Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Inhaled Corticosteroids in Patients with Chronic Obstructive Pulmonary Disease and Risk of Acquiring Streptococcus pneumoniae Infection. A Multiregional Epidemiological Study
Authors Heerfordt CK ![]() , Eklöf J, Sivapalan P, Ingebrigtsen TS, Biering-Sørensen T, Harboe ZB
, Eklöf J, Sivapalan P, Ingebrigtsen TS, Biering-Sørensen T, Harboe ZB ![]() , Koefod Petersen J, Andersen CØ, Boel JB
, Koefod Petersen J, Andersen CØ, Boel JB ![]() , Bock AK, Mathioudakis AG, Hurst JR
, Bock AK, Mathioudakis AG, Hurst JR ![]() , Kolekar S
, Kolekar S ![]() , Johansson SL, Bangsborg JM, Jarløv JO, Dessau RB
, Johansson SL, Bangsborg JM, Jarløv JO, Dessau RB ![]() , Laursen CB, Perch M, Jensen JUS
, Laursen CB, Perch M, Jensen JUS ![]()
Received 8 September 2022
Accepted for publication 2 February 2023
Published 21 March 2023 Volume 2023:18 Pages 373—384
DOI https://doi.org/10.2147/COPD.S386518
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Richard Russell
Christian Kjer Heerfordt,1 Josefin Eklöf,1 Pradeesh Sivapalan,1 Truls Sylvan Ingebrigtsen,1 Tor Biering-Sørensen,2– 4 Zitta Barrella Harboe,4,5 Jesper Koefod Petersen,6,7 Christian Østergaard Andersen,8 Jonas Bredtoft Boel,9 Anne Kathrine Bock,10 Alexander G Mathioudakis,11,12 John R Hurst,13 Shailesh Kolekar,7 Sofie Lock Johansson,14 Jette Marie Bangsborg,9 Jens Otto Jarløv,9 Ram Benny Dessau,15 Christian Borbjerg Laursen,14,16 Michael Perch,4,17 Jens-Ulrik Stæhr Jensen1,4,18
1Section of Respiratory Medicine, Department of Medicine, Copenhagen University Hospital Herlev and Gentofte Hospital, Hellerup, Denmark; 2Department of Cardiology, Herlev and Gentofte Hospital, Cardiovascular Non-Invasive Imaging Research Laboratory, University of Copenhagen, Copenhagen, Denmark; 3Faculty of Biomedical Sciences, Copenhagen University, Copenhagen, Denmark; 4Department of Clinical Medicine Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark; 5Department of Respiratory Medicine and Infectious Diseases, Copenhagen University Hospital, North Zealand, Denmark; 6Department of Respiratory Medicine, Zealand University Hospital Naestved, Naestved, Denmark; 7Department of Pulmonary Medicine, Zealand University Hospital, Roskilde, Denmark; 8Department of Clinical Microbiology, Hvidovre University Hospital, Hvidovre, Denmark; 9Department of Clinical Microbiology, Herlev and Gentofte Hospital, University of Copenhagen, Herlev, Denmark; 10Department of Respiratory Diseases and Allergy, Aarhus University Hospital, Aarhus, Denmark; 11The North West Lung Centre, Wythenshawe Hospital, Manchester University NHS Foundation Trust, Manchester, UK; 12Division of Infection, Immunity and Respiratory Medicine, School of Biological Sciences, The University of Manchester, Manchester Academic Health Science Centre, Manchester, UK; 13UCL Respiratory, University College London, London, UK; 14Department of Respiratory Medicine, Odense University Hospital, Odense, Denmark; 15Department of Clinical Microbiology, Zealand University Hospital, Slagelse Hospital, Slagelse, Denmark; 16Institute for Clinical Research, University of Southern Denmark, Odense, Denmark; 17Department of Cardiology, Section for Lung Transplantation, Rigshospitalet, Copenhagen, Denmark; 18PERSIMUNE & CHIP: Department of Infectious Diseases, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark
Correspondence: Christian Kjer Heerfordt, Section of Respiratory Medicine, Department of Medicine, Copenhagen University Hospital Herlev and Gentofte Hospital, Hellerup, Denmark, Tel +4523303431, Email [email protected]
Background: Inhaled corticosteroids (ICS) are associated with an increased risk of clinical pneumonia among patients with chronic obstructive pulmonary disease (COPD). It is unknown whether the risk of microbiologically verified pneumonia such as pneumococcal pneumonia is increased in ICS users.
Methods: The study population consists of all COPD patients followed in outpatient clinics in eastern Denmark during 2010– 2017. ICS use was categorized into four categories based on accumulated use. A Cox proportional hazard regression model was used adjusting for age, body mass index, sex, airflow limitation, use of oral corticosteroids, smoking, and year of cohort entry. A propensity score matched analysis was performed for sensitivity analyses.
