Back to Journals » Clinical Epidemiology » Volume 15
Initiation of Medical Therapy for Heart Failure Patients According to Kidney Function: A Danish Nationwide Study
Authors Zahir Anjum D, Strange JE, Fosbøl E, Garred CH, Malik ME, Andersson C, Jhund PS ![]() , McMurray JJV, Petrie MC, Kober L
, McMurray JJV, Petrie MC, Kober L ![]() , Schou M
, Schou M
Received 30 March 2023
Accepted for publication 9 June 2023
Published 19 July 2023 Volume 2023:15 Pages 855—866
DOI https://doi.org/10.2147/CLEP.S412787
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lars Pedersen
Deewa Zahir Anjum,1 Jarl Emanuel Strange,1 Emil Fosbøl,2 Caroline Hartwell Garred,1 Mariam Elmegaard Malik,1 Charlotte Andersson,1,3 Pardeep S Jhund,4 John J V McMurray,4 Mark C Petrie,4 Lars Kober,2,5 Morten Schou1,5
1Department of Cardiology, Copenhagen University Hospital, Hellerup, Denmark; 2Department of Cardiology, Rigshospitalet, Copenhagen University Hospital, Copenhagen, Denmark; 3Cardiovascular Division, Brigham and Women’s Hospital, Boston, MA, USA; 4BHF Cardiovascular Research Centre, University of Glasgow, Glasgow, UK; 5Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark
Correspondence: Deewa Zahir Anjum, Department of Cardiology, Copenhagen University Hospital Herlev and Gentofte, Gentofte Hospitalsvej 8., 3.sal, Hellerup, 2900, Denmark, Tel +45 22951918, Email [email protected]
Background: Use of medical therapies for heart failure (HF) patients with moderate kidney dysfunction is low. We hypothesized that lack of initiation of HF therapy reflects the clinicians’ reluctance in very elderly and frail patients more than kidney dysfunction itself.
Methods: HF patients were identified from nationwide registers between 2014 and 2021. Information was obtained on eGFR, frailty status, and prescription of HF therapy. Patients were divided into three groups: normal kidney function (eGFR ≥ 60); moderate kidney dysfunction (GFR between 30 and 59); and severe kidney dysfunction (GFR < 30). Multivariate Cox models were used to study the association of eGFR, age, and frailty with use of HF therapy.
Results: Of the 42,320 HF patients included those with lower eGFR were significantly older and frailer (median age 74.3 years and 37.8% frail). The crude initiation rate of all three drug classes decreased with decreasing eGFR in a stepwise fashion. After adjusting for age and frailty status, initiation of MRA decreased with decreasing kidney function (moderate kidney function HR 0.80(95% CI 0.77– 0.84) and severe kidney function HR 0.24(0.21– 0.27)). After adjusting for age and frailty status, initiation of RAS inhibitor and BB was not significantly lower for moderate kidney dysfunction (HR 0.97(0.93– 1.02), and HR 1.06(0.97– 1.16, respectively)). Initiation of RAS inhibitor was significantly lower for patients with severe kidney dysfunction, HR 0.45(0.41– 0.50), but not for BB initiation HR 1.09(1.05– 1.14).
Conclusion: In a real-world HF cohort, patients with moderate and severe kidney dysfunction were associated with reduced use of MRA irrespective of age and frailty. Reduced use of RASi was associated with severe kidney dysfunction, whereas for patients with moderate kidney dysfunction, reduced use was mainly driven by aging and frailty. Reduced use of BB seemed to be primarily explained by aging and frailty.
Keywords: heart failure, epidemiology, chronic kidney disease, guideline-directed medical therapy, real-world data
Introduction
The management of patients with heart failure (HF) in the presence of kidney dysfunction is complex. The frequent coexistence of these two conditions often results in a poorer prognosis,1 and patients with heart failure and kidney dysfunction tend to be older, frailer, and have a greater number of comorbidities compared to those without kidney dysfunction.2–4 In addition, when kidney dysfunction is present, as indicated by an estimated glomerular filtration rate (eGFR) of less than 60 mL/min/1.73 m2, there is a tendency to underutilize HF therapy, resulting in a risk-treatment paradox. This means that patients who have a higher risk of mortality are actually treated with fewer disease-modifying medical therapies.5 As patients with HF and coexisting kidney dysfunction, older age, and frailty are considered a high-risk group, it is especially crucial to optimize HF therapy in this population.
While non-use of certain HF therapy in patients with HF with an eGFR<30 mL/min/1.73 m2 may be appropriate, this is not the case for use of HF therapy in patients with eGFR between 30 and 59 mL/min/1.73 m2.6 The reason for the undertreatment of HF therapy in patients with HF and eGFR between 30 and 59 mL/min/1.73 m2 is less clear. Although this may reflect concern about kidney dysfunction per se, low eGFR is often inextricably linked to advanced age and frailty and it may be these associated problems that lead to undertreatment.
Therefore, in this real-world cohort study of patients with HF across the entire spectrum of eGFR, we evaluated the association of eGFR at baseline on the initiation of renin-angiotensin-system (RAS) inhibitors, mineralocorticoid receptor antagonists (MRA) and betablockers (BB) before and after adjustment for age and frailty status.
