Back to Journals » ClinicoEconomics and Outcomes Research » Volume 15
Infrared Thermography Compared to Standard Care in the Prevention and Care of Diabetic Foot: A Cost Analysis Utilizing Real-World Data and an Expert Panel
Authors Kurkela O ![]() , Lahtela J, Arffman M
, Lahtela J, Arffman M ![]() , Forma L
, Forma L ![]()
Received 10 November 2022
Accepted for publication 12 January 2023
Published 22 February 2023 Volume 2023:15 Pages 111—123
DOI https://doi.org/10.2147/CEOR.S396137
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Olli Kurkela,1– 3 Jorma Lahtela,4 Martti Arffman,1,2 Leena Forma1,3
1Faculty of Social Sciences, Tampere University, Tampere, 30014, Finland; 2Department of Public Health and Welfare, Finnish Institute for Health and Welfare (THL), Helsinki, 00271, Finland; 3Laurea University of Applied Sciences, Vantaa, 01300, Finland; 4Tampere University Hospital, Tampere, 33520, Finland
Correspondence: Olli Kurkela, Health Sciences, Faculty of Social Sciences, Tampere University, P.O. Box 100, Tampere, 33014, Finland, Tel +358 50 5099170, Email [email protected]
Aim: Infrared thermography (IRT) is a non-invasive technology for screening and early detection of diabetic foot. Real-world data and the Delphi technique were used to assess IRT’s potential effect on typical care pathways of diabetic foot and their costs in the Finnish healthcare setting.
Methods: The most typical care pathways of diabetic foot were identified from national healthcare registers from 2011 to 2017. The effect of IRT in terms of avoidable care episodes was assessed by a Delphi panel including Finnish diabetic foot specialists (n=13). By combining a series of decision-analytic models, the IRT’s potential effect on the costs of each pathway and their sensitivity to model assumptions were estimated.
Results: Hypothetical annual savings were estimated to be EUR ~1.7 million (EUR ~1.3 million–EUR ~2.5 million), constituting approximately 20% of the total annual care pathway costs examined. In the longer and more complex pathways, the application of IRT was estimated to result in notable savings while in the shorter pathways, IRT could increase costs.
Conclusion: Our modeling suggests that IRT could potentially reduce costs in a Finnish healthcare setting. Given our analysis, generation of robust evidence on the effectiveness of recent IRT technologies with up-to-date protocols seems appropriate.
Keywords: foot complication, infrared thermography, healthcare costs, cost analysis, expert panel, diabetic foot
Introduction
Diabetic foot syndrome is a public health issue resulting in disability, reduced quality of life, and increased healthcare costs. The global prevalence of diabetic foot is over 6% and it occurs more often among men than women and people with type 2 than type 1 diabetes mellitus.1 In Finland, the age-standardized incidence and prevalence of diabetic foot were 111 and 989 per 10,000 people with diabetes in 2015–2017. In the coming years, the prevalence is expected to increase due to the aging diabetes population.2
The economic burden of diabetic foot on healthcare systems is also substantial. The severity of the condition and the specifics of provided health services incorporate variability in the costs,3–6 of which the latter highlights the need for country-specific studies. According to two recent Finnish studies, annual per-person costs related to diabetes foot complications were the highest of all complications, varying from 13,694 € to 17,666 € (2017 euros), while the total costs were approximately one-third of cardiovascular complications and around one-sixth of total costs of diagnosis-specific costs of complications.7,8
Infrared thermography (IRT) is a non-invasive technology used in screening and early detection of diabetic foot. IRT detects infrared radiation resulting from increased skin surface temperature induced by inflammation in the tissue. The assessment of side-to-side and local differences in temperature can enable early detection of ulcers.9 Although studies have shown successful applications of IRT in a variety of fields in medicine including diabetic foot,10 conflicting evidence on its effectiveness has restricted its role to complement diagnostic information provided by other methods.
IRT has been recommended by the International Working Group on the Diabetic Foot (IWGDF) as an option to prevent ulcers, mainly based on evidence from three randomized controlled trials (RCTs) conducted in early 2000s. These studies showed large effects of IRT in the reduction of foot ulcer recurrence,11–14 however, these findings have been contradicted by more recent RCTs.15–17 The estimated technology and characteristics of the study setting arguably affect the effectiveness estimates. Since no consensus has yet been reached among experts on IRT’s effectiveness, studies evaluating its economic efficiency are limited. The lack of evidence is the most probable reason for the rather low adaptation of IRT to routine care, which is also the case in Finland.
This ex-ante study assessed the effects of IRT on typical care pathways of diabetic foot and their costs when applied at regular check-ups. The assessment was made from a healthcare perspective and was based on care pathways identified from population-wide real-world data. Since IRT is not yet used regularly and patient data are therefore not available, its effects on the pathways were assessed using the Delphi method.18 Based on the expert panel’s opinion, the effect of IRT on each current care pathway was estimated and results were illustrated using decision analytic models. More specifically, we aimed to assess how the application of IRT 1) would affect the current care pathways and 2) would affect the costs of current care pathways, if applied as a standard practice.
This study provides preliminary estimates of IRT’s potential effect on current care pathways and their costs in a real-world setting. These estimates provide useful information for healthcare professionals and decision-makers involved in diabetic foot care to develop treatment and care pathways for diabetic foot. Furthermore, the estimates could guide the design of more controlled experiments on IRT’s effectiveness and cost-effectiveness.