Findings: A total of 21,438 patients were included. Five hundred and eighty-two (2.6%) patients acquired a positive lower airway tract sample with S. pneumoniae during follow-up. In the multivariable analysis ICS-use was associated with a dose-dependent risk of S. pneumoniae as follows: low ICS dose: HR 1.11, 95% CI 0.84 to 1.45, p = 0.5; moderate ICS dose: HR 1.47, 95% CI 1.13 to 1.90, p = 0.004; high ICS dose: HR 1.77, 95% CI 1.38 to 2.29, p < 0.0001, compared to no ICS use. Sensitivity analyses confirmed these results.
Interpretation: Use of ICS in patients with severe COPD was associated with an increased and dose-dependent risk of acquiring S. pneumoniae, but only for moderate and high dose. Caution should be taken when administering high dose of ICS to patients with COPD. Low dose of ICS seemed not to carry this risk.
Keywords: COPD, inhaled corticosteroids, Streptococcus pneumoniae, clinical epidemiology
Introduction
Chronic obstructive pulmonary disease (COPD) is often associated with an abnormal inflammatory response in the lungs.1 Inhaled corticosteroids (ICS) in different combinations with bronchodilators have in several randomized trials showed reduction in exacerbation risk.2–5 However, ICS appear to have minimal or no impact on decline of lung function6 and patients without eosinophilic inflammation may not benefit from such treatment.7 ICS treatment is known to confer increased risk of clinical pneumonia.8 Whilst ICS are first-line therapy for patients with asthma, the efficacy, safety and role of ICS in the management of patients with COPD is of a more complex nature and adverse effects may outweigh the benefits.6
Streptococcus pneumoniae (S. pneumoniae) is one of the most common causes of community acquired pneumonia. Lower respiratory tract infections due to S. pneumoniae are associated with significant morbidity and mortality worldwide, particularly among elderly, immunocompromised, and patients with COPD.9,10 The risk for pneumonia-related mortality is almost threefold higher when pneumonia is pneumococcal.10 Patients with chronic respiratory diseases have an increased risk of acquiring pneumococcal pneumonia (Rate ratio 3.7–9.8) and an increased risk of invasive pneumococcal disease (Rate ratio 2.5–7.7).9
Previously, the increased risk of pneumonia related to ICS usage has been investigated solely by clinical or radiological defined pneumonia. In this study, we used microbial samples from the lower airways which is a more specific method since clinical pneumonia can be caused by many pathogens, and may be purely inflammatory without microbiological cause. Furthermore, it is unknown whether ICS dosage affects the risk of specific pneumonia etiologies such as S. pneumoniae.
This study aimed to determine the risk of accruing a positive S. pneumoniae lower airway tract sample associated with dosages of ICS in COPD patients.
Methods
Study Design
This observational cohort study consisted of COPD patients with an outpatient clinic visit registered between January 2010 and February 2018. The first clinical visit was defined as study entry. Data on hospital admission, comorbidities, and medication were gathered from the previous year to cohort entry. Age, body mass index (BMI), Forced Expiratory Volume in the first second (FEV1), Medical Research Council dyspnea score (MRC), and smoking status were collected on study entry. If a value of a given variable on study entry was missing, the value was taken from the next clinical visit with a registered value leading to high data completeness. We followed the patients for one year or until the end of the study period (19th February 2018). Follow up ended if the patient had a positive S. pneumoniae lower airway tract sample or if the patient died. The primary outcome was a positive S. pneumoniae sample obtained from the lower part of the respiratory tract (ie, expectorate, tracheal secretion, or bronchial alveolar lavage). Samples are not routinely gathered from patients without signs of infection. Selection criteria are summarized in Figure 1. We excluded the following: (1) patients from the western regions of Denmark because of no access to microbiological data, (2) patients with a positive S. pneumoniae sample from the lower respiratory tract within the month prior to cohort entry, (3) patients receiving any disease-modifying antirheumatic drugs (Anatomical Therapeutic Chemical (ATC) codes:11 L04AX03, L01AA01, A07EC01, L04AD01, L04AA13, L04AX01, L04AA06, P01BA02) one year before cohort entry, and (5) patients with immunodeficiency (International Classification of Disease (ICD-10) codes: D80-85, D89) or malignant disease (ICD-10 codes: C00-C97) diagnosed within 5 years prior to cohort entry. ICD-10 codes are summarized in Supplementary Table 1. This study is written in accordance with STROBE guidelines. The protocol with an analysis plan was written before the data analysis and is available online on the COP:TRIN website.12