Methods
Data Sources
We obtained the data for this study from Danish nationwide registers, which include information on all Danish citizens through the unique personal number assigned to each individual in the Civil Registration Registry.7 Specifically, we utilized data from four national registries in Denmark: (i) The Danish National Patient Registry, which contains data on all hospital in- and outpatient contacts using the 10th edition of the International Classification of Diseases (ICD-10) codes,8 (ii) the National Prescription Registry, which contains information on all medical prescriptions filled at Danish pharmacies categorized by the Anatomical Therapeutic Chemical Classification System (ATC) codes,9 (iii) the Danish Registry on Regular Dialysis and Transplantation, which holds complete information on all Danish citizens undergoing chronic kidney replacement therapy,10 and (iv) the Register of Laboratory Results for Research, which stores laboratory test results from four out of the five administrative regions in Denmark.11
Study Population and Outcome
We included all patients aged 18 to 95 years with a first-time registered primary in-hospital or outpatient HF diagnosis between January 1, 2014, and December 31, 2021. Baseline was defined as the day of HF diagnosis, and patients were followed until the initiation of HF therapy, emigration, death, or end of study period (Supplemental Figure 1). Patients were included in the study if they had a creatinine plasma sample taken within 90 days prior to being diagnosed with HF. If more than one creatinine measurement was performed in this period, the most recent measurement prior to the HF diagnosis was selected. Patients were excluded if they died during initial admission. Patients who were receiving the therapy of interest were excluded from the analysis of each drug class. Patients were divided into three groups based on their measured kidney function at inclusion, 1) eGFR ≥60 mL/min/1.73 m2; 2) eGFR between 30 and 59 mL/min/1.73 m2; 3) eGFR <30 mL/min/1.73 m2), calculated with the 2021 CKD-EPI creatinine formula which has been shown to be superior to other estimations of kidney function.12
The primary outcome was the initiation of HF therapy, including RAS inhibitors, MRA, and BB. Details on HF medication and corresponding ATC-codes are provided in Supplemental Table 1. Angiotensin receptor neprilysin inhibitor (ARNi) were not included because the Danish HF guidelines require patients to have attempted RAS inhibitors prior to initiating ARNi.13 Additionally, sodium-glucose cotransporter-2 inhibitors were not included in the analysis as they were only recently introduced in Denmark on March 1, 2021.
Variables
To evaluate frailty, we utilized the Hospital Frailty Risk Score, which is an established method for identifying frailty risk based on ICD-10 diagnosis codes obtained from administrative health registers. We categorized patients into three groups based on their frailty risk score: low, intermediate, and high. The Hospital Frailty Risk Score has been demonstrated to be as effective as or better than other frailty or risk stratification tools.14 For more information on the selection and scoring of the frailty variable, please refer to Supplemental Table 2.
Comorbidities were identified from registered ICD-10 codes up to five years before inclusion (Supplemental Table 3). Concomitant medication at baseline was defined as at least one redeemed prescription up to 180 days before inclusion based on ATC codes (Supplemental Table 3). Plasma potassium, sodium, and haemoglobin were determined up to 90 days before inclusion. Anaemia was defined according to WHO criteria (7.7 mmol/l (13 g/dl) in men and 7.4 mmol/l (12 g/dl) in women)15 and hyponatraemia was defined as plasma sodium below 135 mmol/l.16
Statistics
Baseline descriptive data were presented as percentages for categorical variables and as medians with interquartile ranges (IQR) or means with standard deviation (SD) for continuous variables, as appropriate. The Pearson χ2 and Kruskal–Wallis tests were used to compare differences for categorical and continuous variables, respectively.
We estimated and compared the six-month rates of HF therapy initiation using cumulative incidence functions with the Aalen-Johansen estimator, accounting for the competing risk of all-cause mortality or censoring due to emigration or end-of-study. We employed four multivariable Cox proportional hazard models to evaluate the association between age and frailty on the relationship between kidney function and HF therapy initiation. Model 1 was unadjusted, model 2 adjusted for sex, diagnostic setting (inpatient vs outpatient), calendar year, concomitant comorbidity, pharmacotherapy, and age, model 3 adjusted for sex, diagnostic setting (inpatient vs outpatient), calendar year, concomitant comorbidity, pharmacotherapy, and frailty status, and model 4 was the fully adjusted model with both age and frailty status included. We tested the model assumptions, such as the linearity of continuous variables, proportional hazard assumption, and lack of clinically meaningful interactions, and found them to be valid.
Supplemental Analysis
We performed an additional analysis on a subgroup of patients with HF and reduced ejection fraction (HFrEF), as determined by a previously validated method.17 This analysis aimed to examine the cumulative incidence of the initiation of MRA treatment and identify factors associated with MRA use. Additionally, we investigated the impact of the baseline potassium level on the initiation of HF therapy in a supplemental analysis.
All data management and analyses were conducted using SAS, version 9.4 (SAS Institute, Cary, NC, USA), and R (R version 4.2.1, R Foundation for Statistical Computing). A two-sided p-value of <0.05 was considered statistically significant.
Ethics
In Denmark, retrospective register-based studies do not require ethical approval. The Danish Data Protection Agency approved our data access with the approval number P-2019-393.
