Back to Journals » Journal of Inflammation Research » Volume 18
Ineffective Recanalization and Complications in Patients with Acute Ischemic Stroke Receiving Endovascular Treatment: Predictive Value of the c-Reactive Protein-Albumin-Lymphocyte (CALLY) Index
Authors Zhu L, Jie S, Wu S, Chen Q, Zhang X ![]() , Yang W, Wu Y
, Yang W, Wu Y ![]()
Received 22 April 2025
Accepted for publication 8 October 2025
Published 22 October 2025 Volume 2025:18 Pages 14649—14661
DOI https://doi.org/10.2147/JIR.S535881
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rongxue Wu
Lin Zhu,1 Sanming Jie,1 Shuhua Wu,1 Qin Chen,1 Xuhui Zhang,1 Wenwu Yang,2 Yongming Wu1
1Department of Neurology, Nanfang Hospital, Southern Medical University, Guangzhou, People’s Republic of China; 2Department of Neurosurgery, the 981 Hospital of the Chinese People’s Liberation Army, Chengde, People’s Republic of China
Correspondence: Wenwu Yang, Department of Neurosurgery, the 981 Hospital of the Chinese People’s Liberation Army, Puning Road, Shuangqiao District, Chengde, 067000, People’s Republic of China, Email [email protected] Yongming Wu, Department of Neurology, Nanfang Hospital, Southern Medical University, Guangzhou North Avenue 1838#, Guangzhou, 510515, People’s Republic of China, Tel +86 13711530187, Email [email protected]
Purpose: The C-reactive protein–albumin–lymphocyte (CALLY) index, as a composite biomarker reflecting nutritional reserves and immunosuppression, has demonstrated important predictive value in various disease. We aimed to investigate the CALLY index’s predictive value versus previous inflammatory-nutritional biomarker for ineffective recanalization and complications in acute ischemic stroke (AIS) patients who received emergency endovascular therapy (EVT).
Methods: We retrospectively reviewed 705 AIS patients admitted to Nanfang Hospital for EVT from January 2019 to December 2023. We calculated the CALLY index, Geriatric Nutritional Risk Index, Controlling Nutritional Status score, Prognostic Nutritional Index, and C-reactive protein-to-albumin ratio, and assessed their predictive significance for ineffective recanalization using univariate and multivariate logistic regression. Predictive efficacy was compared via receiver operating characteristic (ROC) curve analysis, while the Net Reclassification Improvement (NRI) and Integrated Discrimination Improvement (IDI) quantified the incremental value of models incorporating these biomarkers. In addition, we explored the relationship between the CALLY index and post-EVT complications.
Results: The CALLY index had the best predictive validity with an area under the ROC curve of 0.73. The new model incorporating the CALLY index had the best optimization effect (NRI of 0.157, P=0.028; IDI of 0.029, P=0.008). A significant correlation was also shown between the CALLY index and stroke-associated pneumonia.
Conclusion: The CALLY Index demonstrated its potential as an innovative and accessible indicator for prognosis.
Keywords: acute ischemic stroke, prognosis, biomarker, stroke-associated pneumonia, nutrition, inflammation
Introduction
The efficacy and safety of endovascular treatment (EVT) relative to pharmacologic therapy were validated in patients with anterior circulation large vessel occlusion stroke.1,2 However, despite successful recanalization of the occluded artery in many patients with acute ischemic stroke (AIS) who undergo EVT, nearly half of them did not experience a favorable outcome.3 What’s more, complications during the perioperative period, such as malignant cerebral edema (MCE), early neurological deterioration (END), and stroke-associated pneumonia (SAP), may further contribute to poor prognosis in these patients.4–6 These conditions impose a huge economic burden on society. Therefore, identifying high-risk patients for poor outcomes and complications is necessary and clinically meaningful.
Previous studies have demonstrated that malnutrition, which was associated with longer hospitalization, poor functional recovery, and mortality, affects approximately 30% of AIS patients.7,8 Nutritional biomarker such as the CONUT score, and serum albumin level can serve as prognostic indicators.9–11 Furthermore, malnutrition and systemic inflammation can interact with each other.12,13 Malnourished AIS patients exhibit an impaired ability to maintain immune homeostasis by balancing oxidative stress and pro-inflammatory mediator production.14,15 Various inflammation-nutrition-related indicators have shown prognostic significance, for instance, c-reactive protein to albumin ratio (CAR) was associated with risk of long-term mortality in stroke patients.16–18
The C-reactive protein–albumin–lymphocyte (CALLY) index, a novel composite marker integrating inflammation (CRP), nutritional reserve (albumin), and immune status (lymphocyte count), has demonstrated prognostic utility in acute myocardial infarction by predicting mortality and functional recovery.19 However, its role in AIS remains unexplored. We aimed to determine whether the CALLY index outperforms traditional markers including CONUT, CAR in predicting EVT-related complications and ineffective recanalization in AIS patients.
Methods
Study Design and Population
Our study retrospectively reviewed a prospective cohort of all AIS patients with anterior circulation admitted to Nanfang Hospital for emergent EVT from 2019 to 2023 (n=705). A team of three senior neurointerventionalists, who were blinded to the study, performed the diagnoses and procedures.