Materials and Methods
The phases of the study are illustrated in Figure 1. The first phase involved the identification of 10 typical care pathways from national healthcare registers. Steps 1.1 and 1.2 have been described in detail in.19 In the second phase, 10 randomly sampled care pathways were presented to an expert panel, which assessed the effect of IRT on these pathways. Based on these assessments, hypothetical pathways were constructed including potential effects and additional cost of the IRT procedure. In the third phase, original and hypothetical pathways and their costs were compared to quantify the potential effect of IRT on the pathways. The study was carried out in adherence to Recommendations for the Conducting and Reporting of Delphi Studies (CREDES) and Consolidated Health Economic Evaluation Reporting Standards 2022 (CHEERS 2022).20,21
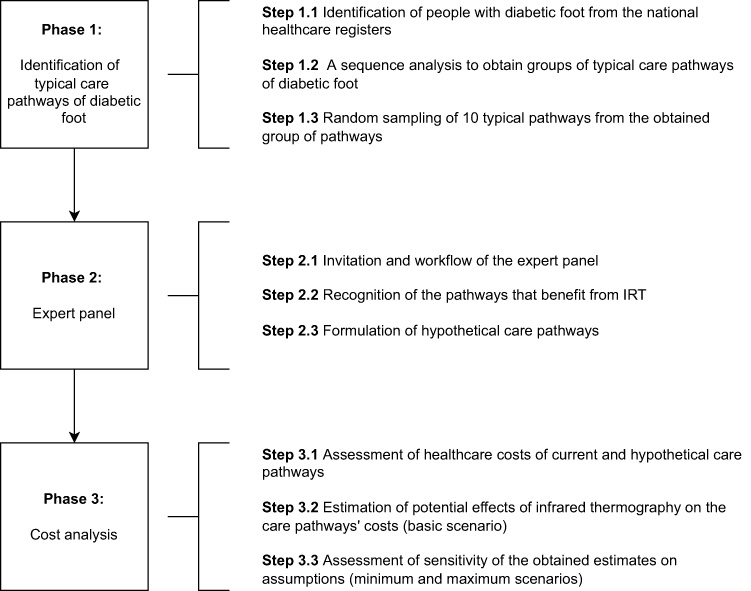 |
Figure 1 Study phases. |
Identification of Typical Care Pathways of Diabetic Foot (Phase 1)
Study Population
The study was based on the Diabetes in Finland (FinDM) cohort that comprised all patients with diagnosed diabetes mellitus in Finland between 1964 and 2017.22 For each patient, data included information on health service use in both primary health care (PHC) and specialized health care (SHC), reimbursed costs of medication, diabetes (type, date of diagnosis) and date of birth. In Step 1.1 (Figure 1), patients with initial diabetic foot diagnoses (Supplementary Table 1) between 2011 and 2016 (n = 63,900) were identified from the cohort. The study population was further restricted to patients who had a full two-year follow-up (n = 41,635) starting from the initial diabetic foot diagnosis.
Sequence Analysis
In Step 1.2 (Figure 1), the care pathway of the initial foot-related diabetes complication was defined for each patient based on their health service use. Each care pathway was restricted to diabetic foot care episodes. A sequence analysis was used to define groups of similar pathways.19,23,24 In the analysis, each care pathway was represented as a sequence of equal number of states with each state representing either a care episode or the absence of care episodes. A hierarchical clustering algorithm was then applied to identify groups of similar sequences (group of pathways).
Selection of Ten Typical Pathways
Since significant heterogeneity remained within each identified group of pathways, they were further divided into subgroups based on the number and type of care episodes they contained [20]. In each group of pathways, the two largest subgroups comprised the majority of pathways. Thus, nine pathways were randomly selected from the two largest subgroups within each group of pathways (Step 1.3, Figure 1). By removing the outlier pathways, the heterogeneity in the examined pathways could be reduced with only a modest decrease in representativeness. A care pathway involving an amputation was also included, since despite amputation being quite an infrequent event (present in 2% of all pathways), its costs and effects on quality of life are substantial.25 The amputation pathway was randomly selected from all pathways including amputation.
Expert Panel (Phase 2)
The Delphi method was used to assess the effect of IRT on typical care pathways. The method aims to achieve consensus among experts, in this study the diabetic foot specialists, on a particular issue to provide estimates in cases when more robust methods are not feasible.18
Invitation and Workflow of the Expert Panel
In Step 2.1 (Figure 1), an expert panel was invited to estimate the effect of IRT on the care pathways (the Delphi method).18 Eight physicians and five podiatrists were invited to the panel, a total of 13 experts. Podiatrists and physicians from both university and central hospitals and non-governmental organizations were invited with the aim to cover all relevant specialties involved in the multidisciplinary care of diabetic foot: diabetology, physiatry, vascular surgery, orthopedics and plastic surgery. Most of the experts had previous knowledge of IRT, although not wide experience. While on the panel, they did not represent their employers. They were not affiliated with the study funder and received no compensation. The expert panel were asked to respond anonymously to two rounds (December 2020 and January 2021) of an electronic questionnaire.
Recognition of the Pathways Benefiting from IRT
In the first round, diagrams of 10 typical care pathways (Step 2.2, Figure 1, Supplementary Figure 1a and b) were presented to the panel together with a description of the technology and its implementation. It was assumed that IRT would take place during an annual routine check-up and no additional healthcare visit was necessary.
Specifics of the care pathways included care episodes and related ICD-10 codes (Supplementary Table 1), the duration and sector of care (PHC or SHC), time between each care episode and patient characteristics (age, diabetes duration, whether or not the patient was on insulin medication and had late-stage complications). Each patient was considered to belong to IWGDF risk class 2 or 3.26 For each pathway, the panel was asked to assess:
- If IRT of the feet was performed on an annual basis, what is the probability that the first occurrence and care episodes following this could be avoided?
- In addition to IRT, what other kinds of examination/diagnostic methods would be required?
- How important is the regular application of IRT in this care pathway after the first contact?
- For care pathways 5, 6, and 10: If IRT was performed after the first procedure in the care pathway, what is the probability that the first occurrence and care episodes following this could be avoided?
In the second round, six care pathways were presented to the panel. Based on the responses to the first round, these six pathways were most affected by IRT (at least 30% probability of avoiding the first care episode). For each care pathway, a summary of responses from the first round was given. In this way, the respondents could adjust their opinion based on the responses of other experts (attempt at achieving consensus).18 The remaining variation was illustrated by sensitivity analyses. In the second round, question 2 was not included; however, two additional questions were asked:
- How often (how many times per year) should IRT be performed in this pathway in the future?
- How reliably the aforementioned items can be assessed based on the information provided in the questionnaire (1 not at all reliable, 5 very reliable)?
In both rounds, respondents were asked to give justifications for their responses, although that was not compulsory.
Formulation of Hypothetical Care Pathways
In Step 2.3, the potential effect of IRT on the care episodes (avoidance of subsequent care episodes) on the six typical care pathways was illustrated using tree diagrams (Figure 1). In the diagrams, each branch represents a hypothetical care pathway and was associated with the probability of the pathway occurring together with a simplified description of the care episodes in the pathway (level of care and length of stay) and associated costs.
Cost Analysis (Phase 3)
Assessing the Costs of Current and Hypothetical Pathways
Care pathway costs included the costs of outpatient and inpatient care episodes in both public PHC and public and private SHC, as well as the procedures performed. Moreover, the costs included medication administered during care episodes.