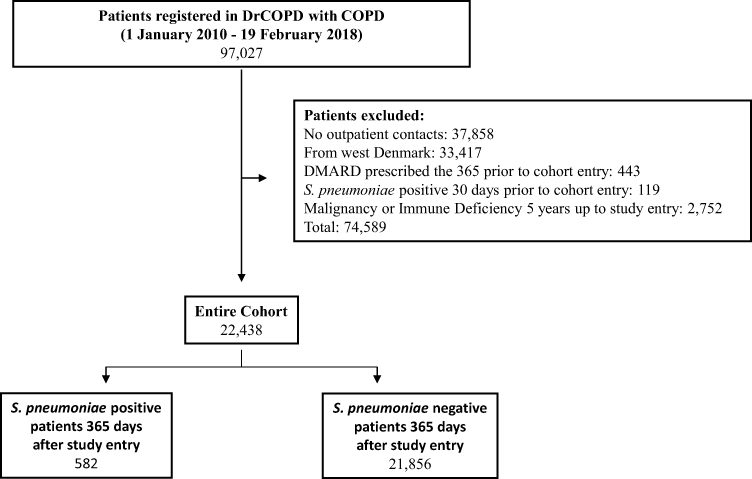 |
Figure 1 Selection criteria flowchart. The entire cohort consists of 22,438 patients, of which 582 acquired a positive S. pneumoniae from a lower airway tract sample during follow up period of 365 days. Abbreviations: DRCOPD, Danish Register of Chronic Obstructive Pulmonary Disease; DMARD, Disease Modifying Anti-Rheumatic Drugs; S. pneumoniae, Streptococcus pneumoniae. |
Source of Data
This study combined four different Danish national health databases. Access was granted in agreement with the Danish law on Data protection. The following 4 registers were used: The Danish Register of Chronic Obstructive Pulmonary Disease (DrCOPD) is a national register. DrCOPD comprises data on all patients with a diagnosis of COPD registered in Danish hospitals and around 90% complete datasets. The database allowed us to find COPD patients with outpatient clinic visits at pulmonologist, and provides data on age, BMI, pulmonary parameters, and smoking status.13 The Danish National Database of Reimbursed Prescriptions (DNDRP) holds information of all nationwide redeemed prescriptions since 2004. Drugs are registered after the Anatomical Therapeutic Chemical (ATC) classification.14 This database was used to collect information about ICS exposure, other inhalation medicine, and antibiotics. Microbiological data were supplied from the Clinical Microbiology Departments in Eastern Denmark (Region Zealand and the Capital Region) to retrieve patients with positive S. pneumoniae samples from lower respiratory tract samples. The Danish National Patient Registry (DNPR) contains data on hospital admissions and outpatient visits including information on registered comorbidities.15 The linking of databases is possible due to the Danish civil personal registry number, a 10-digit number unique for every Danish citizen.
ICS Exposure
Exposure to ICS was calculated as the accumulated budesonide equivalent dose using all ICS prescriptions reimbursed within 365 days prior to study entry. An accumulated dose was calculated, and the different ICS types were converted into budesonide-equivalent doses, mometasone and beclomethasone were considered equivalent to budesonide ciclesonide at 2.5:1, fluticasone propionate at 2:1, and fluticasone furoate at 10:1.,16 ICS-users were categorized into tertiles, low, moderate, and high ICS use based on accumulated budesonide-equivalent dose.
Statistical Analysis
The risk of obtaining a positive S. pneumoniae sample associated with ICS use was estimated by a Cox proportional hazard regression model. Death was censored. The model was adjusted for the following suspected confounders: GOLD stage17 (percentage of predicted FEV1; stage 1–4), BMI (class 1–5, class 2 used as reference), smoking status (active or not active. Never smokers were categorized as not active smokers due to the rarity of never smokers in the Danish COPD population), age (group 1–4 as shown in Table 1), sex (male or female), the accumulated dose of oral corticosteroid (OCS) used one year prior to study entry (no OCS, low or high use), and calendar year for study entry. Groups used in the Cox analysis are shown in Table 1. The model was checked for proportionality. Continuous variable used in the model met the linearity criteria for the Cox regression. Additionally, we conducted stratified Cox analyses for budesonide and fluticasone users, adjusting for the same variables as in the main analysis. The propensity matching was made based on the same covariates adjusted for in the Cox analysis using the Greedy-Match algorithm suggested by the Mayo Clinic.18 Patients exposed to low tertile and no ICS dose were matched with patients exposed to middle and high tertile of ICS equivalent accumulated dose in a one-to-one ratio. An unadjusted Cox proportional hazard regression was used to estimate the risk of S. pneumoniae in the propensity matched population.