Exclusion criteria: 1) Posterior circulation cerebral infarction; 2) Unsuccessful vascularization, defined as modified thrombolysis in cerebral infarction (mTICI) score <2b; 3) Presence of any of the following conditions: tumors, infections on admission, autoimmune diseases, renal failure, cirrhosis, acute myocardial infarction; 4) Modified Rankin Scale (mRS) score >1 before onset; 5) Missing essential data; 6) Loss to follow-up.
After applying the above criteria, 249 patients were enrolled in the subsequent analysis. Patient data were collected from the electronic medical record system, including demographic characteristics, medical history, clinical assessment findings, and laboratory data, eg, Lymphocyte Count, Fasting Glucose, Total Cholesterol, C-reactive protein (CRP), and other biochemical markers.
This study was conducted in accordance with the Declaration of Helsinki and approved by the Nanfang Hospital’s ethics committee on clinical research (NFEC-2024-646).
Assessment of Various Inflammatory-Nutritional Indicators
Different indicators for assessing nutritional and inflammatory status were calculated based on the patient’s height, weight at admission, and the results of fasting peripheral blood tests obtained within 24 hours after admission. These included the CALLY index, Geriatric Nutritional Risk Index (GNRI), Prognostic Nutritional Index (PNI), Controlling Nutritional Status (CONUT) score, and C-reactive protein-to-albumin ratio (CAR). The formulas for each indicator are as follows:
CALLY index = Serum albumin (g/L) × Lymphocyte count (x109/L) /(CRP (mg/L) ×10).
GNRI=(1.489 × 10 × serum albumin (g/dL)) + (41.7 × weight (kg)/ideal body weight (kg)). The ideal body weight is 0.75 × height (cm)—62.5 for male patients, and 0.60 × height (cm)—40 for female patients.
PNI=5 × Lymphocyte count (x109/L) + Serum albumin (g/L)
CAR =CRP (mg/L) /Albumin (g/L)
The CONUT score was calculated based on the degree of decrease in serum albumin concentration, total lymphocyte count, and total cholesterol concentration compared with the normal range. The albumin score was categorized as 0-2-4-6, while the lymphocyte count and total cholesterol score were both 0-1-2-3 (see Supplement Table S1).
Definition of Outcome Indicators
Patients were grouped according to clinically validated outcome thresholds. The primary outcome was prognosis: 3 months after the onset of stroke, two neurologists with over 10 years of experience assessed the patients’ mRS scores. The secondary outcomes were complications: After receiving treatment according to standard quality protocols, patients were closely monitored by a specialized medical and nursing team. Diagnosis of SAP, MCE, or END during hospitalization was defined as a secondary outcome indicator. The specific definitions are as follows:
Primary outcome indicator: The mRS ≥3 means a poor functional prognosis, ie, patients who were successfully revascularized may have received clinically ineffective reperfusion.3 Conversely, the mRS score < 3 indicates that reperfusion therapy was effective.
Secondary outcome indicators: (1) According to the 2015 consensus, the diagnostic criteria for SAP include clinical signs of pneumonia, such as fever, cough, and dyspnea, in patients with AIS within 1 week after stroke onset, and combined with a positive chest computed tomography scan or positive laboratory tests.20 SAP diagnosis was confirmed based on antibiotic administration records during hospitalization and medical records. (2) MCE was defined by clinical signs indicating brain herniation, including decreased consciousness and/or unequal pupils, along with significant imaging evidence of brain swelling, such as midline displacement of brain structures by >1 cm, or loss of basal cisterns.21,22 (3) END was defined as an increase in National Institute of Health Stroke Scale (NIHSS) score of ≥2 points from optimal neurologic functioning during the first 7 days after stroke onset.5
Analyze Statistics
Shapiro–Wilk’s test was used to evaluate the normality of the data distribution. Continuous variables were presented as mean ± standard deviation or median (25–75% quartiles) depending on normal distribution or not. Comparisons between the groups were conducted using the t-test or Mann–Whitney U-test. Categorical variables were presented as frequency (percentage) and compared using the χ2 test or Fisher’s exact test. Factors with statistically significant (p < 0.1) differences in univariate analyses were included in multivariate stepwise regression to determine the independent effect of each nutrition/inflammation-related indicator on outcome. The results were reported as odds ratios (ORs) and 95% confidence intervals (CIs). A post-hoc power analysis was performed to validate the sample size for significant differences (≥0.8 for adequate power validation), which was implemented in software G*Power 3.1.
To assess the predictive ability of various inflammatory-nutritional indicators for functional outcomes, we first constructed receiver operating characteristic (ROC) curves and calculated the area under the ROC curve (AUC) as an indicator of accuracy. Next, backward stepwise logistic regression analysis was performed to obtain the model with the smallest Akaike information criterion (AIC), which was used as the basic prediction model. The risk reclassification ability was assessed by calculating the Net Reclassification Improvement (NRI) and Integrated Discriminant Improvement (IDI) indices of the new model (basic prediction model combined with inflammatory-nutritional indicators) compared with the basic prediction model. The likelihood ratio test was also employed to determine whether the new model provided a better fit. Finally, subgroup analysis was applied to further validate the reliability of the results.
In addition, we converted the CALLY index into a categorical variable using the optimal cutoff value, determined by the highest specificity and sensitivity from the ROC curve, as the threshold for categorization. Whether it remained independently associated with functional prognosis was assessed by multivariate logistic regression analysis.