The pathway costs were calculated (Step 3.1) based on the expense information in healthcare registers and using the national unit costs (2011) reported by the Finnish Institute for Health and Welfare.27 A detailed description of costing of care episodes is described in detail.19 The cost of a hypothetical pathway comprised the cost of each care episode in that particular pathway, the cost of the IRT procedure and the cost of an additional podiatrist visit.
The cost of an IRT procedure was calculated based on the acquisition cost and the actual capacity estimate. The acquisition cost was based on two available technologies by a Finnish manufacturer (Thermidas Oy, Tampere, Finland): a clinical IR system and a handheld IR system with the annual costs of EUR 9000 and EUR 4000, respectively, assuming a service life of 5 years.28 The actual capacity estimate was based on a university hospital setting. Based on a specialist’s opinion, we assumed an annual maximum capacity of 4800 procedures and an annual actual capacity of 960 procedures (20% of maximum capacity). Consequently, an additional cost of EUR 9 and EUR 4 per procedure was applied for a clinical IR system and a handheld IR system, respectively.
The Finnish Current Care Guidelines recommend at least one annual visit to a podiatrist for patients in risk class 1, 2 or 3.26 Assuming that a follow-up by a podiatrist was necessary after a positive finding using IRT, the cost of podiatrist visit(s) was included in the hypothetical pathways. The cost of the visit was based on the national average cost (EUR 90).27
All monetary values are presented in 2017 euros (last year of the study) and converted using the price index for public expenditure provided by Statistics Finland.29 The total costs were further converted into US dollars using an exchange rate of 1.1993 (31 December 2017).30
Estimation of Effects of IRT on Pathways’ Costs
In Step 3.2 (Figure 1), we estimated the effect of IRT on each pathway’s costs by calculating the expected cost of each hypothetical pathway and by reducing the cost of the corresponding current care pathway (treatment as usual) to obtain pathway-specific estimates (IRT’s effect). The expected cost was calculated for each pathway as follows: the cost of each hypothetical pathway (branch of the tree) was multiplied by its probability of occurrence and the resulting costs were added. Each pathway-specific difference in costs was then multiplied by the number of pathways in the subgroup from which the pathway was originally sampled to obtain an estimate of total effect. The sum of these total effects represented the potential savings that could have been achieved in typical care pathways of diabetic foot that has started between 2011 and 2015.
Sensitivity Analysis
There was uncertainty associated with each hypothetical pathway’s probability of occurrence, the necessary number of additional visits to a podiatrist and additional examinations, all of which have an impact on the estimated effect. Furthermore, we incorporated variation in costs related to the choice of technology.
Since IRT is not a sufficient method for the diagnosis of diabetic foot, the diagnosis should be confirmed with additional examinations. The necessity of these additional examinations differed by care pathways and by respondent. Thus, the sensitivity of costs to the number of necessary additional examinations was assessed. Out of the suggested additional examinations, it was assumed that plain (x-ray) film, magnetic resonance imaging (MRI), angiography and electroneuromyography (ENMG) would create additional costs of EUR 140, EUR 1217 and EUR 674, respectively.27,31
To address the sensitivity of the estimates to various assumptions (Step 3.3, Figure 1), we created three scenarios for the potential effect: basic, minimum and maximum scenarios, which differed in the aforementioned factors (Table 1). In the minimum scenario, the probability of each additional examination was defined as the proportion of respondents suggesting the particular examination and the total number of respondents who answered the question (Supplementary Table 2).
 |
Table 1 Three Scenarios for Potential Effect of Infrared Thermography on Current Care Pathways and Related Assumptions |
All analyses were conducted using R statistical software (version 4.0.3).32
Results
Typical Care Pathways (Phase 1)
A total of 41,640 people with initial foot-related diabetes complications and at least 2 years of follow-up was identified during the study period. Sequence analysis resulted in six groups of typical care pathways that differed notably in type and number of pathways. The results of this study phase are reported and discussed in detail elsewhere.19
Assessments of the Expert Panel (Phase 2)
In the first round, nine respondents (75%) filled the questionnaire. Four of the respondents were physicians and five of them were podiatrists (Supplementary Table 3). With regard to questions 1 and 4, the assessed probabilities varied notably between the respondents. Six out of 10 care pathways had a median probability of at least 30% and were selected for the second round. These pathways represented 25% of all original care pathways. With regard to question 3, the median of importance of regular IRT was 3 or 4 for six care pathways and 1 or 2 for four care pathways (scale 1–5, higher values indicating higher importance). The panelists stated that optimal benefits would be achieved if IRT were performed at least once per year. Thus, a question about the optimal frequency of IRT was added to the questionnaire in the second round.
In the second round, 11 respondents (85%, 6 physicians and 5 podiatrists) filled the questionnaire (Supplementary Table 3). The variation of probabilities of Questions 1 and 4 were lower compared to the first round. In all six care pathways, IRT was considered important (a median of at least 3, Question 3). The panelists’ assessments of the optimal frequency of IRT varied from 1 to 4, 1 to 6 or 1 to 10 times per year, depending on the pathway (Question 5). In addition to IRT, the panelists described many other examination/diagnostic methods (Question 2, Supplementary Table 4). All question-specific responses were utilized for analyses in both rounds, regardless of whether the respondent had returned an incomplete questionnaire.
Further justifications from both rounds emphasized two major benefits of IRT: first, discovery of areas with excess load at an early stage of the condition could prevent its deterioration if appropriate actions were taken and second, observation in an IRT image could support the actual diagnosis of the condition. The panel also pointed out that when carried out in PHC, IRT could prevent visits to secondary health care, motivate patients to engage in better self-care and support the assessment of the suitability of diabetic footwear. Regarding pathways in which the clinical status was assessed to be clear, IRT would not provide any additional benefits (eg, fungal nail infection and hallux valgus). The justifications were similar in both rounds. The respondents stated that questions assessments could be made reliably (Question 6, Supplementary Table 3).
Based on the responses regarding the current care pathways presented to the expert panel in the second round, we formulated hypothetical pathways that would result from the application of IRT within the current pathways (Figure 2).