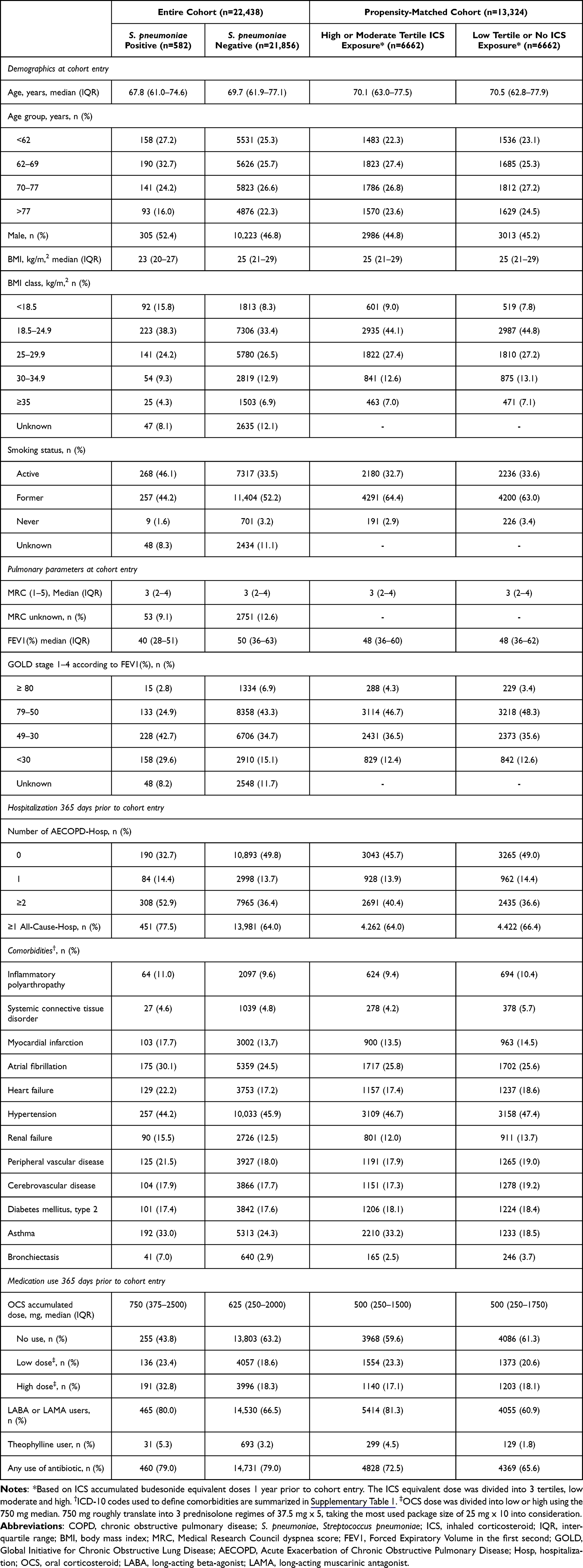 |
Table 1 Patient Characteristics for the Study Cohort Based on the Danish COPD Register (n = 22,438) According to Findings of S. pneumoniae Isolated from Lower Respiratory Tract Samples and the Propensity-Matched Cohort (n = 13,324). There Were No Significant Differences on the Matched Variables in the Propensity-Matched Cohort |
To address missing values for the Cox and the Propensity match these were replaced with the most common value for the given parameter to minimize attrition bias.
Results
We included 22,438 patients with COPD with a minimum of one outpatient visit (Figure 1). A total of 582 patients had a positive S. pneumoniae sample from the lower respiratory tract within 365 days after cohort entry. The study populations median age was 70 years, median BMI was 25 kg/m2, and the median FEV1% was 50%. Characteristics for patients with and without a positive S. pneumoniae sample and for the propensity matched cohort are reported in Table 1.
The average daily ICS equivalent dose for the entire cohort was 546 µg. Budesonide and fluticasone were the most frequently prescribed ICS. Characteristics of ICS usage are reported in Table 2.
 |
Table 2 Use of ICS the 365 Days Prior to Cohort Entry According to Findings of S. pneumoniae Isolated from Lower Respiratory Tract Samples |
The lowest tertile of ICS users did not have an increased risk of S. pneumoniae carriage in the adjusted analysis (HR 1.11, 95% CI 0.84–1.45, p=0.5), whereas the moderate (HR 1.47, 95% CI 1.13–1.90, p=0.004), and highest tertile (HR 1.77, 95% CI 1.38–2.29, p<0.0001) had a substantially higher risk as reported in Table 3. Figure 2 illustrates the cumulative incidence. In the propensity-matched sensitivity analysis, 6662 patients in subgroups were analyzed: (1) no or lower tertile of ICS users or (2) middle or highest subgroup of ICS users. No significant difference was found on the baseline characteristics we matched on. An unadjusted Cox was performed on the Propensity-matched cohort with similar results with a non-increased risk of S. pneumoniae in the group with lowest tertile (HR 1.24, 95% CI 0.90–1.70, p=0.2) of ICS users and increased risk in the moderate (HR 1.40, 95% CI 1.02–1.88, p=0.03) and the highest tertile (HR 1.75, 95% CI 1.30–2.36, p=0.0002) as reported in Table 3.