All statistical analyses were conducted by SPSS Statistics 27.0 and R 4.4.1. A two-sided p-value of less than 0.05 was considered statistically significant.
Results
Patient Demographics
A total of 249 AIS patients with anterior circulation who were successfully revascularized by EVT were included (Figure 1). The mean age of the cohort was 62 years, and 188 (75.5%) patients were male. 123 (49%) patients had a poor functional prognosis. Table 1 summarizes the characteristics of the study cohort, both for the entire group and for patients grouped by prognosis. Patients in the poor outcome group were older, had a lower percentage of smokers, higher admission NIHSS scores, higher fasting glucose levels and neutrophil counts, and lower systolic blood pressure, triglyceride levels and lymphocyte counts compared with those in the good outcome group (p<0.05).
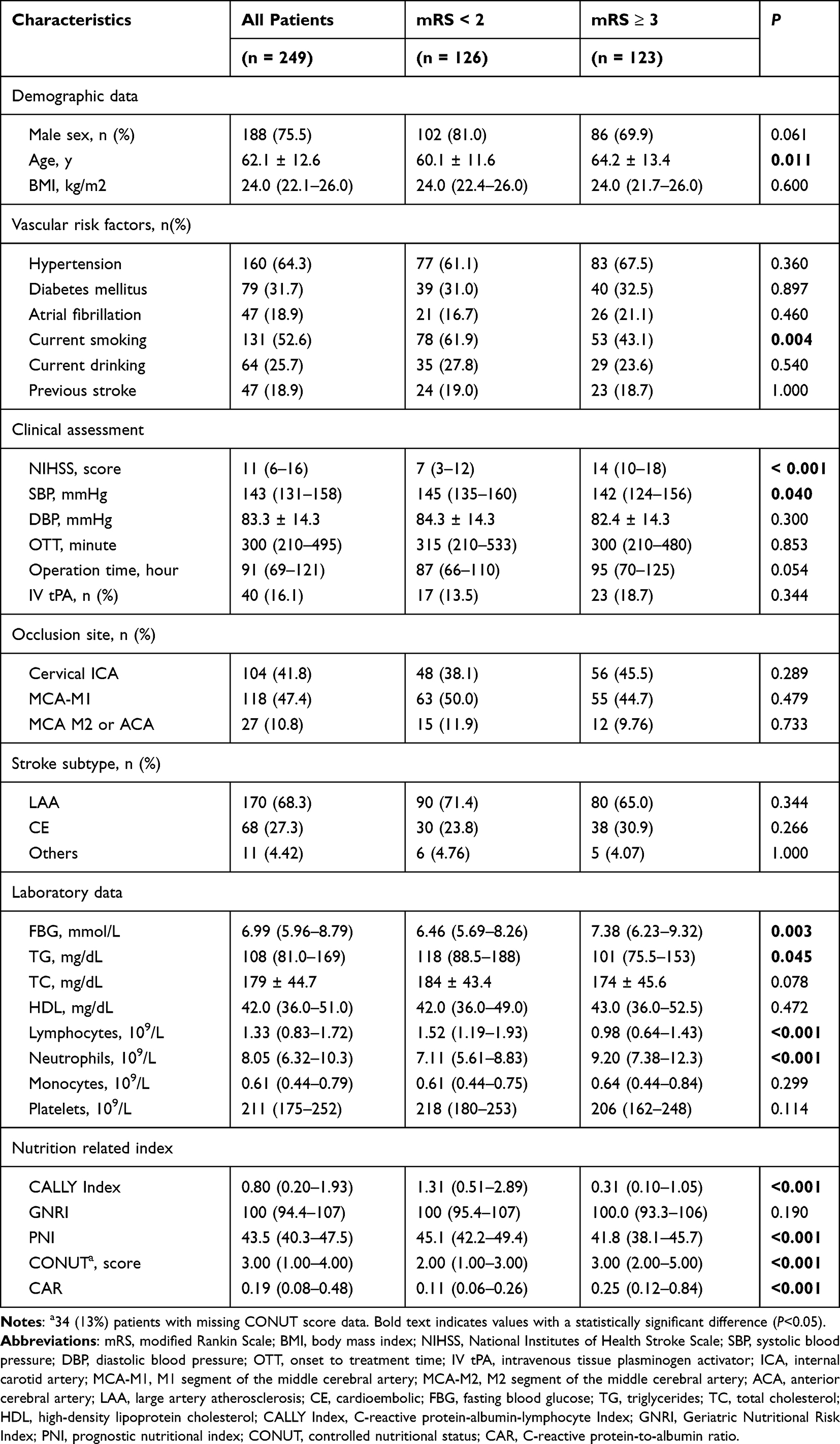 |
Table 1 Characteristics of Patients with Favorable and Unfavorable Functional Outcomes |
 |
Figure 1 Flow chart of study patients. Abbreviations: AIS, acute ischemic stroke; EVT, endovascular thrombectomy; mRS, modified Rankin Scale. |
Furthermore, several nutrition-related indicators significantly differed between the two patient groups. Patients in the poor outcome group had lower CALLY index (median 0.31 vs 1.31, p<0.001) and PNI (median 41.8 vs 45.1, p<0.001), but higher CONUT (median 3 vs 2, p<0.001) and CAR (0.25 vs 0.11, p<0.001) (Table 1).