Results
Of the 52,633 patients identified, 10,313 (19.6%) did not meet the inclusion criteria, leaving a final cohort of 42,320 patients with HF (Figure 1).
 |
Figure 1 Flowchart. Abbreviations: HF, heart failure; eGFR, estimated glomerular filtration rate. |
Study Demographics
The baseline characteristics of the study population for each eGFR subgroup are presented in Table 1. The median age was 74.3 years [IQR 57.4–91.2], and 26,208 patients (61.9%) were male. Mean eGFR was 66.8 mL/min/1.73 m2 (SD 34.6). At baseline, 32.4% of patients had an eGFR between 30 and 59 mL/min/1.73 m2 and 7.5% had an eGFR <30 mL/min/1.73 m2. Those with lower eGFR were significantly older and frailer. Lower eGFR was associated with male sex, outpatient diagnosis, and a higher use of beta-blockers, loop-diuretics, glucose-lowering drugs, and platelet inhibitors at baseline. Similarly, the prevalence of ischaemic heart disease, peripheral artery disease, and cancer was higher for patients with lower eGFR. Overall, the use of devices was very rare.
 |
Table 1 Baseline Characteristics of the Study Population at Time of HF Diagnosis Stratified According to eGFR at Baseline |
HF Therapy Initiation According to eGFR at Baseline
Figure 2 shows six-month initiation rates for HF therapy according to eGFR at baseline. For patients with no prior prescription of RAS inhibitor treatment, the initiation rate decreased with decreasing eGFR in a stepwise fashion (Figure 2a: 61.2% for patients with eGFR ≥60 mL/min/1.73 m2, 48.2% for patients with eGFR between 30 and 59 mL/min/1.73 m2 and 22.0% for patients with eGFR <30 mL/min/1.73 m2). A similar pattern of decrease in rates of MRA initiation by eGFR categories was noted (Figure 2b: 35.5% for patients with eGFR ≥60 mL/min/1.73 m2, 24.7% for patients with eGFR between 30 and 59 mL/min/1.73 m2 and 6.4% for patients with eGFR <30 mL/min/1.73 m2). Similarly, there was a graded, significant decrease in initiation rates of BB initiation by eGFR categories (Figure 2c: 60.6% for patients with eGFR ≥60 mL/min/1.73 m2, 51.6% for patients with eGFR between 30 and 59 mL/min/1.73 m2 and 40.7% for patients with eGFR <30 mL/min/1.73 m2).
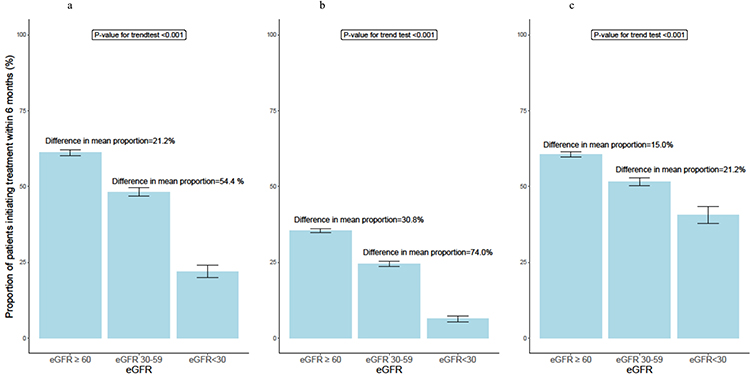 |
Figure 2 Six-month initiation rates of HF therapy treatment according to eGFR at baseline. (a) RAS inhibitor treatment. (b) MRA treatment. (c) BB treatment. |
Frailty Status and Age
To examine the impact of frailty and age on the likelihood of initiating HF therapy, we carried out four Cox regression models (Figure 3). After adjusting for age and frailty, the association between eGFR and RAS inhibitor initiation only remained significant for patients with eGFR <30 mL/min/1.73 m2 (hazard ratio (HR) 0.45; 95% CI 0.41–0.50, P < 0.001, Figure 3a). For MRA initiation, the association was significant for both patient groups with eGFR between 30 and 59 mL/min/1.73 m2 (HR 0.80; 95% CI 0.77–0.84, P < 0.001) and eGFR <30 mL/min/1.73 m2 (HR: 0.24; 95% CI 0.21–0.27, P < 0.001, Figure 3b). For BB initiation, after adjusting for age and frailty there was a slightly higher rate of initiation for patients with eGFR between 30 and 59 mL/min/1.73 m2 (HR 1.09; 95% CI 1.05–1.14, P < 0.001), whereas the association for patients with eGFR <30 mL/min/1.73 m2 was not significant (HR 1.06, 95% CI 0.97–1.16, P = 0.186, Figure 3c). Table 2 shows the corresponding hazard ratios (HR) for the fully adjusted model for the initiation of HF therapy. The analysis conducted on a subgroup of patients with HFrEF yielded comparable findings for the MRA treatment (Supplemental Figure 2). Furthermore, a higher baseline potassium level was found to be associated with lower rates of initiating all three classes of HF therapy, with the most notable impact observed for MRA and RAS inhibitors (Supplemental Figure 3).
