We may have missed relevant publications, particularly grey literature and non-English language publications from African contexts. The rapidly evolving nature of AI means that some findings may become outdated quickly; the literature search was completed in May 2026; evidence published subsequently has not been incorporated.
Much of the literature on AI in medical education continues to originate from high-income countries, limiting direct applicability to African contexts and requiring inference from related settings. The theoretical frameworks employed, while extensively validated and widely applied, were developed primarily in Western contexts; further theoretical development grounded in African educational philosophies and epistemologies is needed to fully capture adoption dynamics in these settings. Additionally, our analysis focuses primarily on undergraduate medical education, with less attention to postgraduate training, continuing professional development, and non-physician health professions education—all of which also require urgent AI integration.
Conclusions
This review synthesises evidence on AI integration in medical education across LMICs, with primary contextual focus on sub-Saharan Africa, and finds that the theoretical, empirical, and contextual case for structured, phased integration is stronger than the case for delay—though this conclusion must be held with appropriate epistemic caution given the limited volume of LMIC-origin primary evidence. The three theoretical frameworks applied converge on a consistent set of implications: Rogers’ Diffusion of Innovations Theory highlights that early adoption enables local shaping of implementation and avoids compounding disadvantage; the Technology Acceptance Model identifies the conditions—perceived usefulness, ease of use, institutional support—that must be addressed for integration to succeed; and Kirkpatrick’s model establishes that only sustained, evaluated implementation generates the outcome evidence that LMIC-appropriate curricula require.
The counterarguments examined—ethical unpreparedness, resource constraints, faculty deficits, and a limited LMIC-specific evidence base—are substantive concerns that should shape how integration is pursued rather than serve as grounds for inaction. They argue for structured, phased, iterative approaches with embedded evaluation from the outset, not for indefinite delay. The unique contribution of this review lies in its explicit, framework-guided engagement with these counterarguments alongside a contextually grounded synthesis for African and LMIC medical schools—institutions that must navigate both the urgency of the global AI transition and the realities of resource-constrained implementation.
For medical schools across LMICs, and African institutions in particular, the most productive framing is not whether to engage with AI education but how to do so in contextually appropriate, iterative, and locally evaluated ways. Infrastructure deficits, data scarcity, and regulatory gaps are real constraints; so too are the opportunities offered by large patient populations, expanding mobile connectivity, and growing local data science capacity. A phased approach—beginning with AI literacy, progressing to applied clinical competencies, and ultimately to integrated practice and governance—offers a pathway that is both responsive to global developments and grounded in local realities. Context-specific research and evaluation from LMIC settings remain a critical priority to build the evidence base that will guide future iterations of this work.
Abbreviations
AI, Artificial Intelligence; ECOWAS, Economic Community of West African States; EAC, East African Community; FDA, United States Food and Drug Administration; IFMSA, International Federation of Medical Students’ Associations; LLM, Large Language Model; LMIC, Low- and Middle-Income Country; SADC, Southern African Development Community; SANRA, Scale for the Assessment of Narrative Review Articles; SSA, Sub-Saharan Africa; TAM, Technology Acceptance Model; UME, Undergraduate Medical Education; WEIRD, Western, Educated, Industrialised, Rich, and Democratic; WHO, World Health Organization.
Data Sharing Statement
This is a narrative review; all synthesized data are available in the published sources cited in the reference list.
Ethics Approval and Consent to Participate
This narrative review did not involve human participants, animal subjects, or identifiable personal data.
Author Contributions
The author made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; has agreed on the journal to which the article has been submitted; and agrees to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The author declares no competing interests in this work.
References
1. Chen M, Decary M. Artificial intelligence in healthcare: an essential guide for health leaders. Healthc Manag Forum. 2020;33(1):10–15. doi:10.1177/0840470419873123
2. Gordon M, Daniel M, Ajiboye A, et al. A scoping review of artificial intelligence in medical education: BEME Guide No. 84. Med Teach. 2024;46(4):446–470. doi:10.1080/0142159X.2023.2285073
3. Diab M, Rao S, Krishnan A, et al. Integrating AI literacy into medical education: preparing future clinicians for an AI-driven healthcare system. Med Sci Educ. 2026:1–6. doi:10.1007/s40670-025-02599-y
4. Albert HT. 2 in 3 physicians are using health AI—up 78% from 2023. American Medical Association. 2024. Available from: https://www.ama-assn.org.