Association Between Inflammatory-Nutritional Markers and Ineffective Recanalization of EVT in Patients with AIS
To determine the independent effects of each nutrition- and inflammation-related index on 3-month functional outcomes, variables that were significant in univariate analyses (p<0.1) and gender were included in multivariate analyses. Due to potential collinearity, nutrition- and inflammation-related variables were added to the regression model on a one-by-one basis. After adjusting for gender, age, smoking status, NIHSS score on admission, systolic blood pressure, surgical operation time, fasting blood glucose, triglycerides, and neutrophil count, in multivariate models the CALLY index (aOR, 0.759, 95% CI, 0.618–0.933, p=0.009), PNI (aOR, 0.915, 95% CI, 0.860–0.973, p=0.005) and CONUT scores (aOR, 1.273, 95% CI, 1.073–1.511, p=0.006) were significantly associated with functional outcome (Table 2).
 |
Table 2 Logistic Regression Analysis Associated with Unfavorable Functional Outcome |
Predictive Values of Various Nutritional and Inflammatory Indicators for Unfavorable Outcomes
First, the predictive ability of each nutrition/inflammation-related index was compared by calculating the AUC. The AUC value of the CALLY index was 0.73 (95% CI 0.68–0.79, p<0.001), with an optimal cutoff value of 0.83, a sensitivity of 0.72, and a specificity of 0.65. The CALLY index demonstrated the best discriminative power compared with the PNI and CONUT scores (Figure 2).
 |
Figure 2 Receiver operating characteristic (ROC) curve analysis performed to evaluate the predictive value of various nutrition related index for poor clinical outcome. Abbreviations: AUC, area under the curve; CALLY, Index C-reactive protein-albumin-lymphocyte Index; GNRI, Geriatric Nutritional Risk Index; PNI, prognostic nutritional index; CONUT, controlled nutritional status; CAR, C-reactive protein-to-albumin ratio. |
Next, the added predictive values of each nutritional and inflammatory indicator were assessed. A model with a minimum AIC value of 220.96 was adopted as the basic predictive model, which included four variables: baseline NIHSS score, operative time, smoking, and neutrophil count. Then the model’s risk assessment capability was evaluated by calculating NRI and IDI. The addition of PNI or CONUT scores to the base model only increased the model’s IDI. However, the inclusion of the CALLY index improved both the NRI (p = 0.028) and the IDI (p = 0.008), suggesting that adding the CALLY index enhances the model’s discriminatory power and risk reclassification for poor outcomes (Table 3). A likelihood ratio test further confirmed that the inclusion of the CALLY index significantly improved the predictive accuracy for poor prognosis (p < 0.05, Table 3).
 |
Table 3 Performance Metrics of Models with and Without Various Nutrition Index to Predict 90-Day Poor Functional Outcome After EVT |
Additionally, we analyzed the CALLY index as a categorical variable to investigate its association with poor prognosis. After adjusting for confounding variables, the CALLY index remained independently associated with poor outcomes (Supplement Table S2).
Subgroup Analysis of Poor Outcomes
To further validate the reliability of these findings, patients were stratified according to sex, age (>65 or ≤65 years), BMI (>24 or ≤24), smoking status, and history of hypertension and diabetes. The correlation between the CALLY index and prognosis after adjustment for confounders was analyzed. The results showed that a lower CALLY index was associated with an increased risk of poor prognosis, especially in patients with a BMI >24 and no history of smoking or diabetes (p<0.015, Figure 3).
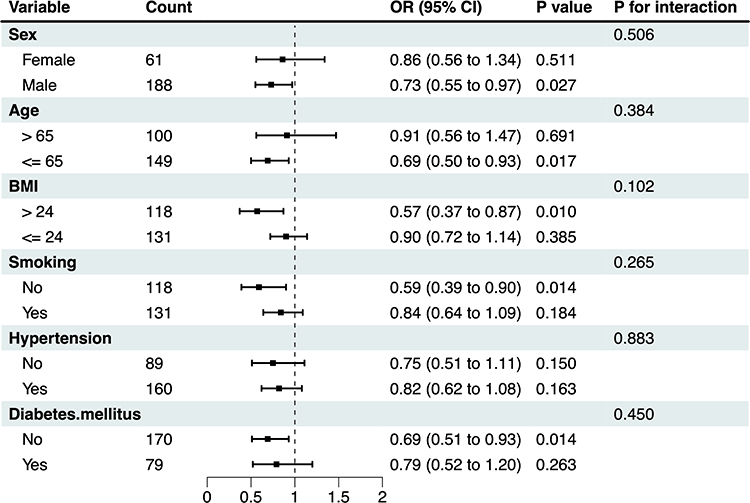 |
Figure 3 Subgroup analyses for the risk of poor outcomes by CALLY index. The above model is adjusted for sex, age, smoking, NIHSS score, operation time, systolic blood pressure, fasting blood glucose, triglycerides, and neutrophils. |
Relationship of CALLY Index with SAP, MCE, END
Compared with the higher CALLY group (CALLY ≥0.83), patients with lower CALLY index were older and had higher baseline NIHSS scores, higher baseline fasting glucose, total cholesterol, neutrophil and monocyte counts, and lower total triglycerides. Notably, the incidence of SAP, MCE, and END was significantly higher in the lower CALLY index group (p<0.05, Table 4).