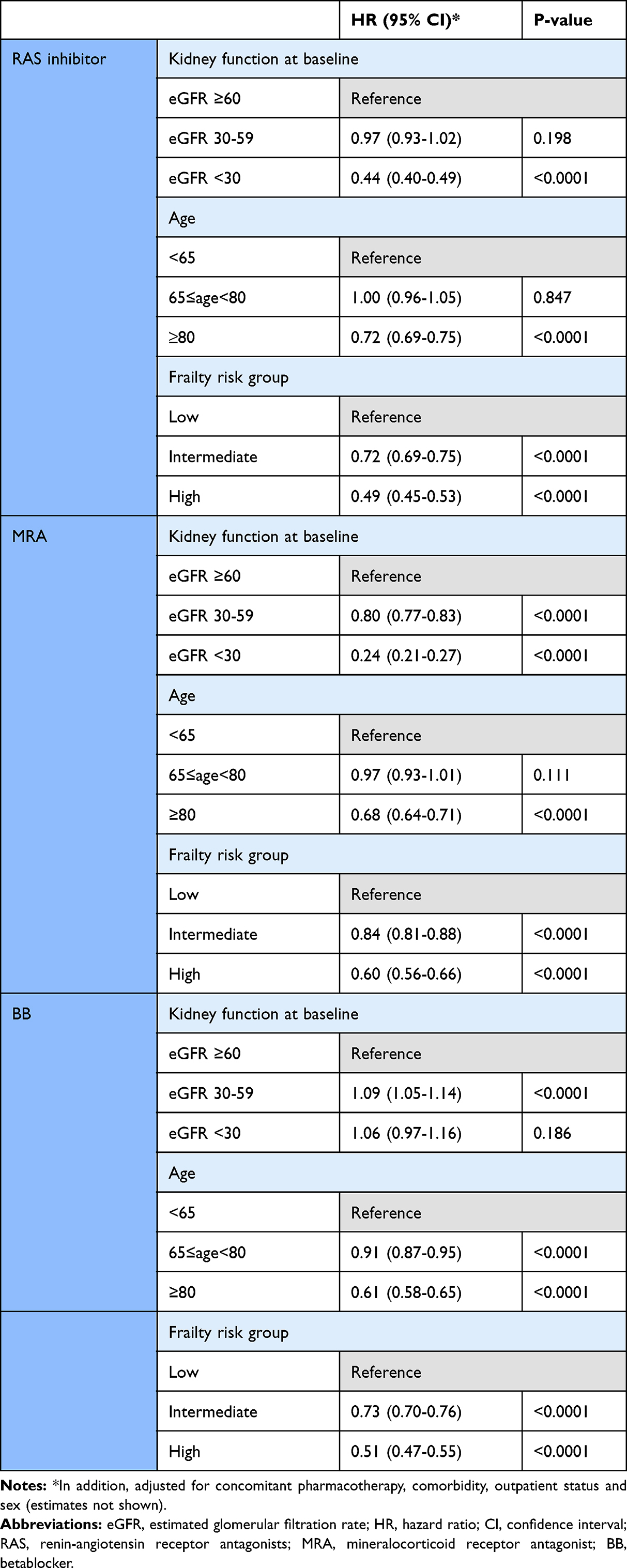 |
Table 2 Multivariate adjusted Hazard Ratios and 95 % Confidence Interval for HF therapy initiation |
 |
Figure 3 Cox proportional hazards models for HF therapy initiation according to eGFR at baseline. (a) RAS inhibitor treatment. (b) MRA treatment. (c) BB treatment. Notes: Model 1: Unadjusted model. Model 2: Adjusted for sex, diagnostic setting, calendar year, concomitant comorbidity, plasma potassium, pharmacotherapy, and age. Model 3: Adjusted for sex, diagnostic setting, concomitant comorbidity, plasma potassium, pharmacotherapy, and frailty status. Model 4: Fully adjusted model, adjusted for sex, diagnostic setting, concomitant comorbidity, plasma potassium, pharmacotherapy, age, and frailty status. |
Discussion
Main Findings
In a real-world HF cohort encompassing the entire spectrum of eGFR, we found that patients with moderate and severe kidney dysfunction were associated with reduced use of MRA irrespective of age and frailty. The reduced use of RASi displayed a combination of factors, where severe kidney dysfunction was associated with lack of initiation, while for patients with moderate kidney dysfunction, lack of initiation was mainly driven by aging and frailty. The reduced use of BB conversely seemed to be explained by aging and frailty more than kidney function per se. Barriers to prescription of HF therapy should not be eGFR between 30 and 59 mL/min/1.73 m2, or advanced age and frailty. Outcomes for these patients could be improved with appropriate education about the safety and efficacy of HF therapy in older and frailer individuals with moderate kidney dysfunction.