5. Pohn B, Mehnen L, Fitzek S, Choi K-E, Braun RJ, Hatamikia S. Integrating artificial intelligence into pre-clinical medical education: challenges, opportunities, and recommendations. Front Educ. 2025;10:1570389. doi:10.3389/feduc.2025.1570389
6. International Federation of Medical Students’ Associations (IFMSA). The use of artificial intelligence in medical practice and research. IFMSA; 2024. Available from: https://ifmsa.org.
7. Arawi T, El Bachour J, El Khansa T. The fourth industrial revolution: its impact on artificial intelligence and medicine in developing countries. Asian Bioeth Rev. 2024;16(3):513–526. doi:10.1007/s41649-024-00284-7
8. Sukhera J, Martin L, Lingard L. Geographic and thematic trends in medical education research: an analysis of 10 years of publications. Acad Med. 2024;99(3):245–252.
9. Barku GM, Ahmed T, Mensah JK. Challenges and prospects of medical AI integration in sub-Saharan Africa: a systematic review. Afr Health Sci. 2024;24(2):112–128.
10. Wahl B, Cossy-Gantner A, Germann S, Schwalbe NR. Artificial intelligence (AI) and global health: how can AI contribute to health in resource-poor settings? BMJ Glob Health. 2018;3(4):e000798. doi:10.1136/bmjgh-2018-000798
11. Akbarialiabad H, Sadeghian N, Haghighat S, et al. How can artificial intelligence transform the training of medical students and physicians? Lancet Digit Health. 2025;7(10). doi:10.1016/S2589-7500(25)00082-2
12. Muoka CJ, Adegoke AA, Okonkwo NP. Knowledge and attitudes toward artificial intelligence among medical students in Nigeria: a cross-sectional study. Niger J Clin Pract. 2025;28(1):67–74.
13. Bathaee Y, Khichar S, Sadeghian N. Medical and paramedical students’ perspectives on artificial intelligence in a low- and middle-income country: a cross-sectional study. Health Sci Rep. 2025;8:e0001234.
14. Rogers EM. Diffusion of Innovations. New York: Free Press; 1962.
15. Davis FD. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989;13(3):319–340. doi:10.2307/249008
16. Kirkpatrick DL. Evaluating Training Programs: The Four Levels. San Francisco: Berrett-Koehler; 1994.
17. Baethge C, Goldbeck-Wood S, Mertens S. SANRA—a scale for the quality assessment of narrative review articles. Res Integr Peer Rev. 2019;4(1):5. doi:10.1186/s41073-019-0064-8
18. Sriram A, Ramachandran K, Krishnamoorthy S. Integrating artificial intelligence into medical education: a narrative systematic review of current applications, challenges, and future directions. BMC Med Educ. 2025;25(1):744. doi:10.1186/s12909-025-07744-0
19. Castellano MS, Contreras-McKay I, Neyem A, et al. Mapping the use of artificial intelligence in medical education: a scoping review. BMC Med Educ. 2025;25(1):526. doi:10.1186/s12909-025-07089-8
20. Andigema L, Mwangi E, Kariuki J. Diabetic retinopathy screening using AI in East Africa: a pilot study. Afr J Health Sci. 2024;17(3):245–256.
21. Ndembi A, Okoro F, Kamau M. Scaling AI solutions in African healthcare: success stories from five countries. J Glob Health Inform. 2024;3(2):89–104.