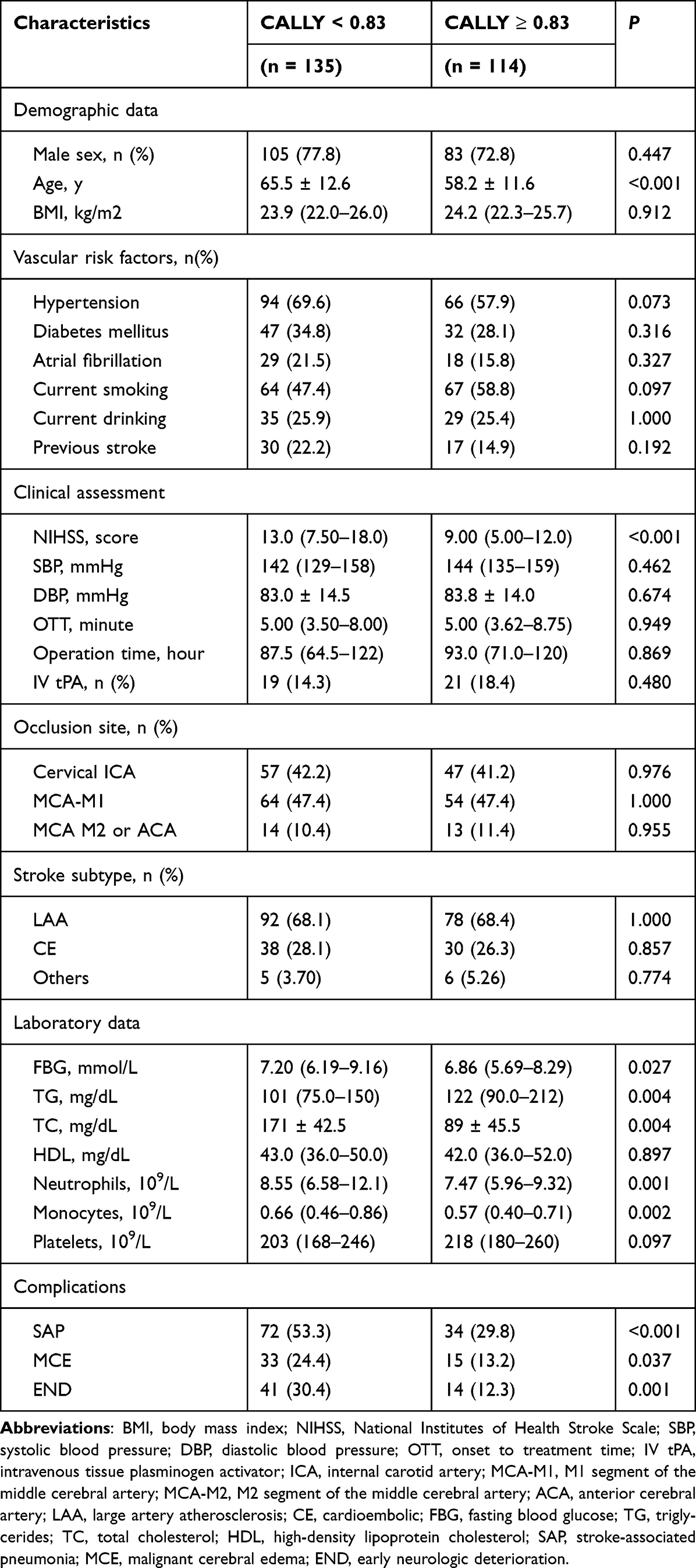 |
Table 4 Characteristics of Patients with Low and High CALLY Index |
To assess whether the CALLY index was an independent predictor of complications, logistic regression analysis was also used. Variables that were significant in univariate analyses (p<0.05) were included in the multivariate model (detailed information on analyses according to the grouping of complications is provided in Supplement Tables S3–S5). After adjusting for confounders separately, both as continuous and categorical variables, the association between the CALLY index and MCE and END was not significant in the multivariate logistic regression model (Table 5), however, the CALLY index was significantly associated with SAP (Continuous: aOR, 0.715, 95% CI, 0.555–0.921, p=0.009; Categorical: aOR, 2.123, 95% CI, 1.011–4.462, p=0.047).
 |
Table 5 Logistic Regression Analysis Associated with Stroke-Associated Pneumonia, Malignant Cerebral Edema and Early Neurologic Deterioration |
Discussion
In our study, we systematically investigated several key questions. First, in AIS patients treated with EVT, we found that selected nutritional and inflammation-related indicators such as CALLY Index, PNI and CONUT score could serve as independent predictors of poor outcomes. Based on ROC curve analysis and the evaluation of additional predictive value, the CALLY index emerged as the strongest predictor of prognosis. Specifically, a lower CALLY index was associated with a greater likelihood of poor functional outcomes. Second, the association between a lower CALLY index and increased risk of poor prognosis was most pronounced in AIS patients with a BMI >24. Finally, after adjusting for confounders, a reduced CALLY index emerged as an independent risk factor for SAP, although it was not a significant predictor of END or MCE.