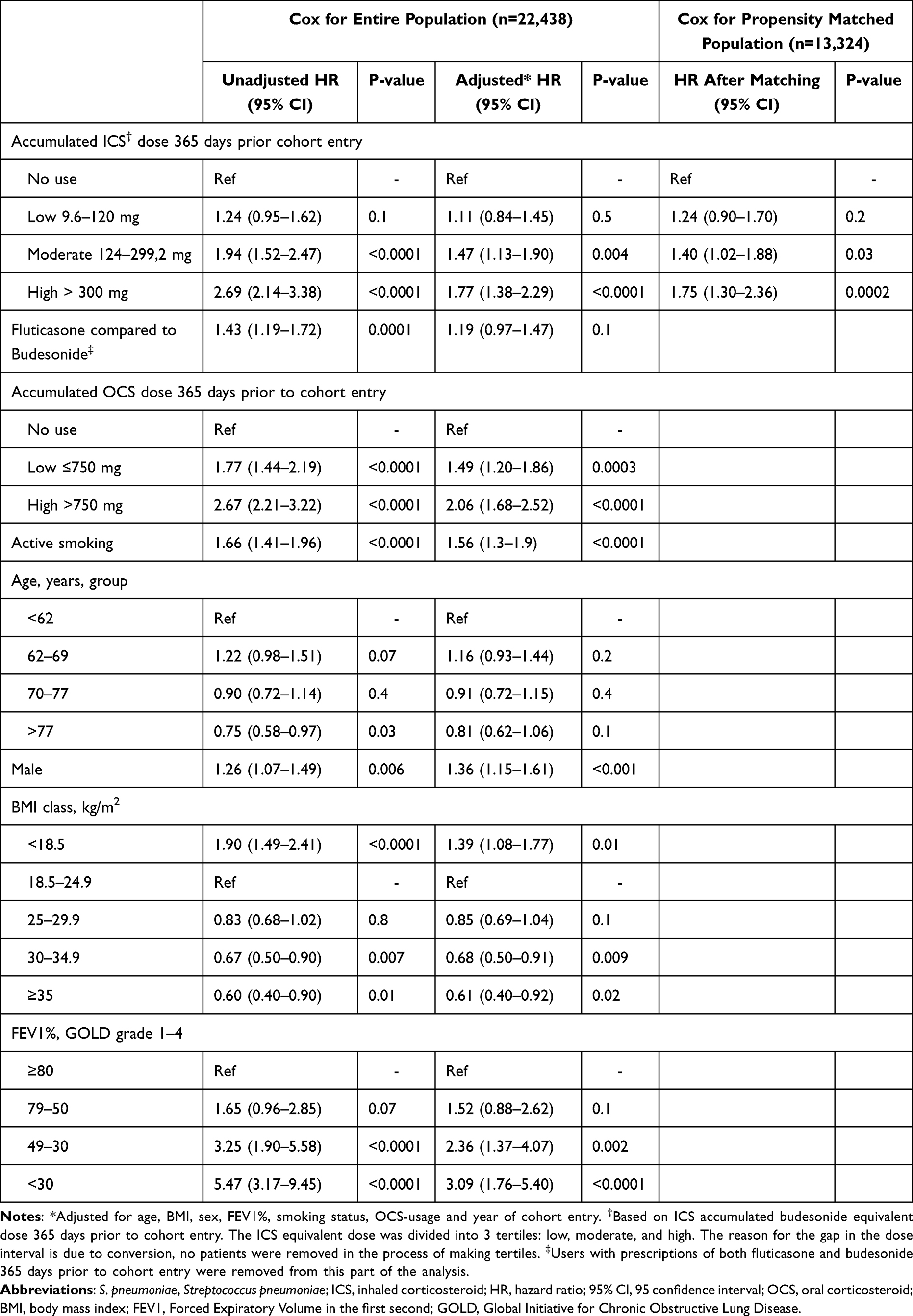 |
Table 3 Unadjusted and Adjusted* Cox-Regression Hazard Estimates for Risk of S. pneumoniae with Use of ICS in the Study Population (n = 22,438) and Propensity Score Matched Population (n = 13,324) |
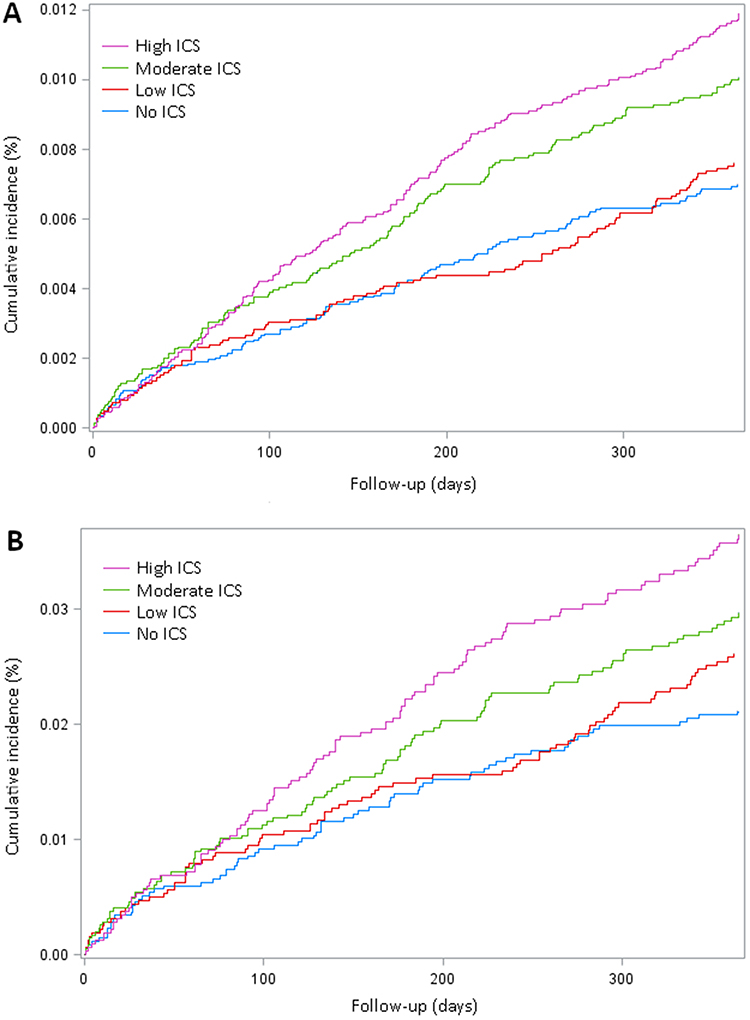 |
Figure 2 Cumulative incidence of S. pneumoniae positive lower airway tract sample according to ICS exposure divided into tertiles for the entire COPD cohort (n = 22,438) adjusted for age, BMI, sex, FEV1%, smoking status, OCS-usage and year of cohort entry (n = 22,438) (A) and for the propensity matched cohort (n = 13,324) (B). Abbreviations: S. pneumoniae, Streptococcus pneumoniae; ICS, inhaled corticosteroid; COPD, chronic obstructive pulmonary disease; BMI, body mass index; FEV1%, Forced Expiratory Volume in the first second; OCS, oral corticosteroid. |
In the follow-up period, a total of 16,446 lower respiratory tract samples were collected from 5060 patients. The three most common etiologies were Haemophilus influenzae (1081), Moraxella catarrhalis (672), and S. pneumoniae (668). Six thousand seven hundred (41.1%) tests were negative for any detectable pathogen.