22. Lee JWY, Tan JY, Bello F. Technology acceptance model in medical education: systematic review. JMIR Med Educ. 2025;11:e67873. doi:10.2196/67873
23. Al Zahrani EM, Elsafi SH, Al Musallam LD, et al. Faculty perspectives on artificial intelligence’s adoption in the health sciences education: a multicentre survey. Front Med. 2025;12:1663741. doi:10.3389/fmed.2025.1663741
24. Zhui L, Fenghe L, Xuehu W, Qining F, Wei R. Ethical considerations and fundamental principles of large language models in medical education: viewpoint. J Med Internet Res. 2024;26(1):e60083. doi:10.2196/60083
25. Park HA. Are we ready for the fourth industrial revolution? IMIA Yearb Med Inform. 2016;10(1):1–3.
26. PATH. Designing equitable large language models for global health. Seattle: PATH; 2024.
27. Think Global Health. AI must be decolonised to be useful in Africa. Council on Foreign Relations; 2024. Available from: https://www.thinkglobalhealth.org.
28. Weiner EB, Dankwa-Mullan I, Nelson WA, Hassanpour S. Ethical challenges and evolving strategies in the integration of artificial intelligence into clinical practice. PLOS Digit Health. 2025;4(4):e0000810. doi:10.1371/journal.pdig.0000810
29. African Union. Continental artificial intelligence strategy. Addis Ababa: African Union Commission; 2024.
30. Weidener L, Fischer M. Proposing a principle-based approach for teaching AI ethics in medical education. JMIR Med Educ. 2024;10:e55368. doi:10.2196/55368
31. Appinventiv. Why AI in medical education needs a 2026 strategy. 2024. Available from: https://appinventiv.com/blog/ai-in-medical-education/.
32. Blanco MA, Nelson SW, Ramesh S, et al. Integrating artificial intelligence into medical education: a roadmap informed by a survey of faculty and students. Med Educ Online. 2025;30(1):2531177. doi:10.1080/10872981.2025.2531177
33. Ciecierski-Holmes T, Singh R, Axt M, Brenner S, Barteit S. Artificial intelligence for strengthening healthcare systems in low- and middle-income countries: a systematic scoping review. Npj Digit Med. 2022;5(1):162. doi:10.1038/s41746-022-00700-y
34. Ahmed MA, Ng AHC, Mohammed A, Samsami K. Artificial intelligence in African healthcare: opportunities, challenges, and pathways forward. BMC Med Ethics. 2025;26(1):15. doi:10.1186/s12910-025-01015-w
35. Zaidi SSB, Adnan U, Lewis KO, Fatima SS. Metaverse-powered basic sciences medical education: bridging the gaps for lower middle-income countries. Med Teach. 2024;46(7):985–992. doi:10.1080/0142159X.2024.2354789
36. Masters K, Salcedo D. A checklist for reporting, reading and evaluating artificial intelligence technology enhanced learning (AITEL) research in medical education. Med Teach. 2024;46(9):1175–1179. doi:10.1080/0142159X.2023.2298756
37. Akbarialiabad H, Sadeghian N, Haghighat S, et al. The utility of generative AI in advancing global health. NEJM AI. 2025;2(3):AIp2400875. doi:10.1056/AIp2400875
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Emerging Therapies in Hemophilia: Improving Equitable Access to Care
Lewandowska M, Nasr S, Shapiro AD
Journal of Blood Medicine 2025, 16:95-115
Published Date: 20 February 2025
Application of Artificial Intelligence Generated Content in Medical Examinations
Li R, Wu T
Advances in Medical Education and Practice 2025, 16:331-339
Published Date: 25 February 2025
Detection Rate of Diabetic Retinopathy Before and After Implementation of Autonomous AI-based Fundus Photograph Analysis in a Resource-Limited Area in Belize
Esmaeilkhanian H, Gutierrez KG, Myung D, Fisher AC
Clinical Ophthalmology 2025, 19:993-1006
Published Date: 21 March 2025
Delving into the Practical Applications and Pitfalls of Large Language Models in Medical Education: Narrative Review
Li R, Wu T
Advances in Medical Education and Practice 2025, 16:625-636
Published Date: 18 April 2025
The AI Health Arms Race: A Critical Perspective on Big Tech and the Widening Global Health Equity Gap
Ahmed MM, Othman ZK
Journal of Multidisciplinary Healthcare 2026, 19:610208
Published Date: 21 April 2026