The CALLY index demonstrated superior prognostic performance in our study, which integrates not only inflammation and nutritional reserve, but also immune status. It effectively predicted 3-month functional outcomes in EVT-treated patients (AUC>0.7) and enhanced the accuracy and comprehensiveness of the predictive model compared with established markers like the CONUT score and PNI. The CALLY index’s superior predictive ability may be partly attributed to the role of immune status. Lymphocytes which can indicate immune status are pivotal in the development and progression of AIS, influencing neuroinflammation through various pathways, including immune modulation, interactions with brain-resident immune cells, and the regulation of neurogenesis and angiogenesis.23,24 The findings of our study support the incorporation of the CALLY index in the evaluation process of stroke patients undergoing EVT. Meanwhile, 0.83 can be used as a threshold for the CALLY index to assess the need for more aggressive nutritional support and anti-inflammatory therapy.
The potential mechanisms underlying associations between nutrition, inflammation, immune status and outcomes are multifaceted. Firstly, the immune system, sympathetic nervous system, and hypothalamic-pituitary-adrenal axis are activated during the onset of stressors such as stroke.25–27 The release of pro-inflammatory cytokines, including interleukin 6, interleukin 1β, and tumor necrosis factor-alpha (TNF-α), triggers various pathogenetic mechanisms of malnutrition, like physiological processes affecting appetite, protein catabolism, and synthesis.28,29 Previous animal studies have shown that protein-energy malnutrition can affect neuroinflammation in stroke patients, in addition to causing a decrease in peripheral immune function.30 Malnourished stroke patients have an impaired ability to maintain immune homeostasis by balancing oxidative and pro-inflammatory mediator production, which might hinder clinical recovery. Secondly, the disruption of cerebral blood flow following a stroke leads to blood-brain barrier (BBB) compromise, with damaged neurons releasing damage-associated molecular patterns into the systemic circulation via the BBB and cerebrospinal fluid drainage system, inducing a systemic inflammatory response. Importantly, stroke can induce long-term inflammatory changes in monocytes/macrophages systemically, thereby driving multi-organ dysfunction, which has also been confirmed in stroke mouse models.31 Similarly, various leukocyte subtypes infiltrate the brain parenchyma causing secondary damage, eg, infiltrating neutrophils mediate reactive oxygen species and matrix metalloproteinases regulating BBB damage and promoting further infiltration of peripheral immune cells.32–34 In conclusion, the interactions between malnutrition, systemic inflammation, and oxidative stress may have a synergistic effect that impairs physiological reserves and diminishes the ability of stroke patients to recover function.
The relationship between obesity, malnutrition, and prognosis remains controversial. A cohort study found no significant differences in poor outcome incidence between obese and non-obese malnourished patients.35 Conversely, some studies suggest that maintaining weight may support rehabilitation of daily living activities in malnourished stroke patients.36 These conflicting findings may be attributable to inconsistencies in methods and criteria used to define malnutrition and obesity across studies. In our study, the association between a lower CALLY index and an increased risk of poor prognosis appeared to be more significant in the group of patients with a BMI >24. This result may indicate that the coexistence of overweight and malnutrition exacerbates stroke prognosis. But we must notice that in our subgroup analyses, the interaction between BMI and CALLY index was not statistically significant, which suggests that the reliability of the results obtained after grouping according to BMI is weak and therefore the relationship between these variables is uncertain. We still need to conduct more large-sample studies to explore this in the future.
The association between CALLY index and SAP is in line with our previous hypothesis. Stroke induces an immunosuppressive state, which in turn increases the susceptibility to SAP. Immunosuppressive markers help identify patients at higher risk for this complication.37,38 Malnutrition could aggravate immunosuppression. Previous studies have shown that malnourished patients are more likely to develop pneumonia, as well as other infections and gastrointestinal bleeding during hospitalization.8 Experimental studies further suggest macrophages and monocytes from malnourished mice expressed significantly higher levels of arginase, both in vitro and in vivo, which as an enzyme associated with immunosuppression and increased pathogen replication can increase an individual’s susceptibility to infection.39 In contrast to the relationship with SAP, the relationship between the CALLY index and END or MCE was not significant. We believe there may be several reasons for this. First, END and MCE are more localized complications, and the CALLY index, which reflects systemic status, has a relatively weak effect on them. The second is that END and MCE were present in only 55 (22%) and 48 (19%) patients, and future studies with larger sample sizes are needed to validate the relationship between them.
This study is the first to evaluate the CALLY index as an independent predictor of functional prognosis in AIS patients who have undergone EVT. The CALLY index demonstrates higher accuracy compared with other nutritional and inflammatory markers, making it a valuable tool for early prediction of poor functional recovery and complications like SAP. The CALLY index, being simple to calculate and easily available from routine clinical data, significantly enhances the feasibility of identifying patients at risk for adverse outcomes after EVT. This underscores its clinical utility as a convenient and reliable marker for identifying high-risk patients who may benefit from targeted monitoring and early intervention.
Certainly, there are limitations to our existence. First, this study is a single-center retrospective observational study, which requires further validation by large-scale prospective studies involving multiple centers. Second, our research lacks serial biomarker monitoring. This makes it impossible to analyze the causal relationship between dynamic changes and prognosis. In addition, the absence of nutritional intervention hinders the assessment of whether early nutritional intervention can improve prognosis. Third, although we excluded patients with significant motion artifacts through strict imaging quality control, we acknowledge that including patients with mild artifacts may still influence the assessment of clinical outcomes. Finally, the CALLY index was not as effective as expected in predicting the occurrence of END and MCE complications, although this may be explained by the small sample size of this study. Thus, these limitations highlight the need for future prospective studies incorporating long-term biomarker assessments and protocolized nutritional support to elucidate the comprehensive impact of nutrition-inflammation dynamics on ischemic stroke outcomes.