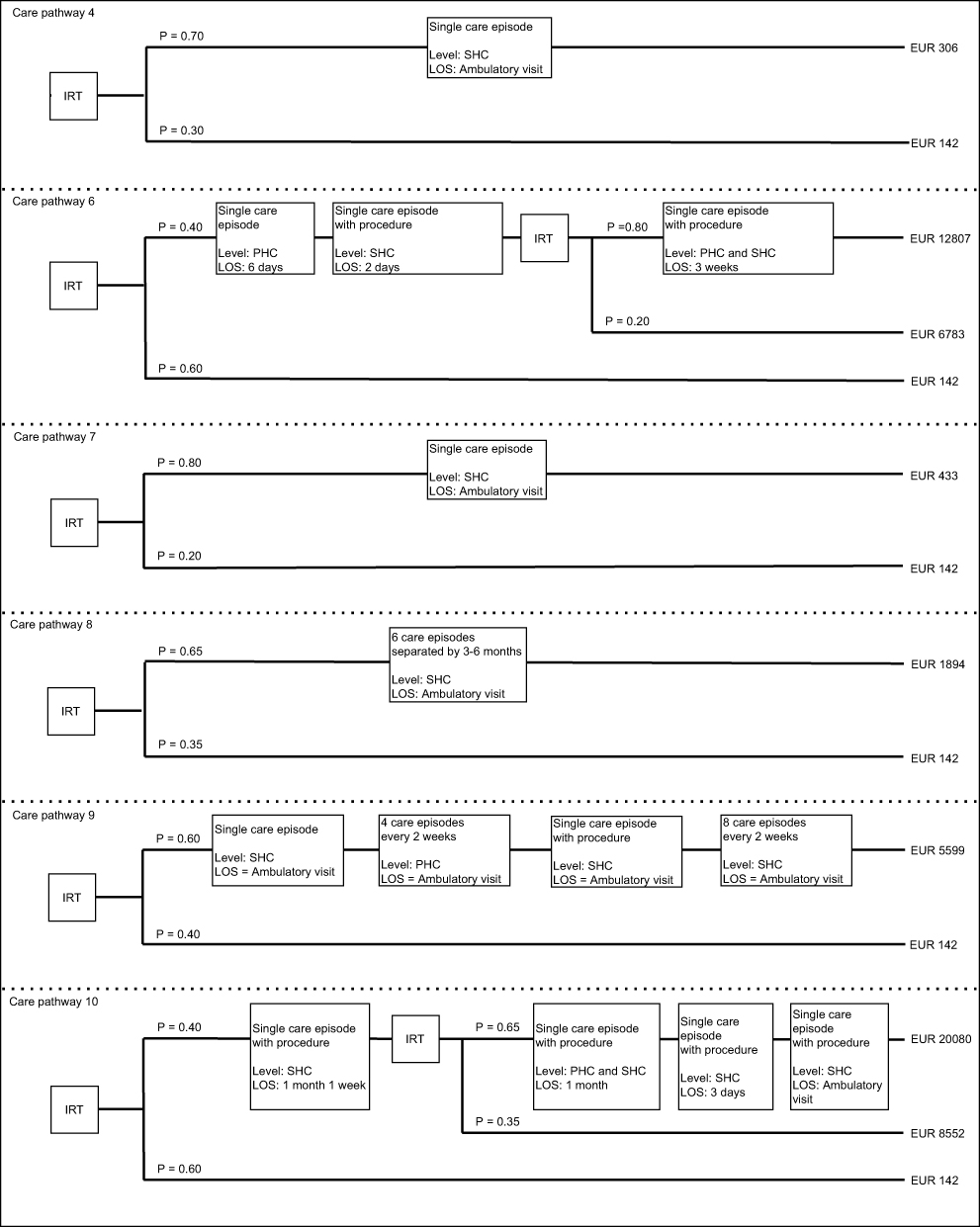 |
Figure 2 Hypothetical care pathways including infrared thermography and their costs. Current care pathways are presented in Supplementary Figure 1a and b. Abbreviations: PHC, primary health care; SHC, specialized health care; IRT, infrared thermography; LOS, length of stay. Notes: Hypothetical care pathways are presented in a simplified form including the probability of the pathway occurring, the number, length of stay (LOS) and healthcare level on which care is provided and cost of the pathway. |
Effect of IRT on Pathways’ Costs: Current vs Hypothetical Care Pathways (Phase 3)
The current care pathways presented to the expert panel in the second round (Table 2) differed notably in terms of number of care episodes and costs (Table 2). The size of the patient subgroups that each pathway represented varied from hundreds to a few thousand.
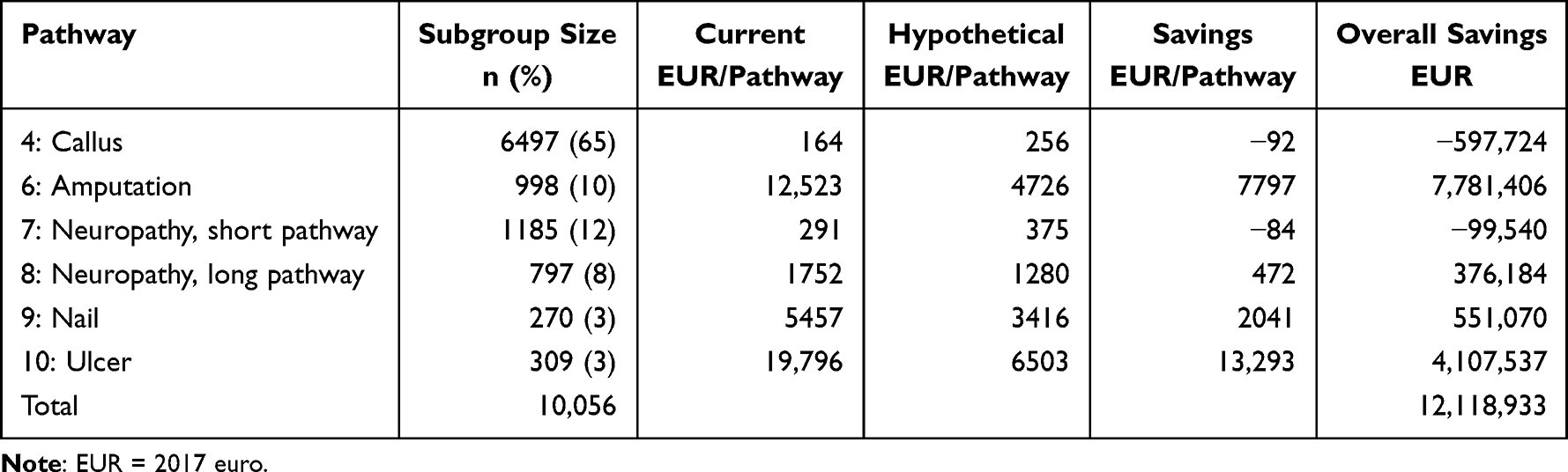 |
Table 2 Potential Effects of Infrared Thermography on Costs of Pathways That Started Between 2011 and 2015 (Basic Scenario) |
Basic Scenario
Within this basic scenario, the estimated costs of hypothetical care pathways were notably lower compared to current care pathways (Table 2) among longer and more complex care pathways (amputation, long neuropathy, nail and ulcer pathways). At highest, costs were approximately 70% lower (ulcer pathway). Among shorter pathways, the costs of hypothetical pathways (callus and short neuropathy pathways) were higher compared to current pathways (50% increase at highest, callus pathway).