Frequency of Advanced Aging and Frailty Status According to eGFR
Among patients with HF, the prevalence of kidney dysfunction as defined by eGFR <60 mL/min/1.73 m2 is high. We found that 39.9% of HF patients had kidney dysfunction at the time of HF diagnosis. The prevalence of CKD in HF patients varies depending on the severity of HF and the criteria used to define CKD. Data on HF patients admitted for acute HF including both new onset and worsening HF have shown a higher burden of kidney dysfunction of 60–65%.5 Our data are the first, to our knowledge, from both an in- and outpatient HF cohort. In this real-world population of incident HF patients, the proportion of individuals above 80 years was substantial, especially among patients with eGFR <60 mL/min/1.73 m2 where approximately 50% of the patients were above 80 years of age. This proportion is higher than reported in large HF trials. In addition to older age, decreasing eGFR was associated with a higher prevalence of greater frailty. This is in accordance with the SGTL2 inhibitor trials DELIVER18 and DAPA-HF.19
Initiation of HF Therapy
In the present study, we showed that HF patients with severe kidney dysfunction (eGFR < 30 mL/min/1.73 m2) had a significantly lower initiation rate of all three classes of HF therapy. These findings are in accordance with the CHAMP-HF registry, where kidney dysfunction was associated with lower HF therapy utilization in outpatient setting.20 This is particularly concerning given the high-risk nature of combined kidney dysfunction and HF. Pivotal HF RCTs have previously excluded patients with severe kidney dysfunction,21–23 leading to limited information on the safety and efficacy of commonly used HF therapies in this patient group. Therefore, recommendations for patients with severe kidney dysfunction must be extrapolated from subgroup analyses. Recent trials with novel HF drug classes have included patients with eGFR from 15–29 mL/min/1.73 m2.24–26 MRA is recommended for HF patients with eGFR≥30 mL/min/1.73 m2 according to both American and European guidelines for HF.27,28 However, there are no similar contraindications for BB,29 and RAS inhibitors can be cautiously initiated at lower dosage and with more intensive monitoring. The guidelines recommend 1A level of recommendation for the three classes of HF therapy for HFrEF patients but not for HFmrEF and HFpEF patients. It is crucial to acknowledge that not all patients in our study met the criteria for HF therapy, which is a notable limitation. Nevertheless, subgroup analyses involving HFrEF patients yielded comparable findings. It is worth mentioning that the evolving trend in HF treatment is moving towards considering all patients with heart failure, EF for appropriate interventions and therapies.
The lack of initiation of BB and RAS inhibitors in this patient group may reflect clinicians’ reluctance to extrapolate the results from RCTs to daily clinical practice. Specifically, there may be concerns about the risk of developing hyperkalemia, which is particularly pronounced in patients with CKD, especially for the use of MRA and RAS inhibitors. Our data suggests that moderately elevated baseline potassium levels, which are not considered a contraindication, are associated with lower rates of initiation for all three classes of HF therapy, with the most significant impact observed for MRA and RAS inhibitors. In light of the poor prognosis of this high-risk population, it is important to treat eligible patients with available HF therapy and to target further RCTs on developing novel, safe, and effective treatments for HF patients with concomitant severe kidney dysfunction as well as include patients with severe kidney dysfunction in RCTs with existing therapies.
For HF patients with moderate kidney dysfunction (eGFR 30–59 mL/min/1.73 m2), where there is a clear guideline indication for treatment and ample evidence on the efficacy and safety,6 the suboptimal use of RAS inhibitors and BB with decreasing kidney function was driven largely by advanced age and worse frailty status. Whether this observation reflects treatment inertia in elderly and frail patients with kidney dysfunction or a focus on treatment of quality of life and symptoms with diuretics instead of initiation of disease-modifying therapies cannot be deduced from our results. Age-related changes in renal function can lead to reduced eGFR, but this does not necessarily imply that older patients are unable to tolerate HF therapy.30 In fact, older patients with HF are often in need of effective management to improve their outcomes. Frailty should also not be a barrier to the prescription of HF therapy. While frailty can increase the risk of adverse events,31 the benefits of HF therapy in improving patient outcomes in frail patients have been well-established.18,19,32
For MRA, we observed that moderate kidney dysfunction was associated with a lack of initiation of MRA even after adjustment for age and frailty status. Lack of initiation of MRA is, therefore closer associated with moderate kidney dysfunction than for RAS inhibitors and BB, and this lack of initiation of MRA is not guideline-based as the evidence of efficacy and safety of MRA for patients with moderate kidney dysfunction is well-established.33 This is in accordance with previous studies that have suggested that physicians are overly cautious about moderately reduced kidney function.34
Methodical Considerations
The major strength of this study is that it included a large population of HF patients in Danish national registries both out- and inpatient diagnostic setting and had minimal loss-to-follow-up. We examined HF patients across the entire spectrum of eGFR using the creatinine-based CKD-EPI formula to estimate eGFR, which is more accurate than the MDRD (Modification of Diet in Renal Disease) equation for eGFR estimation used by previous studies.35
There are some limitations to be acknowledged. First, the major limitation is inherent in the observational design of the study, which limits causal inference based on the observed differences. Secondly, only baseline levels of creatinine were considered. Due to the repeated measurements of creatinine in HF patients, it can be difficult to determine which one should be included in the analyses. However, we mitigated this issue by prespecifying the creatinine measurement taken just before the HF diagnosis limiting the knowledge of the effect on kidney function after initiation of HF therapy. Third, the study population consisted of HF patients with reduced, mid-range, and preserved ejection fraction, and the lack of data on LVEF can influence the results as patients with preserved ejection fraction are more likely frail and elder. The study lacked data on clinical and lifestyle parameters such as blood pressure including hypotension, NT-proBNP, albuminuria, smoking, socioeconomic status, and body composition which may have resulted in residual and unmeasured confounding which may have affected the strength of association between advanced kidney dysfunction and the different outcomes. Especially hypotension in elderly patients can presumably explain some part of the lack of initiation of HF therapy. Lastly, we used the Hospital Frailty Risk Score to define frailty.14 This is a risk score, which relies solely on a patients’ medical history rather than also incorporating clinical measurements.