Fluticasone compared to budesonide only had an increased risk of getting a positive S. pneumoniae lower airway tract sample in the unadjusted analysis as seen in Table 3. In the stratified analysis of patients receiving budesonide or fluticasone, we found no significant increased risk of acquiring a positive S. pneumoniae lower airway tract sample for patients receiving low ICS doses in either the budesonide group or the fluticasone group. However, there was a significant increased risk in the moderate and high ICS groups, see Table 4.
 |
Table 4 Adjusted* Cox-Regression Hazard Estimates for Risk of S. pneumoniae for Patients Treated with Low, Moderate and High ICS Compared to No Use, for Budesonide and Fluticasone Users |
We performed a number needed to harm analysis (NNH) on the propensity matched population. With one year follow up NNH in the high ICS tertile was 66 and in the moderate ICS tertile 121.
Discussion
In this large multiregional cohort study consisting patients with COPD followed in outpatient clinics, we showed that ICS use was associated with an increased risk of acquiring a positive S. pneumoniae lower respiratory airway sample. The cohort consisted of more than 20.000 patients. We found an increased risk of S. pneumoniae in the moderate and high tertile of ICS users but no increased risk in the low tertile of ICS users. Furthermore, high use of OCS, active smoking, low age, male gender, low FEV1%, and low BMI were associated with increased risk of S. pneumoniae, indicating these were relevant confounders in our model. This study was conducted on well-described population of patients diagnosed with COPD, which made it possible to adjust for multiple confounders. The degree of data completeness was high. DNDRP is nationwide and includes data on all reimbursed prescriptions redeemed at Danish community pharmacies since 2004. Microbiological data from the Clinical Microbiology Departments in Eastern Denmark (Region Zealand and Capital Region) consist of approximately 2.6 million inhabitants. DrCOPD had approximately 90% data completeness for variables such as FEV1%, MRC, BMI, and smoking status, see Table 1. The results were tested in a propensity-matched cohort with similar results. To improve the chance of ruling out a non-causal relationship, this study was designed with a chronological course with ICS usage 365 days prior to study entry and risk of S. pneumoniae up to 365 days post-study entry. The result is biologically plausible since corticosteroids are known to modify the innate and adaptive immune response leading to an increased risk of infections.19
Several studies have shown increased risk of clinical pneumonia as an adverse effect to ICS.8 This study used a more specific outcome of microbiology verified lower airway tract positive S. pneumoniae sample. Previously, only a few studies have investigated how ICS affect specific etiologies. ICS are known to give an increased risk of acquiring Mycobacteria and Pseudomonas aeruginosa infections.20–22 Other microbiological etiologies might also be affected by high ICS usage. This knowledge could be useful for the clinician but is currently unknown.