The potential total effect of IRT on pathways’ costs was estimated to be approximately EUR 12 million during the study period (Table 2). The largest savings were estimated in the amputation pathway, approximately EUR 8 million, while the highest cost increase was associated with the callus pathway (EUR 0.6 million).
Minimum and Maximum Scenarios
The estimated potential effects of IRT were sensitive to the assumptions made (Table 3). In the minimum and maximum scenarios, the potential total savings were approximately EUR 9 million and EUR 18 million, respectively. In the maximum scenario, the costs of hypothetical care pathways were 4–75% lower than in the basic scenario. In the minimum scenario, the costs of hypothetical care pathways were 20–36% higher compared to the basic scenario. Regardless of scenario, savings could not be achieved with the callus pathway, while savings remained notable in other pathways (excluding short neuropathy).
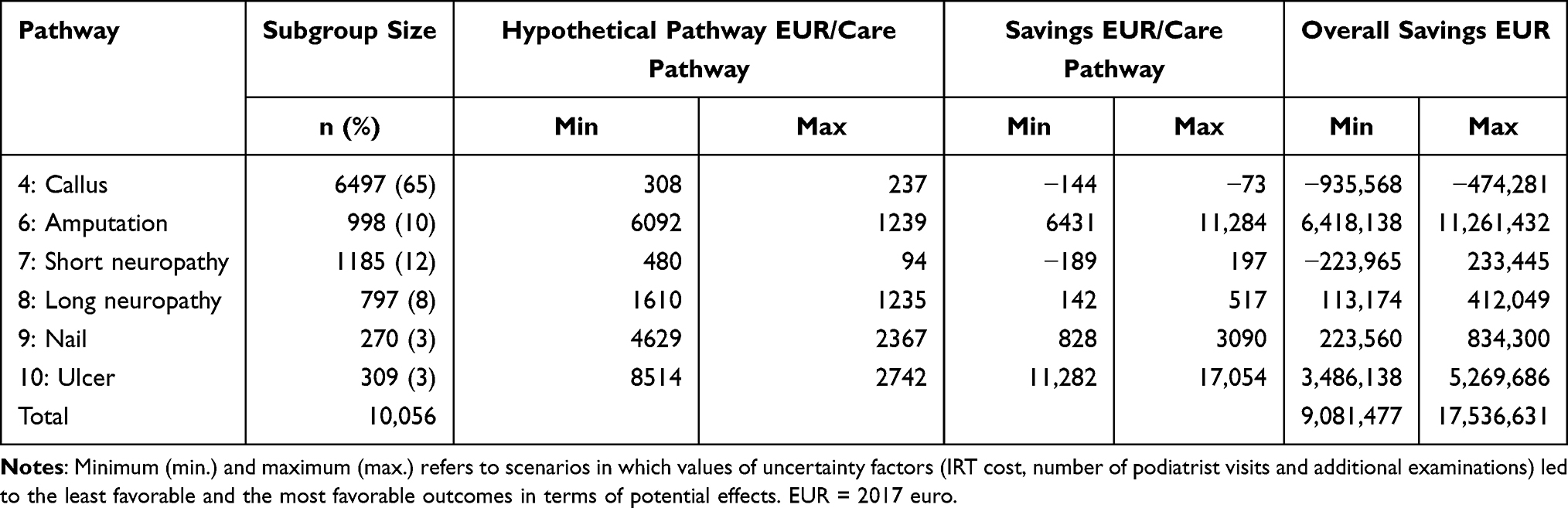 |
Table 3 Minimum (Min) and Maximum (Max) Scenarios of Infrared Thermography’s Potential Effect on Costs of Pathways That Started Between 2011 and 2015 |
Discussion
In this study, the effects of IRT on the typical care pathways of diabetic foot identified from population-wide real-world data were assessed by an expert panel. The potential effects on each pathway’s costs were then estimated utilizing decision analytic models.
Overall, the expert panel assessed that by using IRT, care episodes could be avoided in six out of 10 care pathways (callus, amputation, neuropathy, nail and ulcer pathways). These six care pathways represented approximately 25% of all identified pathways. Common to all six pathways was that the clinical status of patient on each pathway was not considered clear by some respondents, and therefore IRT would provide additional benefit. This was not the case with other care pathways (eg, fungal nail infection and hallux valgus), which were assessed not to benefit from IRT.
Most recent assessments of IRT’s effectiveness include two large RCTs,16,17 that with higher statistical power, have contradicted previous positive estimates.12–14 Nonetheless, their focus has been entirely on assessing the feasibility of IRT in avoiding diabetic ulcer recurrence using technology and treatment protocol that differs to a large extent from those of this study. Based on the expert panel’s assessment, we estimated that regular use of IRT could prevent 60% of the ulcer pathways that would result to pathway-specific saving of over EUR 13000 and total savings of over 4 million euros in the Finnish healthcare system. However, those results are not directly comparable due to differences in study design.
In total, the application of IRT was assessed to result in notable total savings with regard to the six care pathways. Longer care pathways contributed largely to the total savings, while in the Callus pathway application of IRT was estimated to increase costs due to additional examinations and visits to a podiatrist.
By dividing the total savings by number of years in the study period, we arrived at an average annual saving of approximately EUR 1.7 million (USD 2.1 million) in healthcare costs between 2011 and 2017, totaling up to 18% of the costs of the examined care pathways in this study. The savings would be due to care episodes and related expensive procedures that could be avoided by early detection of problematic areas using IRT. The savings for pathways that were not considered typical (37%) could not be assessed.