Clinical Perspectives
In this study, we observe that 8% of newly diagnosed HF patients have severe kidney dysfunction at the time of diagnosis and these patients rarely are initiated in RAS inhibitors and MRAs. Furthermore, 32% of HF patients have moderate kidney dysfunction, where lack of initiation of RAS inhibitors and BB in this patient group seem to be explained by advanced age and severe frailty status in contrast to lack of initiation of MRA that seem to be explained by kidney dysfunction. Focus on the optimal care and future RCTSs of these high-risk patients with kidney dysfunction, advanced age and frailty is needed. It may be appropriate to prioritize improving quality of life as a treatment goal for some patients, while focusing on preventing the progression of HF in others. Barriers to prescription of HF therapy should not be moderate kidney dysfunction, or advanced age and frailty.
Conclusion
Despite increasing focus on the optimization of HF therapy, we found that HF patients with moderate and severe kidney dysfunction was associated with reduced use of MRA irrespective of age and frailty. Further, reduced use of RASi was associated with severe kidney dysfunction, while for patients with moderate kidney dysfunction, reduced use was mainly driven by aging and frailty. Reduced use of BB seemed to be explained by aging and frailty more than kidney function per se.
Abbreviations
HF, Heart failure; eGFR, Estimated glomerular filtration rate; LVEF, Left ventricular ejection fraction; ICD-10, International Classification of Diseases, Tenth Revision; RAS, Renin-angiotensin-system; BB, Beta-blocker; MRA, Mineralocorticoid receptor antagonist; ARNi, Angiotensin receptor neprilysin inhibitor; SGLT2, Sodium-glucose cotransporter-2; RCT, Randomized clinical trials.
Disclosure
Professor Pardeep S Jhund reports grants, Speakers fees, Advisory board fees, and work on clinical trials from AstraZeneca, Speakers fees, Advisory board fees, and work on clinical trials from Novartis, grants from Analog Devices, Advisory Board fees from Boehringer Ingelheim, Work on clinical trials from NovoNordisk, Work on clinical trials from Bayer AG, outside the submitted work; and Director GCTP Ltd. Professor John J V McMurray reports My employer, Glasgow University, has been paid by AstraZeneca (who market dapagliflozin) for my time spent as principal/co-principal investigator of the DAPA-HF, DELIVER, DETERMINE trials and DAPA-Resist trial with dapagliflozin in heart failure and Steering Committee member for the DAPA-CKD trial with dapagliflozin in chronic kidney disease. These payments were made through a Consultancy with Glasgow University and I have not received personal payments in relation to this trial/this drug. My employer, Glasgow University, has been paid by Amgen for my time spent as Steering Committee member for the ATOMIC-HF, COSMIC-HF and GALACTIC-HF trials and meetings and other activities related to these trials. Amgen has also paid my travel and accommodation for some of these meetings/activities. These payments were made through a Consultancy with Glasgow University and I have not received personal payments in relation to these trials/this drug. My employer, Glasgow University, has been paid by Bayer for my time spent as co-principal investigator of the FINEARTS trial with finerenone. These payments were made through a Consultancy with Glasgow University and I have not received personal payments in relation to these trials/drugs. My employer, Glasgow University, has been paid by Cardurion for my participation in a company advisory board about development in connection with drug development and design of clinical trials. My employer, Glasgow University, has been paid by Cytokinetics for my time spent as Steering Committee member for the GALACTIC-HF trial and meetings and other activities related to this trial. Cytokinetics has also paid my travel and accommodation for some of these meetings/activities. These payments were made through a Consultancy with Glasgow University and I have not received personal payments in relation to these trials/this drug. My employer, Glasgow University, has been paid by GSK for my time spent as Steering Committee member for two trials, ASCEND-D and ASCEND-ND, using daprodustat, and meetings related to these trials. GSK has also paid my travel and accommodation for some of these meetings. These payments were made through a Consultancy with Glasgow University and I have not received personal payments in relation to these trials/drugs. My employer, Glasgow University, has been paid by KBP Biosciences for my time spent scientific advisor to company to help guide clinical development in cardio-renal disease, inflammation & infection. My employer, Glasgow University, has been paid by Novartis for my time spent as co-principal investigator for the PARAGON-HF trial and Steering Committee member for PARADISE-MI, PERSPECTIVE and PARACHUTE-HF trials (all with sacubitril/valsartan) and meetings related to