Limitations: ICS usage was calculated based on patient-collected prescriptions and not actual adherence. Thus, if a part of the patients were not adherent, this would cause a conservative bias leading to an underestimate of the risk. Due to the observational study design, it is not possible to prove a causality association due to possible residual confounding. Our data set did not provide information on pneumococcal vaccination status. If more severely ill COPD patients are more likely to receive a vaccine and also a higher dose of ICS, this could result in an underestimate of the association between ICS use and a positive S. pneumoniae sample, particularly for higher doses of ICS. Patients with a positive S. Pneumoniae lower airway tract sample 30 days prior to cohort entry were excluded. It is plausible that some of our defined cases of positive lower airway tract S. pneumoniae samples are due to colonization and not pneumonia. However, respiratory tract samples were not collected routinely, but when health care professionals observe indications of an infection, such as increased coughing, elevated infections markers, or changes a chest X-ray, according to Danish national COPD treatment guidelines.23 Although S. pneumoniae in few cases colonize airways in elderly adults without seeming infection, such carriage is also associated with invasive pneumococcal infection24 and is therefore also an unwanted outcome. Additionally, a longer exclusion timeframe would lead to a potential exclusion of patients reinfected rather than colonized with S. pneumoniae. The most frequently prescribed types of ICS were budesonide and fluticasone. Previous studies have shown an increased risk of pneumonia in fluticasone users compared with budesonide users.25 However, we only see a significantly increased risk of S. pneumoniae in the fluticasone users in the unadjusted analysis, see Table 3. Fluticasone users in our cohort received on average more than twice as much ICS in budesonide equivalent doses. Importantly, when adjusting for budesonide equivalent dose and disease severity, we did not observe an increased risk of S. pneumoniae in the fluticasone group compared to the budesonide group. Similarly, in the stratified analysis of budesonide and fluticasone users, we only found a significant increased risk of a positive S. pneumoniae lower airway tract sample for patients receiving moderate or high doses of ICS. While the hazard ratio for fluticasone users appeared to be higher compared to budesonide users, the confidence intervals overlapped.
To our knowledge, this study is the first ever to explore in a large well-characterized cohort of COPD outpatients the association between different exposures to ICS and risk of microbiologically verified positive lower airway tract samples of S. pneumoniae. Our study strengthens the mounting body of evidence that ICS may, in some patients and when given in high dose, carry serious adverse effects. Opposite we did find that low dose ICS therapy did not significantly increase the risk of a positive sample of S. pneumoniae low airway tract sample. This observation can be used in daily clinical practice: when ICS prescription is necessary in a COPD patient, the lowest possible dose should be given.
Conclusion
High doses of ICS were associated with a significantly increased risk of acquiring S. pneumoniae in patients with severe COPD, but low doses did not seem to carry an excess risk and our results support a restrictive strategy of ICS use in COPD patients.
Ethical Statement
This study was approved by the Danish Data Protection Agency. The Committee on Health Research Ethics, Capital Region of Denmark confirmed specifically that this study could be initiated without further ethical approval since retrospective use of register data does not require ethical approval or patient consent in Denmark. Data were only available on closed servers via the Danish Health Data Authority.
Acknowledgment
The abstract was published prior to submission due to presentation at the Nordic Lung Congress 2022.26
Funding
The study was financed by grants from Novo Nordisk Fonden (No. NNF20OC0060657). The funding sources had no influence on study design, data collection, analysis or reporting of data.
Disclosure
The authors declare that there are no conflicts of interest regarding this article. However, to ensure full transparency, we disclose the following potential conflicts of interest: PS received payment for lectures by Boehringer Ingelheim AstraZeneca, and GSK. TBS received grants from Sanofi Pasteur, Novo Nordisk Foundation, and Lundbeck foundation, received Consulting fees from Sanofi Pasteur, and Amgen, and received payment for lectures by Sanofi Pasteur, and GSK. TBS participates on Data Safety Monitoring Board or Advisory Board for Sanofi Pasteur and Amgen. ZBH received support for meetings and/or travel by Phizer. AKB received support for meetings and/or travel by PulmonX and reports non-financial support from GSK, during the conduct of the study. AGM received grants from Boehringer Ingelheim and is associated with the startup “Healthy network” producing automated e-stethoscopes. JRH received consulting fees from AstraZeneca, received payment for lectures by Boehringer Ingelheim, and Takeda, and received support to meetings and/or travel by AstraZeneca, and participates in AstraZeneca’s Advisory board and British Thoracic Society. MP received grants from Roche, received consulting fees from Takeda, Therakos, Zambon, and received payment for lectures by Mallinckrodt, PulmonX, and Glaxo-smith Kline, received support for meetings and/or travel by Boehringer-Ingelheim and is Chair of Danish transplant Society, and associated with The ERS group for transplantation. All other authors declare no competing interests in this work.