To date, cost studies or cost-effectiveness analyses of IRT are limited, to our knowledge, to a single modeling-based study from USA comparing use of IRT in addition to standard care compared to standard care alone.33 Based on a decision tree analysis, Brooks et al estimated annual per-patient savings of over USD 8000 and total savings of USD 38593 per additional ulcer case. Our estimate concerning the Ulcer pathway was notably more conservative (EUR 13293). Nevertheless, studies differ profoundly in terms of technology: in our study, the IRT was applied by a healthcare professional in a healthcare setting compared to remote foot temperature monitoring technology in the US study.33 Nevertheless, the study has faced critique on both its assumption of potential effectiveness and costs of treatment of ulcer34 and further assessments are welcomed.
Our estimates were sensitive to the modeling assumptions, and this sensitivity was characterized by the minimum and maximum scenarios. These alternative scenarios assumed different values for the most important uncertainty factors and reflected situations that were most favorable and least favorable with respect to effects of IRT. Overall, all scenarios resulted in savings ranging from 18% to 23% of total costs. Savings were confined to longer pathways, regardless of scenario.
The modeling assumptions deserve further scrutiny. First, the effects of IRT were based on assessments of the expert panel (n=13). Despite being positive towards application of IRT, the assessed probability in each pathway had large variability within respondents. We are not sure, however, if this variability could be reduced by increasing the panel size, since the number of foot care experts with knowledge or experience on IRT in Finland is limited. Nevertheless, the panel comprised representatives from all relevant specialties involved in treatment of diabetic foot and a response rate as high as 85% was achieved, while 77% of panelists completed the questionnaire. We have no reason to assume that there would be a non-response bias between the respondents and non-respondents. However, since the number of panelists was moderate, subgroup analyses, for example, between panelists with and without IRT experience, were not possible. The panel’s work was based on typical care pathways identified from population-wide real-world data, which strengthens the usability of the panel’s work.35
Second, there are several IRT technologies available with evidence on their effectiveness, ranging from technologies applied in a clinical setting to technologies applied by a patient at home.16,17 We depicted a scenario with a technology applied in a university hospital setting by a foot care specialist and the additional cost of IRT was determined based on two such technologies available in Finland. Naturally, additional cost of the procedure may differ to some extent in other settings. We want to emphasize that the expert panel was not asked to assess these particular products but instead the technology overall in a given setting. In addition, several other factors such as the duration of the procedure and who performs it (including interpretation of findings) affect the total cost. As appropriate values could not be found on these factors, they were not considered in our calculations.
Third, the expert panel assessed that after a positive finding, in part of the care pathways clinical examination was sufficient, while in other, multiple additional examinations and diagnostic methods were required. Confirmatory examinations naturally increase the cost of a care pathway, which was characterized using the minimum scenario. If the IRT becomes a more established practice, these uncertainty factors will be easier to assess.
The analysis was conducted from a healthcare perspective and aimed to serve decision-makers involved in treatment of diabetic foot. Therefore, some significant cost items were excluded from the analysis; social care (mainly care for older people), rehabilitation costs, direct and time costs to patients and their families, as well as productivity losses36 were not considered. Further studies hopefully clarify their role.
The analyses were based on reliable national, ie, population-wide, registers including all patients with a diabetes diagnosis in Finland,22,37 which is a major strength of the study. From this extensive dataset, we were able to extract a wide array of typical care pathways using sequence analysis.19 These real-world pathways represented healthcare use related to different foot-related complications comprising real-world variation in patient characteristics, thus providing a wide perspective on IRT’s potential. Most of the published RCTs to date have focused on ulcer recurrence with restricted patient population. In our study, ulcer pathways represented only 3% of all pathways. In practice, investigation using real-world data may be the only feasible option to assess IRTs effectiveness and cost-effectiveness with regard to some of the foot complications.
The modeling-based approach required multiple assumptions to be made, which relied heavily on the clinical expertise in the research group. If IRT becomes a more established practice, their assessment may be more strongly supported by data. We found it challenging to estimate the number of annual IRT procedures necessary to detect changes in skin temperature effectively and therefore we based our estimate on typical frequency of patient visits in routine care of patients with diabetes. The expert panel suggested a range of 1 to 10 IRT procedures per year, depending on the pathway, while published RCTs have typically applied daily or monthly monitoring of skin temperature.15–17 Very high intense monitoring in a clinical setting may not be a feasible practice in many of these pathways. Nevertheless, the modeling-based approach is useful in estimating the potential of IRT in a Finnish healthcare setting and guiding setups of future effectiveness and cost-effectiveness studies.
A factor largely determining the success of IRT is patients’ compliance with the long-term monitoring, which depends highly on its frequency and the applied technology. The issue of compliance is emphasized among patients with diabetes, due to often already high load of monitoring and previous studies have reported low adherence to technologies requiring daily self-monitoring.17 This study assumed that IRT was applied mainly at routine check-ups by a healthcare professional, which could possibly result in higher concordance among patients. Factors affecting patients’ compliance are an important topic for future research.
As a major shortcoming, the data did not cover care given in private outpatient and occupational health care. However, these sectors contribute only little to the treatment of diabetic foot in Finland, and therefore introduce only minimal bias in representativeness of the examined care pathways. In addition, we lacked data on some relevant cost items. Even though the costs of reimbursed outpatient medication were available in the registers, it was not possible to specifically identify which forms of medications were prescribed to treat the complications in question. In Finland, outpatient medication expenses are partly covered by the Social Insurance Institution of Finland and partly by patients. Thus, the costs do not entirely devolve on the healthcare system. Finally, national databases do not comprise information on the use and costs of diabetic footwear. The absence of such knowledge may significantly impact the cost estimates of shorter pathways, since in some cases the cost of diabetic shoes may exceed the cost of the whole pathway.
This modeling study contributes to the treatment of diabetic foot by providing first assessment of IRT’s potential as a standard procedure in the prevention and treatment of diabetic foot in the Finnish healthcare setting. Moreover, it is one of the rare studies assessing the IRT’s effect on costs. Our approach provides an alternative point of view to published RCTs by examining a wider set of conditions based on real-world data. Based on our estimates, IRT could provide savings in most of the typical care pathways of diabetic foot and the results suggest that the evaluation of IRT should proceed into more controlled studies in a Finnish healthcare setting, when feasible. Further evidence on IRT’s effectiveness and cost-effectiveness, however, is necessary for the decision on whether IRT should be adapted as part of the standard practice.