these trials. Novartis has also paid my travel and accommodation for some of these meetings. These payments were made through a Consultancy with Glasgow University and I have not received personal payments from Novartis in relation to these trials/drugs. Personal fees from Alnylam, personal fees from Bayer, personal fees from BMS, personal fees from Ionis Pharma., personal fees from Novartis, personal fees from Regeneron Pharma., personal fees from River 2 Renal Corp., personal fees from Abbott, personal fees from Alkem Metabolics, personal fees from Astra Zeneca, personal fees from Blue Ocean Scientific Solutions Ltd., personal fees from Boehringer Ingelheim, personal fees from Canadian Medical and Surgical Knowledge, personal fees from Emcure Pharmaceuticals Ltd., personal fees from Eris Lifesciences, personal fees from European Academy of CME, personal fees from Hikma Pharmaceuticals, personal fees from Imagica Health, personal fees from Intas Pharma., personal fees from J.B. Chemicals & Pharma., personal fees from Lupin Pharma., personal fees from Medscape/Heart.Org., personal fees from ProfAdWise Communications, personal fees from Radcliffe Cardiology, personal fees from Sun Pharma., personal fees from The Corpus, personal fees from Translation Research Group, personal fees from Translational Medicine Academy, outside the submitted work. Professor Mark C Petrie reports grants, personal fees from SQ Innovation, grants, personal fees from Astra Zeneca, grants, personal fees from Novo Nordisk, grants, personal fees from Boehringer Ingelheim, grants from Teikoku, grants, personal fees from Novartis, grants, personal fees from Pharmacosmos, grants, personal fees from Vifor, outside the submitted work. Professor Lars Kober reports personal fees from Speakers fee from AstraZeneca, Bayer, Boehringer and Novartis, outside the submitted work. Professor Morten Schou reports lecture fees from Novo, Bohringer, Astra, and Novartis during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Smith DH, Thorp ML, Gurwitz JH, et al. Chronic kidney disease and outcomes in heart failure with preserved versus reduced ejection fraction: the Cardiovascular Research Network PRESERVE study. Circ Cardiovasc Qual Outcomes. 2013;6:333–342. doi:10.1161/CIRCOUTCOMES.113.000221
2. Damman K, Valente MAE, Voors AA, et al. Renal impairment, worsening renal function, and outcome in patients with heart failure: an updated meta-analysis. Eur Heart J. 2014;35:455–469. doi:10.1093/eurheartj/eht386
3. McCullough PA, Amin A, Pantalone KM, Ronco C. Cardiorenal nexus: a review with focus on combined chronic heart and kidney failure, and insights from recent clinical trials. J Am Heart Assoc. 2022;11. doi:10.1161/JAHA.121.024139
4. Hillege HL, Nitsch D, Pfeffer MA, et al. Renal function as a predictor of outcome in a broad spectrum of patients with heart failure. Circulation. 2006;113:671–678. doi:10.1161/CIRCULATIONAHA.105.580506
5. Patel RB, Fonarow GC, Greene SJ, et al. Kidney function and outcomes in patients hospitalized with heart failure. J Am Coll Cardiol. 2021;78:330–343. doi:10.1016/j.jacc.2021.05.002
6. Beldhuis IE, Lam CSP, Testani JM, et al. Evidence-based medical therapy in patients with heart failure with reduced ejection fraction and chronic kidney disease. Circulation. 2022;145:693–712. doi:10.1161/CIRCULATIONAHA.121.052792
7. Pedersen CB. The Danish civil registration system. Scand J Public Health. 2011;39:22–25. doi:10.1177/1403494810387965
8. Lynge E, Sandegaard JL, Rebolj M. The Danish national patient register. Scand J Public Health. 2011;39:30–33. doi:10.1177/1403494811401482
9. Wallach Kildemoes H, Toft Sørensen H, Hallas J. The Danish national prescription registry. Scand J Public Health. 2011;39:38–41. doi:10.1177/1403494810394717
10. Hommel K, Rasmussen S, Madsen M, Kamper AL. The Danish Registry on regular dialysis and transplantation:completeness and validity of incident patient registration. Nephrol Dial Transplant. 2010;25:947–951. doi:10.1093/ndt/gfp571
11. Arendt JFH, Hansen AT, Ladefoged SA, et al. Existing data sources in clinical epidemiology: laboratory information system databases in Denmark. Clin Epidemiol. 2020;12:469–475. doi:10.2147/CLEP.S245060
12. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150:604–612. doi:10.7326/0003-4819-150-9-200905050-00006
13. Hjertesvigt D. Arbejdsgruppe for Kronisk hjertesvigt. Dansk Cardiol Selsk. 2014;3:15.
14. Gilbert T, Neuburger J, Kraindler J, et al. Development and validation of a Hospital Frailty Risk Score focusing on older people in acute care settings using electronic hospital records: an observational study. Lancet. 2018;391:1775–1782. doi:10.1016/S0140-6736(18)30668-8
15. Chan M; World Health Organization. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Geneva, Switzerland: World Health Organization; 2011:1–6. Available from: http://scholar.google.com/scholar?hl=en&btnG=Search&q=intitle:Haemoglobin+concentrations+for+the+diagnosis+of+anaemia+and+assessment+of+severity#1.