Conclusion
Various index, such as CALLY index, PNI and CONUT score, are independent predictors of futile reperfusion in AIS patients undergoing EVT. CALLY index has the best predictive value, especially in BMI> 24 patients. In addition, a lower CALLY index was also associated with an increased risk of SAP, while it was not significantly with MCE or END.
Data Sharing Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author Yongming Wu upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Nanfang Hospital’s ethics committee on clinical research (NFEC-2024-646). All participants provided their written informed consent.
Consent to Participate
Informed consent has been obtained from all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Guangdong Basic and Applied Basic Research Foundation, 2023A1515220136.
Disclosure
There is no conflict of interest.
References
1. Berkhemer OA, Fransen PS, Beumer D, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015;372(1):11–20. doi:10.1056/NEJMoa1411587
2. Albers GW, Marks MP, Kemp S, et al. Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging. N Engl J Med. 2018;378(8):708–718. doi:10.1056/NEJMoa1713973
3. Nie X, Leng X, Miao Z, Fisher M, Liu L. Clinically ineffective reperfusion after endovascular therapy in acute ischemic stroke. Stroke. 2023;54(3):873–881. doi:10.1161/strokeaha.122.038466
4. Krishnan R, Mays W, Elijovich L. Complications of mechanical thrombectomy in acute ischemic stroke. Neurology. 2021;97(20 Suppl 2):S115–s125. doi:10.1212/wnl.0000000000012803
5. Kim JM, Bae JH, Park KY, et al. Incidence and mechanism of early neurological deterioration after endovascular thrombectomy. J Neurol. 2019;266(3):609–615. doi:10.1007/s00415-018-09173-0
6. Saleem Y, Nogueira RG, Rodrigues GM, et al. Acute neurological deterioration in large vessel occlusions and mild symptoms managed medically. Stroke. 2020;51(5):1428–1434. doi:10.1161/strokeaha.119.027011
7. Huppertz V, Guida S, Holdoway A, et al. Impaired nutritional condition after stroke from the hyperacute to the chronic phase: a systematic review and meta-analysis. Front Neurol. 2021;12:780080. doi:10.3389/fneur.2021.780080
8. FOOD Trial Collaboration. Poor nutritional status on admission predicts poor outcomes after stroke: observational data from the FOOD trial. Stroke. 2003;34(6):1450–1456. doi:10.1161/01.Str.0000074037.49197.8c
9. Di Vincenzo O, D’Elia L, Ballarin G, Pasanisi F, Scalfi L. Controlling Nutritional Status (CONUT) score and the risk of mortality or impaired physical function in stroke patients: a systematic review and meta-analysis. Nutr Metab Cardiovasc Dis. 2023;33(8):1501–1510. doi:10.1016/j.numecd.2023.05.012
10. Dziedzic T, Slowik A, Szczudlik A. Serum albumin level as a predictor of ischemic stroke outcome. Stroke. 2004;35(6):e156–8. doi:10.1161/01.STR.0000126609.18735.be
11. Zhang M, Ye S, Huang X, et al. Comparing the prognostic significance of nutritional screening tools and ESPEN-DCM on 3-month and 12-month outcomes in stroke patients. Clin Nutr. 2021;40(5):3346–3353. doi:10.1016/j.clnu.2020.11.001
12. Macrez R, Ali C, Toutirais O, et al. Stroke and the immune system: from pathophysiology to new therapeutic strategies. Lancet Neurol. 2011;10(5):471–480. doi:10.1016/s1474-4422(11)70066-7
13. Ciancarelli I, Morone G, Iosa M, et al. Influence of oxidative stress and inflammation on nutritional status and neural plasticity: new perspectives on post-stroke neurorehabilitative outcome. Nutrients. 2022;15(1):108. doi:10.3390/nu15010108
14. Chandra RK. Nutrition and the immune system from birth to old age. Eur J Clin Nutr. 2002;56 Suppl 3(S3):S73–6. doi:10.1038/sj.ejcn.1601492
15. Takele Y, Adem E, Getahun M, et al. Malnutrition in healthy individuals results in increased mixed cytokine profiles, altered neutrophil subsets and function. PLoS One. 2016;11(8):e0157919. doi:10.1371/journal.pone.0157919
16. Yuan J, Cheng Y, Han X, et al. Association between C-reactive protein/albumin ratio and all-cause mortality in patients with stroke: evidence from NHANES cohort study. Nutr Metab Cardiovasc Dis. 2024;34(10):2305–2314. doi:10.1016/j.numecd.2024.05.024
17. Hou C, Huang X, Wang J, et al. Inflammation and nutritional status in relation to mortality risk from cardio-cerebrovascular events: evidence from NHANES. Front Nutr. 2024;11:1504946. doi:10.3389/fnut.2024.1504946
18. Zhao G, Chen Y, Gu Y, Xia X. The clinical value of nutritional and inflammatory indicators in predicting pneumonia among patients with intracerebral hemorrhage. Sci Rep. 2024;14(1):16171. doi:10.1038/s41598-024-67227-y