To effectively prevent a condition from deteriorating, it needs to be detected at an early stage.38 Therefore, a major patient group that could benefit from IRT are patients with diagnosed loss of protective sensation (LOPS) who have not yet developed an ulcer. IRT could then be applied in PHC and visits to SHC and expensive procedures could potentially be avoided. In case of detection of complication delays, overall costs could increase. Ensuring a functional care pathway after a positive finding is crucial.
In case the application of IRT becomes more common, prospective studies using also individual-level outcome data are needed. In addition to resource use and costs, also benefits in terms of quality of life should be considered. Only recently, a procedure code indicating IRT became available in Finland that enables healthcare professionals to associate an IRT procedure to a care episode. This will hopefully enable monitoring of technology’s adaptation as part of standard care and future real-world studies of its effectiveness and cost-effectiveness using national healthcare registers.
Conclusions
In conclusion, our model suggested that hypothetical annual savings of more than EUR 1.7 million could be achieved by using IRT as a standard procedure. Despite the estimates being somewhat sensitive to the assumptions of the model, annual savings were achieved in all scenarios (1.3 to 2.5 million euros). This study contributes by providing insights for healthcare professionals and decision-makers involved in diabetic foot care when considering and implementing treatment methods. As the prevalence of diabetic foot is expected to increase in the coming years, imposing an escalating burden on healthcare systems, continuous follow-up of costs and effectiveness of diabetic foot treatments is essential.
Abbreviations
ENMG, electroneuromyography; FinDM, Diabetes in Finland study; ICD-10, International Classification of Diseases 10; IRT, infrared thermography; LOS, length of stay; MRI, magnetic resonance imaging; PHC, primary health care; SHC, specialized health care.
Data Sharing Statement
The data that support the findings of this study are available from the Finnish Institute of Health and Welfare. However, restrictions apply to the availability of these data, which were used under license for the current study and are therefore not in the public domain. However, the data are available from the authors upon reasonable request and with the permission of the Finnish Institute of Health and Welfare (author to contact: MA, [email protected]).
Ethics Approval and Informed Consent
The FinDM study protocol was approved by the Research Ethics Committee of Finnish Institute for Health and Welfare (decision number 2018/§787). Permission to use the register data was obtained from the competent register authorities (Finnish Institute for Health and Welfare, Social Insurance Institution of Finland, Statistics Finland, Finnish Centre of Pensions, Finnish Kidney and Liver Association). Informed consent was not required as this is a retrospective register-based study. Study data was pseudonymized before use.
Acknowledgments
We would like to thank the expert panel members for their insights, the steering group of FinDM for permission to use the data and MSc Gregrey Oko-Oboh for the preliminary literature search.
Funding
The study was partly funded by TherMidas Oy. The funder did not contribute to the design, collection, analysis or interpretation of the data, nor to the writing of the manuscript.
Disclosure
OK, MA and LF received funding from TherMidas Oy, which is a for-profit organization that manufactures infrared thermography equipment. The funder commissioned the study on economic viability of IRT in treatment of diabetic foot. The funder did not contribute to study design, collection, analysis or interpretation of the data, nor to the writing of the manuscript. JL declares that he has no competing interests.
References
1. Zhang P, Lu J, Jing Y, Tang S, Zhu D, Bi Y. Global epidemiology of diabetic foot ulceration: a systematic review and meta-analysis. Ann Med. 2017;49(2):106–116. doi:10.1080/07853890.2016.1231932
2. Arffman M, Ilanne-Parikka P, Keskimäki I, et al. Incidence and prevalence of type 1 and type 2 diabetes and their complications in Finland 2000-2017. [Tyypin 1 ja 2 diabeteksen ja niiden lisäsairauksien ilmaantuvuus ja esiintyvyys Suomessa vuosina 2000–2017]. Data Brief 8/2020 [Tutkimuksesta tiiviisti 8/2020]. Finnish Institute for Health and Welfare; 2020.
3. Cavanagh P, Attinger C, Abbas Z, Bal A, Rojas N, Xu Z. Cost of treating diabetic foot ulcers in five different countries. Diabetes Metab Res Rev. 2012;28:107–111. doi:10.1002/dmrr.2245
4. Ray JA, Valentine WJ, Secnik K, et al. Review of the cost of diabetes complications in Australia, Canada, France, Germany, Italy and Spain. Curr Med Res Opin. 2005;21(10):1617–1629. doi:10.1185/030079905X65349
5. Kerr M, Barron E, Chadwick P, et al. The cost of diabetic foot ulcers and amputations to the national health service in England. Diabet Med. 2019;36(8):995–1002. doi:10.1111/dme.13973
6. American Diabetes Association. Economic costs of diabetes in the US in 2017. Diabetes Care. 2018;41(5):917–928. doi:10.2337/dci18-0007
7. Kurkela O, Raitanen J, Tuovinen M, Ilanne-Parikka P, Forma L. Lisäsairaudet voivat moninkertaistaa tyypin 2 diabetesta sairastavan terveydenhuollon kustannukset [Complications may significantly intensify healthcare use of patients with type 2 diabetes]. Finnish Med J. 2022;78:e32697.
8. Sund R, Peltonen T, Lehtimäki A-V, Martikainen J. Hospital treatment costs associated with incident complications in patients with type 2 diabetes—real-world study based on electronic patient information systems. BMC Health Serv Res. 2022;22(1):1–13. doi:10.1186/s12913-022-07895-6
9. Ilo A. Infrared thermography in vascular disorders: screening and follow-up [Internet]. Acta Universitatis Ouluensis; 2020. Available from: http://jultika.oulu.fi/files/isbn9789526228044.pdf.
10. Lahiri BB, Bagavathiappan S, Jayakumar T, Philip J. Medical applications of infrared thermography: a review. Infrared Phys Technol. 2012;55(4):221–235. doi:10.1016/j.infrared.2012.03.007
11. Bus SA, Lavery LA, Monteiro‐Soares M, et al. Guidelines on the prevention of foot ulcers in persons with diabetes (IWGDF 2019 update). Diabetes Metab Res Rev. 2020;36:e3269.