16. Biswas M, Davies JS. Hyponatraemia in clinical practice. Postgrad Med J. 2007;83:373–378. doi:10.1136/pgmj.2006.056515
17. Madelaire C, Gustafsson F, Køber L, et al. Identification of patients with new-onset heart failure and reduced ejection fraction in Danish administrative registers. Clin Epidemiol. 2020;12:589–594. doi:10.2147/CLEP.S251710
18. Butt JH, Jhund PS, Belohlávek J, et al. Efficacy and safety of dapagliflozin according to frailty in patients with heart failure: a prespecified analysis of the DELIVER trial. Circulation. 2022;146:1210–1224. doi:10.1161/CIRCULATIONAHA.122.061754
19. Butt JH, Dewan P, Merkely B, et al. Efficacy and safety of dapagliflozin according to frailty in heart failure with reduced ejection fraction A post hoc analysis of the DAPA-HF trial. Ann Intern Med. 2022;175:820–830. doi:10.7326/M21-4776
20. Greene SJ, Butler J, Albert NM, et al. Medical therapy for heart failure with reduced ejection fraction: the CHAMP-HF registry. J Am Coll Cardiol. 2018;72:351–366. doi:10.1016/j.jacc.2018.04.070
21. Pitt B, Remme W, Zannad F, et al. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med. 2003;348:1309–1321. doi:10.1056/NEJMoa030207
22. Zannad F, McMurray JJV, Krum H, et al. Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med. 2011;364:11–21. doi:10.1056/NEJMoa1009492
23. McMurray J, Solomon SD, Inzucchi SE, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381:1995–2008. doi:10.1056/NEJMoa1911303
24. Packer M, Anker SD, Butler J, et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med. 2020;383:1413–1424. doi:10.1056/NEJMoa2022190
25. Anker SD, Butler J, Filippatos G, et al. Empagliflozin in heart failure with a preserved ejection fraction. N Engl J Med. 2021;385:1451–1461. doi:10.1056/NEJMoa2107038
26. Solomon SD, McMurray JJV, Claggett B, et al. Dapagliflozin in heart failure with mildly reduced or preserved ejection fraction. N Engl J Med. 2022;387:1089–1098. doi:10.1056/NEJMoa2206286
27. Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145:E895–E1032. doi:10.1161/CIR.0000000000001063
28. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42:3599–3726. doi:10.1093/eurheartj/ehab368
29. Kotecha D, Gill SK, Flather MD, et al. Impact of renal impairment on beta-blocker efficacy in patients with heart failure. J Am Coll Cardiol. 2019;74:2893–2904. doi:10.1016/j.jacc.2019.09.059
30. Flather MD, Shibata MC, Coats AJS, et al. FASTTRACK Randomized trial to determine the effect of nebivolol on mortality and cardiovascular hospital admission in elderly patients with heart failure (SENIORS). Eur Heart J. 2005;26:215–225. doi:10.1093/eurheartj/ehi115
31. Khan MS, Segar MW, Usman MS, et al. Frailty, guideline-directed medical therapy, and outcomes in HFrEF: from the GUIDE-IT trial. JACC Hear Fail. 2022;10:266–275. doi:10.1016/j.jchf.2021.12.004
32. Butt JH, Dewan P, Jhund PS, et al. Sacubitril/valsartan and frailty in patients with heart failure and preserved ejection fraction. J Am Coll Cardiol. 2022;80:1130–1143. doi:10.1016/j.jacc.2022.06.037
33. Eschalier R, McMurray JJV, Swedberg K, et al. Safety and efficacy of eplerenone in patients at high risk for hyperkalemia and/or worsening renal function: analyses of the EMPHASIS-HF study subgroups (eplerenone in mild patients hospitalization and survival study in heart failure). J Am Coll Cardiol. 2013;62:1585–1593. doi:10.1016/j.jacc.2013.04.086
34. Jonsson A, Norberg H, Bergdahl E, Lindmark K. Obstacles to mineralocorticoid receptor antagonists in a community-based heart failure population. Cardiovasc Ther. 2018;36:e12459. doi:10.1111/1755-5922.12459
35. Matsushita K, Mahmoodi BK, Woodward M, et al. Comparison of risk prediction using the CKD-EPI equation and the MDRD study equation for estimated glomerular filtration rate. JAMA. 2012;307:1941–1951. doi:10.1001/jama.2012.3954
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Efficacy, Safety, Tolerability, and Real-World Data of Patiromer for the Treatment of Hyperkalemia
Colbert G, Sannapaneni S, Lerma EV
Drug, Healthcare and Patient Safety 2022, 14:87-96
Published Date: 14 July 2022
The DIAbetes MANagement and Treatment (DIAMANT) Cohort
Overbeek JA, Swart KMA, van der Pal EYM, Blom MT, Beulens JWJ, Nijpels G, Elders PJM, Herings RMC
Clinical Epidemiology 2022, 14:1453-1462
Published Date: 5 December 2022
Empagliflozin in Adults with Chronic Kidney Disease (CKD): Current Evidence and Place in Therapy
Colbert GB, Madariaga HM, Gaddy A, Elrggal ME, Lerma EV
Therapeutics and Clinical Risk Management 2023, 19:133-142
Published Date: 2 February 2023
Acute Cardiovascular Events After COVID-19 in England in 2020: A Self-Controlled Case Series Study

Davidson JA, Banerjee A, Strongman H, Herrett E, Smeeth L, Breuer J, Warren-Gash C
Clinical Epidemiology 2023, 15:911-921
Published Date: 1 September 2023
Underdiagnosis of COPD: The Japan COPD Real-World Data Epidemiological (CORE) Study
Koga Y, Deguchi S, Matsuo T, Suzuki A, Terashima G, Tajima T, Shibata Y, Sagara H
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:1011-1019
Published Date: 7 May 2024