References
1. Stănescu D, Sanna A, Veriter C, et al. Airways obstruction, chronic expectoration, and rapid decline of FEV1 in smokers are associated with increased levels of sputum neutrophils. Thorax. 1996;51(3):267–271. doi:10.1136/thx.51.3.267
2. Calverley PM, Anderson JA, Celli B, et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356(8):775–789. doi:10.1056/NEJMoa063070
3. Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378(18):1671–1680. doi:10.1056/NEJMoa1713901
4. Papi A, Vestbo J, Fabbri L, et al. Extrafine inhaled triple therapy versus dual bronchodilator therapy in chronic obstructive pulmonary disease (TRIBUTE): a double-blind, parallel group, randomised controlled trial. Lancet. 2018;391(10125):1076–1084. doi:10.1016/S0140-6736(18)30206-X
5. Vestbo J, Anderson JA, Brook RD, et al. Fluticasone furoate and vilanterol and survival in chronic obstructive pulmonary disease with heightened cardiovascular risk (SUMMIT): a double-blind randomised controlled trial. Lancet. 2016;387(10030):1817–1826. doi:10.1016/S0140-6736(16)30069-1
6. Agusti A, Fabbri LM, Singh D, et al. Inhaled corticosteroids in COPD: friend or foe? Eur Respir J. 2018;52(6):1801219. doi:10.1183/13993003.01219-2018
7. Watz H, Tetzlaff K, Wouters EF, et al. Blood eosinophil count and exacerbations in severe chronic obstructive pulmonary disease after withdrawal of inhaled corticosteroids: a post-hoc analysis of the WISDOM trial. Lancet Respir Med. 2016;4(5):390–398. doi:10.1016/S2213-2600(16)00100-4
8. Kew KM, Seniukovich A. Inhaled steroids and risk of pneumonia for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2014;2014(12). doi:10.1002/14651858.CD010115.pub2
9. Torres A, Blasi F, Dartois N, Akova M. Which individuals are at increased risk of pneumococcal disease and why? Impact of COPD, asthma, smoking, diabetes, and/or chronic heart disease on community-acquired pneumonia and invasive pneumococcal disease. Thorax. 2015;70(10):984–989. doi:10.1136/thoraxjnl-2015-206780
10. Welte T, Torres A, Nathwani D. Clinical and economic burden of community-acquired pneumonia among adults in Europe. Thorax. 2012;67(1):71–79. doi:10.1136/thx.2009.129502
11. WHO collaborating centre for drug statistics methodology - ATC. Available from: https://www.whocc.no/atc/structure_and_principles/.
12. Uploaded protocol. Available from: http://coptrin.dk/wp-content/uploads/2021/10/Protocol-ICS-and-Streptococcus-pneumoniae.pdf.
13. Lange P, Tøttenborg SS, Sorknæs AD, et al. Danish Register of chronic obstructive pulmonary disease. Clin Epidemiol. 2016;8:673–678. doi:10.2147/CLEP.S99489
14. Johannesdottir SA, Horváth-Puhó E, Ehrenstein V, Schmidt M, Pedersen L, Sørensen HT. Existing data sources for clinical epidemiology: the Danish National Database of Reimbursed Prescriptions. Clin Epidemiol. 2012;4:303–313. doi:10.2147/CLEP.S37587
15. Lynge E, Sandegaard JL, Rebolj M. The Danish National Patient Register. Scand J Public Health. 2011;39(7 Suppl):30–33. doi:10.1177/1403494811401482
16. Inhaled corticosteroid doses for NICE’s asthma guideline. National Institute for Health and Care Excellence; 2018 Available from: https://www.nice.org.uk/guidance/ng80/resources/inhaled-corticosteroid-doses-pdf-4731528781
17. Global strategy for prevention, diagnosis and management of COPD: 2022 report. Available from: https://goldcopd.org/2022-gold-reports-2/.
18. Biomedical statistics and informatics software packages; 2018. Available from: https://bioinformaticstools.mayo.edu/downloads/sas/gmatch.sas.
19. Singanayagam A, Glanville N, Cuthbertson L, et al. Inhaled corticosteroid suppression of cathelicidin drives dysbiosis and bacterial infection in chronic obstructive pulmonary disease. Sci Transl Med. 2019;11(507). doi:10.1126/scitranslmed.aav3879
20. Castellana G, Castellana M, Castellana C, et al. Inhaled corticosteroids and risk of tuberculosis in patients with obstructive lung diseases: a systematic review and meta-analysis of non-randomized studies. Int J Chron Obstruct Pulmon Dis. 2019;14:2219–2227. doi:10.2147/COPD.S209273
21. Eklöf J, Ingebrigtsen TS, Sørensen R, et al. Use of inhaled corticosteroids and risk of acquiring Pseudomonas aeruginosa in patients with chronic obstructive pulmonary disease. Thorax. 2021;77(6):573–580. doi:10.1136/thoraxjnl-2021-217160
22. Ni S, Fu Z, Zhao J, Liu H. Inhaled corticosteroids (ICS) and risk of mycobacterium in patients with chronic respiratory diseases: a meta-analysis. J Thorac Dis. 2014;6(7):971–978. doi:10.3978/j.issn.2072-1439.2014.07.03
23. Danish national COPD treatment guidelines. Available from: https://lungemedicin.dk/kol-vejledning/.
24. Smith EL, Wheeler I, Adler H, et al. Upper airways colonisation of Streptococcus pneumoniae in adults aged 60 years and older: a systematic review of prevalence and individual participant data meta-analysis of risk factors. J Infect. 2020;81(4):540–548. doi:10.1016/j.jinf.2020.06.028
25. Lodise TP, Li J, Gandhi HN, O’Brien G, Sethi S. Intraclass difference in pneumonia risk with fluticasone and budesonide in COPD: a systematic review of evidence from direct-comparison studies. Int J Chron Obstruct Pulmon Dis. 2020;15:2889–2900. doi:10.2147/COPD.S269637
26. Backer V, Hilberg O, Ulrik C. NLC abstracts. Eur Clin Respir J. 2022;9(sup1):14. doi:10.1080/20018525.2022.2058255
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.