12. Lavery LA, Higgins KR, Lanctot DR, et al. Home monitoring of foot skin temperatures to prevent ulceration. Diabetes Care. 2004;27(11):2642–2647. doi:10.2337/diacare.27.11.2642
13. Lavery LA, Higgins KR, Lanctot DR, et al. Preventing diabetic foot ulcer recurrence in high-risk patients: use of temperature monitoring as a self-assessment tool. Diabetes Care. 2007;30(1):14–20. doi:10.2337/dc06-1600
14. Armstrong DG, Holtz-Neiderer K, Wendel C, Mohler MJ, Kimbriel HR, Lavery LA. Skin temperature monitoring reduces the risk for diabetic foot ulceration in high-risk patients. Am J Med. 2007;120(12):1042–1046. doi:10.1016/j.amjmed.2007.06.028
15. Skafjeld A, Iversen M, Holme I, Ribu L, Hvaal K, Kilhovd B. A pilot study testing the feasibility of skin temperature monitoring to reduce recurrent foot ulcers in patients with diabetes–a randomized controlled trial. BMC Endocr Disord. 2015;15(1):1–7. doi:10.1186/s12902-015-0054-x
16. Petrova NL, Donaldson NK, Tang W, et al. Infrared thermography and ulcer prevention in the high‐risk diabetic foot: data from a single‐blind multicentre controlled clinical trial. Diabet Med. 2020;37(1):95–104. doi:10.1111/dme.14152
17. Bus SA, Wouter B, van Baal JG, Busch-Westbroek TE, Nollet F, van Netten JJ. Effectiveness of at-home skin temperature monitoring in reducing the incidence of foot ulcer recurrence in people with diabetes: a multicenter randomized controlled trial (DIATEMP). BMJ Open Diabetes Res Care. 2021;9(1):e002392. doi:10.1136/bmjdrc-2021-002392
18. Niederberger M, Spranger J. Delphi technique in health sciences: a map. Front Public Health. 2020;8(September):1–10.
19. Kurkela O, Nevalainen J, Arffman M, Lahtela J, Forma L. Foot-related diabetes complications: care pathways, patient profiles and costs. BMC Health Serv Res. 2022;22(1):1–11. doi:10.1186/s12913-022-07853-2
20. Jünger S, Payne SA, Brine J, Radbruch L, Brearley SG. Guidance on Conducting and REporting DElphi Studies (CREDES) in palliative care: recommendations based on a methodological systematic review. Palliat Med. 2017;31(8):684–706. doi:10.1177/0269216317690685
21. Husereau D, Drummond M, Augustovski F, et al. Consolidated Health Economic Evaluation Reporting Standards 2022 (CHEERS 2022) statement: updated reporting guidance for health economic evaluations. Int J Technol Assess Health Care. 2022;38(1). doi:10.1017/S0266462321001732
22. Arffman M, Ilanne-Parikka P, Keskimäki I, et al. FinDM Database on Diabetes in Finland. Helsinki; 2020.
23. Gabadinho A, Ritschard G, Mueller NS, Studer M. Analyzing and visualizing state sequences in R with TraMineR. J Stat Softw. 2011;40(4):1–37. doi:10.18637/jss.v040.i04
24. Gabadinho A, Ritschard G, Studer M, Müller NS. Mining Sequence Data in R with the TraMineR Package: A User’s Guide. Geneva: Dep Econom Lab Demogr Univ Geneva; 2009.
25. Ragnarson Tennvall G, Apelqvist J. Health-related quality of life in patients with diabetes mellitus and foot ulcers. J Diabetes Complications. 2000;14(5):235–241. doi:10.1016/S1056-8727(00)00133-1
26. Schaper NC, van Netten JJ, Apelqvist J, et al. Practical guidelines on the prevention and management of diabetic foot disease (IWGDF 2019 update). Diabetes Metab Res Rev. 2020;36:e3266. doi:10.1002/dmrr.3266
27. Kapiainen S, Väisänen A, Haula T. Terveyden- ja sosiaalihuollon yksikkökustannukset Suomessa vuonna 2011 [Social and health care unit costs in Finland 2011]. Terveyden ja hyvinvoinnin laitos; 2014:1–124. Available from: https://www.julkari.fi/bitstream/handle/10024/114683/THL_RAPO3_2014_web.pdf?sequence=1.
28. TherMidas OY. Thermal imaging for early diagnostics. Available from: https://thermidas.fi/applications/.
29. Official Statistics of Finland. Price index of public expenditure [e-publication]. Statistics Finland. Available from: http://www.stat.fi/til/jmhi/index_en.html.
30. European Central Bank. Euro foreign exchange reference rates. Available from: https://www.ecb.europa.eu/stats/policy_and_exchange_rates/euro_reference_exchange_rates/html/index.en.html.
31. Pirkanmaa Hospital District. Tuotteet ja hinnat 2017 [Products and prices 2017]; 2016. Available from: www.pshp.fi.
32. R Core Team. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2013.
33. Brooks E, Burns M, Ma R, Scholten HJ, Becker S. Remote diabetic foot temperature monitoring for early detection of diabetic foot ulcers: a cost-effectiveness analysis. Clin Outcomes Res CEOR. 2021;13:873.
34. van Netten JJ, Dijkgraaf MGW, Bus SA. Response to: remote diabetic foot temperature monitoring for early detection of diabetic foot ulcers: a cost-effectiveness analysis. Clin Outcomes Res. 2022;14:49–51. doi:10.2147/CEOR.S354729
35. Jorm AF. Using the delphi expert consensus method in mental health research. Aust N Z J Psychiatry. 2015;49(10):887–897. doi:10.1177/0004867415600891
36. Kurkela O, Forma L, Ilanne-Parikka P, Nevalainen J, Rissanen P. Association of diabetes type and chronic diabetes complications with early exit from the labour force: register-based study of people with diabetes in Finland. Diabetologia. 2021;64(4):795–804. doi:10.1007/s00125-020-05363-6
37. Sund R, Nurmi-Lüthje I, Lüthje P, Tanninen S, Narinen A, Keskimäki I. Comparing properties of audit data and routinely collected register data in case of performance assessment of hip fracture treatment in Finland. Methods Inf Med. 2007;46(5):558–566. doi:10.1160/ME0382
38. Jeffcoate WJ, Vileikyte L, Boyko EJ, Armstrong DG, Boulton AJM. Current challenges and opportunities in the prevention and management of diabetic foot ulcers. Diabetes Care. 2018;41(4):645–652. doi:10.2337/dc17-1836
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.