19. Ji H, Luo Z, Ye L, et al. Prognostic significance of C-reactive protein-albumin-lymphocyte (CALLY) index after primary percutaneous coronary intervention in patients with ST-segment elevation myocardial infarction. Int Immunopharmacol. 2024;141:112860. doi:10.1016/j.intimp.2024.112860
20. Smith CJ, Kishore AK, Vail A, et al. Diagnosis of stroke-associated pneumonia: recommendations from the pneumonia in stroke consensus group. Stroke. 2015;46(8):2335–2340. doi:10.1161/strokeaha.115.009617
21. Wu S, Yuan R, Wang Y, et al. Early prediction of malignant brain edema after ischemic stroke. Stroke. 2018;49(12):2918–2927. doi:10.1161/strokeaha.118.022001
22. Wang C, Zhu Q, Cui T, et al. Early prediction of malignant edema after successful recanalization in patients with acute ischemic stroke. Neurocrit Care. 2022;36(3):822–830. doi:10.1007/s12028-021-01380-4
23. Lei TY, Ye YZ, Zhu XQ, et al. The immune response of T cells and therapeutic targets related to regulating the levels of T helper cells after ischaemic stroke. J Neuroinflammation. 2021;18(1):25. doi:10.1186/s12974-020-02057-z
24. Wang H, Zhang S, Xie L, Zhong Z, Yan F. Neuroinflammation and peripheral immunity: focus on ischemic stroke. Int Immunopharmacol. 2023;120:110332. doi:10.1016/j.intimp.2023.110332
25. Morley JE, Thomas DR, Wilson MM. Cachexia: pathophysiology and clinical relevance. Am J Clin Nutr. 2006;83(4):735–743. doi:10.1093/ajcn/83.4.735
26. Preiser JC, Ichai C, Orban JC, Groeneveld AB. Metabolic response to the stress of critical illness. Br J Anaesth. 2014;113(6):945–954. doi:10.1093/bja/aeu187
27. Mueller B, Figueroa A, Robinson-Papp J. Structural and functional connections between the autonomic nervous system, hypothalamic-pituitary-adrenal axis, and the immune system: a context and time dependent stress response network. Neurol Sci. 2022;43(2):951–960. doi:10.1007/s10072-021-05810-1
28. Stumpf F, Keller B, Gressies C, Schuetz P. Inflammation and nutrition: friend or foe? Nutrients. 2023;15(5). doi:10.3390/nu15051159
29. Lambertsen KL, Biber K, Finsen B. Inflammatory cytokines in experimental and human stroke. J Cereb Blood Flow Metab. 2012;32(9):1677–1698. doi:10.1038/jcbfm.2012.88
30. Alaverdashvili M, Caine S, Li X, et al. Protein-energy malnutrition exacerbates stroke-induced forelimb abnormalities and dampens neuroinflammation. Transl Stroke Res. 2018;9(6):622–630. doi:10.1007/s12975-018-0613-3
31. Simats A, Zhang S, Messerer D, et al. Innate immune memory after brain injury drives inflammatory cardiac dysfunction. Cell. 2024;187(17):4637–4655.e26. doi:10.1016/j.cell.2024.06.028
32. Herz J, Sabellek P, Lane TE, Gunzer M, Hermann DM, Doeppner TR. Role of neutrophils in exacerbation of brain injury after focal cerebral ischemia in hyperlipidemic mice. Stroke. 2015;46(10):2916–2925. doi:10.1161/strokeaha.115.010620
33. Kolaczkowska E, Kubes P. Neutrophil recruitment and function in health and inflammation. Nat Rev Immunol. 2013;13(3):159–175. doi:10.1038/nri3399
34. Forrester SJ, Kikuchi DS, Hernandes MS, Xu Q, Griendling KK. Reactive oxygen species in metabolic and inflammatory signaling. Circ Res. 2018;122(6):877–902. doi:10.1161/circresaha.117.311401
35. Niu H, Chu M, Yang N, et al. Prognosis of patients with coexisting obesity and malnutrition after ischemic stroke: a cohort study. Clin Nutr. 2024;43(5):1171–1179. doi:10.1016/j.clnu.2024.04.005
36. Nishioka S, Wakabayashi H, Nishioka E, Yoshida T, Mori N, Watanabe R. Nutritional improvement correlates with recovery of activities of daily living among malnourished elderly stroke patients in the convalescent stage: a cross-sectional study. J Acad Nutr Diet. 2016;116(5):837–843. doi:10.1016/j.jand.2015.09.014
37. Hoffmann S, Harms H, Ulm L, et al. Stroke-induced immunodepression and dysphagia independently predict stroke-associated pneumonia - The PREDICT study. J Cereb Blood Flow Metab. 2017;37(12):3671–3682. doi:10.1177/0271678x16671964
38. Li J, Luo H, Chen Y, et al. Comparison of the predictive value of inflammatory biomarkers for the risk of stroke-associated pneumonia in patients with acute ischemic stroke. Clin Interv Aging. 2023;18:1477–1490. doi:10.2147/cia.S425393
39. Corware K, Yardley V, Mack C, et al. Protein energy malnutrition increases arginase activity in monocytes and macrophages. Nutr Metab. 2014;11(1):51. doi:10.1186/1743-7075-11-51
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.